This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set 7868C9)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
Slide 1 Slide 2
You are planning a tendon transfer to help correct deformity in a patient with hereditary sensory motor neuropathy. Which of the following muscles will be used for the transfer based upon the clinical appearance of the foot (Slide 1 and Slide 2):
1
Posterior tibial
2
Anterior tibial
3
Extensor hallucis longus
4
Peroneus brevis
5
Flexor hallucis longus
The posterior tibial tendon transfer is a commonly performed surgery for correction of cavus foot deformity associated with weakness of the anterior tibial muscle and varying degrees of drop foot deformity. The removal of the force of the posterior tibial tendon adds to the correction of the deformity of the foot by balancing the absent peroneus brevis. Although the extensor hallucis longus can be used as a tendon transfer, it will not be the primary muscle used or sufficient to correct deformity.
QUESTION 2 OF 50
Figure 1
A 19-year-old man presents for treatment in the emergency department following a motorcycle accident. He sustained an isolated injury to his foot and ankle. The recommended treatment is:
1
Primary talonavicular arthrodesis
2
Open reduction internal fixation
3
C losed reduction cast immobilization
4
C losed reduction external fixation
5
C losed reduction percutaneous pin fixation
The prognosis following fracture dislocation of the navicular is not good regardless of treatment. Although one may be tempted to perform an open reduction and immediate primary talonavicular arthrodesis, this is not necessary. Following open reduction and internal fixation, arthritis of the talonavicular joint may occur.
QUESTION 3 OF 50
of 100
Figures 1 through 3 are the radiographs and 3D reconstruction of a 13-year-old right-hand dominant boy who landed onto a flexed right elbow and now has pain, swelling, and crepitation in the right elbow.
The most appropriate treatment would be
1
open reduction with percutaneous pinning with 2.0 mm Kirschner wires.
2
closed reduction and percutaneous pinning with 2.0 mm Kirschner wires.
3
open reduction and internal fixation.
4
traction.
■
Imaging demonstrates a displaced, T-type intra-articular distal humerus fracture. Anatomic restoration of the articular surface and stable fixation to enable early motion are imperative in this fracture pattern. Thus, open reduction enables articular reduction, safe identification, and protection of the ulnar nerve, and plate osteosynthesis of both condylar fragments. Olecranon osteotomy is not required, given the lack of comminution and large size of the condylar fracture fragments. The proximal position and lateral plane obliquity of the transverse metaphyseal fracture line render stable percutaneous pinning of the distal fragments to the shaft difficult. Additionally, interfragmentary compression of the articular surface is not attainable with percutaneous Kirschner wire fixation. Traction is of historical interest only and not an appropriate treatment at this time.
QUESTION 4 OF 50
A 12-year-old patient with osteogenic sarcoma metastatic to the spine is noted to have new onset of weakness of both lower extremities. Magnetic resonance imaging shows a mass expanding posteriorly and encroaching on the spinal cord. The recommended initial step is:
1
Radiation therapy and steroids
2
Increasing the dose of chemotherapy
3
Surgical resection
4
Steroids and observation alone
5
Observation only
Radiation therapy combined with steroids should be tried first to try to halt progression of the tumor. Unfortunately, the prognosis for this child is extremely poor.
Increasing the dose of chemotherapy is not likely to work because the metastasis has already progressed despite initial treatment.
Surgical resection must be tried if radiation does not produce improvement. Steroids are an adjunct to treatment but not sufficient alone.
The patient is likely to have progressive paraparesis and loss of bowel function. In order to improve the quality of life remaining, surgical resection should be offered to the patient.
QUESTION 5 OF 50
of 100
A 4-year-old girl who attends daycare had knee swelling for 21 days. She has been afebrile, her white blood cell (WBC) count is 13000/mm3 (reference range [rr], 4500-11000 /µL), and her C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) are slightly elevated. The child is unable to walk because of her pain. Radiographs show a knee effusion. A sedated knee aspiration reveals 22000 cells/ml (a normal result is less than 1000 cells/mL). A culture of the aspirate is pending. What is the best next step?
1
Presumptively treat for toxic synovitis of the knee
2
Presumptively treat for juvenile idiopathic arthritis
3
Perform polymerase chain reaction (PCR) screening for Kingella kingae (K. kingae)
4
Perform arthroscopic debridement and knee irrigation
K. kingae is variably invasive and is a facultative anaerobic gram-negative bacillus. K. kingae is a common bacteria that causes osteoarticular infections in young children. Presentation is often delayed because of the moderate course of the infection. Ten percent of young children are colonized with K. kingae. Colonization occurs in the oropharynx and is a prerequisite for invasive K. kingae septic arthritis. The PCR test screens for the RTX protein,
the factor responsible for the bacteria’s cytotoxicity. Among children in daycare centers, 28% are colonized. The sensitivity of the oropharyngeal swab PCR has been reported at 100%, and the specificity is 90.5%.
RESPONSES FOR QUESTIONS 70 THROUGH 74
1. Thrower's elbow/physeal irritation of the medial epicondylar physis
2. Osteochondritis dissecans (OCD)
3. Supracondylar humeral stress fracture
4. Patellar sleeve fracture
5. Distal femoral physeal fracture
6. Sinding-Larsen-Johansson syndrome/inferior pole patella apophysitis
7. Medial meniscal tear
8. Patellar tendon rupture
9. Patellofemoral pain syndrome
10. Popliteal cyst
11. Osteochondroma
12. Synovial sarcoma
Match the appropriate orthopaedic condition above with the clinical scenario below.
QUESTION 6 OF 50
1230) A 72-year-old male sustains the injury shown in Figure A as a result of a fall from a ladder. Which of the following factors has been shown to be associated with increased collapse or sliding displacement?
1
Use of a long intramedullary device
2
Use of a short intramedullary device
3
Use of external fixation
4
Postoperative weight bearing status
5
Intraoperative fracture of the lateral femoral wall
Intertrochanteric hip fractures with lateral wall fractures should be treated with an intramedullary device as opposed to a sliding hip screw, as the intact lateral wall provides a buttress for the proximal fragment facilitating fracture impaction as well as rotational and varus stability.
Palm et al showed that 22% of patients with a fractured lateral femoral wall underwent reoperation for collapse of fracture compared to 3% with an intact lateral femoral wall. Interestingly, 74% of the lateral proximal femoral wall fractures were iatrogenic during the procedure itself.
Gotfried et al reported on 24 patients with postoperative intertrochanteric hip fracture collapse and noted that this complication followed fracture of the lateral wall in every instance and resulted in a protracted period of disability until fracture healing. They recommend care when drilling at the base of the lateral wall intraoperatively.
Lindskog et al review the diagnosis, treatment, as well as biomechanical reviews of treatment options for unstable intertrochanteric hip fractures.
Incorrect Answers:
Answer 1, 2, and 3: No difference in collapse has been shown between long or short intramedullary devices and an external fixator in stable intertrochanteric hip fractures.
Answer 4: Early postoperative weightbearing is the goal after repair, and no differences have been shown in collapse rates with different weight bearing protocols.
QUESTION 7 OF 50
of 100
Figure 1 is an axial MRI at the L4-5 level obtained from a 62-year-old man with a 6month history of severe right leg pain and weakness in the ankle dorsiflexors. He has numbness along the medial ankle and dorsolateral aspect of his foot. The structure identified by the arrow is compressing what neural structure?
1
Traversing right L4 nerve root
2
Exiting right L5 nerve root
3
Exiting left L4 nerve root
4
Exiting right L4 nerve root
■ This patient has the clinical symptoms of a right L4 lumbar radiculopathy. The MRI taken at L4-5 shows a far-lateral/foraminal disk herniation. This disk herniation would compress the exiting L4 nerve root along with its dorsal root ganglion. The traversing right L4 nerve root would be seen best in an axial MRI at the L3-4 level. The exiting right L5 nerve root would be seen best in an axial MRI at the L5-S1 level. The disk herniation in question is right sided. The left neuroforamen is free in the axial MRI.
QUESTION 8 OF 50
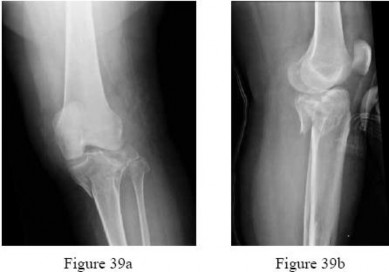
A 65-year-old woman landed on her nondominant left shoulder in a fall. An AP radiograph is shown in Figure 39. Management should consist of
1
closed reduction and immobilization.
2
closed reduction and percutaneous pinning.
3
open reduction and internal fixation.
4
humeral hemiarthroplasty with tuberosity repair.
5
total shoulder arthroplasty.
The radiograph reveals a four-part fracture-dislocation of the proximal humerus. Humeral hemiarthroplasty and tuberosity repair is the treatment of choice because the risk of osteonecrosis is high after attempted repair of this injury. Glenoid resurfacing is reserved for acute fractures in which there is significant preexisting glenoid arthrosis, such as in patients with rheumatoid arthritis.
REFERENCES: Neer CS II: Displaced proximal humeral fractures: II. Treatment of three- and four-part displacement. J Bone Joint Surg Am 1970;52:1090-1103.
Robinson CM, Page RS, Hill RM, et al: Primary hemiarthroplasty for treatment of proximal humeral fractures. J Bone Joint Surg Am 2003;85:1215-1223.
QUESTION 9 OF 50
of 100
A 15-year-old high school basketball player has pain over a medial midfoot prominence on his right foot. There has been no trauma and no specific treatment. He has bilateral flexible pes planus and pain with inversion against resistance on the right. His pain is disrupting or preventing his daily and sports activities.
1
Observation
2
Arizona brace
3
Medial arch support
4
Casting
5
Hindfoot fusion
- Casting
QUESTION 10 OF 50
..A 25-year-old man is planning to have an elbow contracture release. His elbow range of motion is 40 degrees to 90 degrees of flexion. He has no heterotopic ossification. His ring and small fingers become numb as his elbow approaches his flexion endpoint. There is no evidence of instability of the ulna-humeral or radioulnar joints. To achieve the best possible outcome, the surgeon should
1
include postsurgical elbow continuous passive motion (CPM).
2
perform the surgery open.
3
decompress the ulnar nerve.
4
release the anterior band of the medial collateral ligament.
DISCUSSION..The patient is exhibiting signs of ulnar neuropathy. The surgeon should be sure to decompress and possibly transpose the ulnar nerve, if unstable, to prevent worsening neuropathy after surgery. CPM has not been shown to be of benefit after contracture release. Equal success rates have been shown for open and arthroscopic contracture releases. The anterior band of the medial collateral ligament is important to maintain valgus stability of the elbow. The posterior band can be released to improve flexion without increasing concern for elbow instability.
- decompress the ulnar nerve.
QUESTION 11 OF 50
A 7-year-old boy has a swollen and deformed right arm after falling off his bicycle. Radiographs reveal a completely displaced posterolateral supracondylar humeral fracture. Examination reveals a warm, pink hand and forearm but absent pulses. What is the next most appropriate step in management?
1
Angiography
2
Immediate closed reduction and casting in extension
3
Surgical exploration and repair of the artery, followed by skeletal stabilization
4
Closed reduction and pinning, followed by reassessment of the vascular status
5
Magnetic resonance angiography (MRA)
The incidence of vascular injury in supracondylar humeral fractures is directly related to the degree and direction of displacement. Significant posterior lateral displacement tends to result in brachial artery and median nerve injuries, and posterior medial displacement may lead to radial nerve injury. The brachial artery is always injured at the level of the fracture; therefore, angiography or MRA will not assist in locating the injury. The treatment of choice is surgical reduction and stabilization of the fracture, followed by reassessment of the vascular status. If the hand is pink and warm or pulses can be detected with doppler, it is reasonable to follow the extremity closely after surgery. If the arm becomes pulseless and white, immediate anterior exploration of the arm is indicated. The artery is often entrapped in the fracture and once extricated, will provide adequate blood flow. If the artery is injured, a primary repair or vein graft is needed.
REFERENCES: Shaw BA: The role of angiography in assessing vascular injuries associated with supracondylar humerus fractures remains controversial. J Pediatr Orthop 1998;18:273.
Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Schoenecker PL, Delgado E, Rotman M, et al: Pulseless arm in association with totally displaced supracondylar fracture. J Orthop Trauma 1996;10:410-415.
QUESTION 12 OF 50
A 35-year-old man who snowboards sustained the injury shown in Figures 4a through 4c. What is the mechanism of injury?
1
Inversion and external rotation
2
Axial loading and internal rotation
3
Plantar flexion, axial loading, and inversion
4
Dorsiflexion and axial loading
5
Dorsiflexion, axial loading, inversion, and external rotation
Fractures of the lateral process of the talus in snowboarders have been thought to result from pure dorsiflexion, inversion, and axial loading. In a cadaveric study, 10 cadavers were placed in fixed dorsiflexion and inversion with an axial load. This was combined with or without external rotation. No fractures occurred after axial loading in the dorsiflexed-inverted position. Fractures of the lateral process of the talus occurred in 75% of the specimens with the addition of external rotation.
REFERENCES: Boon AJ, Smith J, Zobitz ME, et al: Snowboarder’s talus fracture: Mechanism of injury. Am J Sports Med 2001;29:333-338.
Kirkpatrick DP, Hunter RE, Janes PC, et al: The snowboarder’s foot and ankle. Am J Sports Med 1998;26:271-277.
9. A 63-year-old man with type I diabetes mellitus who underwent open forefoot amputation now has a high fever, and an elevated WBC count and blood glucose levels. Repeat laboratory studies the day after surgery show a WBC count of 9,500/mm3, a serum albumin level of 1.9 g/dL, and a total lymphocyte count of 1,900/mm3. Examination reveals that he is afebrile, and his blood glucose level is now normal. An ultrasound Doppler of the dorsalis pedis artery shows an ankle-brachial index of 0.6. A transcutaneous partial pressure measurement of oxygen at the ankle joint shows a level of 38 mm Hg. What is the best course of action?
1- Guillotine transtibial amputation
2- Standard transtibial amputation with a posterior myocutaneous flap and immediate prosthetic limb fitting
3- Culture-specific antibiotic therapy, open wound management, and metabolic/nutritional therapy
4- Culture-specific antibiotic therapy and Syme ankle disarticulation
5- Two-stage Syme ankle disarticulation
PREFERRED RESPONSE: 3
DISCUSSION: This patient appears to have adequate blood supply to heal a Syme’s ankle disarticulation but is currently malnourished because of the systemic infection, and is likely to progress to wound failure. Therefore, the initial management of choice is culture-specific antibiotic therapy, open wound management, and nutritional supplementation. If his serum albumin rises to a minimum of 2.5 gm/dL, he can undergo elective Syme’s ankle disarticulation. If the serum albumin does not rise within a short period of time, he should undergo transtibial amputation.
REFERENCE: Pinzur MS, Stuck RM, Sage R, et al: Syme ankle disarticulation in patients with diabetes. J Bone Joint Surg Am 2003;85:1667-1672.
QUESTION 13 OF 50
**A prospective outcome study is performed at a single institution to analyze the potential differences in treating intertrochanteric hip fractures with a plate/screw device versus an intramedullary device. No specific randomization is performed because an equal number of surgeons have p
Scientific References
for the use of one of these devices and they are allowed to continue their preferred method. Hip- specific and general health-related outcome measures are used, an excellent follow-up rate of 85% of the patients at 2 years is accomplished, and there appears to be results that favor the intramedullary device but the confidence intervals are wide. This study would be considered to carry what level of evidence?**
1
I
2
II
3
III
4
IV
5
V
#
**
This is a prospective comparative study but is not randomized or blinded and
is therefore a Level II therapeutic study. To qualify as Level I, it would need to be a high- quality randomized trial with narrow confidence intervals regardless of a significant difference or no difference in outcomes. Level III would be
case-control studies or retrospective comparisons. Level IV is case series and Level V is expert opinion.
QUESTION 14 OF 50
of 100
The most appropriate pedorthic management of symptomatic interdigital neuroma involves
1
a metatarsal pad.
2
a dancer's pad.
3
a custom foot orthosis.
4
a medial heel wedge.
- a metatarsal pad.
QUESTION 15 OF 50
of 100
The most common complication associated with corticosteroid injection for the treatment of interdigital neuroma is
1
Infection
2
Chronic regional pain syndrome (CRPS)
3
Hammertoe deformity
4
Hives
Interdigital neuromas represent perineural fibrosis of the intermetatarsal nerve most commonly seen in the second and third web spaces. The photographs depict a neuroma in the second web space, which is less common than in the third space. Its hypoechoic appearance is characteristic on ultrasound. PVNS occurs in joints. Lipomas are fatty tumors. A ganglion cyst can occasionally occur adjacent to a nerve, but it has a cystic appearance.
The most popular theory on the etiology of interdigital neuromas is compression neuropathy by the intermetatarsal ligament. The plantar approach for the resection of interdigital neuromas has become more popular, especially for recurrent neuromas. The major advantage is better visualization and access to the neuromas.
Infection and allergic reactions such as hives are rare after steroid injection. CRPS is not known to occur in this setting. Hammertoe formation can occur, especially after multiple steroid injections into an interdigital neuroma.
RECOMMENDED READINGS
Schon LC, Reed MA. Disorder of the nerves. In: Coughlin MJ, Saltzman CL, Anderson RB, eds. Mann's Surgery of the Foot and Ankle. 9th ed. Philadelphia, PA: Elsevier-Saunders; 2014:622-641.
[Gauthier G. Thomas Morton's disease: a nerve entrapment syndrome. A new surgical technique. Clin Orthop Relat Res. 1979 Jul-Aug;(142):90-2. PubMed PMID: 498653. ](http://www.ncbi.nlm.nih.gov/pubmed/498653)[View](http://www.ncbi.nlm.nih.gov/pubmed/498653)[ ](http://www.ncbi.nlm.nih.gov/pubmed/498653)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/498653)
CLINICAL SITUATION FOR QUESTIONS 96 THROUGH 98
Figure 96 is the anteroposterior projection foot radiograph of a 35-year-old woman who is injured in a high-speed motorcycle collision. Her assessment reveals an isolated injury. Her pulses are palpable and her neuromotor examination is intact. There is tenting of skin with ecchymosis over the second metatarsal. The foot is extremely swollen but not tense. Passive toe range of motion is painless.
QUESTION 16 OF 50
Which of the following defects occurs in Albright hereditary osteodystrophy (pseudohypoparathyroidism):
1
Type X collagen
2
Sulfate transporter gene
3
Beta glucosidase
4
Galpha S (GNAS1)
5
C arbonic anhydrase type II, proton pump
Pseudohypoparathyroidism (PHP) (Albright Hereditary Osteodystrophy [AHO]) - end organ insensitivity; in AHO, germline mutation that leads to loss of function of Galpha S (GNAS1); causes end-organ resistance to PTH (Zaleske).
1/. PHP - short stature, short metacarpals (4th and 5th), rounded facies a. Mental retardation, tetany
b. Sex-linked dominant
2/. Laboratory features a. Hypocalcemia
b. Hyperphopshatemia c. Normal PTH
3/. Other features
The other responses refer to:
Metaphyseal chondrodysplasia (Schmid type): Type X collagen
Diastrophic dysplasia: Sulfate transporter gene
Gaucher's disease: Beta glucosidase
Osteopetrosis: C arbonic anhydrase type II, proton pump
QUESTION 17 OF 50
Figure 1
A 15-year-old boy presents with a 2-year history of pain in the foot associated with a sense stiffness and of giving way of the ankle. Upon examination, pain in the sinus tarsi, slightly decreased subtalar motion, and normal ankle motion with no apparent instability are noted. A lateral foot radiograph is presented. The next radiograph to obtain is:
1
Anteroposterior view of the ankle
2
Inversion stress view of the ankle
3
Axial view of the hindfoot
4
30° internal oblique view of the foot
5
Anteroposterior view of the foot
This child presents with symptoms suggestive of a tarsal coalition. There is stiffness, and symptoms of ankle discomfort or instability. On the lateral radiograph, there is consolidation of trabeculation under the posterior facet in the shape of a âC â, a typical finding of a middle facet coalition, which should be investigated further with an axial view of the subtalar joint (Harris).
QUESTION 18 OF 50
-is the radiograph of a 58-year-old woman who is right-hand dominant and has fallen on her flexed right elbow and is seen in the emergency department reporting isolated episodes of right elbow pain. Examination reveals that the skin is contused but intact, and her distal neurovascular examination is normal. What is the most appropriate treatment?
1
Percutaneous pinning
2
Closed reduction and extension casting
3
Fragment excision and triceps advancement
4
Open reduction and internal fixation with plate fixation
5
Open reduction and internal fixation with tension band wire construct
Musculoskeletal Trauma Self-Assessment Examination DISCUSSION: The patient has sustained an isolated, closed fracture of the olecranon without associated
instability. The bone is radiographically osteopenic and the fracture is displaced, comminuted, and
includes articular marginal impaction. Plate fixation is preferred in the presence of comminution or
associated transolecranon or radiocapitellar instability. Displaced fractures are generally treated surgically
in an effort to restore articular congruity, restore extensor function, and to allow for early mobilization in an effort to maximize functional outcomes. A tension band wire construct is a commonly used technique but is reserved for simple fracture patterns without comminution. Excision and triceps advancement can be considered in elderly, low-demand patients that have small unreconstructable fracture patterns without associated elbow instability.
No detailed explanation provided for this question.
QUESTION 19 OF 50
A 53-year-old man reports acute, severe left shoulder pain after undergoing abdominal surgery 10 days ago. Initial management, consisting of anti-inflammatory drugs, physical therapy, and a subacromial injection of corticosteroid, fails to provide relief. Reexamination of the shoulder 2 months after the onset of symptoms reveals atrophy of the infraspinous and supraspinous fossa and profound weakness of active abduction and external rotation. His neck is supple with a full range of motion. Plain radiographs and an MRI scan of the shoulder are normal. What diagnostic study should be performed next in the evaluation of this patient?**
1
Shoulder arthrography
2
MRI of the cervical spine
3
CT of the head
4
Technetium Tc 99m bone scan
5
Electromyography and nerve conduction velocity studies
Suprascapular nerve palsy is a fairly uncommon yet well-known cause of shoulder pain and weakness. A variety of causes have been described, including compression by a ganglion cyst, an anomalous or thickened superior transverse scapular ligament, a humeral and scapular fracture, and traction or kinking of the nerve in the suprascapular notch.
In this patient, the injury is most likely caused by traction or compression of the nerve in the suprascapular notch as the result of positioning during abdominal surgery; therefore, the studies of choice are electromyography and nerve conduction velocity studies. While MRI of the cervical spine may be of some value in ruling out a radiculopathy, the clinical history does not support such a cause for this condition.
REFERENCES: Rengachary SS, Neff JP, Singer PA, Brackett CE: Suprascapular entrapment neuropathy: A clinical, anatomical, and comparative study. Part 1: Clinical study. Neurosurgery 1979;5:441-446.
Rengachary SS, Burr D, Lucas S, Hassanein KM, Mohn MP, Matzke H: Suprascapular entrapment neuropathy: A clinical, anatomical and comparative study. Part 2: Anatomical study. Neurosurgery 1979;5:447-451.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthoscopy 1990;6:301-305.
QUESTION 20 OF 50
of 100
With respect to the structure identified by the arrow in Figure 22b, the meniscofemoral 25
ligaments are
1
uniformly present, and are positioned posterior to the injured ligament.
2
uniformly present, with one positioned anterior and the other positioned posterior to the injured ligament.
3
variably present, and are positioned posterior to the injured ligament.
4
variably present, with one positioned anterior and the other positioned posterior to the injured ligament.
The stress radiographs demonstrate posterior instability of the right knee in flexion. The MR images demonstrate injury to both the anterior and posterior cruciate ligament (PCL), with the stump identified with the arrow on the MR image (Figure 22b). The PCL has 2 functional bands. The anterolateral bundle originates from the roof of the intercondylar notch. It runs in a posterolateral direction onto the tibial crest between the posterior attachment of the medial and lateral menisci. During a double-bundled posterior ligament reconstruction, the
anterolateral bundle is tensioned with the knee in a position of mid flexion. The posteromedial bundle has a variable pattern of tension both in extension and in high flexion. Tensioning of the posteromedial bundle in extension may contribute to resistance against knee hyperextension.
The meniscofemoral ligaments are variably present. Although 93% of knees have been reported to have at least 1 meniscofemoral ligament present, both ligaments are simultaneously present in approximately 50% of knees. The ligament of Humphrey (anterior meniscofemoral ligament) and ligament of Wrisberg (posterior meniscofemoral ligament) are delineated by their anatomic relationship to the posterior cruciate.
RECOMMENDED READINGS
1. [Amis AA, Bull AM, Gupte CM, Hijazi I, Race A, Robinson JR. Biomechanics of the PCL and related structures: posterolateral, posteromedial and meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2003 Sep;11(5):271-81. Epub 2003 Sep 5. Review. PubMed PMID: 12961064.](http://www.ncbi.nlm.nih.gov/pubmed/12961064)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12961064)
2. Amis AA, Gupte CM, Bull AM, Edwards A. Anatomy of the posterior cruciate ligament and the meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):257-63. Epub 2005 Oct 14. Review. PubMed PMID: 16228178.
View Abstract at PubMed . 26
QUESTION 21 OF 50
A 45-year-old woman sustains an injury to her lower leg. Examination reveals that there is a deformity with no neurologic or vascular problems. The skin is intact. Radiographs are shown in Figures 46a and 46b. Which of the following factors would make closed management the least appropriate choice for this injury?
1
Spiral fracture pattern
2
Low-energy mechanism
3
Amount of shortening
4
Fracture of the fibula at a different level
5
Ipsilateral femoral fracture
All the factors listed, with the exception of an ipsilateral femoral fracture, are representative of a low-energy stable tibial shaft fracture that will do well with closed reduction and immobilization in a long leg cast, followed by weight bearing as tolerated and then a functional brace or patellar tendon bearing cast until union is achieved. Shortening will not increase from that seen on these initial radiographs. The spiral fracture provides a broad surface for healing, and the fibular fracture at another level indicates a stable soft-tissue envelope which, with the immobilization device, will stabilize the fracture reduction. An ipsilateral femoral fracture is a strong indication to surgically stabilize both fractures.
REFERENCES: Trafton PG: Tibial shaft fractures, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 2153-2169.
Martinez A, Sarmiento A, Latta LL: Closed fractures of the proximal tibia treated with a functional brace. Clin Orthop 2003;417:293-302.
QUESTION 22 OF 50
of 100
A 65-year-old woman with diabetes has fever and erythema 2 weeks after undergoing instrumented spinal fusion.
1
Postoperative deep surgical site infection
2
Proximal junctional kyphosis
3
Pedicle screw cut-out
4
Pseudarthrosis
5
Sagittal imbalance
- Postoperative deep surgical site infection
QUESTION 23 OF 50
A 66-year-old woman who underwent a right total knee arthroplasty 13 years ago now has pain, knee effusion, squeaking, and grinding in the operated knee. The patellar view radiograph is shown in Figure 54. What is most likely to be encountered during revision arthroplasty?
1
Loose femoral and/or tibial component
2
Fractured patella
3
Extensive metallosis
4
Patellar clunk
5
Ruptured extensor mechanism
DISCUSSION: Wear of the polyethylene insert of a metal-backed patellar or tibial component is a well- recognized complication following total knee arthroplasty. If the polyethylene insert completely wears out, the underlying metal-backed base plate will be in direct contact with the femoral component, resulting in scratching of the components and release of metal debris. The released metal debris results in black “tattooing” of the tissues or so-called metallosis. In addition, reactive synovitis and osteolysis occur secondary to a host response to both polyethylene debris and metal particles. Patients may report knee pain, swelling, squeaking, and an unstable feeling during walking and standing. Patellar clunk syndrome is characterized by the development of a fibrous nodule on the deep aspect of the quadriceps tendon that falls into the intercondylar notch of the femoral component during knee flexion.
REFERENCES: Chang FY, Tseng KF, Chen WM, et al: Metal-backed patellar component failure in total knee arthroplasty presenting as a giant calf mass. J Arthroplasty 2003;18:227-230.
Leopold SS, Berger RA, Patterson L, et al: Serum titanium level for diagnosis of a failed, metal-backed patellar
component. J Arthroplasty 2000;15:938-943.
Patel J, Ries MD, Bozic KJ: Extensor mechanism complications after total knee arthroplasty. Instr Course Lect 2008;57:283-294.
Figure 55a Figure 55b
QUESTION 24 OF 50
of 100 A 45-year-old construction worker sees a surgeon 23 days after sustaining an eccentric injury to his dominant right elbow. An MRI demonstrates a distal biceps tendon rupture with 5 cm of proximal retraction. In the operating room, the surgeon encounters good tissue quality but finds that primary repair can only be performed with the elbow hyperflexed to 70°. What is the best next step?
1
Proceed with primary repair with the elbow hyperflexed
2
Use interposition allograft to reconstruct with elbow in extension
3
Tenodese distal biceps tendon to underlying brachialis muscle
4
Forego primary repair, but perform stump debridement
DISCUSSION:
Distal biceps ruptures, although relatively less common in comparison with other upper extremity tendon injuries, still garner considerable attention in the orthopaedic literature. The mechanism of injury typically results from an eccentric extension load to a flexed elbow. A biceps-deficient arm can result in up to 40% loss of supination strength and up to 80% loss of supination endurance. A delay in diagnosis can compromise the ability to reduce the tendon back to its anatomic insertion without having to hyperflex the elbow. Current literature confirms the ability to safely proceed with primary repair even with the elbow flexed up to 100° without fear of developing a flexion contracture. With time, patients can anticipate restoration of full elbow extension. An interposition graft should be used for a poor residual tendon quality stump <4 cm in length and in cases of delay to surgery of >6 weeks. Biceps to brachialis tendon transfer does not restore supination
strength. Isolated debridement of the distal tendon would not be an appropriate treatment.
QUESTION 25 OF 50
of 100
Germline alterations associated with this condition
1
affect proteins exostosin-1 (EXT1) and exostosin-2 (EXT2).
2
encode the alpha subunit of the stimulatory G-protein-coupled receptor, Gsa.
3
cause neoplastic cells to express vimentin, CD99, and FLI-1.
4
produce the WWTR1-CAMTA1 fusion.
The radiograph reveals multiple osteochondromas consistent with multiple hereditary exostoses (also termed osteochondromatosis). This is inherited in an autosomal-dominant fashion through the EXT1 and EXT2 genes. Thus, the likelihood of this patient’s children being affected is 50% for each child. An autosomal dominant manner with germiline alterations in EXT1 located at 8q24 and EXT2 located at 11p11-p12 occurs in approximately 1 in 50,000 people.
Multiple hereditary exostoses is a disease in a spectrum of diseases caused by alterations in either EXT1 or EXT2. The gene products of EXT1 and EXT2 genes are considered essential for the function of fibroblast growth factor and Indian hedgehog signaling in the normal growth plate and catalyze heparin sulphate polymerization. The G-protein-couple receptor is involved in fibrous dysplasia, the expression of vimentin, and CD99. FLI-1 is associated with Ewing sarcoma, and WWTR1-CAMTA1 fusion is associated with epithelioid hemangioma, which is not related to multiple hereditary exostoses.
RECOMMENDED READINGS
36. Multiple hereditary osteochondromatosis. In: Nielsen GP, Rosenberg AE, eds. _Diagnostic Pathology: Bone_. Manitoba, Canada: Amirsys; 2013:12-15.
37. [Busse-Wicher M, Wicher KB, Kusche-Gullberg M. The exostosin family: proteins with many functions. Matrix Biol. 2014 Apr;35:25-33. doi: 10.1016/j.matbio.2013.10.001. Epub 2013 Oct 12. Review. PubMed PMID: 24128412.](http://www.ncbi.nlm.nih.gov/pubmed/24128412)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24128412)
CLINICAL SITUATION FOR QUESTIONS 51 THROUGH 54
Figures 51a and 51b are the radiographs of an 83-year-old active, independent, and healthy woman who has experienced 2 months of right lower thigh and knee pain. Her arthroplasty was previously well functioning, but her pain has increased progressively for several weeks. While exiting a car she “bumped” her knee against the door, felt a “crack,” and developed excruciating pain. She can no longer ambulate and was brought to the hospital
QUESTION 26 OF 50
What is the most common maxillofacial/dental injury in ice hockey?
1
Temporomandibular
2
Lip laceration
3
Tooth avulsion
4
Crown fracture
5
Mandible fracture
DISCUSSION: Lahti and associates reported that the most common dental injury in a study of 479 injured ice hockey players was a noncomplicated crown fracture, which accounted for 43.5% of all maxillofacial/ dental injuries. The most common cause of injury was a blow from an ice hockey stick. As a cause of injury, the stick was approximately three times as common in games as in training, and only 10% of injured players wore some sort of protective guard. A tooth avulsion is a partial or complete
displacement of the tooth from aleveolar support. A crown fracture is an incomplete loss or fracture of the tooth enamel without loss of the tooth. The other injuries (mandible fracture, lip laceration, tooth
avulsion, and temporomandibular contusion) occur but are not nearly as common.
Scientific References
: Lahti H, Sane J, Ylipaavalniemi P: Dental injuries in ice hockey games and training. Med Sci Sports Exerc 2002;34:400-402.
Minkoff J, Stecker S, Varlotta GP, et al: Ice hockey, in Fu FH, Stone DA (eds): Sports Injuries, ed 2.
Philadelphia, PA, 2001, pp 516-517.
Figure 2a Figure 2b Figure 2c
QUESTION 27 OF 50
of 100 A 54-year-old woman undergoes an interposition arthroplasty that fails and requires conversion to a total elbow arthroplasty. She has progressive elbow pain and radiographic loosening. Erythrocyte sedimentation rate and C-reactive protein are normal. Joint aspiration is positive for Staphylococcus epidermidis. What surgical treatment would best optimize function and decrease risk of recurrence?
1
Resection arthroplasty
2
Single-stage revision total elbow arthroplasty
3
Two-stage revision elbow arthroplasty
4
Aggressive arthroscopic debridement and retention of components
DISCUSSION
The most reliable surgical option in this case for eradicating a deep infection following a total elbow arthroplasty is a two-stage revision. One study, however, reported that staged reimplantation of an infected total elbow replacement could be successful in the setting of organisms other than S epidermidis. Arthroscopic debridement is not a viable option with poorly fixed or loose components. A single-stage revision, while considered an option in hip and knee arthroplasty, has not been definitively proven to be an option for revision total elbow arthroplasty. Single-stage revision has shown moderate success in the setting of Staphylococcus aureus infections, although with only short-term follow-up. A resection arthroplasty would likely be successful in managing the deep infection but would not optimize the functional result. Resection arthroplasty
is best reserved for low-demand or infirm patients.
QUESTION 28 OF 50
A 12-year-old boy has a head-on head collision while playing soccer. He had no loss of consciousness
but has persistent headaches for 2 weeks. The patient is now back to school and has no headaches. What is the best next step?
1
Return to full soccer activity
2
Start light aerobic activity
3
Obtain baseline neuropsychological testing
4
MRI scan of the brain
Mild traumatic brain injury is common in the adolescent child. Neuropsychological examination is widely used but, in this case, the patient is asymptomatic and has no baseline testing. There is a limited role for MRI in the recovery process of concussions. Furthermore, higher levels of physical/cognitive activity should be avoided due to their potential to increase total recovery time. In this scenario, a graduated return to activity is most appropriate thus, the next appropriate step is to start light aerobic activity.
QUESTION 29 OF 50
When a Workers' Compensation patient recovers after an injury to a point that further restoration of function is no longer anticipated, he or she is said to have reached which of the following?
1
Functional capacity
2
Maximum medical improvement
3
Permanent disability
4
Impairment rating
5
Predesignation
#
**
This is the definition of maximum medical improvement (MMI). The patient has essentially reached the plateau of his improvement.
Functional capacity evaluations (FCE) are based upon a theoretical model of comparing job demands to worker capabilities. The results of FCEs are often used to determine musculoskeletal capacity to return to work.
Strong et al. reported on the use of FCE in the Workers' Compensation system, and note how these FCE results are required by employers to determine the level of return to work of their employees. They also mention that the reports are frequently perceived with a negative tone. The employees reported a wider range of restrictions in their varied life roles than did the FCE reports, which deal more narrowly with work roles.
Pransky et al. reported that although FCE's are relied upon for determination of ability to perform physical work, several scientific, legal, and practical concerns persist. They note that test criteria often do not accurately reflect real-life job requirements or performance, and subjective evaluation remains common. They conclude that more research into predictive linking of FCE outcomes with occupational outcomes is necessary to determine their role in the Workers' Compensation system.
Incorrect Answers:
1: A functional capacity evaluation (FCE) is set of tests, practices and observations that are combined to determine the ability of the evaluated to function in a variety of circumstances (most often employment) in an objective manner.
3: Permanent disability is any lasting disability that results in a reduced earning capacity after maximum medical improvement is reached; this implies that MMI must be reached before this is determined.
4: Impairment rating is an objective data point obtained by a physician reviewing the patient's overall condition during a functional capacity evaluation.
5: This is the process a patient uses to tell their employer they want a personal physician to treat them for a work injury.
QUESTION 30 OF 50
Osteomyelitis in the child
1
requires operative debridement in the majority of cases.
2
requires antibiotic therapy for 3 to 6 weeks.
3
never causes growth disturbance of the involved bone.
4
occurs in the diaphysis in most cases.
5
Always crosses the physis in children
Osteomyelitis in the child requires 3-6 weeks of antiobiotics which may be administered parenterally or internally.C orrect Answer:
requires antibiotic therapy for 3 to 6 weeks.
QUESTION 31 OF 50
All of the following statements are true regarding the Bernese osteotomy except:
1
The Bernese osteotomy was popularized by Ganz.
2
The Bernese osteotomy is a reorientation osteotomy.
3
The Bernese osteotomy allows for unrestricted correction while keeping the pelviCring intact.
4
The Bernese osteotomy can be used in approximately 15% of dysplastiChips.
5
The Bernese osteotomy can be used only in anteverted dysplastiChips.
The Bernese periacetabular osteotomy, which was popularized by Ganz, is a reorientation osteotomy that allows for unrestrained correction while keeping the pelviCring intact and can be used in approximately 17% of dysplastiChips. The Bernese osteotomy can be used in anteverted and retroverted dysplastiChips
QUESTION 32 OF 50
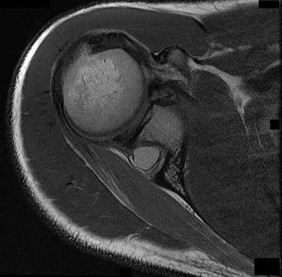
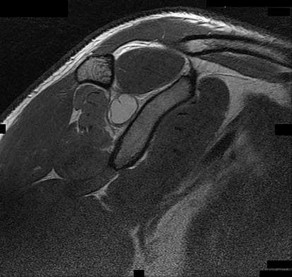
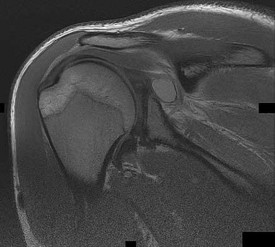
of 100
The cystic lesion shown on the MR images in Figures 46a through 46c should cause denervation changes in which muscle? A B
1
Subscapularis
2
Teres major
3
Infraspinatus
4
Supraspinatus
42
The cystic lesion is shown in an area adjacent to the spinoglenoid notch. A space-occupying lesion in this area has the potential to compress the suprascapular nerve as it passes through the spinoglenoid notch to innervate the infraspinatus. Compression of the nerve can cause denervation and atrophy of the infraspinatus muscle. The supraspinatus is innervated by the suprascapular nerve proximal to the compressive lesions and will not undergo atrophy. The subscapularis and the teres major are innervated by the subscapular nerve.
RECOMMENDED READINGS
1. Getz CL, Ramsey ML, Williams GR. Paralabral cysts of the shoulder. In: Galatz LM, ed. Orthopaedic Knowledge Update: Shoulder and Elbow 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:339-344.
2. [Takagishi K, Saitoh A, Tonegawa M, Ikeda T, Itoman M. Isolated paralysis of the infraspinatus muscle. J Bone Joint Surg Br. 1994 Jul;76(4):584-7. PubMed PMID: 8027145.](http://www.ncbi.nlm.nih.gov/pubmed/8027145)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8027145)
QUESTION 33 OF 50
An otherwise healthy 76-year-old woman has pain 2 years after total hip arthroplasty. The clinical
photograph in Figures below demonstrates her skin envelope, and associated radiograph. Her C-reactive protein level is normal, and her erythrocyte sedimentation rate is mildly elevated. The white blood cell count is normal. Hip aspiration attempted under fluoroscopy generates no fluid. What is the best definitive treatment?
1
Repeat left hip aspiration
2
Initiation of a wound care consult and oral antibiotics
3
Irrigation and debridement with closure of the dehisced wound, performance of a liner exchange, and administration of intravenous antibiotics
4
Debridement of the wound, explant of the total hip, placement of a spacer, and administration of
intravenous antibiotics DISCUSSION:
This patient clearly has a chronically infected total hip arthroplasty, indicated by the open, draining sinus, as well as trochanteric bone resorption on radiographs, and two years of pain. Recently, specific guidelines have been published to better help the clinician define infection. Repeating the hip aspiration is unnecessary, because infection is already evident. Initiating a wound care consult would not address the underlying infection. The determination whether to retain the components or perform a two-stage exchange is based more on the acuity of infection. In this particular case, the patient is chronically infected. Irrigation and debridement with a liner exchange and retention of the components are reserved for the acute setting.
QUESTION 34 OF 50
When conducted at near physiologic strain rates, tensile studies of the inferior glenohumeral ligament (IGHL) have shown that the
1
anterior band of the IGHL has the greatest stiffness and the glenoid insertion site shows greater strain than the ligament midsubstance.
2
anterior band of the IGHL has the greatest stiffness and the ligament midsubstance shows greater strain than the glenoid insertion site.
3
axillary pouch of the IGHL has the greatest stiffness and the glenoid insertion site shows greater strain than the ligament midsubstance.
4
axillary pouch of the IGHL has the greatest stiffness and the ligament midsubstance shows greater strain than the glenoid insertion site.
5
posterior portion of the IGHL has the greatest stiffness and the glenoid insertion site shows greater strain than the ligament midsubstance.
Tensile testing of the inferior glenohumeral ligament at near physiologic strain rates has shown that the anterior band of the IGHL has the greatest stiffness of the three ligament regions and the glenoid insertion site shows greater strain than the ligament midsubstance.
REFERENCES: Bigliani LU, Pollock RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Ticker JB, Bigliani LU, Soslowsky LJ, Pawluk RJ, Flatow EL, Mow VC: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
QUESTION 35 OF 50
of 100
An 18-year-old female collegiate swimmer has a 1-year history of posterior shoulder pain and popping and a bilateral 2-cm sulcus sign.
1
Isolated posterior instability with a posterior labral tear
2
Multidirectional instability
3
Anterior shoulder subluxation
4
Thoracic outlet syndrome
5
Superior labrum anterior to posterior (SLAP) tear
- Multidirectional instability_
QUESTION 36 OF 50
of 100
What is the best next step? 1- Knee aspiration
1
Blood cultures
2
Indium-labeled WBC scan
3
Pelvic radiographs
- Blood cultures
QUESTION 37 OF 50
A 45-year-old woman who recently underwent biopsy of a lymph node in the right posterior cervical triangle now finds it difficult to hold objects overhead and has diffuse aching in the right shoulder region. What is the most likely diagnosis?
1
Rotator cuff tear
2
Rhomboid paralysis
3
Deltoid paralysis
4
Triceps paralysis
5
Trapezius paralysis
The trapezius is innervated by the spinal accessory nerve. The nerve is superficial in the area of the posterior cervical triangle and is prone to injury during dissection. Paralysis of the trapezius causes loss of scapular stability when forward flexion or abduction of the shoulder is attempted.
REFERENCES: Vastamaki M, Solonen KA: Accessory nerve injury. Acta Orthop Scand 1984;55:296-299.
Leffert RD: Neurological Problems, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 759-760.
QUESTION 38 OF 50
A 15-year-old football player was diagnosed with infectious mononucleosis 2 weeks ago. Today he states that he is relatively asymptomatic and would like to return to play. At what point can the patient return to full contact practice?
1
Now if splenomegaly has resolved
2
Now if treated with oral valacyclovir
3
In 2 weeks if splenomegaly has resolved
4
After a 4-week course of oral valacyclovir
Infectious mononucleosis presents with fever, pharyngitis, fatigue and lymph node enlargement. It is common among individuals in their teens and early twenties. Participation in contact activities during an acute illness with unresolved splenomegaly increases the risk of splenic rupture. Evidence- based return to play criteria recommend that a patient may return to full- contact activities 4 weeks after the onset of their symptoms with resolution of splenomegaly. An ultrasonography of the spleen can help confirm that the spleen has returned to normal size. 75
QUESTION 39 OF 50
The percentage of patients 20 to 40 years of age who have recurrent shoulder instability is:
1
10%
2
20%
3
40%
4
50%
5
60%
Suffering from recurrent instability in the shoulder joint depends on a patientâs age and activity level. Ninety percent of patients younger than 20 years of age have recurrent instability. In patients 20 to 40 years of age, 40% have recurrent instability
QUESTION 40 OF 50
Which of the following has been associated with an increased likelihood of stress shielding after cementless total hip arthroplasty?
1
Use of titanium alloy femoral components
2
Use of proximally fixed femoral components
3
Use of distally fixed femoral components
4
Use of press-fit stems in patients with narrow intramedullary canals
5
Use of plasma sprayed components
DISCUSSION: Although stress shielding has not been associated with adverse clinical outcomes to date, it is a commonly observed process after cementless total hip arthroplasty. Factors that increase the magnitude of stress shielding include the use of distally fixed cobalt-chrome stems, particularly in patients with osteoporosis. Large diameter femoral components (larger than 18 mm in diameter) have also been associated with an increased prevalence of stress shielding.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 345-368.
QUESTION 41 OF 50
of 100
Advanced imaging, to include MRI and CT, have been obtained in the workup of patients with low back pain. What imaging finding has been associated with reasons for back pain?
1
Disk degeneration
2
Facet arthropathy
3
Spinal stenosis
4
Spondylolysis
■ Low back pain remains a common presenting condition to not only primary care physicians, but to subspecialists. Studies assessing the anatomy of the spine, to include the intervertebral disks, vertebral body morphology, facet joints, and the paraspinal muscles have been performed. Spinal stenosis is the only advanced imaging finding that has been associated with reproducible reasons for back pain.
QUESTION 42 OF 50
Which of the following statements is true regarding Lyme disease:
1
C ardiac and neurologic symptoms are the most common manifestations of the disease.
2
Arthritic symptoms primarily affect large joints and a majority of patients are cured with antibiotic therapy.
3
The characteristic skin rash occurs late in the disease and can be permanently disfiguring.
4
Arthritic symptoms often do not fully resolve with antibiotic treatment, with a majority of patients progressing on to a rheumatoid-like destructive arthritis.
5
Lyme disease is easy to diagnose and a majority of cases are picked up after a few weeks.
Approximately 60% of patients develop arthritic symptoms that primarily affect large joints. The prognosis for most patients is good after treatment with antibiotics.
C ardiac and neurologic symptoms occur in a minority of patients, however, they can be the most serious symptoms. Erythema chronicum migrans is the characteristic skin rash. The rash tends to remit with antibiotic treatment and permanent disfigurement is not typically a problem.
Only 1%-2% of pediatric patients develop chronic arthritis.
Lyme disease may be difficult to diagnose because of the numerous possible presentations.
QUESTION 43 OF 50
A 50-year-old man fell from a height of 10 feet and sustained an axial loading injury to the cervical spine.He reports neck pain and right upper extremity weakness and has weakness in the lower extremities.An MRI scan is shown Figure 67. What imaging study should be obtained next to further evaluate this patient?
1
Cervical spine flexion and extension radiographs
2
AP radiograph of the cervical spine
3
CT of the cervical, thoracic, and lumbar spine
4
Electromyography and nerve conduction velocity studies of the upper extremities
5
MRI of the lumbar spine
The MRI scan shows a C7 burst fracture. A CT scan of the cervical spine will allow for optimal evaluation of this C7 burst fracture. Specifically, it will provide additional osseous detail and will assist with the detection of additional fractures,
including those of the posterior elements. Additional CT imaging of the thoracic and lumbar spine is required to rule out concommitant injuries (which may be present in 10% to 15% of patients). Anteroposterior and lateral cervical spine radiographs would be a good option for further evaluation but are not included in the available choices here.
Cervical spine flexion and extension radiographs should not be obtained in a patient who is known to have a relatively unstable spine and a neurologic deficit. Electromyography and nerve conduction velocity studies are best used to evaluate for cervical radiculopathy secondary to degenerative abnormalities and are usually not indicated in the acute trauma setting.
QUESTION 44 OF 50
Which of the following bone tumors commonly occurs in patients with closed physes between 20 and 50 years of age:
1
Osteoid osteoma
2
Chondromyxoid fibroma
3
Solitary bone cyst
4
Giant cell tumor
5
Non-ossifying fibroma
Certain bone tumors have a predilection to occur in certain age groups. Non-ossifying fibroma, chondromyxoid fibroma, solitary bone cyst, and osteoid osteoma tend to occur in young patients with open physes. In contrast, giant cell tumor of bone rarely occurs in patients with open physes. When giant cell tumor occurs in children with open physes, it tends to involve only the metaphysis.
The common tumors in children with open physes are:
Benign
Osteoid osteoma Osteochondroma Chondroblastoma Solitary bone cyst
Malignant Osteosarcoma Ewingâs tumor Leukemia
In adults with closed physes, the common tumors are
Benign
Giant cell tumor
Pagetâs disease
QUESTION 45 OF 50
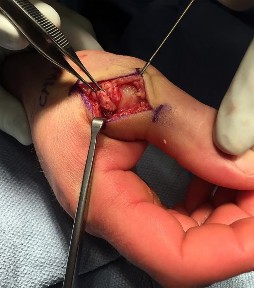
A 32-year-old man sustained an injury to the right thumb metacarpophalangeal (MP) joint ulnar collateral ligament (UCL) and is undergoing surgical repair (Figure 1). What structure in the clinical photograph is blocking reduction of the ulnar collateral ligament?
1
Extensor pollicis longus (EPL) tendon
2
Adductor aponeurosis
3
EPB and dorsal capsule
4
Ulnar sesamoid bone and volar plate
When the thumb MP UCL is torn from the proximal phalanx, the distal stump can be displaced superficial to the adductor aponeurosis, known as a Stener lesion. The adductor aponeurosis effectively blocks reduction of the ligament to the normal attachment site. The EPB and EPL tendons are dorsal to the UCL, and the ulnar sesamoid bone/volar plate are in a volar position in relation to the UCL. The dorsal capsule would also not block reduction of the UCL due to it's anatomic location. The other responses do not block _the UCL with this type of injury._
QUESTION 46 OF 50
Which of the following categories of slipped capital femoral epiphysis (SC FE) is associated with the highest risk of a grade III
slip:
1
Idiopathic SC FE
2
Renal failure
3
Radiation therapy
4
Hypothyroidism
5
Growth hormone deficiency
A grade III slip refers to more than 50% displacement of the epiphysis. Renal failure is associated with the highest risk (43%) of progressing to a grade III slip. Fortunately, these slips are usually stable.
QUESTION 47 OF 50
-When compared with reamed intramedullary nailing for an unstable diaphyseal tibia fracture, undreamed nailing is associated with which of the following?
1
Longer surgical times
2
Higher infection rates
3
Lower functional outcome scores
4
Similar union rates in open fractures
5
Higher incidence of pulmonary complications
No detailed explanation provided for this question.
QUESTION 48 OF 50
The incidence of dermal reactions and positive skin-patch testing to Co, Ni, and Cr in patients with total joint replacement with unstable prostheses is:
1
5% above those of the general population
2
10% above those of the general population
3
15% above those of the general population
4
30% above those of the general population
5
50% above those of the general population
Metal-induced skin reactions can include contact dermatitis, urticaria ,and/or vasculitis. The incidence of dermal reactions and positive skin-patch testing to Co, Ni, and Cr in patients with total joint replacement with stable and loose prostheses increases by
15% and 50% respectively, above those of the general population
QUESTION 49 OF 50
A 78-year-old woman has a history of chronic low back pain. She denies any extremity problems. Her pain is worse in the morning, and gets better, although it does not go away, as the day goes on. An MRI scan of the lumbar spine is shown in Figure 88. She denies any acute worsening of her symptoms, although in general, her symptoms are slowly worsening. She takes nonsteroidal anti-inflammatory drugs as needed for her pain, but otherwise takes no other medications. What is the next most appropriate step in management?
1
DEXA scan
2
Brace treatment with a Jewett hyperextension brace
3
Anterior lumbar corpectomy and arthrodesis with instrumentation
4
Posterior lumbar decompression and fusion
5
Vertebral cement augmentation
#
**
The patient has MRI findings throughout her lumbar spine consistent with old compression fractures. Given the imaging findings and advanced age, she is at high risk for osteoporosis and subsequent fragility fractures. Management should consist of a DEXA scan to evaluate her degree of osteoporosis and
begin medical treatment as appropriate. Because acute fracture is unlikely, and she has no neurologic compromise, neither bracing nor surgical treatment is indicated.
QUESTION 50 OF 50
of 100
A 65-year-old woman undergoes a lumbar laminectomy for spinal stenosis at the L3-L4 level. The surgery and postsurgical course are uncomplicated. Eight weeks after surgery she has severe left anterior thigh, groin, and knee pain with ambulation and standing. Which condition is the most likely cause of her symptoms?
1
Epidural hematoma
2
Osteoarthritis of the hip
3
Miralgia paraesthetica
4
Facet joint pain
Disorders of the hip can mimic and/or coexist with lumbar spine disorders. The prevalence of hip pain lasting longer than 1 month in patients ages 65 to 74 years is 19%. There is often overlap between their respective signs and symptoms. In a patient with failed back surgery syndrome, hip pathology may have been present before back surgery and not recognized. Osteoarthritis of
the hip typically causes groin and anterior thigh pain. Meralgia paraesthetica is more likely to manifest immediately after surgery. Trochanteric bursitis usually affects the proximal lateral thigh and often can radiate to the distal thigh. Facet joint pain causes low-back pain that can be referred to the gluteal region. Epidural hematoma 6 weeks after surgery is highly unlikely.
RECOMMENDED READINGS
Bolt PM, Wahl MM, Schofferman J: The roles of the hip, spine, sacroiliac joint, and other structures in patients with persistent pain after back surgery. Seminars in Spine surgery 2008;20:14-19.
[Brown MD, Gomez-Marin O, Brookfield KF, Li PS. Differential diagnosis of hip disease versus spine disease. Clin Orthop Relat Res. 2004 Feb;(419):280-4. PubMed PMID: 15021166. ](http://www.ncbi.nlm.nih.gov/pubmed/15021166)[View](http://www.ncbi.nlm.nih.gov/pubmed/15021166)[ ](http://www.ncbi.nlm.nih.gov/pubmed/15021166)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15021166)