This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set 74F2E5)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should**
1
insert a standard humeral prosthesis with cerclage wires at the fracture site and autologous cancellous bone graft.
2
insert a standard humeral component and apply a humeral orthosis postoperatively.
3
cement a long-stemmed humeral component to bypass the fracture site and supplement with cerclage wires.
4
remove all instrumentation, perform an open reduction and internal fixation of the fracture, and delay completion of replacement surgery until the fracture has healed.
5
discontinue the procedure and return for completion of total shoulder replacement when the fracture has healed.
The risk of intraoperative fracture in osteopenic rheumatoid bone is significant. Fractures may occur with dislocation of the head and canal reaming, especially while extending and externally rotating the shoulder. If the fracture occurs at the distal tip of the prosthesis, the use of a long-stemmed prosthesis to bypass the fracture site and supplementation with wire cables has been reported with good results.
REFERENCES: Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346.
Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
Petersen SA, Hawkins RJ: Revision of failed total shoulder arthroplasty. Orthop Clin North Am 1998;29:519-533.
QUESTION 2 OF 50
What is the 5-year overall survival rate for adults with high-grade soft-tissue sarcomas?
1
0%
2
30%
3
50%
4
70%
5
90%
DISCUSSION: The 5-year overall survival rate for deep, high-grade soft-tissue sarcomas is around 50%. The overall survival and disease-free survival rates chiefly depend on the tumor stage, but for all stages combined, most cancer treatment centers report a 5-year overall survival rate of around 70% and a disease-free survival rate of 65%.
Scientific References
: Fleming ID, et al: Manual for Staging of Cancer/American Joint Committee on Cancer, ed 5. Philadelphia, PA, Lippincott Raven, 1997, pp 149-156.
Cheng EY, Dusenbery KE, Winters MR, Thompson RC: Soft tissue sarcomas: Preoperative versus postoperative radiation therapy. J Surg Oncol 1996;61:90-99.
QUESTION 3 OF 50
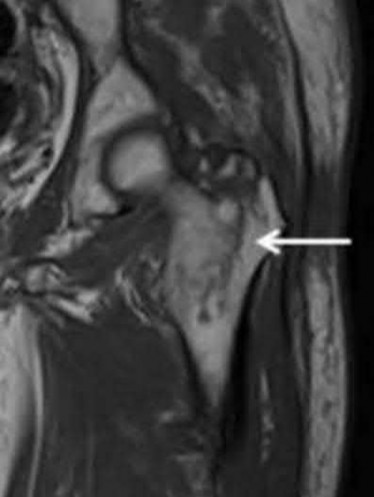
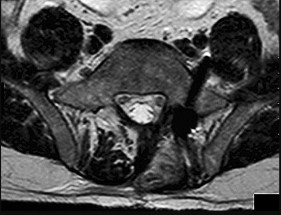
A 58-year-old woman returns for an evaluation of right knee pain after a twisting injury. A small pop was felt at the time of injury. Her pain is medial and she is unable to bear weight. A complete physical examination demonstrated range of motion is 0°to 125°; significant medial joint line tenderness; negative flexion McMurray; negative Lachman; stable to varus and valgus stress at 0° and 30° and negative posterior drawer. Based on her history, physical examination, and the MRI scan shown in Figure 1, what is the diagnosis?
1
Posterior cruciate ligament (PCL) tear
2
Horizontal tear of posterior horn of medial meniscus
3
Posterior root tear of medial meniscus
4
Anterior root tear of medial meniscus
63
The low likelihood that common symptoms associated with meniscal body injury will manifest in patients with root tears makes clinical diagnoses challenging. For instance, patients with a posterior root tear injury may experience joint line pain, but the absence of mechanical symptoms such as locking or catching is probable. Meniscal root tears are also not typically associated with an inciting traumatic event. MRI has become increasingly used in the diagnosis of meniscal root tears. Telltale signs of a root tear include the presence or absence of a ghost sign, which is the absence of an identifiable meniscus in the sagittal plane or high signal replacing the normal dark meniscal signal. The posterior meniscus is seen in sagittal MRI view in all images up to the one that shows the PCL. The posterior root of the medial meniscus attaches anterior to the posterior cruciate ligament (PCL).
QUESTION 4 OF 50
A genetiCmutation accounts for the manifestations of osteopetrosis. Which of the following factors has a genetiCmutation that has been linked to osteopetrosis:
1
Dystrophin
2
PEX (a cellular endopeptidase)
3
CarboniCanhydrase type II proton pump
4
Gs alpha (receptor-coupled signaling protein)
5
EXT1, EXT2 genes
The genetiCdefect in osteopetrosis involves the carboniCanhydrase type II proton pump.
The other answers refer to:
Duchenne muscular dystrophy
 Dystrophin
X-linked hypophosphatemic
rickets PEX (a cellular endopeptidase)
Fibrous dysplasia Gs alpha (receptor-coupled signaling protein)
Multiple hereditary exostoses EXT1, EXT2 genes
QUESTION 5 OF 50
Type I mallet finger injuries must be immobilized constantly for a minimum of:
1
4 weeks
2
5 weeks
3
6 weeks
4
7 weeks
5
8 weeks
Eight weeks of immobilization is preferred. If the finger is immobilized for a shorter period of time, the clock is reset and immobilization is started again.
QUESTION 6 OF 50
What is the most common complication after surgical management of chronic exertional compartment
syndrome (CECS) in the pediatric (≤18 years) population?
1
Recurrent CECS
2
Infection
3
Neurologic dysfunction
4
Hematoma or seroma formation
No detailed explanation provided for this question.
QUESTION 7 OF 50
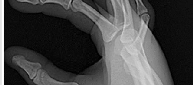
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5° of angulation. When the MCP joint is flexed 30°, a radially directed stress produces 45° of angulation. Radiographs are otherwise normal. Management should consist of
1
a thumb spica cast and reassessment in 3 weeks.
2
a thumb spica cast and reassessment in 6 weeks.
3
repair of the ulnar collateral ligament of the MCP joint.
4
adductor pollicis advancement on the proximal phalanx.
5
repair of the MCP joint dorsal capsule.
Injuries to the ulnar collateral ligament of the MCP joint of the thumb commonly occur in recreational skiers. Historically, this injury has been referred to as “gamekeeper’s thumb.” The ligament consists of the proper collateral ligament and the more volar accessory collateral ligament. In extension, the accessory ligament is taut, and in flexion, the proper ligament is taut. For a complete tear of the ligament complex to occur, there must be laxity in full extension. Incomplete tears respond well to thumb spica splinting or casting for 2 to 3 weeks and gradual resumption of range of motion. Prolonged immobilization of incomplete injuries leads to higher rates of MCP joint stiffness.
REFERENCES: Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint.
J Am Acad Orthop Surg 1997;5:224-229.
QUESTION 8 OF 50
Surgical release in Dupuytrenâs disease is indicated in which of the following:
1
A 15° metacarpophalangeal (MP) joint contracture and a 15° proximal interphalangeal (PIP) joint contracture
2
A 15° MP joint contracture and a 0° PIP joint contracture
3
Palpable spiral cord involving ring and small fingers
4
Palpable spiral cord involving ring and small fingers with multiple skin pits
5
Palpable spiral cord involving ring and small fingers in both of the hands
The indication for surgery in Dupuytrenâs disease is MP joint contracture larger than 30° and any degree of PIP joint deformity. The other answers are incorrect because they are subjective descriptions and do not necessarily indicate joint involvement.
QUESTION 9 OF 50
of 100
64
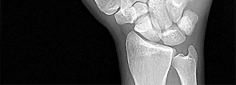
What is the optimal biomechanical screw placement position to treat a waist-level scaphoid fracture?
1
Dorsal one-third of the distal and proximal fragments
2
Dorsal half of the distal and proximal fragments
3
Central axis of the distal and proximal fragments
4
Volar half of the distal and proximal fragments
Dodds and associates looked at short (compared to long) scaphoid screws placed down the central axis in cadavers. A long screw placed along the central axis was significantly more stable when tested in all planes of motion about the wrist. McCallister and associates examined central placement and eccentric placement in a cadaver model. Central positioning produced 43% more stiffness and 113% more load (P < .01).
RECOMMENDED READINGS
1. [Bedi A, Jebson PJ, Hayden RJ, Jacobson JA, Martus JE. Internal fixation of acute, nondisplaced scaphoid waist fractures via a limited dorsal approach: an assessment of radiographic and functional outcomes. J Hand Surg Am. 2007 Mar;32(3):326-33. PubMed PMID: 17336838.](http://www.ncbi.nlm.nih.gov/pubmed/17336838)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17336838)
2. [Dodds SD, Panjabi MM, Slade JF 3rd. Screw fixation of scaphoid fractures: a biomechanical assessment of screw length and screw augmentation. J Hand Surg Am. 2006 Mar;31(3):405-13. PubMed PMID: 16516734. ](http://www.ncbi.nlm.nih.gov/pubmed/16516734)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16516734)
3. [McCallister WV, Knight J, Kaliappan R, Trumble TE. Central placement of the screw in simulated fractures of the scaphoid waist: a biomechanical study. J Bone Joint Surg Am.2003 Jan;85-A(1):72-7.PubMed: 12533575.](http://www.ncbi.nlm.nih.gov/pubmed/12533575)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12533575)
RESPONSES FOR QUESTIONS 72 THROUGH 75
The figures listed above depict the scenarios described below. Please match the appropriate scenarios and figures.
65
A B
C
D
E F
66
G H
QUESTION 10 OF 50
A 62-year-old woman has advanced osteoarthritis of the knee that has been refractory to nonsurgical treatment. She wishes to discuss total knee arthroplasty. She reports a lifelong history of intolerance to most jewelry and is concerned about having an allergic reaction to the metallic knee implant.Hypersensitivity to metal implants is usually classified as what type of Gell-Coombs reaction?
1
I (allergic)
2
II (cytotoxic, antibody-dependent)
3
III (immune complex)
4
IV (delayed type)
Most “metal allergy” is classified as type IV, or delayed-type hypersensitivity response, which is a cellmediated response. Types I, II, and III are not generally associated with metal hypersensitivity responses.Type I reactions are typically anaphylaxis. Type II reactions are antibody mediated, such as seen in Grave’s disease or hemolytic anemia. Type III reactions are immune complex diseases such as serum sickness or systemic lupus erythematosus.
QUESTION 11 OF 50
of 100
Figures 12a through 12c
1
T-type fracture
2
Anterior column fracture
3
Anterior wall fracture
4
Posterior wall fracture
5
Posterior column and posterior wall fracture
- Posterior column and posterior wall fracture_
QUESTION 12 OF 50
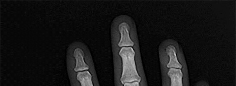
Figures 1 through 4 show the radiographs and MRI obtained from a 40-year-old man who has a 6-week history of ring finger pain, redness, and swelling after puncturing the finger with a toothpick. Purulent drainage from the puncture wound site grew _Eikenella corrodens_. The patient was initially treated with oral antibiotics for 10 days and then intravenous (IV) antibiotics for 3 weeks. What is the best next step in treatment? ---
---
---
---
1
Continued IV antibiotics for 4 weeks
2
Continued oral antibiotics for 6 weeks
3
Bone scan, biopsy, and metastatic work-up
4
Surgical débridement along with antibiotics
This patient has a septic distal interphalangeal joint, which was treated with antibiotics alone. As a result, the patient developed osteomyelitis with bone destruction and abscess. The best way to treat this problem is to perform surgical débridement of bone and soft tissue, along with abscess drainage and an appropriate antibiotic regimen. Antibiotic treatment without surgery would not be successful in eliminating this particular infection. Bone scan with biopsy is not the correct option, because this problem is an infection _and not a tumor, and MRI already has provided enough diagnostic information._
QUESTION 13 OF 50
In comparing the clinical efficacy of intra-articular sodium hyaluronate injections vs triamcinolone injections for the treatment of hallux rigidus, which factor showed significantly better improvement in the sodium hyaluronate group:
1
Gait pain
2
Pain at rest
3
Pain with passive mobilization
4
Use of analgesics
5
Pain with palpation
In a prospective randomized study comparing sodium hyaluronate vs cortisone injections for hallux rigidus, gait pain and AOFAS scores were significantly better in the sodium hyaluronate-treated group. There was no significant difference between the two treatment groups with regard to rest pain, pain with mobilization, pain with palpation, and use of analgesics.
QUESTION 14 OF 50
of 100
A 16-year-old high school football player has anterior shoulder pain after tackling an opponent with his arm in abduction and external rotation.
1
Isolated posterior instability with a posterior labral tear
2
Multidirectional instability
3
Anterior shoulder subluxation
4
Thoracic outlet syndrome
5
Superior labrum anterior to posterior (SLAP) tear
- Anterior shoulder subluxation_
QUESTION 15 OF 50
An 80-year-old female sustained a twist and fall earlier at her home. She currently complains of left hip pain. On physical examination, she has hip pain with motion and is tender to palpation over her greater trochanter. Her injury radiographs are shown in Figure A. Which of the following should be performed next in this patient's care?
1
Fixation with sliding hip screw
2
Fixation with cephalomedullary nail
3
Traction, internal rotation radiograph of the hip
4
Computed tomography of the proximal femur
5
Magnetic resonance imaging (MRI) of the proximal femur
This patient sustained a greater trochanteric (GT) fracture. Evaluation with MRI is the next best step in treatment to evaluate for intertrochanteric (IT) extension.
Isolated fractures of the GT are uncommon. They may be diagnosed on radiography, but the extent of this injury is difficult to ascertain based on radiography alone. MRI has found a role in defining the extent of the fracture line. Though isolated GT fractures are often treated conservatively when they occur in isolation, operative fixation is necessary if there is IT extension. If the extent of the injury is not identified, it may lead to delayed rehabilitation and decreased long-term survival rates.
Kim et al. performed a systematic review to determine what proportion of GT fractures had IT extension and what are the treatment options of GT with occult IT extension. Patients included had an isolated GT fracture on radiographs and underwent MRI scans to determine IT extension. In 99/110 patients (90%), MRI revealed IT extension and surgical fixation followed in 61 patients. They conclude that MRI should be performed in patients presenting with an isolated GT fracture on plain radiograph.
Lee et al. examined the pattern and extent of an injury shown by MRI and radionuclide bone scan (RBS) in patients whose radiographs revealed fractures
limited to the GT. 25 patients were found sustaining a low-energy injury. They found that 3 patients had ITC extension that was not visualized with radiographs or RBS. 8 patients had fractures with MRI evidence of complete extension across the ITC region and 12 had incomplete extension. 11/12 patients with incomplete extension had extension more than 50% to the medial cortex. They recommend that all patients presenting with an isolated GT fracture on the plain radiographs should undergo MRI examination.
Collin et al. performed a study to evaluate the efficacy of CT in diagnosing occult hip fractures compared to MRI. They evaluated 44 consecutive elderly patients with trauma to the hip. All patients had negative CT scans while MRI changed the diagnoses in 27 cases. They conclude that MRI is a more reliable modality for hip fracture diagnosis in comparison to CT and negative CT finding cannot rule out a hip fracture in patients with a clinical suspicion for a hip fracture.
Figure A is an AP pelvis radiograph demonstrating a fracture of the left greater trochanter. Illustration A is a radiograph demonstrating a GT fracture and Illustration B is a T1-weighted MRI of the same patient demonstrating IT extension.
Incorrect Answers:
Answers 1 and 2: Treatment should not be performed until more information with an MRI is obtained.
Answer 3: Traction, internal rotation views are obtained in displaced intertrochanteric fractures to visualize the fracture fragments more accurately and to assess the efficacy of a closed-reduction maneuver.
Answer 4: CT scan of the proximal femur is not the best study to rule out IT extension of this fracture.
QUESTION 16 OF 50
What is the most appropriate treatment for a 17-year-old boy who sustained a gunshot wound to his forearm from a handgun with a muzzle-velocity of 1000 feet/second if he is neurovascularly intact and radiographs reveal no fracture?
1
Irrigation and local wound care in the emergency department
2
Emergent irrigation and debridement in the operating room with vacuum-assisted wound closure
3
Emergent irrigation and debridement in the operating room with 7 days of intravenous antibiotics
4
Wound closure in the emergency department with follow-up wound check in 1 week
5
Exploration and removal of all bullet fragments in the emergency department and 10 day course of oral antibiotics
The question refers to appropriate management of a gunshot wound to the forearm. The first question that must be answered when evaluating gunshot injuries is whether the gunshot is low velocity or high velocity. Low-velocity wounds are less severe, are more common in the civilian population, and are typically attributed to bullets with muzzle velocities below 1,000 to 2,000 feet per second. Tissue damage is usually more substantial with higher-velocity (greater than 2,000 to 3,000 fps) military and hunting weapons. In this question, a muzzle velocity of 1,000 ft/sec is provided. Low velocity injuries with stable, non-operative fractures can be treated with local wound care.
The two referenced articles offer guidance for treating low-velocity gunshot injuries with stable, non-operative fracture patterns. The first article by Geissler et al is a retrospective study comparing 25 patients that prospectively received local irrigation and debridement, tetanus prophylaxis and a long acting cephalosporin intramuscularly to a random retrospective sample of 25 patients with similar ballistic-induced fractures and wounds managed by local debridement and 48h of intravenous antibiotics. One infection occurred in each group, requiring further therapy. It was concluded that patients with low-velocity gunshot induced fractures can be managed without the use of short-term intravenous antibiotics with no increased risk of infection.
In the second study, Dickey et al evaluated the efficacy of an outpatient management protocol for patients with a gunshot-induced fracture with a stable, non-operative configuration. 41 patients with a grade I or II open, nonoperative fracture secondary to a low-velocity bullet were treated with 1gm of cefazolin administered in the emergency room and a 7-day course of oral cephalexin. No patient developed a deep infection. Thus, local I&D, tetanus, and oral antibiotics for 2-3 days is adequate for low velocity gunshot wounds.
QUESTION 17 OF 50
of 100
A 69-year-old woman has rigid painful left pes planus that has become less symptomatic with casting. She has multiple comorbidities and is not a good surgical candidate. She has failed a trial of activity without any supports.
1
Observation
2
Arizona brace
3
Medial arch support
4
Casting
5
Hindfoot fusion
Treatment for pes planus revolves around 2 clinical parameters: pain and rigidity. In the absence of pain, no intervention is warranted because there are no other symptoms that can reasonably be linked to the foot shape. Flexible pes planus (that corrects with heel rise) is usually normal and does not cause symptoms, but it can be associated with a symptomatic accessory navicular, in which case the patient may have pain over the medial navicular from either traction by the tibialis posterior or the act of rubbing against the medial shoe counter. Rigid pes planus is most frequently associated with a tarsal coalition, which classically presents in late adolescence but can become symptomatic for the first time in adults. The initial treatment for painful pes planus, whether flexible or rigid, is immobilization, usually in a walking cast. This often is sufficient to relieve symptoms on a permanent basis. Surgery should be contemplated only when this treatment fails. Adult-acquired flatfoot is most commonly attributable to tibialis posterior tendon dysfunction. In stage 3, the pes planus is rigid. If it is painful, surgical treatment, which consists of a triple arthrodesis, may be considered. However, if medical constraints or patient preference preclude surgery, an Arizona brace can provide sufficient support to reduce symptoms to an acceptable level to perform activities of daily living.
RECOMMENDED READINGS
[Varner KE, Michelson JD. Tarsal coalition in adults. Foot Ankle Int. 2000 Aug;21(8):669-72. PubMed PMID: 10966365. ](http://www.ncbi.nlm.nih.gov/pubmed/10966365)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10966365)
[Lin JL, Balbas J, Richardson EG. Results of non-surgical treatment of stage II posterior tibial tendon dysfunction: a 7- to 10-year followup. Foot Ankle Int. 2008 Aug;29(8):781-6. doi: 10.3113/FAI.2008.0781. PubMed PMID: 18752775. ](http://www.ncbi.nlm.nih.gov/pubmed/18752775)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18752775)
[Chao W, Wapner KL, Lee TH, Adams J, Hecht PJ. Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int. 1996 Dec;17(12):736-41. PubMed PMID: 8973895. ](http://www.ncbi.nlm.nih.gov/pubmed/8973895)[View](http://www.ncbi.nlm.nih.gov/pubmed/8973895)[ ](http://www.ncbi.nlm.nih.gov/pubmed/8973895)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8973895)
Cha SM, Shin HD, Kim KC, Lee JK. Simple excision vs the Kidner procedure for type 2 accessory navicular associated with flatfoot in pediatric population. Foot Ankle Int. 2013 Feb;34(2):167-72. doi: 10.1177/1071100712467616. Epub 2013 Jan 15. PubMed PMID:
[23413054/. ](http://www.ncbi.nlm.nih.gov/pubmed/%2023413054)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2023413054)
[Sullivan JA. Pediatric flatfoot: evaluation and management. J Am Acad Orthop Surg. 1999 Jan;7(1):44-53. PubMed PMID: 9916191.](http://www.ncbi.nlm.nih.gov/pubmed/9916191)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9916191)
CLINICAL SITUATION FOR QUESTIONS 51 AND 52
Figure 51a demonstrates the sneaker wear pattern and Figures 51b and 51c are the weight-bearing radiographs of a 20-year-old National Collegiate Athletic Association Division I basketball player. Throughout his college career he has experienced pain in the lateral aspect of his right foot. He has been treated with a clamshell orthotic, but this preseason his pain is worse than ever. Upon examination he has tenderness to palpation over the fifth metatarsal and his peroneal strength is 5/5 bilaterally
A
B
C
QUESTION 18 OF 50
Which of the following structures is most commonly involved in lateral epicondylitis?
1
Anconeus
2
Extensor digitorum communis
3
Extensor carpi radialis longus
4
Extensor carpi radialis brevis
5
Extensor carpi ulnaris
The most common specific site of involvement is the origin of the extensor carpi radialis brevis. It is usually caused by overuse activities, such as the eccentric overload exhibited during a backhand in tennis. In most patients, the characteristic friable, grayish tissue described as angiofibroblastic hyperplasia or hyaline degeneration is seen at the extensor carpi radialis brevis origin.
REFERENCES: Nirschl RP: Elbow tendinosis/tennis elbow. Clin Sports Med 1992;11:851-870.
Regan W, Wold LE, Coonrad R, Morrey BF: Microscopic histopathology of chronic refractory lateral epicondylitis. Am J Sports Med 1992;20:746-749.
QUESTION 19 OF 50
When first seen in the emergency department, the patient with the injury seen in Figures 15a and 15b was not able to extend the wrist or the thumb. What is the best initial management?
1
Closed reduction and casting, with expected nerve injury recovery with time
2
Closed reduction and percutaneous pinning, with expected nerve injury recovery with time
3
Immediate open reduction with internal fixation and exploration of the radial nerve
4
Immediate open reduction with internal fixation and exploration of the median nerve
5
Immediate open reduction with internal fixation and exploration of the ulnar nerve
DISCUSSION: The injury is a type 3 supracondylar humerus firaacture with a radial nerve injury. Most nerve
injuries associated with fractures recover spontaneously within 6 to 12 weeks. Complete recovery is expected within 3 to 6 months. Closed reduction and percutaneous pinning is the recommended treatment for supracondylar fractures of the elbow. Cast treatment for displaced fractures carries a higher risk of associated compartment syndrome. There is no indication for exploring the radial nerve acutely. Open reduction is necessary only if the closed reduction fails.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 406-409.
Campbell CC, Water PM, Emans JB, et al: Neurovascular injury and displacement in type III
supracondylar humerus fractures. J Pediatr Orthop 1995;15:47-52.
**2010 Pediatric Orthopaedic Examination Answer Book • 19**
Figure 16
QUESTION 20 OF 50
A 10-year-old girl has a right elbow deformity that is the result of trauma 5 years ago. She has no pain despite the arm deformity. The radiographs in Figures 42a and 42b show complete healing. This radiographic appearance demonstrates what complication?
1
Growth arrest of the medial trochlear physis
2
Varus malunion of a supracondylar humeral fracture
3
Valgus malunion of a lateral condylar fracture
4
Posterior and lateral dislocation of the radial head
5
Osteonecrosis of the capitellum
Cubitus varus is a common complication of displaced supracondylar humeral fractures that are treated with closed reduction and cast immobilization. Treatment with closed reduction and percutaneous pinning decreases the incidence of this complication. Cubitus varus also can occur in minimally displaced fractures when unrecognized collapse of the medial column of the distal humerus is not corrected with manipulation. This can be detected on physical examination of the carrying angle or on radiographs measuring Baumann’s angle, both in comparison to the opposite side. Cubitus varus may result in unacceptable cosmesis and may predispose the patient to fractures of the lateral condyle. The lateral radiograph demonstrates the crescent sign from overlap of the distal humerus with the olecranon seen in patients with cubitus varus. Patients with growth arrest to the medial trochlear physis would have atrophy of the trochlea on radiographs.
REFERENCES: Flynn JM, Sarwark JF, Waters PM, et al: The surgical management of pediatric fractures of the upper extremity. Instr Course Lect 2003;52:635-45.
Papandrea R, Waters PM: Posttraumatic reconstruction of the elbow in the pediatric patient. Clin Orthop 2000;370:115-126.
Lins RE, Simovitch RW, Waters PM: Pediatric elbow trauma. Orthop Clin North Am 1999;30:119-132.
QUESTION 21 OF 50
-Decreased sun exposure leads to decreased bone health via what mechanism?
1
Impaired ability of the liver to hydroxylate cholecalciferol
2
Impaired ability of the kidneys to hydroxylate cholecalciferol
3
Impaired parathyroid hormone (PTH) production by the parathyroid glands
4
Impaired absorption of calcium by the gastrointestinal (GI) tract
No detailed explanation provided for this question.
QUESTION 22 OF 50
A 46-year-old male construction worker has right hip pain that has failed to respond to nonsurgical management. His body mass index (BMI) is 32, he is 6’2” tall, and he has no other medical comorbidities. AP and lateral radiographs of the right hip are shown in Figures 23a and 23b. The patient inquires about his suitability for metal-on-metal hip resurfacing. The patient should be educated that he is at higher risk for failure secondary to which of the following?
1
BMI >30
2
Presence of secondary changes of the acetabulum
3
Osteonecrosis of the femoral head
4
Age of younger than 55 years old
5
Male gender
This young patient has osteonecrosis of the femoral head with a large area of collapse.
The results of hip resurfacing arthroplasty have been reported to be best in young, male patients who are younger than 55 years of age with a diagnosis of osteoarthritis. Although some authors advocate metal- on-metal hip resurfacing as an option for patients with osteonecrosis of the femoral head, in this particular patient, given the size of the necrotic segment, he would be at higher risk for failure and a conventional total hip arthroplasty would be a more conservative option. As the acetabulum is resurfaced in metal- on-metal hip resurfacing, the secondary changes of the acetabulum are not an issue and his BMI is in an acceptable range for the procedure.
REFERENCES: Mont MA, Ragland PS, Etienne G, et al: Hip resurfacing arthroplasty. J Am Acad Orthop Surg 2006;14:454-463.
Revell MP, McBryde CW, Bhatnagar S, et al: Metal-on-metal hip resurfacing in osteonecrosis of the femoral head. J Bone Joint Surg Am 2006;88:98-103.
Buergi ML, Walter WL: Hip resurfacing arthroplasty: The Australian experience. J Arthroplasty 2007;22:61-65. Question 24
A 31-year-old woman had disabling right knee pain. An arthroscopic assessment reveals chondromalacia of both the lateral femoral condyle and tibial plateau. The standing femorotibial axis measures 10 degrees of valgus. The
optimum treatment of this condition should include
1. distal femoral varus osteotomy.
2. osteoarticular transplant to the lateral femoral condyle.
3. unicondylar arthroplasty.
4. high tibial osteotomy.
5. Fulkerson tibial tubercle transfer. PREFERRED RESPONSE: 1
DISCUSSION: The long-term outcome of a distal femoral varus osteotomy has been quite favorable and should remain the primary choice for this young active woman. Sharma and associates have shown that a 5-degree valgus malalignment has a five-fold chance of progressing at least one grade within 18 months, making a corrective osteotomy the most important surgical maneuver.
REFERENCES: Sharma L, Song J, Felson DT, et al: The role of knee alignment in disease progression and function decline in knee osteoarthritis. JAMA 2001 ;286:188-195.
Murray PB, Rand JA: Symptomatic valgus knee: The surgical options. J Am Acad Orthop Surg 1993; 1:19.
Figure 25a Figure 25b Figure 25c
QUESTION 23 OF 50
A 32-year-old ballet dancer sustains a distal radius fracture, and is subsequently closed reduced and casted. She presents 11 months later with the radiograph seen in Figure A, complaining of significant wrist pain. What is the appropriate surgical treatment at this time?
1
Distal radius corrective osteotomy
2
Total wrist arthrodesis
3
Proximal row carpectomy
4
Scaphoid excision and four corner fusion
5
Interposition arthroplasty
The lateral wrist radiograph in Figure A shows significant dorsal angulation of the distal radius with a maintained joint space. The most appropriate surgical treatment for this patient would include corrective osteotomy of the distal radius, as there is no evidence of degenerative changes. If degenerative changes would be present, a salvage procedure such as total wrist arthrodesis would become an option.
The referenced article by Fernandez recommended distal radius corrective osteotomy with bone grafting and internal fixation for the following indications:
1) manually active patients who had a symptomatic extra-articular malunion of the distal end of the radius causing angulation of more than 25 to 30 degrees in either the frontal or sagittal plane without significant degenerative changes in the wrist joint (such as narrowing of the joint space, intra-articular incongruency, subchondral sclerosis, and osteophytic reaction) and in whom it
was thought that the result of either a Darrach procedure or shortening osteotomy of the ulna would be uncertain because the deformity of the radius would not be corrected, and 2) patients who wished to have the deformity corrected even though they had adequate function of the wrist.
QUESTION 24 OF 50
Arthrogryposis multiplex congenita:
1
Primarily affects joints, and secondarily the muscles which move them.
2
Is more often neuropathic than myopathic.
3
Is typically asymmetrical.
4
Does not respond to passive joint mobilization.
5
Has a natural history of increasing joint range of motion with time
Arthrogryposis multiplex congenita is an idiopathic disorder that may be due to a primary deficiency of anterior horn cells. Arthrogryposis multiplex congenita results in lack of muscle development; the joint stiffness is secondary to this. It is usually reasonably symmetrical.
QUESTION 25 OF 50
of 100
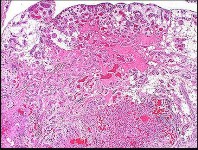
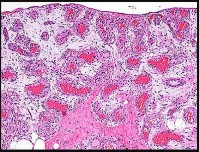
Figures 6a through 6d are the radiographs and T1-weighted sagittal and fat-saturated axial MR images of an otherwise healthy 56-year-old man who has anterior knee pain and intermittent swelling after sustaining a noncontact twisting injury. Low-power and high-power hematoxylin and eosin stained histologic specimens are shown in Figures 6e and 6f. Based on the history, radiographs, CT scan, MR imaging, and histologic findings, what is the most likely diagnosis?
1
Localized pigmented villonodular synovitis (PVNS)
2
Synovial hemangioma
3
Synovial chondromatosis
4
Biphasic synovial sarcoma
The lesion in the posterior intercondylar knee notch is a benign synovial hemangioma. Intralesional calcifications, classically associated with hemangiomas, are frequently not identified on plain radiographs. The MR imaging reveals a hypervascular lesion with multiple filling defects, with hyperintensity on T2-weighted images and low-to-intermediate signal intensity on T1-weighted images. Histologically, vascular lakes within fine capillaries with a synovium on the surface of the lesion are characteristic of this condition. Many patients with synovial hemangioma have pain, swelling, stiffness, or mechanical symptoms. The correlation of symptoms with the hemangioma for this patient is unclear because there was recent trauma and a concurrent meniscus tear. Simultaneous treatment of both potential sources of pain is typically recommended. As with PVNS, the disease can be localized or diffuse. Surgical excision, either open or arthroscopic, is the recommended treatment. PVNS is the most common intra-articular tumor, but hypointensity in either the diffuse or localized type is characteristic in both T1- and T2-weighted images. Synovial sarcoma, although often found close to a joint, is not characteristically found within a joint.
RECOMMENDED READINGS
6. [Lopez-Oliva CL, Wang EH, Cañal JP. Synovial haemangioma of the knee: an under recognised condition. Int Orthop. 2015 Oct;39(10):2037-40. Epub 2015 Jul 31. PMID: 26227920. ](http://www.ncbi.nlm.nih.gov/pubmed/26227920)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/26227920)[ ](http://www.ncbi.nlm.nih.gov/pubmed/26227920)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26227920)
7. [Adelani MA, Wupperman RM, Holt GE. Benign synovial disorders. J Am Acad Orthop Surg. 2008 May;16(5):268-75. Review. PubMed PMID: 18460687.](http://www.ncbi.nlm.nih.gov/pubmed/18460687)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18460687)
8. Weiss SW, Goldblum JR. Benign tumors and tumor-like lesions of blood vessels. In: Weiss SW, Goldblum JR, eds. _Soft Tissue Tumors_. 5th ed. Philadelphia, PA: Mosby Elsevier; 2008:664-665
QUESTION 26 OF 50
What nerve is most likely to develop a traumatic neuroma following open reducation and internal fixation of a talar neck fracture via a posterolateral approach?
1
Dorsal intermediate cutaneous
2
Sural
3
Saphenous
4
Medial plantar
5
Lateral plantar (Baxter)
The preferred approach is posterolateral, placing the sural nerve most at risk. The dorsal intermediate cutaneous nerve is anterolateral to the ankle, and the medial and lateral plantar branches are medial and inferior to the surgical site. The saphenous nerve is anteromedial and away from the surgical approach.
REFERENCES: Swanson TV, Bray TJ, Holmes GB Jr: Fractures of the talar neck: A mechanical study of fixation. J Bone Joint Surg Am 1992;74:544-551.
Lawrence S, Botte M: The sural nerve of the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
QUESTION 27 OF 50
A 8-year-old girl sustained a Gustilo-Anderson grade III open tibia fracture 1 week ago and underwent two debridements with definitive fracture fixation. She now has a soft-tissue defect that measures 7 cm
× 7 cm on the distal third leg that is a 3 centimeters proximal to the ankle. There is exposed bone on the medial aspect of her leg. A Negative pressure wound therapy (NPWT) device was applied to her leg. All of the following are benefits of the NPWT EXCEPT:
1
Decrease likelihood of complex secondary soft tissue reconstruction
2
Permits outpatient management of complex wound
3
Reduce edema to wound
4
Stimulation of granulation tissue
5
Decreases wound angiogenesis
Due to the limited soft tissue coverage of the medial aspect of the distal third of the tibia, full-thickness wound in this region often requires free-flap coverage. However, NWPT is typically applied first, as this has been shown to contribute to all of the above benefits with the exception of decreased wound angiogenesis.
NPWT has a number or purported beneits, including stimulation of angiogenesis, reduction of local edema, increased blood flow at the wound bed, and increased granulation tissue in the wound. These affects accelerate wound healing and may reduce the need for complex wound coverage. NPT has become increasingly popular as a temporizing measure for complex wound management and can enable outpatient treatment.
Caniano et al. reviewed 51 pediatric patients who underwent NPWT using the Vacuum Assisted Closure (VAC) device to aid in soft tissue closure. Nine of these patients had extremity wounds, for which a VAC was applied as a bridge to either a skin graft or a free flap. The VAC was applied intraoperatively, and patients then followed up as an outpatient with dressing changes performed three times weekly. The authors found that NPWT was safe, cost-effective to complex wound care, and permitted outpatien management.
Mooney et al. reviewed 27 patients with complex extremity wounds managed with NPWT. They found that all wounds, whether acute or with prior failed soft tissue procedure, eventually healed with NPWT and without additional complex coverage procedures. The authors noted that patients developed robust granulation tissue, even over exposed bone, tendon, joint, and hardware, which could then be covered with a split thickness graft or allowed to heal by
secondary intention. They concluded that NPWT may decrease need for complex microvascular tissue transfer.
Incorrect Answers:
Answer 1: NPWT decreases the likelihood of complex secondary soft tissue reconstruction.
Answer 2: NPWT often permits outpatient management of complex wounds. Answer 3: NPWT reduces edema to the wound bed.
Answer 4. NPWT stimulates of granulation tissue and prepares the wound for STSG or free flap.
QUESTION 28 OF 50
of 100
The patient is treated with emergent open reduction and internal fixation via a lateral approach to the distal femur. The peroneal nerve is found intact but is under pressure by a proximal bone fragment. After fixation, there is near-anatomic fracture reduction and no tension on the nerve. The patient is comfortable at a postsurgical check 4 hours later. Her toes
are warm and pink and there is no pain with passive dorsiflexion/plantar flexion of the toes. However, she continues to have absent first web space sensation, diminished dorsal foot sensation, and absent toe/ankle dorsiflexion. What is the best next step?
1
Return to surgery emergently for 4-compartment fasciotomy because she has a compartment syndrome and the nerve will not otherwise recover
2
Return to surgery urgently within the next few days for nerve exploration and potential microsurgical repair (vs cable grafting) to the damaged nerve to speed repair
3
Observe the nerve injury with further workup/intervention only if there is no sign of nerve recovery by 3 months after surgery
4
Observe the nerve injury with further workup/intervention only if there is no sign of nerve recovery by 12 months after surgery
- Observe the nerve injury with further workup/intervention only if there is no sign of nerve recovery by 3 months after surgery
QUESTION 29 OF 50
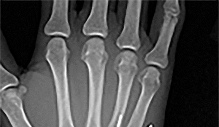
Figures 1 through 3 demonstrate the radiographs obtained from a 25-year-old man who injured his right,
by punching a wall 3 weeks earlier. He notes pain and deformity about the ulnar aspect of his hand. The best treatment option is
1
closed reduction and cast immobilization.
2
open reduction and internal fixation (ORIF).
3
arthrodesis.
4
resection arthroplasty.
The initial radiographs reveal a fourth and fifth carpometacarpal (CMC) joint fracture dislocation. The injury is associated with a shear fracture of the dorsal rim of the hamate. Further assessment with CT might be helpful in fully evaluating the extent of injury. Extensor carpi ulnaris is a deforming force at the base of the fifth metacarpal. This unstable fracture dislocation could be treated with closed reduction and pinning if the patient presented within a few days of injury. However, because he presented in a delayed fashion (3 weeks after injury), open reduction with internal fixation was required (Figures 4 and 5). In the series by Zhang and associates, patients with fourth and fifth CMC fracture dislocations presenting in a delayed fashion and treated nonsurgically had suboptimal results. Therefore, closed reduction and casting are not appropriate. An arthrodesis and resection arthroplasty are salvage procedures considered for a painful arthritic joint and would less likely should not be considered for this acute injury.
QUESTION 30 OF 50
of 100
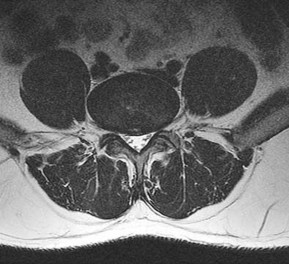
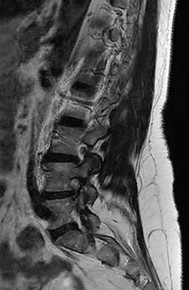
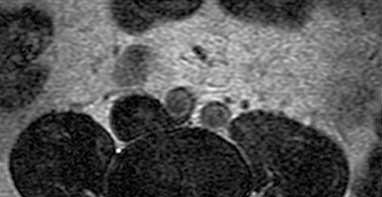
Figures 32a and 32b are the CT and MR image of a man who undergoes fusion for his degenerative spondylolisthesis. He wakes up with a foot drop. Which structure has most likely been injured?
1
S1 nerve root
2
Lumbosacral plexus
3
Peroneal division of the sciatic nerve
4
L5 nerve root
After exiting the L5-S1 neuroforamen, the L5 nerve root lies anterior to the sacral ala. There, if S1 pedicle screws are inadvertently directed laterally toward the ala rather than medially toward the sacral promontory, the L5 nerve root is endangered.
The iliac vein and artery lie more ventral than the L5 nerve root, which is draped closely to the sacral ala. The S1 nerve root exits inferior to the S1 sacral ala and is seen medial to the S1 pedicle on the MR axial image provided. On the CT scan the pedicle screw is aiming medial to lateral and is penetrating several millimeters outside the bone. Although an injury to the peroneal division of the sciatic nerve could result in a foot drop, this is not the most likely cause in this scenario and it lies more peripherally.
RECOMMENDED READINGS
7. [Mirkovic S, Abitbol JJ, Steinman J, Edwards CC, Schaffler M, Massie J, Garfin SR. Anatomic consideration for sacral screw placement. Spine (Phila Pa 1976). 1991 Jun;16(6 Suppl):S289-94. PubMed PMID: 1862427. ](http://www.ncbi.nlm.nih.gov/pubmed/1862427)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/1862427)
8. [Santos ER, Rosner MK, Perra JH, Polly DW Jr. Spinopelvic fixation in deformity: a review. Neurosurg Clin N Am. 2007 Apr;18(2):373-84. Review. PubMed PMID: 17556140. ](http://www.ncbi.nlm.nih.gov/pubmed/17556140)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17556140)
QUESTION 31 OF 50
Slide 1 Slide 2
A 9-year-old boy has a history of multiple fractures. He presents with left leg pain following a minor fall. His anteroposterior
(Slide 1) and lateral (Slide 2) plain radiographs are shown. The most likely genetiCdefect would be:
1
FGF receptor 3
2
Type I collagen
3
Cartilage oligomeriCmatrix protein
4
Fibrillin
5
Type II collagen
The anteroposterior and lateral radiographs show thinned cortices and a gentle S-shaped curve of the tibia. The overall alignment of the tibia, as well as the physes, is normal. These are the radiographiCfeatures of osteogenesis imperfecta.
In osteogenesis imperfecta, the genetiCdefect involves type I collagen. Type I collagen is made up of two alpha-1 chains and one alpha-2 chain in a triple helix. Glycine is the smallest amino acid and is crucial for coiling of the triple helix. Mutations in the
glycine chain lead to severe forms of osteogenesis imperfecta. One should also remember the Silence classification:
Type Inheritance Sclera Severity
I AD Blue Mild form, normal teeth
II AR Blue Lethal form, die early
III AR Normal Severe, progressively deforming
IV AD Normal Moderately severe
Biphosphonate therapy can be used to slow bone remodeling and increase bone mass. With regard to the incorrect choices:
FGF receptor 3 is associated with achondroplasia. Fibrillin is associated with Marfan's syndrome.
Type II collagen is associated with spondyloepiphyseal dsyplasia.
Cartilage oligomeriCmatrix protein is associated with pseudoachondroplasia. Correct Answer: Type I collagen
QUESTION 32 OF 50
A 35-year-old construction worker has developed isolated lateral compartment arthritis. He has lost 50 pounds, now has a body mass index of 30, and still has pain that limits his activities of daily living and work despite receiving a 4-month course of nonsteroidal anti-inflammatory medications and 2 intra-articular cortisone injections. His range of motion is 5° to 110°, and his mechanical axis is 18° of valgus. What is the most appropriate surgical treatment for this patient?
1
Proximal tibial varus osteotomy
2
Lateral unicompartmental arthroplasty
3
Distal femoral varus osteotomy
4
Total knee arthroplasty
60
Knee arthritis in a young laborer is challenging to address. A surgeon could perform an arthroplasty, but there is concern for early failure and the subsequent need for multiple revisions during this patient’s lifespan. Indications for distal femoral varus osteotomy include at least a 12- to 15- degree valgus mechanical axis and range of motion of at least 15° to 90°. Contraindications for this procedure include inflammatory arthritis and restricted knee motion.
QUESTION 33 OF 50
Which of the following procedures is most likely to correct idiopathic toe walking with a single treatment:
1
Stretching program
2
Ankle foot orthosis
3
Stretching cast
4
Botulinum toxin injection
5
Percutaneous tendoachilles lengthening
Percutaneous tendoachilles lengthening is most likely to resolve idiopathic toe walking in a single treatment. The other methods have a higher likelihood of persistent toe walking.
QUESTION 34 OF 50
According to Musculoskeletal Infection Society (MSIS) guidelines, which set of patient laboratory study
results fits the definition of chronic prosthetic joint infection?
1
Erythrocyte sedimentation rate (ESR) 50 mm/hr, C-reactive protein (CRP) 8 mg/L, joint aspiration white blood cell (WBC) count 542, 62% neutrophils, and positive leukocyte esterase
The MSIS definition of periprosthetic joint infection was updated in 2014 with two major and six minor criteria. The presence of one major criterion or three minor criteria is diagnostic for infection. The major criteria are two positive cultures with the same organism or a draining sinus tract. The current MSIS minor criteria are 1) an elevated ESR (more than 30 mm/hr) and CRP level (more than 10 mg/L), 2) an elevated synovial WBC count (more than 3,000 cells per/microliter), 3) an elevated synovial fluid polymorphonuclear count (more than 80%), 4) a positive histological analysis of periprosthetic tissue, and 5) a single positive culture.
QUESTION 35 OF 50
Slide 1
A 53-year-old woman presents for treatment of painful toe and metatarsal deformities (Slide). She underwent surgery to the hallux 2 years ago for correction of arthritis of the hallux metatarsophalangeal joint. Pain in the joint persists. She has no systemic disease, and the opposite foot is normal. What is the ideal surgical correction for her forefoot:
1
C apsulotomy of the lesser toe metatarsophalangeal joints and extensor tendon lengthening with temporary K-wire fixation
2
Resection of the lesser metatarsal heads
3
Arthrodesis of the hallux metatarsophalangeal joint with interposition bone block graft
4
Shortening osteotomies of the lesser toe metatarsals and arthrodesis of the hallux metatarsophalangeal joint
5
Revision resection arthroplasty of the hallux and resection of the lesser metatarsal heads
Resection of the lesser metatarsal heads is an operation that is commonly performed for patients with rheumatoid arthritis; however, this may also be performed for patients with debilitating metatarsalgia in the absence of systemic disease. C apsulotomy and tendon lengthening will not correct the alignment of the lesser toes or address the metatarsalgia. Revision of the resection arthroplasty will not address the metatarsalgia, and recurrent deformity of the hallux is likely. Shortening osteotomies of the metatarsal will decompress the joint, realign the toes, and decrease the metatarsalgia, particularly if performed in conjunction
with metatarsophalangeal arthrodesis. A lengthening bone block fusion is not necessary.
QUESTION 36 OF 50
A 13-year-old football running back is tackled during a game. On impact with the ground, his chest is compressed between the opposing player and the turf. He experiences immediate pain, difficulty breathing, and on physical examination is tender to palpation over the sternoclavicular joint. What is the best next step?
1
Administer bronchodialator
2
Repeat examination in 15 minutes
3
Referral for radiograph with attempted closed reduction
4
Start advanced trauma life support (ATLS) protocol
78
The sternoclavicular joint has a low rate of injury. Usually, it is associated with motor vehicle collision or contact sports. Traumatic sternoclavicular joint injuries are classified from grade I to grade III in ascending severity. Posterior dislocation can be life-threatening, and ATLS protocol and rapid transport to the emergency department is recommended. This injury can be diagnosed by listening for upper airway obstruction or a noticeable change in voice quality as posterior dislocation of the clavicular head obstructs airflow.
QUESTION 37 OF 50
A 71-year-old woman with coronary artery disease underwent an uncomplicated right total hip arthroplasty for osteoarthritis 12 years ago. Her hip has functioned well until approximately 18 months ago when she noted the spontaneous onset of groin, buttock, and proximal thigh pain that is present at rest and made worse with activity. A radiograph is shown in Figure 15. What is the recommended management at this point?
1
Immediate admission to the hospital and emergent revision hip arthroplasty
2
Reassurance and follow-up if symptoms worsen
3
Repeat radiographs in 1 month
4
Protected weight bearing with urgent revision hip arthroplasty when the patient is medically cleared
5
A prescription for alendronate and reevaluation in 1 year
DISCUSSION: The radiograph shows significant osteolysis with loosening of the femoral component. The patient is symptomatic and surgery is indicated because of the extent of osteolysis and the loose femoral component.
Reassurance and follow-up if symptoms worsen places the patient at risk for further bone loss and periprosthetic fracture. Emergent surgery is not required because the symptoms have been present for more than a year; however, urgent revision hip arthroplasty is recommended when the patient is medically cleared. While there is data to suggest that bisphosphonates may slow the progression of osteolysis in animal modes, there is no clear evidence that bisphosphonate treatment prevents the progression of osteolysis in humans. Additionally, this patient has a loose symptomatic femoral component.
REFERENCES: Chiang PP, Burke DW, Freiberg AA, et al: Osteolysis of the pelvis: Evaluation and treatment. Clin Orthop Relat Res 2003;417:164-174.
Dunbar MJ, Blackley HR, Bourne RB: Osteolysis of the femur: Principles of management. Instr Course Lect 2001;50:197-209.
Rubash HE, Dorr LD, Jacobs JJ, et al: Does alendronate inhibit the progression of periprosthetic osteolysis? Trans
Orthop Res Soc 2004;29:1888.
)
Figure 16a Figure 16b
QUESTION 38 OF 50
Syndromes that may be associated with macrodactyly include:
1
Proteus syndrome
2
Freeman-Sheldon syndrome
3
Madelungâs deformity
4
Holt-Oram syndrome
5
Poland syndrome
Some surgeons believe that macrodactyly is a variant of neurofibromatosis. Although macrodactyly is not an inherited anomaly, there are syndromes that may be associated with enlarged digits such as Proteus syndrome. Theoretical causes for macrodactyly include a neural cause, a vascular cause, as well as a humoral mechanism. The most accepted theory is that abnormal nerves exert some influence on the local tissues to stimulate growth.
QUESTION 39 OF 50
Initial enthusiasm of cemented femoral stems in total hip arthroplasty was tempered by:
1
Stem fracture
2
Poor survivorship in patients younger than 50 years of age
3
Recurrent dislocation
4
Infection
5
Fracture
Early outcomes were characterized by poor survivorship in the young population, a situation that corrected with subsequent polyethylene improvements and cement techniques.
QUESTION 40 OF 50
An 18-month-old boy is brought to your office for a clawing deformity of his right hand. The parents inform you that he was born full term after a difficult delivery complicated by shoulder dystocia. The boy weighed 9½ lbs at birth. The child had a brief episode of apnea with an APGAR score of 5 at birth and needed resuscitation and admission to the natal intensive care unit. Parents recall having noted a bump on his right clavicle, which was tender and was diagnosed as clavicle fracture. They also noticed a week later that the child did not flex the fingers of his right hand. The neonatologist had informed them that the
fracture is managed conservatively and the absence of finger flexion is due to the fracture and shall recover. They were warned that the recovery can be prolonged and can take up to 2 years. The boy has grown well and has achieved his milestones on time. His immunization is complete for his age.
You find a healthy, playful boy who tends to use his left hand to reach for objects. His right hand has extension at all the metacarpophalangeal (MC P) joints of the fingers while his proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints are flexed. His thumb is an adducted position and it is difficult to passively bring it to full abduction. There is obvious wasting of the hand and forearm. The child is able to move the arm well with no abnormalities noticed at the shoulder, elbow, and the wrist. The x-ray of his chest shows a healed clavicle fracture with no evidence of diaphragmatic paralysis. There is no evidence of Horner Syndrome and the grasp reflex is absent.
The diagnosis of this boyâs condition is:
1
Erbâs palsy
2
Klumpkeâs palsy
3
C erebrovascular accident
4
Ulnar and median combined nerve injury
This is a case of obstetric brachial plexus injury involving the C 8, T1 roots (Klumpke Palsy). Erbâs palsy involves upper roots only. C ombined nerve injuries can present in a similar fashion; however, low ulnar and median nerve lesions will not have weakness of flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS).
History of large baby, shoulder dystocia and clavicle fracture point to a difficult labor. The most common type of brachial plexus injury related to birth is Erbâs palsy, which is usually associated with a breech presentation. Isolated Klumpkeâs palsy is rare, and involvement of C 8, T1 usually occurs as part of global plexus injury.
QUESTION 41 OF 50
Parathyroid hormone stimulates which of the following cells to secrete neutral protease that degrades the osteoid bone surface:
1
Osteoblasts
2
Mast cells
3
Osteoclasts
4
Osteocytes
5
Osteoclast precursor cells
Osteoblasts have receptors for parathyroid hormone. Osteoblasts have neutral proteases that begin the degradation of the osteoid matrix. Once stimulated, the cells release interleukin-6 (IL-6). IL-6 signals osteoclasts to resorb bone. The osteoblasts secrete neutral proteases that degrade the osteoid surface. Osteoclasts then attach to the bone surface and secrete acid proteases that degrade the bone matrix. Parathyroid hormone related protein increases osteoblast expression of receptor activator of nuclear factor âkB ligand (RANKL). RANKL binds to osteoclast precursor cells for the formation of active osteoclasts
QUESTION 42 OF 50
Figure 68 shows the view from a posterosuperior shoulder arthroscopic portal. The muscle associated with the tendinous structure shown is innervated by what nerve? ](http://www.orthobullets.com/anatomy/10017/biceps-brachii)
1
Axillary
2
Median
3
Musculocutaneous
4
Radial
5
Ulnar
No detailed explanation provided for this question.
QUESTION 43 OF 50
A 28-year-old man has decreased finger proximal interphalangeal (PIP) joint range of motion after open reduction and internal fixation of a proximal phalanx fracture with the use of a side plate. Examination shows greater passive PIP joint flexion with metacarpophalangeal (MP) joint extension, than when the MP joint is flexed. This finding demonstrates contracture/scarring of which of the following structures? ](http://www.orthobullets.com/anatomy/10120/medbullets-onboarding--draft-html)
1
Flexor tendons
2
Extensor tendon
3
Oblique retinacular ligament
4
Intrinsic muscles
5
PIP joint
No detailed explanation provided for this question.
QUESTION 44 OF 50
Slide 1
For 3 years, a 23-year-old female gymnast has experienced recurrent ankle sprains associated with a sense of instability of the hindfoot. Upon examination, a positive anterior drawer test is present and stress radiographs are taken. She has attempted rehabilitation numerous times. She is unable to compete with her current symptoms. The recommended treatment is:
1
Reconstruction of subtalar instability with the peroneus brevis tendon
2
Reconstruction of ankle instability with an anatomic repair (Brostrom procedure)
3
Reconstruction of ankle instability with the split peroneus brevis (Evans procedure)
4
Reconstruction of ankle instability with the split peroneus brevis (C hrisman-Snook procedure)
5
Arthroscopic evaluation of ankle joint followed by reconstruction with split peroneus brevis tendon
For athletes, particularly those involved in activities that require repetitive proprioceptive and balance activities of the foot and ankle, an anatomic repair (Brostrom procedure) with addition of the extensor retinaculum (Gould modification) is the only procedure that will allow this individual to return to athletic activity. Surgeons must not sacrifice the peroneal tendon, or part thereof, since this may unnecessarily weaken the foot.
QUESTION 45 OF 50
A 45-year-old right-hand dominant woman falls onto an outstretched left hand. Imaging shows a complex elbow dislocation. The postreduction CT scan demonstrates a reduced joint, comminuted radial head fracture, and type I coronoid fracture. Surgical intervention is recommended to address the involved structures. Which component of the intervention adds the most rotational stability?
1
ixation of the coronoid fragment
2
Radial head arthroplasty
3
Repair or reconstruction of the lateral collateral ligament (LCL) complex
4
Repair or reconstruction of the medial collateral ligament (MCL)
This represents a terrible triad injury, with elbow dislocation, radial head fracture, and coronoid fracture. The LCL complex is typically disrupted in this injury pattern. Repair or reconstruction of this structure provides the greatest increase in rotational stability of the elbow.
QUESTION 46 OF 50
A 25 year-old-male sustains a closed injury shown in Figure A. If a tibial intramedullary nail is placed with the starting points shown (arrows), what subsequent alignment will occur?
1
Neutral
2
Varus, apex anterior
3
Varus, apex posterior
4
Valgus, apex anterior
5
Valgus, apex posterior
In proximal third tibial shaft fractures, due to the deforming forces of the pes anserine and the extensor mechanism, utilizing standard starting points during intramedullary nailing (IMN) will result in a valgus and apex anterior deformity.
There are several tips and tricks to avoid subsequent deformity following tibial IMN of a proximal third fracture. One way to avoid deformity is to use a more lateral starting point than normal to ensure nail placement in the true center of the canal, which is more lateral when compared to the tibial plateau.
Walker et al. studied 12 cadaveric tibias and inserted a Kirschner wire depending on rotated views of the knee. In order obtain a perfect starting point, a perfect anteroposterior as well as lateral of the knee must be obtained; otherwise, the authors noted that malrotation is bound to occur. With a perfect view, a more lateral starting point correlated with the center of the tibial canal.
McConnell et al. studied cadaveric and subsequent radiographic correlation on a lateral knee x-ray to determine the ideal 'safe zone' for the starting point of a tibial nail. This safe zone is more lateral and posterior, when looking at the axial cut of the plateau.
Figure A exhibits a proximal third tibia fracture with starting points that are not lateral enough, and too distal (on the lateral view), which will result in apex anterior and valgus deformity.
Incorrect answers:
Answer 1 (neutral alignment) will occur if a more lateral and more proximal start point is used.
Answers 2,3, and 5 are deformities that will typically be seen following tibial IMN if desired start points are utilized.
QUESTION 47 OF 50
A 70-year-old woman who underwent total knee replacement 18 months ago has had 3 weeks of moderate
drainage from a previously healed wound. What is the most appropriate treatment?
1
Vacuum-assisted wound closure dressing
2
Intravenous antibiotics for 6 weeks, followed by long-term oral antibiotic administration
3
Irrigation and debridement, followed by polyethylene exchange
4
Two-stage debridement and reconstruction
This situation represents a definitively and chronically infected knee replacement. Antibiotic therapy alone might suppress the infection but would not eradicate it. Debridement and polyethylene exchange would be appropriate treatment for an early postoperative infection. The treatment of choice is to perform a two-stage debridement and reconstruction. Although not among the listed choices, an aspiration or culture could be done presurgically and might help clinicians identify the best antibiotics to treat the condition. Antibiotic selection would not affect the need for the two-stage reconstruction, however.
QUESTION 48 OF 50
- are the radiographs of a 27-year-old man involved in a motorcycle crash who sustained a right proximal humerus fracture. Which of the following is most associated with osteonecrosis?
1
Intact medial hinge
2
Metaphyseal head extension of fracture of less than 8 mm
3
Tobacco use
4
Age
5
Angular displacement of the head of 30 degrees
No detailed explanation provided for this question.
QUESTION 49 OF 50
Figure 1
A 21-year-old man presents for evaluation of high arches, which have been present his entire life. C urrently, he is experiencing some discomfort with running activities. His brother and mother have high arches. He does not recall any trauma as a child, or any other pertinent childhood musculoskeletal problems. C linical examination reveals a rigid deformity bilaterally. The most common cause for his high arches is:
1
Spina bifida
2
Idiopathic cavovarus
3
Hereditary sensorimotor neuropathy
4
Polio
5
Peroneal spastic foot
The most common cause of familial cavovarus foot deformity is hereditary sensorimotor neuropathy (C harcot-Marie-Tooth disease). This is an autosomal dominant condition with variable penetrance. Idiopathic cavus foot is common, but not familial, nor is it associated with this extensive deformity.
QUESTION 50 OF 50
A 12-year-old boy comes to your office 2 weeks after a distal radius physeal fracture, which has been splinted in the emergency department. The epiphysis is displaced dorsally by 50%, and the articular surface has a dorsal tilt of 17°. You recommend:
1
C losed manipulation with sedation
2
C losed manipulation under anesthesia with relaxation
3
Open reduction, internal fixation
4
C ast application and observation
5
Percutaneous pin fixation in current position
Distal radial physeal fractures are common injuries. Reduction should be done gently and not repeated multiple times. Fractures presenting late like this one are difficult to manipulate atraumatically, but have good remodeling potential. Therefore, a cast should be applied to limit any further displacement, but no manipulation or operation is recommended.