This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set 6691DD)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
A 9-year-old boy with cerebral palsy has trouble sitting. His mother states that whenever his diapers are changed or his hips are moved, he begins to cry. Radiographs demonstrate high dislocations of both femoral heads. The femoral heads have an ovoid shape and superolateral flattening. Recommended treatment includes:
1
Botulinum toxin injected into the adductors
2
Bilateral open adductor tenotomy
3
Bilateral femoral osteotomies with acetabuloplasty
4
Bilateral proximal femoral resection
5
Bilateral C olonna arthroplasty
Bilateral proximal femoral resection is the recommended treatment.
Femoral head dislocations may become painful in cerebral palsy at a much earlier age than in nonspastic individuals. Botulinum toxin or adductor tenotomy will not solve the problem.
Replacing the deformed femoral heads into the acetabulum will not achieve the long-term goal of good hip range of motion.
QUESTION 2 OF 50
What are the components of the lateral ligament complex of the elbow?
Ulnar collateral ligament (anterior and posterior bands), transverse ligament
The important ligaments on the lateral side of the elbow are thickenings of the capsule. The lateral collateral ligament complex consists of four components: the lateral (radial) collateral ligament (LCL), the LUCL, the accessory LCL, and the annular ligament. The medial collateral ligament complex is a capsular thickening consisting of three components: the anterior band, the posterior band, and the transverse ligament. The LUCL is the most important portion of the lateral ligament in terms of posterolateral rotatory instability. 76
77
78
QUESTION 3 OF 50
of 100
Figure 88a is an anteroposterior pelvis radiograph of a 50-year-old obese man who has right groin pain. He is a former college athlete. Examination reproduces pain with right hip flexion and internal rotation and adduction, and his Stinchfield test result is positive. Figure 88b is a lateral view of his right hip. What is the most likely cause of his hip pain? A B
75
1
Osteonecrosis
2
Obesity
3
Femoroacetabular impingement, Cam type
4
Femoroacetabular impingement, pincer type
The patient’s history and examination is consistent with an intra-articular hip disorder. The radiographs show a large Cam deformity on the anterosuperior femoral neck. Pincer deformities are seen when there is overcoverage of the acetabulum on the femoral head or a deep socket. Femoroacetabular impingement can also occur in cases of acetabular retroversion. The radiographs do not demonstrate these findings. Signs of femoral head collapse and sclerotic lesions are seen in avascular necrosis but are not present here. Obesity plays a role in development of hip arthritis, but its contribution is not fully known and not the major cause of pain in this patient.
RECOMMENDED READINGS
1. [Leunig M, Parvizi J, Ganz R. Nonarthroplasty surgical treatment of hip osteoarthritis. Instr Course Lect. 2006;55:159-66. Review. PubMed PMID: 16958448. ](http://www.ncbi.nlm.nih.gov/pubmed/16958448)[View](http://www.ncbi.nlm.nih.gov/pubmed/16958448)[ ](http://www.ncbi.nlm.nih.gov/pubmed/16958448)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16958448)
2. [Ganz R, Parvizi J, Beck M, Leunig M, Nötzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003 Dec;(417):112-20. Review. PubMed PMID: 14646708. ](http://www.ncbi.nlm.nih.gov/pubmed/14646708)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14646708)
QUESTION 4 OF 50
Which of the following provides the greatest restraint to anterior dislocation of the shoulder:
1
Superior glenohumeral ligament
2
Supraspinatus
3
Infraspinatus
4
Inferior glenohumeral ligament
5
Joint capsule
The inferior glenohumeral ligament provides the greatest restraint to dislocation of the shoulder. The inferior glenohumeral ligament is under the most stress at 90° of abduction with external rotation and extension. Bracing to restrict this position benefits a patient with instability
QUESTION 5 OF 50
Which of the following is true concerning the repair of acute Achilles tendon ruptures:
1
Open treatment has a higher rerupture and infection rate than nonoperative treatment.
2
Open treatment has a higher rerupture rate but lower infection rate compared to nonoperative treatment.
3
Open treatment has a lower rerupture rate but higher infection rate compared to nonoperative treatment.
4
Open treatment has a lower rerupture rate and lower infection rate compared to nonoperative treatment.
5
Open treatment has the same rerupture rate compared to nonoperative treatment.
Slide 1 Slide 2
A 22-year-old man has experienced pain in his foot and ankle for 10 years. His radiographs are presented (Slide 1 and Slide 2). The foot is flexible, and pain is present in the sinus tarsi and along the medial border of the foot. With the subtalar joint held in a reduced neutral position, the forefoot is in 15° of supination. You attempt orthotic arch supports and when these do not
alleviate his pain, a brace is suggested. He refuses to wear a brace. You plan an osteotomy of the calcaneus with lengthening bone graft at the neck of the calcaneus (lateral column lengthening). The most common complication following this procedure is:
1
C alcaneocuboid joint arthritis
2
Subtalar arthritis
3
Persistent sinus tarsi pain
4
Equinus deformity
5
Elevation of the first metatarsal
This patient demonstrates the common finding of fixed forefoot varus associated with a flexible flatfoot deformity. It is likely that a gastrocnemius contracture is also present, but this is not always the case. Arthritis of the calcaneocuboid joint rarely occurs following a lengthening calcaneal osteotomy in an adult. C orrection of the forefoot varus is best accomplished with an opening wedge osteotomy of the medial cuneiform. Arthrodesis of the first tarsometatarsal joint may be performed in selected patients
with noted instability at this joint.
QUESTION 7 OF 50
The disadvantages of a complete arthroscopiCrepair of a rotator cuff include all of the following except:
1
Complete arthroscopiCrepair limits some suture configuration options in the tendon.
2
Postoperative pain is increased.
3
Complete arthroscopiCrepair is technically difficult to perform.
4
Complex instrumentation is required.
5
Operative time is longer.
ArthroscopiCrepair techniques generally require the use of suture anchors and limit some suture configuration options in the tendon. Complete arthroscopiCrepair is technically difficult, requires significantly greater and more complex instrumentation, and has a potentially longer operative time. However, it decreases postoperative pain
QUESTION 8 OF 50
The most common complication of arthrodesis of the proximal interphalangeal (PIP) joint is:
1
C law toe deformity
2
Mallet toe deformity
3
Hammer toe deformity
4
C urly toe deformity
5
Instability of metatarsophalangeal (MP) joint
With arthrodesis of the proximal interphalangeal joint (PIP), the long flexor tendon that remains intact flexes the toe at the metatarsophalangeal (MP) joint and also at the distal interphalangeal (DIP) joint, thus the development of a mallet toe deformity.
QUESTION 9 OF 50
After surgery to the hallux, a patient complains of burning and numbness along the medial aspect of the first metatarsal. The numbness extends from the medial cuneiform distally to the midportion of the first metatarsal and junction of the plantar and dorsal skin. The nerve involved with the pain is the:
The branches of the various sensory nerves of the foot are important to understand. The normal and aberrant topographic anatomy is important in any foot surgery, and management of posttraumatic neuritis is contingent upon an understanding of the anatomy.
QUESTION 10 OF 50
What is the most common complication after distal biceps tendon repair at the elbow?
1
Lateral antebrachial cutaneous neuritis
2
Radial sensory neuritis
3
Symptomatic heterotopic ossification
4
Rupture of the repair
Cain and associates retrospectively reviewed 198 consecutive surgical repairs of the biceps and noted a 36% overall complication rate, including 26% paresthesia of the lateral antebrachial cutaneous nerve, 6% paresthesia of the sensory branch of the radial nerve, 2% superficial infection, 4% injury to the posterior interosseous nerve, 3% symptomatic heterotopic ossification, and 2% rerupture. Grewal and associates randomized 47 patients to have single-incision repair with two suture anchors and 44 patients to have two-incision transosseous suture repair. They reported that the single-incision technique had a higher rate of transient neurapraxia to the lateral antebrachial cutaneous nerve, affecting 19 of 47 in the suture anchor group and three of 43 in the transosseous group. Also, four reruptures occurred, which appeared to be independent of the repair technique. Recordon and associates found only three complications in their series of 46 patients, 19 having endobutton repair and 27 with transosseous suture repair. They reported two injuries to the lateral antebrachial cutaneous nerve and one case of heterotopic ossification. The review by Banerjee and associates showed one rupture of repair (disengagement of the cortical button), two persistent lesions of the superficial branch of the radial nerve, and one symptomatic heterotopic ossification. Co hen remarked that rerupture of the tendon after repair is uncommon in both one-incision and two-incision techniques. Van den Bogaerde and Shin presented a case of posterior interosseous nerve
incarceration with endobutton repair.
QUESTION 11 OF 50
Which of the following is not a factor in the setting time of cement:
1
Storage temperature of bone cement
2
Ambient temperature
3
Handling and kneading of bone cement
4
Use of a cement gun
5
Introducing bone cement in a warm environment
Storage temperature, ambient temperature, handling and kneading of bone cement, and introducing cement in a warm environment are factors of the setting time of cement. Use of a cement gun is not a factor
QUESTION 12 OF 50
A 45-year-old woman with diabetes has a 3-month history of atraumatic left shoulder pain and motion loss. She previously underwent treatment with nonsteroidal anti-inflammatory medication and a home stretching program, experiencing minimal relief of her symptoms. Examination reveals loss of passive external rotation, abduction, and forward elevation without reduction in strength. Radiographs are normal. What is the most appropriate next step?
1
MRI scan with and without contrast
2
Cortisone injection therapy with continued physical therapy (PT)
3
Closed manipulation under anesthesia
4
Arthroscopic release with manipulation under anesthesia
The patient's history and physical exam are consistent with adhesive capsulitis, or frozen shoulder. Adhesive capsulitis is most commonly an idiopathic process that results in joint pain and loss of motion from capsular contracture. It is reported to affect approximately 2% to 5% of the general population, typically affecting middle-age women. Secondary causes include previous trauma, as well as associated medical conditions such as diabetes, stroke, and cardiac and thyroid disease. Debate remains as to whether a genetic predisposition for the development of adhesive capsulitis exists, despite the increased frequency noted in twin studies. Although the underlying etiology and pathophysiology are not well understood, the consensus is that synovial inflammation and capsular fibrosis result in pain and joint volume loss. It is hypothesized that in patients with diabetes, an increased rate of glycosylation and cross-linking of the shoulder capsule raises the incidence of frozen shoulder.
The natural history of adhesive capsulitis is spontaneous resolution, therefore, conservative measures are the mainstay of treatment. As the patient has seen little benefit from NSAIDs and a home exercise program, more aggressive intervention is reasonable. In terms of injections, glenohumeral corticosteroid injection, subacromial corticosteroid injection, and hydrodilation have all 64
demonstrated benefit. Radiographs are usually obtained to exclude other causes of shoulder pain such as glenohumeral arthrosis, malignancy, calcific tendonitis, impingement, and acromioclavicular degeneration. If pain and stiffness persist beyond 6 months, surgical intervention may be considered in the form of closed manipulation or arthroscopic release. Complications of closed manipulation include humerus fracture, glenohumeral dislocation, hematoma, rotator cuff and labral tears, and brachial plexus injury. Arthroscopic release is advocated by some, as it allows for examination of concomitant pathology and controlled release of capsular tissue, with the potential for reduced force when performing the manipulation portion of the procedure. Controversy remains as to whether posterior capsular release should be routinely performed because studies have shown outcomes to be similar with anterior and combined approaches. Therapy should be initiated early after intervention, with some surgeons advocating admission to the hospital with inpatient therapy for pain management and compliance.
QUESTION 13 OF 50
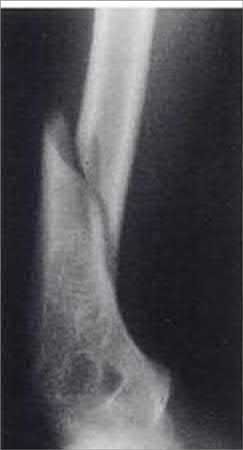
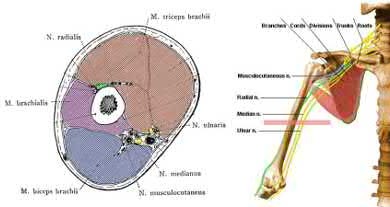
A 68-year-old male sustains the humeral shaft fracture shown in Figures A and B. Upon presentation, he is unable to extend his thumb, fingers, and wrist. After 4 months of non-operative management, the fracture has healed, but his physical exam is unchanged. What is the next most appropriate step in management?
1
EMG and nerve conduction tests followed by possible surgical exploration
2
Continued observation
3
Immediate surgical exploration
4
Shoulder MRI
5
CT scan of the humerus
The clinical presentation is consistent for a residual radial nerve palsy 4 months after a humeral shaft fracture. An EMG is indicated at this time to evaluate the status of the nerve recovery.
A radial nerve injury which occurs during a humeral shaft fracture or after bracing is not an indication for immediate exploration. Most often, the nerve function returns without surgical intervention. An EMG should be performed at 3-5 months to evaluate the status of the nerve recovery. If fasciculations are present, then this represents recovery, and observation should be continued. If fibrillations are present, this represents denervation, and surgical exploration should be considered.
Pollock et al followed 24 humeral-shaft fractures with associated radial-nerve injuries, 2 of which required open exploration and all recovered. They recommend careful observation for return of nerve function and exploration at 3.5-4 months after injury if there is still no clinical or EMG evidence of recovery.
Bostman et al reviewed 59 immediate and 16 secondary radial nerve palsies and no support emerged for routine early exploration in either group.
Figures A and B show an oblique fracture at the junction of the middle and distal 1/3 of the humeral shaft.
Illustration A shows the relative close position of the radial nerve to the humerus at the midlevel of humerus, and why it is at risk with a humerus shaft fracture.
QUESTION 14 OF 50
of 100
Chemotherapy for this condition is
1
contraindicated when pathology is benign.
2
associated with a high risk for subsequent myelodysplastic syndrome.
3
provides dramatic survival benefits.
4
provides modest survival benefits.
This patient has a dedifferentiated liposarcoma within a preexisting atypical lipomatous tumor. The imaging demonstrates a large fatty mass with increased internal septations proximally (the atypical lipomatous tumor) and a solid enhancing mass distally (the dedifferentiated portion). A biopsy reveals a high-grade liposarcoma. The other diagnostic responses do not reflect sarcomatous transformation of the lesion.
Surgical treatment of a high-grade sarcoma involves wide surgical resection. Radiation decreases local recurrence but does not clearly influence overall survival. The role of chemotherapy in high-grade soft-tissue sarcomas remains investigational; there is a modest (8%-15%) associated improvement in overall survival.
Intramuscular lipomas and atypical lipomatous tumors are treated with marginal resection alone. Radiation therapy for soft-tissue sarcomas may be given before or after surgery. When administered before surgery, patients have a higher wound complication rate but better long-term function attributable to lower rates of lymphedema, fibrosis, and contractures.
RECOMMENDED READINGS
1. [Schlieman M, Smith R, Kraybill WG. Adjuvant therapy for extremity sarcomas. Curr Treat Options Oncol. 2006 Nov;7(6):456-63. Review. PubMed PMID: 17032558.](http://www.ncbi.nlm.nih.gov/pubmed/17032558)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17032558)
2. [Yang JC, Chang AE, Baker AR, Sindelar WF, Danforth DN, Topalian SL, DeLaney T, Glatstein E, Steinberg SM, Merino MJ, Rosenberg SA. Randomized prospective study of the benefit of adjuvant radiation therapy in the treatment of soft tissue sarcomas of the extremity. J Clin Oncol. 1998 Jan;16(1):197-203. PubMed PMID: 9440743.](http://www.ncbi.nlm.nih.gov/pubmed/9440743)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9440743)
3. Soft tissue tumors. In: Damron TA, ed. _Orthopaedic Surgery Essentials: Oncology and Basic Science_. Philadelphia, PA: Lippincott Williams and Wilkins; 2008:87-92
QUESTION 15 OF 50
Which of the following is considered a critical element in surgically correcting posttraumatic elbow flexion contractures in adolescents:
1
Lengthening of the biceps muscle
2
Lengthening of the triceps muscle
3
Perioperative indomethacin
4
Pre- or postoperative radiation
5
Postoperative continuous passive motion and physical therapy
Bae and Waters have shown that adolescents with significant posttraumatic elbow flexion contractures can gain an average of 54Â
° of motion with surgical release. They believe postoperative physical therapy and continuous passive motion are considered critical to success of surgical release. Lengthening of the biceps or triceps is not recommended. Measures to prevent postoperative heterotopic ossification did not influence the outcome.
QUESTION 16 OF 50
A 6-year-old boy presents with a Salter-Harris II distal radius fracture 3 weeks after injury. He is nontender and neurologically intact. On radiographs, he has a 35º dorsal angulation. The appropriate course of treatment is:
1
Observe, cast, follow until healed
2
Observe, cast, follow with serial radiographs for at least 2 years
3
C lose reduction and casting
4
C lose reduction and pins
5
Open reduction
For a patient with delayed presentation of a distal radius fracture, appropriate management includes casting and observation for at least 2 years to assess physeal damage and remodeling. The patient may require osteotomy if remodeling does not occur.
QUESTION 17 OF 50
A 5-year-old boy has had a limp for the past 4 weeks with intermittent pain at the foot. He remains normally active and has no history of trauma. He has no fevers, rashes, or swelling. Examination reveals tenderness at the mid-dorsum of the foot medially. Radiographs are seen in Figures la and lb. Treatment should include which of the following?
1
MRI of the foot with gadolinium
2
Open biopsy of the lesion
3
Needle aspiration and culture, followed by antibiotic treatment
4
Observation or an orthotic arch support
5
Steroid injection of the lesion
DISCUSSION: Osteochondrosis of the tarsal navicular is most commonly identified between the ages of 2 and 9 years. The condition is benign and self limited in nature. In patients with severe pain, a period of casting may be warranted, but otherwise management usually consists of observation or a supportive orthotic.
REFERENCES: DiGiovanni CW, Patel A, Calfee R, et al: Osteonecrosis in the foot. J Am Acad Orthop Surg 2007;15:208-217.
Williams GA, Cowell HR: Kohler’s disease of the tarsal navicular. Clin Orthop Relat Res 1981 ;158:53- 58.
**8 • American Academy of Orthopaedic Surgeons**
Figure 2
QUESTION 18 OF 50
A 72-year-old female sustains a displaced proximal humerus fracture after a fall on ice. The patient subsequently undergoes open reduction and internal fixation of her fracture. Of the following answer choices, which correctly orders the predictive accuracy of humeral head ischemia from most to least predictive?
1
calcar length less than 8 mm > humeral head angulation more than 45 degrees > head-split fracture > disrupted medial hinge
2
head-split fracture > calcar length less than 8 mm > disrupted medial hinge
3
humeral head angulation more than 45 degrees
4
disrupted medial hinge > humeral head angulation more than 45 degrees > calcar length less than 8 mm > head-split fracture
5
calcar length less than 8 mm > disrupted medial hinge > humeral head angulation more than 45 degrees > head-split fracture
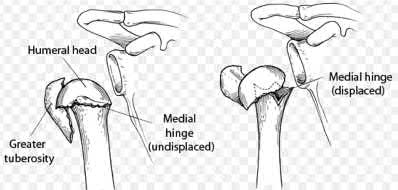
The predictive accuracy of characteristics of humeral head ischemia, from most predictive to least predictive, are: calcar length less than 8 mm, disrupted medial hinge, humeral head angulation more than 45 degrees, and head-split fracture.
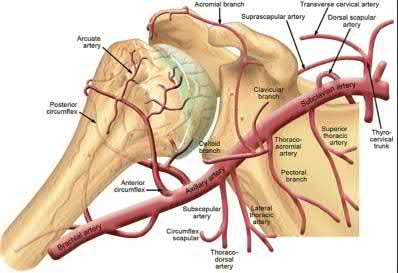
Proximal humerus fractures are the third-most common non-vertebral fracture in the elderly population and represent a treatment challenge for orthopaedic surgeons. Fracture displacement can lead to disruption of the anterior and posterior humeral circumflex arteries, causing humeral head ischemia. Recent evidence has demonstrated that the posterior humeral circumflex artery is likely the main blood supply to the humeral head. The humeral head does have the possibility to revascularize after injury, however, and the presence of humeral head ischemia in the acute injury setting is not a predictor of subsequent avascular necrosis.
Hertel et al. evaluated predictors of humeral head ischemia at the time of surgery in a prospective study of 100 intracapsular proximal humerus fractures. They found the most accurate predictive measures of humeral head ischemia, from most accurate to least accurate, were: a calcar length <8 mm, disruption of the medial hinge, basic fracture pattern, displacement of the humeral head >45 degrees, displacement of the tuberosities >10 mm, glenohumeral dislocation and head-split fractures (equally predictive). The authors concluded that the most relevant predictors of ischemia were the length of the posteromedial calcar, the integrity of the medial hinge, and the basic fracture type.
In a follow-up study, Bastian and Hertel evaluated the occurrence of avascular necrosis in 51 patients whose humeral head vascularity was analyzed at the time of surgery. They found there was no association between acute humeral head ischemia at the time of surgery and the development of avascular necrosis, but the patients who developed collapse of their head had significantly worse clinical outcome scores. The authors concluded that osteosynthesis with preservation of the humeral head is worth considering when adequate reduction can be obtained.
Xu et al. performed a systematic review and meta-analysis of 7 studies with a total of 291 patients to evaluate the risk of avascular necrosis among patients with proximal humerus fractures undergoing operative fixation compared to those who underwent nonoperative management. The authors found no significant differences in the incidence of AVN between the two groups; however, subgroup analysis of the fixation group found that plate fixation was associated with a higher rate of AVN than conservative treatment. The authors concluded that plate fixation was associated with a higher risk of AVN development than conservative treatment.
Illustration A demonstrates the vascular anatomy of the proximal humerus. Illustration B demonstrates differences in posteromedial calcar lengths in
proximal humerus fractures. Illustration C shows the differences between an intact and disrupted medial hinge. Illustration D is an illustration of a head-split fracture.
Answers 1,2,3 and 5: These answers do not correctly order the predictors of humeral head ischemia from most to least accurate.
QUESTION 19 OF 50
A 10-year-old child was referred for spinal curvature and a 2-year history of back pain. She has pain during the day and pain at night that wakes her from sleep and is temporarily relieved with nonsteroidal anti-inflammatory drugs. Examination shows very tight hamstrings and an irritative spinal curvature. Figures 71a through 7Id show radiographs, a bone scan, and a CT scan. What is the most appropriate treatment?
1
Bracing with a thoracolumbosacral orthosis (TLSO)
2
Observation with repeat radiographs of the scoliosis in 3 months and nonsteroidal antiinflammatory drugs for the pain
3
MRI of the neuro-axis
4
Surgical removal
5
Radiofrequency ablation
The history, examination findings, and studies are consistent with an osteoid osteoma. The CT scan shows a classic “target” lesion, and the bone scan has intense uptake at the site of the osteoid osteoma. The child has had a 2-year history of pain that even wakes her from sleep, so observation and anti-inflammatory drugs is not a preferred treatment. Bracing will not help with the discomfort because the pain is not mechanical in nature. MRI would not be needed in addition to the studies already completed. The osteoid osteoma is close to the spinal cord so radiofrequency ablation is not preferred. Surgical removal and biopsy is the treatment of choice.
REFERENCES: Frassica FJ, Waltrip RL, Sponseller PD, et al: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-
574/. Cantwell CP, Obyme J, Eustace S: Current trends in treatment of osteoid osteoma with an emphasis on radiofrequency ablation. Eur Radiol 2004;14:607-617.
Figure 72
QUESTION 20 OF 50
of 100
A diskectomy is performed in which the disk space is not aggressively debrided. When compared to techniques that involve aggressive debridement of the disk space, this results in
1
less intraoperative blood loss.
2
an increased rate of recurrent disk herniation.
3
a shorter length of hospital stay.
4
a higher rate of surgical complications.
This patient has disk herniation at the left L5-S1 level. This will generally affect the traversing S1 nerve. The S1 dermatome is on the lateral aspect and sole of the foot.
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
[PubMed PMID: 24442183. ](http://www.ncbi.nlm.nih.gov/pubmed/24442183)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24442183)
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
[22404142/. ](http://www.ncbi.nlm.nih.gov/pubmed/22404142)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22404142)
[Lee P, Liu JC, Fessler RG. Perioperative results following open and minimally invasive single-level lumbar discectomy. J Clin Neurosci. 2011 Dec;18(12):1667-70. doi: 10.1016/j.jocn.2011.04.004. Epub 2011 Sep 25. PubMed PMID: 21944927. ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[ ](http://www.ncbi.nlm.nih.gov/pubmed/21944927)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21944927)
[Shamji MF, Bains I, Yong E, Sutherland G, Hurlbert RJ. Treatment of Herniated Lumbar Disk by Sequestrectomy or Conventional Diskectomy. World Neurosurg. 2013 Feb 20. pii: S1878-8750(13)00352-5. doi: 10.1016/j.wneu.2013.02.066. [Epub ahead of print] Review. PubMed PMID: 23454687. ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[View ](http://www.ncbi.nlm.nih.gov/pubmed/23454687)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23454687)
[Wang H, Huang B, Li C, Zhang Z, Wang J, Zheng W, Zhou Y. Learning curve for percutaneous endoscopic lumbar discectomy depending on the surgeon's training level of minimally invasive spine surgery. Clin Neurol Neurosurg. 2013 Oct;115(10):1987-91. doi: 10.1016/j.clineuro.2013.06.008. Epub 2013 Jul 2. PubMed PMID: 23830496. ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[View Abstract](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[ ](http://www.ncbi.nlm.nih.gov/pubmed/23830496)[at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23830496)
Soliman J, Harvey A, Howes G, Seibly J, Dossey J, Nardone E. Limited microdiscectomy for lumbar disk herniation: a retrospective long-term outcome analysis. J Spinal Disord Tech. 2014 Feb;27(1):E8-E13. doi: 10.1097/BSD.0b013e31828da8f1. PubMed PMID: 23563332.
[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23563332)
[Radcliff K, Hilibrand A, Lurie JD, Tosteson TD, Delasotta L, Rihn J, Zhao W, Vaccaro A, Albert TJ, Weinstein JN. The impact of epidural steroid injections on the outcomes of patients treated for lumbar disc herniation: a subgroup analysis of the SPORT trial. J Bone Joint Surg Am. 2012 Aug 1;94(15):1353-8. doi: 10.2106/JBJS.K.00341. PubMed PMID: 22739998. ](http://www.ncbi.nlm.nih.gov/pubmed/22739998)[View](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22739998)
QUESTION 21 OF 50
Figures 8a and 8b are the preoperative radiographs of a 47-year-old woman who is being treated for a supple pes plano abductovalgus deformity. She is unable to perform an ipsilateral single leg heel raise. Which of the following is the most likely soft-tissue procedure performed in combination with the bony surgery?
1
Flexor digitorum longus tendon transfer
2
Extensor hallucis longus tendon transfer
3
Spring ligament release
4
Peroneus longus tendon repair
5
Lateral collateral ligament reconstruction
Flexor digitorum longus tendon transfer and augmentation has similar dynamic function to the posterior tibial tendon. Other reported tendon transfers for this procedure include flexor halluces longus and peroneus brevis, but not extensor hallucis longus nor peroneus longus. Spring ligament release accentuates the flatfoot deformity whereas conversely, spring ligament repair/reconstruction is another recognized soft-tissue procedure that may be combined with bony surgery for treatment of flexible acquired flatfoot deformity. Lateral collateral ligament reconstruction addresses lateral ankle instability which the patient does not have.
---
QUESTION 22 OF 50
A 27-year-old male competitive soccer player reports a 1-year history of pain in the adductor region that has prevented him from playing. Examination reveals tenderness about the adductor attachment to the pelvis, and pain at the same site with resisted contraction of the adductors. There is no tenderness over the hip joint and no signs of a sports hernia. Radiographs are normal. MRI does not show any evidence of enthesopathy. What is the next best step in management?
1
Hip arthroscopy
2
Corticosteroid injection
3
Percutaneous adductor tenotomy
4
Bone scan
5
Rheumatology consultation
DISCUSSION: Schilders and associates reported their results of treating adductor-related groin pain in competitive athletes. They reported that a single corticosteroid injection into the pubic cleft can be expected to provide at least 1 year of relief of adductor-related groin pain in a competitive athlete with normal findings on MRI. In contrast, when there is evidence of enthesopathy on MRI in this competitive- athlete population, these injections are not therapeutic and are associated with a high likelihood of recurrence of symptoms. Hip arthroscopy is generally reserved for intra-articular problems. Percutaneous adductor tenotomy is not indicated for this condition. A bone scan is unlikely to provide any useful information for clinical decision-making. Rheumatology consultation is also not indicated in the absence of any evidence of inflammatory arthropathy.
REFERENCES: Schilders E, Bismil Q, Robinson P, et al: Adductor-related groin pain in competitive athletes: Role of adductor enthesis, magnetic resonance imaging, and entheseal pubic cleft injections. J Bone Joint Surg Am 2007;89:2173-2178.
Robinson P, Barron DA, Parsons W, et al: Adductor-related groin pain in athletes: Correlation of MR imaging with clinical findings. Skelet Radiol 2004;33:451-457.
QUESTION 23 OF 50
of 100
A 60-year-old woman is at the emergency department with a one-week history of thoracic back pain along with fevers >103°F. She notes that her legs are becoming slightly numb over the last 24 hours, but she is able to walk normally and she has a normal lower extremity motor examination. Her medical history is significant for diabetes mellitus. Her WBC is 13x109 cells/liter. She would like to avoid surgery. Her T1-weighted post gadolinium MRI scans are shown in Figures 1 and
1
What should you advise her regarding her risks?

2
She is at risk for developing a motor deficit.
3
She is at low risk for developing a motor deficit.
4
She is at low risk for developing a motor deficit if steroids are started immediately.
5
Her WBC count and history of diabetes are not relevant.
■ In a retrospective study of patients with epidural abscess from two academic medical centers, a predictive algorithm was developed to help identify which patients will develop a motor deficit. Multivariate analysis allowed points to be assigned to each risk factor. A sensory deficit was associated with 10 points; urinary retention/incontinence, 8 points; fecal incontinence/retention, 5 points; abscess above the conus medullaris, 4 points; diabetes, 2 points; WBC count >12x109 cells/liter, 2 points, and the presence of multiple epidural abscesses, 4 points. Smoking was not found to be predictive of a motor deficit. A dorsally based abscess was found to be protective of having a deficit, but a ventral or circumferential abscess was not. The use of steroids in the setting of infection is not recommended.
QUESTION 24 OF 50
of 100
Figure 1 is the MRI scan of a patient with cervical spondylotic myelopathy disease. Considering outcome and complications, a surgeon selecting anterior decompression approaches to posterior decompression approaches will see
1
no difference when surgeon discretion used.
2
a higher complication rate.
3
a tendency to treat more diffuse pathology.
4
the approaches are more useful for older patients.
■ The AO Spine Classification Group has initiated a number of prospective studies on the treatment of cervical spondylotic myelopathy. In particular, Fehlings and associates showed that surgeon choice was important in selecting treatment, because the complications and outcomes were similar when comparing anterior to posterior approaches. Previously, studies showed more complications with posterior approaches. Further, anterior approaches are useful for more focal pathology in younger patients.
QUESTION 25 OF 50
Which of the following factors predisposes patients undergoing lateral ankle reconstruction to surgical failure?
1
Low functional demand
2
Anatomic reconstruction
3
Cavovarus foot deformity
4
Planovalgus foot deformity
5
History of acute instability (preoperative)
Bony malalignment such as hindfoot varus, first ray plantar flexion, or cavovarus foot deformity renders patients more susceptible to chronic lateral ankle sprains and can cause failure of isolated lateral ankle reconstruction. Planovalgus foot deformity principally strains the medial ankle ligamentous structures. Low functional demand patients, as well as patients with a preoperative history of acute traumatic ankle instability and patients undergoing anatomic reconstruction all have decreased rates of surgical failure with lateral ankle ligament reconstruction.
QUESTION 26 OF 50
A 21-year-old male is brought to the emergency department after being involved in gang-related violence. A radiograph of his pelvis is shown in Figure A. The patient is hemodynamically stable. Which of the following imaging modalities is the next best step in evaluating this patient for the most common associated injury?
1
Ultrasound bladder to exclude bladder perforation
2
CT abdomen to exclude bowel perforation
3
MRI pelvis to exclude genital injuries
4
CT angiogram exclude laceration of major vessels
5
CT acetabulum to exclude intra-articular foreign body
Low velocity gunshot wounds (GSW) to the hip are most commonly associated with bowel perforation. Consultation with general surgery (or in some facilities, trauma surgery) is necessary to exclude this.
The incidence of GSW is increasing and it is the 2nd leading cause of death in young males in the US after motor vehicle accidents. The incidence of a GSW to the buttock is approximately 8% of all GSW to the extremities. Potential complications of pelvic and acetabular GSW include septic arthritis, enterocutaneous, enteroacetabular, and vesicoacetabular fistulas, infected nonunion, malunion, and injuries to the iliac vessels. The presence or absence of intra-abdominal injuries affects treatment and outcome.
Bartkiw et al. reviewed 2808 GSW and found 1235 associated fractures including 42 fractures of the hip and pelvis. Ten orthopaedic operative
procedures were performed in 7 patients. Associated nonorthopaedic injuries included 15 small/large bowel perforations (36%), 7 vessel lacerations (17%), and 2 urogenital injuries (5%) that required surgery.
Najibi et al. reviewed 39 GSW to acetabulum. They found 32 simple and 7 associated fracture patterns. The most common simple and associated patterns were anterior column and both column, respectively. Bowel injuries were the most common associated injures (42%). Predictors of poor outcome include high-velocity missile, involvement of acetabular dome, abdominal injury, nerve injury, vascular injury, and male gender. Deep infection was associated with primary anastomosis of bowel injury and an associated fracture pattern.
Figure A shows a GSW to the right hip with acetabular fracture and visible bullet fragment.
Incorrect Answers:
Answers 1, 3, 4: Urogenital and vascular injuries are not as common as bowel injuries.
Answer 5: Intraarticular bullet fragments should be removed to prevent lead toxicity (plumbism), which arises from fragments dissolving in synovial fluid. Other reasons for removal include prevention of third body wear, joint sepsis and lead arthropathy. It is not the priority in this case and exclusion of bowel injury must take precedence.
QUESTION 27 OF 50
Operative indications for Dupuytrenâs contracture include:
1
Metacarpophalangeal joint contraction of more than 25º to 30º
2
Proximal interphalangeal joint contracture of 30º or more
3
Palpable cords in the palm
4
Decreased light touch sensation to affected digits
5
Painful palmar nodule
As a general guideline the "table test" is used as an indication for operative intervention. If the patient cannot lay his/her hand flat onto a table, the disease has usually progressed to the point where surgery is required. A metacarpophalangeal joint contracture of 30º to 40º or a proximal interphalangeal joint contracture of 30º or more is an indication for surgery.
QUESTION 28 OF 50
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
1
Inferior glenohumeral ligament
2
Middle glenohumeral ligament
3
Superior labrum
4
Subscapularis tendon
5
Supraspinatus tendon
Subscapularis tears can be associated with disruption of the transverse ligament supporting the biceps. The remaining aspects of the rotator cuff, superior labrum, and capsule can be intact with this injury.
REFERENCES: Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
Gerber C, Sebesta A: Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: A preliminary report. J Shoulder Elbow Surg 2000;9:483-490.
QUESTION 29 OF 50
Figures 1 through 3 are the MRI scans of a 15-year-old boy who sustained an injury to his shoulder after a fall while playing soccer. Following completion of a month-long rehabilitation program, he is able to tolerate sports-specific drills without symptoms. The patient is eager to return to play, as it is mid-season. How should the patient be counseled?
72
1
Patient should not return to play mid-season and should undergo arthroscopic stabilization of the Bankart lesion.
2
Patient may return to play: however, he should be counseled on a moderate risk for recurrence.
3
Patient may not return to play this season, as the patient has evidence of significant glenoid bone loss on MRI scan.
4
Patient may return to play, however, only after a repeat MRI arthrogram confirms interval healing of the Bankart lesion.
Controversy exists regarding optimal treatment of an athlete with a shoulder instability event that has occurred during the competitive season. In the absence of large bony Bankart lesion or significant glenoid or humeral bone loss, particularly in athletes who are not involved in contact sports or throwing, return to sport may be attempted following a course of rehabilitation, provided the patient is asymptomatic following sports-specific drills. However, there is a significant risk of recurrence following nonoperative treatment in patients <20 years, and athletes should be counseled appropriately. Although motion-limiting braces may be associated with subjective improvement in stability, no studies have demonstrated a decreased rate of dislocation associated with bracing.
QUESTION 30 OF 50
Figure 1 is the MRI scan of a 25-year-old left-hand dominant minor league pitcher with a 6 month history of progressive left elbow pain during pitching. He fails nonoperative treatment and undergoes surgery to address the problem. What is the most common complication of this procedure?
1
Ulnar nerve neuropraxia
2
Flexor pronator mass avulsion
3
Posterolateral rotatory instability
4
Symptomatic hardware
The MRI scan shows evidence of a medial collateral ligament (MCL) tear. In a patient with a chronic MCL injury that has failed non-operative treatment, MCL reconstruction would be indicated. Initial MCL reconstruction technique involved routine transposition of the ulnar nerve and detachment of the flexor- pronator mass. Subsequent.
technique modifications have been made to minimize complications by avoiding routine ulnar nerve transposition and performing a muscle-splitting approach. Despite these improvements, transient ulnar nerve neuropraxia remains the most common complication, and patients should be counseled about its occurrence pre-operatively. Flexor pronator mass avulsion is more likely with a muscle-detaching approach, but is not more common than ulnar nerve neuropraxia. Posterolateral rotatory instability is a complication of lateral collateral ligament repair or reconstruction, not medial collateral ligament reconstruction. Symptomatic hardware is not a common complication from this procedure 56
QUESTION 31 OF 50
Figures 1 through 4 are the wrist MR images of a 43-year-old right-hand-dominant bricklayer who reports gradually progressive left hand weakness for 4 months. He describes difficulty gripping objects, tying his shoes, and holding utensils. He denies any numbness, paresthesias, or a previous injury. An examination reveals intact sensation in a median, radial, and ulnar nerve distribution. He has atrophy of hand interossei and a positive Froment sign finding. He has no Tinel sign finding at the wrist or elbow and no exacerbation of symptoms with elbow hyperflexion. Electromyography shows signs of denervation in an ulnar nerve distribution distal to the wrist. What is the best next step?
1
Cubital tunnel release
2
Guyon's canal release
3
Hook-of-hamate excision
4
Excision of the ganglion cyst
The MR images show a lesion consistent with a ganglion cyst located near the hook of the hamate. The ulnar nerve divides into motor and sensory branches just proximal to this lesion. In this case, the ganglion cyst compresses the ulnar nerve motor branch but not the sensory branch, resulting in motor dysfunction but no sensory disturbance. Excision of the ganglion cyst should alleviate his symptoms. Compression of the ulnar nerve proximal to the motor branch take-off (in either the cubital tunnel or proximal Guyon’s canal) would cause both sensory and motor dysfunction. Although chronic nonunion of the hook of the hamate can cause ulnar nerve symptoms, the hook of the hamate appears intact on the MR image. The MR image shows a lesion that is well circumscribed with high intensity on T1 and T2 images, consistent with a benign ganglion cyst, and ganglion cysts are relatively common lesions in this area.
QUESTION 32 OF 50
of 100
A 15-year-old boy is brought to the emergency department after one week of left shoulder pain after lifting weights. He is also complaining of fever, chills, nausea, and fatigue. He appears in distress; his skin is mottled. He decompensates and is transferred to the ICU. Vital signs are temperature of 39.4°C, heart rate 165 bpm, and blood pressure of 80/55. WBC count at admission is 22.4; CRP level is 37.7 mg/dL. Which antibiotic should be started empirically?
1
Vancomycin
2
Clindamycin
3
Ticarcillin-clavulanate
4
Cefazolin
■ The initial antibiotic therapy for suspected methicillin-resistant Staphylococcus aureus (MRSA) infections in patients with sepsis and/or instability is Vancomycin. Clindamycin is useful for first-line therapy in MRSA infections in which the patient is clinically stable, without ongoing bacteremia or intravascular infection. Neither cefazolin nor ticarcillin-clavulanate is appropriate empiric treatment for suspected MRSA.
QUESTION 33 OF 50
of 100
The second-toe deformity is most accurately described as
1
hammer toe.
2
claw toe.
3
curly toe.
4
crossover toe.
- crossover toe.
QUESTION 34 OF 50
..If nonsurgical treatment has failed, what surgical procedure will best reduce the risk for recurrent instability?
1
Diagnostic shoulder arthroscopy with labral repair
2
Diagnostic shoulder arthroscopy with open capsular shift
3
Diagnostic shoulder arthroscopy with coracoid transfer
4
Diagnostic shoulder arthroscopy with thermal capsulorrhaphy
DISCUSSION…If nonsurgical treatment has failed in the revision setting, the amount of bone loss should be quantified. The current standard for quantification of glenoid bone loss is CT scan with or without digital subtraction of the humeral head. An initial diagnostic arthroscopy may permit calculation of glenoid bone loss. The glenoid bare-spot method popularized by Lo and associates provides a reliable estimate of bone loss. Percentage of bone loss is calculated by subtracting the distance from the anterior rim to the bare spot from the posterior rim-bare spot distance divided by twice the posterior rim-bare spot distance. The critical limits of glenoid bone loss are based on a combination of cadaveric and clinical reports. Nonsurgical management may still be a reasonable choice with less than 20% glenoid bone loss in low-demand individuals, patients with high surgical risk secondary to medical comorbidities, and voluntary dislocators. When addressing recurrent anterior instability of the shoulder, it is imperative to assess both soft-tissue and bone injury.
Particular attention must be paid to glenoid and humeral head deficiencies. Patient-specific demands should be considered when discussing treatment options. In a high-demand patient such as this contact athlete, surgical treatment is appropriate. In general, if glenoid bone loss is less than 15%, a soft-tissue stabilization procedure may be all that is necessary. In those with 15% to 25% bone loss, arthroscopic stabilization with bone fragment incorporation may be performed if local bone is available. In the setting of a high-demand patient with no local bone for repair, coracoid transfer, iliac crest bone autograft, or distal tibial allograft is appropriate. With more than 25% bone loss, the glenoid deficiency must be addressed. In this scenario, the athlete demonstrates more than 25% bone loss involving the anteroinferior glenoid. This deficiency must be addressed to restore stability to the glenohumeral joint. In a high-demand patient (contact athlete), augmentation with iliac crest bone graft, distal tibial allograft, or a coracoid transfer procedure is appropriate if local bone is not available.
- CT scan
PREFERRED RESPONSE: 3- Diagnostic shoulder arthroscopy with coracoid transfer
QUESTION 35 OF 50
An 18-year-old man is seen in the office because of back pain in the thoracic region. He has a kyphosis of 65°, a slight wedging in the midthoracic spine, and a Risser sign of 4. Recommended treatment includes:
1
A program of strengthening and stretching exercises
2
A Milwaukee brace
3
A Boston brace
4
A posterior spinal fusion
5
An anterior and posterior spinal fusion
Exercises must be the first treatment for this patient because he is too mature for brace treatment.
Brace treatment is not indicated for someone of this skeletal maturity. Surgery is not indicated unless the patient fails conservative treatment.
QUESTION 36 OF 50
What is the preferred imaging modality to determine the glenoid wear pattern in a patient with rheumatoid arthritis:
1
Plain radiographs
2
Fluoroscopically positioned plain radiographs
3
MagnetiCresonance image
4
Tomograms
5
Computed tomography scan
A computed tomography scan provides important information in regard to the version of the glenoid, wear pattern, amount of wear, glenohumeral subluxation, as well as desired entry point
QUESTION 37 OF 50
of 100
After the patient's wound has healed, which intervention is critical to prevent future ulceration?
1
A well-fitted prosthesis on the left
2
Making sure he wears large shoes to decrease pressure on his feet
3
A bilateral ankle-foot orthoses fitting
4
Custom-molded soft shoe inserts
The most common etiology for plantar ulcers in patients with diabetes is neuropathy; 80% of these patients have adequate vascularity. The pathobiology is increased pressure applied on skin that lacks protective sensation (detected by lack of sensation to Semmes-Weinstein monofilament 5.07). The presence of sensation to light touch is not predictive of ulcer risk, but absent Semmes-Weinstein sensation at 5.07 carries a 30% risk for developing an ulcer. Intact light touch sensation does not rule out loss of protective sensation, and, therefore, does not rule out sensory neuropathy. The grading of an ulcer primarily depends on the existence of deep infection, either an abscess or osteomyelitis. In the presence of deep infection, formal surgical debridement is required. The surgery should be limited to the tissues
that are compromised, without an attempt at primary closure (which increases risk for recurrent infection). Negative-pressure dressings are a significant advance in postsurgical treatment by permitting delayed healing without further surgical intervention. Once healed, the key to preventing recurrent ulceration is the use of orthopaedic shoes with custom-molded soft inserts that accommodate the contours of the feet. This is particularly true when surgery has removed a portion of the foot; the foot otherwise will shift in a shoe that does not include a custom molded insert incorporating a filler that occupies the space left by the surgical resection.
RECOMMENDED READINGS
[Pham H, Armstrong DG, Harvey C, Harkless LB, Giurini JM, Veves A. Screening techniques to identify people at high risk for diabetic foot ulceration: a prospective multicenter trial. Diabetes Care. 2000 May;23(5):606-11. PubMed PMID: 10834417. ](http://www.ncbi.nlm.nih.gov/pubmed/10834417)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10834417) [Pinzur MS, Slovenkai MP, Trepman E, Shields NN; Diabetes Committee of American Orthopaedic Foot and Ankle Society. Guidelines for diabetic foot care: recommendations endorsed by the Diabetes Committee of the American Orthopaedic Foot and Ankle Society. Foot Ankle Int. 2005 Jan;26(1):113-9. PubMed PMID: 15680122. ](http://www.ncbi.nlm.nih.gov/pubmed/%2015680122)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/%2015680122) Chantelau E. Effectiveness of diabetic therapeutic footwear in preventing reulceration: response to Maciejewski et al. Diabetes Care. 2004 Dec;27(12):3024-5; author reply 3025-
[6/. PubMed PMID: 15562237. ](http://www.ncbi.nlm.nih.gov/pubmed/15562237)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/15562237)
QUESTION 38 OF 50
The osteoinductive potential of LIM mineralization protein (LMP)-1 gene has been studied for clinical application in:
1
Fracture repair
2
Spinal fusion
3
Cartilage regeneration
4
Ligament healing
5
Meniscal injury
Identification of LMP-1, a novel intracellular protein, is a step forward in osteoinductive proteins. Unlike bone morphogenetiCprotein, which is a secreted protein that binds to cell-surface receptor to initiate a response, LMP-1 is an intracellular signaling molecule. Boden and colleagues transfected bone marrow cells from rats ex vivo with LMP-1 gene using DNA plasmid vector and used them during posterior thoraciCand lumbar spinal fusion in rats
QUESTION 39 OF 50
A 22-year-old collegiate basketball player presents for treatment of a stress fracture of the base of the fifth metatarsal at the junction of the metaphysis and diaphysis. The fracture was treated operatively, and the patient returned to playing basketball. Three months later, it was apparent that a repeat fracture was present. The fracture was treated with screw removal and a repeat screw fixation. Four months later, after a successful basketball season, he sustained a repeat stress fracture of the metatarsal. On examination, he has a mild cavovarus foot configuration with normal ankle range of motion. Inversion is 15° and eversion is 5°. The base of the fifth metatarsal is prominent. The most likely cause for the repeat fracture is:
1
Abnormal ankle biomechanics
2
C hronic unrecognized ankle instability
3
A varus heel
4
Bone sclerosis of the fifth metatarsal base
5
C hronic avascularity of the fifth metatarsal base
The most common cause of recurrent injury to the fifth metatarsal is unrecognized varus heel deformity. Surgeons must also check for ankle instability, which may be present in this patient. A varus heel, ankle instability, and injury to the fifth metatarsal are associated with recurrent deformity.
QUESTION 40 OF 50
When performing a supracondylar femoral osteotomy, it is recommended to correct the tibiofemoral angle:
1
2°
2
2° to 4°
3
4° to 6°
4
6° to 8°
5
More than 8°
Correcting the tibiofemoral angle between 4° to 6° transfers 80% of the weight to the medial angle
QUESTION 41 OF 50
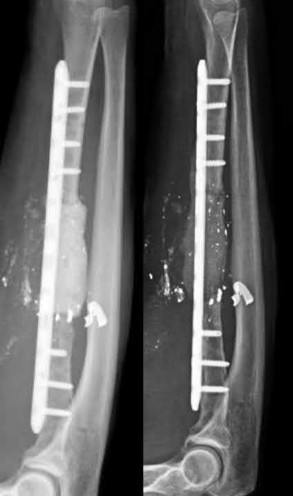
A 37-year-old male presents overnight to your busy trauma hospital after sustaining a gunshot wound to the right forearm. He is neurovascularly intact. Given the bony defect, you decide to proceed with a two-stage Masquelet technique for reconstruction. Which of the following is true with respect to this surgical technique?
1
It is an acceptable method for management of large articular bony defects
2
Iliac crest bone graft (ICBG) has been shown to be superior to reamer irrigator aspirator (RIA) bone grafting
3
The ideal timing of stage 2 reconstruction is 8 weeks after stage 1
4
The induced membrane prevents the resorption of the bone graft placed during stage 2
5
Antibiotics should not be included in the cement spacer due to disruption of pseudomembrane formation
A two-stage Masquelet reconstruction technique may be used to address segmental bone loss such as that in this vignette. The induced membrane formed after the first stage will prevents the resorption of the bone graft placed during the second stage and provide a suitable environment for graft consolidation.
The Masquelet technique is a two-stage method of reconstruction of segmental bony defects resulting from trauma or following debridement of nonviable bone in the setting of infection or non-union. First described by Masquelet in 2000 for the reconstruction of tibial shaft defects, the technique has been expanded for the treatment of other bony defects including the femur, humerus, and forearm. The first stage requires debridement of devitalized or infected bone, followed by filling of the defect with an antibiotic cement spacer and provisional fixation with either external or internal fixation. In cases of infection, the patient would then undergo treatment with culture-specific antibiotics for 6 weeks and then repeat debridement (repeat stage 1) as necessary. During stage 2, the induced membrane or "pseudosynovial vascularized membrane" that forms around the cement spacer is incised and the cement spacer is removed. Autologous bone graft is then harvested (typically from either the femur or iliac crest depending on the size of the defect) and placed into the defect, followed by closure of the membrane, and placement of definitive internal fixation.
Walker et al. performed a retrospective review of 9 patients who underwent the Masquelet technique for bony defects of the forearm. Five of the patients had traumatic defects due to an acute open fracture and the other 4 had nonunions following prior ORIF. The average size of the defect was 4.7 cm. Of the 9 patients, 8 underwent bone grafting with RIA and 1 with ICBG during stage
2/. The authors found that all 9 patients went on to both clinical and radiographic union. They concluded that the Masquelet technique was successful in effectively reconstructing traumatic and posttraumatic bony defects in the forearm with a low incidence of complications.
Azi et al. present a surgical technique article on the Masquelet technique. The authors note that in the setting of infection, the antibiotic specific to the organism from the culture should be added to the cement. In culture-negative or aseptic defects, vancomycin +/- an aminoglycoside was their preferred antibiotic. They also discussed several contraindications to the Masquelet technique to include large osteochondral articular defects, prior irradiation
(given that this would impair adequate pseudomembrane formation), and soft tissue defects not amendable to bony coverage.
Micev et al. review the surgical technique of the Masquelet procedure. The authors noted that at 4 weeks, the induced membrane had the highest expression of vascular endothelial growth factor (VEGF), IL-6, and BMP-2 compared to samples taken at 6, 8 and 12 weeks. They also noted that BMP-2 production peaked at that point and gradually declined over the ensuing month. This led them to conclude that the optimal time of bone grafting to be 4 weeks after the placement of the cement spacer.
Figure A demonstrates a severely comminuted radial shaft fracture with a large bone defect.
Illustration A shows the same patient in Figure A following stage 1 of Masquelet (left) with debridement, placement of a cement spacer and internal fixation; on the right is the same patient following stage 2 with bone grafting.
Incorrect Answers:
Answer 1: The Masquelet technique is not appropriate for large articular defects, which may necessitate other advanced reconstruction techniques such as bulk allograft or prosthetic replacement.
Answer 2: Both femoral RIA and ICBG are the two most commonly used sources of autograft for the second stage of the Masquelet technique, however there is no evidence demonstrating superiority of one over the other.
Answer 3: The optimal timing of stage 2 of the Masquelet technique is 4 to 6 weeks following stage 1, given that this is the time at which the highest amount of BMPs, VEGF and IL-6 are expressed from the induced membrane. Answer 5: While culture-specific antibiotics are recommended for stage 1 in the setting of infected non-union, in the cases of acute bony defects or even aseptic nonunion, this may not be necessary. However antibiotics have not been found to affect pseudomembrane formation.
QUESTION 42 OF 50
Diagnostic work-up concluded that the patient has metastatic lymphoma. He has no neurologic deficit.Based on these findings, what is the most appropriate management for this spinal condition?
1
Cement augmentation
2
En bloc resection
3
Chemotherapy
4
Radiation therapy
5
Intralesional excision
_ _
DISCUSSION FOR QUESTIONS 107 THROUGH 109:
Patients with no prior diagnosis of cancer may present with vertebral lesions. After obtaining initial radiographs, the next most appropriate step is to obtain an MRI with gadolinium. To determine the primary site of the disease, a CT of the chest, abdomen, and pelvis is the next step in establishing a diagnosis. Radiation therapy is the first line of treatment in spinal metastatic disease from lymphoma because it is a highly radiosensitive tumor.
QUESTION 43 OF 50
Which of the following are characteristic signs of PIN palsy:
1
Weakness in finger extension
2
Pain in dorsum of hand
3
Elbow tenderness
4
Weakness in finger extension, and elbow tenderness
5
Weakness in finger extension, elbow tenderness, and pain in dorsum of hand
Painless finger drop is characteristic of posterior interosseous nerve palsy. This syndrome may also involve elbow tenderness in the absence of other clinical findings. Pain in the dorsum of the hand is not associated with this condition because the posterior interosseous nerve contains no sensory component.
QUESTION 44 OF 50
of 100
A 17-year-old male baseball catcher has groin pain and intermittent hip locking. Examination demonstrates reproduction of the pain with hip flexion, internal rotation, and adduction. MR imaging reveals an anterosuperior labral tear.
1
Sclerosis of the proximal femoral epiphysis with subchondral lucency
2
Abnormal femoral head-neck junction offset
3
Widening of the proximal femoral physis with normal femoral head-neck junction offset
4
Absence of the proximal femoral epiphysis secondary ossification center
- Abnormal femoral head-neck junction offset
QUESTION 45 OF 50
of 100 A 51-year-old butcher has an 18-month history of recalcitrant medial elbow pain, which is affecting his occupational demands. He describes the pain as mainly anterior and distal to the medial epicondyle. His symptoms are exacerbated with resisted wrist flexion and forearm pronation. On examination, he is also found to have a positive Tinel’s sign at the elbow with weakness of intrinsic strength. He has attempted physical therapy, activity modification, bracing, and anti-inflammatory medication without any significant improvement. Presurgical counseling should include the understanding that
1
concomitant ulnar neuropathy is a potential poor prognostic factor.
2
a change in occupation will likely be required after surgery.
3
weakness in wrist flexion strength will result postoperatively.
4
prior corticosteriod injections are a potential poor prognostic factor.
DISCUSSION:
Although less common in comparison with lateral elbow tendinopathy, medial elbow tendinopathy remains a significant cause of elbow disability. Fortunately, most patients can anticipate resolution of symptoms with nonsurgical management. For patients with recalcitrant symptoms, surgical intervention should be discussed as a treatment alternative. The literature reports successful results with surgical intervention via debridement
of pathologic tissue, release of the flexor carpi radialis - pronator teres origin, and/or repair of the flexor carpi radialis - pronator teres origin. Several authors have raised concern of the impact of concomitant ulnar neuropathy on results following surgical treatment for medial epicondylitis. Kurvers and Verhaar and Gabel and Morrey, among others, have reported a statistically significant association between concomitant ulnar neuropathy and worse outcomes following surgery. Most patients can anticipate a return to prior activity levels after surgery without any consistently reported loss of flexor/pronator strength. Prior corticosteroid injections
have not been found to impact results.
QUESTION 46 OF 50
The daily elemental calcium requirement for a lactating woman is:
1
500 mg to 700 mg
2
750 mg
3
1,200 mg
4
1,500 mg
5
2,000 mg
The guidelines for the daily elemental calcium requirement are as follows:
Children 500 mg to 700 mg
Growth spurt to young adult
(10 to 25 years of age)
1,300 mg
Adult male 750 mg
Adult female
Postmenopausal Elderly Pregnancy Lactation
  Â
1,500 mg
1,200 mg
1,500 mg
2,000 mg
Note: 1 daily equivalent = 250 mg elemental calcium (one glass of milk) Correct Answer: 2,000 mg
QUESTION 47 OF 50
Which of the following describes the inheritance pattern of Marfanâs syndrome:
1
Autosomal recessive
2
Autosomal dominant
3
X-linked recessive
4
X-linked dominant
5
Sporadic
Structural defects are usually transmitted by an autosomal-dominant pattern. In contrast, with metabolic or enzyme deficiencies, the condition is usually transmitted in an autosomal-recessive pattern.
Remember the major autosomal-dominant conditions: Achondroplasia
Spondyloepiphyseal dysplasia
Multiple epiphyseal dysplasia
Marfan's syndrome Ehlers-Danlos syndrome Osteogenesis imperfecta (I, IV) Multiple hereditary exostosis Polydactyly
QUESTION 48 OF 50
A 78-year-old woman undergoes a reverse total shoulder arthroplasty for cuff tear arthropathy. Her preoperative, 3-month postoperative, and
1
year postoperative radiographs are shown in Figures 1 through
2
What is the cause of the radiographic finding seen here?
17
3
Glenoid component malposition
4
Humeral component malposition
5
Over tensioning of the deltoid
The patient underwent a reverse arthroplasty for cuff tear arthropathy. Her preoperative radiograph shows some superior glenoid wear, which was not corrected at the time of surgery. This has resulted in superior tilt to the glenosphere, which has been identified as a risk factor for scapular notching. This occurs as a result of mechanical impingement between the medial humerus and scapular neck during arm adduction. The Beta angle and reverse shoulder angle have been proposed as measurements that can help identify pathologic glenoid tilt preoperatively. Risk factors for scapular notching include superior tilt of the glenosphere, superior placement of the glenoid baseplate on the glenoid, a 155° humeral implant angle, and incomplete lateralization of the construct.
The humeral component appears well-positioned in this radiograph. Over tensioning of the deltoid and excessive humeral lateralization would risk an acromial stress fracture and could limit shoulder range of motion. This is an inlay humeral stem, which does not lateralize the humerus.
QUESTION 49 OF 50
Scoliosis in Marfan syndrome is characterized by which of the following:
1
Scoliosis curves are more likely to begin in the juvenile period.
2
There is an increased likelihood of left thoracic curves.
3
Brace treatment is more likely to be successful because of the flexibility.
4
Patients are less likely to have back pain.
5
C urves are more likely to be stable in adulthood.
Scoliosis curves are much more likely to begin in the juvenile period than idiopathic scoliosis.
There is no significant difference in the likelihood of left thoracic curves in Marfan syndrome. Brace treatment is less likely to be successful in Marfan syndrome than in idiopathic scoliosis. Marfan patients with scoliosis are more likely to have back pain.
Marfan curves are more likely to progress in adulthood.
QUESTION 50 OF 50
What factor is considered one of the early changes in osteoarthritic cartilage?
1
Decreased water content
2
Increased proteoglycan content
3
Decreased loading of the solid matrix
4
Increased cartilage tissue permeability
The normal regulation of a cartilage surface is a delicate balance of degradation and synthesis. When this normal regulation of the cartilage is disturbed, a proinflammatory state tips the cellular pathway in the direction of degradation. The proinflammatory state upregulates the production of cytokines and proteolytic enzymes, specifically matrix metalloproteinases. These enzymes attack the proteoglycan content of the cartilage, leading to an overall reduction in the proteoglycan content. This reduction in content leads to increased permeability of the cartilage substrate. With increased permeability, water is able to move into the cartilage itself, thereby increasing the overall water content within the cartilage in an arthritic state. Finally, because of the increased permeability and increased water content, the overall load or pressure placed on the underlying solid matrix is increased. Increased water content, decreased proteoglycan content, and an increased load on the solid matrix are typical of an osteoarthritic process within normal cartilage. Therefore, the only correct option is that the cartilage has an increased amount
of permeability in osteoarthritis.