This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set 6766AD)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
A 25-year old right-hand dominant professional baseball pitcher complains of posteromedial right elbow pain that is worsened by throwing. He also reports occasional paresthesias in his small and ring finger after lengthy bullpen sessions. On examination, he is tender along the medial olecranon and complains of pain when extending the elbow >/- 20° of extension. He has negative valgus stress, moving valgus stress, and milking maneuver tests. He is stable to varus stress, chair rise, and lateral pivot shift tests. Radiographs reveal a small osteophyte along the posteromedial border of the olecranon. What is the most likely diagnosis?
1
Valgus extension overload
2
Varus posteromedial rotatory instability (VPMRI)
3
Valgus posterolateral rotatory instability (VPLRI)
4
Olecranon bursitis
The patient has valgus extension overload. This is a spectrum of pathologies, often seen in pitchers, that begins with posteromedial impingement between the medial olecranon and posterior trochlea during forceful elbow extension. As a result, a medial olecranon osteophyte is typically the first notable imaging finding. As pathology increases, there can be progressive damage to the medial collateral ligament (MCL), degeneration of the radiocapitellar articulation, and neuritis of the ulnar nerve. VPMRI is often associated with a large anteromedial coronoid fracture and posterior band MCL rupture. VPLRI occurs when the lateral collateral ligament complex is ruptured. Olecranon bursitis presents with focal swelling or a fluid collection over the posterior aspect of the olecranon.
QUESTION 2 OF 50
Morphogenic factors such as bone morphogenetic protein-2, bone morphogenetic protein-7, and transforming growth factor-beta have been postulated to play a role in reversing the process of intervertebral disk degeneration. These molecules work via what mechanism?
1
Increase cell proliferation leading to increased cell numbers within the disk and enhanced matrix synthesis
2
Inhibit the catabolic effects of matrix metalloproteinases
3
Increase the chondrogenic phenotype of disk cells and increase matrix synthesis
4
Promote increased end plate vascularity and nutritional diffusion within the disk
5
Block receptors for tumor necrosis factor-alpha and interleukin-1
Bone morphogenetic protein-2, bone morphogenetic protein-7, and transforming growth factor-beta are morphogens that have been shown to alter the phenotype of target cells without increasing cellular proliferation. Within the intervertebral disk, these factors have the potential to increase the chondrogenic phenotype among disk cells, and this results in the increased production of disk matrix.Mitogenic molecules, such as insulin-like growth factor-1 and fibroblast growth factor, function to increase cellular proliferation.
QUESTION 3 OF 50
Which combination of muscle weakness is typically associated with hereditary sensory motor neuropathy:
1
Anterior tibial, extensor hallucis longus
2
Peroneus longus, extensor hallucis brevis
3
Gastrocnemius, peroneus brevis
4
Posterior tibial, extensor digitorum brevis
5
Anterior tibial, peroneus brevis
The peroneus brevis is usually the first muscle to atrophy. Varying patterns of loss of the other muscles of the lower extremity include the anterior tibial and, in particular, the intrinsic foot muscles. Weakness in these muscles accounts for the cavus and the claw foot deformities noted in patients with hereditary sensory motor neuropathy.
QUESTION 4 OF 50
Figure 38a shows the cross-sectional anatomy of the proximal thigh. What structure is indicated by the arrow? ](http://www.orthobullets.com/anatomy/10065/adductor-longus)
1
Adductor magnus
2
Adductor longus
3
Adductor brevis
4
Sartorius
5
Gracilis
No detailed explanation provided for this question.
QUESTION 5 OF 50
A 56-year-old woman with rheumatoid arthritis who underwent total hip arthroplasty 17 years ago now reports pain and progressive shortening of the extremity over the past year. An AP radiograph of the hip is shown in Figure 72. Laboratory studies show an erythrocyte sedimentation rate (ESR) of 34 mm/h (normal 0 to 28 mm/h) and a
1
reactive protein of 10.2 (normal 0.2-8.0). She is presently taking oral antibiotics for a urinary tract infection. What is the next most appropriate step in management?
2
Aspiration of the hip joint and if negative, revision of the acetabular component
3
Aspiration of the hip joint and culture once she has discontinued the antibiotics for 3 weeks
4
Triple phase bone scan
5
Indium-111 leukocyte scan
DISCUSSION: The patient has a loose acetabular component, which explains her pain and progressive shortening. She has a history of inflammatory arthritis, elevated ESR and C-reactive protein, and has recently been treated for an infection. Thus, the suspicion for infection is high and must be ruled out. A triple phase bone scan can assist in the identification of component loosening but cannot differentiate infection from noninfectious causes. Indium-111 scans have been shown to have limited utility, although a negative scan can be helpful in ruling out infection. The selective preoperative use of aspiration of the hip joint has been shown to be effective and is most likely to identify infection; however, the patient must be off of antibiotics for a minimum of 2 weeks prior to her aspiration to avoid a false negative culture.
REFERENCES: Della Valle CJ, Zuckerman JD, Di Cesare PE: Periprosthetic sepsis. Clin Orthop Relat Res 2004;420:26-31.
Lachiewicz PF, Rogers GD, Thomason HC: Aspiration of the hip joint before revision total hip arthroplasty:
Clinical and laboratory factors influencing attainment of a positive culture. J Bone Joint Surg Am 1996;78:749-754. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
Figure 73
QUESTION 6 OF 50
A 17-year-old high school soccer player sustains an anterior cruciate ligament (ACL) tear at the beginning of the season. An MRI scan confirms a complete ACL tear with no meniscal injuries. The patient plans an early return to play and would like to avoid surgery. Therefore, the patient and family should be advised that nonsurgical management consisting of rehabilitative exercises and the use of a functional knee brace will most likely result in
1
recurrent buckling with a probable meniscal tear.
2
limitation of motion with a delay in recovery.
3
a full return to activity with no limitations.
4
an improvement in overall performance.
5
an uneventful completion of the soccer season.
While there are athletes who can function at a full level with an ACL tear, they are in the minority. As yet, there is no reliable way to predict the patients who will be able to compensate for the loss of the ACL. Studies have confirmed the risk of recurrent instability and meniscal injury in athletes with an ACL-deficient knee who participate in cutting sports. One study showed that only 12 of 43 patients who attempted rehabilitation and bracing were able to return successfully for the season. Another study showed that 17 of 31 athletes who were able to return to their sport sustained 23 meniscal tears because of recurrent instability.
REFERENCES: Shelton WR, Barrett GR, Dukes A: Early season anterior cruciate ligament tears: A treatment dilemma. Am J Sports Med 1997;25:656-658.
Snyder-Mackler L, Fitzgerald GK, Bartolozzi AR III, Ciccotti MG: The relationship between passive joint laxity and functional outcome after anterior cruciate ligament injury. Am J Sports Med 1997;25:191-195.
QUESTION 7 OF 50
The deltoid inserts on this surface of the clavicle:
1
Superior surface
2
Anterior surface
3
Inferior surface
4
All of the above
The origin of the deltoid on the clavicle is J-shaped and extends from the midline on the superior aspect of the clavicle around the front of the clavicle to the inferior portion of the anterior aspect of the clavicle. Full-thickness fascial flaps must be obtained when the deltoid is released from the clavicle.
QUESTION 8 OF 50
Early postoperative infections following primary total hip arthroplasty are most likely caused by which
organism?
1
Staphylococcus epidermidis
2
Streptococcus viridans
3
Propionibacterium acnes
4
Staphylococcus aureus
S aureus is the most common organism cultured in early (fewer than 4 weeks postoperative) periprosthetic infections. Methicillin-resistant S aureus is becoming a more common pathogen in certain patient populations. B hemolytic Streptococcus and some gram-negative infections can also be found in early postoperative infections. S epidermidis, S viridans, and P acnes are more commonly found in late (more
than 4 weeks postoperative) infections.
QUESTION 9 OF 50
Myositis ossificans is a recognized complication of contusion to the quadriceps muscle. During early rehabilitation, this condition is most likely to be exacerbated by
1
electrical stimulation.
2
iontophoresis.
3
isometric exercise.
4
ice/heat contrast.
5
passive stretching.
Passive stretching is contraindicated during rehabilitation as it may potentiate the severity of the myositis ossificans. Electrical stimulation, iontophoresis, isometric exercise, and ice/heat contrast are not known to exacerbate this process.
REFERENCES: Brunet ME, Hontas RB: The thigh, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Cushner FD, Morwessel RM: Myositis ossificans traumatica. Orthop Rev 1992;21:1319-1326.
QUESTION 10 OF 50
Video 1 depicts a 20-year-old right-hand-dominant man with a 6-month history of left wrist pain and popping that has failed nonsurgical measures. No other positive findings upon examination are noted.
What is the most appropriate course of treatment?
Upon examination, this patient is exhibiting dislocation of the ECU tendon because of a disrupted sheath. He has failed nonsurgical measures, so surgery that would involve either direct repair or reconstruction of the tendon sheath is indicated. An option for reconstruction is to use a portion of the extensor retinaculum as a sheath substitute. Deepening of the ECU tendon groove at the distal ulna with direct repair of the sheath is another option, although a 2016 paper by Ghatan and associates did not find depth of the groove as a risk factor for subluxation. TFCC repair, lunotriquetral fusion, and DRUJ tenodesis are not appropriate because the examination clearly shows ECU tendon dislocation. TFCC and lunotriquetral ligament tears can occur along with ECU tendon dislocation, but no other examination findings suggest these conditions for this patient.
QUESTION 11 OF 50
A 45-year-old woman who recently underwent biopsy of a lymph node in the right posterior cervical triangle now finds it difficult to hold objects overhead and has diffuse aching in the right shoulder region. What is the most likely diagnosis?
1
Rotator cuff tear
2
Rhomboid paralysis
3
Deltoid paralysis
4
Triceps paralysis
5
Trapezius paralysis
The trapezius is innervated by the spinal accessory nerve. The nerve is superficial in the area of the posterior cervical triangle and is prone to injury during dissection. Paralysis of the trapezius causes loss of scapular stability when forward flexion or abduction of the shoulder is attempted.
REFERENCES: Vastamaki M, Solonen KA: Accessory nerve injury. Acta Orthop Scand 1984;55:296-299.
Leffert RD: Neurological Problems, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 759-760.
QUESTION 12 OF 50
of 100
A 15-year-old girl has had 4 months of right hip and groin pain. Upon examination, she has 25° of internal rotation with the hip flexed, which causes pain on the right side. Her left side shows 20° of internal rotation but no significant pain. Plain radiographs show that the patient has no dysplasia and an alpha angle of 68° on the right side and 70° on the left side. She has not undergone any formal treatment to date. What is the best course of initial management?
1
Right hip arthroscopic femoroacetabular impingement (FAI) surgery
2
Bilateral FAI surgery
3
Delayed gadolinium-enhanced MRI of cartilage (dGEMRIC), MRI of bilateral hips
4
Trial of physical therapy
■ Recent studies have shown success in conservative management for adolescent patients with femoroacetabular impingement syndrome. In a patient who has had symptoms for 4 months with no trial of physical therapy, this is the best step. In addition, even though the radiographic and range-of-motion parameters are more profound in the nonpainful hip, multiple authors have documented the presence of FAI morphology in asymptomatic patients, and the role of prophylactic surgery has not been elucidated. In addition, there are recent concerns about retained gadolinium, and its promise in imaging is starting to decline in elective type procedures.
QUESTION 13 OF 50
A 68-year-old right-hand dominant woman has experienced progressive right elbow pain and loss of motion for several years. She has failed nonsurgical treatment and elects to undergo a total elbow arthroplasty (TEA). In comparison to a linked prosthesis, an unlinked prosthesis has which reported distinction with extended follow-up?
1
Improved longevity in comparison to the linked prosthesis
2
A significantly larger flexion-extension arc
3
A higher incidence of postsurgical instability
4
Lower frequency of ulnar nerve dysfunction
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants. 36
QUESTION 14 OF 50
Anterior elbow release in children with cerebral palsy is likely to result in which of the following outcomes:
1
Decreased flexion posture during use
2
Decreased flexion contracture
3
Increased use during bimanual activity
4
Increased strength of elbow flexion
5
Increased grip strength
Anterior elbow release consists of lengthening of the lacertus fibrosus and the brachialis fascia. It may or may not include lengthening of the biceps tendon itself. Anterior elbow release effectively decreases the excessive flexion posture of the elbow during use, which one author has termed the âflexion posture angle.â It does not result in decreased (or increased) strength of elbow flexion if the biceps tendon is preserved. Unfortunately, increased use during bimanual activity and increased grip strength are usually not observed.
QUESTION 15 OF 50
A 45-year-old male injures his wrist during Live Action Role Play in Chicago two weeks ago. He underwent operative fixation by and presents to your clinic for his 2 week follow-up visit. You review his operative note in which the surgeon reports having to apply a volar
locking plate in a distal position to secure the difficult intra-articular fracture. The patient shows you the lateral film in Figure A. You remove his splint, he has no difficulty moving any fingers, very minimal pain, and is not taking any narcotic medication. How do you counsel him about his post-operative period?
1
The plate may need to removed once the fracture is healed to reduce the chance of flexor pollicis longus injury
2
The plate may need to removed once the fracture is healed to reduce the chance of flexor carpi radialis injury
3
The plate may need to removed once the fracture is healed to reduce the chance of flexor digitorum superficialis – index finger injury
4
The patient should undergo revision fixation as soon as possible
5
The plate is in appropriate position and will likely never need to be removed
This patient’s volar locking plate (VLP) is distal to the "watershed line", extending volarly beyond the most volar aspect of the distal radius. He is at greatest risk for an attritional rupture of the FPL.
A VLP placed this distal and volar is more likely to cause flexor tendon injury.
Up to 12% of all patients undergoing volar plate fixation will experience flexor tendon injury, and the FPL is the most common tendon associated with the VLP (57% of total flexor tendon ruptures). The average time from fixation to flexor tendon rupture has been cited at 9 months. To judge if a plate is volar to the watershed line, a plum line can be made in the proximal direction from the most volar edge of the distal radius. If a plate is volar to this (Soong) line, the patient is thought to be at a higher risk for flexor tendon injury. As a result, this patient should be followed closely and if pain with thumb flexion is present after 3 months, the surgeon should consider plate removal so long as the fracture is healed to reduce the chance of FPL rupture. Ruptured tendons require repair, grafting, or transfer with hardware removal.
Griffin and Chhabra comprehensively reviewed the risk factors and adverse events following VLP fixation of distal radius fractures, including flexor tendonitis and rupture. They found that risk factors for flexor tendon rupture following VLP fixation included plate placement distal to the watershed line and that PQ repair does not seem to affect flexor tendonitis.
Agnew et al. analyzed wrist MRIs to determine the relationship between the flexor tendons and the watershed line. They found that at 3mm proximal to the watershed line, the FPL and FDP to the index finger were 2.6 and 2.2mm anterior to the volar rim of the distal radius. The authors suggested that distally placed plates are incredibly close to the flexor tendons.
Chilelli et al. described 24 of 48 wrists which had VLP following distal radius fracture and went on to experiences loss of FPL flexion post-operatively. They found that FPL ROM generally returned after 52 days, however with an associated average loss of 11° in thumb IPJ ROM. The authors attribute this to stripping of FPL from the bone during the volar approach.
Soong et al. divided patients who underwent VLP fixation for distal radius fractures into three groups according to position of plate relative to a plum line extending proximally from the most volar and distal aspect of the distal radius: those with a VLP dorsal to the Soong line (grade 0), those with the VLP volar to the Soong line but proximal to the rim (grade 1), and those with a VLP volar to the Soong line and at or distal to rim (grade 2). Of the 73 cases reviewed, the authors reported three flexor tendon ruptures, two of which were grade 2 position. The authors concluded that both position of plate and type of plate were contributors to flexor tendon injury following VLP fixation.
Figure A is a lateral radiograph of the wrist demonstrating appropriate reduction and fixation but with the VLP volar to the "watershed" or Soong line.
Illustration A is a lateral radiograph with Soong's line drawn to show that this plate is too volar.
Incorrect Answers:
Answer 2: The FCR is very superficial and is not commonly injured following VLP fixation of distal radius fractures.
Answer 3: While the FDP to the index finger is the second most common flexor tendon injury following VLP, injury to the FDS to the index finger is unlikely.
Answer 4: The patient is only two weeks from fixation and has no symptoms. The reduction appears appropriate on the imaging seen. Therefore there is no need for urgent revision fixation.
Answer 5: The VLP shown is volar to the watershed line is therefore not in an appropriate position.
QUESTION 16 OF 50
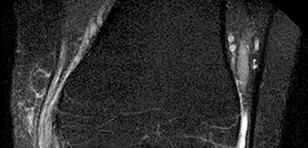
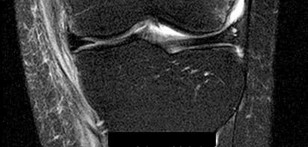
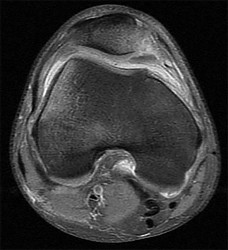
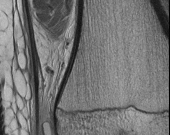
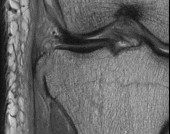
Figures 1 through 3 are the MRI scans of a 26-year-old man who injured his knee wrestling one day prior. He has a moderate effusion, medial knee pain and an inability to extend his knee actively or passively. What is the most appropriate definitive treatment option?
1
Physical therapy
2
Posterior cruciate ligament (PCL) reconstruction
3
Attempted meniscus repair
4
Knee aspiration and manipulation under anesthesia
The images show a bucket handle medial meniscus tear, which is likely responsible for the block to motion. Therefore, surgery should be recommended with a meniscus repair if possible. Physical therapy or knee aspiration/manipulation under anesthesia is not the best definitive treatment.
QUESTION 17 OF 50
An 11-year-old boy stepped on a nail and sustained a puncture to the right forefoot 6 days ago. He was wearing tennis shoes at the time of injury. Treatment in the emergency department consisted of local debridement and tetanus prophylaxis; a radiograph was negative for foreign body, chondral defect, or fracture. He was discharged with a 3-day prescription of amoxicillin and clavulanate. The patient now has increasing pain and tenderness at the puncture site. What is the best course of action?
1
Change the antibiotic to ciprofloxacin
2
Initiate gentamicin
3
Resume the prescription for amoxicillin and clavulanate
4
Observation and follow-up in 48 hours
5
Surgical debridement
The initial treatment consisting of oral antibiotics was appropriate but with progressive symptoms, surgical debridement is necessary. Ciprofloxacin is contraindicated in children, and at this stage, oral antibiotics are inadequate. Intravenous antibiotics may be necessary, but surgical debridement is paramount. Failure to respond to the initial management precludes further observation.
REFERENCES: Riegler HP, Routson T: Complications of deep puncture wounds of the foot.
J Trauma 1979;19:18-22.
Green NE: Musculoskeletal infections in children: Part IV. Pseudomonas infections of the foot following puncture wounds. Instr Course Lect 1983;32:43-46.
QUESTION 18 OF 50
of 100
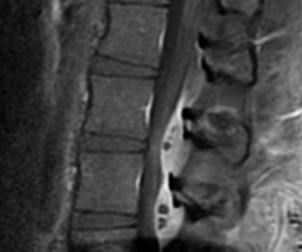
A 35-year-old man who has had a 6-month history of low back pain and tenderness now reports worsening pain and stiffness in the hips and entire back. An AP radiograph of the pelvis demonstrates fusion of the sacroiliac joints bilaterally. What is the next most appropriate step in management?
1
Anesthetic injections in both sacroiliac joints
2
Sacroiliac fusion with plate fixation
3
Anti-inflammatory medications, physical therapy, and HLA-B27 testing
4
Immediate bilateral sacroiliac joint aspiration and culture
■ The patient has a classic presentation of early ankylosing spondylitis. Sacroiliac joint fusion is the earliest radiographic finding and is typically followed by cephalad spinal progression. Early treatment of ankylosing spondylitis consists of nonsteroidal anti-inflammatory drugs and physical therapy to preserve spinal motion. HLA-B27 testing is positive in most (about 95%) patients; however, it is not pathognomonic because it can be positive with other conditions. Considering the progressive nature of this disease, further work-up in a patient with potential ankylosing spondylitis is not warranted. Sacroiliac joint anesthetic injections and sacroiliac fusion are not recommended treatments for early ankylosing spondylitis. Aspiration of the sacroiliac joints can be done if sacroiliac joint infection is suspected; however, in the absence of fever or other constitutional symptoms, infection is unlikely.
QUESTION 19 OF 50
Figures 1 and 2 are the AP and lateral radiographs of a 32-year-old man 10 years after anterior cruciate ligament (ACL) reconstruction. The patient now has worsening medial knee pain and a failed ACL with instability. What is the best surgical option?
1
Revision ACL with bone-patellar tendon-bone (BTB) allograft and meniscal transplant
2
Distal femoral osteotomy
3
Pure sagittal osteotomy
4
Closing wedge and slope neutralizing high-tibial osteoto
Lateral closing wedge (LCW) and medial opening wedge (MOW) high-tibial osteotomies (HTOs) can both correct varus knee alignment and stabilize the ACL–deficient knee. Increasingly, HTO is being proposed as a singular or concomitant procedure with ACL reconstruction for restoring knee stability and as a more reliable slope correction. LCW HTO demonstrates more reliable slope correction than does MOW HTO. Revision ACL with BTB allograft and meniscal transplant will not help early arthritis in varus alignment. Distal femoral osteotomy is usually considered for valgus knee. Pure sagittal osteotomy _would not help the patient’s medial knee pain, arthritis, and malalignment._
QUESTION 20 OF 50
A 10-year-old child was referred for spinal curvature and a 2-year history of back pain. She has pain during the day and pain at night that wakes her from sleep and is temporarily relieved with nonsteroidal anti-inflammatory drugs. Examination shows very tight hamstrings and an irritative spinal curvature. Figures 71a through 7Id show radiographs, a bone scan, and a CT scan. What is the most appropriate treatment?
1
Bracing with a thoracolumbosacral orthosis (TLSO)
2
Observation with repeat radiographs of the scoliosis in 3 months and nonsteroidal antiinflammatory drugs for the pain
3
MRI of the neuro-axis
4
Surgical removal
5
Radiofrequency ablation
The history, examination findings, and studies are consistent with an osteoid osteoma. The CT scan shows a classic “target” lesion, and the bone scan has intense uptake at the site of the osteoid osteoma. The child has had a 2-year history of pain that even wakes her from sleep, so observation and anti-inflammatory drugs is not a preferred treatment. Bracing will not help with the discomfort because the pain is not mechanical in nature. MRI would not be needed in addition to the studies already completed. The osteoid osteoma is close to the spinal cord so radiofrequency ablation is not preferred. Surgical removal and biopsy is the treatment of choice.
REFERENCES: Frassica FJ, Waltrip RL, Sponseller PD, et al: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-
574/. Cantwell CP, Obyme J, Eustace S: Current trends in treatment of osteoid osteoma with an emphasis on radiofrequency ablation. Eur Radiol 2004;14:607-617.
Figure 72
QUESTION 21 OF 50
Ultrasound therapy delivers superficial heat to the tissue and has a penetration depth of 5 mm.
1
True
2
False
Ultrasound is considered a deep heat modality and does not heat the superficial tissues.
QUESTION 22 OF 50
Figure 1
A 59-year-old woman presents for treatment of a painful hallux valgus deformity. She has a prominent bunion, normal motion of the hallux metatarsophalangeal (MP) joint, and painful callosity under the second MP joint. Radiographs of the foot are
presented. The recommended treatment is:
1
Arthrodesis of the hallux MP joint
2
Soft tissue release and distal metatarsal osteotomy
3
Soft tissue release and proximal metatarsal osteotomy
4
Soft tissue release and arthrodesis metatarsocuneiform joint
5
Resection arthroplasty of the hallux MP joint
This patient has probable instability of the metatarsocuneiform joint manifested by the overload phenomenon of the second metatarsal. Although this is not a sufficient indication for performing an arthrodesis of the metatarsocuneiform joint (modified Lapidus procedure), other findings of second metatarsal overload, including thickening of the cortex of the second metatarsal and instability of the first metatatarsocuneiform joint, should be looked for in addition to hypermobility of the first ray.
QUESTION 23 OF 50
Which of the following is the most common finding in diastematomyelia:
1
C utaneous lesions over the spine
2
Anisomelia
3
Foot deformity
4
Neurologic deficit
5
Widened interpedicular distance
Widened interpedicular distance is the most common finding (94% or greater) in patients with diastematomyelia.
Neurologic deficit is present in 60% to 88% of patients with diastematomyelia.
A cutaneous lesion, such as a dimple or hairy patch, is present in 55% to 79% of patients with diastematomyelia. Anisomelia is present in 53% to 58% of patients with diastematomyelia.
Foot deformities are present in 32% to 52% of patients with diastematomyelia.
QUESTION 24 OF 50
of 100 A B C
What is the appropriate first step when confirming the diagnosis of a neurologically intact, 73-year-old man who has the images shown in Figures 25a through 25c?
1
Order a prostate-specific antigen (PSA) level
2
Perform a 2-level corpectomy and reconstruction with tissue sent for pathologic analysis
3
Fine-needle aspiration
4
Bone scan
The radiograph and MR images show an osteoblastic lesion in the T9 and T8 vertebral bodies. In an older man, this finding most likely reveals metastatic prostate cancer. The first and least invasive diagnostic step is to order a PSA level. Gleave and associates found in a retrospective review of patients with prostate cancer that isolated levels of PSA lower than 10 to 20 micrograms per liter are rarely associated with bone metastasis. Vis and associates documented that 10-year prostate cancer survival in a screened population was higher than 60%, and in an unscreened population it was 24%. In a neurologically intact patient with no evidence of neural compression or instability, surgery is not indicated. Fine-needle aspiration may be performed, but the diagnostic yield in a blastic lesion is low. A bone scan may be indicated to complete the metastatic workup, but it will not aid in the diagnosis of tissue source.
RECOMMENDED READINGS
[Gleave ME, Coupland D, Drachenberg D, Cohen L, Kwong S, Goldenberg SL, Sullivan LD. Ability of serum prostate-specific antigen levels to predict normal bone scans in patients with newly diagnosed prostate cancer. Urology. 1996 May;47(5):708-12. PubMed PMID: 8650870. ](http://www.ncbi.nlm.nih.gov/pubmed/8650870)[View ](http://www.ncbi.nlm.nih.gov/pubmed/8650870)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/8650870)
[Vis AN, Roemeling S, Reedijk AM, Otto SJ, Schröder FH. Overall survival in the intervention arm of a randomized controlled screening trial for prostate cancer compared with a clinically diagnosed cohort. Eur Urol. 2008 Jan;53(1):91-8. Epub 2007 Jun 12. PubMed PMID: 17583416. ](http://www.ncbi.nlm.nih.gov/pubmed/17583416)[View ](http://www.ncbi.nlm.nih.gov/pubmed/17583416)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17583416)
Cronen GA, Emery SE. Benign and malignant lesions of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:351-366.
CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29
Figures 26a and 26b are the MR images with gadolinium enhancement of a 40-year-old man who arrives at the emergency department with a 4-day history of fevers and severe back pain without radiation. He is normotensive at presentation with a heart rate of 86 beats per minute. Upon examination he is neurologically intact with normal sensory and motor function. He has a history of alcohol and cocaine abuse. His white blood cell (WBC) count is 12000 (reference range [rr], 4500-11000 /µL) and his C-reactive protein (CRP) level is 100 mg/L (rr, 0.08-3.1 mg/L)
QUESTION 25 OF 50
The clinical variable found to be associated with a higher risk of complications following open reduction and internal fixation of unstable ankle fractures in diabetic patients was:
1
Presence of a severe fracture pattern
2
Presence of an open fracture
3
Insulin-dependent diabetes mellitus
4
Peripheral neuropathy or vasculopathy
5
Presence of nephropathy
A retrospective Level IV study followed 84 patients with diabetes who underwent open reduction internal fixation of unstable ankle fractures. After analyzing multiple patient factors including sex, fracture pattern, open or closed injury, nephropathy, hypertension, vasculopathy, peripheral neuropathy, and diabetic control (insulin-dependent compared with non-insulin- dependent), the only factors that predicted a higher rate of complications were vasculopathy and peripheral neuropathy. There was a 12% rate of postoperative infection and an overall 14% rate of complications.
QUESTION 26 OF 50
of 100
What condition favors pollicization in hypoplasia of the thumb?
1
Extrinsic tendon abnormalities involving the flexor and extensor
2
Narrowing of the first web space
3
Insufficiency of the ulnar collateral ligament of the metaphalangeal joint
4
Unstable carpometacarpal joint
The decision to ablate and pollicize vs preserve and reconstruct is based on the stability of the carpometacarpal joint. A stable thumb is more easily used in prehension activities of grasping and pinching. All other responses are associated with surgical options for reconstruction of the thumb. The carpometacarpal joint is the “keystone” for thumb-to-hand attachment. Without a stable carpometacarpal joint, pollicization may be required. No other response necessitates pollicization.
RECOMMENDED READINGS
1. [McCarroll HR. Congenital anomalies: a 25-year overview. J Hand Surg Am. 2000 Nov;25(6):1007-37. Review. PubMed PMID: 11119659. ](http://www.ncbi.nlm.nih.gov/pubmed/11119659)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11119659)
2. [Manske PR, Goldfarb CA. Congenital failure of formation of the upper limb. Hand Clin. 2009 May;25(2):157-70. doi: 10.1016/j.hcl.2008.10.005. Review. PubMed PMID: 19380058.](http://www.ncbi.nlm.nih.gov/pubmed/19380058)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19380058)
38
RESPONSES FOR QUESTIONS 41 THROUGH 44
Match the patient and image with the treatment listed.
QUESTION 27 OF 50
A 63-year-old woman reports pain in her groin, particularly when rising from a chair and when taking her first steps out of bed in the morning. History reveals that she underwent a left primary total hip arthroplasty 19 years ago. An AP radiograph is shown in Figure 62 and revision surgery is planned. What is the most reliable method for reconstruction of the acetabulum?
1
Use of a cemented, all polyethylene acetabular component
2
Use of a cementless, porous-coated acetabular component with adjunctive screw fixation
3
Use of an antiprotrusio cage
4
Use of a bilobed, cementless acetabular component
5
Use of a bipolar head placed directly into the acetabulum
DISCUSSION: The patient has severe wear and loosening of her cemented, all polyethylene acetabular component with a Paprosky type 2 acetabular defect. Optimal long-term results have been achieved with the use of a cementless, porous-coated acetabular component with adjunctive screw fixation. Cemented, all polyethylene components have been shown to have a high rate of failure when used in the revision setting. Bilobed components and antiprotrusio cages are unnecessary for this straightforward defect and have had mixed results reported in the literature. The use of a bipolar head placed directly into the acetabulum is associated with high rates of persistent pain and progressive acetabular erosion.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 457474.
Della Valle CJ, Schuaipaj T, Berger RA, et al: Revision of the acetabular component without cement after total hip
arthroplasty: A concise follow-up, at fifteen to nineteen years, of a previous report. J Bone Joint Surg Am 2005;87:1795-1800.
Templeton JE, Callaghan JJ, Goetz DD, et al: Revision of a cemented acetabular component to a cementless acetabular component: A ten to fourteen-year follow-up study. J Bone Joint Surg Am
2001;83:1706-1711.
QUESTION 28 OF 50
of 100
A 17-year-old male baseball catcher has groin pain and intermittent hip locking. Examination demonstrates reproduction of the pain with hip flexion, internal rotation, and adduction. MR imaging reveals an anterosuperior labral tear.
1
Sclerosis of the proximal femoral epiphysis with subchondral lucency
2
Abnormal femoral head-neck junction offset
3
Widening of the proximal femoral physis with normal femoral head-neck junction offset
4
Absence of the proximal femoral epiphysis secondary ossification center
- Abnormal femoral head-neck junction offset
QUESTION 29 OF 50
A 26-year-old man was thrown from a car and sustained the injury seen in Figures 44a and 44b. Nonsurgical management of this injury is recommended. Which of the following factors increases the risk of nonunion?
1
Male gender
2
Diaphyseal location
3
Comminuted displaced fracture
4
Young age
5
Associated injuries
The patient has a displaced comminuted clavicle middle one third fracture from a high-energy mechanism. Recent literature on high-energy clavicular fractures suggests a higher rate of nonunion than previously reported. A nonunion rate of 30% has been reported by Hill and associates when the fracture fragments are displaced more than 1.5 cm. In addition, several patients had neurologic symptoms related to the injury. Robinson and associates reported an increased risk of nonunion in women, elderly patients, comminuted fractures, and injuries with a lack of cortical contact.
REFERENCES: Hill JM, McGuire MH, Crosby LA: Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br 1997;79:537-539.
Wick M, Muller EJ, Kollig E: Midshaft fractures of the clavicle with a shortening of more than
2 cm predispose to nonunion. Arch Orthop Trauma Surg 2001;121:207-211.
Robinson CM, Court-Brown CM, McQueen MM, et al: Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am
2004;86:1359-1365.
QUESTION 30 OF 50
An African-American mother brings her 18-month-old baby in for examination because he has bowing of the legs. The childâs past medical history is normal including height and weight. The child is still breast-fed. Radiographs reveal mild widening and irregularity of the physes. Which of the following conditions is likely to be found on laboratory examination:
1
Elevated phosphorus
2
Decreased alkaline phosphatase
3
Normal 1,25 dihydroxyvitamin D
4
Elevated creatinine
5
Elevated parathyroid hormone
This patient has nutritional rickets because of a combination of decreased vitamin D intake and increased need for sunlight due to dark skin. The laboratory findings should include a lowânormal calcium phosphate, elevated alkaline phosphatase and parathryoid hormone, and low vitamin D levels and precursors. Vitamin D supplementation without bracing is adequate treatment.
QUESTION 31 OF 50
The ABER (abducted and externally rotated) position in the shoulder MRI scan shown in Figure 1 can be helpful in identifying a variety of subtle pathologies including rotator cuff tears and capsulolabral injury. While in the ABER position, the humerus and glenoid are seen predominantly in what planes, respectively?
1
Sagittal and coronal
2
Coronal and axial
3
Axial and sagittal
4
Axial and coronal
While in the ABER position in the MRI machine, the MRI technician aligns the cut lines along the axis of the humerus and perpendicular through the glenoid, from superior to inferior. According to this, one might assume that the humerus would be seen in a sagittal plane and the glenoid in an axial plane. However, while the glenoid
does stay fixed in an axial plane, the humerus is externally rotated, resulting in a coronal view of the proximal humerus. All of the other options do not depict the anatomic relationship of the humerus and glenoid properly while in the ABER sequence.
QUESTION 32 OF 50
A 16-year-old boy falls while playing soccer. He reports that his knee buckled when he planted his leg to kick a ball. He noticed an obvious deformity of his knee, which spontaneously resolved with a “clunk.” He could not finish the game but was able to bear weight with a limp. He has had two similar episodes but has never sought medical attention. An initial examination demonstrated an effusion, tenderness at the proximal medial collateral region and medial patellofemoral retinaculum, decreased range of motion, and patella apprehension. A lateral patellar glide performed at 30° of flexion was 3+. He was otherwise ligamentously stable, and there were no other noteworthy findings.Figures 3 and 4 are this patient's proton density fat-saturated MR images. His tibial tubercle-trochlear groove (TT-TG) distance is 12 mm, and he has normal limb-alignment film findings. Treatment at this stage should include --- ---
1
hinged knee bracing, protected weight bearing, and physical therapy.
2
anteromedialization of the tibial tubercle.
3
internal fixation and medial patellofemoral ligament (MPFL) reconstruction.
4
arthroscopic lateral retinacular release.
This patient’s examination and history indicate recurrent patellar dislocations. Radiographs show an osseous or osteochondral loose fragment. There is no evidence of an obvious nondisplaced fracture or physeal changes. In the setting of suspected patella dislocation or subluxation with loose fragment seen on radiograph, an MRI is indicated. Lateral release alone is seldom indicated in a knee that is normal before injury. The examination and MRI do not indicate a need for medial collateral ligament repair.
Treatment should consist of arthroscopy or arthrotomy and attempted internal fixation of this fragment. If fixation is not possible, the loose body can be removed. Normal TT-TG values, an increased lateral patellar glide, and a history of recurrent patellar dislocations after trauma suggest MPFL incompetence _and the need for reconstruction._
QUESTION 33 OF 50
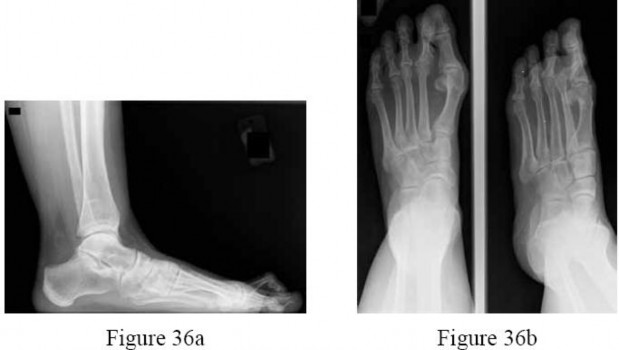
Figures 36a and 36b are the AP and lateral radiographs of a 65-year-old woman who has a dislocated second toe and a prominent bunion. Besides repairing the bunion, what procedures are recommended to address the fixed second hammertoe and the resulting metatarsalgia? ---
PIP resection arthroplasty, extensor tendon lengthening, and Weil osteotomy
3
Flexor to extensor tendon transfer and metatarsal head excision
4
PIP fusion and DuVries arthroplasty
5
Metatarsal head excision and proximal phalanx resection
The patient has a subluxated second metatarsophalangeal (MTP) joint, but no evidence of second metatarsal head destruction. The patient also has a fixed claw toe. The claw toe is repaired with a PIP resection arthroplasty or a PIP fusion. The likelihood of
completely correcting the MTP joint dislocation with just these two procedures, however, is small and the addition of the Weil osteotomy is more likely to allow decompression of the joint and complete relocation of the MTP joint. The flexor to extensor transfer is indicated for a flexible hammertoe. A metatarsal head excision is a salvage option of the toe that still cannot be reduced after the Weil osteotomy, but this may lead to transfer lesions.The DuVries arthroplasty will not help reduce the MTP joint. Combined metatarsal head excision and proximal phalanx resection would be extreme and is not recommended.
QUESTION 34 OF 50
A 9-year-old boy is examined due to a closed distal forearm fracture. The radius and ulna are both fractured and translated
100%. After manipulation twice with sedation, the translation cannot be reduced. There is 10-mm shortening of the radius and 5- mm shortening of the ulna. The distal radial angulation on the anteroposterior view is 5° less than normal. The least invasive treatment which would produce acceptable results is:
1
C losed reduction in the operating room under general anesthesia
2
Open reduction and cast application
3
Open reduction and percutaneous pin fixation
4
Open reduction and plate fixation
5
Acceptance of the reduction and maintenance with a cast
The translation and shortening are not problems and the amount of angulation will easily remodel with this fracture. There is nothing to be gained from operative reduction.
QUESTION 35 OF 50
A 72-year-old female presents to the office 5 weeks after distal radius fracture surgery with the findings seen in Figure A. She performed daily cleansing with soap and water and dry dressings.
Which of the following has been shown to decrease the risk of developing this complication?
1
A solution of 0.45% sodium chloride and hydrogen peroxide
2
A solution of 0.9% sodium chloride and hydrogen peroxide
3
A solution of 0.45% sodium chloride and chlorhexidine
4
A solution of 0.9% sodium chloride and chlorhexidine
5
None of the above, as specialized cleansing solutions do not decrease the risk this complication
There is no difference between daily showers with soap, water and dry dressings, and solutions comprising (1) saline and chlorhexidine, or (2) saline and hydrogen peroxide.
The risks of external fixation include cellulitis, pin-track drainage, osteomyelitis and pin loosening. The rate of complications is about 20%. Chlorhexidine gluconate has broad spectrum activity against gram-positive and negative bacteria by disrupting cell membranes. It is not affected by blood and has low skin irritancy. Studies show that simple pin-site care (showers, dry dressings) maintains a low infection rate.
Egol et al. performed a randomized trial examining external fixation pin tracts about the wrist. They compared (1) weekly dry dressings, (2) daily pin care with half normal saline (NS) and hydrogen peroxide (H2O2) and (3) chlorhexidine discs with weekly changes. They found pin-site complications in 19%, with no difference between the 3 groups. They do not recommend additional wound care beyond sterile dressings.
Stinner et al. performed a survey on the use of half-pins by the limb lengthening and reconstruction society. They found that most respondents preferred hydroxyapatite coating (81%) because of improved fixation and decreased loosening (less radiographic pin-tract rarefaction and greater extraction torque, which may lead to lower infection rates). Most encouraged
shower (60%) and washing solution (67%)(soap and water, peroxide or saline) for pin site care.
Figure A shows an external fixator around the wrist with cellulitis around the proximal half-pins.
Incorrect Answers
Answers 1-4: Hydrogen peroxide and chlorhexidine based solutions have not been conclusively shown to decrease the rate of pin site complications.
QUESTION 36 OF 50
A patient sustained a periprosthetic femoral fracture. The proximal femur is comminuted and the femoral component is loose. The patient has absent pulses and poor capillary refill. An emergent arteriogram is shown in Figure 82. What is the most appropriate management?
1
Open reduction and internal fixation of the fracture
2
Traction, followed by revision total hip arthroplasty and vascular repair
3
Revision total hip arthroplasty, four compartment fasciotomy, and sequential neurovascular examination
4
Revision total hip arthroplasty, followed by vascular repair
5
Traction, followed by vascular shunting, revision total hip arthroplasty, and definitive vascular repair
DISCUSSION: The patient requires emergent revascularization with signs of ischemia of unknown duration. The leg has shortened substantially and initial management requires traction to return the leg to length. This should be followed by revascularization of the leg. A temporary shunt may be helpful until the fracture has been stabilized (revision total hip arthroplasty) with the leg at full length. Definitive vascular bypass should then be performed.
REFERENCES: Calligaro KD, Dougherty MJ, Ryan S, et al: Acute arterial complications associated with total hip and knee arthroplasty. J Vase Surg 2003;38:1170-1177.
Brady OH, Garbuz DS, Masri BA, et al: Classification of the hip. Orthop Clin North Am 1999;30;215- 220. Question 83
During normal human knee flexion (beginning with the knee fully extended), which of the following statements best describes tibial rotation with respect to the femur?
1. ### Rotation is constantly occurring in both directions during the flexion cycle.
2. ### The tibia initially externally rotates, then progressively internally rotates.
3. ### The tibia initially internally rotates, then progressively externally rotates.
4. ### The tibia initially internally rotates, then remains in that rotational position until deep flexion when further internal rotation occurs.
5. ### The tibia initially externally rotates, then remains in that rotational position until deep flexion when further external rotation occurs.
PREFERRED RESPONSE: 4
DISCUSSION: During knee flexion, the tibia initially rotates internally in approximately the first 20 degrees and generally maintains this rotational position until flexion past 90 degrees when significantly more internal rotation occurs.
REFERENCE: Coughlin KM, Incavo SJ, Churchill DL, et al: Tibial axis and patellar position relative to the femoral epicondylar axis during squatting. J Arthroplasty 2003;18:1048-1055.
QUESTION 37 OF 50
The ideal range of micromotion to stimulate bone ingrowth into cementless implants is:
1
Less than 20 microns
2
30 microns to 150 microns
3
200 microns to 500 microns
4
600 microns to 800 microns
5
Greater than 900 microns
Ideal values of micromotion that stimulate bone ingrowth are 28 microns to 150 microns. Values greater than 150 microns are associated with fibrous ingrowth
QUESTION 38 OF 50
Smoking has been associated with lower fusion rates in both cervical and lumbar fusion. Which of the following statements best describes an explanation for these findings?
1
Nicotine impairs osteoblast activity, thus interfering with bone remodeling.
2
The effects of smoking on bone healing are multifactorial and not yet fully understood.
3
The vasoconstrictive and platelet-activating properties of nicotine inhibit fracture healing.
4
Nicotine inhibits the function of fibroblasts, red blood cells, and macrophages.
5
Hydrogen cyanide inhibits oxidative metabolism at the cellular level.
of the mechanism mediating this effect. Whereas all of the above have been postulated as explanations, more recent studies have
demonstrated that nicotine delivered via a transdermal patch significantly enhanced posterior spinal fusion in rabbits. Thus it appears that the effects of smoking on fracture healing are multifactorial and not yet fully understood.
QUESTION 39 OF 50
Evidence of cementless acetabular implant loosening is radiographically observed as:
1
Surrounding cystiClesions
2
HeterotopiCbone formation
3
Increased radiodensity
4
Implant spot welds
5
Radiolucency surrounding the shell
Of the choices listed, only radiolucency provides evidence of acetabular loosening. CystiClesions, known as osteolysis, may exist without the presence of loosening
QUESTION 40 OF 50
What is the preferred treatment for a type CperiprosthetiCfracture with a well-fixed humeral component:
1
Open reduction internal fixation with a plate
2
Long stem prosthesis
3
Strut allograft and cerclage wires
4
Nonoperative treatment
5
Long stem with a strut
In patients with a type CperiprosthetiCfracture (distal to the tip of the prosthesis) and a well-fixed humeral component, the injury can be treated similar to a closed humerus fracture
QUESTION 41 OF 50
A 42-year-old male sustains the closed injury shown in Figure A. Which of the following factors is associated with improved outcomes with open reduction and internal fixation?
1
Age > 40
2
Smoking
3
Male sex
4
No worker's compensation involvement
5
Career as construction worker
The clinical and radiographic presentation is consistent with a closed, displaced, comminuted calcaneus fracture. Non-worker's compensation patients have improved outcomes with operative treatment.
Buckley et al performed a multicenter prospective randomized study of over 300 displaced calcaneus fractures comparing nonoperative vs. operative treatment. They looked at patient satisfaction, SF-36 scores, and Bohler’s angle. They showed improved outcome in at least one measure after an operation vs. no operation for intraarticular calcaneal fractures in: 1) Women
2) Age <30 3) Non Smokers 4) Light work laborers 5) Non worker’s compensation patients.
Sanders et al reviews calcaneus fractures, including treatment techniques. They recommend getting two-dimensional computed tomographic scans in both the coronal and the transverse plane. They report with operative treatment, the goal is restoring not only articular congruency, but also the shape and alignment of the calcaneus.
QUESTION 42 OF 50
of 100
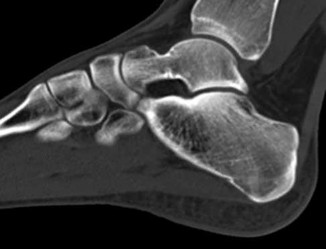
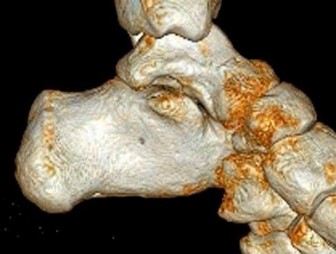
Figures 6a through 6j A B 7
C F
D E G H
1
Normal foot
2
Calcaneonavicular (CN) coalition
3
Talocalcaneal (TC) middle facet coalition
4
TC posterior facet coalition
- Calcaneonavicular (CN) coalition
QUESTION 43 OF 50
Patients with homocystinuria phenotypically resemble patients with:
1
Achondroplasia
2
Larsen's syndrome
3
Marfan syndrome
4
Gaucher's disease
5
Noonan's syndrome
Patients with homocystinuria may phenotypically resemble patients with Marfan syndrome. Patients with homocystinuria and
Marfan syndrome are tall with long limbs, arachnodactyly, scoliosis, chest wall deformities, and lens dislocations.
Achondroplasia is characterized by short stature, frontal bossing, and rhizomelic shortening of the limbs. Larsen's syndrome is a disorder characterized by short stature and multiple joint dislocations.
Gaucher's disease is a lysosomal storage disease characterized by accumulation of cerebroside in cells of the reticuloendothelial system. As in patients with homocystinuria, patients with Gaucher's disease have osteoporosis, however, they do not develop any of the other phenotypic features seen in homocystinuria.
Noonan's syndrome effects boys and clinical features include short stature, a webbed neck, and cubitus valgus deformities.
QUESTION 44 OF 50
-A 20-year-old concert pianist sustained a diaphyseal radius fracture and underwent open reduction and internal fixation 3 years ago. She is thin and reports that the plate is irritating her after playing the piano for an hour or more. She undergoes elective plate removal of the 3.5 mm plate and 2 weeks later she refractures the radius. Which of the following statements is most accurate?
1
Diaphyseal plate removals are at higher risk of refracture.
2
Postoperative splinting increases the chance of refracture.
3
The patient would not have sustained a refracture if the plate was 4.5 mm.
4
The risk of fracture increased because the plate was removed within 5 years.
5
Waiting 5 years to remove the hardware would have decreased the risk of refracture.
No detailed explanation provided for this question.
QUESTION 45 OF 50
A 70-year-old golfer has pain in her dominant shoulder. She reports that initially the pain was at night but now she is unable to play. Examination reveals weakness in external rotation and shoulder abduction. Radiographs reveal the humeral head articulating with a thin acromion. Management should consist of
1
a scapular and rotator cuff strengthening program.
2
arthroscopy.
3
review of her golf technique.
4
humeral head replacement.
5
an erythrocyte sedimentation rate.
Chronic rotator cuff tears should be nonsurgically managed initially with a strengthening program. A cortisone injection may reduce inflammation. Surgery is reserved for patients who continue to have pain and lose sleep despite the use of physical therapy. Blood tests for infection or inflammation are nonspecific. Arthroscopy may play a role, but surgical replacement is reserved for advanced cases.
REFERENCES: Bokor DJ, Hawkins RJ, Huckell GH, et al: Results of nonoperative management of full-thickness tears of the rotator cuff. Clin Orthop 1993;294:103-110.
Wirth MA, Basamania C, Rockwood CA Jr: Nonoperative management of full-thickness tears of the rotator cuff. Orthop Clin North Am 1997;28:59-67.
QUESTION 46 OF 50
of 100
What is the most common complication following distal biceps tendon repair?
1
Posterior interosseous nerve palsy
2
Rerupture of the repair
3
Lateral antebrachial cutaneous neuropraxia
4
Superficial radial sensory neuropathy
The distal biceps tendon is commonly torn with an eccentric contraction of the biceps when the elbow is taken into extension. Patients treated nonsurgically will note loss of at least 50% supination strength and may develop discomfort with resistive activities. The video shows the squeeze test to evaluate the integrity of the biceps tendon. The test is similar to the Thompson test in the evaluation of an Achilles tendon rupture. The distal arm is squeezed with the elbow flexed 60 to 80 degrees and the forearm pronated. By shortening the musculotendinous unit, the intact biceps tendon will lead to forearm supination. If the biceps is torn, the forearm will not supinate as shown in the video. The maneuver is performed with the elbow in flexion to minimize tension on the brachialis muscle and isolate the biceps. Ruland and associates evaluated 25 patients with suspected distal biceps ruptures and correctly diagnosed all but 1 false-positive result that involved a partial tear. The lacertus fibrosus is not evaluated with this maneuver.
When considering a repair, a 1- or 2-incision technique may be performed. Chavan and associates performed a systematic review comparing the 2 techniques and reported similar complication rates. The 2-incision technique was associated with more instances of significant loss of forearm rotation and more unsatisfactory clinical results. The 1-incision technique is associated with a higher incidence of lateral antebrachial cutaneous neuropathy likely attributable to retraction. The biceps insertion is a thin semilunar area on the posterior/ulnar aspect of the radial tuberosity centered at approximately 30 degrees anterior to the lateral/coronal plane with the arm fully supinated. Forthman and associates used CT scan to asses 30 cadaveric specimens and noted that the biceps tuberosity orientation would prohibit an anatomic repair in 35% of arms for which the 1-incision technique was used.
Mazzocca and associates reported the highest load to failure of the Endobutton (440 newton (N)) compared to fixation with suture anchor (381 N), Wartenberg syndrome (310 N), and an interference screw (232 N). Greenberg and associates noted greater load to failure for the Endobutton (584 N) compared to suture anchor (254 N) and transosseous tunnel (178 N) constructs. Spang and associates reported comparable strength of the Endobutton repair when compared to suture anchors. Fifty N of force is required to hold the elbow flexed at 90 degrees against gravity, which is well below the strength of the repairs studied.
Neuropraxia of the lateral antebrachial cutaneous nerve branch is the most common complication associated with distal biceps repair, with a reported incidence as high as 40%. The nerve branch lies between the biceps and brachialis as it crosses the surgical field in the antecubital fossa. The neuropathy may be related to aggressive retraction, particularly when using the 1-incision technique, and often resolves with time. Cain and associates reported minor complications were common (but major complications uncommon) following distal biceps repair. Reported complications are lateral antebrachial cutaneous paresthesia (26%), radial sensory nerve paresthesia (6%), posterior interosseous nerve injury (4%), and rerupture (2%).
RECOMMENDED READINGS
1. Ruland RT, Dunbar RP, Bowen JD. The biceps squeeze test for diagnosis of distal biceps tendon ruptures. Clin Orthop Relat Res. 2005 Aug;(437):128-31. PubMed PMID: 16056039.
2. Forthman CL, Zimmerman RM, Sullivan MJ, Gabel GT. Cross-sectional anatomy of the bicipital tuberosity and biceps brachii tendon insertion: relevance to anatomic tendon repair. J Shoulder Elbow Surg. 2008 May-Jun;17(3):522-6. doi: 10.1016/j.jse.2007.11.002. Epub 2008 Mar 6. PubMed PMID: 18325797.
3. Chavan PR, Duquin TR, Bisson LJ. Repair of the ruptured distal biceps tendon: a systematic review. Am J Sports Med. 2008 Aug;36(8):1618-24. doi: 10.1177/0363546508321482. Review. PubMed PMID: 18658024.
4. Mazzocca AD, Burton KJ, Romeo AA, Santangelo S, Adams DA, Arciero RA. Biomechanical evaluation of 4 techniques of distal biceps brachii tendon repair. Am J Sports Med. 2007 Feb;35(2):252-
8/. Epub 2006 Dec 27. PubMed PMID: 17192318.
5. Cain RA, Nydick JA, Stein MI, Williams BD, Polikandriotis JA, Hess AV. Complications following distal biceps repair. J Hand Surg Am. 2012 Oct;37(10):2112-7. doi: 10.1016/j.jhsa.2012.06.022. Epub 2012 Aug 30. PubMed PMID: 22938802.
6. Greenberg JA, Fernandez JJ, Wang T, Turner C. EndoButton-assisted repair of distal biceps tendon ruptures. J Shoulder Elbow Surg. 2003 Sep-Oct;12(5):484-90. Erratum in: J Shoulder Elbow Surg. 2005 Mar-Apr;14(2):231. PubMed PMID: 14564273.
7. Spang JT, Weinhold PS, Karas SG. A biomechanical comparison of EndoButton versus suture anchor repair of distal biceps tendon injuries. J Shoulder Elbow Surg. 2006 Jul-Aug;15(4):509-14. PubMed PMID: 16831659.
QUESTION 47 OF 50
--An otherwise healthy 50-year-old man who is a smoker undergoes a posterior spine fusion with instrumentation for spondylolisthesis. What can the patient do to minimize his risk for pseudarthrosis?
1
Increase calcium and vitamin D intake
2
Avoid all nonsteroidal anti-inflammatory drugs (NSAIDs)
3
Maintain smoking cessation
4
Engage in early physical therapy to strengthen the trunk musculature
No detailed explanation provided for this question.
QUESTION 48 OF 50
Figures 1 and 2 are the radiograph and MRI scan of a 16-year-old boy who injured his right knee by a lateral side impact while playing football. The MRI indicates what structure was most likely injured?
1
Lateral collateral ligament
2
Tibial spine
3
Medial meniscus
4
Anterior cruciate ligament (ACL)
This is a rupture of the anterolateral ligament complex and a portion of the IT band. This injury is highly correlated with a complete ACL injury. In the MRI, the curvilinear or elliptic bone fragment (Segond fracture) projected parallel to the lateral aspect of the tibial plateau, the lateral capsular sign, is seen. The lateral capsular sign is also associated with ACL tears. Thus, this is an MRI showing a complete ACL _tear._
QUESTION 49 OF 50
Which of the following is an indication for an anteromedial approach:
1
Post-traumatiCarthritis with severe scarring
2
Rheumatoid arthritis
3
Revision shoulder arthroplasty
4
All of the above
The anteromedial approach facilitates shoulder arthroplasty in patients with severe scarring, distortion of anatomy, as well as patients with frail bone and soft tissue.
QUESTION 50 OF 50
A hockey player had a puck hit his foot. Radiographs taken immediately after the game were negative. He still has persistent pain 5 days after the injury and difficulty weight bearing. What is the best next step?
1
Repeat radiographs
2
Full clearance to return to play
3
Bone scan
4
MRI scan
Ice hockey injuries demand a thorough assessment because they have the potential to be significant. In hockey players, bone injuries in the foot and ankle can be missed or improperly diagnosed through routine radiographic imaging. MRI can display bone injuries that are not found radiographically; this is because _some fractures and contusions involve the medial ankle and midfoot bones._