This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set 20F57B)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
Slide 1
Which of the following antibiotics has the highest concentration locally from Palacos-R (Biomet, Warsaw, IN) cement:
1
Tobramycin
2
Lincomycin
3
Bacitracin
4
Gentamicin
5
Keflex
The Slide represents different antibiotics that may be used with bone cement and the release of antibiotics over a 10-day period. Gentamicin leads the way with a high concentration locally. Bacitracin, for instance, does not leach in high concentrations from Palacos-R bone cement
QUESTION 2 OF 50
Slide 1
A 56-year-old patient sustained an ankle fracture 3 years ago that was treated with closed reduction and cast immobilization. Since the injury, she has experienced pain upon ambulation and ankle stiffness. On examination, the range of motion of the ankle is 5° of dorsiflexion and 30° of plantarflexion. C repitus with motion is not present, but the patient does experience severe pain. A radiograph is presented (Slide). The recommended procedure to alleviate the patientâs pain and improve function is:
1
Total ankle replacement
2
Ankle arthrodesis
3
Ankle arthroscopy and joint debridement
4
Osteotomy of the fibula
5
Anterior ankle cheilectomy, Achilles lengthening, and joint debridement
The arthritis in this joint is not severe, but there is joint malalignment associated with a short and externally rotated fibula. Joint malalignment is correctable with a lengthening and rotational (internal) osteotomy of the fibula with bone graft. Joint debridement, either open or arthroscopic, is not effective in the management of posttraumatic ankle arthritis. Arthrodesis and arthroplasty are not necessary at this stage.
QUESTION 3 OF 50
The virus associated with the most immune reactions is:
1
Adeno-associated virus
2
Gutted adenovirus
3
Adenovirus
4
Retrovirus
5
Herpes simplex virus
Adenoviral vectors can cause inflammatory reaction due to immune activation, an event linked to the first death related to gene therapy. This occurred in September 1999 at the University of Pennsylvania in a clinical trial in which an 18-year-old patient received infusion of more than a trillion adenoviral vectors directed to his liver, which triggered a systemiCinflammatory response that became uncontrollable, leading to organ failure and death. Newer-generation gutted or gutless adenovirus vectors are nonimmunogenic
QUESTION 4 OF 50
Figures below show the radiographs, MRI, and MR arthrogram obtained from a 25-year-old collegiate
soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy. What is the primary cause of a cam deformity?
1
A genetic problem
2
Repetitive activities involving an open proximal femoral physis
3
Early closure of the proximal femoral physis
4
Hip dysplasia
Multiple studies have confirmed that cam or pincer anatomy is commonly present in asymptomatic hips. According to a large systematic review, cam deformities are present in approximately one-third of asymptomatic hips in young adults, and the proportion is higher than 50% in the subgroup of athletes. Ganz and associates proposed that femoral acetabular impingement is the root cause of osteoarthritis in most nontraumatic, nondysplastic hips, and functional improvement with surgical correction of the deformity has been demonstrated. Despite the link between cam deformity and hip osteoarthritis, a corresponding link between the correction of the deformity and prevention of osteoarthritis has never been proven. The results of cam deformity correction, typically including repair of the degenerative labral tear, are much poorer when substantial joint space loss is present. A typical joint space cutoff of 2 mm or less is used to recommend against hip preservation surgery.
QUESTION 5 OF 50
Figures 1 through 3 are the radiographs of a 55-year-old woman who fell on her outstretched right arm, resulting in acute elbow pain and swelling. On examination, she has lateral elbow bruising and tenderness, with a mechanical block to forearm supination and pronation. She has no medial tenderness. During surgery through a direct lateral approach, the surgeon observes a completely bare lateral epicondyle and surgical repair is performed, resulting in a stable and congruent joint. Initial postoperative rehabilitation should include
1
3 weeks of cast immobilization.
2
elbow extension exercises with the forearm supinated.
3
elbow extension exercises with the forearm pronated.
4
elbow extension exercises with the forearm in neutral rotation.
Radial head fractures are thought to occur as a result of valgus posterolateral rotary load across the elbow, although the mechanism can certainly vary. Minimally or nondisplaced fractures without any clinical instability or block to motion can often be successfully managed non-surgically. Fractures with >2 mm of displacement or fragments that block motion require surgical repair. A critical aspect during surgery is identifying concomitant injury to the lateral collateral ligament complex (LCL). When encountered, the LCL is most often avulsed from its origin at the lateral epicondyle, resulting in a bare area. After the radial head is either repaired or replaced (Figures 4 and 5), the LCL should
16
be repaired back to its anatomic origin. Postoperatively, the surgeon must communicate to the therapist that elbow extension exercises should be performed with the forearm in pronation as a result of the compromised LCL, as this position places the least stress on the ligamentous repair. Elbow extension exercises in supination or neutral are recommended for compromise of the medial collateral ligament, or combined medial and lateral ligament injury, respectively. Without any medial elbow bruising, swelling, or tenderness, it is unlikely that the patient has an injury to the medial collateral ligament.
QUESTION 6 OF 50
Which of the following is associated with Marfan's syndrome:
1
Sulfate transporter gene
2
Fibroblast growth factor 3 (FGF-3) (receptor)
3
C arbonic anhydrase type II, proton pump
4
C ore binding factor alpha 1 (C bfa1)
5
Fibrillin
The defective gene (located on chromosome 15) in Marfan's syndrome encodes for fibrillin. Fibrillin is a structural component of elastin and contains microfibrils (Dietz).
Features of Marfan's syndrome include: Long, thin limbs (dolichostenomelia)
Pectus excavatum, carinatum
Scoliosis
High and narrow palate
Ectopia lentis
Dilation of the ascending aorta
Dural ectasia
The other responses refer to:
Achondroplasia: FGF-3 receptor
Diastrophic dysplasia: Sulfate transporter gene
C leidocranial dysplasia: C bfa1
Osteopetrosis: C arbonic anhydrase type II, proton pump
QUESTION 7 OF 50
of 100
What kinematic relationship occurs between the anteromedial and posterolateral bundles of the injured structure identified in these images?
1
Both are tight in extension and in flexion.
2
Both are tight in extension and loose in flexion.
3
The anteromedial bundles are tight in extension and loose in flexion, and the posterolateral bundle is tight in both flexion and extension.
4
The posterolateral bundle is tight in extension and loose in flexion, and the anteromedial bundle is tight in both flexion and extension.
- The posterolateral bundle is tight in extension and loose in flexion, and the anteromedial bundle is tight in both flexion and extension.
QUESTION 8 OF 50
A 68-year-old man embarks on a 24-week strength training program. He trains at 80% of his single repetition maximum for both the upper and lower extremities. Which of the following changes can be anticipated?**
1
An absolute decrease in aerobic capacity
2
A decrease in capillary density in the trained muscles
3
A significant increase in strength
4
A significant improvement in Vo2max
5
No change in the cross-sectional area of the trained muscles
Consistent, long-term exercise training in older athletes has proven very beneficial in reversing both endurance and strength losses that traditionally have been seen with aging. This patient’s program will lead to a significant increase in the strength, cross-sectional area, and capillary density of the trained muscles. No major changes in aerobic capacity are anticipated. Strength improvements of up to 5% per day, similar to those for younger athletes, have been identified in this population in one study.
REFERENCES: Kirkendall DT, Garrett WE Jr: The effects of aging and training on skeletal muscle. Am J Sports Med 1998;26:598-602.
Frontera WR, Meredith CN, O’Reilly KP, Knuttgen HG, Evans WJ: Strength conditioning in older men: Skeletal muscle hypertrophy and improved function. J Appl Physiol 1988;64:1038-1044.
QUESTION 9 OF 50
C ongenital pseudarthrosis of the clavicle occurs most commonly on which side:
1
Bilateral
2
Right
3
Left
4
The side more involved with fibrous dysplasia
5
The side with the proximal focal femoral dysplasia
Ninety percent of cases are noted on the right side. Ten percent of cases are bilateral and have been associated with bilateral cervical ribs. Only a few cases of left-sided pseudarthrosis have been described and have been associated with dextrocardia.
Only
of 100
Despite adequate medical management, the patient continues to experience leg pain that interferes with even the lowest demands of daily living. You recommend prophylactic intramedullary nailing of the tibia with interlocking screws. Prior to the surgery, you should recommend
1
an echocardiogram.
2
an endocrinology consultation.
3
a serum calcium level.
4
a repeat nuclear bone scan.
- an endocrinology consultation._
QUESTION 12 OF 50
of 100
This pathology most likely causes mechanical low-back pain.
1
Figure 72a Figure 72b
2
Figure 72c Figure 72d
3
Figure 72e Figure 72f
4
Figure 72g Figure 72h 67
- Figure 72e Figure 72f
QUESTION 13 OF 50
of 100
Figures 82a and 82b are the clinical photographs of a 16-year-old boy who has a 2-day history of pain, swelling, nausea, and erythema in his entire left upper extremity. His temperature is 38.8°C and his white blood cell count is 25,000/µL (reference range, 4,500-11,000µl). What is the most appropriate course of treatment?
1
Oral antibiotics
2
Intravenous (IV) antibiotics
3
MR imaging
4
Immediate surgery
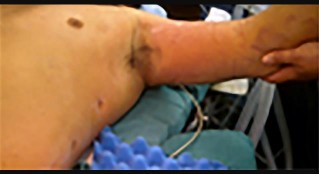

This patient has all the signs of necrotizing fasciitis. Advancing erythema, fever, pain, and elevated white blood cell counts are all indications of a serious soft-tissue infection that necessitates immediate surgical debridement. IV antibiotics alone will not resolve this infection.
Although necrotizing soft-tissue infections are uncommon and often are seen in patients who are immunocompromised, they also can occur in healthy individuals and may be associated with only minor trauma. Swelling, erythema, pain, fever, and blistering are classic symptoms. Laboratory and radiograph studies including MR imaging should help confirm the diagnosis but should not delay surgery.
Wide surgical excision of the fascia subcutaneous tissue and skin, if needed, should be performed (Figures 82c and 82d). Debridement should extend to normal tissue. Wound debridement and inspection should be done on a daily basis. Associated mortality is high and survival is dependent upon early diagnosis and surgical debridement.
RECOMMENDED READINGS
68. Stevens DL. The flesh-eating bacterium: what's next? J Infect Dis. 1999 Mar;179 Suppl 2:S366-74. Review. PubMed PMID: 10081509.
69. Sudarsky LA, Laschinger JC, Coppa GF, Spencer FC. Improved results from a standardized approach in treating patients with necrotizing fasciitis. Ann Surg. 1987 Nov;206(5):661-5. PubMed PMID: 3314752.
70. Ogilvie CM, Miclau T. Necrotizing soft tissue infections of the extremities and back. Clin Orthop Relat Res. 2006 Jun;447:179-86. PubMed PMID: 16672902.
71. Chauhan A, Wigton MD, Palmer BA. Necrotizing fasciitis. J Hand Surg Am. 2014 Aug;39(8):1598-601; quiz 1602. doi: 10.1016/j.jhsa.2014.04.010. Epub 2014 May 23. Review. PubMed PMID:
QUESTION 14 OF 50
Figures 33a and 33b show the standing posteroanterior and lateral radiographs of a 59-year-old woman with adult idiopathic scoliosis. She underwent a prior decompressive laminectomy and fusion at L4-S1 to address lumbar stenosis. She now reports progressive lower back pain and a feeling of being shifted to the right. If surgical intervention is considered, what is the most important goal in improving her healthrelated quality of life (HRQL) outcomes?
1
Correction of the thoracolumbar curve
2
Sagittal balance
3
Coronal balance
4
Correction of the thoracic curve
5
Shoulder balance
Sagittal balance is the most reliable predictor of clinical symptoms and HRQL outcomes on the SRS 29, SF-12, and Oswestry Disability Index. Coronal balance, shoulder balance,curve magnitude, and degree of curve correction are less critical in determining clinical symptoms and outcomes.
QUESTION 15 OF 50
What finding would most likely be present on an AP radiograph of a nondislocated elbow with an anteromedial coronoid fracture?
1
A “fleck” sign
2
The AP radiograph would appear normal
3
Equal joint spaces between the medial trochlea and the coronoid
4
Progressive narrowing of the joint space from lateral to medial between the medial trochlea and the coronoid
5
Progressive narrowing of the joint space from medial to lateral between the medial trochlea and the coronoid
No detailed explanation provided for this question.
QUESTION 16 OF 50
If a metacarpal shaft fracture shortens 4 mm, what will the theoretical amount of extensor lag be at the metacarpophalangeal joint:
1
0°
2
5°
3
7°
4
14°
5
20°
For each 2 mm of shortening, a 7° extensor lag exists. Thus, with 4 mm of shortening, there will be a 14° extensor lag at the metacarpophalangeal joint.
QUESTION 17 OF 50
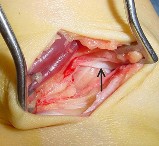
A 29-year-old woman has had a 6-month history of chronic left anterolateral ankle pain after sustaining an inversion ankle sprain while playing soccer. Management consisting of rest, nonsteroidal anti-inflammatory drugs, immobilization, a cortisone injection, and 2 months of physical therapy has failed to allow her to return to her previous level of activities. Examination reveals good strength, motion, and ligamentous stability, with anterolateral ankle tenderness. Radiographs are normal. During an anterolateral approach to the left ankle, the structure labeled with the arrow in Figure 56a is noted to be impinging on the anterolateral dome of the talus and is removed as shown in Figure 56b. Removal of this structure will most likely result in which of the following? ](http://www.orthobullets.com/anatomy/10122/blank)Review Topic
1
Alleviation of her symptoms
2
Destabilization of the syndesmosis
3
Increase the anterior drawer but not influence the talar tilt
4
Increase the talar tilt but not influence the anterior drawer
5
Have no effect on her symptoms or her ankle instability
No detailed explanation provided for this question.
QUESTION 18 OF 50
A 36-year-old woman dislocated her elbow 6 months ago. The elbow was congruently reduced and rehabilitated. She continues to have a sense of painful clunking in her elbow when she pushes up from a chair with forearm supination, but not pronation. What structure did not heal properly?
1
Posterior band of the medial collateral ligament
2
Anterior band of the medial collateral ligament
3
Radial collateral ligament
4
Lateral ulnar collateral ligament
The patient is showing signs of posterolateral rotatory instability after elbow dislocation. The lateral ulnar collateral ligament is responsible for stabilizing the elbow against this type of instability. The posterior and anterior bands of the medial collateral ligament are primarily resistors of valgus load, with the anterior band being the most significant contributor. The radial collateral ligament does not control the posterolateral rotatory instability described.
QUESTION 19 OF 50
An 8-month-old child is seen in the emergency department with seizures and a fractured femur. The mother states that the child fe**l** off the bed at the babysitter’s house. There are bilateral bruises on the anterior and posterior chest walls. Retinal hemorrhages are present. The temperature is 98.9 degrees F (37.2 degrees C). What is the most likely diagnosis?
1
Febrile seizure
2
Fractured skull
3
Subdural hematoma
4
Shaken baby syndrome
5
Contracoup brain injury
DISCUSSION: Shaken baby syndrome is associated with chest ecchymosis and head trauma. Retinal
hemorrhages are often found, but are not pathognomonic. Contracoup injury was originally implicated, but more recent evidence shows that the head is actually struck against a hard object that causes a subdural hematoma.
REFERENCES: LeFanu J, Edwards-Brown R: Patterns of presentation of shaken baby syndrome: Subdural and retinal haemorrhages are not necessarily signs of abuse. BMJ 2004;328:767.
Richards PG, Bertocci GE, Bonshek RE, et al: Shaken baby syndrome. Arch Dis Child 2006;91:205-206.
QUESTION 20 OF 50
A 70-year-old man reports symptomatic medial knee pain that has become progressively worse during
the past year. MRI reveals a complex, posterior horn medial meniscus tear with associated medial lateral and patellofemoral cartilage defects. Radiographs reveal medial joint space narrowing and osteophytes in the other compartments. What treatment is most likely to provide long-term, durable relief of symptoms?
1
High tibial osteotomy
2
Total knee replacement
3
Unicondylar knee replacement
4
Arthroscopic partial meniscectomy
Total knee replacement is a well-established surgery for diffuse, symptomatic osteoarthritis of the knee joint, and its efficacy has been shown in many studies. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee, arthroscopy in the setting of existing osteoarthritis is efficacious for relieving the signs and symptoms of a torn meniscus but not for osteoarthritis. Likewise, in young and active patients, clinical outcomes show improvement after realignment osteotomy for single- compartment osteoarthritis. Unicondylar knee replacement is not indicated for tricompartmental disease
of the knee.
QUESTION 21 OF 50
..He started physical therapy while continuing light duty at work. Eight weeks later, his pain remained unchanged. An MRI scan is shown in Figure 5. What histologic changes are likely to be found in the supraspinatus
tendon?
1
Disorganized collagen fibers with mucoid degeneration
2
Disorganized collagen fibers and acute inflammatory
3
Normal tendon fibers infiltrated with capillary proliferation
4
Normal tendon fibers infiltrated with acute inflammatory cells
DISCUSSION..This patient has impingement syndrome based on the history and examination. The best way to confirm the diagnosis is by performing a subacromial injection with lidocaine, which is also called a Neer impingement test. If the
pain is relieved, the patient’s pain is coming from the subacromial space. An MRI scan would not confirm the diagnosis of impingement, although it can aid in diagnosis of other causes of anterior shoulder pain such as a rotator cuff tear. This patient has normal rotator cuff strength, so that diagnosis is less likely. A radiograph can show acromial morphology, which would support the diagnosis of impingement, but it does not rule out impingement if the radiograph findings are normal. Ultrasound would not support the diagnosis of impingement, but, like an MRI scan, it can reveal pathologies other than impingement. The MRI scan shows a supraspinatus tendon with changes consistent with tendinopathy, which is defined by disorganized collagen fibers with mucoid degeneration on the microscopic level. Although there are always exceptions, most tendinopathy occurs without inflammatory cells or capillary proliferation.
- Subacromial injection with lidocaine
PREFERRED RESPONSE: 1- Disorganized collagen fibers with mucoid degeneration
CLINICAL SITUATION FOR QUESTIONS 7 THROUGH 9
A 26-year-old man has the chief complaint of right shoulder instability. He underwent an uncomplicated arthroscopic Bankart repair following an injury sustained while playing high school football. His condition was stable for 7 years, but he redislocated his shoulder in a fall 6 months ago. He describes weekly anterior instability events that he can reduce on his own. Radiographs reveal a located glenohumeral joint, but a Hill-Sachs lesion is noted. A CT scan reveals a 20% anteroinferior glenoid deficiency and a Hill-Sachs lesion involving 20% of the humeral head.
QUESTION 22 OF 50
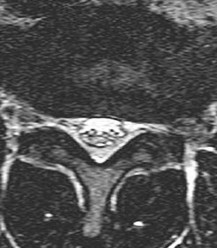
of 100 Figure 5 is a T2-weighted MR image of a 26-year-old man who has had left leg pain for 3 months that has failed nonsurgical treatment. Surgical decompression is planned. Which approach would provide the most direct ability to perform surgical decompression?
1
Posterior midline approach
2
Retroperitoneal approach
3
Far lateral approach
4
Transpsoas approach
The MR image shows a far lateral disk herniation impinging on the exiting nerve root lateral to the exiting foramen. This is reached most directly with a far lateral (Wiltse) approach. This is a posterior paramedian approach that uses the interval between the paraspinal muscles (multifidus and longissimus) and arrives onto the facet joints. The intertransverse membrane can then be released, exposing the far lateral disk herniation. A posterior midline approach will allow easy access to the spinal canal, which is medial to the disk herniation, and will not allow for easy disk removal without the need for a facetectomy, which would destabilize the level. An anterior approach would not allow for access to the far lateral disk herniation, nor would a traditional retroperitoneal or newer transpsoas approach.
RECOMMENDED READINGS
[Wiltse LL, Spencer CW. New uses and refinements of the paraspinal approach to the lumbar spine. Spine (Phila Pa 1976). 1988 Jun;13(6):696-706. PubMed PMID: 3175760. ](http://www.ncbi.nlm.nih.gov/pubmed/3175760)[View](http://www.ncbi.nlm.nih.gov/pubmed/3175760)[ ](http://www.ncbi.nlm.nih.gov/pubmed/3175760)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3175760)
[Epstein NE. Evaluation of varied surgical approaches used in the management of 170 far-lateral lumbar disc herniations: indications and results. J Neurosurg. 1995 Oct;83(4):648-56. PubMed PMID: 7674015. ](http://www.ncbi.nlm.nih.gov/pubmed/7674015)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7674015)
QUESTION 23 OF 50
of 100
In this age group, symptomatic SLAP lesions are best treated with
1
biceps tenodesis.
2
open labral repair.
3
arthroscopic labral repair.
4
repair with bioabsorbable tacks.
SLAP lesions are difficult to diagnose with MR imaging. Radiologic review generates a high number of false-positive reports. For this reason, initial nonsurgical evaluation with MR imaging that suggests a SLAP lesion is appropriate. Most authors contend that SLAP repair should be performed in no more than 3% of cases, even in a tertiary care shoulder practice. An examination, MRI scanning with or without contrast, and surgeon agreement on visual pathology at surgery are all highly variable. Many older patients will have increased signal in the labrum as a normal variant. Several studies suggest that SLAP lesions in older people may be better addressed with biceps tenodesis than labral repair.
RECOMMENDED READINGS
12. [Boileau P, Parratte S, Chuinard C, Roussanne Y, Shia D, Bicknell R. Arthroscopic treatment of isolated type II SLAP lesions: biceps tenodesis as an alternative to reinsertion. Am J Sports Med. 2009 May;37(5):929-36.Epub 2009 Feb 19. PubMed PMID: 19229046. ](http://www.ncbi.nlm.nih.gov/pubmed/19229046)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19229046)
13. [Burns JP, Bahk M, Snyder SJ. Superior labral tears: repair versus biceps tenodesis. J Shoulder Elbow Surg. 2011 Mar;20(2 Suppl):S2-8. doi: 10.1016/j.jse.2010.11.013. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/21281918)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/21281918)
14. Gobezie R, Zurakowski D, Lavery K, Millett PJ, Cole BJ, Warner JJ. Analysis of interobserver and intraobserver variability in the diagnosis and treatment of SLAP tears using the Snyder classification. Am J Sports Med. 2008 Jul;36(7):1373-9. doi: 10.1177/0363546508314795. Epub 2008 Mar 19.
[PubMed PMID: 18354142. ](http://www.ncbi.nlm.nih.gov/pubmed/18354142)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18354142)
15. [Katz LM, Hsu S, Miller SL, Richmond JC, Khetia E, Kohli N, Curtis AS. Poor outcomes after SLAP repair: descriptive analysis and prognosis. Arthroscopy. 2009 Aug;25(8):849-55. doi: 10.1016/j.arthro.2009.02.022. Erratum in: Arthroscopy. 2009 Nov;25(11):1361. Ketia, Eric [corrected to Khetia, Eric]. PubMed PMID: 19664504. ](http://www.ncbi.nlm.nih.gov/pubmed/19664504)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19664504)
16. [Sassmannshausen G, Sukay M, Mair SD. Broken or dislodged poly-L-lactic acid bioabsorbable tacks in patients after SLAP lesion surgery. Arthroscopy. 2006 Jun;22(6):615-9.](http://www.ncbi.nlm.nih.gov/pubmed/16762699)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16762699)
17. [Weber SC, Martin DF, Seiler JG 3rd, Harrast JJ. Superior labrum anterior and posterior lesions of the shoulder: incidence rates, complications, and outcomes as reported by American Board of Orthopedic Surgery. Part II candidates. Am J Sports Med. 2012 Jul;40(7):1538-43. doi: 10.1177/ 0363546512447785. Epub 2012 May 24. PubMed PMID: 22628153.](http://www.ncbi.nlm.nih.gov/pubmed/22628153)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/22628153)
QUESTION 24 OF 50
A 32-year-old woman has had pain and a visibly growing mass in the shoulder for 3 years but denies any history of trauma. Examination reveals a swollen, boggy shoulder mass. The AP radiograph and MRI scan are shown in Figures 20a and 20b. Figures 20c through 20e show a portion of the excised mass and the photomicrographs of the biopsy specimen. What is the most likely diagnosis?
1
Synovial chondromatosis
2
Pigmented villonodular synovitis
3
Synovial cell sarcoma
4
Tuberculosis
5
Chondrosarcoma
The radiographic findings are classic for synovial chondromatosis because of the small calcified opacities within the joint surrounding the synovium. The histologic findings show cartilaginous foci of metaplasia, which may be markedly cellular. However, unlike low-grade chondrosarcoma, it lacks cellular and nuclear pleomorphism.
REFERENCES: Murphy FP, Dahlin DC, Sullivan CR: Articular synovial chondromatosis. J Bone Joint Surg Am 1982;44:77-86.
Milgram JW: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801.
QUESTION 25 OF 50
-What mechanism is most likely responsible for the initiation of mechanical failure seen at the midstem modular junction of modular revision hip stems?
1
Fretting fatigue
2
Etching
3
Crevice corrosion
4
Abrasive wear
No detailed explanation provided for this question.
QUESTION 26 OF 50
Contraindications to high tibial osteotomy include:
1
Lateral compartment narrowing
2
Lateral tibial subluxation more than 1 cm
3
Medial compartment bone loss of more than 3 mm
4
Ligament instability
5
All of the above
Lateral compartment narrowing, lateral tibial subluxation of more than 1 cm, medial compartment bone loss of more than 3 mm, and ligament instability are contraindications to high tibial osteotomy
QUESTION 27 OF 50
of 100
Figures 24a and 24b are the right femur radiograph and bone scan of a 71-year-old man with longstanding metastatic prostate cancer who has experienced increasing right thigh pain for 2 months. The pain is worse with activity and is alleviated with rest. He experienced similar pain in his left thigh 18 months ago and subsequently sustained a left subtrochanteric femur fracture after a low-energy twisting injury. He was successfully treated with an intramedullary nail. He had been receiving zoledronic acid for 4 years prior to the fracture. This patient’s history includes heavy steroid use. His current symptoms are most likely the result of
1
a prostaglandin-secreting prostate metastasis.
2
inhibition of osteoclastic function.
3
right L4 radiculopathy secondary to prostate metastasis.
4
direct inhibition of osteoclast prenylation.
_
This patient’s history and imaging are most consistent with an atypical femoral fracture attributable to impaired bone remodeling. Both bisphosphonates and denosumab are associated with atypical
femur fractures. Atypical fractures may occur in the diaphysis and the subtrochanteric region. The patient’s prior femur fracture was attributable to bisphosphonate (zoledronic acid) use. Bisphosphonates directly inhibit osteoclasts. He subsequently experienced a long symptom-free interval during which he took denosumab, which is an indirect osteoclast inhibitor. The imaging is not consistent with a symptomatic prostate metastasis. L4 radiculopathy may cause thigh pain, but there is no evidence (other than the mention of spine metastasis) supporting this diagnosis.
RECOMMENDED READINGS
10. [Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster DW, Ebeling PR, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Lane JM, McKiernan F, McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Howe TS, van der Meulen MC, Weinstein RS, Whyte MP. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2014 Jan;29(1):1-23. doi: 10.1002/jbmr.1998. Epub 2013 Oct 1. Review. PubMed PMID: 23712442. ](http://www.ncbi.nlm.nih.gov/pubmed/23712442)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/23712442)
11. [Schilcher J, Koeppen V, Aspenberg P, Michaëlsson K. Risk of atypical femoral fracture during and after bisphosphonate use. N Engl J Med. 2014 Sep 4;371(10):974-6. doi: 10.1056/NEJMc1403799. PubMed PMID: 25184886.](http://www.ncbi.nlm.nih.gov/pubmed/25184886)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/25184886)
QUESTION 28 OF 50
Which of the flowing trajectories is preferred for placement of C1 lateral mass screws?
1
7.5 degrees lateral and 5 degrees cephalad
2
7.5 degrees medial and 10 degrees cephalad
3
10 degrees medial and 22 degrees cephalad
4
10 degrees lateral and 22 degrees cephalad
5
20 degrees medial and 22 degrees caudal
The C1 lateral mass can safely accommodate screw fixation. Trajectory of 10 degrees medial and 22 degrees cephalad was safely applied in a series of 50 patients.
Postoperative CT scans confirmed the safe trajectory. The benefit of lateral mass screws is that they can be safely placed despite the existence of an anomalous vertebral artery that could preclude the safe placement of transarticular screws.
QUESTION 29 OF 50
A 71-year-old man has worsening left hip pain and is indicated for a left total hip arthroplasty (THA). Figure 1 shows a preoperative plan for the patient. The patient is scheduled for a left THA using a direct anterior approach with the pictured implants. If this plan is followed as pictured, what is the likely outcome for this patient?
Figure could not be loaded
1
Successful THA with significant shortening of the operative limb
2
Compromised THA with a high likelihood of persistent trochanteric bursitis
3
Successful THA with significant lengthening of the operative limb
4
Compromised THA with a Trendelenburg gait and hip instability
The focus should be on the pictured plan. This shows a medialized cup and a stem that has insufficient offset (distance between the center of rotation and a line down the center of the femoral shaft) to recreate the patient’s anatomy. The cup sets the hip center of rotation (dot in the middle of the cup), and the femoral head reduces to this point. In this patient, inadequate offset could lead to a decrease in abductor efficiency and a Trendelenburg gait and even worse dislocation due to component impingement and/or muscular insufficiency. Compromised THA with a high likelihood of persistent trochanteric bursitis would be accurate if too much offset was restored for the patient. Regarding limb lengths, it appears the height of the implant is sufficient and as it stands would likely not change the leg lengths much at all. The concepts of limb length and offset restoration are critical to performing a successful THA and limiting adverse events and poor outcomes from an acquired limb length discrepancy, limb instability or persistent trochanteric bursitis.
QUESTION 30 OF 50
Which of the following terms is used to describe complete severance of a peripheral nerve with loss of the nerve trunk continuity:
1
First-degree injury (neuropraxia)
2
Second-degree (axonotmesis)
3
Third-degree
4
Fourth-degree
5
Fifth-degree
A fifth-degree injury refers to complete disruption of the nerve trunk.
First-degree: Neuropraxia, the nerve structure is intact, full recovery is expected
Second-degree: Axonotmesis, severance of the axon leading to Wallerian degeneration, continuity of endoneurial sheath is maintained, repair is orderly, complete motor and sensory loss with denervation and fibrillation potentials
Third-degree: Injury to axons and the endoneurial tube, arrangement of individual fascicles is maintained (perineurium intact), recovery is variable
Fourth-degree: Injury to axons, endoneurial tube, fascicles with the nerve trunk being intact, Wallerian degeneration and a higher incidence of proximal nerve cell body degeneration, repair is unlikely and surgical repair of the nerve is necessary (excision and grafting)
Fifth-degree: Loss of nerve trunk continuity, neuroma formation in the proximal stump, Wallerian degeneration distally
QUESTION 31 OF 50
An 18-year-old man sustained a traumatic laceration of the common peroneal nerve when glass fell on the outer part of his leg 1 year ago. He has used a molded foot and ankle orthosis for the past 10 months,but would now like surgical intervention. Electromyography shows no function in the anterior or lateral compartments. He has 5/5 muscle strength of the superficial and deep posterior compartments. What is the most appropriate treatment?
1
Gastrocsoleus recession
2
Subtalar fusion
3
Split anterior tibial tendon transfer
4
Split posterior tibial tendon transfer
5
Flexor hallucis longus tendon transfer
In a patient with a drop foot and with 5/5 muscle strength of the posterior tibial tendon, a split posterior tibial tendon transfer would be the most appropriate treatment option based on the options presented. The deep peroneal nerve innervates the anterior tibial tendon. This muscle has been affected by the injury; therefore, the anterior tibial tendon cannot be transferred. A subtalar fusion would help correct inversion and eversion deformities, but is not effective for plantar flexion deformities.
The foot drop is caused by a neurologic condition in this patient, not a contracture of the gastrocsoleus complex.Therefore, a recession would not be beneficial. A flexor hallucis longus tendon transfer would not take the deforming force and make it a corrective force.
QUESTION 32 OF 50
Following surgery for an ankle fracture, which of the following is considered the most important factor in achieving a satisfactory outcome?
1
Physical therapy
2
Early weight bearing
3
Anatomic alignment
4
Early range of motion of the ankle
5
Calcium and vitamin D administration
The only factor that is prognostic for outcomes is the quality of the reduction. None of the other factors has any effect on the outcome. Early range of motion or physical therapy may offer temporary effects, but these small advantages do not last beyond 3 months after surgery.
QUESTION 33 OF 50
The most important requirement for a diagnostic magnetic resonance image (MRI) study in cases of scaphoid-lunate ligament injury is:
1
2 mm thin slices
2
Tangential cuts
3
Gallium-enhanced scan
4
Dedicated wrist coil
5
MRI in neutral, radial, and ulnar deviation
MRI is not considered the technique of choice for the evaluation of the scaphoid-lunate ligament. Standard MRI coils are not adequate for the evaluation of the ligaments of the wrist. To maximize the yield from a wrist MRI, high-field strength and high- resolution images must be obtained using dedicated wrist coils. Only with such dedicated coils can detailed information be derived regarding the continuity of the scapoid-lunate ligament. Physical examination and wrist arthroscopy remain the gold standards for the evaluation of a torn scaphoid-lunate ligament.
QUESTION 34 OF 50
Arab Board Orthopedic MCQs Online Bank - Improve Your Knowledge and Skills
26/. A 14-year-old boy complains of pain along the medial aspect of the thigh, more severe at night. A bone scan reveals a double density sign with a maximum uptake in the center of a 1cm diameter lesion. The most likely diagnosis would be:
1
A. Sclerosing periostitis
2
B. Osteoblastoma
3
C. Osteoid osteoma
4
D. Stress fracture
5
E. Eosinophilic granuloma
No detailed explanation provided for this question.
QUESTION 35 OF 50
A 25-year-old woman undergoes surgical treatment of a displaced proximal humeral fracture via a deltopectoral approach. At the first postoperative visit, she reports a tingling numbness along the anterolateral aspect of the forearm. What structure is most likely injured?
1
Medial cord of the brachial plexus
2
Radial nerve
3
Median nerve
4
Axillary nerve
5
Musculocutaneous nerve
Sensation along the anterolateral aspect of the forearm is supplied by the lateral antebrachial cutaneous nerve, the terminal branch of the musculocutaneous nerve. The musculocutaneous nerve can be injured by proximal humeral fractures or dislocations, and is also at risk during surgical exposure if excessive retraction is placed on the conjoint tendon. The musculocutaneous nerve enters the conjoint tendon 1 cm to 5 cm distal to the coracoid process.
REFERENCES: McIlveen SJ, Duralde XA, D’Alessandro DF, et al: Isolated nerve injuries about the shoulder. Clin Orthop 1994;306:54-63.
Warner JP: Frozen shoulder: Diagnosis and management. J Am Acad Orthop Surg
1997;5:130-140.
QUESTION 36 OF 50
Which of the following noncollagenous proteins aid in regulating the maturation of bone mineral crystals:
1
Aggrecan
2
Vitronectin
3
Bone sialoprotein (bone sialoprotein 2)
4
Osteopontin (bone sialoprotein 1)
5
Osetocalcin (bone Gla protein)
Bone sialoproteins are important in the initiation of mineralization of collagen. They promote apatite nucleation and growth of the crystals. Osteocalcin (bone Gla protein) is important for mineral proliferation and maturation.
Note the role of promoters and inhibitors: Apatite nucleation and growth Promoters
Type I collagen Bone sialoprotein Matrix vesicles Phosphoproteins Proteolipids Biglycan
Inhibitors
Large proteoglycans Pyrophosphate Adenosine triphosphate Citrate
Mineral proliferation
Regulators
Osteocalcin Phosphoproteins Proteoglycans
QUESTION 37 OF 50
A non-communicative 16-year-old girl with spastic quadriplegic cerebral palsy and a 75-degree thoracolumbar scoliosis undergoes a successful posterior spinal fusion with instrumentation. What is the most predictable outcome of the surgical procedure?
1
Improved cognitive function
2
Improved caregiver satisfaction
3
Improved nutrition
4
Decreased pain
5
Improved mobility
DISCUSSION: Surgical treatment of spinal deformity in a totally involved child with cerebral palsy has been shown on outcomes instruments to significantly improve the caregiver’s perception of the child’s comfort. The other parameters mentioned are difficult to measure and unpredictable.
REFERENCES: Tsirikos Al, Lipton G, Chang WN, et al: Surgical correction of scoliosis in pediatric patients with cerebral palsy using the unit rod instrumentation. Spine 2008;33:1133-1140.
Cassidy C, Craig CL, Perry A, et al: A reassessment of spinal stabilization in severe cerebral palsy. J Pediatr Orthop 1994;14:731-739.
Figure 87
QUESTION 38 OF 50
Which of the following is the most appropriate clinical scenario to utilize locking plate and screw technology?
1
Intra-articular fracture
2
Oblique ulnar diaphyseal fracture
3
Osteoporotic periprosthetic distal femur fracture
4
Transverse tibial diaphyseal fracture
5
Spiral humeral diaphyseal-metaphyseal fracture
Conventional plating provides stable internal fixation when fractures are anatomically reduced. Stability of this type of fixation relies on the plate/bone interface and the friction that develops between this interface. Locked plates rely on the plate/screw interface, and each provides not only axial stability but also angular stability; each screw acts as a fixed angle device. Indications for locked plating for indirect reduction include: 1. metaphyseal/diaphyseal fractures 2. comminuted diaphyseal fractures 3. comminuted metaphyseal fractures. 4. short segment fixation. Locked plates are not indicated for displaced articular fractures unless anatomic rigid fixation of the articular surface is done first (locking technology cannot reduce fractures/lag segments together).
The referenced article by Gardner et al reviews locking technology and reminds us that compression technology using non-locking screws and plates is still needed for many fractures and is even required for proper treatment of some fractures.
The referenced article by Wagner is an instructional paper on how to use hybrid plating technology and reviews concepts such as the necessity of lag screw fixation before locking.
The referenced study by Egol et al is a review paper that notes that locked plates and conventional plates rely on completely different mechanical principles to provide fracture fixation and in so doing they provide different biological environments for healing. They report that locked plates are indicated for: indirect fracture reduction, diaphyseal/metaphyseal fractures in osteoporotic bone, and with bridging severely comminuted fractures.
QUESTION 39 OF 50
A 34-year-old man is involved in a motor vehicle accident and sustains an open tibia fracture and is treated with intramedullary nailing. For the next 4 years, he continues to have pain and persistent discharge from a sinus over his shin. He ambulates with crutches and refrains from putting weight on the extremity. The clinical appearance and radiographs are seen in Figures A and B. Wound culture reveals methicillin-resistant Staphylococcus aureus (MRSA). What is the next step in treatment?
1
Retention of tibial nail, lifelong intravenous antibiotic suppression
2
Debridement and lavage, exchange nailing using a larger diameter nail, intravenous antibiotics for 6 weeks.
3
Debridement and lavage, excision of sinus tract, implant removal, intravenous antibiotics for 6 weeks.
4
Debridement and lavage, addition of ring fixator, intravenous antibiotics for 6 weeks.
5
Debridement and lavage, excision of sinus tract, exchange nailing using antibiotic impregnated-cement nail, intravenous antibiotics for 6 weeks.
The patient has chronic osteomyelitis and an infected nonunion complicating previous IM nailing of an open tibia fracture. Successful treatment requires debridement, removal of the existing tibial nail, placement of an antibiotic-impregnated rod and IV antibiotics. Sinus tract excision and biopsy is important to exclude malignant transformation (Marjolin's ulcer).
Intramedullary infection is a recognized complication of IM nailing, especially in the setting of an open fracture. When the fracture fails to unite prior to deep infection treatment options include: nail removal and antibiotic exchange nailing, nail removal, intramedullary debridement and uniplanar external
fixation, or nail removal and resection of the infected segment with circular frame application and bone transport.
Paley et al. first described the treatment of intramedullary infection with antibiotic-impregnated cement nails in 6 femora, 2 tibiae and 1 humerus. There was no recurrence of infection. The antibiotic-impregnated cement nail fills the canal dead space while locally eluting high concentrations of antibiotics (for up to 36 wk), and is easy to remove.
QUESTION 40 OF 50
Which of the following has been associated with an increased likelihood of stress shielding after cementless total hip arthroplasty?
1
Use of titanium alloy femoral components
2
Use of proximally fixed femoral components
3
Use of distally fixed femoral components
4
Use of press-fit stems in patients with narrow intramedullary canals
5
Use of plasma sprayed components
DISCUSSION: Although stress shielding has not been associated with adverse clinical outcomes to date, it is a commonly observed process after cementless total hip arthroplasty. Factors that increase the magnitude of stress shielding include the use of distally fixed cobalt-chrome stems, particularly in patients with osteoporosis. Large diameter femoral components (larger than 18 mm in diameter) have also been associated with an increased prevalence of stress shielding.
REFERENCE: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 345-368.
QUESTION 41 OF 50
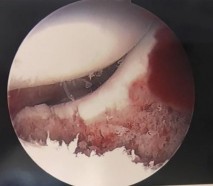
In the arthroscopic photograph shown in Figure 5, the structure labeled “A” functions primarily as a restraint to translation of the humeral head in what direction?
1
Inferiorly with the arm adducted to the side
2
Anteriorly with the arm abducted to 45 degrees and at neutral rotation
3
Anteriorly with the arm abducted to 45 degrees and maximally externally rotated
4
Anteriorly with the arm abducted to 90 degrees and at neutral rotation
5
Anteriorly with the arm abducted to 90 degrees and maximally externally rotated
The superior glenohumeral ligament identified as “A” in the figure functions primarily as a restraint to inferior glenohumeral translation of the adducted arm. The middle glenohumeral ligament is highly variable and pooly defined in up to 40% of the population and functions to restrain anterior translation of the externally rotated arm in the midrange of abduction. The anterior band of the inferior glenohumeral ligament is the primary restraint to anterior/inferior translation of the head with the shoulder abducted to 90 degrees and in maximum external rotation.
REFERENCES: Ticker JB, Bigliani LU, Soslowskiy LJ, et al: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
Owen MD, Kregel KC, Wall PT, Gisolfi CV: Effects of ingesting carbohydrate beverages during exercise in the heat. Med Sci Sports Exerc 1986;18:568-575.
QUESTION 42 OF 50
of 100
Advanced imaging, to include MRI and CT, have been obtained in the workup of patients with low back pain. What imaging finding has been associated with reasons for back pain?
1
Disk degeneration
2
Facet arthropathy
3
Spinal stenosis
4
Spondylolysis
■ Low back pain remains a common presenting condition to not only primary care physicians, but to subspecialists. Studies assessing the anatomy of the spine, to include the intervertebral disks, vertebral body morphology, facet joints, and the paraspinal muscles have been performed. Spinal stenosis is the only advanced imaging finding that has been associated with reproducible reasons for back pain.
QUESTION 43 OF 50
Figures 1 through 4 are the CT scans and intraoperative image of a 17-year-old boy who sustained a gunshot wound to his knee. What is the most appropriate definitive surgical management for his articular cartilage defect? --- --- --- ---
1
Microfracture
2
Autologous chondrocyte implantation
3
Osteochondral allograft transfer
4
Dejour trochleoplasty
The images show a full-thickness cartilage defect with significant bony involvement >4 cm2. Microfracture should be considered for lesions <2 cm2 without an underlying osseous defect. Autologous chondrocyte implantation, although used for lesions between 1 and 10 cm2, should be restricted for defects with minimal (<8 mm depth) bone loss. Osteochondral allograft transfer with the mosaicplasty technique (transfer of multiple plugs) would be well-suited for this large defect with significant osseous involvement. Dejour trochleoplasty is performed for patellar instability to correct trochlear dysplasia and _would not be indicated in this case._
QUESTION 44 OF 50
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?
1
Abundance of basic calcium phosphate crystals
2
Abundance of calcium pyrophosphate crystals
3
Gout
4
Rheumatoid arthritis
5
Osteonecrosis
Neer and associates focused on mechanical and nutritional factors as the etiology of rotator cuff arthropathy. McCarty and associates, in describing a similar syndrome known as Milwaukee shoulder, focused on an inflammatory cause in proposing the pathogenic role of hydroxyapatite, a basic calcium phosphate.
REFERENCES: Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
McCarty DJ, Halverson PB, Carrera GF, Brewer BJ, Kozin F: Milwaukee shoulder: Association of microspheroids containing hydroxyapatite crystals, active collagenase, and neutral protease with rotator cuff defects. I: Clinical aspects. Arthritis Rheum 1981;24:464-473.
QUESTION 45 OF 50
Which of the following methods reduce radiation exposure to a surgeon during fluoroscopic procedures:
1
Avoiding the inverted C -arm position
2
Avoiding collimation of the radiation beam
3
Limiting the use of the foot pedal for controlling the fluoroscopy unit
4
Always standing on the opposite side of the C -arm
5
Increasing the amperage of each exposure
One of the best ways to limit radiation exposure is to increase distance from the C -arm. Surgeons should always stand on the opposite side of the C -arm and remember the following methods for reducing radiation exposure:
Increase distance (doubling distance reduces exposure by a factor of 4) Inverted position of the C -arm (increases distance)
Shielding: 90% attenuated by 0.25-mm apron
C ollimation (reduces the size of the beam)
Foot pedal to control the fluoroscopy unit (decreases the amount of exposure)
QUESTION 46 OF 50
Figure 1 is the clinical photograph of a 42-year-old woman who has a lesion that has failed prior silver nitrate applications. She experiences frequent bleeding from this lesion. A tissue biopsy performed by a dermatologist revealed capillary hypertrophy with lobular arrangement. Which treatment is most appropriate to minimize recurrence?
1
Sclerotherapy
2
Shave excision with cautery
3
Cryotherapy
4
Wide surgical excision
This lesion is a pyogenic granuloma, which is a common benign vascular lesion that can occur on skin or mucosa. The etiology is unclear, although this lesion tends to occur in areas of physical trauma. Initial treatment with silver nitrate with an average of 1.6 applications has a success rate of 85%. This patient, however, has failed silver nitrate applications. Wide surgical excision (Figures below) is associated with the lowest recurrence rate and offers the benefit of a single procedure. Other options often necessitate repeated procedures to completely eradicate this lesion.
QUESTION 47 OF 50
A 32-year-old man underwent a total medial meniscectomy 2 years ago. He now reports pain and recurrent swelling for the past 3 months. Work-up includes full standing hip-knee-ankle radiographs, standing AP radiographs of both knees in full extension, an axial view of the patellofemoral joint, and a 45-degree flexion AP radiograph. Contraindication to meniscus allograft transplantation includes which of the following?
1
4 mm of tibiofemoral joint space on a 45-degree weight-bearing AP radiograph
2
Intact anterior cruciate ligament on MRI and physical examination
3
Recurrent effusions
4
Flattening of the femoral condyles
5
Healed high tibial osteotomy
DISCUSSION: Flattening of the femoral condyles indicates the onset of significant arthritis of the joint
and is a contraindication to meniscus allograft transplantation. Criteria to proceed with allograft transplantation includes prior total meniscectomy, age of 50 years or younger, BMI of less than 30, clinical symptoms of pain in the involved tibiofemoral compartment, 2 mm or more of tibiofemoral joint space on a 45-degree weight-bearing AP radiograph, ligamentous stability, normal alignment, and no radiographic evidence of advanced arthrosis. Recurrent effusions are associated with chronic meniscus deficiency, and is one criteria for meniscal transplantation. High tibial osteotomy is often considered in conjunction with meniscal transplantation to correct tibiofemoral malalignment.
REFERENCES: Noyes FR, Barber-Westin SD: Meniscus transplantation: Indications, techniques, clinical outcomes. Instr Course Lect 2005;54:341-353.
Kang RW, Lattermann C, Cole BJ: Allograft meniscus transplantation: Background, indications, techniques, and outcomes. J Knee Surg 2006;19:220-230.
QUESTION 48 OF 50
When comparing surgical and nonsurgical extremities in patients who underwent anterior cruciate ligament (ACL) reconstruction using patellar tendon or hamstrings autografts, isokinetic strength measurements obtained 6 months after the surgery would most
likely reveal **
1
significant quadricep weakness in the pateller tendon compared with the hamstring.
2
significant quadricep weakness in the hamstring compared with the pateller tendon.
3
significant weakness in the hamstring compared with the patellar tendon.
4
significant hamstring weakness in the pateller tendon compared with the hamstring.
5
no significant difference between the hamstring and the pateller tendon.
Follow-up examination at 6 months revealed no statistically significant differences in quadricep or hamstring strength when comparing surgical versus nonsurgical extremities isokinetically. Therefore, the selection of autogenous hamstring or patellar tendon for ACL reconstruction should not be based solely on the assumption of the graft tissue source altering the recovery of quadricep and/or hamstring strength.
REFERENCES: Carter TR, Edinger S: Isokinetic evaluation of anterior cruciate ligament reconstruction: Hamstring versus patellar tendon. Arthroscopy 1999;15:169-172
Howell SM, Taylor MA: Brace-free rehabilitation, with early return to activity, for knees reconstructed with a double-looped semitendinosus and gracilis graft. J Bone Joint Surg Am 1996;78:814-825.
Shelbourne KD, Nitz P: Accelerated rehabilitation after anterior cruciate ligament reconstruction. Am J Sports Med 1990;18:292-299.
QUESTION 49 OF 50
Slide 1 Slide 2 Slide 3
A 65-year-old man has severe foot pain. His plain radiograph is shown in Slide 1, and a needle biopsy specimen in Slides 2 and
3/. The most appropriate treatment for this patient is:
1
Irrigation/debridement followed by antibiotics
2
Chemotherapy followed by wide resection
3
Diphosphonate therapy
4
Nonsteriodal anti-inflammatory agents
5
ArthroscopiCdebridement
Gout is caused by the deposition of monosodium urate crystals in tissues, typically around joints. Common locations of gout include the great toe, heel, ankle, and knee. In approximately 50% of patients, the first affected location is the great toe. Gout commonly occurs inside a joint for two reasons - synovial fluid is a poorer solvent than plasma and lower temperatures (as in peripheral joints) favor crystallization.
Neutrophils ingest the crystals and release potent lysosomal enzymes. Punched lesions may be seen on radiographs in chroniCcases, and one can often see an overlying lip of cortex at the edge of the lesion.
Histologically, the tophi have several features: Acellular amorphous material
Macrophages
Foreign body giant cells
In this patient, the joint space is preserved on the plain radiographs. The biopsy specimen has the characteristiCfeatures of gout - acellular amorphous material, macrophages, and foreign body giant cells.
The treatment of gout includes nonsteroidal anti-inflammatory drugs and medications such as allopurinol and colchicines, which lower hyperuricemia.
QUESTION 50 OF 50
Slide 1 Slide 2
A 9-year-old boy has a history of multiple fractures. He presents with left leg pain following a minor fall. His anteroposterior
(Slide 1) and lateral (Slide 2) plain radiographs are shown. Which of the following can be an effective pharmacologiCtreatment:
1
Diphosphonate therapy
2
Vitamin D and calcium
3
CytotoxiCmulti-agent chemotherapy
4
SystemiCantibiotics
5
Growth hormone
The anteroposterior and lateral radiographs show thinned cortices and a gentle S-shaped curve of the tibia. The overall alignment of the tibia, as well as the physes, is normal. These are the radiographiCfeatures of osteogenesis imperfecta.
In osteogenesis imperfecta, the genetiCdefect involves type I collagen. Type I collagen is made up of two alpha-1 chains and one alpha-2 chain in a triple helix. Glycine is the smallest amino acid and is crucial for coiling of the triple helix. Mutations in the
glycine chain lead to severe forms of osteogenesis imperfecta. One should also remember the Silence classification:
Type Inheritance Sclera Severity
I AD Blue Mild form, normal teeth
II AR Blue Lethal form, die early
III AR Normal Severe, progressively deforming
IV AD Normal Moderately severe
Biphosphonate therapy can be used to slow bone remodeling and increase bone mass. Correct Answer: Diphosphonate therapy