Score: 0%
Advanced Orthopedic Mock Exam (Set 407640)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks.
Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
Figure 7 shows the radiograph of an 18-year-old hockey player who sustained a shoulder injury during a fall into the side boards. Examination reveals a significant prominence at the acromioclavicular joint. Management should consist of
1
a figure-of-8 clavicle strap.
2
a sling for comfort, followed by early range-of-motion and strengthening exercises.
3
open reduction and stabilization.
4
immobilization in a spica cast.
5
resection of the distal clavicle.
The radiograph shows a type V acromioclavicular separation with greater than 100% superior elevation of the clavicle. This finding implies detachment of the deltoid and trapezius from the distal clavicle. Because of severe compromise of function and potential compromise to the overlying skin, surgery is the treatment of choice for type V acromioclavicular separations. During reduction and repair, meticulous repair of the deltotrapezial fascia will also aid in securing the repair.
REFERENCES: Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocations. Am J Sports Med 1995;23:324-331.
REFERENCES: Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocations. Am J Sports Med 1995;23:324-331.
QUESTION 2 OF 50
In a mouse model, if the gene for fibroblast growth factor receptor 3 (FGFR3) is knocked out, which of the following occurs:
1
Marked inhibition of enchondral ossification
2
Absence of bilateral clavicles
3
Marked decrease in sulfate transport into the cells
4
Increased vertebral height and long bone length
5
Defects in limb development and patterning (synpolydactyly)
I. Important facts concerning fibroblast growth factor receptor 3 (FGFR3) physiology and disorders
A. Gain in function mutation results in achondroplasia
1/. Point mutation
2/. Homogenous (single, constant amino acid change)
3/. Receptor is active even without ligand binding
4/. Autosomal dominant
B. Regulates cell growth, proliferation, and differentiation
C . Ligand binding results in phosphorylation of the tyrosine kinase domain
D. Activation of the receptor limits enchondral ossification
E. Deficiency of the receptor results in elongation of the vertebral column and long bones (knockout mice) II. The other responses
A. Runx2 (C baf1) deficiency: C leidocranial dysplasia, absent clavicles
B. Diastrophic dysplasia sulfate transporter gene (DTDST): Transport of sulfate into cells; needed for proteoglycan production
C . Hoxd-13 deficiency: Defects in development and patterning limb, results in synpolydactyly
C orrect Answer: Increased vertebral height and long bone length
A. Gain in function mutation results in achondroplasia
1/. Point mutation
2/. Homogenous (single, constant amino acid change)
3/. Receptor is active even without ligand binding
4/. Autosomal dominant
B. Regulates cell growth, proliferation, and differentiation
C . Ligand binding results in phosphorylation of the tyrosine kinase domain
D. Activation of the receptor limits enchondral ossification
E. Deficiency of the receptor results in elongation of the vertebral column and long bones (knockout mice) II. The other responses
A. Runx2 (C baf1) deficiency: C leidocranial dysplasia, absent clavicles
B. Diastrophic dysplasia sulfate transporter gene (DTDST): Transport of sulfate into cells; needed for proteoglycan production
C . Hoxd-13 deficiency: Defects in development and patterning limb, results in synpolydactyly
C orrect Answer: Increased vertebral height and long bone length
QUESTION 3 OF 50
A 19-year-old man sustains a low-velocity gunshot wound to the forearm. What
factor most strongly correlates with the development of compartment syndrome
after this injury?
factor most strongly correlates with the development of compartment syndrome
after this injury?
1
Fracture comminution
2
Fracture of both the radius and ulna
3
Fracture of the proximal third of the forearm
4
Fracture displacement of more than 10 mm
5
Retained bullet fragments
In a multivariate analysis, the strongest factor for the development of compartment syndrome is fracture of the proximal third of the forearm. However, compartment syndrome can still occur without a fracture. Therefore, these patients should be followed with a high level of suspicion for the development of compartment syndrome.
REFERENCES: Moed BR, Fakhouri AJ: Compartment syndrome after low-velocity gunshot wounds to the forearm. J Orthop Trauma 1991;5:134-137.
Hahn M, Strauss E, Yang EC: Gunshot wounds to the forearm. Orthop Clin North Am 1995;26:85-93.
REFERENCES: Moed BR, Fakhouri AJ: Compartment syndrome after low-velocity gunshot wounds to the forearm. J Orthop Trauma 1991;5:134-137.
Hahn M, Strauss E, Yang EC: Gunshot wounds to the forearm. Orthop Clin North Am 1995;26:85-93.
QUESTION 4 OF 50
Examination of an 18-year-old professional soccer player who was forcefully kicked across the shin while attempting a slide tackle reveals a marked effusion and limited motion of the knee. The tibia translates 12 mm posterior to the femoral condyles when the knee is held in 90 degrees of flexion. There is no posteromedial or posterolateral instability. Management should consist of
1
early reconstruction of all injured structures.
2
knee immobilization in 30 degrees of flexion for 2 to 4 weeks.
3
knee immobilization in full extension for 2 to 4 weeks.
4
protected weight bearing and intense hamstring strengthening.
5
no weight bearing, followed by a gradual return to sports.
The patient has an acute grade III posterior cruciate ligament injury. The majority of grade I and II injuries can be treated with protected weight bearing and quadriceps rehabilitation, and most patients can return to sports within 2 to 4 weeks. In contrast, grade III injuries require immobilization in full extension for 2 to 4 weeks to protect the posterior cruciate ligament and the other posterolateral structures presumed to be damaged. The mainstay of postinjury rehabilitation for all posterior cruciate ligament injuries is quadriceps strengthening exercises, which have been shown to counteract posterior tibial subluxation.
REFERENCES: Miller MD, Bergfeld JA, Fowler PJ, Harner CD, Noyes FR: The posterior cruciate ligament injured knee: Principles of evaluation and treatment. Instr Course Lect 1999;48:199-207.
Posterior Cruciate Ligament Injuries in Principles and Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott, Williams and Wilkins, 2000.
REFERENCES: Miller MD, Bergfeld JA, Fowler PJ, Harner CD, Noyes FR: The posterior cruciate ligament injured knee: Principles of evaluation and treatment. Instr Course Lect 1999;48:199-207.
Posterior Cruciate Ligament Injuries in Principles and Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott, Williams and Wilkins, 2000.
QUESTION 5 OF 50
of 100
What is the most common complication following distal biceps tendon repair?
What is the most common complication following distal biceps tendon repair?
1
Posterior interosseous nerve palsy
2
Rerupture of the repair
3
Lateral antebrachial cutaneous neuropraxia
4
Superficial radial sensory neuropathy
The distal biceps tendon is commonly torn with an eccentric contraction of the biceps when the elbow is taken into extension. Patients treated nonsurgically will note loss of at least 50% supination strength and may develop discomfort with resistive activities. The video shows the squeeze test to evaluate the integrity of the biceps tendon. The test is similar to the Thompson test in the evaluation of an Achilles tendon rupture. The distal arm is squeezed with the elbow flexed 60 to 80 degrees and the forearm pronated. By shortening the musculotendinous unit, the intact biceps tendon will lead to forearm supination. If the biceps is torn, the forearm will not supinate as shown in the video. The maneuver is performed with the elbow in flexion to minimize tension on the brachialis muscle and isolate the biceps. Ruland and associates evaluated 25 patients with suspected distal biceps ruptures and correctly diagnosed all but 1 false-positive result that involved a partial tear. The lacertus fibrosus is not evaluated with this maneuver.
When considering a repair, a 1- or 2-incision technique may be performed. Chavan and associates performed a systematic review comparing the 2 techniques and reported similar complication rates. The 2-incision technique was associated with more instances of significant loss of forearm rotation and more unsatisfactory clinical results. The 1-incision technique is associated with a higher incidence of lateral antebrachial cutaneous neuropathy likely attributable to retraction. The biceps insertion is a thin semilunar area on the posterior/ulnar aspect of the radial tuberosity centered at approximately 30 degrees anterior to the lateral/coronal plane with the arm fully supinated. Forthman and associates used CT scan to asses 30 cadaveric specimens and noted that the biceps tuberosity orientation would prohibit an anatomic repair in 35% of arms for which the 1-incision technique was used.
Mazzocca and associates reported the highest load to failure of the Endobutton (440 newton (N)) compared to fixation with suture anchor (381 N), Wartenberg syndrome (310 N), and an interference screw (232 N). Greenberg and associates noted greater load to failure for the Endobutton (584 N) compared to suture anchor (254 N) and transosseous tunnel (178 N) constructs. Spang and associates reported comparable strength of the Endobutton repair when compared to suture anchors. Fifty N of force is required to hold the elbow flexed at 90 degrees against gravity, which is well below the strength of the repairs studied.
Neuropraxia of the lateral antebrachial cutaneous nerve branch is the most common complication associated with distal biceps repair, with a reported incidence as high as 40%. The nerve branch lies between the biceps and brachialis as it crosses the surgical field in the antecubital fossa. The neuropathy may be related to aggressive retraction, particularly when using the 1-incision technique, and often resolves with time. Cain and associates reported minor complications were common (but major complications uncommon) following distal biceps repair. Reported complications are lateral antebrachial cutaneous paresthesia (26%), radial sensory nerve paresthesia (6%), posterior interosseous nerve injury (4%), and rerupture (2%).
RECOMMENDED READINGS
1. Ruland RT, Dunbar RP, Bowen JD. The biceps squeeze test for diagnosis of distal biceps tendon ruptures. Clin Orthop Relat Res. 2005 Aug;(437):128-31. PubMed PMID: 16056039.
2. Forthman CL, Zimmerman RM, Sullivan MJ, Gabel GT. Cross-sectional anatomy of the bicipital tuberosity and biceps brachii tendon insertion: relevance to anatomic tendon repair. J Shoulder Elbow Surg. 2008 May-Jun;17(3):522-6. doi: 10.1016/j.jse.2007.11.002. Epub 2008 Mar 6. PubMed PMID: 18325797.
3. Chavan PR, Duquin TR, Bisson LJ. Repair of the ruptured distal biceps tendon: a systematic review. Am J Sports Med. 2008 Aug;36(8):1618-24. doi: 10.1177/0363546508321482. Review. PubMed PMID: 18658024.
4. Mazzocca AD, Burton KJ, Romeo AA, Santangelo S, Adams DA, Arciero RA. Biomechanical evaluation of 4 techniques of distal biceps brachii tendon repair. Am J Sports Med. 2007 Feb;35(2):252-
8/. Epub 2006 Dec 27. PubMed PMID: 17192318.
5. Cain RA, Nydick JA, Stein MI, Williams BD, Polikandriotis JA, Hess AV. Complications following distal biceps repair. J Hand Surg Am. 2012 Oct;37(10):2112-7. doi: 10.1016/j.jhsa.2012.06.022. Epub 2012 Aug 30. PubMed PMID: 22938802.
6. Greenberg JA, Fernandez JJ, Wang T, Turner C. EndoButton-assisted repair of distal biceps tendon ruptures. J Shoulder Elbow Surg. 2003 Sep-Oct;12(5):484-90. Erratum in: J Shoulder Elbow Surg. 2005 Mar-Apr;14(2):231. PubMed PMID: 14564273.
7. Spang JT, Weinhold PS, Karas SG. A biomechanical comparison of EndoButton versus suture anchor repair of distal biceps tendon injuries. J Shoulder Elbow Surg. 2006 Jul-Aug;15(4):509-14. PubMed PMID: 16831659.
When considering a repair, a 1- or 2-incision technique may be performed. Chavan and associates performed a systematic review comparing the 2 techniques and reported similar complication rates. The 2-incision technique was associated with more instances of significant loss of forearm rotation and more unsatisfactory clinical results. The 1-incision technique is associated with a higher incidence of lateral antebrachial cutaneous neuropathy likely attributable to retraction. The biceps insertion is a thin semilunar area on the posterior/ulnar aspect of the radial tuberosity centered at approximately 30 degrees anterior to the lateral/coronal plane with the arm fully supinated. Forthman and associates used CT scan to asses 30 cadaveric specimens and noted that the biceps tuberosity orientation would prohibit an anatomic repair in 35% of arms for which the 1-incision technique was used.
Mazzocca and associates reported the highest load to failure of the Endobutton (440 newton (N)) compared to fixation with suture anchor (381 N), Wartenberg syndrome (310 N), and an interference screw (232 N). Greenberg and associates noted greater load to failure for the Endobutton (584 N) compared to suture anchor (254 N) and transosseous tunnel (178 N) constructs. Spang and associates reported comparable strength of the Endobutton repair when compared to suture anchors. Fifty N of force is required to hold the elbow flexed at 90 degrees against gravity, which is well below the strength of the repairs studied.
Neuropraxia of the lateral antebrachial cutaneous nerve branch is the most common complication associated with distal biceps repair, with a reported incidence as high as 40%. The nerve branch lies between the biceps and brachialis as it crosses the surgical field in the antecubital fossa. The neuropathy may be related to aggressive retraction, particularly when using the 1-incision technique, and often resolves with time. Cain and associates reported minor complications were common (but major complications uncommon) following distal biceps repair. Reported complications are lateral antebrachial cutaneous paresthesia (26%), radial sensory nerve paresthesia (6%), posterior interosseous nerve injury (4%), and rerupture (2%).
RECOMMENDED READINGS
1. Ruland RT, Dunbar RP, Bowen JD. The biceps squeeze test for diagnosis of distal biceps tendon ruptures. Clin Orthop Relat Res. 2005 Aug;(437):128-31. PubMed PMID: 16056039.
2. Forthman CL, Zimmerman RM, Sullivan MJ, Gabel GT. Cross-sectional anatomy of the bicipital tuberosity and biceps brachii tendon insertion: relevance to anatomic tendon repair. J Shoulder Elbow Surg. 2008 May-Jun;17(3):522-6. doi: 10.1016/j.jse.2007.11.002. Epub 2008 Mar 6. PubMed PMID: 18325797.
3. Chavan PR, Duquin TR, Bisson LJ. Repair of the ruptured distal biceps tendon: a systematic review. Am J Sports Med. 2008 Aug;36(8):1618-24. doi: 10.1177/0363546508321482. Review. PubMed PMID: 18658024.
4. Mazzocca AD, Burton KJ, Romeo AA, Santangelo S, Adams DA, Arciero RA. Biomechanical evaluation of 4 techniques of distal biceps brachii tendon repair. Am J Sports Med. 2007 Feb;35(2):252-
8/. Epub 2006 Dec 27. PubMed PMID: 17192318.
5. Cain RA, Nydick JA, Stein MI, Williams BD, Polikandriotis JA, Hess AV. Complications following distal biceps repair. J Hand Surg Am. 2012 Oct;37(10):2112-7. doi: 10.1016/j.jhsa.2012.06.022. Epub 2012 Aug 30. PubMed PMID: 22938802.
6. Greenberg JA, Fernandez JJ, Wang T, Turner C. EndoButton-assisted repair of distal biceps tendon ruptures. J Shoulder Elbow Surg. 2003 Sep-Oct;12(5):484-90. Erratum in: J Shoulder Elbow Surg. 2005 Mar-Apr;14(2):231. PubMed PMID: 14564273.
7. Spang JT, Weinhold PS, Karas SG. A biomechanical comparison of EndoButton versus suture anchor repair of distal biceps tendon injuries. J Shoulder Elbow Surg. 2006 Jul-Aug;15(4):509-14. PubMed PMID: 16831659.
QUESTION 6 OF 50
Figures 1 and 2 show the clinical photograph and radiograph obtained from a 62-year-old man who has deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?
51
51
1
A Vancouver type B1 fracture
2
Residual leg-length discrepancy
3
Loosening and subsidence of the femoral stem into anteversion
4
Loosening and subsidence of the femoral stem into retroversion
Figure 1 reveals an external rotation deformity of the right lower extremity. This deformity can have numerous causes, including extra-articular deformity. Figure 2 reveals a loose, subsided femoral component. Femoral stems typically subside into retroversion due to proximal femoral biomechanics, which cause a compensatory external rotation deformity. The combined findings from both images suggest an external rotation deformity most likely related to subsidence into retroversion.
QUESTION 7 OF 50
Figure 8 shows the AP radiograph of a 33-year-old woman who sustained a midshaft clavicle fracture from a motorcycle accident 15 months ago. She continues to have significant pain with activities of daily living. Management should consist of
1
use of an electrical bone stimulation unit.
2
open reduction and internal fixation with a dynamic compression plate placed superiorly and autogenous bone grafting.
3
open reduction and internal fixation with a dynamic compression plate placed inferiorly and autogenous bone grafting.
4
intramedullary screw fixation.
5
partial claviculectomy.
The patient has a symptomatic painful atrophic midclavicular nonunion, and the treatment of choice is rigid internal fixation with a dynamic compression plate and autogenous bone grafting. A tension band effect is desired and achieved by placing the plate superiorly. Excellent success rates of 90% to 100% have been reported using this technique. Intramedullary screw fixation without bone grafting has a decreased success rate. Partial claviculectomy is not a preferred option.
REFERENCES: Jupiter JB, Leffert RD: Non-union of the clavicle: Associated complications and surgical management. J Bone Joint Surg Am 1987;69:753-760.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
REFERENCES: Jupiter JB, Leffert RD: Non-union of the clavicle: Associated complications and surgical management. J Bone Joint Surg Am 1987;69:753-760.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
QUESTION 8 OF 50
A patient presents for treatment of a dislocated second metatarsophalangeal joint. Radiographs demonstrate the dislocation. In addition to soft tissue balancing, you perform an oblique shortening osteotomy of the second metatarsal head (Weil). The most common complication following this osteotomy is:
1
Recurrent dislocation
2
Avascular necrosis of the metatarsal head
3
Arthritis of the second metatarsophalangeal joint
4
Elevation of the second toe
5
C law toe deformity
The Weil osteotomy is a good procedure to correct deformity about the lesser metatarsophalangeal joint but is associated with potential complications, the most common of which is elevation of the second toe. As a result of shortening and plantar shifting of the metatarsal, the intrinsic muscles shift dorsally and can function as a dorsiflexor of the metatarsophalangeal joint.
QUESTION 9 OF 50
Slide 1 Slide 2 Slide 3
A 44-year-old obese man presents for treatment of acute ankle pain. He does not have a history of trauma or a systemic history of note. His opposite foot has had multiple episodes of acute pain in the past, lasting from 3 to 5 days. On examination, the
ankle is warm, swollen, and exquisitely tender to palpation and any range of motion (Slide1, Slide 2, and Slide 3). C oncerned about the source of pain, you aspirate the joint and send the sample for analysis. You expect to find:
A 44-year-old obese man presents for treatment of acute ankle pain. He does not have a history of trauma or a systemic history of note. His opposite foot has had multiple episodes of acute pain in the past, lasting from 3 to 5 days. On examination, the
ankle is warm, swollen, and exquisitely tender to palpation and any range of motion (Slide1, Slide 2, and Slide 3). C oncerned about the source of pain, you aspirate the joint and send the sample for analysis. You expect to find:
1
Gram-positive cocci
2
Gram-negative rods
3
Normal joint fluid
4
Sodium monourate crystals
5
A high red cell count
This patient most likely has an acute attack of gout. The prior episodes of foot pain and the sudden onset lasting 5 days for each bout is characteristic. The ankle is not a common location for gout (the most frequent site is the hallux metatarsophalangeal joint). The treatment should consist of injection of a corticosteroid into the joint and administration of appropriate oral anti-inflammatory medication.
QUESTION 10 OF 50
of 100
Figures 15a and 15b are the radiographs of a 36-year-old right-hand-dominant man who has had persistent wrist pain for 6 months after a motor vehicle collision. The initial treatment was splint immobilization. What is the best next step?


Figures 15a and 15b are the radiographs of a 36-year-old right-hand-dominant man who has had persistent wrist pain for 6 months after a motor vehicle collision. The initial treatment was splint immobilization. What is the best next step?
1
Therapy/rehabilitation
2
Open reduction and internal fixation (ORIF)
3
Proximal row carpectomy
4
Wrist arthrodesis
This patient has a chronic untreated volar lunate dislocation. Lunate dislocations are usually the result of a high-energy injury. Recommended treatment for an acute lunate dislocation is ORIF with repair of injured structures (ligament and bone). If the patient has paresthesias in a median nerve distribution, carpal tunnel release is recommended in the same setting as ORIF. Six months after injury, the prognosis for successful ORIF is poor and proximal row carpectomy is recommended. Among perilunate/lunate dislocations, 25% are initially missed. If a patient arrives for treatment and there is evidence of radiocarpal and midcarpal arthrosis, wrist arthrodesis is recommended.
RECOMMENDED READINGS
15. Stanbury SJ, Elfar JC. Perilunate dislocation and perilunate fracture-dislocation. J Am Acad Orthop Surg. 2011 Sep;19(9):554-62. Review. PubMed PMID: 21885701.View Abstract at PubMed
16. Budoff JE. Treatment of acute lunate and perilunate dislocations. J Hand Surg Am. 2008 Oct;33(8):1424-32. doi: 10.1016/j.jhsa.2008.07.016. Review. PubMed PMID: 18929215.
RECOMMENDED READINGS
15. Stanbury SJ, Elfar JC. Perilunate dislocation and perilunate fracture-dislocation. J Am Acad Orthop Surg. 2011 Sep;19(9):554-62. Review. PubMed PMID: 21885701.View Abstract at PubMed
16. Budoff JE. Treatment of acute lunate and perilunate dislocations. J Hand Surg Am. 2008 Oct;33(8):1424-32. doi: 10.1016/j.jhsa.2008.07.016. Review. PubMed PMID: 18929215.
QUESTION 11 OF 50
Horner syndrome includes all of the following except:
1
Miosis
2
Anhidrosis
3
Enophthalmos
4
Exophthalmos
Horner syndrome is due to disruption of sympathetic innervation and is characterized by enophthalmos not exophthalmos.
QUESTION 12 OF 50
Figures 1 and 2 are intrasurgical photographs from the posterolateral viewing portal that were taken at the beginning and end of a right shoulder arthroscopic procedure performed on a 54-year-old man. This technique demonstrates superior results compared with traditional arthroscopic techniques when evaluating which outcome?








1
Time to healing
2
Retear rate
3
Functional outcome scores
4
Postsurgical pain scores
The images reveal a medium-sized tear of the rotator cuff. As more clinical studies are published comparing double-row with single-row rotator cuff repair, it has become clear that the retear rate is lower with a double-row construct for small and medium-sized tears. This may be attributable to the stronger time-zero repair construct that double-row repair provides. No study to date has demonstrated a significant difference in clinical outcomes (functional and pain scores at any time) or time to healing between the two techniques.
QUESTION 13 OF 50
of 100
A 56-year-old woman fell off a stepladder and sustained the injury shown in Figures 18a and 18b. In addition to the pain from her injury, she has numbness and weakness in her foot. Upon examination, the findings most consistent with her radiographs are decreased sensation
21
A B


A 56-year-old woman fell off a stepladder and sustained the injury shown in Figures 18a and 18b. In addition to the pain from her injury, she has numbness and weakness in her foot. Upon examination, the findings most consistent with her radiographs are decreased sensation
21
A B
1
in her first interspace and an inability to dorsiflex her toes.
2
over her lateral forefoot and an inability to evert her foot.
3
over her medial forefoot and an inability to invert her foot.
4
over her lateral forefoot and an inability to plantar flex her first metatarsal.
The radiographs reveal a tibial pilon fracture with an extruded and rotated anterior tibial fragment that lies deep to the anterior compartment neurovascular bundle, which contains the deep peroneal nerve. This nerve innervates the anterior compartment muscles and the extensor digitorum brevis and extensor hallucis brevis muscles and provides sensation to the dorsal aspect of the first interspace. An injury to the deep peroneal nerve at this level will only affect the innervation to the extensor digitorum brevis and extensor hallucis brevis muscles and the innervation of the first interspace. The superficial peroneal nerve innervates
the lateral compartment muscles above the level of this injury and innervates the dorsum of the foot. The medial forefoot is innervated by the saphenous nerve and the posterior tibial nerve innervates the posterior compartment muscles above the level of the injury. The sural nerve innervates the lateral foot and has no motor component, and the superficial peroneal nerve innervates the peroneus longus, which plantar flexes the first metatarsal above the level of the injury.
RECOMMENDED READINGS
1. Agur AM, Dalley AF, eds. Grant’s Atlas of Anatomy. 13th ed. Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins; 2013:362-370.
2. Hoppenfeld S, de Boer P, Buckley R, eds. Surgical Exposures in Orthopaedics: The Anatomic Approach. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:625-673.
the lateral compartment muscles above the level of this injury and innervates the dorsum of the foot. The medial forefoot is innervated by the saphenous nerve and the posterior tibial nerve innervates the posterior compartment muscles above the level of the injury. The sural nerve innervates the lateral foot and has no motor component, and the superficial peroneal nerve innervates the peroneus longus, which plantar flexes the first metatarsal above the level of the injury.
RECOMMENDED READINGS
1. Agur AM, Dalley AF, eds. Grant’s Atlas of Anatomy. 13th ed. Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins; 2013:362-370.
2. Hoppenfeld S, de Boer P, Buckley R, eds. Surgical Exposures in Orthopaedics: The Anatomic Approach. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:625-673.
QUESTION 14 OF 50
Which metal ion concentrates in the epithelial cells of the proximal tubules and can impair renal function, induce tubular necrosis, and cause marked interstitial changes in experimental animals and humans:
1
Al
2
Co
3
Cr
4
V
5
Ni
Cr is concentrated in the epithelial cells of the proximal renal tubules and can impair renal function, induce tubular necrosis, and cause marked interstitial changes in experimental animals and humans. Indicators of tubular dysfunction have been identified in human objects exposed to Cr (VI) through occupation. Al, Ni, and Co are all rapidly excreted by the kidney, hence renal toxicity tends to require significantly larger doses
QUESTION 15 OF 50
Which of the following collagens forms part of the matrix immediately surrounding the chondrocytes and may help attach the chondrocyte to the matrix macromolecular framework:
1
Type II
2
Type IX
3
Type XI
4
Type VI
5
Type X
Type II, IX, and XI collagen forms a fibrillar network that gives cartilage its form and tensile stiffness and strength. Type VI collagen forms part of the matrix immediately surrounding chondrocytes and may help attach the cells attach to the matrix macromolecular framework.
QUESTION 16 OF 50
of 100
Figures 15a through 15c are the radiograph and MR images of a 16-year-old girl who experienced posterior knee pain after a dance recital 3 weeks ago; the pain resolved 1 week ago with ibuprofen use. What is the most appropriate treatment for this patient?

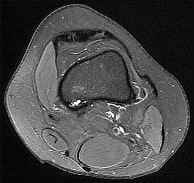

Figures 15a through 15c are the radiograph and MR images of a 16-year-old girl who experienced posterior knee pain after a dance recital 3 weeks ago; the pain resolved 1 week ago with ibuprofen use. What is the most appropriate treatment for this patient?
1
Image-guided core needle biopsy
2
Clinical observation and serial radiographs
3
Tc-99 whole-body bone scan
4
CT scan with sagittal and coronal reconstructions



The images reveal a small reactive-type lesion in the posteromedial aspect of the distal femur consistent with an avulsive cortical irregularity. Also referred to as a cortical desmoid, periosteal desmoid, or “tug lesion,” this lesion is seen most commonly in young adolescents, with a slight preponderance in boys, with one-third occurring bilaterally. It is thought to be related to repeated microtrauma from pulling of the adductor magnus or medial gastrocnemius on their respective periosteal attachment sites. Proper treatment involves recognition of this benign disorder without further workup. Often best seen on an oblique radiograph, the lack of soft-tissue mass or bone destruction leads to the benign diagnosis. Serial radiographs typically show complete resolution by age 20.
RECOMMENDED READINGS
25. [Gould CF, Ly JQ, Lattin GE Jr, Beall DP, Sutcliffe JB 3rd. Bone tumor mimics: avoiding misdiagnosis. Curr Probl Diagn Radiol. 2007 May-Jun;36(3):124-41. Review. PubMed PMID: 17484955. ](http://www.ncbi.nlm.nih.gov/pubmed/17484955)[View](http://www.ncbi.nlm.nih.gov/pubmed/17484955)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17484955)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17484955)
26. [Yamazaki T, Maruoka S, Takahashi S, Saito H, Takase K, Nakamura M, Sakamoto K. MR findings of avulsive cortical irregularity of the distal femur. Skeletal Radiol. 1995 Jan;24(1):43-6. PubMed PMID: 7709251. ](http://www.ncbi.nlm.nih.gov/pubmed/7709251)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7709251)
27. [Damron TA, Morris C, Rougraff B, Tamurian R. Diagnosis and treatment of joint-related tumors that mimic sports-related injuries. Instr Course Lect. 2009;58:833-47. PubMed PMID: 19385590. ](http://www.ncbi.nlm.nih.gov/pubmed/19385590)[View](http://www.ncbi.nlm.nih.gov/pubmed/19385590)[ ](http://www.ncbi.nlm.nih.gov/pubmed/19385590)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19385590)
RECOMMENDED READINGS
25. [Gould CF, Ly JQ, Lattin GE Jr, Beall DP, Sutcliffe JB 3rd. Bone tumor mimics: avoiding misdiagnosis. Curr Probl Diagn Radiol. 2007 May-Jun;36(3):124-41. Review. PubMed PMID: 17484955. ](http://www.ncbi.nlm.nih.gov/pubmed/17484955)[View](http://www.ncbi.nlm.nih.gov/pubmed/17484955)[ ](http://www.ncbi.nlm.nih.gov/pubmed/17484955)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17484955)
26. [Yamazaki T, Maruoka S, Takahashi S, Saito H, Takase K, Nakamura M, Sakamoto K. MR findings of avulsive cortical irregularity of the distal femur. Skeletal Radiol. 1995 Jan;24(1):43-6. PubMed PMID: 7709251. ](http://www.ncbi.nlm.nih.gov/pubmed/7709251)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7709251)
27. [Damron TA, Morris C, Rougraff B, Tamurian R. Diagnosis and treatment of joint-related tumors that mimic sports-related injuries. Instr Course Lect. 2009;58:833-47. PubMed PMID: 19385590. ](http://www.ncbi.nlm.nih.gov/pubmed/19385590)[View](http://www.ncbi.nlm.nih.gov/pubmed/19385590)[ ](http://www.ncbi.nlm.nih.gov/pubmed/19385590)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19385590)
QUESTION 17 OF 50
of 100
Figures 1 through 4 are the radiographs and CT scans of a 13-year-old male cross-country runner who has had vague posterior thigh pain for more than a year. Pain is worse at night than while running. History is negative for trauma, fevers, or constitutional signs or symptoms. Pain is relieved with nonsteroidal anti-inflammatory drugs (NSAIDs). Labs and inflammatory markers are all normal. What is the most appropriate treatment for this patient?

Figures 1 through 4 are the radiographs and CT scans of a 13-year-old male cross-country runner who has had vague posterior thigh pain for more than a year. Pain is worse at night than while running. History is negative for trauma, fevers, or constitutional signs or symptoms. Pain is relieved with nonsteroidal anti-inflammatory drugs (NSAIDs). Labs and inflammatory markers are all normal. What is the most appropriate treatment for this patient?
1
CT-guided biopsy to confirm diagnosis and enable prognostic prediction
2
Continued symptomatic management with NSAID therapy with expected resolution of symptoms
3
Activity restriction and touch down weightbearing with potential need for stress fracture stabilization
4
Empiric antibiotics with expectant resolution of lesion after 6 weeks of therapy
■
Plain films, CT and MRI evidence an intracortical lucency <1.5 cm in diameter consistent with a benign nidus of an osteoid osteoma. Open biopsy is not required, as the imaging findings are pathognomonic. In this case, symptoms are chronic and well-controlled with NSAIDs, thus more aggressive intervention is not indicated. The natural history of untreated osteoid osteomas is often for spontaneous resolution in 2 to 3 years. Treatment options for osteoid osteomas causing disabling symptoms despite NSAID therapy include open surgical excision or minimally invasive image-guided procedures (i.e., cryotherapy, radiofrequency ablation). The imaging findings are not representative of a ‘dreaded black line’, as in a stress fracture. Normal labs direct against an infectious etiology for this patient's symptoms.
QUESTION 18 OF 50
of 100
A 55-year-old man falls from a ladder and dislocates his nondominant shoulder. He undergoes a sedated reduction in the emergency department without complications. Postreduction radiographs reveal a small Hill-Sachs lesion and no other bony abnormalities. Six weeks after the dislocation, he has persistent pain at rest and forward elevation and external rotation weakness. He has no abnormal sensation. What is the best next step?
A 55-year-old man falls from a ladder and dislocates his nondominant shoulder. He undergoes a sedated reduction in the emergency department without complications. Postreduction radiographs reveal a small Hill-Sachs lesion and no other bony abnormalities. Six weeks after the dislocation, he has persistent pain at rest and forward elevation and external rotation weakness. He has no abnormal sensation. What is the best next step?
1
Physical therapy with electrical stimulation and iontophoresis
2
Corticosteroid injection
3
MR imaging of the shoulder
4
Electromyography (EMG) of the arm
For a patient in his mid 50s who has shoulder instability and persistent weakness, MR imaging is indicated to evaluate rotator cuff integrity. EMG is not indicated because this patient has no evidence of deltoid functional abnormality. Corticosteroid injections and physical therapy modalities do not address the concern about his potential for a rotator cuff tear.
RECOMMENDED READINGS
21. [Gombera MM, Sekiya JK. Rotator cuff tear and glenohumeral instability: a systematic review. Clin Orthop Relat Res. 2014 Aug;472(8):2448-56. doi: 10.1007/s11999-013-3290-2. Review. Erratum in: Clin Orthop Relat Res. 2015 Feb;473(2):751. Gomberawalla, M Mustafa ](http://www.ncbi.nlm.nih.gov/pubmed/24043432)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24043432)
22. [Paxton ES, Dodson CC, Lazarus MD. Shoulder instability in older patients. Orthop Clin North Am. 2014 Jul;45(3):377-85. doi: 10.1016/j.ocl.2014.04.002. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/24975764)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24975764)
RECOMMENDED READINGS
21. [Gombera MM, Sekiya JK. Rotator cuff tear and glenohumeral instability: a systematic review. Clin Orthop Relat Res. 2014 Aug;472(8):2448-56. doi: 10.1007/s11999-013-3290-2. Review. Erratum in: Clin Orthop Relat Res. 2015 Feb;473(2):751. Gomberawalla, M Mustafa ](http://www.ncbi.nlm.nih.gov/pubmed/24043432)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24043432)
22. [Paxton ES, Dodson CC, Lazarus MD. Shoulder instability in older patients. Orthop Clin North Am. 2014 Jul;45(3):377-85. doi: 10.1016/j.ocl.2014.04.002. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/24975764)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24975764)
QUESTION 19 OF 50
of 100
Which treatment of the current fracture will provide the best long-term outcome?




Which treatment of the current fracture will provide the best long-term outcome?
1
Casting it in its current position, which is acceptable alignment
2
Closed reduction and casting
3
Functional brace because this is a stable fracture
4
Open reduction with revision of the current implants
Many patients with mild dominant OI (the most common type) appear “normal,” and a diagnosis cannot be made without a careful personal history, family history, and observance of blue sclera. More than 3 fractures during childhood places someone outside of the mean and should merit further investigation. There is no sign of rickets on this radiograph (physeal widening/cupping). Similarly, the history and examination finding of blue sclera in the patient and his mother should raise concern for OI. Many parents of children with OI have inappropriately been accused of abuse despite obvious examination, radiograph, and family history findings that suggest OI. Low-energy mechanisms that create displaced fractures are a hallmark of OI and do not in isolation raise suspicion for nonaccidental trauma.
Based on the history and examination, mild-form OI caused by a defect in the type I collagen gene is most likely. Defects in type II collagen genes affect articular cartilage and cause epiphyseal dysplasia. Defects in the LEPRE cause severe-form OI involving clinically bowed limbs, marked short stature, and white sclera. There is no sign on radiographs of rickets, so severe vitamin D deficiency is not present. The history, examination, and radiographs all point toward OI/osteoporosis rather than nonaccidental trauma.
Peri-implant fractures occur because of a difference in elasticity between the bone with implants and the bone adjacent to it without implants. This is particularly important in the setting of osteoporotic bone in which the difference in elasticity and rigidity will be much more pronounced than in normal bone. Load-sharing implants are preferred when possible. The original fracture occurred proximal to the current fracture in the middle of the plated bone and looks healed with no sign of infection.
This fracture is in unacceptable alignment with subluxation of the radiocapitellar joint. The plates are bent, so closed reduction will not solve the alignment problem. In early childhood, load-sharing implants (flexible rods or wires) should be used to solve the elasticity mismatch that contributed to the current fracture.
Figure 51a
Figure 51b
Figure 51c
CLINICAL SITUATION FOR QUESTIONS 51 THROUGH 54
Figures 51a through 51c are the radiographs of an 8-year-old boy with a shoulder deformity and limited cervical range of motion. He has no significant medical problems and plays baseball, pitching with his right arm. His active shoulder abduction is 180 degrees on the left and 150 degrees on the right.
Based on the history and examination, mild-form OI caused by a defect in the type I collagen gene is most likely. Defects in type II collagen genes affect articular cartilage and cause epiphyseal dysplasia. Defects in the LEPRE cause severe-form OI involving clinically bowed limbs, marked short stature, and white sclera. There is no sign on radiographs of rickets, so severe vitamin D deficiency is not present. The history, examination, and radiographs all point toward OI/osteoporosis rather than nonaccidental trauma.
Peri-implant fractures occur because of a difference in elasticity between the bone with implants and the bone adjacent to it without implants. This is particularly important in the setting of osteoporotic bone in which the difference in elasticity and rigidity will be much more pronounced than in normal bone. Load-sharing implants are preferred when possible. The original fracture occurred proximal to the current fracture in the middle of the plated bone and looks healed with no sign of infection.
This fracture is in unacceptable alignment with subluxation of the radiocapitellar joint. The plates are bent, so closed reduction will not solve the alignment problem. In early childhood, load-sharing implants (flexible rods or wires) should be used to solve the elasticity mismatch that contributed to the current fracture.
Figure 51a
Figure 51b
Figure 51c
CLINICAL SITUATION FOR QUESTIONS 51 THROUGH 54
Figures 51a through 51c are the radiographs of an 8-year-old boy with a shoulder deformity and limited cervical range of motion. He has no significant medical problems and plays baseball, pitching with his right arm. His active shoulder abduction is 180 degrees on the left and 150 degrees on the right.
QUESTION 20 OF 50
Which of the following measures has not been shown to decrease rates of injury in healthy children participating in recreational sports:
1
Knee braces during basketball and football
2
Ankle braces in basketball
3
Helmets for bicyclists
4
Mouth guards for basketball
5
Break-away bases for baseball
Knee braces have been shown not to reduce injury rates for children for children with sound knees. All other measures have been shown to reduce injury rates.
QUESTION 21 OF 50
After performing an uneventful partial palmar fasciectomy for Dupuytren contracture of the palm and ring finger, a general postsurgical pain medication prescription should include how many narcotic pills?
1
0
2
10
3
20
4
30
After the designation of pain as the fifth vital sign, opioid analgesic use has steadily increased. Many surgeons routinely prescribe 30 or more pills after elective hand surgery. However, studies show that patients generally use fewer than 30 pills. Patients who underwent bone procedures used 14 pills, and those undergoing soft-tissue procedures used 9 pills. Education and decision aids may help physicians size prescriptions appropriately to avoid overmedication. Patients undergoing small soft-tissue surgeries such as trigger releases should not need narcotics. Those undergoing small-joint surgeries, carpal tunnel releases, and Dupuytren fasciectomy may benefit from a prescription of 10 pills. More extensive surgery, such as open fracture treatment, may justify more pills, but prescriptions should not exceed 40 tablets _under typical circumstances._
QUESTION 22 OF 50
of 100
After discussing his diagnosis along with surgical and nonsurgical treatment options, the patient wishes to proceed with surgical intervention. He has done some online research and has questions about which procedure will produce the best outcome. Based on the current literature, what is the optimal next procedure?


After discussing his diagnosis along with surgical and nonsurgical treatment options, the patient wishes to proceed with surgical intervention. He has done some online research and has questions about which procedure will produce the best outcome. Based on the current literature, what is the optimal next procedure?
1
Arthroscopic glenohumeral debridement with biceps tenotomy
2
Hemiarthroplasty
3
Total shoulder arthroplasty (TSA)
4
Reverse TSA (rTSA)
- Total shoulder arthroplasty (TSA)_
QUESTION 23 OF 50
A 70-year-old patient with a history of Parkinson’s disease sustains a fall onto his hip. He denies a history of antecedent hip pain
and is otherwise healthy. A radiograph of the affected hip is shown in Figure A. What is the best treatment option and best rationale for this patient?

and is otherwise healthy. A radiograph of the affected hip is shown in Figure A. What is the best treatment option and best rationale for this patient?
1
Total hip arthroplasty; decrease his risk for dislocations
2
Total hip arthroplasty; decrease his risk for infection
3
Total hip arthroplasty; use a minimally invasive approach
4
Hip hemiarthroplasty; decrease his risk for dislocations
5
Hip hemiarthroplasty; decrease his risk for infection
This patient has sustained a Garden IV femoral neck fracture. The optimal treatment for this patient is a hip hemiarthroplasty to limit his risk for dislocation.
Displaced femoral neck fractures are often treated with arthroplasty. Although functional outcomes are better with total hip arthroplasty (THA), the risk of dislocation is seven times higher. Patients who are at risk for falls and/or demonstrate cognitive decline (ie. Parkinson’s disease), should be treated with a hemiarthroplasty.
Lee et al. reviewed 126 cases of THA used to treat acute femoral neck fractures. They noted long-term survival of the prosthesis and good clinical results despite a higher rate of complications.
Ricci et al. reviewed 29 THAs performed in 26 patients who did not have Parkinson’s disease or other evidence of cognitive/ambulatory dysfunction. Factors associated with low dislocation rates include selecting the right patients
and intraoperative technique focused on stability of the hip.
Zuckerman et al. review the diagnosis and orthopaedic management of the Parkinson’s disease patient. They report for patients with femoral neck fractures, use of hip hemiarthroplasty has improved their ambulatory capacity. In contrast, complication rates following total hip arthroplasty approach 26%.
Figure A shows an AP radiograph of the pelvis. There is a Garden IV fracture of the femoral neck of the right hip. On the left hip, notice thinning of the medial wall of the acetabulum, with loss of sphericity of the femoral head and significant protrusion of the hip.
Incorrect Answers:
Answer 1: THA would increase his risk for dislocations.
Answers 2, 5: Implant placement would still put the patient at risk for infection.
Answer 3: Although a minimally invasive choice could be taken, a THA is not appropriate for this patient.
Displaced femoral neck fractures are often treated with arthroplasty. Although functional outcomes are better with total hip arthroplasty (THA), the risk of dislocation is seven times higher. Patients who are at risk for falls and/or demonstrate cognitive decline (ie. Parkinson’s disease), should be treated with a hemiarthroplasty.
Lee et al. reviewed 126 cases of THA used to treat acute femoral neck fractures. They noted long-term survival of the prosthesis and good clinical results despite a higher rate of complications.
Ricci et al. reviewed 29 THAs performed in 26 patients who did not have Parkinson’s disease or other evidence of cognitive/ambulatory dysfunction. Factors associated with low dislocation rates include selecting the right patients
and intraoperative technique focused on stability of the hip.
Zuckerman et al. review the diagnosis and orthopaedic management of the Parkinson’s disease patient. They report for patients with femoral neck fractures, use of hip hemiarthroplasty has improved their ambulatory capacity. In contrast, complication rates following total hip arthroplasty approach 26%.
Figure A shows an AP radiograph of the pelvis. There is a Garden IV fracture of the femoral neck of the right hip. On the left hip, notice thinning of the medial wall of the acetabulum, with loss of sphericity of the femoral head and significant protrusion of the hip.
Incorrect Answers:
Answer 1: THA would increase his risk for dislocations.
Answers 2, 5: Implant placement would still put the patient at risk for infection.
Answer 3: Although a minimally invasive choice could be taken, a THA is not appropriate for this patient.
QUESTION 24 OF 50
A 13-year-old girl is seen in clinic for bunion. She is asymptomatic but has a hallux valgus angle of 29°, an intermetatarsal angle of 15°, and a medial prominence over the first metatarsal head. The family asks whether anything can be done to prevent future problems with the foot. You recommend:
1
Osteotomy of the first metatarsal base
2
Hemiepiphyseodesis of the medial physis of the first metatarsal
3
Double osteotomy of the first metatarsal
4
Mitchell osteotomy
5
Shoe modifications if symptoms develop
Bunions may often be treated conservatively, and it is impossible to predict which ones will later develop symptoms. Surgical reconstruction of bunions in adolescents has a higher rate of recurrence than in adults in many reported series. For all of these reasons, nonoperative treatment is preferred for asymptomatic patients.
QUESTION 25 OF 50
Superficial peroneal nerve injury following ankle fracture:
1
Does not occur with nonoperative treatment
2
C an best be avoided during open reduction internal fixation with a posterolateral approach to the fibula
3
Did not ultimately affect the final AOFAS ankle-hindfoot score
4
Occurs in fewer than 5% of operatively fixed fibula fractures
5
C an best be avoided during open reduction internal fixation with an anterolateral approach to the fibula
One hundred twenty patients with ankle fractures were evaluated. Symptomatic superficial peroneal nerve injury was identified in
21% of patients who underwent open reduction internal fixation and 9% of nonoperatively treated patients. AOFAS scores were decreased in patients with symptomatic superficial peroneal nerve injury. No injuries to the superficial peroneal nerve occurred in patients who underwent surgery involving a posterolateral approach to the fibula.
21% of patients who underwent open reduction internal fixation and 9% of nonoperatively treated patients. AOFAS scores were decreased in patients with symptomatic superficial peroneal nerve injury. No injuries to the superficial peroneal nerve occurred in patients who underwent surgery involving a posterolateral approach to the fibula.
QUESTION 26 OF 50
A 42-year-old woman reports neck stiffness, upper extremity pain, clumsiness, weakness, and instability of gait. Examination reveals 4+ of 5 strength in the upper extremities and 3+ biceps, brachioradialis, and patellar reflexes with a positive Hoffman sign bilaterally. MRI and CT scans are shown in Figures 10a and 10b. Based on the history and imaging findings, what is the most likely diagnosis?
1
Diffuse idiopathic skeletal hyperostosis
2
Ankylosing spondylitis
3
Ossification of the posterior longitudinal ligament
4
Rheumatoid arthritis
5
Degenerative cervical stenosis
The sagittal T2-weighted MRI scan shows moderate-severe multilevel cervical stenosis.The cord compression is noted to be not only
at the disk levels but also at the midvertebral body levels,and the posterior longitudinal ligament appears to be thickened. The CT scan confirms that the posterior longitudinal ligament is indeed thickened and ossified, compatible with a diagnosis of ossification of the posterior longitudinal ligament. This diagnosis is most common in individuals of
Japanese descent and has a genetic linkage. The anterior osteophytes are smaller than those seen in diffuse idiopathic skeletal hyperostosis and are not syndesmotic. Patients with ankylosing spondylitis typically have non-marginal syndesmophytes. Patients with rheumatoid arthritis may have evidence of instability at C1-C2 on flexionextension radiographs and subaxial subluxations.
at the disk levels but also at the midvertebral body levels,and the posterior longitudinal ligament appears to be thickened. The CT scan confirms that the posterior longitudinal ligament is indeed thickened and ossified, compatible with a diagnosis of ossification of the posterior longitudinal ligament. This diagnosis is most common in individuals of
Japanese descent and has a genetic linkage. The anterior osteophytes are smaller than those seen in diffuse idiopathic skeletal hyperostosis and are not syndesmotic. Patients with ankylosing spondylitis typically have non-marginal syndesmophytes. Patients with rheumatoid arthritis may have evidence of instability at C1-C2 on flexionextension radiographs and subaxial subluxations.
QUESTION 27 OF 50
**ORTHOPEDIC MCQS ONLINE HIP AND KNEE RECON 07**
1/. A patient is scheduled to undergo total knee arthroplasty (TKA) following failure of nonsurgical management. History reveals that she underwent a patellectomy as a teenager as the result of a motor vehicle accident. Examination reveals normal ligamentous stability. For the most predictable outcome, which of the following implants should be used?
1/. A patient is scheduled to undergo total knee arthroplasty (TKA) following failure of nonsurgical management. History reveals that she underwent a patellectomy as a teenager as the result of a motor vehicle accident. Examination reveals normal ligamentous stability. For the most predictable outcome, which of the following implants should be used?
1
Mobile-bearing knee
2
Posterior cruciate ligament-sparing knee
3
Posterior cruciate ligament-substituting knee
4
Semiconstrained-style knee
5
Triaxial hinged knee
Paletta and Laskins performed a retrospective study of the results of TKA with cement in 22 patients who had a previous patellectomy. Nine of the patients had insertion of a posterior cruciate ligament-substituting implant. Thirteen patients had insertion of a posterior cruciate ligament-sparing implant. The 5-year postoperative knee scores were 89 for the posterior cruciate ligament-substituting knee versus 67 for the posterior cruciate
ligament-sparing knee (P < 0.01). The patella functions to increase the lever arm of the extensor mechanism and to position the quadriceps tendon and the patellar ligament roughly parallel to the anterior cruciate ligament and posterior cruciate ligament, respectively. The patellar ligament thereby provides a strong reinforcing structure that functions to prevent excessive anterior translation of the femur during flexion of the knee. The absence of the patella results in the patellar ligament and the quadriceps tendon being relatively in line with one another. After a patellectomy, the resultant quadriceps force is no longer parallel to the posterior cruciate ligament. This results in loss of the reinforcing function of the patellar ligament. The authors believe this loss of reinforcing function may place increased stresses on the posterior cruciate ligament and posterior aspect of the capsule, which may result in stretching of these structures over time. They found a high rate of anteroposterior instability, a high prevalence of recurvatum, and a high rate of loss of full active extension compared with passive extension in the posterior cruciate ligament-sparing group, which supports their theory. **
**
ligament-sparing knee (P < 0.01). The patella functions to increase the lever arm of the extensor mechanism and to position the quadriceps tendon and the patellar ligament roughly parallel to the anterior cruciate ligament and posterior cruciate ligament, respectively. The patellar ligament thereby provides a strong reinforcing structure that functions to prevent excessive anterior translation of the femur during flexion of the knee. The absence of the patella results in the patellar ligament and the quadriceps tendon being relatively in line with one another. After a patellectomy, the resultant quadriceps force is no longer parallel to the posterior cruciate ligament. This results in loss of the reinforcing function of the patellar ligament. The authors believe this loss of reinforcing function may place increased stresses on the posterior cruciate ligament and posterior aspect of the capsule, which may result in stretching of these structures over time. They found a high rate of anteroposterior instability, a high prevalence of recurvatum, and a high rate of loss of full active extension compared with passive extension in the posterior cruciate ligament-sparing group, which supports their theory. **
**
Scientific References
- : Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.**
**Paletta GA Jr, Laskins RS: Total knee arthroplasty after a previous patellectomy. J Bone Joint Surg Am 1995;77:1708-1712.**
**2/. Figure 1 shows the radiograph of a patient who underwent a total knee revision with a posterior stabilized mobile-bearing prosthesis and now has recurrent knee dislocations. What is the most likely cause?
1- Loose extension gap
2- Loose flexion gap
3- Malrotation of the tibial component
4- Malrotation of the femoral component
5- Poor prosthetic design
PREFERRED RESPONSE: 2**
**DISCUSSION: The patient has a posterior stabilized total knee revision, and the femoral component has dislocated over the tibial polyethylene cam/post. This usually indicates a loose flexion gap, or “flexion instability.” A loose flexion gap can occur due to undersizing of the femoral component, anteriorization of the femoral component, excessive distal augmentation of the distal femur, or collateral ligament insufficiency, especially if combined with posterior capsular insufficiency. Isolated laxity of the extension gap (with a well-balanced flexion gap) causes varus/valgus instability, but it rarely causes the femoral component to “jump” the tibial cam of a posterior stabilized tibial insert. Malrotation of the components may cause patellar instability or a rotational instability of the tibiofemoral joint but should not cause a frank posterior dislocation of the tibia, unless combined with other errors of balancing. Although a mobile-bearing total knee arthroplasty may be more sensitive to errors in balancing than a
fixed-bearing total knee arthroplasty, this complication does not reflect a faulty prosthetic design.**
**REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 339-365.**
**Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott-Raven, 1999, pp 173-186, 227-249.**
**Clarke HD, Scuderi GR: Flexion instability in primary total knee replacement. J Knee Surg 2003;16:123-128.**
**3/. A metal-on-metal bearing used for total hip arthroplasty shows which of the
following properties?
1- Baseline serum ion levels increase with increasing activity levels.
2- The risk of cancer is substantially increased.
3- Linear ion production increases over time.
4- Ions produced are excreted primarily through the kidney.
5- Nickel is the most prevalent ion released into circulation.
PREFERRED RESPONSE: 4**
**DISCUSSION: Activity levels do not affect cobalt and chromium ion levels, which are the bulk of serum ion levels. The majority of ions are produced in the run-in period in the first several years. A gradual reduction in ion levels occurs thereafter. The kidneys are responsible for the bulk of clearance from the serum, and to date there is no relationship of cancer to ion levels in the serum.**
**REFERENCE: Heisel C, Silva M, Skipor AK, et al: The relationship between activity and ions in patients with metal-on-metal bearing hip prostheses. J Bone Joint Surg Am 2005;87:781-787.**
**4/. Which of the following treatment regimens for thromboembolic prophylaxis meets the American College of Chest Physicians Guidelines for 10-day treatment after total hip arthroplasty and total knee arthroplasty?
1- Low-molecular-weight heparin
2- Adjusted dose unfractionated heparin
3- Aspirin
4- Warfarin, INR 1.5 to 2.0
5- Elastic compressive stockings
PREFERRED RESPONSE: 1**
**DISCUSSION: Only three thromboembolic treatment protocols have reached Grade 1A status for the American College of Chest Physicians Guidelines for thromboembolic prophylaxis after total hip arthroplasty and total knee arthroplasty. Grade 1A evidence shows a clear benefit/risk improvement with supportive data from randomized clinical trials, which are strongly applicable in most clinical circumstances. Warfarin is recommended but at an INR level of 2 to 3.
Low-molecular-weight heparin and fondaparinox are also acceptable treatment options. Aspirin, adjusted dose unfractionated heparin, and elastic compressive stockings are not recommended as stand-alone options. **
**REFERENCES: Colwell C: Evidence based guidelines for prevention of venous thromboembolism: Symposia. Proceedings of the 2005 AAOS Annual Meeting. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 15-18.**
**Freedman KB, Brookenthal KR, Fitzgerald RH, et al: A meta-analysis of thromboembolic prophylaxis following elective total hip arthroplasty. J Bone Joint Surg Am 2000;82:929-938.**
**5/. Figures 2a and 2b show the radiographs of a 72-year-old man with aseptic loosening of the tibial component of his total knee arthroplasty. Optimal management should include
1- tibial revision only, without stems or augmentations.
2- tibial revision only, with stems and augmentations.
3- revision of the tibial and femoral components, without stems or augmentations.
4- revision of the tibial and femoral components, with stems and augmentations.
5- primary arthrodesis.
PREFERRED RESPONSE: 4**
**DISCUSSION: The radiographs show massive subsidence of the lateral side of the tibia with severe tibial bone loss and a fractured proximal fibula. Reconstruction should consist of a large metal or bony lateral tibial augmentation, and a stem long enough to bypass the defect is required. The femoral and tibial components are articulating without any remaining polyethylene medially; therefore, the femoral component is damaged and needs revision.
The insertions of the lateral ligaments are absent, thereby rendering the lateral side of the knee predictably unstable. Also, the large valgus deformity compromises the medial collateral ligament. The posterior cruciate ligament is also likely to be deficient with this much tibial bone destruction. The patient requires a posterior stabilized femoral component at the minimum, and possibly a constrained femoral component. Retention of the femoral component, even though it may be well-fixed, jeopardizes the outcome.**
**REFERENCES: Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott-Raven, 1999, pp 137-250.**
**Insall JN, Windsor RE, Scott WN, et al: (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 935-957.**
**Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 339-365.**
**6/. Which of the following factors is responsible for causing the distal femur to pivot about a medial axis as the knee moves from full extension into early flexion?
1- Differential forces generated from the vastus lateralis and vastus medialis
2- Differential tension within the bundles of the posterior cruciate ligament
3- Differential radius of curvature between the medial and lateral femoral condyles
4- Asymmetry of the tibial tubercle on the anterior surface of the tibia
5- Asymmetric forces generated from the uneven patellar facets
PREFERRED RESPONSE: 3**
**DISCUSSION: The radius of curvature of the distal femur is greater over the distal aspect of the lateral femoral condyle than the distal aspect of the medial femoral condyle. As the femur rolls posteriorly during early knee flexion, both condyles undergo similar angular changes equal to the amount of flexion. With a similar amount of angular rotation, the sphere with the larger radius experiences greater net rollback, producing a pivoting motion. Although the anterior cruciate ligament plays a role in producing tibial rotations, the posterior cruciate ligament does not play a significant role in producing such rotations. Similarly, the tibial tubercle does not play a significant role in producing normal rotations of the femur relative to the tibia. The popliteus may also play a role in producing rotational pivots, as might differential laxity of the medial and lateral collateral ligaments in early knee flexion.**
**REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 239-240.**
**Insall JN, Windsor RE, Scott WN, et al (eds): Surgery of the Knee, ed 2. New York, Churchill Livingstone, 1993, pp 1-13.**
**7/. Figure 3 shows the AP radiograph of a patient with diabetes mellitus who has knee pain. A semiconstrained knee prosthesis was used in this patient to prevent which of the following complications?
1- Infection
2- Instability
3- Stiffness
4- Bone loss
5- Malalignment
PREFERRED RESPONSE: 2**
**DISCUSSION: The radiographic appearance of the joint is highly suspicious for neuropathic joint (Charcot’s joint). Evidence of bone loss on both the tibial and the femoral sides may necessitate the use of metal and/or bone augments. Patients with a neuropathic joint often have excellent range of motion, and postoperative stiffness is not a problem. The main problem with these patients is instability that occurs secondary to ligamentous laxity. Use of a semiconstrained prosthesis prevents the latter complication.**
**REFERENCES: Parvizi J, Marrs J, Morrey BF: Total knee arthroplasty for neuropathic (Charcot) joints. Clin Orthop 2003;416:145-150.**
**Kim YH, Kim JS, Oh SW: Total knee arthroplasty in neuropathic arthropathy. J Bone Joint
Surg Br 2002;84:216-219.**
**8/. Based on the radiograph shown in Figure 4, the innervation of what muscle is most at risk with total hip arthroplasty?
1- Quadriceps
2- Extensor hallucis longus
3- Lateral gastrocnemius
4- Adductor magnus
5- Semitendinosus
PREFERRED RESPONSE: 2**
**DISCUSSION: The radiograph reveals a Crowe IV deformity in a patient with developmental dysplasia of the hip. If hip arthroplasty is performed, then some degree of limb lengthening is anticipated. Excessive limb lengthening can result in sciatic nerve palsy in these patients. The peroneal branch of the sciatic nerve is most often affected. Of the muscles listed, only the extensor hallucis longus is innervated by the peroneal branch of the sciatic nerve.**
**REFERENCES: Eggli S, Hankemayer S, Muller ME: Nerve palsy after leg lengthening in total replacement arthroplasty for developmental dysplasia of the hip. J Bone Joint Surg Br 1999;81:843-845.**
**Schmalzried TP, Amstutz HC, Dorey FJ: Nerve palsy associated with total hip replacement:
Risk factors and prognosis. J Bone Joint Surg Am 1991;73:1074-1080.**
**9/. A 75-year-old woman who fell on her right knee now reports pain and is unable to bear weight. History reveals that she underwent total knee arthroplasty on the right knee
6 years ago. Radiographs are shown in Figure 5. Management should now consist of
1- closed reduction and casting for 6 weeks.
2- open reduction and internal fixation, using a locked intramedullary rod.
3- open reduction and internal fixation, using two cancellous screws.
4- open reduction and internal fixation, using a locked plate and screws.
5- open reduction and internal fixation and revision of the femoral component.
PREFERRED RESPONSE: 5**
**DISCUSSION: The radiographs show a loose femoral component with an associated medial condyle distal femoral fracture. The treatment of choice is open reduction and internal fixation with revision of the femoral component because of the femoral component loosening.**
**REFERENCES: Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209.**
**McLaren AC, DuPont JA, Schroeber DC: Open reduction internal fixation of supracondylar fractures above total knee arthroplasties using the intramedullary supracondylar rod. Clin Orthop 1994;302:194-198.**
**Figgie MP, Goldberg VM, Figgie HE III, et al: The results of treatment of supracondylar fracture above total knee arthroplasty. J Arthroplasty 1990;5:267-276.**
**10/. Which of the following nutraceuticals has been associated with perioperative bleeding?
1- Glucosamine
2- Chondroitin sulfate
3- Ginseng
4- Nitric oxide
5- Ginkgo biloba
PREFERRED RESPONSE: 5**
**DISCUSSION: Ginkgo biloba is a popular nutraceutical for patients who have early dementia, intermittent claudication secondary to peripheral vascular disease, vertigo, and tinnitus. It is reported to improve mental alertness and cognitive deficiency. It has antiplatelet properties as a result of one of its components, ginkgolide B, which displaces platelet-activating factor from its receptor binding sight. Rowin and Lewis reported on spontaneous bilateral subdural hematomas associated with chronic ginkgo biloba ingestion. Vale also reported on subarachnoid hemorrhage associated with ginkgo biloba. Bebbington and associates reported on persistent postoperative bleeding after total hip arthroplasty secondary to ginkgo biloba usage. Furthermore, the use of ginkgo biloba with aspirin or other antiplatelet agents or anticoagulants represents a relative contraindication. Physicians should be aware not only of prescribed medications but also alternative nutraceuticals that are used by the patient.**
**REFERENCES: Rowin J, Lewis SL: Spontaneous bilateral subdural hematomas associated with chronic ginkgo biloba ingestion. Neurology 1996;46:1775-1776.**
**Vale S: Subarachnoid hemorrhage associated with ginkgo biloba. Lancet 1998;352:36.**
**Bebbington A, Kulkarni R, Roberts P: Ginkgo biloba: Persistent bleeding after total hip arthroplasty caused by herbal self-medication. J Arthroplasty 2005;20:125-126.**
**11/. A 64-year-old man undergoes a primary total knee arthroplasty. Three months after surgery he reports persistent pain, weakness, and difficulty ambulating. Postoperative radiographs are shown in Figures 6a through 6c. What is the best course of action at
this time?
1- Hinged knee brace
2- Patellar component revision with a tantalum implant and lateralization of the patella
3- Revision knee arthroplasty with greater internal rotation of the tibial component
4- Revision total knee arthroplasty with a lateral release and external rotation of the femoral component
5- Revision total knee arthroplasty with a lateral release and internal rotation of the femoral component
PREFERRED RESPONSE: 4**
**DISCUSSION: The Merchant view reveals subluxation of the patellar component. The etiology of maltracking of the patella includes internal rotation of the femoral component, internal rotation of the tibial component, excessive patellar height, and lateralization of the patella component. The treatment of choice in this patient is revision total knee arthroplasty with external rotation of the femoral component. Preoperatively the patient also may require a lateral release, revision of the tibial component if it is internally rotated, and possibly a soft-tissue realignment. Component malalignment needs to be addressed first.**
**REFERENCES: Kelly MA: Extensor mechanism complications in total knee arthroplasty.
Instr Course Lect 2004;53:193-199.**
**Malkani AL, Karandikar N: Complications following total knee arthroplasty. Sem Arthroplasty 2003;14:203-214.**
**Norman AJ, Scott S, David GN (eds): Master Techniques in Knee Arthroplasty, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2003. **
**12/. Compared to metal-on-polyethylene total hip bearing surfaces, the debris particles generated by metal-on-metal articulations are
1- larger and less numerous.
2- larger and more numerous.
3- smaller and less numerous.
4- smaller and more numerous.
5- not detectable.
PREFERRED RESPONSE: 4**
**DISCUSSION: Retrieval studies have shown that the debris particles produced by
metal-on-metal articulations in total hip arthroplasty are several orders of magnitude smaller
and may be up to 100 times more numerous than those found with metal-on-polyethylene articulations.**
**REFERENCES: Davies AP, Willert HG, Campbell PA, et al: An unusual lymphocytic perivascular infiltration in tissues around contemporary metal-on-metal joint replacements.
J Bone Joint Surg Am 2005;87:18-27.**
**Firkins PJ, Tipper JL, Saadatzadeh MR, et al: Quantitative analysis of wear and wear debris from metal-on-metal hip prostheses tested in a physiological hip joint simulator. Biomed Mater Eng 2001;11:143-157.**
**13/. A 60-year-old patient had the procedure shown in Figure 7 performed 5 years ago. When converting this patient to a total knee arthroplasty (TKA), what patellar problem is commonly encountered intraoperatively?
1- Fracture
2- Patella baja
3- Patella alta
4- Osteonecrosis
5- Maltracking
PREFERRED RESPONSE: 2**
**DISCUSSION: Patella baja is commonly encountered when converting a high tibial osteotomy (HTO) to a TKA. Patella baja most likely occurs because of scarring. Meding and associates’ study did not show an increased rate of lateral release when converting a knee that had undergone a previous HTO.**
**REFERENCES: Yoshino N, Shinro T: Total knee arthroplasty after failed high tibial osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA,
JB Lippincott, 2003, vol 2, pp 1265-1271.**
**Meding JB, Keating EM, Ritter MA, et al: Total knee arthroplasty after high tibial osteotomy:
A comparison study in patients who had bilateral total knee replacement. J Bone Joint Surg Am 2000;82:1252-1259.**
**14/. Antibiotic-loaded bone cement prostheses, such as that shown in Figure 8, are best created by using which of the following methods?
1- Using commercially available antibiotic-loaded bone cement
2- Adding 0.5 g vancomycin to commercially available antibiotic-loaded bone cement
3- Adding 0.5 g tobramycin and 0.5 g vancomycin/unit of standard bone cement
4- Adding either 1.0 g vancomycin or 1.2 g tobramycin per 40 g of standard bone cement
5- Adding a minimum of 3.6 g tobramycin and 1.0 g vancomycin per 40 g of bone cement
PREFERRED RESPONSE: 5**
**DISCUSSION: In a review of the practical applications of antibiotic-loaded bone cement for the treatment of the infected total joint arthroplasties, Hanssen and Spangehl described commercially available antibiotic-loaded bone cement as low-dose antibiotic cements. These cements generally contained 0.5 g of either tobramycin or gentamicin per 40 g of cement. They are indicated for use in prophylaxis and not for treatment of infected total joint arthroplasties.
High-dose antibiotic-loaded bone cements are described as those containing greater than 1.0 g of antibiotic per 40 g of cement. Effective elution levels have been documented with 3.6 g tobramycin and 1.0 g vancomycin per 40 g of bone cement. This was documented by Penner and associates. Furthermore, it was shown that the combination of the two antibiotics in the bone cement improved the elution of both antibiotics.**
**REFERENCES: Hanssen AD, Spangehl MJ: Practical applications of antibiotic-loaded bone cement for treatment of infected joint replacements. Clin Orthop 2004;427:79-85.**
**Penner MJ, Masri BA, Duncan CP: Elution characteristics of vancomycin and tobramycin combined in acrylic bone-cement. J Arthroplasty 1996;11:939-944.**
**15/. Figures 9a and 9b show the radiographs of a 75-year-old man who underwent a revision total knee arthroplasty with a long-stemmed tibial component. In rehabilitation, he reports fullness and tenderness in the proximal medial leg (at the knee). The strategy that would best limit this postoperative problem is use of
1- a base plate with an offset tibial stem attachment.
2- a bone ingrowth surface on the augment.
3- a nonstemmed tibial base plate.
4- allograft bone instead of metal augments.
5- bone cement to smooth the outline of the proximal medial tibia.
PREFERRED RESPONSE: 1**
**DISCUSSION: The problem with this reconstruction is the medial protrusion of the base plate. The use of a base plate with an offset stem can prevent the protrusion and thus the impingement and pain. Allograft bone or smoothing the outline with cement would be just as prominent and likely to cause pain. An ingrowth surface may improve soft-tissue attachment but would still leave the implant protruding medially and likely to cause pain. A nonstemmed tibial base plate would lead to less medial protrusion but at the expense of a smaller area for load carriage on the proximal tibia.**
**REFERENCE: Gustke K: Cemented tibial stems are not requisite in revision. Orthopedics 2004;27:991-992.**
**16/. Figure 10 shows the AP radiograph of an ambulatory 76-year-old patient. What is the most appropriate surgical treatment option for this patient?
1- Revision arthroplasty using a cemented femoral component
2- Impaction allografting of the femoral component
3- Proximal femoral replacement arthroplasty
4- Resection arthroplasty
5- Hip arthrodesis
PREFERRED RESPONSE: 3**
**DISCUSSION: The patient has a periprosthetic fracture around a loose cemented femoral component. The proximal bone stock is poor; therefore, this fracture may be categorized as Vancouver 3-B. Hip arthrodesis and resection arthroplasty provide suboptimal results, particularly for ambulatory patients. Although impaction allografting may be an option to restore the bone stock in a younger patient, the latter procedure will be very difficult to perform when the proximal bone is poor in quality and fractured. Cementing another component into this wide femur is not an option. The best option for revision of the femoral component in this elderly patient is proximal femoral replacement arthroplasty.**
**REFERENCES: Malkani AL, Settecerri JJ, Sim FH, et al: Long-term results of proximal femoral replacement for non-neoplastic disorders. J Bone Joint Surg Br 1995;77:351-356.**
**Parvizi J, Sim FH: Proximal femoral replacements with megaprostheses. Clin Orthop 2004;420:169-175.**
**17/. A 74-year-old woman has had acute medial right knee pain for the past 3 months. She denies any history of trauma or previous problems. Coronal and sagittal MRI scans are shown in Figures 11a and 11b. What is the most likely diagnosis?
1- Osteoarthritis
2- Rheumatoid arthritis
3- Medial meniscal tear
4- Osteonecrosis
5- Transient osteoporosis
PREFERRED RESPONSE: 4**
**DISCUSSION: Spontaneous osteonecrosis of the medial femoral condyle is seen in the MRI scans, and is most common in women older than age 60 years. Although usually present in the weight-bearing portion of the medial femoral condyle, spontaneous osteonecrosis has also been described involving the lateral femoral condyle and patella. Most patients are seen postcollapse, and the treatment of choice is arthroplasty. Optimal treatment in precollapse stages is controversial.**
**REFERENCES: Kidwai AS, Hemphill SD, Griffiths HJ: Spontaneous osteonecrosis of the knee reclassified as insufficiency fracture. Orthopedics 2005;28:236,333-336.**
**Soucacos PN, Xenakis TH, Beris AE, et al: Idiopathic osteonecrosis of the medial femoral condyle: Classification and treatment. Clin Orthop 1997;341:82-89.**
**Yamamoto T, Bullough PG: Spontaneous osteonecrosis of the knee: The result of subchondral insufficiency fracture. J Bone Joint Surg Am 2000;82:858-866.**
**18/. Patients with patellar clunk syndrome are best managed by which of the
following methods?
1- Rest and nonsteroidal anti-inflammatory drugs
2- Surgical debridement
3- Patellectomy
4- Patellar revision
5- Lateral release/patellar realignment
PREFERRED RESPONSE: 2**
**DISCUSSION: Patellar clunk syndrome is usually the result of a fibrous nodule that forms on the undersurface of the distal quadriceps tendon. It may get entrapped in the intercondylar notch of the femoral component during flexion, and lead to a sudden snap as the nodule is pulled out of the notch during active extension. Nonsurgical management is rarely successful. Surgical debridement is usually curative, with only rare recurrence. More aggressive procedures such as realignment, revision, or patellectomy are usually not necessary, and are reserved for cases resistant to soft-tissue debridement.**
**REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 329.**
**Diduch DR, Scuderi GR, Scott WN, et al: The efficacy of arthroscopy following total knee replacement. Arthroscopy 1997;13:166-171.**
**Lucas TS, DeLuca PF, Nazarian DG, et al: Arthroscopic treatment of patellar clunk. Clin Orthop 1999;367:226-229.**
**19/. Increasing articular conformity of the tibial polyethylene insert of a fixed-bearing
total knee arthroplasty (TKA) prosthesis will have which of the following
biomechanical effects?
1- Decreased contact stress within the polyethylene
2- Decreased risk of patellofemoral instability
3- Decreased risk of mechanical loosening
4- Increased risk of subsurface polyethylene cracking
5- Increased tibial rollback during flexion
PREFERRED RESPONSE: 1**
**DISCUSSION: Increasing articular conformity increases the surface area for contact between the polyethylene and the femoral component. Advantages of this include lower peak contact stress within the polyethylene and less risk of polyethylene fatigue failure. Patellofemoral tracking is unchanged by increasing conformity unless gross component apposition is present. A potential disadvantage of increasing conformity includes some restriction in tibial rollback. Modest changes in conformity have not been shown to alter the rate of mechanical loosening. If conformity was increased to the extent of significant constraint, a potential increased risk of loosening would be expected, not a decrease. Design of modern TKAs includes a compromise in achieving enough constraint to lower polyethylene stress, without providing so much constraint as to limit kinematics and stress the fixation interfaces.**
**REFERENCES: D’Lima DD, Chen PC, Colwell CW Jr: Polyethylene contact stresses, articular congruity, and knee alignment. Clin Orthop 2001;392:232-238.**
**Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 265-274.**
**20/. A 63-year-old woman reports giving way of the knee and pain after undergoing primary total knee arthroplasty (TKA) 1 year ago. Examination reveals that the knee is stable in full extension but has gross anteroposterior instability at 90 degrees of flexion. The patient can fully extend her knee with normal quadriceps strength. Studies for infection are negative. AP and lateral radiographs are shown in Figures 12a and 12b, respectively. What is the appropriate management?
1- Anti-inflammatory drugs
2- Knee brace
3- Physical therapy for quadriceps strengthening
4- Revision to a thicker polyethylene insert
5- Revision to a larger, posterior stabilized implant
PREFERRED RESPONSE: 5**
**DISCUSSION: The radiographs show posterior flexion instability that is the result of a
flexion-extension gap imbalance and posterior cruciate ligament incompetence after a posterior cruciate ligament-retaining TKA. The femur is anteriorly displaced on the tibia, with lift-off of the femoral component from the tibial polyethylene. Revision to a larger femoral component will address the larger flexion gap relative to the extension gap, and a posterior stabilized implant will address the posterior cruciate ligament insufficiency. Pagnano and associates, reporting on a series of painful TKAs previously diagnosed as pain of unknown etiology, showed that the pain was secondary to flexion instability. Pain relief was achieved by revision to a posterior stabilized implant.**
**REFERENCES: Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary posterior cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46.**
**Fehring TK, Valadie AL: Knee instability after total knee arthroplasty. Clin Orthop 1994;299:157-162.**
**Fehring TK, Odum S, Griffin WL, et al: Early failures in total knee arthroplasty. Clin Orthop 2001;392:315-318.**
**21/. A 72-year-old woman who underwent right total hip arthroplasty 7 years ago now
reports right hip pain and limb shortening. Studies for infection are negative. AP
and lateral radiographs are shown in Figures 13a and 13b. What is the most
appropriate management?
1- Observation only
2- Nonsteroidal anti-inflammatory drugs and protected weight bearing
3- Revision of the acetabular component with a jumbo cup with screws
4- Revision of the acetabular component with a reinforcement cage and bone grafting
5- Resection arthroplasty
PREFERRED RESPONSE: 4**
**DISCUSSION: Current literature supports the use of reinforcement cages for the reconstruction of failed, loosened acetabular components associated with major bone loss as seen in this patient. Although results of revision using the so-called jumbo cup with screws generally have been good, the amount of bone loss and medial wall penetration shown here and the likelihood of pelvic discontinuity precludes the use of that technique. With either technique, bone grafting of remaining defects is recommended.**
**REFERENCES: Sporer SM, O’Rourke M, Paprosky WG: The treatment of pelvic discontinuity during acetablular revision. J Arthroplasty 2005;20:79-84.**
**Paprosky WG, O’Rourke M, Sporer SM: The treatment of acetabular bone defects with an associated pelvic discontinuity. Clin Orthop 2005;441:216-220.**
**22/. What is the most prevalent adverse event associated with allogeneic blood transfusion?
1- Clerical error leading to transfusion reaction
2- Anaphylactic reaction
3- HIV transmission
4- Hepatitis C transmission
5- Bacterial contamination leading to sepsis/shock
PREFERRED RESPONSE: 1**
**DISCUSSION: Clerical error leading to acute hemolysis and even death occurs in 1:12,000 to 1:50,000 transfusions. Bacterial contamination leading to sepsis/shock occurs in 1:1 million transfusions. HIV transmission is approximately 1:500,000 transfusions and hepatitis C is 1:103,000 transfusions. Anaphylactic reactions occur in 1:150,000 transfusions.**
**REFERENCES: Aubuchon JP, Birkmeyer JD, Busch MP: Safety of the blood supply in the United States: Opportunities and controversies. Ann Intern Med 1997;127:904-909.**
**Popovsky MA, Whitaker B, Arnold NL: Severe outcomes of allogeneic and autologous blood donation: Frequency and characterization. Transfusion 1995;35:734-737.**
**23/. At the time of the revision surgery shown in Figure 14, the acetabular component was found to be stable. Polyethylene exchange with a standard ultra-high molecular weight polyethylene liner and grafting was performed. The patient is at significantly increased risk for
1- loosening of the femoral component.
2- loosening of the acetabular component.
3- prosthetic hip dislocation.
4- rapid wear of the polyethylene.
5- continued expansion of the lytic defects.
PREFERRED RESPONSE: 3**
**DISCUSSION: Maloney and associates reported a 35% increased risk of pelvic osteolysis after total hip arthroplasty with a porous-coated acetabular component without cement. All components were stable at the time of revision. Only liners were exchanged and debridement of the granuloma with or without bone graft was performed. No defects progressed and one third of the lesions were no longer visible on radiographs, regardless of bone grafting. Unfortunately, despite the technical ease of many of these types of revisions, the dislocation rate for these cases is significant. Precautions should be taken postoperatively, and patients should be educated about this risk preoperatively.**
**REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 411-424.**
**Boucher HR, Lynch C, Young AM, et al: Dislocation after polyethylene liner exchange in total hip arthroplasty. J Arthroplasty 2003;18:654-657.**
**Maloney WJ, Herzwurm P, Paprosky W, et al: Treatment of pelvic osteolysis associated with a stable acetabular component inserted without cement as part of a total hip replacement. J Bone Joint Surg Am 1997;79:1628-1634.**
**24/. What is the most frequent complication of both lateral closing wedge high tibial osteotomy and medial opening wedge osteotomy?
1- Patella baja
2- Fracture
3- Peroneal nerve palsy
4- Compartment syndrome
5- Infection
PREFERRED RESPONSE: 1**
**DISCUSSION: Scuderi and associates reported on patellar height after a high tibial osteotomy. Eighty-nine percent of the patellae, as measured by the Insall-Salvati index, and 76.3 percent, as measured by the Blackburne-Peel index, were observed to be lowered. More recently, Wright and associates reported a 64% incidence of patella baja in patients undergoing a medial opening wedge osteotomy. The incidence of intra-articular fracture during medial opening wedge osteotomy has been reported to be as high as 11% by Hernigou and associates, whereas the incidence of intra-articular fracture during lateral closing wedge high tibial osteotomy has been reported to be 10% to 20% by Matthews and associates. The incidence of peroneal nerve palsy with a lateral closing wedge high tibial osteotomy ranges from 0% to 20%, according to Marti and associates, whereas the incidence of peroneal palsy following a medial opening wedge osteotomy has been reported to be 15.7% by Flierl and associates. The exact incidence of compartment syndrome after a high tibial osteotomy is not known; however, it does not reach the level of patella baja. The incidence of deep infection after a lateral closing wedge high tibial osteotomy ranges from 0% to 4% according to Billings and associates.**
**REFERENCES: Scuderi GR, Windsor RE, Insall JN: Observations on patellar height after proximal tibial osteotomy. J Bone Joint Surg Am 1989;71:245-248.**
**Wright JM, Crockett HC, Slawski DP, et al: High tibial osteotomy. J Am Acad Orthop Surg 2005;13:279-289.**
**Hernigou P, Medevielle D, Debeyre J, et al: Proximal tibial osteotomy for osteoarthritis
with varus deformity: A ten to thirteen-year follow-up study. J Bone Joint Surg Am 1987;69:332-354.**
**Matthews LS, Goldstein SA, Malvitz TA, et al: Proximal tibial osteotomy: Factors that influence the duration of satisfactory function. Clin Orthop 1988;229:193-200.**
**Marti CB, Gautier E, Wachtl SW, et al: Accuracy of frontal and sagittal plane correction in open-wedge high tibial osteotomy. Arthroscopy 2004;20:366-372.**
**Marti RK, Verhigan RA, Kerkhoffs GM, et al: Proximal tibial varus osteotomy: Indications, technique, and five to twenty-one-year results. J Bone Joint Surg Am 2001;83:164-170.**
**Flierl S, Sabo D, Hornig K, et al: Open wedge high tibial osteotomy using fractioned drill osteotomy: A surgical modification that lowers the complication rate. Knee Surg Sports Traumatol Arthrosc 1996;4:149-153.**
**Billings A, Scott DF, Camargo MP, et al: High tibial osteotomy with a calibrated osteotomy guide, rigid internal fixation, and early motion: Long-term follow-up. J Bone Joint Surg Am 2000;82:70-79.**
**25/. Stiffness can occur following total knee arthroplasty. What is the most appropriate management for a patient who has deteriorating arc of motion after undergoing a revision knee arthroplasty 9 months ago?
1- Aggressive physical therapy
2- Manipulation under anesthesia
3- Investigation for periprosthetic infection
4- Revision knee arthroplasty
5- Resection arthroplasty
PREFERRED RESPONSE: 3**
**DISCUSSION: Stiffness following total knee arthroplasty can be a disabling condition. There are many reasons for loss of knee motion following total knee arthroplasty. Technical errors, such as overstuffing of the patella, malpositioning of the components, and ligamentous imbalance, are all known to result in stiffness following total knee arthroplasty. In some patients with a possible genetic predisposition, aggressive arthrofibrosis may develop and result in loss of knee motion. In any patient who has deteriorating knee motion, particularly after revision arthroplasty, deep infection should be ruled out. Although on occasion surgical intervention may be required to address knee stiffness, the outcome of revision surgery is poor if no reason for stiffness can be determined.**
**REFERENCES: Kim J, Nelson CL, Lotke PA: Stiffness after total knee arthroplasty: Prevalence of the complication and outcomes of revision. J Bone Joint Surg Am 2004;86:1479-1484.**
**Gonzalez MH, Mekhail AO: The failed total knee arthroplasty: Evaluation and etiology. J Am Acad Orthop Surg 2004;12:436-446.**
**26/. A 59-year-old woman who underwent a total hip arthroplasty 5 years ago now has recurrent dislocation following bariatric surgery and a weight loss of 200 lb. An attempt at converting to a larger head size and trochanteric advancement has failed. Her components are well aligned. What is the best course of action?
1- Resection arthroplasty
2- Hip abduction brace
3- Constrained acetabular liner
4- Thermal ablation of the posterior capsule
5- Conversion to a bipolar prosthesis
PREFERRED RESPONSE: 3**
**DISCUSSION: When a patient has well-aligned components and soft-tissue tensioning with a larger femoral head and trochanteric advancement has failed, options are limited. The use of a constrained acetabular liner is the best option in this situation. Goetz and associates and Shrader and associates have demonstrated good results with these implants. Shrader used this device on 109 patients with recurrent instability with a successful outcome in all but 2 patients. Resection arthroplasty is a salvage situation and is not the best option at the present time. A hip abduction brace does not address the soft-tissue laxity. Conversion to a bipolar arthroplasty, although possibly minimizing the incidence of dislocation, will lead to groin pain and migration of the component with diminished functional results.**
**REFERENCES: Goetz DD, Capello WN, Callaghan JJ, et al: Salvage of recurrently
dislocating hip prosthesis with use of a constrained acetabular component: A retrospective analysis of fifty-six cases. J Bone Joint Surg Am 1998;80:502-509.**
**Shrader MW, Parvizi J, Lewallen DG: The use of constrained acetabular component to treat instability after total hip arthroplasty. J Bone Joint Surg Am 2003;85:2179-2183.**
**Hamilton WG, McAuley JP: Evaluation of the unstable total hip arthroplasty. Inst Course Lect 2004;53:87-92.**
**27/. Figure 15 shows the radiograph of an active 60-year-old woman. Which of the following variables is considered the strongest contraindication to a unicompartmental knee arthroplasty in this patient?
1- Obesity
2- Fixed varus deformity of more than 15 degrees
3- Five degree flexion contracture
4- Contralateral knee osteoarthritis
5- Joint subluxation of 5 mm
PREFERRED RESPONSE: 2**
**DISCUSSION: Unicompartmental arthroplasty of the knee for single compartment arthrosis has recently become more popular. Contraindications to unicompartmental knee arthroplasty include fixed varus or valgus deformity of more than 5 degrees, restricted range of motion, fixed flexion contracture, joint subluxation of 5 mm or greater, and arthrosis of the opposite and/or patellofemoral compartment.**
**REFERENCES: Cossey AJ, Spriggins AJ: The use of computer-assisted surgical navigation to prevent malalignment in unicompartmental knee arthroplasty. J Arthroplasty 2005;20:29-34.**
**Iorio R, Healy WL: Unicompartmental arthritis of the knee. J Bone Joint Surg Am 2003;85:1351-1364.**
**Argenson JN, Chevrol-Benkeddache Y, Aubaniac JM: Modern unicompartmental knee arthroplasty with cement: A three to ten-year follow-up study. J Bone Joint Surg Am 2002;84:2235-2239.**
**28/. Figure 16 shows the radiograph of an otherwise healthy 62-year-old woman who fell. Management should consist of
1- revision total hip arthroplasty with a cemented femoral component and adjuvant fracture fixation.
2- revision total hip arthroplasty with a cementless femoral component and adjuvant fracture fixation.
3- open reduction and internal fixation of the fracture and retention of the original components.
4- removal of the components, open reduction and internal fixation of the fracture, and delayed replantation of the components when the fracture is healed.
5- resection arthroplasty and internal fixation of the fracture.
PREFERRED RESPONSE: 2**
**DISCUSSION: The radiograph reveals that the femoral component is grossly loose as evidenced by disruption of the cement column; therefore, retention of the original components will not yield a successful outcome. A cementless revision is the procedure of choice. A strut graft and/or plate may be added at the surgeon’s discretion. A resection arthroplasty would only be considered in a nonambulatory patient. Cemented fixation of the revision component would be problematic given the numerous fracture fragments and the inability to contain the cement.**
**REFERENCES: Springer BD, Berry DJ, Lewallen DG: Treatment of periprosthetic fractures following total hip arthroplasty with femoral component revision. J Bone Joint Surg Am 2003;85:2156-2162.**
**Duwelius PJ, Schmidt AH, Kyle RF, et al: A prospective, modernized treatment protocol for periprosthetic femur fractures. Orthop Clin North Am 2004;35:485-492.**
**29/. Which of the following is the strongest contraindication to unicompartmental knee arthroplasty (UKA)?
1- Patient age of younger than 60 years
2- Patient age of older than 80 years
3- Anterior cruciate ligament (ACL) deficiency
4- Varus deformity of 5 degrees
5- Outerbridge grade II chondromalacia of the patella
PREFERRED RESPONSE: 3**
**DISCUSSION: UKA prostheses cannot substitute for an absent ACL, and if arthroplasty is indicated, these patients should receive a total knee arthroplasty rather than a UKA. Age is not an absolute contraindication, and the procedure has been advocated for young patients as well as older patients if they meet the appropriate indications for an arthroplasty. Varus deformities of the mechanical axis of up to 10 degrees generally are not a contraindication to unicompartmental arthroplasty, as long as the knee can be properly balanced at the time of surgery. Modest chondromalacia of the patellofemoral joint, especially if asymptomatic, is not a contraindication to UKA.**
**REFERENCES: Lotke PA (ed): Knee Arthroplasty: Master Techniques in Orthopaedic Surgery. New York, NY, Raven Press, 1995, pp 275-293.**
**Insall JN, Windsor RE, Scott WN, et al (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 805-814.**
**Tabor OB Jr, Tabor OB: Unicompartmental arthroplasty: A long-term follow-up study.
J Arthroplasty 1998;13:373-379.**
**30/. Figure 17 shows the AP radiograph of a 75-year-old man with right hip pain. The femoral component is loose. The mechanism of loosening is most likely secondary to
1- osteolysis.
2- fatigue failure of the implant.
3- failure of bone ingrowth.
4- wear debris from cerclage wire.
5- trochanteric impingement.
PREFERRED RESPONSE: 3**
**DISCUSSION: The femoral construct shown in the radiograph has failed to produce ingrowth of the stem. The stem has subsided and rotated. Impingement of the trochanter did not occur until after the stem subsided. There is no evidence of osteolysis or third-body wear debris from the cerclage wire. A larger femoral stem needs to be implanted to achieve rigid fixation.**
**REFERENCES: Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 217-238.**
**Peter CL, Rivero DP, Kull LR, et al: Revision total hip arthroplasty without cement: Subsidence of proximally porous-coated femoral components. J Bone Joint Surg Am 1995;77:1217-1226.**
**31/. A 75-year-old woman undergoes hybrid total hip arthroplasty for osteoarthritis. A postoperative radiograph obtained in the recovery room is shown in Figure 18. Treatment should now consist of
1- open reduction and internal fixation with strut graft and cerclage wire.
2- open reduction and internal fixation with a plate, screws, and bone graft.
3- exchange of the femoral components with insertion of a long stem cementless implant.
4- cast immobilization.
5- minimal weight bearing and observation.
PREFERRED RESPONSE: 5**
**DISCUSSION: Intraoperative femoral fractures can often be avoided by careful preoperative planning to optimize implant design and size. Most fractures occur during implantation of a cementless implant; many can be avoided by careful femoral preparation and component implantation, with particular caution in osteopenic bone. Intraoperative femoral fractures are managed according to fracture severity. Minor cracks that do not affect stability or femoral integrity can often be managed intraoperatively with cerclage fixation, limited weight bearing, and observation. Femoral fractures that compromise implant stability or femoral integrity require fracture fixation with cerclage wires, strut grafts, or plates and may require conversion to a long stem implant. This patient’s fracture is nondisplaced and the implant is well seated; therefore, limited weight bearing is considered appropriate management.**
**REFERENCES: Lee SR, Bostrom MP: Periprosthetic fractures of the femur after total hip arthroplasty. Instr Course Lect 2004;53:111-118.**
**Kelley SS: Periprosthetic femoral fractures. J Am Acad Orthop Surg 1994;2:164-172.**
**Berry DJ: Management of periprosthetic fractures: The hip. J Arthroplasty 2002;17:11-13.**
**32/. A 42-year-old man undergoes right total hip arthroplasty for hip dysplasia. Postoperatively, he has a significant limb-length increase with a foot drop. A preoperative radiograph is shown in Figure 19. Which of the following should have been considered preoperatively to avoid this complication?
1- Medialization of the acetabular component
2- Use of a modular femoral implant
3- Anterolateral approach to the hip
4- Femoral shortening
5- Electromyography
PREFERRED RESPONSE: 4**
**DISCUSSION: In a patient with bilateral hip dysplasia, there are significant technical challenges that need to be addressed to ensure a successful total hip arthroplasty. Restoring the center of the hip may cause significant lengthening and require femoral shortening. Lengthening of greater than 4 cm can lead to sciatic nerve palsy that will present clinically as a foot drop. A high hip center can be used when there is inadequate bone stock in the acetabulum to achieve adequate host bone coverage. A modular femoral implant may be used for a dysplastic hip with significant rotational deformity. Although an anterolateral approach to the hip may decrease the incidence of sciatic nerve palsy during the exposure, it will not be helpful when there is more than 4 cm of limb lengthening.**
**REFERENCES: Schmalzried TP, Amstutz HC, Dorey FJ: Nerve palsy associated with total hip replacement: Risk factors and prognosis. J Bone Joint Surg Am 1991;73:1074-1080.**
**Papagelopoulos PJ, Trousdale RT, Lewallen DG: Total hip arthroplasty with femoral osteotomy for proximal femoral deformity. Clin Orthop 1996;332:151-162.**
**Huo MH, Zatorski LE, Keggi KJ: Oblique femoral osteotomy in cementless total hip arthroplasty: Prospective consecutive series with a 3-year minimum follow-up period.**
**J Arthroplasty 1995;10:319-327.**
**33/. A 58-year-old man reports a 2-month onset of groin pain with no history of trauma. Examination reveals that range of motion of the hip is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figure 20. Treatment should consist of
1- protected weight bearing and anti-inflammatory drugs.
2- core decompression of the femoral head.
3- vascularized free fibular grafting to the femoral head.
4- bipolar hemiarthroplasty of the hip.
5- total hip arthroplasty.
PREFERRED RESPONSE: 1**
**DISCUSSION: The MRI findings show highly increased signal through the entire femoral head and neck on STIR imaging, diagnostic of transient osteoporosis of the femoral head. This disease entity can be seen in middle-aged men, and should be treated nonsurgically. The natural history is that of self-resolution.**
**REFERENCES: Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.**
**Urbanski SR, de Lange EE, Eschenroeder HC Jr: Magnetic resonance imaging of transient osteoporosis of the hip: A case report. J Bone Joint Surg Am 1991;73:451-455.**
**34/. Figure 21 shows the radiograph of a 32-year-old patient with right hip pain that has failed to respond to nonsurgical management. What is the most appropriate surgical treatment at this time?
1- Femoral derotational osteotomy
2- Total hip arthroplasty
3- Arthrodesis
4- Surgical dislocation of the hip
5- Periacetabular osteotomy
PREFERRED RESPONSE: 5**
**DISCUSSION: The radiograph reveals developmental dysplasia of both hips. The patient has classic anterolateral undercoverage of the femoral head on the right side as demonstrated by a high acetabular index (measured at 27 degrees). Anterior undercoverage can be determined by drawing the marking for the anterior wall that fails to overlap the femoral head in this patient. Currently in North America, the most accepted surgical management for symptomatic dysplasia of the hip with good joint space is a Bernese (Ganz) periacetabular osteotomy. Surgical dislocation of the hip and femoroacetabular osteoplasty may be considered for patients with symptomatic femoroacetabular impingement of the hip.**
**REFERENCES: Ganz R, Klaue K, Vinh TS, et al: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.**
**Trousdale RT, Ekkernkamp A, Ganz R, et al: Periacetabular and intertrochanteric osteotomy for the treatment of osteoarthrosis in dysplastic hips. J Bone Joint Surg Am 1995;77:73-85.**
**35/. A patient reports pain in the hip with functional positioning. With the patient supine, pain in which of the following positions would be typical for femoral acetabular impingement?
1- Hip is internally rotated, passively flexed to 90 degrees, and adducted
2- Hip is internally rotated, passively flexed to 90 degrees, and abducted
3- Hip is externally rotated, maximally flexed to 90 degrees, and adducted
4- Hip is externally rotated, passively flexed to 90 degrees, and abducted
5- Hip is externally rotated, maximally flexed, and abducted
PREFERRED RESPONSE: 1**
**DISCUSSION: Patients with dysplasia often have a hypertrophic labrum. Abnormal contact between the femoral neck and the acetabular rim leads to labral injury, especially in the anterior-superior acetabular zone. Typically, young patients with the condition report pain with activity or long periods of sitting or driving. The hips often have limited motion, in particular in internal rotation and flexion. Forceful adduction with the maneuver causes pain.**
**REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 411-424.**
**Beck M, Leunig M, Parvizi J, et al: Anterior femoroacetabular impingement: Part II. Midterm results of surgical treatment. Clin Orthop 2004;418:67-73.**
**McCarthy JC, Noble PC, Schuck MR, et al: The role of labral lesions to development of early degenerative hip disease. Clin Orthop 2001;393:25-37.
36/. A patient who underwent a total knee arthroplasty for osteoarthritis 18 months ago now reports the sudden development of pain in the ipsilateral knee. Radiographs and examination of the knee are unremarkable. Aspiration of the synovial fluid 3 days later reveals a WBC count of 1,500/mm3. The cells consist of 30% neutrophils and 70% monocytes. Culture results will not be available for several days. The patient has not been on antibiotics prior to this point. Based on these findings, what is the most appropriate management?
1- Arthrotomy, debridement, and polyethylene exchange
2- One-stage exchange arthroplasty
3- Two-stage exchange arthroplasty
4- Parenteral antibiotics
5- Nonsurgical management without antibiotics
PREFERRED RESPONSE: 5
DISCUSSION: Synovial fluid analysis is a very sensitive tool for detecting infection in total knee arthroplasties. Several studies have demonstrated that an absolute leukocyte count in the synovial fluid of less than 1,700 to 2,500/mm3 is an accurate predictor of absence of infection. Similarly, a differential cell count of the WBCs demonstrating less than 50% to 60% neutrophils is an accurate predictor of absence of infection. If both parameters are normal, it is unlikely that the patient has an infection. The three surgical options are contraindicated based on the normal examination findings and laboratory parameters. Similarly, antibiotics should be avoided. The work-up should include tests to evaluate noninfectious sources of knee pain and sources of referred knee pain.
REFERENCES: Trampuz A, Hanssen AD, Osmon DR, et al: Synovial fluid leukocyte count and differential for the diagnosis of prosthetic knee infection. Am J Med 2004;117:556-562.**
**Mason JB, Fehring TK, Odum SM, et al: The value of white blood cell counts before revision total knee arthroplasty. J Arthroplasty 2003;18:1038-1043.**
**Kersey R, Benjamin J, Mason B: White blood cell counts and differential in synovial fluid of aseptically failed total knee arthroplasty. J Arthroplasty 2000;15:301-304.**
**37/. A 38-year-old man who is an avid tennis player has had persistent pain over the medial aspect of his knee for the past 6 years. He notes that the pain occurs on a daily basis with any significant activity. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 22a and 22b. What is the best course of action?
1- Total knee arthroplasty
2- Unicompartmental arthroplasty
3- Insertion of a unispacer
4- Tibial osteotomy
5- Knee arthroscopy
PREFERRED RESPONSE: 4**
**DISCUSSION: In a relatively young patient who is an avid tennis player, the treatment of choice is a joint preserving procedure. The radiographs reveal varus alignment with loading of the medial compartment. After all nonsurgical management options have been used, the best treatment option is a medial opening wedge osteotomy. A lateral closing wedge osteotomy of the proximal tibia is also a reasonable option, but it is not one of the choices. A unicompartmental arthroplasty or a total knee arthroplasty would place significant restrictions in this patient. A unispacer may be a temporizing procedure but is controversial and without substantial data in the literature. The knee arthroscopy will not address the medial compartment osteoarthritis.**
**REFERENCES: Nagel A, Insall JN, Scuderi GR: Proximal tibial osteotomy: A subjective outcome study. J Bone Joint Surg Am 1996;78:1353-1358.**
**Rinonapoli E, Mancini GB, Corvaglia A, et al: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.**
**Manifold SG, Kelly MA, Richardson L, et al: Osteotomies about the knee, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 947-961.**
**38/. Which of the following statements best describes the outcome of the routine use of continuous passive motion (CPM) machines after total knee arthroplasty (TKA)?
1- CPM is likely to improve early range of motion and final range of motion.
2- CPM may improve early range of motion but is unlikely to improve final range of motion.
3- CPM is likely to decrease postoperative pain.
4- CPM is likely to improve extension but not flexion.
5- CPM is likely to restore quicker ambulatory ability.
PREFERRED RESPONSE: 2**
**DISCUSSION: Although CPM machines are used widely in the United States for patients undergoing TKA, the benefit seems to be marginal, if any. Numerous randomized trials have shown that final outcomes after total knee arthroplasty are unaffected by the use of CPM machines postoperatively. Some studies have suggested that use of CPM may improve flexion in the first few weeks, but any short-term benefit from the machine was lost by intermediate-term follow-up. Aside from potential improvement in flexion within the first few postoperative weeks, there does not appear to be any benefit from the machines. There is no improvement in pain, ambulation, or extension. The cost-effectiveness of these machines has been questioned by many authors.**
**REFERENCES: Pellicci PM, Tria AJ, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 287-293.**
**McInnes J, Larson MG, Daltroy LH, et al: A controlled evaluation of continuous passive motion in patients undergoing total knee arthroplasty. JAMA 1992;268:1423-1428.**
**Kumar PJ, McPherson EJ, Dorr LD, et al: Rehabilitation after total knee arthroplasty: A comparison of 2 rehabilitation techniques. Clin Orthop 1996;331:93-101.**
**39/. When performing knee arthroplasty, which of the following procedures provides the most consistent fixation for the tibial component?
1- Cementless fixation of the tibial component
2- Augmenting cementless fixation of the tibial component with pegs or screws
3- Cementing the metaphyseal portion and press fitting the keel of the tibial component
4- Cementing the metaphyseal and keel portions of the tibial component
5- Cemented fixation of the tibial component with screws
PREFERRED RESPONSE: 4**
**DISCUSSION: All of the options, except cementing the metaphyseal portion and press fitting the keel of the tibial component, have been shown to create strong and long-lasting constructs; however, cementing of both the platform and the keel offers the most predictable solution. Cementing the platform and not the keel has been shown to have a higher loosening rate than the more traditional methods of fully cementing or using screws to augment fixation.**
**REFERENCE: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 457-468.**
**40/. Sterilization of ultra-high molecular weight polyethylene by gamma irradiation in air will degrade its wear performance because of
1- oxidation.
2- melting.
3- cross-linking.
4- corrosion.
5- creep.
PREFERRED RESPONSE: 1**
**DISCUSSION: Gamma irradiation has long been used as a sterilization method for polyethylene. Exposure to gamma irradiation causes breakage of the chemical bonds in the polyethylene, and oxidation will occur if the material is subsequently exposed to air. The amount of oxidation and decrease in wear performance is also related to the length of time that the gamma-irradiated polyethylene is exposed to oxygen.**
**REFERENCES: Collier JP, Sutula LC, Currier BH, et al: Overview of polyethylene as a bearing material: Comparison of sterilization methods. Clin Orthop 1996;333:76-86.**
**McKellop H, Shen FW, Lu B, et al: Effect of sterilization method and other modifications on the wear resistance of acetabular cups made of ultra-high molecular weight polyethylene: A hip-simulator study. J Bone Joint Surg Am 2000;82:1708-1725.**
**Sychterz CJ, Young AM, Orishimo K, et al: The relationship between shelf life and in vivo wear for polyethylene acetabular liners. J Arthroplasty 2005;20:168-173.**
**41/. Figure 23 shows failure of the femoral stem in a patient. What is the most likely reason for the failure?
1- Torsional loading
2- Cantilever bending
3- Pistoning
4- Subsidence
5- Torque
PREFERRED RESPONSE: 2**
**DISCUSSION: A two-dimensional stress analysis has been used to study the effects of some of the factors leading to early fatigue failure of the femoral stem in total hip arthroplasty. It has been demonstrated that loss of proximal stem support at the level of the calcar femorale and subsequent stem stress can lead to fatigue failure. In addition, the role of body weight and range of cyclic stress fluctuation play an important role in fatigue life under conditions where the stem has lost proximal support. These results indicate that stem design could be improved by incorporating some means of adequate support at the calcar femorale where maximum tensile stresses are found to occur. Femoral component fracture is a rare but well-documented complication after total hip arthroplasty. Historically, most stem fractures occur at the middle third of the implant where proximal stem loosening and solid distal stem fixation result in cantilever bending and eventual fatigue failure. The component shown is a modular fluted cementless stem that occasionally fractures at the modular junction in patients with poor proximal bone support.**
**REFERENCES: Andriacchi TP, Galante JO, Belytschko TB, et al: A stress analysis of the femoral stem in total hip prostheses. J Bone Joint Surg Am 1976;58:618-624.**
**Gruen TA, McNeice GM, Amstutz HC: “Modes of failure” of cemented stem-type femoral components: A radiographic analysis of loosening. Clin Orthop 1979;141:17-27.**
**42/. What property of titanium alloys accounts for their high corrosion resistance in vivo?
1- Self-passivation
2- Ductility
3- Hardness
4- Modulus of elasticity
5- Conductivity
PREFERRED RESPONSE: 1**
**DISCUSSION: In both room temperature air and physiologic fluids, titanium alloys self-passivate or spontaneously form a layer of titanium oxide very rapidly. This layer makes titanium alloys resistant to surface breakdown.**
**REFERENCES: Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, Lippincott, 2003, vol 1, pp 269-278.**
**Lemons JE: Metallic alloys, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 19-27.**
**43/. Which of the following aids in correction of patellar tracking after total knee arthroplasty (TKA)?
1- Internal rotation of the femoral component
2- Internal rotation of the tibial component
3- Increasing size of the tibial component
4- Medialization of the patellar component
5- Joint line elevation
PREFERRED RESPONSE: 4**
**DISCUSSION: Correct patellofemoral tracking has proven to be a crucial aspect in TKA because a large percent of problems after TKA are related to the patellofemoral articulation. External rotation of the femoral and tibial components has been shown to aid in tracking. Likewise, medialization of the patellar button aids in patellar tracking and prevention of lateral subluxations and dislocations. Attention to the distal femoral cut is critical in maintaining the joint line and preventing patella baja or alta. Tibial sizing, however, is not directly related to patellar tracking after TKA.**
**REFERENCES: Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 1245-1258.**
**Merkow RL, Soudry M, Insall JN: Patellar dislocation following total knee replacement. J Bone Joint Surg Am 1985;67:1321-1327.**
**44/. Figure 24 shows the radiograph of a 36-year-old volleyball player with right hip pain. What is the cause of the pain?
1- Osteonecrosis
2- Rheumatoid arthritis
3- Developmental dysplasia of the acetabulum
4- Femoral neck fracture
5- Femoral acetabular impingement
PREFERRED RESPONSE: 5**
**DISCUSSION: Femoral acetabular impingement usually presents in active young adults with the slow onset of groin pain that often starts after a minor trauma. Physical examination reveals limitation of motion with a positive impingement test which consists of forceful internal rotation with flexion and adduction. Femoral acetabular impingement is a mechanism for the development of early osteoarthritis in nondysplastic hips. Surgical debridement of the impinging, nonspherical portion of the femoral head restores offset and improves the clearance of the head, thus preventing abutment of the neck against the acetabular rim. The patient has no evidence of osteonecrosis, developmental dysplasia of the hip, rheumatoid arthritis, or femoral neck fracture.**
**REFERENCES: Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for osteoarthritis of the hip. Clin Orthop 2003;417:112-120.**
**Beck M, Leunig M, Parvizi J, et al: Anterior femoroacetabular impingement: Part II. Midterm results of surgical treatment. Clin Orthop 2004;418:67-73.**
**45/. Figure 25 shows the radiograph of an 84-year-old woman who has pain and is unable to extend her knee. History reveals that she underwent total knee arthroplasty 8 years ago. Aspiration and studies for infection are negative. During revision surgery, management of the tibial bone loss should consist of
1- reconstruction with a metal augmented revision tibial implant.
2- reconstruction with a hinged prosthesis.
3- reconstruction with a structural allograft.
4- reconstruction with iliac crest bone graft.
5- filling the defect with cement.
PREFERRED RESPONSE: 1**
**DISCUSSION: Massive bone loss encountered in revision total knee arthroplasty remains a significant challenge. Recent reports have shown high success rates using structural allograft to reconstruct large structural bone defects. A hinged prosthesis is not required in this setting. In this patient, a large amount of posterior cortex has been lost, making the area too large to fill with cement or iliac crest bone graft. Because of her age, the treatment of choice is a revision tibial implant and metal augments. Structural allograft would be suitable in a younger patient.**
**REFERENCES: Mow CS, Wiedel JD: Structural allografting in revision total knee arthroplasty. J Arthroplasty 1996;11:235-241.**
**Engh GA, Herzwurm PJ, Parks NL: Treatment of major defects of bone with bulk allografts and stemmed components during total knee arthroplasty. J Bone Joint Surg Am 1997;79:1030-1039.**
**Clatworthy MG, Ballance J, Brick GW, et al: The use of structural allograft for uncontained defects in revision total knee arthroplasty: A minimum five-year review. J Bone Joint Surg Am 2001;83:404-411.**
**46/. A 62-year-old woman with a bone mass density (BMD) T-score of -2.0 sustained a subcapital fracture of her hip. She is an avid tennis player, and history reveals no previous fractures. What is the most appropriate follow-up care?
1- Antiresorptive bisphosphonate medication
2- A repeat dual-energy x-ray absorptiometry scan (DEXA) and treatment if the
T-score is less than -2.5
3- A repeat DEXA scan and treatment if the T-score is greater than -1.5
4- No treatment since the BMD is not in osteoporotic range
5- (PTH) taraparatide hormone followed by surgery
PREFERRED RESPONSE: 1**
**DISCUSSION: A DEXA scan is most appropriately used to establish a baseline score. Even if the bone mineral density is not within the osteoporotic range (T-score less than -2.5), a prior fragility fracture is a strong risk factor for a second fracture as a result of factors other than bone density, such as worsening vision or balance, confusion, or other predispositions to falls. The guidelines of the National Osteoporosis Foundation indicate that, following a fragility hip fracture, active anti-osteoporotic medication should be initiated, whether or not a DEXA scan is performed. A recent study showed that antiresorptive therapy following a hip fracture reduces not only the risk of a second fracture but also overall mortality.**
**REFERENCE: Gardner MJ, Brophy RH, Demetrakopoulos D, et al: Interventions to improve osteoporosis treatment following hip fracture: A prospective, randomized trial. J Bone Joint Surg Am 2005;87:3-7.**
**47/. A 58-year-old patient who underwent bilateral hip arthroplasty 12 years ago now reports pain in his hips and difficulty with ambulation to the point where he now uses crutches. A radiograph of the hip and pelvis is shown in Figure 26. What is the best treatment option for this patient?
1- Revision hip arthroplasty with a bipolar implant
2- Revision hip arthroplasty with impaction grafting on the femoral and acetabular side
3- Revision hip arthroplasty with a cemented jumbo acetabular component
4- Revision hip arthroplasty with a cementless acetabular component
5- Acetabular component revision with a tri-flange protrusio ring
PREFERRED RESPONSE: 4**
**DISCUSSION: The radiographs reveal acetabular component failure with bone loss. There
are several treatment options available. The best option for survivorship is a cementless
porous-coated acetabular component. This patient may or may not require structural bone graft, which may need to be determined at the time of surgery. Bipolar implants and cemented acetabular components for revision surgery have not demonstrated long-term success. The use of a protrusio ring is reserved primarily for massive bone loss such as a Paprosky type III bone loss with significant superior migration of the acetabular component. The best clinical results for acetabular component revision have been achieved with cementless porous-coated implants. **
**REFERENCES: Haddad FS, Masri BA, Garbuz DS, et al: Acetabulum, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 923-936.**
**D’Antonio JA: Periprosthetic bone loss of the acetabulum: Classification and management. Orthop Clin North Am 1992;23:279-290.**
**Rubash HE, Sinha RK, Paprosky W, et al: A new classification system for the management of acetabular osteolysis after total hip arthroplasty. Instr Course Lect 1999;48:37-42.**
**48/. Figure 27 shows the AP radiograph of a patient who has late instability. The problem most likely occurred as a result of
1- greater trochanter detachment.
2- femoral stem loosening.
3- wear.
4- osteolysis.
5- infection.
PREFERRED RESPONSE: 3**
**DISCUSSION: Although dislocation can occur anytime after hip arthroplasty, the highest incidence is observed within the first few months. Dislocation occurring many years after arthroplasty has also been described. In contrast to early dislocation, it appears that late dislocation frequently requires surgical intervention. Recent studies suggest that the incidence of late dislocation may be greater than initially appreciated and that the cumulative rate of dislocation rises with increasing follow-up. The presumed etiologic factors for late instability include long-standing problems with the prosthesis (such as malpositioning of the components) with late manifestation, trauma, deterioration in the neurologic status of the patient, and polyethylene wear. The eccentric position of the femoral head in this patient confirms polyethylene wear. The femoral stem is well-fixed, and the greater trochanter osteotomy has united well. The minor osteolysis observed around the proximal femur is also the consequence of wear and is not the cause of instability. Infection, without component loosening and massive soft-tissue destruction, is not otherwise known to result in late instability.**
**REFERENCES: Berry DJ, von Knoch M, Schleck CD, et al: The cumulative long-term risk of dislocation after primary Charnley total hip arthroplasty. J Bone Joint Surg Am 2004;86:9-14.**
**Parvizi J, Wade FA, Rapuri VR, et al: Revision hip arthroplasty for late instability secondary to polyethylene wear. Clin Orthop 2006, in press.**
**49/. Figure 28 shows the postoperative radiograph of a 36-year-old patient. The cerclage cable was placed for a minimal medial calcar fracture seen during femoral preparation. In the immediate postoperative period, what is the highest level of activity that would be safely permitted?
1- Immediate full weight bearing
2- Protected weight bearing
3- Toe touch weight bearing
4- Non-weight-bearing
5- 50% weight bearing
PREFERRED RESPONSE: 1**
**DISCUSSION: The incidence of femoral fracture in primary cementless total hip arthroplasty ranges from 1.5% to 27.8%. It is imperative that the implant and fracture are stable both intraoperatively and postoperatively. Cerclage wiring or cerclage cabling is the current recommended treatment for nondisplaced calcar fractures and minimally displaced proximal fractures. Berend and associates reviewed the results of 58 total hips in 55 patients with intraoperative calcar fracture managed with single or multiple cerclage wires or cables and immediate full weight bearing. Follow-up averaged 7.5 years, and there were no revisions of the femoral component. No patients had severe thigh pain.**
**REFERENCES: Berend KR, Lombardi AV Jr, Mallory TH, et al: Cerclage wires or cables for the management of intraoperative fracture associated with a cementless, tapered femoral prosthesis: Results at 2 to 16 years. J Arthroplasty 2004;19:17-21.**
**Schmidt AH, Kyle RF: Periprosthetic fractures of the femur. Orthop Clin North Am 2002;33:143-152.**
**Greidanus NV, Mitchell PA, Masri BA, et al: Principles of management and results of treating the fractured femur during and after total hip arthroplasty. Instr Course Lect 2003;52:309-322.**
**50/. Embolic material generated during total knee arthroplasty (TKA) shown in Figure 29 is composed of which of the following substances?
1- Fat only
2- Fat and air
3- Fat and marrow
4- Fat and cement
5- Fat and bone
PREFERRED RESPONSE: 3**
**DISCUSSION: Emboli are created during TKA. Usually there is an increased incidence with the use of intramedullary rods that disrupt the marrow contents. These are not fat emboli per se. They are material composed of fat cells and marrow that act like pulmonary emboli to obstruct small arterioles in the lung. They are different from free fat emboli that are seen in fractures and that lead to chemical injury to the lung rather than obstructive injury.**
**REFERENCES: Markel DC, Femino JE, Farkas P, et al: Analysis of lower extremity embolic material after total knee arthroplasty in a canine model. J Arthroplasty 1999;14:227-232.**
**Pell AC, Christie J, Keating JF, et al: The detection of fat embolism by transoesophageal echocardiography during reamed intramedullary nailing: A study of 24 patients with femoral and tibial fractures. J Bone Joint Surg Br 1993;75:921-925.**
**McGrath BJ, Hsia J, Boyd A, et al: Venous embolization after deflation of lower extremity tourniquets. Anesth Analg 1994;78:349-353.**
**51/. Figure 30 shows the MRI scan of a 68-year-old woman who has left hip pain. What is the most appropriate treatment?
1- Open reduction and internal fixation
2- Total hip arthroplasty
3- Incisional biopsy
4- Proximal femoral resection and reconstruction
5- Arthrodesis
PREFERRED RESPONSE: 2**
**DISCUSSION: The patient has a large zone of osteonecrosis of the left femoral head. The wedge-shaped zone of decreased signal intensity on the T1 image in the subchondral region of the femoral head is typical. Based on these findings, total hip arthroplasty is the most appropriate treatment. Open reduction and internal fixation will not help this condition. Incisional biopsy is indicated only if the MRI scan shows a probable neoplasm. Resection of the proximal femur is indicated only for aggressive malignancy. Arthrodesis may be considered in a younger patient but not in a 68-year-old individual. Other treatments, not listed, such as core decompression, vascularized fibular transplant, and osteotomy may be options in selected patients.**
**REFERENCES: Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 213-223.**
**Watson RM, Roach NA, Dalinka MK: Avascular necrosis and bone marrow edema syndrome. Radiol Clin North Am 2004;42:207-219.**
**52/. There is increasing concern about the ethical relationship of orthopaedists to the orthopaedic equipment industry. Which of the following describes the most appropriate relationship?
1- Industry-paid travel, hotel (for the surgeon and spouse), and registration at a university-sponsored CME course
2- Industry-paid travel and hotel for a faculty member at an industry-sponsored meeting that is not CME approved
3- Consultation agreement ($50,000/annum) between the surgeon and the company for evaluation of the implant system with required oral reporting of impressions
4- A restricted grant from a company to an orthopaedic residency program with the stipulation that the third year residents be sent to an industry-sponsored course
5- Industry-paid dinner at a premium restaurant ($200/person) for surgeon and office staff at which a new set of surgical instrumentation is presented
PREFERRED RESPONSE: 2**
**DISCUSSION: It is appropriate for orthopaedic surgeons to have relationships with industry as long as the relationship is for the good of the patient and no “quid pro quo” intent exists. A grant to cover registration at a CME event is appropriate but travel and hotel for a spouse is not. For orthopaedists who are faculty at a meeting sponsored by industry, it is appropriate for travel and expenses to be covered for that faculty member. Care must be exercised that the faculty member contributes in an amount appropriate for the expenses paid. The faculty member must ensure that information presented is unbiased and based on reasonable data and opinion. Consulting agreements should spell out specifically the duties of the agreement and payment should be appropriate for the time spent. There should be a defined work product for the consulting. Agreements that are thinly veiled payments for use of a company’s products must be avoided. In all cases, the agreements must stand up to public scrutiny. Restricted grants for specific industry-sponsored programs aimed at residents are not appropriate. Unrestricted grants intended for attendance at approved CME courses are appropriate. Dinners at which information is presented about topics that can aid in patient care are appropriate as long as the expense is reasonable ($100 or less/person) and the guest list includes individuals who can use the information in a patient case. Clearly a “premium” dinner for office staff to review new surgical instrumentation would not pass this test.**
**REFERENCE: Opinions on ethics and professionalism, in Guide to The Ethical Practice of Orthopaedic Surgery, ed 6. American Academy of Orthopaedic Surgeons, Rosemont, IL, 2006, pp 38-42.**
**53/. A 30-year-old patient has had severe left hip pain and difficulty ambulating, necessitating the use of a cane, for the past 6 months. A photomicrograph of the femoral head sectioned at the time of surgery is shown in Figure 31. What is the most likely diagnosis?
1- Renal osteodystrophy
2- Pyogenic osteomyelitis
3- Osteoarthritis
4- Osteonecrosis
5- Tuberculosis osteomyelitis
PREFERRED RESPONSE: 4**
**DISCUSSION: The photomicrograph demonstrates a wedge-shaped infarct with femoral head collapse; therefore, the diagnosis is osteonecrosis of the femoral head. Perthes disease and osteoarthritis do not involve a wedge-shaped defect. Tuberculosis of the hip joint results in greater destruction of the articular cartilage.**
**REFERENCES: Basset LW, Mirra JM, Cracchiolo A III: Ischemic necrosis of the femoral head: Correlation between magnetic resonance imaging and histologic sections. Clin Orthop 1987;223:181-187.**
**Sugano N: Osteonecrosis, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopedics. St Louis, MO, Mosby, 2002, pp 878-887.**
**54/. When comparing mobile-bearing total knee arthroplasty (TKA) to fixed-bearing total condylar arthroplasty, the mobile-bearing procedure provides
1- no improvement in survivorship.
2- approximately 15 degrees greater flexion.
3- appreciable reduction in wear rates.
4- a faster recovery profile.
5- better quadriceps strength.
PREFERRED RESPONSE: 1**
**DISCUSSION: Survivorship is similar in the two groups. In a recent study, mobile-bearing TKAs showed a slightly higher maximum flexion than the total condylar fixed-bearing-type designs (112 degrees versus 108 degrees with no difference in recovery rate). Using a fixed-bearing or a mobile-bearing design did not seem to influence the recovery rate in early results after knee arthroplasty. Mobile-bearing arthroplasties are suggested, in theory, to offer a reduction in polyethylene wear; however, clinical studies have not yet proven this. Recovery rates have yet to be statistically seen as improved with either method. Differences in strength have not been shown.**
**REFERENCES: Aglietti P, Baldini A, Buzzi R, et al: Comparison of mobile-bearing and fixed-bearing total knee arthroplasty: A prospective randomized study. J Arthroplasty 2005;20:145-153.**
**Sorrells RB: The rotating platform mobile bearing TKA. Orthopedics 1996;19:793-796.**
**Dennis DA, Komistek RD: Kinematics of mobile-bearing total knee arthroplasty. Instr Course Lect 2005;54:207-220.**
**55/. Based on the type of articulation shown in Figure 32, wear is not affected by which of the following factors?
1- Radial mismatch of the femoral head to the acetabular component
2- Sphericity of the bearings
3- Surface finish of the articulation
4- Carbon content of the metal-on-metal bearing
5- Head-to-neck ratio
PREFERRED RESPONSE: 5**
**DISCUSSION: Wear in total hip arthroplasty is a very complex phenomenon. The radial mismatch of the femoral head to the acetabular component has been shown in multiple studies to be a significant factor in wear. The mismatch can neither be too small nor too large. When the mismatch is too small, seizing of the implants can occur. When the mismatch is too large, contact stresses increase and produce exceptionally high wear. The ideal radial mismatch should be approximately 50 microns. Surface roughness and ball sphericity are two items that are extremely important with respect to wear. High carbon content has been shown to decrease wear. This device has a very large head-to-neck ratio, so impingement-related wear is unlikely.**
**REFERENCES: Amstutz HC, Grigoris P: Metal on metal bearings in hip arthroplasty. Clin Orthop 1996;329:S11-S34.**
**Amstutz HC, Campbell P, McKellop H, et al: Metal on metal total hip replacement workshop consensus document. Clin Orthop 1996;329:S297-S303.**
**McKellop H, Park SH, Chiesa R, et al: In vivo wear of three types of metal on metal hip prostheses during two decades of use. Clin Orthop 1996;329:S128-S140.**
**56/. Figure 33 shows the venogram of a patient who has a long history of alcohol abuse. Warfarin should be used cautiously because of the interaction with which of the following factors?
1- IV
2- V
3- VI
4- VII
5- VIII
PREFERRED RESPONSE: 4**
**DISCUSSION: Warfarin acts by inhibiting clotting factors II, VII, IX, X. The actual
mechanism of action is by inhibition of hepatic enzymes, vitamin K epoxide, and perhaps vitamin K reductase. This inhibition results in lack of carboxylation of vitamin K-dependent proteins (II, VII, IX, X). The anticoagulant effect of warfarin can be reversed with vitamin K or fresh-frozen plasma. The use of alcohol may lead to liver dysfunction and an even more limited margin of available factors.**
**REFERENCES: Lieberman JR, Wollaeger J, Dorey F, et al: The efficacy of prophylaxis with low-dose warfarin for prevention of pulmonary embolism following total hip arthroplasty.**
**J Bone Joint Surg Am 1997;79:319-325.**
**Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 63-72.**
**57/. A 78-year-old patient undergoing revision total knee arthroplasty has bone loss throughout the knee at the time of revision. A distal femoral augment is used to restore the joint line. One month after surgery, the patient reports pain and is unable to ambulate. A lateral radiograph is shown in Figure 34. What is the most likely etiology of this problem?
1- Inadequate restoration of the joint line
2- Patellar tendon rupture
3- Excessive internal rotation of the tibial component
4- Flexion gap instability
5- Hyperextension of the femoral component
PREFERRED RESPONSE: 4**
**DISCUSSION: Instability is a leading cause of failure following total knee arthroplasty. Instability can present as global instability, extension gap (varus/valgus) instability, or flexion gap (anterior/posterior) instability. Treatment options are numerous based on the exact pathology. The radiograph reveals anterior/posterior instability with dislocation consistent with flexion gap instability. A loose flexion gap can allow the femoral component to ride above the tibial cam post mechanism, resulting in dislocation. Distal femoral augments treat extension gap instability, whereas tibial augments can treat both flexion and extension gap instability. Posterior condyle augments at the distal femur can also be used to treat flexion gap instability. Flexion gap instability is further aggravated by extension mechanism incompetence. Note the excessively thin patella on the lateral radiograph.**
**REFERENCES: Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46.**
**McAuley J, Engh GA, Ammeen DJ: Treatment of the unstable total knee arthroplasty. Inst Course Lect 2004;53:237-241.**
**Naudie DD, Rorabeck CH: Managing instability in total knee arthroplasty with constrained and linked implants. Instr Course Lect 2004;53:207-215.**
**58/. Figure 35 shows the AP radiograph of a patient who underwent a previous upper tibial osteotomy (UTO). The patient may be at risk for which of the following during total knee arthroplasty (TKA)?
1- Bone loss
2- Patella alta
3- Myositis ossificans
4- Fracture
5- Instability
PREFERRED RESPONSE: 5**
**DISCUSSION: The results of TKA for patients with a prior UTO are reported to be slightly suboptimal. The major problems are patella baja, difficulty in exposure, and instability. Most of the patients exhibit some degree of instability prior to TKA, and ligamentous balancing may be difficult. Ligamentous structures are at risk of rupture during the difficult exposure. The problem of ligamentous balancing is exacerbated by the change in the joint slope that can occur after UTO.**
**REFERENCES: Parvizi J, Hanssen AD, Spangehl MJ: Total knee arthroplasty following proximal tibial osteotomy: Risk factors for failure. J Bone Joint Surg Am 2004;86:474-479.**
**Meding JB, Keating EM, Ritter MA, et al: Total knee arthroplasty after high tibial osteotomy: A comparison study in patients who had bilateral total knee replacement. J Bone Joint Surg Am 2000;82:1252-1259.**
**59/. Figure 36 shows the radiograph of a patient who has hip pain and is unable to ambulate. What is the most appropriate management for this patient?
1- Bisphosphonates
2- Protected weight bearing
3- Open reduction and internal fixation
4- Revision total hip arthroplasty
5- Resection arthroplasty
PREFERRED RESPONSE: 4**
**DISCUSSION: The patient has a periprosthetic fracture of the greater trochanter - Vancouver A. The reason for the fracture of the greater trochanter is the extensive periarticular osteolysis that has occurred as a result of polyethylene wear. The latter is demonstrated by eccentric seating of the large femoral head in the acetabulum. The most appropriate management is to reverse the osteolysis process, which involves exchange of the acetabular liner with or without revision of the other components depending on their fixation and position. The greater trochanter can also be fixed during revision surgery.**
**REFERENCES: Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304.**
**Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.**
**60/. When polyethylene is exposed to radiation and subsequently heated, certain chemical changes occur in the material. Which of the following statements best describes these changes?
1- The process converts an otherwise interpenetrating networking structure of polymer chains into a linear, high molecular weight polyethylene macromolecule.
2- The process increases the ductility of the material.
3- The process leads to fewer particles that are larger in size than the untreated material.
4- The process improves (lowers) the wear rate but may increase the risk of fracture.
5- The process decreases the wear rate of the material, compared to untreated polyethylene, when tested against a rough counterface.
PREFERRED RESPONSE: 4**
**DISCUSSION: Exposure of polyethylene to radiation and then heating it to quench the free radicals leads to a cross-linked material. It converts a high molecular weight polyethylene macromolecule to an interpenetrating network structure of polymer chains. The ductility of the material is decreased, hence the greater risk of fracture. While the wear rate (measured as fewer and smaller particles) against a smooth counterface is markedly reduced, cross-linked polyethylene has shown a larger increase in wear rate when a rougher counterface is used compared to noncross-linked material. Due to reduced mechanical strength, highly cross-linked polyethylene is less resistant to abrasive wear.**
**REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 32-33.**
**61/. Familial (Leiden) thrombophilia is of importance in joint arthroplasty because of an abnormality in the clotting cascade. Which of the following statements best describes the condition?
1- It is a disease caused by an abnormality of platelets that leads to increased blood clotting.
2- It is a disease caused by an abnormality of vascular endothelium that leads to increased blood clotting.
3- It is a disease caused by an abnormality of hepatic metabolism that leads to decreased production of factor V and decreased blood clotting.
4- It is a disease caused by an abnormality of factor V that leads to decreased inactivation of factor Va by activated protein C (aPC) and increased blood clotting.
5- It is a familial, genetic disease that requires placement of a Greenfield filter in all individuals who have the abnormality, prior to surgery.
PREFERRED RESPONSE: 4**
**DISCUSSION: Factor V Leiden is a disease caused by an abnormality of factor V in which a single amino acid substitution of glutamine for arginine in the protein C cleavage region leads to decreased inactivation of factor V and thus a greater tendency to form clots. More than half of all individuals with Factor V Leiden will develop deep venous thrombosis in the presence of a single additional risk factor such as long bone fracture or total joint arthroplasty.**
**REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 14-15.**
**62/. Figure 37 reveals a periprosthetic fracture around a cemented femoral stem in an
81-year-old patient with Paget’s disease and mild coagulopathy. What is the most appropriate reconstructive management on the femoral side?
1- Open reduction and internal fixation
2- Impaction allografting
3- Proximally coated femoral stem
4- Allograft prosthetic composite (APC)
5- Proximal femoral replacement (PFR)
PREFERRED RESPONSE: 5**
**DISCUSSION: This is an example of a Vancouver B3 periprosthetic fracture that consists of a fracture around a loose femoral stem with poor proximal bone support. Therefore, open reduction and internal fixation is not an option. PFR is an excellent choice for elderly inactive patients with poor femoral bone stock. The surgery can be performed in an expeditious manner, which is very important in a patient with mild coagulopathy. Impaction allografting and APC are both options for younger patients who have bone stock that needs to be restored. The results of revision arthroplasty using proximally coated stems, especially under these circumstances, are poor.**
**REFERENCES: Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304.**
**Parvizi J, Sim FH: Proximal femoral replacements with megaprostheses. Clin Orthop 2004;420:169-175.**
**Klein GR, Parvizi J, Rapuri V, et al: Proximal femoral replacement for treatment of periprosthetic fractures. J Bone Joint Surg Am 2005;87:1777-1781.**
**63/. A patient with a documented allergy to nickel requires a total knee arthroplasty. Which of the following prostheses is most likely to provide long-term success in this individual?
1- All-polyethylene tibial component and pure titanium femoral component
2- All-polyethylene tibial component and cobalt-chromium alloy femoral component
3- Cobalt-chromium alloy tibial component and cobalt-chromium alloy femoral component
4- Modular titanium tibial component and pure titanium femoral component
5- Modular titanium tibial component and oxidized zirconium femoral component
PREFERRED RESPONSE: 5**
**DISCUSSION: Nickel allergy is not an infrequent preoperative finding. The ramifications of such allergies in arthroplasty patients are poorly understood at this time. Stainless steel and cobalt-chromium alloys contain relatively high concentrations of nickel. Titanium, oxidized zirconium, and polyethylene do not contain significant amounts of nickel. Titanium is not a good surface for the articulating portion of the femoral component because of its propensity for metallosis. Oxidized zirconium is the only suitable femoral component for patients allergic to nickel. A modular titanium tibial component or an all-polyethylene tibial component would be satisfactory for these patients.**
**REFERENCES: Laskin RS: An oxidized Zr ceramic surfaced femoral component for total knee arthroplasty. Clin Orthop 2003;416:191-196.**
**Nasser S, Campbell PA, Kilgus D, et al: Cementless total joint arthroplasty prostheses with titanium-alloy articular surfaces: A human retrieval analysis. Clin Orthop 1990;261:171-185.**
**64/. Which of the following is accurate regarding low-molecular-weight heparin used for deep venous thrombosis (DVT) prophylaxis in total joint arthroplasty?
1- The incidence of thrombocytopenia is lower with low-molecular-weight heparin than with unfractionated heparin.
2- The half-life of low-molecular-weight heparin is less than that of unfractionated heparin.
3- Low-molecular-weight heparin affects circulating thrombin (Factor IIa) to a greater extent than unfractionated heparin.
4- The mechanism of action of low-molecular-weight heparin is primarily by targeting Factor Xa.
5- There is a significant decrease in postoperative bleeding with the use of low-molecular-weight heparin compared to warfarin.
PREFERRED RESPONSE: 4**
**DISCUSSION: Low-molecular-weight heparin is highly bioavailable with a half-life
of 3 to 18 hours. This is greater than the 1 hour half-life of unfractionated heparin.
Low-molecular-weight heparin offers an advantage over unfractionated heparin by selectively targeting Factor Xa while having a lesser effect on circulating thrombin (Factor IIa). Circulating thrombin Factor IIa is needed for local hemostasis at the site of the surgical wound. Clinical studies have shown a reduction by one third in the incidence of thrombocytopenia with the use of low-molecular-weight heparin. Low-molecular-weight heparin has been shown to demonstrate similar clinical results compared to warfarin with respect to preventing thromboembolic disease after total hip arthroplasty and complications such as bleeding. **
**REFERENCES: Zimlich RH, Fulbright BM, Friedman RJ: Current status of anticoagulation therapy after total hip and total knee arthroplasty. J Am Acad Orthop Surg 1996;4:54-62.**
**Colwell CW Jr, Spiro TE, Trowbridge AA, et al: Use of enoxaparin, a low-molecular-weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14.**
**Torholm C, Broeng L, Jorgensen PS, et al: Thromboprophylaxis by low-molecular-weight heparin in elective hip surgery: A placebo controlled study. J Bone Joint Surg Br 1991;73:434-438.**
**65/. A 42-year-old man reports the recent onset of right hip pain. A radiograph and MRI scan are shown in Figures 38a and 38b. A WBC count, erythrocyte sedimentation rate, and hip aspiration are within normal limits. Management should now consist of
1- core decompression.
2- biopsy of the femoral head.
3- protected weight bearing and observation.
4- total hip arthroplasty.
5- percutaneous cannulated pin fixation of the femoral neck.
PREFERRED RESPONSE: 3
DISCUSSION: Transient osteoporosis of the hip is an uncommon problem, usually affecting women in the last trimester of pregnancy and middle-aged men. Symptoms include pain in the involved hip with temporary osteopenia; however, there is no joint space involvement. In this patient, the imaging findings are consistent with transient osteoporosis. Short TR/TE (repetition time/echo time) images reveal diffusely decreased signal intensity in the femoral head and intracapsular region of the femoral neck. Increased signal intensity is seen with increased T2-weighting. Within a few months, the pain, as well as the imaging findings, will completely resolve without intervention. Distinguishing the diffuse features of transient osteoporosis of the hip from the segmental findings of osteonecrosis is essential. Unlike transient osteoporosis of the hip, osteonecrosis will have a double-density signal on MRI and may progress radiographically. Surgical intervention and oral corticosteriods are not indicated for treatment. Protected weight bearing until the pain resolves may decrease symptoms while the transient osteoporosis resolves.
REFERENCES: Potter H, Moran M, Scheider R, et al: Magnetic resonance imaging in diagnosis of transient osteoporosis of the hip. Clin Orthop 1992;280:223-229.**
**Bijl M, van Leeuwen MA, van Rijswijk MH: Transient osteoporosis of the hip: Presentation of typical cases for review of the literature. Clin Exp Rheumatol 1999;17:601-604.**
**Montella BJ; Nunley JA, Urbaniak JR: Osteonecrosis of the femoral head associated with pregnancy: A preliminary report. J Bone Joint Surg Am 1999;81:790-798.**
**66/. During cemented total hip arthroplasty, peak pulmonary embolization of marrow contents occurs when the
1- hip is dislocated.
2- femoral neck is osteotomized.
3- acetabulum is prepared.
4- acetabular component is inserted.
5- femoral stem is inserted.
PREFERRED RESPONSE: 5**
**DISCUSSION: Peak embolization is observed during femoral stem insertion. Embolization is also observed during acetabular preparation and hip reduction.**
**REFERENCES: Lewallen DG, Parvizi J, Ereth MH: Perioperative mortality associated with hip and knee arthroplasty, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 119-127.**
**Ereth MH, Weber JG, Abel MD, et al: Cemented versus noncemented total hip arthroplasty: Embolism, hemodynamics, and intrapulmonary shunting. Mayo Clin Proc 1992;67:1066-1074.**
**67/. What are the optimal conditions for leaving the acetabular shell in place, replacing the acetabular liner, and grafting the osteolytic defect shown in Figure 39?
1- Nonmodular implant
2- Instability
3- Well-designed, well-fixed modular implant
4- Complete radiolucency of the acetabular component
5- Migration of the acetabular component
PREFERRED RESPONSE: 3**
**DISCUSSION: Dense pods of ingrowth into the porous coating of cementless ingrowth sockets are seen. Channels through the non-ingrown portion allow access to the trabecular bone of the ilium. Polyethylene wear debris can enter these areas through screw holes. Expansile, lytic lesions can result, which can become large without compromising implant fixation. Loosening is late and results from catastrophic loss of bone. A well-fixed acetabular component with a modular design, a well-designed locking mechanism, and a good survivorship history is a candidate for exchange of the liner and grafting of the osteolytic lesion.**
**REFERENCES: Ries MD: Complications in primary total hip arthroplasty: Avoidance and management. Wear. Instr Course Lect 2003;52:257-265.**
**Dumbleton JH, Manley MT, Edidin AA: A literature review of the association between wear rate and osteolysis in total hip arthroplasty. J Arthroplasty 2002;17:649-661.**
**Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,**
**pp 175-180.**
**68/. A 53-year-old patient is seen in the emergency department after sustaining a fall onto her left hip. A current radiograph is shown in Figure 40. What is the best treatment option?
1- Bed rest and non-weight-bearing for 6 to 8 weeks
2- Component retention and open reduction and internal fixation
3- Proximal femoral replacement prosthesis
4- Revision arthroplasty with a long cemented stem
5- Revision arthroplasty with a long porous-coated cylindrical stem
PREFERRED RESPONSE: 5**
**DISCUSSION: The patient has sustained a Vancouver B2 periprosthetic femoral fracture
(a femoral fracture that occurs around or just distal to a loose stem, with adequate proximal bone stock). The stem is no longer fixed to proximal bone; therefore, retention of the femoral component is not recommended. Nonsurgical management is contraindicated because of the high risk of nonunion and malunion with significant component settling in the distal fragment and leg shortening. Revision femoral arthroplasty must attain distal fixation in adequate host bone, which is usually successful with a porous-coated cylindrical stem.**
**REFERENCES: Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol for proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.**
**Springer BD, Berry DJ, Lewallen DG: Treatment of periprosthetic femoral fractures following total hip arthroplasty with femoral component revision. J Bone Joint Surg Am 2003;85:2156-2162.**
**69/. A 67-year-old patient seen in the emergency department reports the acute onset of pain and is unable to ambulate. History reveals that the patient underwent surgical treatment for a periprosthetic femoral fracture 6 months ago. A radiograph is shown in Figure 41. What is the best treatment option at this time?
1- Open reduction and internal fixation with cortical onlay strut grafts and bone morphogenic protein
2- Resection arthroplasty
3- Revision hip arthroplasty with an allograft prosthetic composite
4- Revision hip surgery with distal stem fixation using a long stem implant with strut grafts
5- Revision hip arthroplasty with a proximally coated implant
PREFERRED RESPONSE: 4**
**DISCUSSION: The radiograph reveals a periprosthetic fracture at the tip of the stem with a stable cemented implant. This is classified as a Vancouver type B1 periprosthetic fracture. An attempt at internal fixation has already failed; therefore, the most predictable results would be achieved with distal fixation. After removal of the well-fixed cemented implant, the proximal bone may not be suitable for proximal fixation. Adequate bone stock is available such that an allograft prosthetic composite or a tumor prosthesis is not necessary. The best option is a long stem implant with distal fixation, which serves as an intramedullary device to restore alignment and increase the likelihood of union. Cortical onlay strut grafts are used as an adjunct to definitive fixation.**
**REFERENCES: Younger AS, Dunwoody I, Duncan CP: Periprosthetic hip and knee fractures: The scope of the problem. Inst Course Lect 1998;47:251-256.**
**Lee SR, Bostrom MP: Periprosthetic fractures of the femur after total hip arthroplasty. Inst Course Lect 2004;53:111-118.**
**70/. With the increasing availability of total hip arthroplasty (THA) to younger patients with hip osteoarthritis, there has been increased use of alternative bearing surfaces. Compared to a ceramic-on-ceramic articulation, which of the following is a specific advantage of a metal-on-metal bearing surface?
1- Increased wettability
2- Increased hardness
3- Increased fracture toughness
4- Decreased surface roughness
5- Lower coefficient of friction
PREFERRED RESPONSE: 3**
**DISCUSSION: Alternative bearing surfaces in THA have received much attention in recent years as more and more hip arthroplasties are being performed on younger patients with hip arthritis. The two most popular nonmetal-on-polyethylene bearing surfaces are metal-on-metal and ceramic-on-ceramic. There are arguments supporting the use of either, but ceramic bearings have been shown to have a theoretic increased risk of fracture compared with cobalt-chromium. This has been shown to be clinically relevant with zirconium ceramics. Newer alumina ceramics are being produced with lower porosity and grain size and with higher density and purity, resulting in lower fracture risk but still greater than that of cobalt-chromium.**
**REFERENCES: Heisel C, Silva M, Schmalzried TP: Bearing surface options for total hip replacement in young patients. Instr Course Lect 2004;53:49-65.**
**D’Antonio J, Capello W, Manley M, et al: New experience with alumina-on-alumina ceramic bearings for total hip arthroplasty. J Arthroplasty 2002;17:390-397.**
**71/. Which of the following prophylactic regimens for the prevention of deep venous thrombosis after knee arthroplasty has received a grade 1A recommendation in favor of its use from the American College of Chest Physicians (ACCP) in the 2004 guidelines?
1- Warfarin with a targeted international normalized ratio (INR) of 2.0 to 3.0 for
10 to 14 days
2- Low-molecular-weight heparin used for at least 3 days
3- Pneumatic compression sleeves used while the patient is in the hospital
4- Fondaparinux used for 5 to 7 days
5- Aspirin for 4 weeks
PREFERRED RESPONSE: 1**
**DISCUSSION: In the 2004 ACCP guidelines, there were three prophylactic regimens that received a grade 1A favorable recommendation. These included low-molecular-weight heparin, warfarin, or fondaparinux, as long as they are used for at least 10 days. If warfarin is used, the target INR should be 2.0 to 3.0, according to the guidelines. Pneumatic compression sleeves have gained popularity in the orthopaedic community but have not received a grade 1A rating from the ACCP at this time. Use of aspirin by itself is discouraged by the ACCP.**
**REFERENCE: Geerts WH, Pineo GF, Heit JA, et al: Prevention of venous thromboembolism: The seventh ACCP Conference on antithrombotic and thrombolytic therapy. Chest 2004;126:338S-400S.**
**72/. In the radiograph shown in Figure 42, the fracture pattern around this well-fixed stem is classified as Vancouver type
1- A.
2- B1.
3- B2.
4- B3.
5- C.
PREFERRED RESPONSE: 2**
**DISCUSSION: The Vancouver classifications describes periprosthetic hip fractures in the following way. Type A fractures are in the trochanteric region. Type B1 fractures occur around the stem or at the tip in the face of a well-fixed stem. These are usually treated with open reduction and internal fixation, usually including struts, cable, and/or cable plates. Type B2 fractures occur in the same region with a loose stem. Type B3 fractures occur with a loose stem where the proximal bone is of poor quality and/or severely comminuted. Type C fractures occur well below the stem.**
**REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 149-154.**
**Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol for proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.**
**Masri BA, Meek RM, Duncan CP: Periprosthetic fractures evaluation and treatment. Clin Orthop 2004;420:80-95.
73/. Figures 43a and 43b show the T1/- and T2-weighted MRI scans of a 78-year-old woman who reports the sudden atraumatic onset of well-localized medial knee pain. Pain is worse at night and also occurs with weight-bearing activity. What is the most likely diagnosis?
1- Complex regional pain syndrome
2- Osteoarthritis
3- Osteosarcoma
4- Osteonecrosis
5- Inflammatory arthritis
PREFERRED RESPONSE: 4**
**DISCUSSION: Osteonecrosis of the tibial plateau occurs infrequently. The symptoms are similar to those of idiopathic osteonecrosis of the medial femoral condyle and include pain and tenderness of the medial aspect of the knee and a slight synovitis. The range of motion of the knee remains within normal limits, and no gross deformity is present. Osteonecrosis of the tibial plateau is easily misdiagnosed as degenerative meniscus or osteoarthritis of the compartment of the knee. Review of lateral radiographs may reveal an osteopenic area in the subchondral bone of the medial tibial plateau. The diagnosis is more easily established with a bone scan where increased uptake of radionucleides is shown over the medial tibial plateau. In osteoarthritic involvement of the medial compartment, uptake is over both the medial femoral condyle and the medial tibial plateau, whereas if osteoarthritis involves the entire knee, uptake is diffuse over the entire joint. Radiographic findings in complex regional pain syndrome are normal as opposed to the findings for osteonecrosis or osteoarthritis. Osteosarcoma has a characteristic radiographic appearance of a bone-forming tumor. Loose bodies can derive from osteochondral fractures; a history of trauma is usually elicited. Osteoarthritis usually presents with joint space narrowing accompanying the weight-bearing pain.**
**REFERENCES: Soucacos PN, Berris AE, Xenakis TH, et al: Knee osteonecrosis: Distinguishing features in differential diagnosis, in Urbanik JR, Jones JD (eds): Osteonecrosis. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 413-424.**
**Ecker ML, Lotke PA: Osteonecrosis of the medial part of the tibial plateau. J Bone Joint Surg Am 1995;77:596-601.**
**74/. Figure 44 shows the radiograph of a 65-year-old man who underwent a revision arthroplasty to remove a loose, cemented femoral stem. When planning the postoperative restrictions, the surgeon should be aware that
1- the approach used reduces the torque-to-failure (fracture) of the construct to less than 50% of the intact femur.
2- the technique of repair can return the reconstructed prosthesis/bone composite to nearly the strength of the intact femur.
3- there is no relationship between the density of the native bone and the strength of the prosthesis/bone composite.
4- the addition of bone graft substitute or autograft has been shown to lessen the time to complete healing.
5- there is a one in five chance of fracture with this technique; therefore, the surgeon must carefully weigh the potential benefits versus this risk.
PREFERRED RESPONSE: 1**
**DISCUSSION: The transfemoral approach, also known as the extended trochanteric osteotomy, is an important technique to master for revision hip surgery. When performed correctly, it allows excellent exposure of the femoral canal and aids in exposure of the acetabulum. As demonstrated in the study cited, however, it markedly reduces the torque that the composite can withstand without failure. This type of basic science study is important to guide postoperative rehabilitation.**
**REFERENCE: Noble AR, Branham D, Willis M, et al: Mechanical effects of the extended trochanteric osteotomy. J Bone Joint Surg Am 2005;87:521-529.**
**75/. A 75-year-old patient returns for follow-up after undergoing bilateral total hip arthroplasty (THA). The right hip is a hybrid THA performed 12 years ago, whereas the left hip is a cementless THA performed 10 years ago. Both acetabular components are the same type, same size, and from the same manufacturer. Both femoral heads are
28-mm cobalt-chromium components. What is the most likely explanation for the advanced polyethylene wear in one hip?
1- Presence of a third-party abrasive particle
2- Disproportionate use of the limbs by the patient
3- Defective femoral head
4- Method of fixation of the femoral component
5- Method of sterilization and shelf life of the polyethylene
PREFERRED RESPONSE: 5**
**DISCUSSION: Over the past three decades, gamma irradiation and air has been the most common method of sterilizing polyethylene used in total joint arthroplasty. This method of sterilization results in breakage of the chemical bonds within the polymer. While this promotes cross-linking, it also leaves the polyethylene vulnerable to oxidation, especially if packaged in an air environment. Oxidation has been shown to decrease polyethylene’s molecular weight, ultimate tensile strength, elongation, and toughness which results in a stiffer, more brittle material that is less resistant to wear. Severity of oxidation and a decrease in mechanical properties have been shown to be related to the length of time that the component is exposed to air (the shelf life). Currier and associates studied the clinical performance of gamma irradiated in air polyethylene components that had been shelf aged. They demonstrated that for the first
5 years of shelf life, polyethylene oxidized rather slowly. However, polyethylene components with a shelf life of more than 5 years would be expected to have minimal mechanical toughness and would likely fail rapidly if implanted. Bohl and associates evaluated 135 patients who had undergone total knee arthroplasty. Survivorship at 5 years was 100% for components with a shelf life of less than 4 years, 89% for components with a shelf life of 4 to 8 years, and 79% for components with a shelf life of more than 8 years. Sychterz and associates reported no correlation between shelf life and true wear rates for components with a shelf life of less
than 3 years. In summary, both in vivo and in vitro data suggest that shelf life in excess of
3 to 5 years has a direct effect on wear of polyethylene. **
**REFERENCES: Currier BH, Currier JH, Collier JP, et al: Shelf life and in vivo duration: Impacts on performance of tibial bearings. Clin Orthop 1997;342:111-122.**
**Bohl JR, Bohl WR, Postak PD, et al: The Coventry Award: The effects of shelf life on clinical outcome for gamma sterilized polyethylene tibial components. Clin Orthop 1999;367:28-38.**
**Sychterz CJ, Young AM, Orishimo K, et al: The relationship between shelf life and in vivo wear for polyethylene acetabular liners. J Arthroplasty 2005;20:168-173.**
**76/. A 37-year-old man who works in a factory has isolated, lateral unicompartmental pain about his knee with activities. Nonsurgical management has failed to provide relief. The radiograph shown in Figure 45 reveals a tibiofemoral angle of approximately 15 degrees which is clinically correctable to neutral. What is the best surgical option in this patient?
1- Unicompartmental arthroplasty
2- Total knee arthroplasty
3- Lateral closing wedge proximal tibial osteotomy
4- Medial opening wedge proximal tibial osteotomy
5- Medial closing wedge supracondylar femoral osteotomy
PREFERRED RESPONSE: 5**
**DISCUSSION: Patients with a valgus alignment about the knee can have lateral compartment arthritis. Similar to a high tibial osteotomy, a supracondylar femoral osteotomy is indicated in younger patients who have a more active lifestyle and isolated unicompartmental disease. In this young patient who works in a factory and has a valgus knee, a medial closing wedge supracondylar femoral osteotomy is the treatment of choice. The role of arthroplasty is limited in younger patients.**
**REFERENCES: Mathews J, Cobb AG, Richardson S, et al: Distal femoral osteotomy for lateral compartment osteoarthritis of the knee. Orthopedics 1998;21:437-440.**
**Cameron HU, Botsford DJ, Park YS: Prognostic factors in the outcome of supracondylar femoral osteotomy for lateral compartment osteoarthritis of the knee. Can J Surg 1997;40:114-118.**
**77/. Figure 46 shows the AP radiograph of an active 80-year-old patient with an acetabular fracture. The fracture was initially managed nonsurgically; however, the patient is now scheduled to undergo total hip arthroplasty. What is the treatment of choice for the contained acetabular bone defect?
1- Bipolar femoral component
2- Acetabular cage
3- Large structural allograft
4- Use of the femoral head
5- Double-bubble acetabular cup
PREFERRED RESPONSE: 4**
**DISCUSSION: Acetabular fractures can result in a relative or actual acetabular bone defect. The medial blow-out fracture of the acetabulum has united well in this patient. It is likely that a medial shell of bone will be present during hip arthroplasty. The femoral head may be used as morcellized or structural bone to augment the medial defect and is preferred to structural allograft. Bipolar hip arthroplasty is notorious for medial migration in patients without a medial bone defect; therefore, it will not be a good choice in this patient. Filling the defect with methylmethacrylate cement, though an option, is not the best option in this active patient with an extensive medial defect. A double-bubble acetabular cup is used for patients with deficiency of the bone in the dome region.**
**REFERENCES: Mears DC: Surgical treatment of acetabular fractures in elderly patients with osteoporotic bone. J Am Acad Orthop Surg 1999;7:128-141.**
**Bellabarba C, Berger RA, Bentley CD, et al: Cementless acetabular reconstruction after acetabular fracture. J Bone Joint Surg Am 2001;83:868-876.**
**78/. A 28-year-old woman who is an avid runner reports pain about the left hip with activities. Nonsurgical management has failed to provide relief. An MRI arthrogram is shown in Figure 47. What is the most likely diagnosis?
1- Osteonecrosis
2- Transient osteoporosis
3- Loose chondral fragment
4- Labral tear
5- Femoral neck stress fracture
PREFERRED RESPONSE: 4**
**DISCUSSION: The MRI arthrogram reveals dye extravasation into the labrum, consistent with a labral tear. The MRI findings are not typical of osteonecrosis, stress fracture, or transient osteoporosis. There is no increase in bone marrow edema in the neck or femoral head.**
**REFERENCES: Guanche CA, Sikka RS: Acetabular labral tears with underlying chondralmalacia: A possible association with high-level running. Arthroscopy 2005;21:580-585.**
**McCarthy JC: The diagnosis and treatment of labral and chondral injuries. Instr Course Lect 2004;53:573-577.**
**79/. Figure 48a shows the full-leg standing radiograph of a patient with a prior femoral fracture. Figure 48b shows the lateral view of the same joint. The patient is scheduled to undergo total knee arthroplasty. Because the mechanical axis of the lower extremity in patients with a prior femoral fracture may be disrupted, which of the following should be used during surgery to restore the mechanical axis of the lower extremity in this patient?
1- Customized components
2- Specialized intramedullary jigs
3- Hinged prosthesis
4- Extra-articular osteotomy
5- Routine knee prosthesis
PREFERRED RESPONSE: 5**
**DISCUSSION: The radiograph shows hardware that was used for fixation of a prior femoral fracture. The mechanical axis of the lower extremity in this patient is nearly normal
(3 degrees valgus), and the deformity at the healed fracture site (14 degrees) does not appear to affect the joint alignment and is acceptable. Use of a routine knee prosthesis will be possible in this patient. To avoid hardware removal, extramedullary jigs and/or computerized navigation may be used to measure and restore the long axis of the femur. The use of a hinged prosthesis does not influence the mechanical axis directly. Extra-articular osteotomy is occasionally needed to reverse severe deformities.**
**REFERENCES: Papadopoulos EC, Parvizi J, Lai CH, et al: Total knee arthroplasty following distal femoral fractures. Knee 2002;9:267-274.**
**Lonner JH, Siliski JM, Lotke PA: Simultaneous femoral osteotomy and total knee arthroplasty for treatment of osteoarthritis associated with severe extra-articular deformity. J Bone Joint Surg Am 2000;82:342-348.**
**80/. Figure 49 shows a histologic section of the lung in a patient who died during total hip arthroplasty. What unexpected finding is seen in the pulmonary capillaries?
1- Pulmonary embolism
2- Methylmethacrylate cement
3- Hemorrhagic infarct
4- Granuloma formation
5- Amyloid
PREFERRED RESPONSE: 2**
**DISCUSSION: Sudden death during total hip arthroplasty has been reported. In a report from the Mayo Clinic, intraoperative death occurred during cemented total hip arthroplasty in
23 patients. Fat and marrow embolization during preparation of the femur or cementing of the femoral component was believed to be responsible for the cardiopulmonary collapse that occurred during arthroplasty. Although fat and marrow emboli were found in the pulmonary capillaries of most of the patients on autopsy, this histologic section shows two particles of cement in the pulmonary capillaries.**
**REFERENCES: Parvizi J, Holiday AD, Ereth MH, et al: The Frank Stinchfield Award. Sudden death during primary hip arthroplasty. Clin Orthop 1999;369:39-48.**
**Patterson BM, Healy JH, Cornell CN, et al: Cardiac arrest during hip arthroplasty with a cemented long-stem component: A report of seven cases. J Bone Joint Surg Am
1991;73:271-277.**
**81/. After trial placement of components in a primary total knee arthroplasty, the knee is unable to come to full extension, but the flexion gap is appropriately balanced. After adequate soft-tissue releases have been performed, what is the next most appropriate action to balance the reconstruction?
1- Use a larger femoral component
2- Use a thinner polyethylene insert
3- Add posterior femoral augments
4- Resect more proximal tibia
5- Resect additional distal femur
PREFERRED RESPONSE: 5**
**DISCUSSION: The reconstruction requires additional resection of the distal femur to allow increased extension while maintaining the current flexion gap tension. Resecting more proximal tibia or decreasing the tibial polyethylene thickness will decrease flexion tension as well as extension tension. Adding posterior femoral augments and using a larger femoral component will increase flexion tension.**
**REFERENCES: Ayers DC, Dennis DA, Johanson NA, et al: Common complications of total knee arthroplasty. J Bone Joint Surg Am 1997;79:278-311.**
**Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 281-286.**
**82/. Figure 50 shows the cross table lateral radiograph of a 31-year-old paratrooper who has recalcitrant groin pain. The pain is worse after activities such as standing or sitting (driving). Examination reveals that pain can be reproduced by internal rotation of the leg with the hip and knee in 90 degrees of flexion. Extensive nonsurgical management has failed to provide relief. What is the treatment of choice?
1- Periacetabular osteotomy
2- Femoral neck osteotomy
3- Femoroacetabular osteoplasty
4- Hip arthroscopy and labral debridement
5- Hip arthrodesis
PREFERRED RESPONSE: 3**
**DISCUSSION: The radiograph reveals the classic “bump” that is seen in patients with femoroacetabular impingement (FAI). Ganz and associates described two types of FAI. This patient has cam impingement, which describes a nonspherical femoral head being forced into the acetabulum during hip motion and resulting in labral and chondral injury. Hip arthroscopy and labral debridement is unlikely to control the symptoms because the underlying anatomic abnormality is often difficult to address with arthroscopy. The treatment involves surgical dislocation of the hip with preservation of the blood supply to the femoral head, removal of the asphericity on the femoral side (femoral osteoplasty), and removal of the acetabular rim (acetabular osteoplasty) if the latter is found to contribute to impingement.**
**REFERENCES: Ganz R, Gill TJ, Gautier E, et al: Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-1124.**
**Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for early osteoarthritis of the hip. Clin Orthop 2003;417:112-120.**
**Beck M, Leunig M, Parvizi J, et al: Anterior femoroacetabular impingement: Part II. Midterm results of surgical treatment. Clin Orthop 2004;418:67-73.**
**83/. During total knee arthroplasty, the patella is noted to subluxate laterally despite a lateral retinacular release. Which of the following methods is most likely to improve patellar stability?
1- Slight external rotation of the tibial component
2- Slight internal rotation of the femoral component
3- Slight anterior translation of the tibial component
4- Use of a fixed-bearing knee as opposed to a mobile-bearing knee
5- Use of a thicker patellar component
PREFERRED RESPONSE: 1**
**DISCUSSION: Slight external rotation of the tibial component will cause a net medialization of the tibial tubercle when the knee is articulated. This will help centralize the extensor mechanism over the trochlear groove and minimize the tendency for lateral subluxation. Internal rotation of the femoral component increases the risk of patellar instability. Anterior translation of the tibial component moves the patellar tendon insertion posteriorly, and may increase force on the patella but should not substantially alter patellar tracking. Clinical studies have shown no patellofemoral benefits to the use of fixed- or mobile-bearing designs. Thicker patellar components will not improve tracking, and may compound the problem.**
**REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 207, 323-337**
**Pagnano MW, Trousdale RT, Stuart MJ, et al: Rotating platform knees did not improve patellar tracking: A prospective, randomized study of 240 primary total knee arthroplasties. Clin Orthop 2004;428:221-227.**
**Lotke PA, Garino JP (eds): Revision Total Knee Arthroplasty. Philadelphia PA, Lippincott-Raven, 1999, pp 427-435.**
**84/. A 73-year-old man has stiffness after undergoing primary posterior cruciate
ligament-retaining total knee arthroplasty 18 months ago. Extensive physiotherapy, dynamic splinting, and manipulations under anesthesia have failed to result in improvement. Examination reveals range of motion from 30 degrees to 60 degrees of flexion. The components are well fixed, and the evaluation for infection is negative. In discussing the possibility of revision arthroplasty, the patient should be advised that**
**
1- the success of improving range of motion to a functional range of 0 degrees
to 90 degrees in the literature is between 75% to 80%.
2- the preoperative arc of motion will not influence the ultimate range of motion after formal component revision.
3- change from a posterior cruciate ligament-retaining to a posterior cruciate ligament-substituting design has a much greater chance of success.
4- manipulation under anesthesia will effectively improve range of motion if postoperative stiffness develops following revision.
5- the major postoperative focus will be to regain near full extension.
PREFERRED RESPONSE: 5**
**DISCUSSION: Stiffness following primary total knee arthroplasty remains a vexing problem. Treatment options have included extensive physical therapy, dynamic splinting, manipulation under anesthesia, arthroscopic arthrolysis, open arthrolysis with polyethylene exchange, and ultimately revision arthroplasty. Results are not as gratifying as would be expected. Babis and associates performed an open arthrolysis and polyethylene exchange on seven patients who were followed for a mean of 4.2 months. The results were poor. The mean improvement in arc of motion was only 20 degrees. Nicholls and Dorr treated 13 patients for stiffness. Only 40% of those patients obtained good to excellent results. Four patients (30%) required manipulation because of recurrent stiffness postoperatively. They noted they could not predictably improve the arc of motion with a revision operation. Haidukewych and associates reported on 15 patients who underwent revision of well-fixed components after total knee arthroplasty for stiffness. Of the 15 patients, 10 (66%) were satisfied with the outcome revision. Interestingly, they noted that in patients for whom the total arc of motion did not improve but who regained near full extension, there was a greater amount of satisfaction with the procedure than for those who did not regain full extension.**
**REFERENCES: Babis GC, Trousdale RT, Pagnano MW, et al: Poor outcomes of isolated tibial insert exchange and arthrolysis for the management of stiffness following total knee arthroplasty. J Bone Joint Surg Am 2001;83:1534-1536.**
**Nicholls DW, Dorr LD: Revision surgery for stiff total knee arthroplasty. J Arthroplasty 1990;5:S73-S77.**
**Haidukewych GJ, Jacofsky DJ, Pagnano MW, et al: Functional results after revision of well-fixed components for stiffness after primary total knee arthroplasty. J Arthroplasty 2005;20:133-138.**
**85/. A 62-year-old patient is seen for routine follow-up after undergoing cementless total hip arthroplasty 2 years ago. The patient reports limited range of motion that severely affects daily activities. A radiograph is shown in Figure 51. Management should now consist of
1- observation only.
2- nonsteroidal anti-inflammatory drugs and protected weight bearing.
3- irradiation to the affected area.
4- surgical excision.
5- surgical excision and postoperative irradiation.
PREFERRED RESPONSE: 5**
**DISCUSSION: The patient has symptomatic postoperative heterotopic ossification after total hip arthroplasty. Postoperative prophylactic treatments include nonsteroidal anti-inflammatory drugs (usually indomethacin) or low-dose irradiation. The heterotopic ossification shown here is quite mature; therefore, nonsurgical management will not be successful. Surgical excision of grade III or IV heterotopic ossification should be followed with postoperative irradiation to minimize the chances of recurrence.**
**REFERENCES: Ayers DC, Evarts CM, Parkinson JR: The prevention of heterotopic ossification in high-risk patients by low-dose radiation therapy after total hip arthroplasty. J Bone Joint Surg Am 1986;68:1423-1430.**
**Healy WL, Lo TC, DeSimone AA, et al: Single-dose irradiation for the prevention of heterotopic ossification after total hip arthroplasty: A comparison of doses of five hundred and fifty and seven hundred centigray. J Bone Joint Surg Am 1995;77:590-595.**
**86/. What bilateral surgical intervention is considered inappropriate based on the findings shown in the radiograph in Figure 52?
1- Vascularized fibular graft
2- Proximal femoral osteotomy
3- Core decompression
4- Hip arthrodesis
5- Femoral resurfacing
PREFERRED RESPONSE: 4**
**DISCUSSION: The radiograph reveals osteonecrosis of both femoral heads with reasonably maintained joint surfaces. There may be some slight flattening of the femoral heads. Hip arthrodesis is difficult to perform because of the necrotic bone. Its use in patients with osteonecrotic hips is limited because of the 80% bilaterality; therefore, it is not an acceptable alternative. All the other options are acceptable interventions.**
**REFERENCES: Mont MA, Jones LC, Sotereanos DG, et al: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect 2000;49:169-185.**
**Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.**
**87/. Figure 53a shows the AP radiograph of a 70-year-old patient who is scheduled to undergo unicompartmental knee arthroplasty. Figure 53b shows the immediate postoperative radiograph, and the radiograph shown in Figure 53c, obtained 6 months after surgery, shows a medial tibial plateau fracture. The etiology of the fracture is best related to
1- marked osteoporosis.
2- reduced contact area of a unicompartmental knee arthroplasty for load transmission.
3- excessive medial placement of the tibial component of the unicompartmental knee arthroplasty.
4- multiple drill holes that violate the medial cortex.
5- osteonecrosis of the medial tibial plateau.
PREFERRED RESPONSE: 4**
**DISCUSSION: While all of the above may contribute to the etiology of a tibial plateau fracture following unicompartmental knee arthroplasty, the recent literature has clearly noted that pin placement for fixation of tibial resection guides is the most critical factor associated with a tibial plateau fracture following unicompartmental knee arthroplasty. Vince and Cyran suggest that fractures associated with unicompartmental knee arthroplasty might be avoidable by limiting the number and paying attention to the location of the pin holes that are created to secure the tibial resection guides. Brumby and associates suggest avoiding multiple guide pin holes in the proximal tibia for unicompartmental knee arthroplasty. They currently recommend the use of one centrally placed pin and an ankle clamp to stabilize the resection guide. Yang and associates note that a medial tibial plateau fracture in association with minimally invasive unicompartmental knee arthroplasty can be eliminated by avoiding fixation pins close to the medial tibial cortex.**
**REFERENCES: Brumby SA, Carrington R, Zayontz S, et al: Tibial plateau stress fracture: A complication of unicompartmental knee arthroplasty using 4 guide pinholes. J Arthroplasty 2003;18:809-812.**
**Yang KY, Yeo SJ, Lo NN: Stress fracture of the medial tibial plateau after minimally invasive unicompartmental knee arthroplasty: A report of 2 cases. J Arthroplasty 2003;18:801-803.**
**Vince KG, Cyran LT: Unicompartmental knee arthroplasty: New indications, more complications? J Arthroplasty 2004;19:9-16.**
**88/. During impaction of a cementless acetabular component, the posterior column was fractured and found to be displaced. Which of the following is considered the most appropriate surgical option?
1- Exchange of the cementless cup to a larger component
2- Retention of the component and bone grafting of the fracture
3- Retention of the component and postoperative weight protection until the posterior column heals
4- Removal of the cup, fixation of the posterior column, and application of an antiprotrusio cage
5- Removal of the cup and cementing of an all-polyethylene liner
PREFERRED RESPONSE: 4**
**DISCUSSION: Acetabular bone loss presents a challenge during reconstruction. A cementless hemispherical cup can be used in most patients provided that the acetabular rim, particularly the posterior column, is intact. When the posterior column is disrupted, fixation with a reconstruction plate and/or the use of an antiprotrusio cage is recommended. The latter is particularly important when the posterior column is fractured and displaced, such as in this patient. Under these circumstances, reduction of the fracture and application of an antiprotrusio cage is recommended. In this particular type of case, some surgeons may elect to retain the hemispherical cup and apply an antiprotrusio cage over the cup (“cage over cup” technique).**
**REFERENCES: Berry DJ: Antiprotrusio cages for acetabular revision. Clin Orthop 2004;420:106-112.**
**Peterson CA, Lewallen DG: Periprosthetic fracture of the acetabulum after total hip arthroplasty. J Bone Joint Surg Am 1996;78:1206-1213.**
**89/. Which of the following factors increases the risk of sciatic nerve injury in primary total hip arthroplasty (THA)?
1- Male gender
2- Anterolateral approach
3- Posterior superior quadrant acetabular screw placement
4- Osteonecrosis
5- Developmental dysplasia of the hip
PREFERRED RESPONSE: 5**
**DISCUSSION: Injury to the sciatic nerve is a relatively rare but serious complication of THA. Dissection of the sciatic nerve is not typically done during primary THA, although the nerve can be identified during the surgical approach. An anterolateral approach to THA would not necessarily be associated with any greater incidence of sciatic nerve injury than other approaches. Screw fixation for the acetabular component is often a matter of surgeon preference. Provided that the anatomic safe zones for screw fixation (posterior inferior and posterior superior) are recognized, injury to the sciatic nerve from acetabular screws can be minimized. Restoration of anatomic length is important in primary THA. Overlengthening can result in sciatic nerve palsy. Developmental dysplasia of the hip can lead to a congenitally shortened extremity with concomitant congenital shortening of the associated neurovascular structures. Overlengthening of the extremity during THA for developmental dysplasia of the hip can lead to sciatic palsy. Osteonecrosis is not an associated risk factor for sciatic nerve palsy.**
**REFERENCES: DeHart MM, Riley LH Jr: Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg 1999;7:101-111.**
**Anas P, Felix B: Evaluation and prevention of postoperative complications, in Neurologic Injury in Revision THA. New York, NY, Springer Verlag, 1999, pp 361-371.**
**90/. A 68-year-old woman who underwent a right total hip arthroplasty 1 year ago has dislocated her hip five times since surgery. Radiographs show a retroverted acetabular component. What is the best treatment for this patient?
1- Use a constrained acetabular liner
2- Revise the femoral component to provide greater femoral offset
3- Revise the femoral head from a 28-mm head size to a 36-mm head size
4- Revise the acetabular component to 15 degrees of anteversion and 45 degrees of abduction
5- Perform a greater trochanteric osteotomy to improve soft-tissue tension
PREFERRED RESPONSE: 4**
**DISCUSSION: The most common cause of recurrent dislocation following total hip arthroplasty continues to be component malposition. Component malposition should be addressed prior to any other treatment options, such as increasing soft-tissue tension with increased femoral offset or greater trochanteric advancement. A larger femoral head size may help, but correcting the component malposition should give more predictable results. A retroverted acetabular component should be revised to 15 degrees to 20 degrees of anteversion, matching the patient’s anatomy with an abduction angle close to 45 degrees.**
**REFERENCES: Daly PJ, Morrey BF: Operative correction of an unstable total hip arthroplasty. J Bone Joint Surg Am 1992;74:1334-1343.**
**Jolles BM, Zangger P, Leyvraz PF: Factors predisposing to dislocation after primary total hip arthroplasty: A multivariate analysis. J Arthroplasty 2002;17-282-288.**
**Hamilton W, McAuley JP: Evaluation of the unstable total hip arthroplasty. Inst Course Lect 2004;53:87-92.**
**91/. Figure 54 shows the preoperative radiograph of a 45-year-old woman who is considering total hip arthroplasty with her orthopaedic surgeon. What femoral characteristic is a typical concern in this patient?
1- Osteopenia
2- Excessive anteversion
3- Excessive varus
4- Excessive bowing
5- Stove-pipe femur
PREFERRED RESPONSE: 2**
**DISCUSSION: Developmental dysplasia of the hip (DDH) leads to early arthritis of the hip as seen in this patient. Although DDH is believed to mostly affect the acetabulum, most patients with DDH also have anatomic aberrations of the femur. Using three-dimensional computer models generated by reconstruction of CT scans, dysplastic femurs were shown to have shorter necks and smaller, straighter canals than the controls. The shape of the canal became more abnormal with increasing subluxation. The studies also have shown that the primary deformity of the dysplastic femur is rotational, with an increase in anteversion of 5 degrees to 16 degrees, depending on the degree of subluxation of the hip. The rotational deformity of the dysplastic femur arises within the diaphysis between the lesser trochanter and the isthmus and is not attributable to a torsional deformity of the metaphysis. Osteopenia is not a concern in a patient with an excellent cortical index (thick cortices and narrow canal). Femoral varus or bowing of the femur is not a typical finding in patients with DDH.**
**REFERENCES: Noble PC, Kamaric E, Sugano N, et al: Three-dimensional shape of the dysplastic femur: Implications for THR. Clin Orthop 2003;417:27-40.**
**Sugano N, Noble PC, Kamaric E, et al: The morphology of the femur in developmental dysplasia of the hip. J Bone Joint Surg Br 1998;80:711-719.
92/. A 68-year-old man with no significant medical history underwent a total knee arthroplasty 4 years ago. A radiograph is shown in Figure 55. He reports that he had no problems with the knee until 6 weeks ago when he noted the gradual onset of pain following a colonoscopy. Examination reveals a painful, swollen knee. Knee aspiration reveals a WBC count of 40,000/mm3. Management should consist of
1- suppressive antibiotics.
2- open irrigation and debridement with polyethylene exchange.
3- one-stage resection arthroplasty and reimplantation.
4- two-stage resection arthroplasty and reimplantation.
5- arthroscopic irrigation and debridement.
PREFERRED RESPONSE: 4**
**DISCUSSION: The treatment of choice for a late hematogenous infection is two-stage resection arthroplasty and reimplantation, with parenteral antibiotics prior to reimplantation. This is particularly true when septic loosening has occurred as in this patient. Open irrigation and debridement with polyethylene exchange has been used successfully when the duration of symptoms is 3 weeks or less. Long-term suppressive antibiotics are most commonly used when the patient’s medical condition precludes further surgery. Delayed reimplantation has been shown to be superior to immediate reimplantation in multiple studies. Little data support the use of arthroscopic irrigation and debridement.**
**REFERENCES: Swanson KC, Windsor RE: Diagnosis of infection after total knee arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1485-1491.**
**Hanssen AD, Rand JA, Osmon DR: Management of the infected total knee arthroplasty, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 1070-1089.**
**93/. Which of the following substances makes up the majority by weight of the extracellular matrix for articular cartilage?
1- Keratin sulfate
2- Collagen type II
3- Water
4- Protein
5- Chondroitin sulfate
PREFERRED RESPONSE: 3**
**DISCUSSION: The extracellular matrix consists of water, proteoglycans, and collagen. Water makes up the majority (approximately 65% to 80%) of wet weight; 95% of the collage is type II with much smaller amounts of other collagens, including types IV, VI, IX, X, and XI. The exact functions of these other collagens are unknown, but they are believed to be important in matrix attachment and stabilization of the diameter of collagen fibrils.**
**REFERENCES: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 444-445.**
**Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 3-18.**
**94/. A 58-year-old woman is seen in the emergency department after falling at home. History reveals that she underwent right total knee arthroplasty 2 years ago. Radiographs are shown in Figures 56a and 56b. What is the most appropriate treatment?
1- Closed reduction and casting
2- Bed rest and skeletal traction
3- Open reduction and internal fixation
4- Retrograde intramedullary nailing
5- Revision of the femoral component with a stemmed component
PREFERRED RESPONSE: 3**
**DISCUSSION: The radiographs show an oblique periprosthetic distal femoral fracture. Of the options listed, open reduction and internal fixation is the most appropriate surgical option because a well-fixed, posterior stabilized closed box femoral component is present. Nonsurgical methods are not favored because of the highly displaced, unstable fracture pattern and prolonged immobility. Revision with a stemmed component is an option but would sacrifice more bone stock in this younger patient.**
**REFERENCES: Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209.**
**Raab GE, Davis CM III: Early healing with locked condylar plating of periprosthetic fractures around the knee. J Arthroplasty 2005;20:984-989.**
**Tharani R, Nakasone C, Vince KG: Periprosthetic fractures after total knee arhtroplasty.**
**J Arthroplasty 2005;20:27-32.**
**95/. A patient with a valgus knee and lateral compartment bone loss undergoes a total knee arthroplasty using posterior condylar referencing instrumentation. Six months after surgery, the patient reports significant anterior knee pain, and radiographs reveal severe lateral patellar tilt. Management should consist of
1- lateral retinacular release.
2- femoral component revision.
3- medialization of the patellar component.
4- patellectomy.
5- tibial tubercle transfer.
PREFERRED RESPONSE: 2**
**DISCUSSION: Severe valgus deformity is frequently accompanied by hypoplasia of the lateral femoral condyle. Posterior referencing instrumentation can substantially internally rotate the femoral component with respect to the transepicondylar axis and Whiteside’s line. The femoral component malrotation must be corrected to properly address this problem.**
**REFERENCES: Berger RA, Della Valle CJ, Rubash HE: Patellofemoral problems in total knee arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1245-1258.**
**Whiteside LA, Arima J: The anteroposterior axis for femoral rotational alignment in valgus total knee arthroplasty. Clin Orthop 1995;321:168-172.**
**96/. Figures 57a through 57c show the radiographs of a patient who has pain, discomfort, and a popping sensation localized to the posterior aspect of the knee after undergoing primary left total knee arthroplasty 6 months ago. Examination reveals that the patient is able to ambulate without a limp. There is no significant swelling, erythema, or effusion. Range of motion is 0 degrees to 115 degrees, and a palpable crepitation or snapping is detected at the posterior lateral joint line. What is the most likely diagnosis?
1- Popliteal snapping syndrome
2- Patellar clunk syndrome
3- Subluxation secondary to a tight posterior cruciate ligament
4- Soft-tissue irritation secondary to retained polymethylmethacrylate
5- Patellar subluxation secondary to a tight lateral retinaculum
PREFERRED RESPONSE: 1**
**DISCUSSION: Popliteal snapping syndrome represents the most likely diagnosis. Barnes and Scott noted that the popliteus tendon can be a potential source of internal derangement after total knee arthroplasty. They noted that it can be subluxated anteriorly and posteriorly over a retained lateral femoral condyle osteophyte. Allardyce and associates described the condition as a popliteus condition, snapping as it rolls over a retained lateral femoral condylar osteophyte. Patellar clunk syndrome is a distinct syndrome associated with the patella and has been reported in posterior stabilized knees. In addition to crepitation with range of motion, the patella literally snaps or jumps as the knee is taken from flexion to extension.**
**REFERENCES: Beight JL, Yao B, Hozack WJ, et al: The patellar “clunk” syndrome after posterior stabilized total knee arthroplasty. Clin Orthop 1994;299:139-142.**
**Barnes CL, Scott RD: Popliteus tendon dysfunction following total knee arthroplasty.**
**J Arthroplasty 1995;10:543-545.**
**Allardyce TJ, Scuderi GR, Insall JN: Arthroscopic treatment of popliteus tendon dysfunction following total knee arthroplasty. J Arthroplasty 1997;12:353-355.**
**97/. Which of the following is the primary mechanism of polyethylene wear in the hip?
1- Fatigue cracking and delamination
2- Oscillatory fretting
3- Crevice corrosion
4- Oxidative degradation
5- Adhesion and abrasion
PREFERRED RESPONSE: 5**
**DISCUSSION: Although previous theories on acetabular wear implicated fatigue cracking and delamination as primary wear mechanisms, these have actually manifested as major modes of polyethylene wear in knees. The primary mechanism of wear in polyethylene acetabular components appears to be adhesion and abrasion. In an analysis of 128 components retrieved at autopsy or revision surgery, wear appeared to occur mostly at the surface of the components and was the result of large strain plastic deformation and orientation of the surface layers into fibrils that subsequently ruptured during multidirectional motion. It was also shown conclusively that 32-mm heads displayed significantly more wear (volumetric wear) than either 22-mm or
26-/28-mm heads (1-mm increase in size increased volumetric wear by 10%). The wear at the articulating surface was characterized by highly worn polished areas superiorly and less worn areas inferiorly separated by a ridge. Abrasion was very common, occurring after adhesion and plastic deformation of polyethylene fibrils, and abrasion secondary to third-body wear. Wear rates decreased with longer survival of components, indicating a “bedding in” phenomenon, arguing against oxidative and fatigue wear. Crevice corrosion occurs in fatigue cracks with low oxygen tension (under screw heads, etc). Oscillatory fretting consists of cyclical abrading of the outer surface from small movements. Fatigue and delamination is predominant in total knee arthroplasty where stresses are maximum just below the surface of the polyethylene component, causing fatigue over time with subsequent delamination. In contrast, hip wear occurs primarily at the surface of the polyethylene component.**
**REFERENCES: Jasty M, Goetz DD, Bragdon CR, et al: Wear of polyethylene acetabular components in total hip arthroplasty: An analysis of one hundred and twenty-eight components retrieved at autopsy or revision operations. J Bone Joint Surg Am 1997;79:349-358.**
**Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 47-53.**
**Bell CJ, Walker PS, Abeysundera MR, et al: Effect of oxidation on delamination of**
**ultrahigh-molecular-weight polyethylene tibial components. J Arthroplasty 1998;13:280-290.**
**Sutula LC, Collier JP, Saum KA, et al: The Otto Aufranc Award: Impact of gamma sterilization on clinical performance of polyethylene in the hip. Clin Orthop 1995;319:28-40.**
**98/. Which of the following complications may occur subsequent to resurfacing hip arthroplasty for osteonecrosis of the hip but not after total hip arthroplasty?
1- Aseptic loosening of the acetabular component
2- Fracture of the femoral neck
3- Fracture of the acetabulum
4- Infection
5- Groin pain
PREFERRED RESPONSE: 2**
**DISCUSSION: Advocates of resurfacing hip arthroplasty cite preservation of the proximal femoral bone stock as the main advantage of this procedure over total hip arthroplasty. Fracture of the retained femoral neck has been reported following resurfacing arthroplasty. The exact etiology of the latter is unknown. Technical errors, such as notching of the femoral neck or possibly disruption of the blood supply to the femoral head during extensive soft-tissue exposure, may result in femoral neck fracture.**
**REFERENCES: Gabriel JL, Trousdale RT: Stem fracture after hemiresurfacing for femoral head osteonecrosis. J Arthroplasty 2003;18:96-99.**
**Amstutz HC, Campbell PA, Le Duff MJ: Fracture of the neck of the femur after surface arthroplasty of the hip. J Bone Joint Surg Am 2004;86:1874-1877.**
**99/. Which of the following statements best describes results that have been reported with roentgen stereophotogrammetric analysis (RSA)?
1- Cemented total hip stems do not migrate.
2- Well-fixed total hip stems (cemented or cementless) migrate approximately
3 degrees and 5 mm in the first year.
3- Any early migration (ie, greater than 0 mm less than 6 months after surgery) portends failure of the component.
4- Migration greater than 1 mm to 2 mm in the first year is associated with a higher risk of loosening.
5- The system has been proven to not be as accurate as claimed and has been abandoned.
PREFERRED RESPONSE: 4**
**DISCUSSION: Migration of total hip femoral components has been measured by RSA, a technique that affords accuracy of 2 degrees and 0.5 mm. Several published studies on total hip arthroplasty femoral components have established the importance of this technique. Both cemented and cementless components migrate, with the rate of migration suggesting the adequacy of fixation of a component. Migration of 1 mm to 2 mm (occurring in either the
varus-coronal plane and retroversion-transverse plane, or both) has been associated with a higher risk of loosening of the component.**
**REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 100.**
**100/. Osteonecrosis of the large joints may develop in patients with which of the
following conditions?
1- Collagen I disease
2- Antiphospholipid syndrome (APS)
3- Hemochromatosis
4- Achondroplasia
5- Paget’s disease
PREFERRED RESPONSE: 2**
**DISCUSSION: Osteonecrosis of major joints can occur in patients exposed to corticosteroids, alcohol, and antiseizure medications, as well as patients with hemaglobulinopathy, such as sickle cell anemia. In addition, patients with primary APS who had not taken corticosteroids were also found to be at high risk for osteonecrosis of the hip. In one study of 30 patients with primary APS, asymptomatic osteonecrosis was evident in 20%. A recent article has also found a high association between idiopathic osteonecrosis of the hip and collagen II mutation. None of the other conditions has been shown to be associated with a higher risk of osteonecrosis.**
**REFERENCES: Tektonidou MG, Malagari K, Vlachoyiannopoulos PG, et al: Asymptomatic avascular necrosis in patients with primary antiphospholipid syndrome in the absence of corticosteroid use: A prospective study by magnetic resonance imaging. Arthritis Rheum 2003;48:732-736.**
**Liu YF, Chen WM, Lin YF, et al: Type II collagen gene variants and inherited osteonecrosis of the femoral head. N Engl J Med 2005;352:2294-2301.**
QUESTION 28 OF 50
In patients with a closed tibia fracture and suspected compartment syndrome, the region of the leg that will most likely have the highest tissue pressure measurement is:
1
The middle of the leg
2
5 cm proximal to the fracture site
3
At the level of the fracture
4
5 cm distal to the fracture site
5
The proximal one-third of the leg
In a study by Heckman and colleagues, the level of the fracture site is the region with the highest tissue pressure. This was found to be true in all four components. The highest pressures are located in the anterior and deep posterior components.
QUESTION 29 OF 50
of 100
What is the strongest risk factor for plantar fasciitis?
What is the strongest risk factor for plantar fasciitis?
1
Female gender
2
African American ancestry
3
BMI higher than 30
4
Weight lifting and body building
- BMI higher than 30
QUESTION 30 OF 50
You are asked to consult on a 4-day-old neonate admitted because of failure to thrive. She has swelling of her left shoulder. Examination reveals limited motion of her hips and left shoulder. Radiographs of the shoulder and pelvis are negative. Laboratory studies show a WBC count of 24,000/mm3, an erythrocyte sedimentation rate of 50/h, and C-reactive protein is 16.4. What is the next most appropriate step in management?
1
Ultrasound of the hip and shoulder
2
Bone scan
3
MRI of the shoulder
4
Pavlik harness
5
Excision and drainage
DISCUSSION: Ultrasound of both the hip and the shoulder can show the presence of septic arthritis and osteomyelitis. Multiple sites of infection are common in neonates. A bone scan can be used to identify other areas of involvement.
REFERENCES: Wong M, Isaacs D, Howman-Giles R, et al: Clinical and diagnostic features of osteomyelitis occurring in the first three months of life. Pediatr Infect Dis J 1995;14:1047-1053.
Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 57-73.
REFERENCES: Wong M, Isaacs D, Howman-Giles R, et al: Clinical and diagnostic features of osteomyelitis occurring in the first three months of life. Pediatr Infect Dis J 1995;14:1047-1053.
Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 57-73.
QUESTION 31 OF 50
A 16-year-old boy with osteochondritis dissecans of the capitellum has intermittent symptoms of catching and locking. Examination is unremarkable. Radiographs reveal a loose body anteriorly with a diameter of 10 mm. To remove the loose body, elbow arthroscopy is being considered. Which of the following procedures would minimize the risk of neurovascular complication during the procedure?
1
Keeping a smooth plastic cannula in each portal after it is established
2
Using an image intensifier to localize the loose body
3
Distending the elbow joint capsule prior to establishing the anterolateral portal
4
Placing the scope in the proximal anteromedial portal and then enlarging the anterolateral portal so that it is bigger than the maximum diameter of the loose body
5
Breaking up the loose body into several pieces prior to extracting it
Complications of elbow arthroscopy are usually minor or temporary. However, serious complications include nerve injuries. The deep radial nerve is the closest to any of the portals, resting as close as 1 mm away from the scope inserted in the anterolateral portal. The capsule can be displaced anteriorly by distending the joint with about 25 mL of saline solution, thus moving the deep radial nerve approximately 1 cm anteriorly and decreasing the risk of injuring it while establishing the anterolateral portal. Keeping plastic cannulae in the portals may help to diminish fluid extravasation and swelling, which is more of an impediment than a serious complication. The image intensifier has no documented role in guiding loose body removal. While the proximal anteromedial portal is probably the safest anterior portal to establish, it is actually easier to remove a large loose body from this portal while viewing it from an anterolateral position. There is less tendon and muscle bulk to pass through at the site of the proximal anteromedial portal than at the anterolateral portal, making it less likely for the loose body to get stuck in the soft tissues. Techniques have been developed to permit removal of loose bodies as large as 2 cm in diameter without breaking them up into pieces. If it is possible to remove a large loose body intact, doing so greatly simplifies and shortens the procedure.
REFERENCES: Lynch GJ, Meyers JF, Whipple TL, Caspari RB: Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy 1986;2:190-197.
O’Driscoll S: Loose bodies and synovial conditions, in Green D, Hotchkiss R, Pederson W (eds): Green’s Operative Hand Surgery. New York, NY, Churchill Livingstone, 1999, pp 235-249.
REFERENCES: Lynch GJ, Meyers JF, Whipple TL, Caspari RB: Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy 1986;2:190-197.
O’Driscoll S: Loose bodies and synovial conditions, in Green D, Hotchkiss R, Pederson W (eds): Green’s Operative Hand Surgery. New York, NY, Churchill Livingstone, 1999, pp 235-249.
QUESTION 32 OF 50
Which of the following structures are found in the anterior tarsal tunnel?
1
Extensor hallucis longus, tibialis anterior, extensor digitorum longus, dorsalis pedis artery, deep peroneal nerve
2
Extensor hallucis longus, tibialis anterior, extensor digitorum longus, dorsalis pedis artery, superficial peroneal nerve
3
Extensor hallucis longus, tibialis anterior, extensor digitorum longus, dorsalis pedis artery, deep peroneal nerve, superficial peroneal nerve
4
Extensor hallucis brevis, extensor hallucis longus, extensor digitorum longus, dorsalis pedis artery, deep peroneal nerve
5
Dorsalis pedis artery, deep peroneal nerve, superficial peroneal nerve
The contents of the anterior tarsal tunnel are the extensor hallucis longus, tibialis anterior, extensor digitorum longus, dorsalis pedis artery, and the deep peroneal nerve. The term “anterior tarsal tunnel syndrome” is used to specifically describe the compression of the deep peroneal nerve under the inferior extensor retinaculum. With nerve compression, patients report a burning sensation across the dorsum of the foot with paresthesias in the first web space. There also may be wasting and weakness of the extensor digitorum brevis.
REFERENCES: Kuritz HM: Anterior entrapment syndromes. J Foot Surg 1976;15:143-148.
Sarrafian S: The Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 113-158.
REFERENCES: Kuritz HM: Anterior entrapment syndromes. J Foot Surg 1976;15:143-148.
Sarrafian S: The Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 113-158.
QUESTION 33 OF 50
Accurate evaluation of the upper portion of the subscapularis muscle is best accomplished with active internal rotation**
1
in adduction and the arm in external rotation.
2
in adduction and the arm in neutral rotation.
3
with the dorsum of the hand on the buttocks.
4
with the dorsum of the hand on the midlumbar level.
5
with the palm of the hand pressing against the belly.
Internal rotators of the shoulder include the subscapularis, pectoralis major, teres major, and latissimus dorsi muscles. The subscapularis has two portions, with the upper portion receiving its innervation from the upper subscapular nerve (C5) and the lower portion from the lower subscapular nerve (C5-6). The two tests commonly performed to isolate the internal rotation to the subscapularis muscle are the lift-off test and the belly press test. Electromyographic findings have shown the lift-off test to be more accurate for the lower portion of the subscapularis and the belly press test to be more sensitive for the upper portion.
REFERENCES: Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ: Electromyographic activity and applied load during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med 1998;26:210-220.
Greis PE, Kuhn JE, Schultheis J, Hintermeister R, Hawkins R: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
REFERENCES: Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ: Electromyographic activity and applied load during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med 1998;26:210-220.
Greis PE, Kuhn JE, Schultheis J, Hintermeister R, Hawkins R: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
QUESTION 34 OF 50
Which of the following muscles is innervated by the posterior interosseous nerve:
1
Extensor carpi ulnaris
2
Extensor digiti minimi
3
Extensor pollicis brevis and longus
4
Abductor pollicis longus
5
All of the above
The posterior interosseous nerve innervates a number of muscles involved primarily in finger extension, including the extensor carpi ulnaris, extensor digitorum, extensor digiti minimi, extensor pollicis brevis and longus, abductor pollicis longus, and extensor indices.
QUESTION 35 OF 50
..The fracture seen in Figure 17 is most likely associated with injury to what ligamentous structure?
1
Inferior glenohumeral ligament
2
Acromioclavicular (AC) ligaments
3
Coracoclavicular ligaments
4
Coracoacromial ligament
DISCUSSION..The radiograph shows an extra-articular distal clavicle fracture lateral to the clavicular attachment point of the
coracoclavicular ligaments (conoid and trapezoid). However, unlike a scenario featuring a typical Neer type I fracture, the interval between coracoid and clavicle is clearly widened and there is marked fracture displacement. It is clear that the coracoclavicular ligaments must also be torn. The inferior glenohumeral ligament is important to glenohumeral joint stability, but has no effect on the relationship between clavicle and scapula. The AC ligaments are thickenings of the AC joint capsule. They have been shown to be responsible for 90% of anteroposterior stability of the AC joint. The coracoclavicular ligaments are responsible for 77% of stability for superior translation (as in this case). The coracoacromial ligament connects 2 parts of the scapula (coracoids and acromion) and is part of the arch that supports the rotator cuff.
- Coracoclavicular ligaments
QUESTION 36 OF 50
Figure A shows a below the knee amputation performed in a diabetic patient with significant vascular disease. Removal of the "dog ears", indicated by the red arrows, could cause direct damage to what vasculature leading to flap necrosis?

1
Anterior tibial artery
2
Saphenous and sural arteries
3
Posterior tibial artery
4
Peroneal artery
5
Lower popliteal artery
"Dog ears" at the edge of a long posterior flap BKA incision are typically left intact because removal risks posterior flap blood supply.
Gray et al conducted an anatomic study to examine the BKA vascular anatomy and specifically the blood supply contribution of the soleus muscle. In their article, they describe the saphenous and sural arteries as being the main blood supply to the proximal posterior aspect of the calf. These arteries lie on the medial and lateral border of a long posterior flap, and can be at risk for transection when excising "dog ears". These arteries are particularly important in patients with severe vascular disease, as the popliteal artery and its immediate branches may be occluded, while the collateral smaller vessels (ie. saphenous and sural arteries) remain patent. Of note, the authors did conclude that the soleus muscle does not contribute blood supply to a long posterior flap, and it should be entirely excised.
Faltie-Jensen et al compared the rate of complications with long posterior flaps vs. equal sagittal flaps in diabetic and non-diabetic patients. They found that in diabetic patients, there was a higher incidence of infection and failure of wound healing in patients with the long posterior flap.
Manoli argues against the use of equal coronal flap, "fish mouth" incisions for below the knee amputations in patients with diabetes and peripheral vascular disease because of the increased risk of anterior flap necrosis.
Gray et al conducted an anatomic study to examine the BKA vascular anatomy and specifically the blood supply contribution of the soleus muscle. In their article, they describe the saphenous and sural arteries as being the main blood supply to the proximal posterior aspect of the calf. These arteries lie on the medial and lateral border of a long posterior flap, and can be at risk for transection when excising "dog ears". These arteries are particularly important in patients with severe vascular disease, as the popliteal artery and its immediate branches may be occluded, while the collateral smaller vessels (ie. saphenous and sural arteries) remain patent. Of note, the authors did conclude that the soleus muscle does not contribute blood supply to a long posterior flap, and it should be entirely excised.
Faltie-Jensen et al compared the rate of complications with long posterior flaps vs. equal sagittal flaps in diabetic and non-diabetic patients. They found that in diabetic patients, there was a higher incidence of infection and failure of wound healing in patients with the long posterior flap.
Manoli argues against the use of equal coronal flap, "fish mouth" incisions for below the knee amputations in patients with diabetes and peripheral vascular disease because of the increased risk of anterior flap necrosis.
QUESTION 37 OF 50
of 100
A 44-year-old patient who has had a proximal first metatarsal osteotomy has recurrent pain and difficulty wearing many types of shoes. Radiographs show a large 1-2 intermetatarsal angle (IMA).

A 44-year-old patient who has had a proximal first metatarsal osteotomy has recurrent pain and difficulty wearing many types of shoes. Radiographs show a large 1-2 intermetatarsal angle (IMA).
1
Lapidus procedure
2
First metatarsophalangeal (MTP) joint arthrodesis and lesser metatarsal head resection
3
Proximal first metatarsal osteotomy
4
Distal first metatarsal chevron osteotomy
5
Biplanar distal first metatarsal osteotomy
- Lapidus procedure
QUESTION 38 OF 50
A 44-year-old man has a 2-year history of pain in his hallux. The pain is accompanied by limited range of motion, pain on passive dorsiflexion of the hallux, and difficulty with athletic activities. Radiographs demonstrate that the plantar two-thirds of the joint is normal, with osteophytes of the dorsal surface of the joint. He has been unsuccessful with shoe wear modifications, and he requests surgery. The ideal procedure for him would be:
1
Resection arthroplasty
2
Implant arthroplasty
3
Osteotomy of the first metatarsal
4
C heilectomy of the hallux
5
Arthrodesis of the metatarsophalangeal joint
Preservation of the joint and maintaining range of motion are important to any active individual. Any procedure, such as resection or implant arthroplasty, is contraindicated in this age group. Arthritis has not progressed to the degree that arthrodesis is necessary.
QUESTION 39 OF 50
Figures 1 through 3 are the radiographs of a 65-year-old man who sustained a fracture from a fall. The patient elects open reduction and internal fixation of the distal radius. After plating the distal radius, the distal radioulnar joint (DRUJ) is examined and found to be unstable in both pronation and supination. What is the best next step?
---
---
---








---
---
---
1
Early range of motion (ROM) program with a removable short-arm splint
2
Long-arm casting in pronation for 4 weeks
3
Pin fixation of the DRUJ
4
Fixation of the ulnar styloid fracture
styloid fracture were found to increase risk for DRUJ instability. An ulnar styloid base fracture involves the insertion of the radioulnar ligaments and can cause DRUJ instability if displaced. If persistent instability is present after fixation of the ulnar styloid, DRUJ pinning is a reasonable option. Early ROM
The initial radiographs show a comminuted displaced distal radius fracture, along with a displaced fracture of the base of the ulnar styloid. The displacement is best seen on the oblique view. After reduction and fixation of the radius, DRUJ stability should be assessed. The majority of scenarios that involve this injury pattern will not be unstable because of the oblique band of the interosseous ligament. When DRUJ instability is present after fixation of the radius, reduction and fixation of the ulnar styloid fracture is the best option to provide stability of the distal radioulnar joint (DRUJ) (Figure below). A study by Lawton and associates revealed that all distal radius fractures complicated by DRUJ instability were accompanied by an ulnar styloid fracture. A fracture at the ulnar styloid’s base and substantial displacement of an ulnar
with splinting would not allow reduction or healing of the ulnar styloid and would result in persistent instability. Short-arm casting also would not allow stability of the DRUJ and would be a less reliable method with which to achieve healing of the ulnar styloid.
---
The initial radiographs show a comminuted displaced distal radius fracture, along with a displaced fracture of the base of the ulnar styloid. The displacement is best seen on the oblique view. After reduction and fixation of the radius, DRUJ stability should be assessed. The majority of scenarios that involve this injury pattern will not be unstable because of the oblique band of the interosseous ligament. When DRUJ instability is present after fixation of the radius, reduction and fixation of the ulnar styloid fracture is the best option to provide stability of the distal radioulnar joint (DRUJ) (Figure below). A study by Lawton and associates revealed that all distal radius fractures complicated by DRUJ instability were accompanied by an ulnar styloid fracture. A fracture at the ulnar styloid’s base and substantial displacement of an ulnar
with splinting would not allow reduction or healing of the ulnar styloid and would result in persistent instability. Short-arm casting also would not allow stability of the DRUJ and would be a less reliable method with which to achieve healing of the ulnar styloid.
---
QUESTION 40 OF 50
of 100
Figure 62
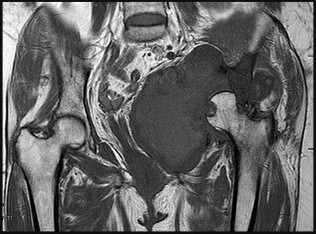
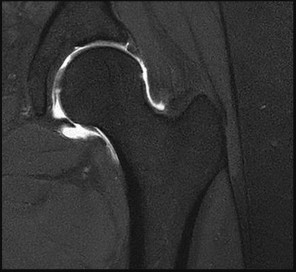
Figure 62
1
Osteonecrosis
2
Chondrosarcoma
3
Hip dysplasia
4
Transient osteoporosis of the hip
5
Femoral neck fracture
- Chondrosarcoma_
QUESTION 41 OF 50
-Decreased sun exposure leads to decreased bone health via what mechanism?
1
Impaired ability of the liver to hydroxylate cholecalciferol
2
Impaired ability of the kidneys to hydroxylate cholecalciferol
3
Impaired parathyroid hormone (PTH) production by the parathyroid glands
4
Impaired absorption of calcium by the gastrointestinal (GI) tract
No detailed explanation provided for this question.
QUESTION 42 OF 50
Figures 12a and 12b show the radiographs of a 56-year-old man with diabetes mellitus who has had left foot swelling with no pain for the past several weeks. He denies any history of trauma. Examination reveals warmth, moderate swelling, no tenderness, and mild pes planus with standing. Pulses are palpable, and his sensory examination is grossly intact to light touch. Standing radiographs are shown in Figures 12c and 12d. What is the most likely diagnosis?
1
Acute traumatic Lisfranc fracture-dislocation
2
Acquired pes planus due to rupture of the posterior tibial tendon
3
Neuropathic arthropathy
4
Osteomyelitis
5
Metatarsal stress fracture
The radiographs show tarsometatarsal joint subluxation without fragmentation. The clinical history and delay in presentation with the radiographic findings suggest a neuropathic or Charcot arthropathy involving the midfoot area. Intact sensory examination to light touch is not diagnostic for an intact peripheral neurologic system; monofilament testing is a more accurate office baseline examination for the presence of sensory peripheral neuropathy. With an acute traumatic Lisfranc fracture-dislocation, a history of a traumatic event is necessary, and radiographic abnormalities are expected, although nonstanding radiographs still may be misleading. Acquired pes planus due to posterior tibial tendon rupture may have negative nonstanding radiographs. Standing radiographs may reveal pes planus. However, intermetatarsal disruption is not expected as seen in a Lisfranc abnormality. Localized osteomyelitis of the foot without a penetrating injury or cutaneous ulceration is extremely unlikely and does not fit with the clinical picture described. An isolated metatarsal stress fracture would show osseous irregularity without the instability pattern pictured.
REFERENCES: Brodsky JW: The diabetic foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 895-969.
Myerson MS: Diabetic neuroarthropathy, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 439-465.
REFERENCES: Brodsky JW: The diabetic foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 895-969.
Myerson MS: Diabetic neuroarthropathy, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 439-465.
QUESTION 43 OF 50
A posterior spine fusion with segmental hook fixation from T4-L4 is performed for idiopathic scoliosis in a 15-year-old girl. Somatosensory evoked potential monitoring is normal throughout the procedure. The patient awakens and is unable to move either lower extremity, but she does have some sensation in the lower extremities. Recommended treatment includes:
1
Removal of instrumentation
2
Myelogram
3
Laminectomy above the conus medullaris
4
Administration of corticosteroids and observation for 6 hours
5
Full heparinization of the patient
Spinal cord injury occurs in approximately 1% of patients operated upon for idiopathic scoliosis. In some cases, sensory spinal cord monitoring may be unchanged, especially if the injury preserves the dorsal columns. The instrumentation should be removed as soon as possible in case spinal traction or derotation or implant protrusion is producing effects on the cord or its blood supply.
C orticosteroids should be administered at spinal cord injury doses, but this should not be the only measure. Obtaining a myelogram may delay the removal of instrumentation and should not be the first step. Heparinization has no proven effect.
C orticosteroids should be administered at spinal cord injury doses, but this should not be the only measure. Obtaining a myelogram may delay the removal of instrumentation and should not be the first step. Heparinization has no proven effect.
QUESTION 44 OF 50
Slide 1
A patient had a fixed deformity of the hallux interphalangeal (IP) joint (Slide) for 3 years following forefoot surgery. She complains of pain over the distal aspect of the hallux where rubbing occurs on the shoe. On examination, the hallux is flexible at the metatarsophalangeal (MP) and IP joints, there is no crepitus of the MP joint, and radiographs demonstrate normal alignment of the first metatarsal. The recommended procedure for correcting this deformity is:
A patient had a fixed deformity of the hallux interphalangeal (IP) joint (Slide) for 3 years following forefoot surgery. She complains of pain over the distal aspect of the hallux where rubbing occurs on the shoe. On examination, the hallux is flexible at the metatarsophalangeal (MP) and IP joints, there is no crepitus of the MP joint, and radiographs demonstrate normal alignment of the first metatarsal. The recommended procedure for correcting this deformity is:
1
Arthrodesis of the hallux MP joint
2
Resection arthroplasty of the hallux MP joint
3
Transfer of the extensor hallucis brevis tendon
4
Arthrodesis of the hallux IP joint with transfer of the flexor hallucis longus tendon
5
Lengthening of the abductor hallucis and repair of the lateral capsule and the flexor hallucis brevis tendon with a bone suture anchor
Arthrodesis and resection arthroplasty of the hallux MP joint are indicated in the presence of arthritis of the hallux MP joint. A tendon transfer is preferred, and the extensor hallucis brevis tendon is an effective transfer. Use of the extensor hallucis longus tendon with arthrodesis of the hallux IP joint is indicated when there is a fixed deformity of the hallux IP joint.
QUESTION 45 OF 50
Figures 1 through 5 show the radiographs, MRI, and MR arthrogram obtained from a 25-year-old
collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain
with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy. Approximately what percentage of asymptomatic
athletes have cam deformities of the hip?
collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain
with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy. Approximately what percentage of asymptomatic
athletes have cam deformities of the hip?
1
5%
2
10%
3
25%
4
At least 50%
Multiple studies have confirmed that cam or pincer anatomy is commonly present in asymptomatic hips. According to a large systematic review, cam deformities are present in approximately one-third of asymptomatic hips in young adults, and the proportion is higher than 50% in the subgroup of athletes. Ganz and associates proposed that femoral acetabular impingement is the root cause of osteoarthritis in most nontraumatic, nondysplastic hips, and functional improvement with surgical correction of the deformity has been demonstrated. Despite the link between cam deformity and hip osteoarthritis, a corresponding link between the correction of the deformity and prevention of osteoarthritis has never been proven. The results of cam deformity correction, typically including repair of the degenerative labral tear, are much poorer when substantial joint space loss is present. A typical joint space cutoff of 2 mm or less is used to recommend against hip preservation surgery.
QUESTION 46 OF 50
The most common complication following triple arthrodesis in the adult patient is:
1
Malunion of the arthrodesis
2
Nonunion of the arthrodesis
3
Ankle instability
4
Ankle arthritis
5
Transverse tarsal arthritis
Each of the possible answers may occur following triple arthrodesis. In numerous studies, ankle arthritis is the complication most likely to occur regardless of the underlying disease process.
QUESTION 47 OF 50
A 20-year-old woman is involved in a high-speed motor vehicle collision and sustains bilateral tibial plateau fractures as well as the clavicle fracture shown in Figure A. What is the most appropriate management of the clavicular injury?

1
Closed reduction and figure of 8 splinting
2
Open reduction and plate fixation
3
Open reduction and percutaneous pinning
4
Simple sling to involved side
5
Sling with abduction pillow to involved side
The radiograph shows a comminuted clavicle fracture with significant displacement. Indications for surgical fixation of clavicle fractures include: open fractures, underlying neurovascular injury, or impending open fracture from internal bony pressure causing skin compromise. Relative indications for fixation include: greater than 15 mm of shortening, greater than 100% displacement (no bony contact), highly comminuted fractures, and polytrauma patients.
Jeray et al review the evaluation and treatment of midshaft clavicle fractures. They state "when midshaft clavicular fractures are completely displaced or comminuted, and when they occur in elderly patients or females, the risk of nonunion, cosmetic deformity, and poor outcome may be markedly higher.
Thus, some surgeons propose surgical stabilization of a complex midshaft
clavicular fracture with either plate-and-screw fixation or intramedullary devices. Further randomized, prospective trials are needed to provide better data on which to base treatment decisions."
Jeray et al review the evaluation and treatment of midshaft clavicle fractures. They state "when midshaft clavicular fractures are completely displaced or comminuted, and when they occur in elderly patients or females, the risk of nonunion, cosmetic deformity, and poor outcome may be markedly higher.
Thus, some surgeons propose surgical stabilization of a complex midshaft
clavicular fracture with either plate-and-screw fixation or intramedullary devices. Further randomized, prospective trials are needed to provide better data on which to base treatment decisions."
QUESTION 48 OF 50
A 30-year-old farmer undergoes replantation of an above-the-elbow amputation. What form of management is most important following this surgery?
1
High volume diuresis with alkalinization of the urine
2
Systemic heparinization of the patient for 72 hours
3
Elevation of the extremity, with maintanence of the patient’s room temperature at 80 degrees F (26.6 degrees C)
4
Satellite ganglion continuous sympathetic block
5
Daily IV administration of low-molecular-weight dextran
After major limb replantation, the occurrence of ischemic rhabdomyonecrosis can result in lactic acidosis and myoglobulinemia. These complications can be limited by rapid repair of the arterial supply, potentially using a shunt before skeletal stability. Repair of the venous system should be performed after repair of the artery. High volume fluid replacement will maintain a diuresis, thus limiting the complications from myoglobulinemia.
REFERENCES: Wood MB: Replantations about the elbow, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1985, pp 472-480.
Goldner RD, Nunley JA: Replantation proximal to the wrist, in Wood MD (ed) Hand Clinics: Microsurgery. Philadelphia, PA, WB Saunders, 1992, pp 413-425.
REFERENCES: Wood MB: Replantations about the elbow, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1985, pp 472-480.
Goldner RD, Nunley JA: Replantation proximal to the wrist, in Wood MD (ed) Hand Clinics: Microsurgery. Philadelphia, PA, WB Saunders, 1992, pp 413-425.
QUESTION 49 OF 50
A 55-year-old woman with a 15-year history of systemic lupus erythematosus has had left shoulder pain for the past 3 months. She reports that the pain has grown progressively worse over the past few months, and her shoulder function is severely limited. She is presently being treated with azathioprine and has used corticosteroids in the past. AP and axillary radiographs are shown in Figures 19a and 19b, and MRI scans are shown in Figures 19c and 19d. Which of the following forms of management will yield the most predictable pain relief and return of shoulder function?
1
Stretching exercises with a physical therapist
2
Arthroscopic debridement
3
Core decompression of the humeral head
4
Humeral hemiarthroplasty
5
Resection of the proximal humerus
Prosthetic shoulder arthroplasty has been shown to provide predictable results for treating stage III and stage IV osteonecrosis of the humeral head. The decision to resurface the glenoid (total shoulder arthroplasty versus humeral hemiarthroplasty) usually is made based on the radiographic and intraoperative appearance of the glenoid. Core decompression of the humeral head has been reported to be effective for earlier stages (pre collapse) but would not be appropriate for a patient with stage IV disease.
REFERENCES: Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Results of replacement. J Shoulder Elbow Surg 2000;9:177-182.
L’Insalata JC, Pagnani MJ, Warren RF, et al: Humeral head osteonecrosis: Clinical course and radiographic predictors of outcome. J Shoulder Elbow Surg 1996;5:355-361.
Cruess RL: Steroid-induced avascular necrosis of the head of the humerus: Natural history and management. J Bone Joint Surg Br 1976;58:313-317.
REFERENCES: Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Results of replacement. J Shoulder Elbow Surg 2000;9:177-182.
L’Insalata JC, Pagnani MJ, Warren RF, et al: Humeral head osteonecrosis: Clinical course and radiographic predictors of outcome. J Shoulder Elbow Surg 1996;5:355-361.
Cruess RL: Steroid-induced avascular necrosis of the head of the humerus: Natural history and management. J Bone Joint Surg Br 1976;58:313-317.
QUESTION 50 OF 50
Which of the following cells has receptors for parathyroid hormone:
1
Osteocytes
2
Osteoclasts
3
Plasma cells
4
Osteoblasts
5
Osteoclast precursor cells
Osteoblasts have receptors for parathyroid hormone. Once stimulated, the cells release interleukin-6 (IL-6). IL-6 signals osteoclasts to resorb bone. The osteoblasts secrete neutral proteases that degrade the osteoid surface. Osteoclasts then attach to the bone surface and secrete acid proteases that degrade the bone matrix. Parathyroid hormone related protein increases osteoblast expression of receptor activator of nuclear factor âkB ligand (RANKL). RANKL binds to osteoclast precursor cells for the formation of active osteoclasts
