This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set 674211)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
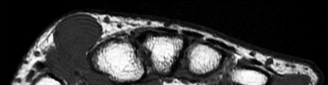
Figure 10 is the radiograph of a middle-aged woman who has had midfoot pain for the past several years without antecedent trauma. What is the most likely etiology of her condition?
1
Osteomyelitis
2
Kohler disease
3
Rheumatoid arthritis
4
Primary osteoarthritis
5
Osteochondritis dissecans
#
**
The radiograph shows isolated degeneration in the talonavicular joint that is symmetric. The symmetry of the degeneration is characteristic of an inflammatory arthritis. In the absence of trauma, isolated arthritis in this joint is uncommon. The navicular is normal sized, ruling out Kohler disease (as well as the patient being in the wrong age group). There are no erosions indicative of osteomyelitis. Osteochondritis dissecans appears as focal osteochondral lesions, which are not present in the radiograph.
QUESTION 2 OF 50
of 100
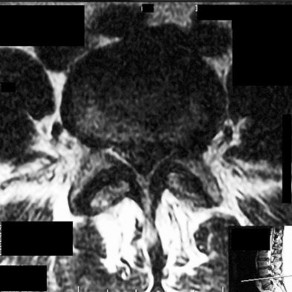
Figures 7a through 7d are the images of a 31-year-old obese woman who has a long history of low-back pain and intermittent bilateral lower extremity pain. Five days ago her symptoms increased markedly and she was given pain medications upon presentation to her primary care physician. Three days ago she noticed that her bed was wet upon awakening; she also had numbness and tingling in her peroneal area and lower extremities and weakness in her lower extremities. She is brought to your office in a wheelchair. Her examination reveals diminished sensation to light touch in the L4 to S4 dermatomes and 0-1/5 strength in all muscle groups in her bilateral lower
extremities with the exception of her hip flexors, hip adductors, and quadriceps, which are 5/5 in strength. She has decreased sphincter tone on rectal examination. You recommend immediate decompressive laminectomy. What is the likelihood she will regain bladder function after surgery?
A B C D
1
0% to 20%
2
21% to 40%
3
41% to 60%
4
61% to 80%
This patient has congenital and acquired spinal stenosis with multilevel disk protrusions that have both chronic (calcified) and acute components, resulting is multilevel cauda equina compression and acute cauda equina syndrome of more than 48 hours duration. Most studies indicate that patients who undergo decompression within 48 hours of symptom onset have a better prognosis for neurologic recovery than those who undergo decompression after 48 hours. Among patients with urinary incontinence, 1 study indicated that 43% remained incontinent at follow-up visits, but this study included a mix of early and late surgical patients. In another series of 44 patients with acute cauda equina syndrome, chronic bowel and bladder dysfunction were issues for 63% of those for whom surgery was delayed for more than 48 hours after symptom onset.
RECOMMENDED READINGS
McCarthy MJ, Aylott CE, Grevitt MP, Hegarty J. Cauda equina syndrome: factors affecting long-term functional and sphincteric outcome. Spine (Phila Pa 1976). 2007 Jan 15;32(2):207-
[16/. PubMed PMID: 17224816. ](http://www.ncbi.nlm.nih.gov/pubmed/%2017224816)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2017224816)
[Ahn UM, Ahn NU, Buchowski JM, Garrett ES, Sieber AN, Kostuik JP. Cauda equina syndrome secondary to lumbar disc herniation: a meta-analysis of surgical outcomes. Spine (Phila Pa 1976). 2000 Jun 15;25(12):1515-22. PubMed PMID: 10851100. ](http://www.ncbi.nlm.nih.gov/pubmed/%2010851100)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2010851100) [Shapiro S. Medical realities of cauda equina syndrome secondary to lumbar disc herniation. Spine (Phila Pa 1976). 2000 Feb 1;25(3):348-51; discussion 352. PubMed PMID: 10703108. ](http://www.ncbi.nlm.nih.gov/pubmed/10703108)[View ](http://www.ncbi.nlm.nih.gov/pubmed/10703108)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10703108)
QUESTION 3 OF 50
Which of the following is not a clinical sign of rickets?
1
Irritability
2
Frontal bossing
3
Localized bone pain
4
Short stature
5
Enlarged epiphyses
Localized bone pain is not a common finding in rickets. In contrast, in osteomalacia, bone pain is very common. The features of rickets that one should remember include:
* Apathy
* Irritability
* Short stature
* Positive Gowers sign
* Laxity
* Frontal bossing
* RachitiCrosary, Harrisonâs groove enlarged physes
QUESTION 4 OF 50
Figure 12 is the radiograph of a patient with type 2 diabetes, a body mass index of 42, and an Hgb A1c of 8. What is the most appropriate management for this injury?
1
Fracture boot immobilization
2
Casting the ankle in its current position
3
Closed reduction and definitive casting
4
Closed reduction and application of external fixation
5
Open reduction and internal fixation (ORIF)
Several recent studies have shown that while there is an increased risk of complications following ORIF of displaced ankle fractures in diabetic patients compared with nondiabetic patients,the overall risks of treatment are less than that associated with nonsurgical treatment in diabetics. There is also the possibility that ORIF of unstable ankle fractures may forestall the development of Charcot changes in the ankle, although this is not definitively known. Extra rigid fixation may be required because of the patient’s size and poorly controlled diabetes. Nonsurgical management is associated with poorer functional outcomes (due to arthritis secondary to poor reduction of the fracture) and a higher rate of skin breakdown, due to the need for higher skin pressures from the use of highly molded casting used to maintain a closed reduction.
QUESTION 5 OF 50
A 33-year-old woman reports a 3-month history of pain in both feet while running. Examination reveals bilateral point tenderness over the plantar fascia at its origin, and the pain is accentuated when the ankle is dorsiflexed. Management should consist of
1
steroid injection
2
stretching of the heel cord
3
surgical release of the plantar fascia
4
application of a short leg cast for 6 to 8 weeks
5
wearing dorsiflexion night splints
This question refers to plantar fascitis. Heel spurs are noted in approximately 50% of the cases of subcalcaneal pain syndrome. In this patient, diagnosis should rule out lumbar radiculopathy since the symptoms are bilateral.
The most common site for heel pain is where the plantar fascia and intrinsic muscles arise from the medial calcaneal tuberosity on the anteromedial aspect of the heel.
First line treatment is NSAID’s, Physical therapy involving heel cord stretching and an orthosis. Second line therapy after these treatments are unsuccessful involve steroid injection and plaster immobilization. Surgical intervention should be the very last choice in the options given.
QUESTION 6 OF 50
Cathepsin K is an enzyme produced by osteoclasts. What is the function of cathepsin K?
1
Reduction of disulfide bonds in the extracellular matrix
2
Bone resorption
3
Activation of RANK (Receptor activator of nuclear factor kappa-B)
4
Antagonize the action of RANK
5
Absorb water in the extracellular matrix
#
**
Cathepsin K is an enzyme produced and released by osteoclasts at the ruffled border that functions to resorb bone. Cathepsin K inhibitors are being clinically evaluated as potential anti-resorptive drugs for use in osteoporosis treatment. Other proteins associated with osteoclasts include tartrate-resistant acid phosphatase (TRAP) and calcitonin receptor.
Illustration A is a drawing that depicts the action of cathepsin k within osteoclasts.
QUESTION 7 OF 50
A 9-year-old boy with cerebral palsy has trouble sitting. His mother states that whenever his diapers are changed or his hips are moved, he begins to cry. Radiographs demonstrate high dislocations of both femoral heads. The femoral heads have an ovoid shape and superolateral flattening. Recommended treatment is:
1
Botulinum toxin injected into the adductors
2
Bilateral open adductor tenotomy
3
Bilateral femoral osteotomies with acetabuloplasty
4
Bilateral proximal femoral resection
5
Bilateral C olonna arthroplasty
Bilateral proximal femoral resection is the recommended treatment.
Femoral head dislocations may become painful in cerebral palsy at a much earlier age than in nonspastic individuals. Botulinum toxin or adductor tenotomy will not solve the problem.
Replacing the deformed femoral heads into the acetabulum will not achieve the long-term goal of good hip range of motion.
QUESTION 8 OF 50
Which of the following symptoms is least common in patients with osteomyelitis of the pubis:
1
Distal anterior pelviCpain
2
Adductor muscle spasm
3
Rectus muscle spasm
4
Abductor muscle spasm
5
Wide-based waddling gait
Osteomyelitis of the pubiCsymphysis is a rare condition, occurring in 2% to 11% of all patients with osteomyelitis of the pelvis. The osteitis pubis is the least affected area. Signs and symptoms of osteomyelitis of the pubiCsymphysis include distal anterior pelviCpain, adductor and rectus muscle spasms, and a wide-based waddling gait. Fever, leukocytosis, elevated erythrocyte sedimentation rate, and positive blood cultures may also be present. Unilateral rarefaction and sclerosis with cystiCchanges may be seen on radiographs 10 to 14 days after symptoms begin. Radionucleotide scans, computed tomography, and magnetiCresonance imaging may aid in the diagnosis
QUESTION 9 OF 50
While experts disagree whether the postpolio syndrome is caused by a reactivation of the dormant virus or by an attritional aging phenomena of muscles that have been overworked over a period of time, both groups recommend which of the following guidelines for optimizing function in this population?
1
Refrain from exercise.
2
Exercise muscles to exhaustion, but allow 1 day in between exercise sessions to allow the muscles to recover.
3
Exercise muscles to exhaustion, but allow 2 days in between exercise sessions to allow the muscles to recover.
4
Exercise daily at a subexhaustion level.
5
Exercise should be limited to postural and antigravity muscles.
Most leaders in orthopaedic surgery support Jacqueline Perry’s theory that the postpolio syndrome is an attritional degenerative process that is the result of overuse of muscles and joints that are unable to adequately tolerate overload, and have little functional reserve. For that reason, aerobic conditioning and exercise are important. Overload and exhaustion of involved muscles should be avoided.
REFERENCE: Garrett AL: Poliomyelitis, in Nickel VL (ed): Orthopaedic Rehabilitation. New York, NY, Churchill Livingston, 1982, pp 449-458.
QUESTION 10 OF 50
What is the most important factor regarding the risk of recurrent instability in a patient with an acute anterior dislocation of the shoulder?
1
Age of the patient
2
Time from injury to reduction
3
Completion of 3 weeks of immobilization
4
The degree of athletic participation
5
Bilateral instability
The recurrence rate of anterior dislocation of the shoulder after the first episode in athletes younger than age 20 years is thought to be as high as 90%, making surgery after the initial episode a consideration. The rate drops from 50% to 75% in the 20- to 25-year age group and down to 15% in patients older than age 40 years. An excellent prospective study of 257 patients in Sweden showed that there was no difference in those who did or did not complete 3 weeks of immobilization. The study also showed variability among different age groups in the importance of athletic participation; athletes in the 12- to 22-year age group had a higher recurrence rate, whereas the more sedentary patients in the 23- to 29-year age group had a higher rate.
REFERENCES: Hovelius L: The natural history of primary anterior dislocation of the shoulder in the young. J Orthop Sci 1999;4:307-317.
Simonet WT, Cofield RH: Prognosis in anterior shoulder dislocation. Am J Sports Med 1984;12:19-24.
QUESTION 11 OF 50
A 15-year-old athlete collapses suddenly during practice and dies. What is the most likely cause of death?
1
Hypertrophic cardiomyopathy
2
Atrial fibrillation
3
Pulmonary embolism
4
Ruptured aorta
5
Mitral valve prolapse
The number one cause of sudden death in the young athlete is myocardial pathology, with hypertrophic cardiomyopathy being most common. Because of cardiac muscle hypertrophy, the ventricular capacity is diminished and can result in decreased cardiac output. During exertional activities, the increased demand may not be able to be met and leads to sudden death. While the other choices can be the cause of sudden death in an otherwise healthy young athlete, their incidence is even more rare.
REFERENCES: Van Camp SP, Bloor CM, Mueller FO, et al: Nontraumatic sports death in high school and college athletes. Med Sci Sports Exerc 1995;27:641-647.
Maron BJ, Shirani J, Pollac LC, et al: Sudden death in young competitive athletes: Clinical, demographic, and pathological profiles. JAMA 1996;276:199-204.
Mills JD, Moore GE, Thompson PD: The athlete’s heart. Clin Sports Med 1997;16:725-737.
QUESTION 12 OF 50
A patient undergoes open surgical dislocation of the hip to address femoroacetabular impingement. During which stage of the surgical approach is the blood supply to the femoral head at greatest risk? ](http://www.orthobullets.com/anatomy/10123/hip-blood-supply)
1
Release of the piriformis tendon
2
Release of the anteroinferior capsule
3
Release of the posterosuperior capsule
4
Trochanteric osteotomy lateral to the piriformis
5
Anterior dislocation of the femoral head
No detailed explanation provided for this question.
QUESTION 13 OF 50
A 10-year-old patient with Hurler syndrome has undergone a bone marrow transplant and is currently medically stable. He has developed a painful thoracolumbar kyphosis that measures 50° with 25% subluxation T12 on L1. Recommended treatment includes which of the following:
1
Exercise program for the trunk extensor muscles
2
Thoracolumbar orthosis
3
Halo traction followed by orthosis
4
Anterior spinal fusion
5
Anterior and posterior spinal fusion
Anterior and posterior fusion will correct the translation, instability, and ensure a solid fusion. In some cases, posterior fusion alone will suffice if pedicle fixation is good.
Exercises will not correct the subluxation, which is the cause of the pain. A thoracolumbar orthosis is not corrective or well tolerated.
There is no need for halo traction.
Anterior fusion alone is not enough to control this focal instability if the patient is well enough to tolerate a more involved procedure.
QUESTION 14 OF 50
AcryliCbone cement is composed of:
1
A polymer powder and a polymer liquid component
2
A monomer powder and a monomer liquid component
3
A polymer powder and a monomer liquid component
4
A monomer powder and a polymer liquid component
5
Polymethylmethacrylate (PMMA) only
Polymethylmethacrylate (PMMA) is one of the ingredients of acryliCbone cement. The two components of bone cement are a polymer powder component and a monomer liquid component. A blend of ingredients in the polymer and monomer (which includes PMMA) gives cement its unique characteristics
QUESTION 15 OF 50
What is the most common complication after distal biceps tendon repair at the elbow?
1
Lateral antebrachial cutaneous neuritis
2
Radial sensory neuritis
3
Symptomatic heterotopic ossification
4
Rupture of the repair
Cain and associates retrospectively reviewed 198 consecutive surgical repairs of the biceps and noted a 36% overall complication rate, including 26% paresthesia of the lateral antebrachial cutaneous nerve, 6% paresthesia of the sensory branch of the radial nerve, 2% superficial infection, 4% injury to the posterior interosseous nerve, 3% symptomatic heterotopic ossification, and 2% rerupture. Grewal and associates randomized 47 patients to have single-incision repair with two suture anchors and 44 patients to have two-incision transosseous suture repair. They reported that the single-incision technique had a higher rate of transient neurapraxia to the lateral antebrachial cutaneous nerve, affecting 19 of 47 in the suture anchor group and three of 43 in the transosseous group. Also, four reruptures occurred, which appeared to be independent of the repair technique. Recordon and associates found only three complications in their series of 46 patients, 19 having endobutton repair and 27 with transosseous suture repair. They reported two injuries to the lateral antebrachial cutaneous nerve and one case of heterotopic ossification. The review by Banerjee and associates showed one rupture of repair (disengagement of the cortical button), two persistent lesions of the superficial branch of the radial nerve, and one symptomatic heterotopic ossification. Co hen remarked that rerupture of the tendon after repair is uncommon in both one-incision and two-incision techniques. Van den Bogaerde and Shin presented a case of posterior interosseous nerve
incarceration with endobutton repair.
QUESTION 16 OF 50
..A 61-year-old right-hand-dominant woman sustains a fall down 3 stairs, resulting in a left anteroinferior dislocation and noncomminuted greater tuberosity fracture. A closed glenohumeral reduction with intravenous sedation is performed in the emergency department. After reduction, the greater tuberosity fragment remains displaced by 2 mm.
What is the most appropriate treatment?
1
Open reduction internal fixation with transosseous sutures
2
Arthroscopic fixation using a suture bridge technique
3
Nonsurgical treatment with early passive range of motion
4
Nonsurgical treatment with sling immobilization for 4 weeks
DISCUSSION..Greater tuberosity fractures and rotator cuff tears associated with a traumatic dislocation are more commonly seen in women older than age 60. Greater tuberosity fractures that are displaced less than 5 mm in the general population and less than 3 mm in laborers and professional athletes can be treated successfully without surgery. Early passive range of motion is important to avoid the complication of stiffness.
- Nonsurgical treatment with early passive range of motion
QUESTION 17 OF 50
Adolescent girls with multiple radiographs for idiopathic scoliosis are statistically at increased risk for which of the following problems later in life:
1
Lung cancer
2
Breast cancer
3
Lymphoma
4
Leukemia
5
Squamous carcinoma
In a historical cohort study, the risk was increased to 1.7 times the expected rate of breast cancer. The radiation dose is currently lower. The exposure to the breast may be lowered by taking posteroanterior rather than anteroposterior films, and eliminating lateral films in routine situations.
QUESTION 18 OF 50
of 100
A 35-year-old man has a markedly displaced distal radius fracture. An initial sensory examination is intact. He undergoes closed reduction of the fracture with acceptable restoration of alignment and is immobilized in a sugar-tong splint with the wrist in 5 degrees of flexion. Eighteen hours later, he returns to the emergency department with worsening pain and progressive numbness in his thumb and index and long fingers. He now cannot feel pin-prick in that distribution. His forearm is soft, minimally swollen, and nontender. What is the best next step?
1
Admission and observation
2
Fracture repair and carpal tunnel release
3
Fracture repair and fasciotomy
4
Change the sugar tong, placing the wrist in 15-degree extension
Acute carpal tunnel syndrome (CTS) can occur following wrist fracture, dislocation, or with any etiology that causes swelling hemorrhage into the carpal tunnel. It is important to differentiate from the more common chronic CTS; acute CTS is analogous to a compartment syndrome and warrants prompt release to optimize the outcome. Acute CTS can be clinically distinguished based upon the temporal history by progressively worsening pain and numbness, whereas a median nerve contusion causes immediate sensory loss posttrauma without the progression seen in acute CTS. Sometimes pressure measurements can help differentiate between contusions and acute CTS. An injection would be insufficient, and observation would result in a needless delay, increasing the chance for a poorer result. Forearm fasciotomy would not have a role here because the clinical findings indicate acute CTS and not a compartment syndrome of the forearm. The initial position of 5 degrees of flexion is not an extreme position for the nerve, and changing to 15 degrees of extension would not substantially relieve pressure within the carpal tunnel.
RECOMMENDED READINGS
20. Ford DJ, Ali MS. Acute carpal tunnel syndrome. Complications of delayed decompression. J Bone Joint Surg Br. 1986 Nov;68(5):758-9. PubMed PMID: 3782239.
21. Michelsen H, Posner MA. Medical history of carpal tunnel syndrome. Hand Clin. 2002 May;18(2):257-
68/. Review. PubMed PMID: 12371028.
QUESTION 19 OF 50
Injuries to what two structures would result in a “floating shoulder"?
1
Clavicle shaft and humeral shaft
2
Scapular body and humeral shaft
3
Rotator cuff and coracoacromial ligament
4
Clavicle shaft and glenoid neck
The superior shoulder suspensory complex (SSSC) is a bone and soft-tissue ring secured to the trunk by superior and inferior bony struts, from which the upper extremity is suspended. The ring is composed of the glenoid process, coracoid process, coracoclavicular ligaments, distal clavicle, acromioclavicular joint, and acromial process. Double lesions of the SSSC are referred to as “floating shoulder” injuries, as in this case in which the injury involves a fractured scapular neck and ipsilateral clavicle fracture. Ipsilateral acromioclavicular dislocation and coracoid fracture is a less common double disruption of the SSSC. Although several case studies have been published on surgical and nonsurgical management of these injuries, no study provides measurable surgical indications beyond the simple presence of the double lesion. This is often referred to as an unstable shoulder girdle. 47
QUESTION 20 OF 50
of 100
Which surgical approach is most commonly used for this fracture (Figure 32)?
1
Corona mortis
2
Tibial division, sciatic nerve
3
Sciatic nerve, peroneal division
4
Fifth lumbar nerve root
5
Kocher-Langenbeck approach
- Kocher-Langenbeck approach
QUESTION 21 OF 50
..The fracture seen in Figure 17 is most likely associated with injury to what ligamentous structure?
1
Inferior glenohumeral ligament
2
Acromioclavicular (AC) ligaments
3
Coracoclavicular ligaments
4
Coracoacromial ligament
DISCUSSION..The radiograph shows an extra-articular distal clavicle fracture lateral to the clavicular attachment point of the
coracoclavicular ligaments (conoid and trapezoid). However, unlike a scenario featuring a typical Neer type I fracture, the interval between coracoid and clavicle is clearly widened and there is marked fracture displacement. It is clear that the coracoclavicular ligaments must also be torn. The inferior glenohumeral ligament is important to glenohumeral joint stability, but has no effect on the relationship between clavicle and scapula. The AC ligaments are thickenings of the AC joint capsule. They have been shown to be responsible for 90% of anteroposterior stability of the AC joint. The coracoclavicular ligaments are responsible for 77% of stability for superior translation (as in this case). The coracoacromial ligament connects 2 parts of the scapula (coracoids and acromion) and is part of the arch that supports the rotator cuff.
- Coracoclavicular ligaments
QUESTION 22 OF 50
The most common type of chronic inflammatory arthritis in childhood is:
1
Pauciarticular juvenile rheumatoid arthritis
2
Polyarticular juvenile rheumatoid arthritis
3
Systemic juvenile rheumatoid arthritis
4
Seronegative spondyloarthropathy
5
Reactive arthropathy
Forty percent to 60% of children afflicted with juvenile rheumatoid arthritis (JRA) have the pauciarticular subtype. Polyarticular JRA is the second most common type occurring in 30%-40%. Systemic onset JRA is the least common form and occurs in approximately 20% of children. Seronegative spondyloarthropathy is more rare in patients 8 years of age. It is associated with haplotype HLA-B27. The long-term prognosis in these children is generally good.
QUESTION 23 OF 50
of 100
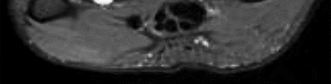
Left shoulder MR imaging results are shown in Figure 19 for a 22-year-old, right-hand-dominant collegiate athlete who reports a 6-month history of weakness in his right arm that first was noticed during weight training. He reports the weakness seems worse now than several months ago. He denies any specific traumatic event, has altered his weight-lifting activities, and has tried over-the-counter ibuprofen without experiencing any benefit. Upon examination of the bilateral upper extremities, there is no appreciable deformity or atrophy. He demonstrates full active shoulder range of motion, and there is no weakness with abduction in the plane of the scapula. Belly press test findings are normal, but there is weakness in external rotation with the arm in adduction. He does not demonstrate anterior apprehension, and there is no instability with load and shift testing. He has normal sensation and pulses to the upper extremity. A standard radiographic shoulder series yields unremarkable results. What is the best surgical option?
1
Arthroscopic labral debridement and biceps tenodesis
2
Shoulder arthroscopy with undersurface cuff debridement and acromioplasty
3
Cyst decompression at the spinoglenoid notch with possible labral repair
4
Cyst decompression at the suprascapular notch with possible labral repair
This patient’s clinical and MR imaging findings are consistent with a posterior paralabral cyst with compression of the suprascapular nerve, specifically at the spinoglenoid notch. Compression of the suprascapular nerve can occur at either the suprascapular or spinoglenoid notch. Compression of the nerve at the suprascapular notch affects innervation to both the supraspinatus and infraspinatus muscles, resulting in weakness in both shoulder abduction and external rotation. However, compression at the spinoglenoid notch only affects innervation to the infraspinatus muscle, resulting in isolated weakness in external rotation.
Compression at the spinoglenoid notch often is seen in overhead athletes, and studies have shown associated posterior labral tears (Piatt and associates). Several studies have addressed nonsurgical and surgical treatment options. The treatment decision should focus on the underlying cause (Martin and associates)—in this patient, the cyst. Nonsurgical treatment in the presence of a known lesion has been associated with a higher failure rate than addressing the lesion, which can result in functional improvement (Chen and associates, Cummins and associates). The best response in this scenario is decompression of the cyst at the spinoglenoid notch with possible labral repair.
RECOMMENDED READINGS
7. [Piasecki DP, Romeo AA, Bach BR Jr, Nicholson GP. Suprascapular neuropathy. J Am Acad Orthop Surg. 2009 Nov;17(11):665-76. Review. PubMed PMID: 19880677.](http://www.ncbi.nlm.nih.gov/pubmed/19880677)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19880677)
8. [Piatt BE, Hawkins RJ, Fritz RC, Ho CP, Wolf E, Schickendantz M. Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg. 2002 Nov-Dec;11(6):600-4. PubMed PMID: 12469086.](http://www.ncbi.nlm.nih.gov/pubmed/12469086)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12469086)
9. [Martin SD, Warren RF, Martin TL, Kennedy K, O'Brien SJ, Wickiewicz TL. Suprascapular neuropathy. Results of non-operative treatment. J Bone Joint Surg Am. 1997 Aug;79(8):1159-65. PubMed PMID: 9278075.](http://www.ncbi.nlm.nih.gov/pubmed/9278075)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9278075)
10. [Chen AL, Ong BC, Rose DJ. Arthroscopic management of spinoglenoid cysts associated with SLAP lesions and suprascapular neuropathy. Arthroscopy. 2003 Jul-Aug;19(6):E15-21. PubMed PMID: 12861219. ](http://www.ncbi.nlm.nih.gov/pubmed/12861219)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12861219)
11. [Cummins CA, Messer TM, Nuber GW. Suprascapular nerve entrapment. J Bone Joint Surg Am. 2000 Mar;82(3):415-24. Review. PubMed PMID: 10724234.](http://www.ncbi.nlm.nih.gov/pubmed/10724234)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10724234)
QUESTION 24 OF 50
A 56-year-old man has had a 2-year history of slowly progressive neck pain and bilateral arm aching.Over the past year, he has noticed intermittent, diffuse numbness in both hands, with decreased grip strength and mild hand clumsiness. He denies any problems with balance. Examination shows a widebased gait, intrinsic ---
wasting, and a postive Hoffman’s sign bilaterally. An MRI scan of the cervical spine is shown in Figure 16. What is the most appropriate treatment?
1
Anterior diskectomy without fusion at C4-C5
2
Epidural injections
3
Anterior diskectomy and fusion at C4-C5 and C5-C6
4
Multilevel laminectomy and fusion
5
Multilevel posterior foraminotomies
The patient has classic symptoms of myelopathy with upper motor neuron signs on examination. His symptoms have been present for years, and are getting worse. The cervical spine MRI scan shows spinal stenosis with multilevel spondylosis causing spinal cord compression at multiple levels. With
the longstanding duration of the patient’s signs and symptoms, combined with involvement of multiple levels in the cervical spine, posterior multilevel laminectomy and fusion is the best treatment option. Two-level anterior diskectomy and fusion would address the two areas of most severe narrowing,but it would fail to decompress the other stenotic areas which also require decompression. Posterior cervical foraminotomies would only address radicular symptoms, which are not present in this patient, and would not succeed in decompression of the spinal cord. Cervical epidural injections are not indicated for myelopathy symptoms, and may in fact place this patient at risk for neurologic deterioration.
QUESTION 25 OF 50
What size tibial insert is associated with easy failure and accelerated osteolysis:
1
6 mm
2
8 mm
3
10 mm
4
12 mm
5
15 mm
Inserts thinner than 6 mm are associated with easy failure and osteolysis, caused by fracture and wear of the polyethylene
QUESTION 26 OF 50
An 82-year-old female sustains a valgus-impacted subcapital femoral neck fracture and undergoes cannulated screw fixation as shown in Figure A. She returns for her first follow-up visit one week later following another fall and now complains of severe hip pain. She is unable to bear weight on the limb, and a new radiograph reveals varus displacement of her fracture. She subsequently undergoes revision fixation but during this procedure, the femoral neck fracture displaces and becomes comminuted. Which is the most appropriate next step in management?
1
Skeletal traction
2
Revision fixation of the femoral neck fracture
3
Hardware removal and placement of a sliding hip screw device
4
Hardware removal and hip arthroplasty
5
Resection hip arthroplasty
In the scenario of an elderly patient with questionable fixation into the femoral head and a non-healed femoral neck fracture, proper treatment is arthroplasty. In a physiologically younger patient, reduction and fixation of the fractures (femoral neck and subtrochanteric, if present) with methods such as a valgus producing osteotomy at the level of the subtrochanteric fracture are
recommended.
Figure A shows cannulated screw fixation of a right femoral neck fracture.
The referenced study by Oakey et al evaluated strength of proximal femurs after cannulated hip screw placement and found that placement of an inverted triangle had a higher ultimate load to failure than placement in a standard triangle format (two screws distal).
QUESTION 27 OF 50
of 100
Figure 50a is the clinical photograph of a 42-year-old woman who has a lesion that has failed prior silver nitrate applications. She experiences frequent bleeding from this lesion. A tissue biopsy performed by a dermatologist revealed capillary hypertrophy with lobular arrangement. Which treatment is most appropriate to minimize recurrence?
1
Sclerotherapy
2
Shave excision with cautery
3
Cryotherapy
4
Wide surgical excision
This lesion is a pyogenic granuloma, which is a common benign vascular lesion that can occur on skin or mucosa. The etiology is unclear, although this lesion tends to occur in areas of physical trauma. Initial treatment with silver nitrate with an average of 1.6 applications has a success rate of 85%. This patient, however, has failed silver nitrate applications. Wide surgical excision is associated with the lowest recurrence rate and offers the benefit of a single procedure. Other options often necessitate repeated procedures to completely eradicate this lesion.
RECOMMENDED READINGS
55. [Quitkin HM, Rosenwasser MP, Strauch RJ. The efficacy of silver nitrate cauterization for pyogenic granuloma of the hand. J Hand Surg Am. 2003 May;28(3):435-8. PubMed PMID: 12772100. ](http://www.ncbi.nlm.nih.gov/pubmed/12772100)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12772100)
56. [Giblin AV, Clover AJ, Athanassopoulos A, Budny PG. Pyogenic granuloma – the quest for optimum treatment: audit of treatment of 408 cases. J Plast Reconstr Aesthet Surg. 2007;60(9):1030-5. Epub 2007 May 2. PubMed PMID: 17478135.](http://www.ncbi.nlm.nih.gov/pubmed/17478135)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17478135)
QUESTION 28 OF 50
Placing the starting point for an antegrade femoral nail too anterior to the axis of the medullary canal can most commonly lead to what intraoperative complication?
1
Nail incarceration
2
Loss of locking screw trajectory into the lesser trochanter
3
Creation of a recurvatum deformity
4
Iatrogenic fracture of the proximal fragment
5
Decrease in hoop stresses
Usage of an anterior starting point that is too anterior leads to creation of significant hoop stresses in the proximal segment, potentially leading to iatrogenic fracture of the proximal segment. The referenced study by Johnson et al reviews the topic of femoral bursting and he notes that even shifting 6mm too far anteriorly can lead to proximal femoral fracture creation. He also reported that overreaming the canal by at least 0.5mm diameter is necessary to decrease hoop stresses throughout the femur, likely due to a mismatch in the radius of curvature of the femur and intramedullary nail.
QUESTION 29 OF 50
A 43-year-old patient presents with pain in the hallux metatarsophalangeal (MP) joint. Motion is limited in dorsiflexion and to some extent in plantarflexion, and mild arthritis is radiographically evident. If a cheilectomy is performed on this patient, what is the primary goal of the procedure in the management of hallux rigidus:
1
To increase the range of motion of the MP joint
2
To remove the osteophytes from the medial and lateral surface of the metatarsal head
3
To decrease the impingement on the terminal branch of the deep peroneal nerve
4
To decrease pain
5
To decrease the likelihood of a subsequent arthrodesis of the MP joint
The goal of cheilectomy is to decrease pain. Although motion may increase, this must not be the goal of surgery because the motion may only be minimally increased. Some patients improve motion markedly after cheilectomy, but this should not be the focus of treatment or promised to the patient.
QUESTION 30 OF 50
The osteoinductive potential of LIM mineralization protein (LMP)-1 gene has been studied for clinical application in:
1
Fracture repair
2
Spinal fusion
3
Cartilage regeneration
4
Ligament healing
5
Meniscal injury
Identification of LMP-1, a novel intracellular protein, is a step forward in osteoinductive proteins. Unlike bone morphogenetiCprotein, which is a secreted protein that binds to cell-surface receptor to initiate a response, LMP-1 is an intracellular signaling molecule. Boden and colleagues transfected bone marrow cells from rats ex vivo with LMP-1 gene using DNA plasmid vector and used them during posterior thoraciCand lumbar spinal fusion in rats
QUESTION 31 OF 50
Which of the following molecules causes the expression of matrix metalloproteinases that can degrade the articular cartilage extracellular matrix:
1
Insulin-dependent growth factor I
2
Transforming growth factor beta
3
Interleukin I
4
Bone morphogenetic protein 2
5
Bone morphogenetic protein 7
Interleukin I has the potential to increase expression of matrix metalloproteinases that can dissolve the extracellular matrix. The other responses are anabolic factors:
Insulin-dependent growth factor I Transforming growth factor beta Bone morphogenetic protein 2
Bone morphogenetic protein 7
QUESTION 32 OF 50
A 40-year-old man who is a manual laborer has had 3 years of worsening medial-sided left knee pain that has inhibited his ability to work. He reports undergoing a left subtotal medial meniscectomy 10 years ago. He has been treated with nonsteroidal anti-inflammatory drugs and two different corticosteroids, with the most recent injection given 1 month ago. Each injection provided him with a few weeks of pain control. His medical history is unremarkable, and he has smoked 20 cigarettes per day for the last 15 years. His BMI is 22. On examination, he has varus alignment of the involved leg and medial joint line tenderness and no lateral or patellofemoral pain. His knee range of motion is 3° shy of full extension to 130° of flexion. He has negative Lachman and posterior drawer test results. He demonstrates no lateral thrust with ambulation. The patient is offered a VPHTO. What aspect of his history will determine the most appropriate VPHTO technique?
1
Prior arthroscopy
2
Current smoking history
3
BMI of 22
4
Age of 40
This patient has a classic presentation of postmeniscectomy medial compartment arthritis. The appropriate diagnostic study is weight-bearing radiographs to confirm the diagnosis. An MRI scan will reveal medial compartment arthritis but will not provide information about alignment. A CT scan would be appropriate to detect an occult fracture; however, this condition is not suspected in this clinical scenario. Ultrasonography can provide information about fluid collection around the knee or a deep vein thrombosis; however, these conditions also are not suspected in this clinical scenario. Because the patient has a correctable deformity (gaps 3 mm with valgus stress), and his symptoms are localized to the involved
compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgical planning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient. A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation, examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not appropriate in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result, current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 years is an indication for HTO _but does not influence technique._
QUESTION 33 OF 50
In a mouse model, if the gene for fibroblast growth factor receptor 3 (FGFR3) is knocked out, which of the following occurs:
1
Marked inhibition of enchondral ossification
2
Absence of bilateral clavicles
3
Marked decrease in sulfate transport into the cells
4
Increased vertebral height and long bone length
5
Defects in limb development and patterning (synpolydactyly)
I. Important facts concerning fibroblast growth factor receptor 3 (FGFR3) physiology and disorders
A. Gain in function mutation results in achondroplasia
1/. Point mutation
2/. Homogenous (single, constant amino acid change)
3/. Receptor is active even without ligand binding
4/. Autosomal dominant
B. Regulates cell growth, proliferation, and differentiation
C . Ligand binding results in phosphorylation of the tyrosine kinase domain
D. Activation of the receptor limits enchondral ossification
E. Deficiency of the receptor results in elongation of the vertebral column and long bones (knockout mice) II. The other responses
A. Runx2 (C baf1) deficiency: C leidocranial dysplasia, absent clavicles
B. Diastrophic dysplasia sulfate transporter gene (DTDST): Transport of sulfate into cells; needed for proteoglycan production
C . Hoxd-13 deficiency: Defects in development and patterning limb, results in synpolydactyly
C orrect Answer: Increased vertebral height and long bone length
QUESTION 34 OF 50
A 70-year-old woman has a preoperative anterior interscalene block prior to undergoing a total shoulder arthroplasty. After seating her in the beach chair position, she becomes acutely hypotensive. What is the most likely cause for the hypotension?
1
Tension pneumothorax
2
Inadvertent epidural injection
3
Inadvertent intravascular injection
4
Laryngeal nerve block
5
Bezold-Jarisch reflex
The beach chair position may cause sudden hypotension and bradycardia as a result of the Bezold-Jarisch reflex. This reflex occurs when venous pooling and increased sympathetic tone induce a low-volume, hypercontractile ventricle, resulting in activation of the parasympathetic nervous system and sympathetic withdrawal. The reported incidence of this phenomenon associated with the sitting position is between 13% to 24%. Left untreated, the result may be cardiac arrest. Pneumothorax or central nervous system toxicity after interscalene block is rare and has an incidence of less than 0.2%. Laryngeal nerve block associated with interscalene nerve block can occur but usually results in hoarseness secondary to ipsilateral vocal cord palsy.
REFERENCES: Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14:546-556.
Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
QUESTION 35 OF 50
All of the following strategies are used to reduce the micromotion between the flexible bone of the femur and a stiff femoral implant except:
1
Providing external porous coatings to the tip of the stem
2
Reducing contact between the tip of the stem and cortical bone
3
Tapering the stem tip
4
Cementing the femoral component
5
Expanding the stem tip so that it compresses on the cortex
Providing external porous coatings to the tip of the stem, reducing contact between the tip of the stem and cortical bone, and tapering the stem tip are strategies that have been used to reduce micromotion. Cementing the femoral component will also reduce micromotion
QUESTION 36 OF 50
A 15-year-old boy has hindfoot pain and very limited subtalar motion. A CT scan reveals a talocalcaneal coalition involving 40% of the middle facet. He has no degeneration of the posterior subtalar facet. Following failure of nonsurgical management, treatment should consist of
1
resection of the coalition with fat graft interposition.
2
Grice extra-articular subtalar arthrodesis.
3
subtalar arthroereisis.
4
intra-articular subtalar fusion.
5
medial sliding calcaneal osteotomy.
The CT scan is an important test to help determine the extent of involvement of the talocalcaneal facet in a talocalcaneal coalition. In a young patient with no arthritis and joint involvement of less than 50%, resection of the coalition and fat pad interposition has been shown to be successful. A calcaneal osteotomy does not address the coalition. Subtalar arthroereisis has been used for treatment of a flexible flatfoot; tarsal coalition patients have a rigid-type flatfoot deformity.
REFERENCES: Sullivan JA: The child’s foot, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 2, pp 1077-1135.
Scranton PE Jr: Treatment of symptomatic talocalcaneal coalition. J Bone Joint Surg Am 1987;69:533-539.
QUESTION 37 OF 50
-Which of the following imaging studies must be obtained for this patient?
1
Duplex scan of both lower extremities
2
MRI scan of the hip
3
Traction internal rotation radiograph of the hip
4
Frog lateral of the hip
5
CT scan of the abdomen and pelvis
No detailed explanation provided for this question.
QUESTION 38 OF 50
A 62-year-old woman has advanced osteoarthritis of the knee that has been refractory to nonsurgical treatment. She wishes to discuss total knee arthroplasty. She reports a lifelong history of intolerance to most jewelry and is concerned about having an allergic reaction to the metallic knee implant.Hypersensitivity to metal implants is usually classified as what type of Gell-Coombs reaction?
1
I (allergic)
2
II (cytotoxic, antibody-dependent)
3
III (immune complex)
4
IV (delayed type)
Most “metal allergy” is classified as type IV, or delayed-type hypersensitivity response, which is a cellmediated response. Types I, II, and III are not generally associated with metal hypersensitivity responses.Type I reactions are typically anaphylaxis. Type II reactions are antibody mediated, such as seen in Grave’s disease or hemolytic anemia. Type III reactions are immune complex diseases such as serum sickness or systemic lupus erythematosus.
QUESTION 39 OF 50
Figure 33 shows the radiograph of a 28-year-old avid golfer who has chronic right wrist pain. Management should consist of
1
cast immobilization.
2
splinting with a bone stimulator.
3
excision of the fracture fragment.
4
arthroscopically assisted percutaneous fixation.
5
trephination of the fibrous union.
The patient’s chronic symptoms are associated with a fracture of the base of the hook of the hamate; therefore, the treatment of choice is simple excision of the fracture fragment, with reasonable expectations of functional return. Acute fractures may be difficult to treat because of the high incidence of nonunion, but once nonunion is discovered, nonsurgical management usually is unsuccessful. Bone grafting may be a surgical alternative, but successful outcomes with percutaneous fixation or trephination of the fibrous union have not been reported.
REFERENCES: Geissler WB: Carpal fractures in athletes. Clin Sports Med 2001;20:167-188.
Rettig ME, Dassa GL, Raskin KB, Melone CP Jr: Wrist fractures in the athlete: Distal radius and carpal fractures. Clin Sports Med 1988;17:469-489.
QUESTION 40 OF 50
Figures 1 through 6 reveal the radiographs and MR images of a 30-year-old man who has a 1-year history
of atraumatic medial-sided left knee pain refractory to nonsurgical measures. What is the most appropriate treatment?
The images illustrate a large unstable osteochondral lesion of the medial femoral condyle. Radiographs and MR images clearly show deep subchondral bone involvement. The appropriate choice of surgery is OCA transplantation, which is indicated for primary treatment of large cartilage lesions, osteochondral lesions, and salvage procedure from failed prior cartilage surgery. Correction of mechanical axis malalignment, ligamentous insufficiency, and meniscal deficiency should also be addressed. ACI alone or an arthroscopic microfracture procedure would not address the bone defect, leaving an uneven articular surface. Although an osteotomy may be a viable choice, a distal femoral varus osteotomy would increase the contact pressure in the medial compartment and worsen the situation. The histologic anatomy of articular cartilage is well described. The superficial layer or lamina splendens contains a small amount of proteoglycan with collagen fibrils arranged parallel to the articular surface. In contrast, the deep zone contains the largest-diameter collagen fibrils, oriented perpendicular to the joint surface, and the highest _concentration of proteoglycans._
QUESTION 41 OF 50
The pathology of the lesion shown in Figures 1 and 2 reveal what cellular pattern?
1
Uniform distribution of stromal cells and giant cells
2
Mixture of mature fat cells and spindle cells
3
Mucin-filled space with occasional spindled fibroblasts
4
Lobular pattern of vascular proliferation with inflammation
No detailed explanation provided for this question.
QUESTION 42 OF 50
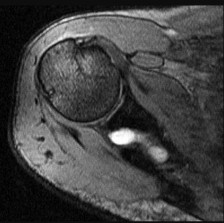
Figure 20 shows the MRI scan of a 20-year-old athlete who has a painful shoulder. This pathology is most commonly seen in
1
baseball pitchers.
2
downhill skiers.
3
football linemen.
4
volleyball players.
5
tennis players.
The MRI scan reveals a posterior labral detachment. This injury is the result of a posteriorly directed force and is common to football players in blocking positions. Although this injury can occur with trauma in all types of athletes, it is seen with relative frequency in football. Treatment is aimed at labral repair with posterior capsulorrhaphy. Both open and arthroscopic techniques can be used.
REFERENCES: Misamore GW, Facibene WA: Posterior capsulorrhaphy for the treatment of traumatic recurrent posterior subluxations of the shoulder in athletes. J Shoulder Elbow Surg 2000;9:403-408.
Mair SD, Zarzour RH, Speer KP: Posterior labral injury in contact athletes. Am J Sports Med 1998;26:753-758.
QUESTION 43 OF 50
of 100
The prognosis for this condition is
1
influenced by the latent time to presentation.
2
generally favorable.
3
variable, with periodic flares and remissions.
4
relatively poor.
This patient has postradiation osteosarcoma of the sacrum after undergoing treatment for pelvic cancer. Examinees should discern that this is a postradiation sarcoma by the imaging findings of an osteoblastic tumor with extraosseous extension arising in the expected radiation field for a patient who was treated with radiation for colorectal cancer 5 years earlier. The histology demonstrates a high-grade sarcoma.
Postradiation sarcomas are treated with chemotherapy and margin-negative surgical resection, but they are associated with a relatively poor prognosis likely attributable to the advanced age of most affected patients and the frequent axial location of these tumors, which can delay diagnosis and make it difficult to obtain an appropriate margin of resection. The imaging reveals a tumor, not an insufficiency fracture or postradiation changes, and the histology shows a sarcoma, not colorectal cancer.
RECOMMENDED READINGS
15. [Mavrogenis AF, Pala E, Guerra G, Ruggieri P. Post-radiation sarcomas. Clinical outcome of 52 Patients. J Surg Oncol. 2012 May;105(6):570-6. doi: 10.1002/jso.22122. Epub 2011 Oct 19. PubMed PMID: 22012601.](http://www.ncbi.nlm.nih.gov/pubmed/22012601)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22012601)
16. [Patel SR. Radiation-induced sarcoma. Curr Treat Options Oncol. 2000 Aug;1(3):258-61. Review. PubMed PMID: 12057168.](http://www.ncbi.nlm.nih.gov/pubmed/12057168)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12057168)
QUESTION 44 OF 50
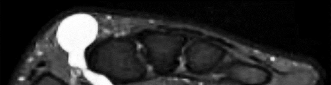
A 24-year-old semiprofessional baseball player has noted increasing medial elbow pain for the past 2 months. This has been associated with a concomitant loss in velocity and control. He denies pain, numbness, or tingling in the hand or digits. Examination demonstrates medial elbow tenderness and swelling. Elbow range of motion is full. There is pain with milking maneuver and valgus stress test. Tinel’s sign is negative over the cubital tunnel, and there is no ulnar nerve subluxation. His MRI scan is shown in Figure
1
After thorough discussion, the player elects to undergo surgical intervention. What surgical variable has been associated with inferior outcomes?
2
Use of palmaris autograft
3
Ulnar nerve transposition
4
Muscle-splitting approach
5
Use of a docking technique
The information and image provided describe a throwing athlete with a complete tear of his ulnar collateral ligament (UCL) of the elbow. Numerous techniques have been described for UCL reconstruction, and at this time, optimal graft choice and fixation methods have not been established. Most studies show no.
major differences in outcome between gracilis autograft palmaris autograft, and allograft. Similarly, no clear advantage has been established when comparing use of bone tunnels with interference screws, tunnels with a docking technique, modified docking techniques, and combination
19
approaches. Use of a muscle-splitting approach, rather than muscle detachment, appears to improve outcomes, with a larger percentage of patients reporting excellent results and a lower rate of postoperative ulnar neuropathy. With regard to the ulnar nerve itself, routine transposition is no longer indicated in patients such as this with no preoperative neurologic symptoms, as limited handling of the nerve is associated with improved patient-reported outcomes and lower rates of postoperative neuropathy
QUESTION 45 OF 50
A 16-year-old boy falls while playing soccer. He reports that his knee buckled when he planted his leg to kick a ball. He noticed an obvious deformity of his knee, which spontaneously resolved with a “clunk.” He could not finish the game but was able to bear weight with a limp. He has had two similar episodes but has never sought medical attention. An initial examination demonstrated an effusion, tenderness at the proximal medial collateral region and medial patellofemoral retinaculum, decreased range of motion, and patella apprehension. A lateral patellar glide performed at 30° of flexion was 3+. He was otherwise ligamentously stable, and there were no other noteworthy findings.Figures 3 and 4 are this patient's proton density fat-saturated MR images. His tibial tubercle-trochlear groove (TT-TG) distance is 12 mm, and he has normal limb-alignment film findings. Treatment at this stage should include
1
hinged knee bracing, protected weight bearing, and physical therapy.
2
anteromedialization of the tibial tubercle.
3
internal fixation and medial patellofemoral ligament (MPFL) reconstruction.
4
arthroscopic lateral retinacular release.
This patient’s examination and history indicate recurrent patellar dislocations. Radiographs show an osseous or osteochondral loose fragment. There is no evidence of an obvious nondisplaced fracture or physeal changes. In the setting of suspected patella dislocation or subluxation with loose fragment seen on radiograph, an MRI is indicated. Lateral release alone is seldom indicated in a knee that is normal before injury. The examination and MRI do not indicate a need for medial collateral ligament repair.
Treatment should consist of arthroscopy or arthrotomy and attempted internal fixation of this fragment. If fixation is not possible, the loose body can be removed. Normal TT-TG values, an increased lateral patellar glide, and a history of recurrent patellar dislocations after trauma suggest MPFL incompetence _and the need for reconstruction._
QUESTION 46 OF 50
Urbaniak and associates reported a success rate of treating osteonecrosis before collapse:
1
10%
2
30%
3
50%
4
70%
5
90%
Urbaniak and associates reported a success rate of 70% with mild collapse and 80% before collapse. Their results have not been duplicated as yet. The results of their study are much better than those reported with fibular graft
QUESTION 47 OF 50
A 32-year-old volleyball player has dull posterior shoulder pain. An examination reveals moderate
external rotation weakness with his arm at his side but normal strength on supraspinatus isolation. Deltoid and supraspinatus bulk appear normal, although there appears to be mild infraspinatus atrophy. Sensation is normal throughout the shoulder and shoulder girdle. What is the most likely diagnosis?
1
Calcified transverse scapular ligament
2
Parsonage-Turner syndrome
3
Spinoglenoid notch cyst
4
Quadrilateral space syndrome
This clinical scenario describes a patient with an isolated injury affecting the infraspinatus muscle. The anatomic location of such a lesion would be at the spinoglenoid notch, at which the suprascapular nerve may be compressed distal to its innervation of the supraspinatus but proximal to the infraspinatus innervation. A calcified transverse scapular ligament would also affect the suprascapular nerve but is proximal to the innervation of both muscles. Quadrilateral space syndrome would affect innervation of the deltoid (and teres minor). Parsonage-Turner syndrome is a more diffuse, and often severely painful, brachial plexus neuropathy.
QUESTION 48 OF 50
What is the preferred treatment for a type CperiprosthetiCfracture with a well-fixed humeral component:
1
Open reduction internal fixation with a plate
2
Long stem prosthesis
3
Strut allograft and cerclage wires
4
Nonoperative treatment
5
Long stem with a strut
In patients with a type CperiprosthetiCfracture (distal to the tip of the prosthesis) and a well-fixed humeral component, the injury can be treated similar to a closed humerus fracture
QUESTION 49 OF 50
full extension.
1
30 degrees of flexion.
2
60 degrees of flexion.
3
90 degrees of flexion.
4
120 degrees of flexion.
DISCUSSION: Tension forces in the healthy, as well as the reconstructed, anterior cruciate ligament were measured and found to be highest with the knee in full extension and decreased as the flexion increased.
Scientific References
: Markolf KL, Burchfield DM, Shapiro MM, et al: Biomechanical consequences of replacement of the anterior cruciate ligament with a patellar ligament allograft. Part II: Forces in the graft compared with forces in the intact ligament. J Bone Joint Surg Am 1996;78:1728-1734.
Beynnon BD, Johnson RJ, Fleming BC, et al: The measurement of elongation of anterior cruciate-ligament grafts in vivo. J Bone Joint Surg Am 1994;76:520-531.
83/. Compared to eumenorrheic athletes, amenorrheic athletes have more frequent occurrences of
QUESTION 50 OF 50
A 65-year-old woman sustains a hip fracture following a minor fall. Which of the following treatments should be considered:
1
A. Hormone replacement therapy
2
Intermittent parathyroid hormone therapy
3
Antiresorptive therapy
4
Prophylactic fixation of the contralateral hip
5
C alcium and vitamin D supplementation and repeat bone mineral density measurement in 1 year
This patient has a new fracture. Because the fracture occurred following minor trauma, the physician should assume that this patient has an insufficiency fracture related to her osteoporosis.
Patients who sustain an osteoporotic hip fracture should be treated with antiresorptive therapy to lower the risk of a subsequent hip or vertebral fracture. A recent randomized trial showed the following:
A large prospective, randomized study showed a reduction in vertebral and nonvertebral fractures when patients were treated with intravenous (IV) zoledronic acid within 90 days of a hip fracture, followed up with annual treatment.
Important points to remember about this study:
Study: Zoledronic acid (5 mg, IV) within 90 days of hip fracture and then annually (1,000 patients in each group) New fractures: 8.6% vs 13.9% (absolute risk reduction, 5.3%; relative risk reduction, 35%)
New fractures
  o   Vertebral: 1.7% vs 3.8% (P = .02)
  o   Nonvertebral: 7.6% vs 10.7% (P = .03)
  o   Hip: 2.0% vs 3.5% (relative risk 30%, not significant)   o   Divergence of fracture-free survival at 12 months
C orrect Answer: Antiresorptive therapy