This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set A8E923)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
A woman has an X-linked dominant condition (single allele being dominant). Which of the following is true:
1
25% of the offspring will be affected
2
100% of the daughters will be affected
3
25% of the sons will be affected
4
100% of the sons will be affected
5
50% of the offspring will be affected
With X-linked dominant, heterozygotes will have the condition. If a woman has this condition, then she will transmit it to 50% of her sons and daughters.
In contrast, affected men transmit the condition to all of his daughters (because the daughter gets his X chromosome), but to none of the sons because the son gets the Y chromosome.
With X-linked recessive, the patterns are different between women and men.
X-linked recessive woman: An X-linked woman with the recessive allele is a carrier, but she is not affected because the allele is recessive.
C arrier females (X-linked recessive) transmit the condition to 50% of her daughters (who become carriers) and 50% of her sons
(the sons are affected because their only X chromosome has the recessive gene). Correct Answer: 50% of the offspring will be affected
QUESTION 2 OF 50
Which of the following proteins or genes is necessary for bone formation and induces osteocalcin:
C ore binding factor alpha 1 (C bfa1) and its gene (Cbfa1) have been described as anabolic regulators of bone. C bfa1 is a transcription factor and is responsible for the differentiation of precursor cells into osteoblasts. It also enhances differentiation of chondrocytes during enchondral bone formation. When there is deficiency of C bfa1, there can be abnormal bone development as in cleidocranial dysplasia.
QUESTION 3 OF 50
What nerve is most frequently injured at the time of a periprosthetiCfracture of the humerus:
1
Median nerve
2
Ulnar nerve
3
Radial nerve
4
Musculocutaneous nerve
5
Axillary nerve
The radial nerve is the most frequently injured nerve at the time of a periprosthetiCfracture. There continues to be debate as to whether the presence of a radial nerve injury constitutes a reason for revision surgery
QUESTION 4 OF 50
of 100
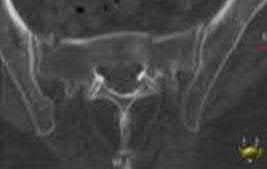
During the workup of her hearing loss, a 21-year-old woman had imaging which lead to further imaging of her spine shown in Figures 1 and
1
She was also noted to be anemic. Her mother died when she was young, and she was told her grandmother had a “bone disease”. Her endocrinologist has diagnosed her with Albers-Schonberg disease. What is the cause of her disease?

2
Mutations in the chloride 7 (CLCN7) gene
3
Mutations in cathepsin K (CTSK) gene
4
Consumption of lead
5
Mutations in tissue non-specific alkaline phosphatase (TNSALP)
■ The patient has autosomal dominant osteopetrosis type II, which is also known as AlbersSchonberg disease. It can be associated with sclerosis of the skull base, leading to cranial nerve dysfunction such as hearing loss. It is also associated with marrow replacement leading to anemia and can be associated with fractures. The images show increased bone density, and osteopetrosis type II can be associated with a “bone within a bone” type appearance. CTSK mutations are associated with pyknodysostosis, and TNSALP is associated with hypophosphatasia. Lead poisoning would not present with these findings.
QUESTION 5 OF 50
Which of the following is true of a knee disarticulation as compared to a transtibial amputation?
1
Faster self-selected walking speeds
2
Improved performance on the Sickness Impact Profile (SIP) questionnaire
3
Physicians were more satisfied with the cosmetic appearance
4
Decreased use of a prosthetic
5
Decreased dependence with patient transfers
Knee disarticulation level is associated with the worst functional result 2 years after injury (compared to transmetatarsal, Symes, AKA, or BKA). The prosthetic use is decreased with a knee disarticulation as compared to a transtibial amputation.
The cohort study by MacKenzie et al prospectively followed 161 patients that were part of the Lower Extremity Assessment Project (LEAP). These patients underwent an above-the-ankle amputation at a trauma center within 3 months following the injury and followed for 2 years. This study revealed that through-the-knee amputations had significantly worse scores for the objective performance measures of self-selected walking speed, independence in transfers, walking, and stair-climbing. Through-the-knee amputees also had worse SIP scores than AKA and BKA patients. Physicians were also less satisfied with both the clinical and the cosmetic recovery of the patients with a through-the-knee amputation. It should be noted that patients with a BKA had a faster walking speed than those with an AKA. Despite the worse SIP scores for through-the-knee amputations, patients actually reported less pain than those with an AKA or BKA, though this wasn't statistically significant.
QUESTION 6 OF 50
of 100
A 21-year-old collegiate baseball player experiences posterior shoulder pain in the lead shoulder while batting.
1
Isolated posterior instability with a posterior labral tear
2
Multidirectional instability
3
Anterior shoulder subluxation
4
Thoracic outlet syndrome
5
Superior labrum anterior to posterior (SLAP) tear
- Isolated posterior instability with a posterior labral tear_
QUESTION 7 OF 50
A 23-year-old woman has had a 3-year history of snapping and pain in her left hip. She notes that the snapping started while marathon training and is only problematic about 15 minutes into a run. Examination is consistent with a negative Stinchfield, negative logroll, negative flexion abduction/external rotation test (FABER) of the hip; however, she has a positive Ober test as she has difficulty adducting her hip across the midline in the lateral decubitus position. Management consisting of nonsteroidal antiinflammatory drugs and stretching has failed to improve her snapping. What is the most reliable surgical treatment?
1
Hip arthroscopy with labral debridement
2
Hip arthroscopy with femoral acetabular impingement lesion debridement
3
Release of the iliopsoas tendon
4
Z-plasty of the iliotibial band
5
Release of the iliotibial band at Gerdy’s tubercle
DISCUSSION: The patient has external-type snapping hip (coxa saltans). It is not uncommon for patients to have a very long duration of symptoms that limit running or other sporting activities, and commonly affects the downward leg (usually the left leg when running on the left side of the road). The snapping causes a profound bursitis at the greater trochanter, and occasionally corticosteroid injections may be helpful. Her physical examination does not suggest an intra-articular process, and is not consistent with an internal-type snapping hip, usually caused by the iliopsoas tendon as it moves over the iliopectineal eminence. Stretching is the mainstay of treatment, as testing with a positive Ober signifies a tight iliotibial band as the thigh has difficulty crossing the midline with adduction. Various iliotibial band lengthening procedures have been described, including a Z-plasty near the proximal origin of the iliotibial band. Release at Gerdy’s tubercle has not been described.
REFERENCES: Provencher MT, Hofmeister EP, Muldoon MP: The surgical treatment of external coxa saltans (the snapping hip) by Z-plasty of the iliotibial band. Am J Sports Med 2004;32:470-476.
Faraj A A, Moulton A, Sirivastava VM: Snapping iliotibial band: Report of ten cases and review of the literature. Acta Orthop Belg 2001;67:19-23.
Brignall CG, Stainsby GD: The snapping hip: Treatment by Z-plasty. J Bone Joint Surg Br 1991 ;73:253-
254.
QUESTION 8 OF 50
of 100
A 37-year-old man with an irreducible posterior 2-part proximal humerus fracture dislocation
1
Initial period of sling immobilization followed by physical therapy
2
Open reduction and internal fixation with or without bone grafting
3
Reverse total shoulder arthroplasty (rTSA)
4
Hemiarthroplasty
5
Unconstrained (TSA)
- Open reduction and internal fixation with or without bone grafting_
QUESTION 9 OF 50
The oblique retinacular ligament connects with what two structures:
1
Flexor tendon to lateral extensor tendon
2
Flexor tendon to central slip
3
Flexor tendon sheath to lateral extensor tendon
4
Flexor tendon sheath to central slip
5
Flexor tendon sheath to head of middle phalanx
Landsmeer (oblique retinacular ligament) runs from the flexor tendon sheath of the proximal phalanx to the lateral extensor tendon as they insert onto the base of the proximal phalanx. A stay or retaining ligament maintains centralization of the extensor tendons.
QUESTION 10 OF 50
Commercially available polymethylmethacrylate cement formulations vary in the consistency of the material as part of its inherent properties. What is the clinical difference between high- and low-viscosity cement formulations?
1
High-viscosity cement has a shorter working time and is a liquid consistency
2
High-viscosity cement has a longer working time and is a doughy consistency.
3
Low-viscosity cement has a longer working time and is a liquid consistency.
4
Lo…w-viscosity cement has a shorter working time and is a doughy
consistency.
Viscosity is the measure of resistance of a fluid to deform under force or the resistance to flow (ie, thickness of a fluid). The lower the viscosity, the more water-like the bone cement will be; the higher the viscosity, the more doughy the bone cement will be after mixing. Additionally, as the cement polymerizes, the process is broken down into four phases: mixing, waiting, working and hardening. Ideally, we would like a cement to have a short mixing, waiting and hardening time and a long working time. The working time is the period of time during which the cement is manageable to use for cementing implants into place. The cement must penetrate into the cancellous bone for it to function like a “grout” as it is supposed to do. There has been a recent push to use high-viscosity cement in total knee arthroplasty, despite concerns that the doughier cement may not penetrate the bone as well. Based on the properties of cement, high-viscosity cement is doughier with a shorter waiting and mixing time and a longer working time versus low-viscosity cement, which is runnier and has a shorter working time.
QUESTION 11 OF 50
A 45-year-old man who underwent an open capsulolabral stabilization procedure
15 years ago now reports pain and has no external rotation on the affected side. Nonsurgical management has failed to provide relief. Examination reveals external rotation to -5 degrees compared with 50 degrees of external rotation on the contralateral side. Radiographs show a small inferior osteophyte and minimal posterior glenoid wear. Which of the following procedures will offer the best chance of restoring motion, decreasing pain, and preserving the native joint?
1
Arthroscopic removal of the osteophytes
2
Arthroscopic debridement and acromioplasty
3
Arthroscopic release of the posterior capsule
4
Release of the rotator interval and anterior capsule
5
Closed manipulation under anesthesia
Loss of external rotation following stabilization procedures can result in progressive degenerative joint disease. A tight anterior capsule results in posterior humeral translation and progressive posterior glenoid wear. Patients with early degenerative joint disease and pain can be treated with anterior release to restore more normal glenohumeral biomechanics. This procedure not only improves function but also decreases pain in most patients. Closed manipulation at 15 years after surgery is unlikely to be successful and carries the risk of complications. Acromioplasty, posterior release, and removal of osteophytes do not address the pathology. Arthroscopic releases are favored for intra-articular procedures that have addressed the pathology of instability. Open releases are recommended for nonanatomic extra-articular repairs that include subscapularis tightening procedures.
REFERENCES: MacDonald PB, Hawkins RJ, Fowler PJ, et al: Release of the subscapularis for internal rotation contracture and pain after anterior repair for recurrent anterior dislocation of the shoulder. J Bone Joint Surg Am 1992;74:734-737.
Warner JJ, Allen AA, Marks PH, et al: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
QUESTION 12 OF 50
A 12-year-old boy has a head-on head collision while playing soccer. He had no loss of consciousness
but has persistent headaches for 2 weeks. The patient is now back to school and has no headaches. What is the best next step?
1
Return to full soccer activity
2
Start light aerobic activity
3
Obtain baseline neuropsychological testing
4
MRI scan of the brain
Mild traumatic brain injury is common in the adolescent child. Neuropsychological examination is widely used but, in this case, the patient is asymptomatic and has no baseline testing. There is a limited role for MRI in the recovery process of concussions. Furthermore, higher levels of physical/cognitive activity should be avoided due to their potential to increase total recovery time. In this scenario, a graduated return to activity is most appropriate thus, the next appropriate step is to start light aerobic activity.
QUESTION 13 OF 50
Figures 9a and 9b are the radiographs of a 32-year-old woman who has right foot pain after falling down a few steps. For the best long-term outcome, initial treatment should include which of the following? ---
1
Splinting with non-weight-bearing as the definitive treatment
2
Walking boot
3
Closed reduction and casting
4
Percutaneous pinning
5
Primary open reduction and internal fixation (ORIF)
The radiographs show a displaced Lisfranc injury. The outcome of treatment is dependent on achieving an anatomic reduction and stabilization, which is only possible with primary ORIF. Some studies indicate primary fusion may provide superior short-term results compared with ORIF. Closed treatment (reduction with casting or splinting) will not achieve or maintain the reduction, whereas delayed treatment by secondary fusion after arthritis occurs yields inferior outcomes to primary ORIF.
---
QUESTION 14 OF 50
of 100
Six months later, the patient’s fracture has healed and a CT scan to further evaluate the physis is performed (Video 85). Based on these findings, how should you advise the family?
1
The fracture is healed and the physis is growing well with no problems expected.
2
Complete physeal closure has occurred. There will be no significant leg length difference because the patient is almost done growing.
3
Complete physeal closure has occurred. There will be a significant (> 2-cm) leg length difference if no other surgical treatment is offered.
4
Asymmetric physeal closure has occurred. There will be an increasing angular deformity at the knee as well as a significant (> 2-cm) leg length difference if no other surgical treatment is offered.
The hypertrophic zone is the weakest biomechanical zone of the physis and is most likely to fracture. The deep peroneal nerve supplies motor innervation to the ankle and toe
dorsiflexors (anterior compartment) and the first web space, which, in this history, have deficits. The superficial peroneal nerve supplies sensation to the dorsum of the foot and motor to the lateral compartment peroneal musculature (ankle evertors), which also has deficits. The injury must involve both peroneal branches (the common peroneal nerve). Because sensation to the sole of the foot and toe/ankle plantar flexion is intact, the tibial nerve is intact.
Because the nerve was visualized intact, a neuropraxia is the most likely type of nerve injury. This should recover in time and does not necessitate urgent exploration. In pediatric patients, an advancing Tinel sign and partial nerve recovery by 3 months is expected and can be followed clinically. If there is no sign of nerve recovery, an electromyogram should be ordered with consideration for nerve exploration if there is no sign of reinnervation. There is no sign of compartment syndrome because the patient has an unchanged neurologic deficit, is comfortable, and has no pain with passive range of motion.
These injuries are associated with a very high rate of growth arrest (up to 80% in some studies). The CT scan shows an asymmetric growth arrest, which suggests angulation through the distal femur.
QUESTION 15 OF 50
of 100
A 45-year-old man has motor weakness of the quadriceps and tibialis anterior, sensory loss of the medial calf, and loss of the knee jerk reflex on his left.
1
Figure 72a Figure 72b
2
Figure 72c Figure 72d
3
Figure 72e Figure 72f
4
Figure 72g Figure 72h
- Figure 72c Figure 72d
QUESTION 16 OF 50
In the evaluation of somatosensory-evoked potential waveforms for intraoperative neuromonitoring for spinal surgery, the minimum criteria for determining potentially significant changes include
1
10% decrease in amplitude, 50% decrease in latency.
2
10% decrease in amplitude, 50% increase in latency.
3
0% loss of amplitude, transient increase in latency.
4
50% decrease in amplitude, 10% increase in latency.
5
50% decrease in amplitude, 10% decrease in latency.
The established criteria for interpreting a significant change are 50% decrease in signal amplitude, 10% latency increase, and/or a complete loss of potential. Intraoperative spinal cord monitoring during spinal surgery generally consists of a combination of monitoring modalities.Somatosensory-evoked potentials in combination with intraoperative electromyography can provide adequate coverage of sensory and motor components of spinal cord and nerve root function. Significant changes in evoked potential waveform characteristics can reflect dysfunction of the ascending somatosensory system.
QUESTION 17 OF 50
Which of the following biomaterials is considered inert:
1
Porous tantalum
2
Autologous chondrocytes
3
Biodegradable polymeric scaffolds
4
C alcium sulfate pellets
5
C obalt-chromium alloys
Biocompatibility refers to materials that can be implanted into the body without causing major adverse reactions. Some materials, such as cobalt chromium alloys, are essentially inert; these materials cause no reaction from the body.
Other materials might be biocompatible, but they are not inert: Porous tantalum is a metal material that grows into bone.
Autologous chondrocytes are grown in vitro and then used as filler for cartilage defects.
Biodegradable polymeric scaffolds are resorbed and new tissues are laid down upon them.
C alcium sulfate pellets are quickly resorbed over a 4- to 6-week period and new bone formation occurs either completely or incompletely.
C orrect Answer: C obalt-chromium alloys
QUESTION 18 OF 50
Which nerve is NOT one of the terminal branches of Baxterâs nerve, also known as the first branch of the lateral plantar nerve:
1
Nerve to the medial calcaneal periosteum (sensory)
2
Lateral dorsal cutaneous nerve (sensory)
3
Nerve to the flexor digitorum brevis muscle (motor)
4
Nerve to the abductor digiti minimi muscle (motor)
5
None of the above
The three terminal branches of Baxterâs nerve are the nerve to the medial calcaneal periosteum, the nerve to the flexor digitorum brevis, and the nerve to the abductor digiti minimi. The lateral dorsal cutaneous nerve is a branch of the sural nerve.
QUESTION 19 OF 50
of 100
Figures 1 and 2 are the lumbar spine radiographs of a 72-year-old man with no significant medical history who has had severe back pain for 3 weeks. He denies radiating symptoms, weakness, or numbness when he is seen in the emergency department. He is sent home with a soft corset. At his follow-up visit he continues to describe significant back pain with activity that is not relieved with oral narcotic mediations. A follow-up CT scan shows a nondisplaced fracture through all 3 columns of the spine. What is the most appropriate treatment?
1
Nonsteroidal anti-inflammatory drugs (SAIDS), physical therapy, and activity modification
2
Continued soft corset use
3
Thoracolumbosacral orthosis (TLSO) bracing
4
Posterior stabilization
■ The patient has previously undiagnosed ankylosing spondylitis. Radiographs reveal nonmarginal syndesmophytes throughout the lumbar spine. The CT scan reveals a nondisplaced 3-column fracture. Many patients with missed spinal injuries present in followup with neurologic worsening or progressive deformity. Fractures can often involve all 3 columns, including the posterior elements. In patients with ankylosing spondylitis, this represents an unstable injury and a high likelihood of displacement with nonsurgical treatment. Surgical treatment in the form of a posterior spinal fusion is indicated. Because the fracture is nondisplaced and the patient is neurologically intact, decompression via an anterior approach is not indicated. Bracing either with a TLSO brace or a soft corset will not provide sufficient stability for this fracture pattern. Physical therapy and NSAIDS are not indicated in this scenario.
QUESTION 20 OF 50
Following first metatarsophalangeal joint cheilectomy for hallux rigidus, which patient parameter is NOT altered compared to preoperative values:
1
Shifting of plantar forefoot pressures medially toward the hallux
2
Increased active dorsiflexion of the first metatarsophalangeal joint
3
Increased first metatarsophalangeal joint dorsiflexion during gait
4
Decreased first metatarsophalangeal joint plantarflexion at rest
5
Increased hallux abduction
The resting position of the hallux in normal patients is 20° of dorsiflexion relative to the first metatarsal shaft. In patients with hallux rigidus, the resting position is decreased to 10° of dorsiflexion relative to the metatarsal shaft. This relatively plantarflexed position was not improved to a more normal value following cheilectomy.
QUESTION 21 OF 50
A 13-year-old boy falls out of a tree and sustains the injury seen in Figures A and B. He is taken to the OR for fixation of his fracture.
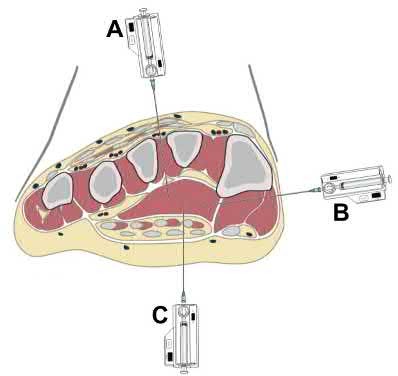
The next morning, the patient’s blood pressure is 185/105 mm Hg and pulse rate is 130. He complains of pain that is not improved with opiates. On physical exam, the foot is firm. The decision is made to obtain compartment pressures to rule out compartment syndrome of the foot. Which of the following paths in Figure C marks the
appropriate location to measure the central compartment, and what would be considered abnormal values?
1
Path A, absolute value of 30-45 mmHg or delta p > 30mmHg
2
Path B, absolute value of 30-45 mmHg or delta p > 30mmHg
3
Path B, absolute value of 30-45 mmHg or delta p < 30mmHg
4
Path C, absolute value of 30-45 mmHg or delta p > 30mmHg
5
Path C, absolute value of 30-45 mmHg or delta p < 30mmHg
The correct approach to measure pressures in the central compartment of the foot is by directing the needle lateral and plantar through the abductor hallicus, just under the base of the first metatarsal. Abnormal values indicating the need for decompression are an absolute value of 30-45 mmHg or a Δp < 30mmHg (the difference between the patient's diastolic blood pressure and compartment pressures).
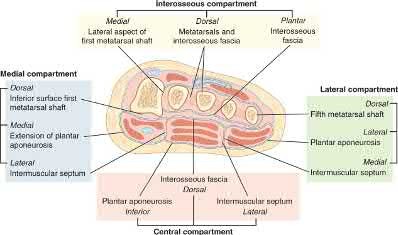
The most common symptom of compartment syndrome in the extremities is intense pain. However, compartment syndrome can be difficult to diagnose in children and patients who are comatose, nonverbal, and/or mentally compromised because they may not be able to properly express their level of pain. Additionally, in compartment syndrome of the foot, pain on passive extension of the toes may or may not be present, and swelling and absence of the dorsalis pedis pulse may be expected findings with extensive trauma to the foot, making the clinical diagnosis even more difficult. Thus, for patients with equivocal findings on physical exam, foot compartment pressures should be measured in order to confirm the diagnosis. There are 8 compartments in the foot: lateral, medial, central, and 4 interosseous. The lateral compartment
contains the abductor digiti minimi and flexor digiti minimi brevis, and is measured by directing the needle 1cm medial and plantar under the midshaft of the 5th metatarsal. The medial compartment contains the abductor hallicus and flexor hallicus brevis, and is measured by directing the needle lateral and plantar under the base of the first metatarsal. The central compartment contains the oblique head of the adductor hallucis, and is measured through the same approach as the medial compartment after advancing the needle more deeply. The 4 interosseous compartments entail the 2nd, 3rd, and 4th web spaces, and can be measured by directing the needle plantar into each respective dorsal webspace.
Ojika et al. performed a systematic review on foot compartment syndrome. They found that the most common cause of foot compartment syndrome was crush injury to the foot, and that diagnosis was mostly made through a combination of clinical findings and compartment pressure measurements.
Badhe et al. reported 4 cases where competent sensate patients developed compartment syndromes without any significant pain. They found that pain is not a reliable clinical indicator for underlying compartment syndrome, so in a competent sensate patient, the absence of pain does not exclude compartment syndrome. They concluded that a high index of clinical suspicion must prevail in association with either continuous compartment pressure monitoring or frequent repeated documented clinical examination with a low threshold for pressure measurement.
Flynn et al. looked at the diagnosis and outcome of acute traumatic compartment syndrome of the leg in children. They found that a delay in diagnosis may occur because acute traumatic compartment syndrome manifests itself more slowly in children or because the diagnosis is harder to establish in this age group. They state that the results of the present study should raise awareness of late presentation and the importance of vigilance for developing compartment syndrome in the early days after injury.
Figures A and B are lateral and Harris radiographs of the foot demonstrating a calcaneus fracture. Figure C is a cross-sectional image of the foot. Illustration A is an image depicting the compartments of the foot.
Incorrect Answers:
Answer 1: Path A is the incorrect approach for measuring the central compartment. Additionally, a Δp < 30mmHg (not > 30mmHg) is considered abnormal.
Answer 2: A Δp < 30mmHg (not > 30mmHg) is considered abnormal. Answer 4: Path C is the incorrect approach for measuring the central
compartment. Additionally, a Δp < 30mmHg (not > 30mmHg) is considered abnormal.
Answer 5: Path C is the incorrect approach for measuring the central compartment.
QUESTION 22 OF 50
A 21-year-old hockey player who has recurrent shoulder subluxations undergoes an anterior capsulorrhaphy under general anesthesia, and an interscalene block is used to relieve postoperative pain. At the 1-week follow-up examination, he reports loss of sensation over the lateral region of the shoulder and is unable to actively contract the deltoid muscle. The remainder of the examination is normal. What is the best course of action at this time?
1
Early exploration and possible repair of the axillary nerve
2
Urgent electromyography to assess for level of nerve injury
3
Continued normal postoperative care and observation of the nerve injury
4
Consultation with the anesthesiologist regarding a complication of the interscalene block
5
MRI to evaluate for a possible hematoma compressing the neurovascular bundle
The patient has an axillary nerve injury, which is relatively uncommon after surgery for instability. This type of injury generally is the result of a stretch injury rather than transection or a hematoma. Therefore, observation is indicated in the early postoperative period. After approximately 6 weeks, electromyography can be used to confirm and document the point of injury. Interscalene blocks can cause prolonged nerve injury but usually are not limited to the axillary nerve.
REFERENCE: Ho E, Cofield RH, Balm MR, et al: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270.
QUESTION 23 OF 50
of 100
A 59-year-old woman with a history of gastric bypass 1 year ago and symptomatic L5S1 isthmic spondylolisthesis is seen. She has been symptomatic with bilateral leg pain for 6 months. She has tried physical therapy, selective nerve root injections, and nonsteroidal anti-inflammatory drugs with minimal relief. She is offered surgical intervention consisting of L5-S1 posterior spinal and interbody fusion along with a Gill laminectomy. As part of surgical planning, the surgeon should consider ordering
1
thyroid laboratories.
2
hemoglobin A1c.
3
dual-energy x-ray absorptiometry (DEXA) scan.
4
medial branch block.
■ Because of the increasing rates of obesity, gastric bypass surgeries are becoming increasingly prevalent. Gastric bypass surgery is associated with negative effects on bone metabolism and can result in decreased bone mass. Some risk factors include changes in absorption (vitamin D), loss of muscle mass, and hormone changes. In a study of 48 patients undergoing Roux-en-Y gastric bypass, DEXA 6 months and 12 months postoperative from gastric bypass noted a 5% and 8% decrease, respectively, in femoral neck bone mineral density, compared with preoperative density. In patients with osteopenia or osteoporosis undergoing instrumented spinal fusion, failure of instrumentation may arise and presurgical planning is required. In patients with a history of gastric bypass undergoing instrumented spinal fusion, preoperative DEXA scan can diagnose osteopenia and/or osteoporosis and an appropriate surgical plan can be formulated.
QUESTION 24 OF 50
Figures 1 through 4 show the radiographs, and Figures 5 through 8 show the MRIs obtained from a 32-year-old man with worsening left knee pain. A
1
foot hip-to-ankle radiograph shows a 13-degree varus knee deformity. The patient sustained a major left knee injury 5 years ago managed nonsurgically with a functional brace but experienced worsening pain. He was seen by an orthopaedic surgeon 18 months ago, and a medial meniscus tear was treated with an arthroscopic partial medial meniscectomy. Since then, his knee has been giving way more often, and he no longer feels safe working on a pitched roof. The patient received 6 months of formal physical therapy and was fitted for a hinged knee brace, but he still has pain and instability. He believes he has exhausted his nonsurgical options and would like to undergo surgery. What is the most appropriate treatment at this time?
28
2
ACL reconstruction and subsequent proximal tibial osteotomy
3
ACL reconstruction alone
4
Distal femoral osteotomy with simultaneous ACL reconstruction
5
Proximal tibial osteotomy with subsequent ACL reconstruction
Proximal tibial osteotomy is the most appropriate intervention to correct varus malalignment and to reduce stress on the ACL. In some cases, proximal tibial osteotomy alone may address both pain and instability, but if instability persists, particularly in the setting in which instability can be dangerous, subsequent ACL reconstruction can further stabilize the knee with less stress on the graft after the correction of malalignment.
29
Varus alignment places increased stress on the native or reconstructed ACL. ACL reconstruction should be performed only at the same time as or following proximal tibial osteotomy to correct alignment in the setting of varus malalignment. It is not appropriate to perform ACL reconstruction prior to proximal tibial osteotomy in this setting. Distal femoral osteotomy is not indicated to correct varus malalignment. Varus alignment places increased stress on the native or reconstructed ACL, and ACL reconstruction alone is not indicated for this patient. A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with prognosis in the setting of reaction to metal debris?
A. Erythrocyte sedimentation rate, C-reactive protein, and white blood cell count
B. Serum cobalt and chromium ion levels
C. MRI with metal artifact reduction sequence (MARS)
D. CT of pelvis
Painful MOM THA and taper corrosion can cause substantial damage to a patient's hip if left untreated. In this case, the workup for a painful MOM THA starts the same as a workup for a painful metal-on-polyethylene bearing couple. Infection must be ruled out in every case with a set of inflammatory markers. If these markers are remotely elevated, this is an indication for joint aspiration. In patients with metal debris, the pathology report often indicates too many cells to count or cellular debris. Metal ion levels do not seem to correlate with prognosis. There are well-functioning patients with high ion levels and poor-functioning patients with low ion levels. Advanced imaging with MARS MRI to evaluate for peritrochanteric fluid collection, a soft-tissue mass, or synovial/capsular hypertrophy will reveal signs of a metal reaction that indicate the need for a revision discussion. A CT scan can show more advanced bony destruction as an indicator of poor prognosis. These films can be used to determine the need for a structural graft or augments for reconstruction of bone loss attributable to metal debris.
Correct answer : C
30
QUESTION 25 OF 50
Slide 1 Slide 2
You are planning a tendon transfer to help correct deformity in a patient with hereditary sensory motor neuropathy. Which of the following muscles will be used for the transfer based upon the clinical appearance of the foot (Slide 1 and Slide 2):
1
Posterior tibial
2
Anterior tibial
3
Extensor hallucis longus
4
Peroneus brevis
5
Flexor hallucis longus
The posterior tibial tendon transfer is a commonly performed surgery for correction of cavus foot deformity associated with weakness of the anterior tibial muscle and varying degrees of drop foot deformity. The removal of the force of the posterior tibial tendon adds to the correction of the deformity of the foot by balancing the absent peroneus brevis. Although the extensor hallucis longus can be used as a tendon transfer, it will not be the primary muscle used or sufficient to correct deformity.
QUESTION 26 OF 50
A 28-year-old professional athlete presents for treatment of foot pain following an inversion injury to her ankle. She has been immobilized in a short leg walker boot for 1 month with minimal relief of symptoms. On examination, pain is present in the sinus tarsi. The patientâs ankle is not painful or unstable. Radiographs demonstrate a calcaneonavicular coalition. Recommended treatment includes:
1
C orticosteroid and lidocaine injection into the sinus tarsi
2
C ontinued immobilization in a boot for an additional month
3
Physical therapy treatments aimed at mobilizing the subtalar joint
4
Subtalar arthrodesis
5
Excision of the tarsal coalition
When a tarsal coalition becomes symptomatic in an adult, surgery becomes necessary. Initial immobilization may be attempted, although prolonged immobilization in an athlete is not ideal. Manipulation of the foot will exacerbate the pain, and therapy is not indicated. If arthrodesis of the hindfoot is performed for treatment of a calcaneonavicular coalition, then a triple arthrodesis is performed. Excision of the adult calcaneonavicular coalition is the preferred treatment.
QUESTION 27 OF 50
Which of the following proteins or vitamins controls the amount of receptor activator of nuclear factor âkB ligand (RANKL)
produced by osteoblasts:
1
Parathyroid hormone
2
25 hydroxyvitamin D3
3
Thyroid hormone
4
1,25 dihydroxyvitamin D3
5
Calcitonin
The active from of vitamin D (1,25 dihydroxyvitamin D3) regulates the control of RANKL production by the osteoblast.
The activation of osteoclasts is a complex process. Surface receptors on the osteoclast precursor cells are called RANK. Receptor activator of nuclear factor âkB ligand (RANKL) is expressed on the surface of osteoblasts/stromal cells. The RANKL proteins leave the osteoblast and attach to the RANK receptor on the osteoclast precursor. Macrophage colony stimulating factor then facilitates the production of active osteoclasts from the osteoclast precursor
QUESTION 28 OF 50
Residual angulation <30° of the humeral shaft after nonoperative fracture treatment has been shown to have what effect on patient reported outcomes?
1
Angulation in the coronal plane has more effect on functional outcomes than in the sagittal plane.
2
Increased angulation corresponds with worse functional outcomes.
3
Angulation >5° in any plane results in an unacceptable cosmetic result.
4
Residual angulation has no correlation with functional outcomes.
Acceptable angulation of humeral shaft fractures for nonoperative treatment is quite generous due to compensatory motion at the shoulder joint. Traditionally, 20° of anterior-posterior and 30° of varus-valgus angulation is acceptable. Indications for surgery have included angulation outside of this range, open fractures, brachial plexus injury, polytrauma, or other factors that preclude functional bracing. Increased amounts of angulation at the conclusion of healing can result in cosmetic dissatisfaction, but this has not been correlated with any specific degree of angulation, as patient factors are a strong influencer. Increased angulation has not been shown to affect functional outcomes within the angulation range previously described.
QUESTION 29 OF 50
A 22-year-old collegiate basketball player presents for treatment of a stress fracture of the base of the fifth metatarsal at the junction of the metaphysis and diaphysis. The fracture was treated operatively, and the patient returned to playing basketball. Three months later, it was apparent that a repeat fracture was present. The fracture was treated with screw removal and a repeat screw fixation. Four months later, after a successful basketball season, he sustained a repeat stress fracture of the metatarsal. On examination, he has a mild cavovarus foot configuration with normal ankle range of motion. Inversion is 15° and eversion is 5°. The base of the fifth metatarsal is prominent. The most likely cause for the repeat fracture is:
1
Abnormal ankle biomechanics
2
C hronic unrecognized ankle instability
3
A varus heel
4
Bone sclerosis of the fifth metatarsal base
5
C hronic avascularity of the fifth metatarsal base
The most common cause of recurrent injury to the fifth metatarsal is unrecognized varus heel deformity. Surgeons must also check for ankle instability, which may be present in this patient. A varus heel, ankle instability, and injury to the fifth metatarsal are associated with recurrent deformity.
QUESTION 30 OF 50
of 100
Figures 97a through 97d are the radiographs and MR images of a 21-year-old man with symptoms of a left medial thigh mass. Upon examination, you palpate a firm, fixed, deep, nontender mass of the medial proximal left thigh. No other masses are found during the examination. The patient fears metastatic disease. What is the risk for malignant transformation throughout this patient’s lifetime?
1
0%
2
Less than 1%
3
Less than 15%
4
More than 15%
The images reveal a solitary pedunculated osteochondroma. Malignant degeneration of solitary osteochondromas occurs in fewer than 1% of patients. A reasonable approach would be to inform the patient of the rare (less than 1%) incidence of malignant degeneration and to return for evaluation if symptoms develop or if the patient notices growth of the lesion.
RECOMMENDED READINGS
104. Schwartz AJ. Benign cartilage tumors. In: Biermann JS, ed. _Orthopaedic Knowledge Update Musculoskeletal Tumors 3_. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2013:97-106.
105. [Aboulafia AJ, Kennon RE, Jelinek JS. Benign bone tumors of childhood. J Am Acad Orthop Surg. 1999 Nov-Dec;7(6):377-88. Review. PubMed PMID: 11505926.](http://www.ncbi.nlm.nih.gov/pubmed/11505926)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11505926)
QUESTION 31 OF 50
of 100
A 2-year-old girl is being evaluated for 3 to 4 weeks of limping. She has been afebrile and has stopped walking, prefering to crawl. Unable to stand from a seated position, she has not gained weight over the last 3 months. She has a non-toxic appearance and has no bruises. Her hips have minimal pain with range of motion. She is able to walk with a waddling/lurching gait. A radiograph and MRI of the pelvis were obtained (Figures 1 and 2). The most appropriate next step in management is/are
1
hip aspiration.
2
a CT-guided biopsy.
3
antistaphylococcal antibiotics.
4
chromosomal analysis.
■ The plain films show decreased joint space and irregularity of the vertebral endplates at L2-L3. This is confirmed by the MRI. There is no evidence of an abscess. These findings are consistent with discitis/ vertebral osteomyelitis. When cultures are positive, the most common organism is Staphylococcus aureus. For this reason, empiric treatment with anti-staphylococcus antibiotics should be the first line of treatment. If there is no improvement, or if there are risk factors for other organisms, (foreign travel, immunocompromised, exposure to unpasteurized milk), CT-guided biopsy may be indicated. Symptoms may also improve with the addition of a brace.
QUESTION 32 OF 50
Figures 1 through 4 are the wrist MR images of a 43-year-old right-hand-dominant bricklayer who reports gradually progressive left hand weakness for 4 months. He describes difficulty gripping objects, tying his shoes, and holding utensils. He denies any numbness, paresthesias, or a previous injury. An examination reveals intact sensation in a median, radial, and ulnar nerve distribution. He has atrophy of hand interossei and a positive Froment sign finding. He has no Tinel sign finding at the wrist or elbow and no exacerbation of symptoms with elbow hyperflexion. Electromyography shows signs of denervation in an ulnar nerve distribution distal to the wrist. What is the best next step? --- ---
1
Cubital tunnel release
2
Guyon's canal release
3
Hook-of-hamate excision
4
Excision of the ganglion cyst
The MR images show a lesion consistent with a ganglion cyst located near the hook of the hamate. The ulnar nerve divides into motor and sensory branches just proximal to this lesion. In this case, the ganglion cyst compresses the ulnar nerve motor branch but not the sensory branch, resulting in motor dysfunction but no sensory disturbance. Excision of the ganglion cyst should alleviate his symptoms. Compression of the ulnar nerve proximal to the motor branch take-off (in either the cubital tunnel or proximal Guyon’s canal) would cause both sensory and motor dysfunction. Although chronic nonunion of the hook of the hamate can cause ulnar nerve symptoms, the hook of the hamate appears intact on the MR image. The MR image shows a lesion that is well circumscribed with high intensity on T1 and T2 images, consistent with a benign ganglion cyst, and ganglion cysts are relatively common lesions in this area.
QUESTION 33 OF 50
The greatest amount of step-off that is well-tolerated in a Bennettâs fracture is:
1
0 mm
2
1 mm to 2 mm
3
2 mm to 3 mm
4
3 mm to 4 mm
5
4 mm to 5 mm
Studies by Livesley, Kjaer-Petersen, and others have shown that patients with fractures with more than a 1-mm step-off after reduction were more likely to develop arthritis at the thumb carpometacarpal joint. Although some studies have not shown functional outcome correlating with the presence of arthritis, Oosterbos and De Boer found that all their patients with fair and poor overall results had nonanatomic reductions. Although a cadaveric study by C ullen has shown that a 2-mm step-off may be acceptable, this contrasts with the clinical evidence currently available.
QUESTION 34 OF 50
Which of the following nerves is susceptible to entrapment near the calcaneal attachment site of the plantar fascia and can mimic or co-exist with plantar fasciitis?
1
First branch of the lateral plantar nerve
2
Dorsal cutaneous branch of the superficial peroneal nerve
3
Medial calcaneal branch of the posterior tibial nerve
4
Lateral branch of the medial plantar nerve
5
Communicating branch of the fourth common digital nerve
The first branch of the lateral plantar nerve is susceptible to entrapment beneath the deep fascia of the adductor hallucis muscle adjacent to the calcaneal attachment of the plantar fascia. This can be a cause of chronic heel pain. Additionally, the nerve is vulnerable to injury by a blind dissection in releasing the plantar fascia. The dorsal cutaneous branch of the superficial peroneal nerve supplies sensation to the dorsum of the foot. The medial calcaneal branch of the posterior tibial nerve lies in the subcutaneous tissues and innervates the skin of the heel. It is vulnerable to injury from skin incisions on the medial side of the heel. The lateral branch of the medial plantar nerve forms the second and third common digital nerves. Entrapment of the proper medial plantar nerve can occur at the master knot of Henry. This is well distal to the calcaneal attachment of the plantar fascia, and the pain usually radiates more distally in the arch, separate from heel pain. The communicating branch of the fourth common digital nerve crosses to the third common digital nerve. Therefore, the third common digital nerve receives supply from both the lateral and medial plantar nerves. This dual supply has been implicated in the increased incidence of digital neuroma of the third common digital nerve.
REFERENCES: Bordelon RL: Heel pain, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 837-857.
Mann RA, Baxter DE: Diseases of the nerves, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 543-574.
Baxter DE: The heel in sport. Clin Sports Med 1994;13:683-693.
QUESTION 35 OF 50
A 9-year-old boy with cerebral palsy has trouble sitting. His mother states that whenever his diapers are changed or his hips are moved, he begins to cry. Radiographs demonstrate high dislocations of both femoral heads. The femoral heads have an ovoid shape and superolateral flattening. Recommended treatment includes:
1
Botulinum toxin injected into the adductors
2
Bilateral open adductor tenotomy
3
Bilateral femoral osteotomies with acetabuloplasty
4
Bilateral proximal femoral resection
5
Bilateral C olonna arthroplasty
Bilateral proximal femoral resection is the recommended treatment.
Femoral head dislocations may become painful in cerebral palsy at a much earlier age than in nonspastic individuals. Botulinum toxin or adductor tenotomy will not solve the problem.
Replacing the deformed femoral heads into the acetabulum will not achieve the long-term goal of good hip range of motion.
QUESTION 36 OF 50
Figures 1 and 2 are the MRI scans of a 57-year-old man who dislocated his left shoulder after a fall while playing tennis. On examination, he had full passive shoulder range of motion, but he was unable to actively elevate his injured shoulder. Sensation was intact to light touch over the lateral shoulder. What is the most likely etiology of his shoulder weakness?
22
1
Axillary nerve injury
2
Cervical radiculopathy involving the C6 nerve root
3
Massive rotator cuff tear with loss of the transverse force couple
4
Long head of the biceps tendon rupture with loss of superior stabilizing effect
This patient has a massive rotator cuff tear resulting in disruption of the transverse force couple between the subscapularis anteriorly and the infraspinatus and teres minor posteriorly. These muscles provide dynamic shoulder stability throughout active elevation, and loss of the force couple produces a pathologic increase in translation of the humeral head and decreased active abduction. Active shoulder elevation <90° in the presence of full passive motion is termed pseudoparalysis. The most common neurologic deficit after shoulder dislocation is isolated injury to the axillary nerve. This patient's sensory examination suggests that the axillary nerve is intact. Cervical radiculopathy is less common after shoulder dislocation but has been reported. Conflicting evidence exists regarding the contribution of the long head of the biceps tendon to glenohumeral stability. One study reported minimal electromyographic activity in the biceps during ten basic shoulder motions. 23
QUESTION 37 OF 50
What is the most likely diagnosis?
1
Fibrous dysplasia
2
Aneurysmal bone cyst
3
Osteosarcoma
4
Giant cell tumor
5
Osteomyelitis
_ _
QUESTION 38 OF 50
An 11-year-old girl has had pain in the medial arch of her foot for the past 3 months. She reports that pain is present even with daily activities such as walking to class at school, and ibuprofen provides some relief. She denies any history of trauma. Examination reveals a flexible pes planus with focal tenderness over a prominent tarsal navicular tuberosity. Radiographs show a prominent accessory navicular. Management should consist of
1
cast immobilization for 4 to 6 weeks.
2
posterior tibial tendon advancement and repair (Kidner procedure).
3
corticosteroid injection of the posterior tibial tendon insertion.
4
triple arthrodesis.
5
needle biopsy of the trochar.
The patient has the classic symptoms, examination findings, and radiographs for a painful accessory navicular. Initial treatment should always be nonsurgical, specifically cast immobilization. Surgery should be reserved for those patients who fail nonsurgical management. Corticosteroids should not be injected into a posterior tibial tendon or insertion point because they can weaken the tendon and possibly cause tendon rupture. Triple arthrodesis and biopsy have no role in the management of a painful accessory navicular.
REFERENCE: Bordelon RL: Flatfoot in children and young adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 717-756.
QUESTION 39 OF 50
The view from an anterosuperior portal of the right shoulder shown in Figure 12 reveals which of the following findings?**
1
Rupture of the subscapularis tendon
2
Tear of the rotator interval
3
Humeral avulsion of the glenohumeral ligament (HAGL) lesion
The arthroscopic view shows a HAGL lesion. With the arthroscope directed anteroinferiorly, muscular striations of the subscapularis can be visualized through the avulsion site. In vitro strain studies indicate that glenohumeral ligament failure on the humeral side occurs in approximately 25% of patients, while clinically this lesion has been reported in approximately 9% of patients with shoulder instability. Failure to recognize and treat this lesion leads to persistent anterior instability. An ALPSA lesion, a Bankart variant, occurs on the glenoid side and is characterized by a sleeve-like medial retraction and inferior rotation. A Bankart lesion is the classic avulsion of the glenohumeral ligament from the glenoid rim. The subscapularis tendon and the rotator interval are not shown in the figure.
REFERENCES: Wolf EM, Cheng JC, Dickson K: Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607.
Bigliani LU, Pollack RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Warner JJ, Beim GM: Combined Bankart and HAGL lesion associated with anterior shoulder instability. Arthroscopy 1997;13:749-752.
QUESTION 40 OF 50
Figure 47a Figure 47bFigures 47a and 47b are the radiograph and CT scan of a 45-year-old man who was involved in a highspeed motor vehicle accident. What is the most appropriate treatment?
1
Subtalar arthrodesis
2
Percutaneous screw fixation
3
Closed reduction and cast application
4
Open reduction and internal fixation
5
Non-weight-bearing and early range of motion
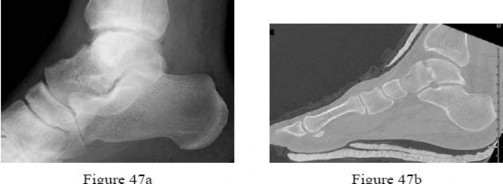
No detailed explanation provided for this question.
QUESTION 41 OF 50
..A 35-year-old man fell off of a roof and sustained an extra-articular supracondylar elbow fracture. He had normal sensation in all fingers after the injury and before undergoing surgery to repair the fracture. The ulnar nerve was not transposed, but it was inspected prior to wound closure. Ten days after surgery, the patient has numbness in his small finger and is unable to cross his fingers. His elbow range of motion is between 40 degrees and 100 degrees. What is the next appropriate treatment step?
1
Elbow splint at 40 degrees at night for 6 weeks
2
Electromyography (EMG)
3
Exploration of the ulnar nerve and transposition
4
Observation
DISCUSSION..This patient has an early postsurgical ulnar nerve palsy. The causes of this injury are laceration of the nerve during surgery, entrapment of the nerve in the fracture or hardware, or traction injury during surgery. If the orthopaedic surgeon is sure that the nerve was not lacerated at the end of the case or entrapped in the hardware, then the nerve is probably intact and will recover. Observation is the best treatment in this case because the nerve was checked before wound closure. Elbow splinting has not been shown to help with postsurgical nerve recovery. EMG findings may not be accurate this early in the injury.
- Observation
QUESTION 42 OF 50
A 7-month-old girl is newly seen for a dislocation of the left hip. The newborn exam was unremarkable; there was no history of trauma or evidence of spasticity. Recommended treatment includes:
1
Exam, arthrogram and attempted closed reduction under anesthesia to guide treatment
2
Pavlik harness
3
Open reduction through a medial approach
4
Open reduction through a lateral approach
5
A Salter osteotomy
An exam under anesthesia and arthrogram should be performed. C losed reduction must be performed if the hip reduces with a medial dye pool less than 4 mm and a safe zone greater than 20°.
The Pavlik harness is not strong enough to hold an infant older than 4 to 6 months. Open reduction is reserved for hips that do not reduce by closed means.
A Salter osteotomy is only indicated if the hip is still unstable after an open reduction.
QUESTION 43 OF 50
Figures 1 and 2 are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg. What examination findings are most consistent with the pathology seen in the radiographs?
1
Pain with resisted hip flexion
2
Pain with a half sit-up, plus tenderness at the pubic ramus
3
Pain with a combination of hip flexion, adduction, and internal rotation
4
Tenderness to palpation at the greater trochanter
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater
trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement. Surgical treatment for cam impingement can be effective for symptomatic patients. Even among high-level athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable with those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment. Byrd and Jones described five patients who developed transient neurapraxias that resolved uneventfully. The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a _periacetabular osteotomy can develop a more retroverted acetabulum as well._
QUESTION 44 OF 50
A 79-year-old female sustained a slip and fall. Injury films are shown in Figures A, B, and C. She has made limited progress with 3 weeks of physical therapy and continues to endorse severe low back pain and difficulty ambulating. What is the next best step in treatment?
1
Examination under anesthesia
2
Observation and physical therapy
3
Magnetic resonance imaging (MRI) of the pelvis
4
Bone scan
5
Percutaneous fixation
This osteoporotic patient has sustained a sacral insufficiency fracture. At this point, given her difficulty ambulating and severe pain percutaneous fixation is the best option.
Sacral fragility fractures encompass both atraumatic sacral fractures as well as sacral fractures that occur as a result of low energy mechanisms in elderly patients with osteopenic bone. Over time, sacral fragility fracture incidence has increased with the aging population. Morbidity of non-op treatment includes pain, loss of independence, need for institutionalization, as well as the ills of recumbency. A number of authors have found that percutaneous iliosacral stabilization of these fractures leads to pain relief and therefore a higher likelihood of early ambulation.
Sanders et al. performed a study to evaluate the effectiveness of transsacral-transiliac screw fixation for the treatment of sacral insufficiency fractures that fail nonoperative treatment. They compared preoperative and postoperative Visual Analog Scale scores and Oswestry Low Back Disability Index scores.
They found that patients experienced statistically significant improvement in both outcome measures after intervention and no complications were encountered. They concluded that transsacral-transiliac screw fixation is a safe and effective treatment for sacral insufficiency fractures recalcitrant to nonoperative management.
Rommens et al. propose a novel classification system for fragility fractures of the pelvic ring. The classification is based on morphological criteria and it corresponds to the degree of instability. They hope that this criterion will help guide treatment based on the degree of instability based on radiological and clinical findings.
Figure A is an AP pelvis radiograph demonstrating no osseous abnormalities. Figures B and C are axial and coronal CT cuts, respectively, demonstrating, fractures of the sacrum. Illustration A is an AP pelvis radiograph following percutaneous skeletal fixation.
Incorrect Answers:
Answer 1: This patient has failed non-operative treatment and therefore requires surgical stabilization. Examination under anesthesia is helpful in diagnosing subtle instability patterns that may not be visible with static imaging.
Answers 2: This patient has failed non-operative treatment and therefore requires surgical stabilization. Sacral fragility fractures may be treated with a trial of weight-bearing and repeat imaging to assess for displacement.
Answers 3 & 4: Additional imaging studies are not necessary in this case as the diagnosis can be made from the CT scan. If no injury is visible on the CT scan and the patient continues to have pain, additional imaging may be warranted.
QUESTION 45 OF 50
Skeletal muscle may remain viable (electrically responsive) following a period of total ischemia. Which of the following is the correct time interval for the tolerance to total muscle ischemia (complete recovery can be expected):
1
3 to 4 hours
2
4 to 6 hours
3
6 to 8 hours
4
8 to 10 hours
5
10 to 12 hours
Skeletal muscle tolerates periods of complete muscle ischemia for 3 to 4 hours without irreversible damage. Variable recovery occurs with ischemia for 6 to 8 hours. When the period of ischemia is more than 8 hours, there is irreversible muscle damage. After 8 hours, the muscle cells degenerate and, grossly, the muscle contracts as the muscle cells are replaced with scar tissue and contracture may result.
Remember to let a tourniquet down after 2 hours of ischemia. One does not want to enter the tolerance period of 3 to 4 hours. Correct Answer: 3 to 4 hours
QUESTION 46 OF 50
When evaluating a patient with a lumbar burst fracture, the integrity of the posterior ligamentous complex must be evaluated. Which of the following is a complete and accurate list of the components of the posterior ligamentous complex?
1
Supraspinous ligament, interspinous ligament, ligamentum flavum, and the facet joint capsules
Supraspinous ligament, interspinous ligament, and ligamentum flavum
4
Supraspinous ligament, interspinous ligament, ligamentum flavum, and the facet joints
5
Supraspinous ligament, interspinous ligament, ligamentum flavum, facet joint capsules, facet joints, and the posterior longitudinal ligament
DISCUSSION: The components of the posterior ligamentous complex are the supraspinous ligament,interspinous ligament, ligamentum flavum, and the facet joint capsules. Recent studies have emphasized the importance of the posterior ligamentous complex. The Thoracolumbar Injury Classification and Severity Score (TLICS) is a classification system that allows for efficient and effective classification of thoracolumbar spine injuries. It evaluates three characteristics of the injury:
No detailed explanation provided for this question.
QUESTION 47 OF 50
What effect does deep freezing have on allograft tissue?
1
Causes no deleterious clinical effect on ligamentous grafts
2
Causes a less deleterious effect on cartilage than on ligamentous grafts
3
Causes degradation of the extracellular matrix
4
Allows for preservation of cells with tissue
5
Eliminates the chance of human immunodeficiency virus (HIV) transmission
Deep freezing is the simplest and most widely used method of ligament allograft storage. All cells in the tissue are destroyed with the freezing. However, for this reason, it is not a preferred storage method for menisci or cartilage allografts. Although this method may enhance success because it removes potential antigens located on the cells, it cannot guarantee elimination of HIV transmission. The advantage of cryopreservation storage is that a significant number of cells will survive the process, a factor important in meniscal allograft survival after implantation. No deleterious effects are noted clinically because of the acellularity of the tissue.
REFERENCES: Shelton WR, Treacy SH, Dukes AD, Bomboy AL: Use of allografts in
knee reconstruction: I. Basic science aspects and current status. J Am Acad Orthop Surg 1998;6:165-168.
Caspari RB, Botherfield S, Horwitz RL, et al: HIV transmission via allograft organs and tissues. Sports Med Arthroscopy Rev 1993;1:42-46.
QUESTION 48 OF 50
Slide 1
A 37-year-old woman injured her ankle 17 weeks ago when stepping off a sidewalk. She has experienced pain in the ankle since that time, and no treatment has yet been initiated. Presented is a view of the ankle performed with external rotation stress (Slide). The recommended treatment at this time is:
1
Repair of the deltoid ligament
2
Repair of the deltoid ligament and open reduction of the syndesmosis
3
Screw fixation of the syndesmosis
4
Open reduction internal fixation of a high fibular fracture
5
Open reduction internal fixation of a high fibular fracture and repair of the deltoid ligament
This unstable ankle is associated with a complete disruption of the syndesmosis. With the information available, it is not likely that a high fibular fracture is present. One has to assume that the injury is limited to the syndesmosis. Although the deltoid ligament may be torn, one cannot determine this until the time of surgery. At surgery, if the mortise reduces well following insertion of screw(s), then the deltoid is left alone. If the talus does not reduce, then there may be deltoid tissue that needs to be removed before the reduction can be accomplished.
QUESTION 49 OF 50
Four days ago, a 13-year-old boy stubbed his toe on a chair while running barefoot through his home.
He received no treatment at the time. He is now seen at the orthopaedic clinic with the radiograph and clinical photograph shown in Figures 27a and 27b. What is the next step in management?
1
Buddy taping to the adjacent toe and use of a hard-soled shoe for 2 weeks
2
Buddy taping to the adjacent toe and use of a cast extending to the tips of the toes for 3 weeks
3
Open reduction and internal fixation of the fracture, with irrigation of the wound and postoperative
antibiotics
4
Antibiotics and closed treatment of the fracture
5
Closed pinning of the phalanx fracture
The boy has a Seymour’s fracture of the toe. The germinal matrix of the nail bed is trapped in the fracture site; thus this should be considered an open fracture. Ideally, it should be treated with open reduction and internal fixation and use of antibiotics at the time of injury. Because this is a delayed presentation, it is even more important to do a formal open reduction and a good irrigation and debridement, followed by the use of postoperative antibiotics. Because the fracture has been displaced for several days, overall management will be easier if the fracture reduction is maintained with pin fixation.
REFERENCE: Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL. American Academy of Orthopaedic Surgeons, 2008, p 737.
QUESTION 50 OF 50
What is the most common associated pathology in patients who have suprascapular nerve entrapment secondary to ganglion cysts?
1
Glenohumeral arthritis
2
Fracture of the clavicle
3
Tear of the rotator cuff
4
Rupture of the long head of the biceps tendon
5
Superior labrum anterior and posterior (SLAP) lesion
It is well known that suprascapular nerve entrapment can be secondary to many entities, and its association with ganglion cysts and SLAP lesions has been well documented. Because of a superior labral tear, synovial fluid will leak out of the joint underneath the labrum, causing the cyst and secondary compression of the nerve.
REFERENCES: Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
Iannotti JP, Ramesey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Moore TP, Fritts HM, Quick DC, Buss DD: Suprascapular nerve entrapment caused by supraglenoid cyst compression. J Shoulder Elbow Surg 1997;6:455-462.