Score: 0%
Advanced Orthopedic Mock Exam (Set 1F7639)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks.
Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
Aneurysmal bone cyst of the spine is most likely in this age group:
1
First decade
2
Second decade
3
Third decade
4
Fourth decade
5
Fifth decade
The most common age is the second decade; the mean age is 13 years old.
QUESTION 2 OF 50
Slide 1
A 23-year-old carpenter fell off a roof 4 weeks ago. He has pain in the ankle and a deformity. The lateral radiograph is presented (Slide). Which of the following treatments is most likely to return this patient to work with a functioning foot and ankle:
A 23-year-old carpenter fell off a roof 4 weeks ago. He has pain in the ankle and a deformity. The lateral radiograph is presented (Slide). Which of the following treatments is most likely to return this patient to work with a functioning foot and ankle:
1
Open reduction internal fixation of the calcaneus fracture
2
Short leg cast, no weight bearing for 8 weeks, followed by physical therapy
3
Immediate vigorous physical therapy emphasizing range of motion
4
Open reduction internal fixation of the calcaneus fracture with primary subtalar arthrodesis
5
Physical therapy, followed by subtalar arthrodesis at 6 months
The calcaneus fracture is associated with subluxation of the subtalar joint, giving the appearance of injury to the talus and calcaneus. The true extent of the injury cannot be determined without a computed tomography scan; however, the question is not as to the outcome of treatment, but the ability to return this patient to his occupation. At 4 weeks following injury, while open reduction internal fixation of the fracture is possible, anatomic reduction may be difficult. The most likely means of returning this patient to work is with early arthrodesis, which should be combined with an open reduction internal fixation of the calcaneus.
QUESTION 3 OF 50
A 6-year-old boy with spina bifida and L3 motor level presents to the clinic with bilateral swollen legs (below the knees). His legs have been swollen for the past 3 days and his knees are warm. The patient has an oral temperature of 38.1°C . He denies any pain. There is no history of systemic infection or of any other trauma. The problem may be most likely diagnosed by ordering:
1
A venogram of both lower extremities
2
A duplex ultrasound of both lower extremities and the pelvic veins
3
C ell count, gram stain, and culture of synovial fluid of both knees
4
Aspirate of both distal femoral metaphyses
5
Plain and stress varus-valgus radiographs of both knees
Low-energy fractures are the most likely cause of the patientâs bilateral swollen legs. The fractures may occur with everyday activities, and they do not cause pain because of the patientâs high neurologic level. If plain radiographs do not give the diagnosis, stress radiographs should be obtained to detect undisplaced physeal fractures.
Deep vein thrombosis is rare in this age group, especially bilaterally.
Spontaneous joint infection and spontaneous osteomyelitis are not any more likely in patients with spina bifida than in the general population.
Deep vein thrombosis is rare in this age group, especially bilaterally.
Spontaneous joint infection and spontaneous osteomyelitis are not any more likely in patients with spina bifida than in the general population.
QUESTION 4 OF 50
Equinovarus positioning of the foot is normal during which stage of embryonic life:
1
No stage
2
Eighth to tenth week
3
Thirteenth to fifteenth week
4
Seventeenth to nineteenth week
5
Twentieth to twenty-third week
As the foot matures, it passes through a normal stage when it resembles a clubfoot in the eighth to tenth week. After this, the foot normally corrects itself.
QUESTION 5 OF 50
Figures 11a and 11b show the AP and lateral radiographs of a 32-year-old patient on hemodialysis who has increasing elbow pain and a visibly growing mass over the extensor surface. Figure 11c shows the photomicrograph of the biopsy specimen. What is the most likely diagnosis?
1
Myositis ossificans
2
Tumoral calcinosis
3
Synovial cell sarcoma
4
Fungal granuloma
5
Hemochromatosis
The radiographic findings are classic for tumoral calcinosis; they are not consistent with myositis ossificans, fungal granuloma, or hemochromatosis. The condition typically appears as large aggregations of dense calcified lobules confined to the surrounding soft tissues. Hyperphosphatemia is a fundamental factor in many patients with this condition. Tumoral calcinosis also occurs in the setting of chronic renal failure when mineral homeostasis is not controlled. The histologic appearance is essentially a foreign body granuloma reaction. Multilocular cysts with purplish amorphous material are surrounded by thick connective tissue capsules. The fibrous walls contain numerous foreign body giant cells. Surgical excision is indicated if the tumor causes discomfort or interferes with function.
REFERENCES: Sisson HA, Murray RO, Kemp HBS (eds): Orthopaedic Diagnosis: Clinical, Radiological and Pathological Coordinates. New York, NY, Springer-Verlag, 1984.
Boskey AL, Vigorita VJ, Sencer O, Stuchin SA, Lane JM: Chemical, microscopic, and ultrastructural characterization of the mineral deposits in tumoral calcinosis. Clin Orthop 1983;178:258-269.
REFERENCES: Sisson HA, Murray RO, Kemp HBS (eds): Orthopaedic Diagnosis: Clinical, Radiological and Pathological Coordinates. New York, NY, Springer-Verlag, 1984.
Boskey AL, Vigorita VJ, Sencer O, Stuchin SA, Lane JM: Chemical, microscopic, and ultrastructural characterization of the mineral deposits in tumoral calcinosis. Clin Orthop 1983;178:258-269.
QUESTION 6 OF 50
What is the most common organism implicated in periprosthetic infection of the shoulder?
1
Methicillin-resistant Staphylococcus aureus (MRSA)
2
Cutibacterium acnes
3
Enterococcus species
4
Staphylococcus epidermidis
C acnes is the most common organism recovered in prosthetic shoulder infections (33%), Coagulase-negative Staphylococcus is second (21%), Methicillin-sensitive S aureus (13%), and S epidermidis (10%). MRSA accounts for 5% and Enterococcus species, 1.5%.
54
54
QUESTION 7 OF 50
An active 49-year-old woman who sustained a diaphyseal fracture of the clavicle 8 months ago now reports persistent shoulder pain with daily activities. An AP radiograph is shown in Figure 8. Management should consist of
1
external electrical stimulation.
2
external ultrasound stimulation.
3
implanted electrical stimulation.
4
closed reduction and percutaneous fixation.
5
open reduction and internal fixation with bone graft.
The radiograph reveals an atrophic nonunion of the diaphysis of the clavicle. Electrical or ultrasound stimulation may be an option in diaphyseal nonunions that have
shown some healing response with callus formation, but these techniques are not successful
in an atrophic nonunion. The preferred technique for achieving union is open reduction and internal fixation with bone graft. Percutaneous fixation has no role in treatment of nonunions
of the clavicle.
REFERENCES: Boyer MI, Axelrod TS: Atrophic nonunion of the clavicle: Treatment by compression plating, lag-screw fixation and bone graft. J Bone Joint Surg Br 1997;79:301-303.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
shown some healing response with callus formation, but these techniques are not successful
in an atrophic nonunion. The preferred technique for achieving union is open reduction and internal fixation with bone graft. Percutaneous fixation has no role in treatment of nonunions
of the clavicle.
REFERENCES: Boyer MI, Axelrod TS: Atrophic nonunion of the clavicle: Treatment by compression plating, lag-screw fixation and bone graft. J Bone Joint Surg Br 1997;79:301-303.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
QUESTION 8 OF 50
What are some potential benefits of performing arthroscopiCcompared to open acromioplasty in a patient who develops impingement syndrome following hemiarthroplasty:
1
Ability to evaluate the status of the glenoid
2
Capacity to address intra-articular pathology
3
More rapid postoperative recovery
4
Less violation of the deltoid
5
All of the above
ArthroscopiCacromioplasty has been used for the treatment of impingement following shoulder arthroplasty. It has the potential benefits of less tissue disruption, more rapid recovery, as well as increased ability to address intra-articular pathology compared to an open procedure.
QUESTION 9 OF 50
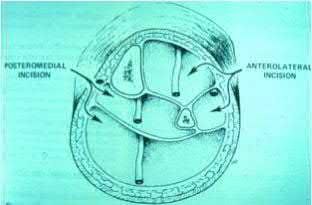
A 27-year-old man presents to the emergency department after a fall from a motorcycle. Imaging reveals a displaced glenoid neck fracture, and surgical intervention is planned through a modified Judet approach. What internervous plane is encountered between the infraspinatus and teres minor muscles?
1
Long thoracic nerve and axillary nerve
2
Suprascapular nerve and axillary nerve
3
Suprascapular nerve and long thoracic nerve
4
Spinal accessory nerve and axillary nerve
Surgical indications for scapular fractures are debatable in the literature. Historical indications for extra-articular fractures of the glenoid neck have ranged from 10-25 mm of medial displacement, 25-40⁰ of angular deformity of the glenoid, and a glenopolar angle cut-off of 20-30⁰. While the Judet approach can offer access to the entire scapular body, a modified Judet approach is a more limited approach that allows access to the glenoid neck in the interval
7
between the infraspinatus and teres minor. The infraspinatus is innervated by the suprascapular nerve, whereas the teres minor is innervated by the axillary nerve. The long thoracic nerve innervates the serratus anterior muscle. The spinal accessory nerve innervates the sternocleidomastoid and trapezius muscles.
7
between the infraspinatus and teres minor. The infraspinatus is innervated by the suprascapular nerve, whereas the teres minor is innervated by the axillary nerve. The long thoracic nerve innervates the serratus anterior muscle. The spinal accessory nerve innervates the sternocleidomastoid and trapezius muscles.
QUESTION 10 OF 50
of 100
In medical malpractice cases against spine surgeons, what factor is associated with a judgement for the plaintiff?
In medical malpractice cases against spine surgeons, what factor is associated with a judgement for the plaintiff?
1
Orthopaedic spine surgeon as the defendant
2
Neurosurgeon as the defendant
3
Male patient
4
Case of diagnostic delay
■
Medical litigation is common in spine surgery. In a study evaluating “spine surgery” related legal cases from 1988 to 2015, 234 cases met the inclusion criteria. Diagnostic delay cases were significantly associated with plaintiff verdict or settlement. Therapeutic delay cases were also associated with plaintiff verdict or settlement. Catastrophic complications resulted in larger payouts (6.1 million) as compared with noncatastrophic complications (2.9 million). There is no association between specialty (neurosurgery or orthopaedic spine surgery), patient age/sex, and case outcome or award.
Medical litigation is common in spine surgery. In a study evaluating “spine surgery” related legal cases from 1988 to 2015, 234 cases met the inclusion criteria. Diagnostic delay cases were significantly associated with plaintiff verdict or settlement. Therapeutic delay cases were also associated with plaintiff verdict or settlement. Catastrophic complications resulted in larger payouts (6.1 million) as compared with noncatastrophic complications (2.9 million). There is no association between specialty (neurosurgery or orthopaedic spine surgery), patient age/sex, and case outcome or award.
QUESTION 11 OF 50
of 100
Figures 1 and 2 are the radiographs of a 16-year-old boy who falls following a seizure. He is unable to bear weight on the right lower extremity following the fall. Over the subsequent 24 hours, his leg becomes progressively more painful and swollen. He is taken to the emergency department where on initial assessment his pain is out of proportion, positive stretch pain, tense leg swelling, and decreased motor function of his foot muscles with decreased sensations throughout the foot. Toes are warm and well-perfused. What is the best next step in management of this patient?

Figures 1 and 2 are the radiographs of a 16-year-old boy who falls following a seizure. He is unable to bear weight on the right lower extremity following the fall. Over the subsequent 24 hours, his leg becomes progressively more painful and swollen. He is taken to the emergency department where on initial assessment his pain is out of proportion, positive stretch pain, tense leg swelling, and decreased motor function of his foot muscles with decreased sensations throughout the foot. Toes are warm and well-perfused. What is the best next step in management of this patient?
1
Emergent fasciotomy of the leg
2
Open reduction and internal fixation (ORIF) of the fracture
3
CT scan of the knee
4
Closed reduction with long leg cast application
■
The radiographs reveal an Ogden type 4 tibial tubercle fracture. The clinical examination of the patient is highly suggestive of compartment syndrome.
Tibial tubercle fractures have been associated with the development of compartment syndrome, with rates as high as 10% reported in literature. It is caused by disruption of the branches of the recurrent anterior tibial artery, which travels on the lateral border of the tubercle. At the time of injury, the artery may be injured and retract under the fascia in the anterior compartment of the leg, leading to excessive bleeding in the anterior compartment. Patients with compartment syndrome should be emergently taken to the OR for fasciotomy and ORIF of the fracture.
Emergent fasciotomy of the leg with posterior splint is not called for, as this fracture needs anatomic reduction and fixation to prevent procurvatum deformity of proximal tibia. CT scan of the knee is not appropriate because this is compartment syndrome, which needs emergent fasciotomy.
This situation needs ORIF for anatomic reduction of the fracture with emergent fasciotomy for compartment syndrome of the leg. Closed reduction and percutaneous screw fixation is not the right option here.
QUESTION 12 OF 50
Indications for high tibial osteotomy include all of the following except:
1
10° to 15° of varus deformity on weight-bearing radiographs
2
90° preoperative range of motion
3
Flexion contracture less than 15°
4
60° preoperative range of motion
5
Age younger than 60 years
Indications for a high tibial osteotomy include age younger than 60 years, 10° to 15° varus deformity, 90° preoperative arCrange of motion, and flexion contracture less than 15°
QUESTION 13 OF 50
Which of the following soft tissue tumors may cause tumor-induced osteomalacia:
1
Liposarcoma
2
Malignant fibrous histiocytoma
3
Synovial sarcoma
4
Hemangiopericytoma
5
Atypical lipoma
Tumor-induced osteomalacia can be caused by a small tumor of bone or soft tissue (phosphaturic tumor). Small tumors may not be detected.
I. General Features
A. Presentation
1/. C hronic, vague symptoms - principally, bone pain
2/. Muscle weakness
3/. Fractures may occur
B. Metabolic profile
1/. Hypophosphatemia
2/. Low reabsorption of phosphate from the kidney
3/. 1,25 dihydroxy vitamin D - low or normal
4/. 25 hydroxy vitamin D, 24,25 dihydroxy vitamin D - normal
C . Tumor types
1/. Soft tissue
a. Hemangiopericytoma b. Sclerosing angioma
c. Benign angiofibroma d. Neurofibromatosis
D. Pathophysiology
1/. A molecule that wastes phosphorus - phosphatonin
E. Radiographic features
1/. Osteopenia
2/. Pseudofractures
3/. C oarsened trabeculae
4/. Soft tissue - a small, well-circumscribed soft tissue mass may be noted
F. Treatment
1/. Oral phosphate
2/. 1,25 dihydroxy vitamin D Correct Answer: Hemangiopericytoma
I. General Features
A. Presentation
1/. C hronic, vague symptoms - principally, bone pain
2/. Muscle weakness
3/. Fractures may occur
B. Metabolic profile
1/. Hypophosphatemia
2/. Low reabsorption of phosphate from the kidney
3/. 1,25 dihydroxy vitamin D - low or normal
4/. 25 hydroxy vitamin D, 24,25 dihydroxy vitamin D - normal
C . Tumor types
1/. Soft tissue
a. Hemangiopericytoma b. Sclerosing angioma
c. Benign angiofibroma d. Neurofibromatosis
D. Pathophysiology
1/. A molecule that wastes phosphorus - phosphatonin
E. Radiographic features
1/. Osteopenia
2/. Pseudofractures
3/. C oarsened trabeculae
4/. Soft tissue - a small, well-circumscribed soft tissue mass may be noted
F. Treatment
1/. Oral phosphate
2/. 1,25 dihydroxy vitamin D Correct Answer: Hemangiopericytoma
QUESTION 14 OF 50
Slide 1
This patient is a 17-year-old athlete who presents for treatment of a feeling of giving way of the ankle. The inversion clinical stress is demonstrated below (Slide). Which statement concerning the image presented below is correct:
This patient is a 17-year-old athlete who presents for treatment of a feeling of giving way of the ankle. The inversion clinical stress is demonstrated below (Slide). Which statement concerning the image presented below is correct:
1
Ankle instability is present.
2
Subtalar instability is present.
3
Ankle and subtalar instability are present.
4
Generalized ligamentous laxity is present.
5
No determination of instability can be made from this picture.
Although some laxity may be present in this patient, it is impossible to determine whether this is present in the ankle or the subtalar joint based upon this clinical test. Simple inversion stress without simultaneously palpating the lateral shoulder of the
talus cannot indicate the presence or the type of instability. An anterior drawer that is positive and, in particular, is associated with a vacuum phenomenon in the anterolateral ankle is more diagnostic of ankle instability.
talus cannot indicate the presence or the type of instability. An anterior drawer that is positive and, in particular, is associated with a vacuum phenomenon in the anterolateral ankle is more diagnostic of ankle instability.
QUESTION 15 OF 50
**CLINICAL SITUATION**
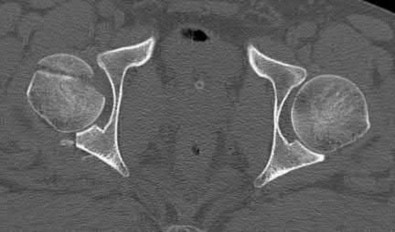
Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
She undergoes a closed reduction in the emergency department. Figures 2 through 5 are post-reduction CT images. What is the ideal surgical approach to address this fracture?
---
---
---
---
---

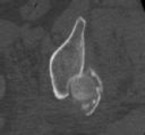


Figure 1 is the radiograph of a 67-year-old woman who is involved in a motor vehicle collision and sustains an isolated injury to her left hip. She is a community ambulatory who does not use any assistive devices.
She undergoes a closed reduction in the emergency department. Figures 2 through 5 are post-reduction CT images. What is the ideal surgical approach to address this fracture?
---
---
---
---
---
1
Kocher-Langenbeck
2
Ilioinguinal
3
Extended iliofemoral
4
Anterior intrapelvic Discussion: A
The patient sustained a posterior wall fracture dislocation. For acetabular fractures, the position of the limb in space at the time of impact (in terms of the amount of flexion/extension, internal/external rotation, and adduction/abduction) will dictate the fracture pattern. For posterior wall fracture patterns, the limb is in some degree of flexion, adduction, and internal rotation. Other combinations are possible to contribute to an acetabular fracture but not likely to contribute to a posterior wall pattern.
This posterior wall fracture pattern can be addressed from a standard Kocher-Langenbeck approach for both fixation and arthroplasty. There is no significant cranial or anterior extension of the fracture that would necessitate a modified posterior approach or greater trochanteric osteotomy. The other listed approaches would not be appropriate.
Indications for total hip arthroplasty are continuing to evolve and many patient-specific and fracture specific variables are involved. Several studies have investigated this issue and the common variables that influence the success of primary fixation are related to the age of the patient, greater than 50 years as well as associated bone quality and how these are affected with the fracture. The presence of marginal impaction suggests significant insult to the cartilage. In the presence of pre-existing cartilage wear, the likelihood of success with primary fixation is decreased. The presence of significant comminution of the fracture (greater than 3 fragments) also suggests decreased success with primary fixation. The other factors listed can contribute to perioperative morbidity but not as clearly when compared to the three listed in
. In the clinical setting of a patient older than 50 years old with a comminuted fracture, marginal impaction, and femoral head damage, there should be serious consideration for combined fracture fixation and acute total hip arthroplasty. Delayed arthroplasty can be an option in some patients, but clinical outcomes have not been as favorable as acute combined treatment.
Although urethral tears, rib fractures, and subdural hematoma are commonly involved with high-energy accidents and are routinely investigated through advanced trauma life support (ATLS) protocols, the ipsilateral knee has not received such focus. In a recent multi-center study, 15% of patients were found to have ipsilateral knee symptoms within a period of 1 year from the date of injury. The patterns of knee injury included 56 fractures (29%), 49 ligamentous lesions (25%), and 88 miscellaneous (46%) causes, including bone bruises, wounds, and swelling.
Multi-ligamentous knee injuries can be occult and a detailed examination of the knee should be standard in these patients upon secondary and tertiary surveys.
This posterior wall fracture pattern can be addressed from a standard Kocher-Langenbeck approach for both fixation and arthroplasty. There is no significant cranial or anterior extension of the fracture that would necessitate a modified posterior approach or greater trochanteric osteotomy. The other listed approaches would not be appropriate.
Indications for total hip arthroplasty are continuing to evolve and many patient-specific and fracture specific variables are involved. Several studies have investigated this issue and the common variables that influence the success of primary fixation are related to the age of the patient, greater than 50 years as well as associated bone quality and how these are affected with the fracture. The presence of marginal impaction suggests significant insult to the cartilage. In the presence of pre-existing cartilage wear, the likelihood of success with primary fixation is decreased. The presence of significant comminution of the fracture (greater than 3 fragments) also suggests decreased success with primary fixation. The other factors listed can contribute to perioperative morbidity but not as clearly when compared to the three listed in
. In the clinical setting of a patient older than 50 years old with a comminuted fracture, marginal impaction, and femoral head damage, there should be serious consideration for combined fracture fixation and acute total hip arthroplasty. Delayed arthroplasty can be an option in some patients, but clinical outcomes have not been as favorable as acute combined treatment.
Although urethral tears, rib fractures, and subdural hematoma are commonly involved with high-energy accidents and are routinely investigated through advanced trauma life support (ATLS) protocols, the ipsilateral knee has not received such focus. In a recent multi-center study, 15% of patients were found to have ipsilateral knee symptoms within a period of 1 year from the date of injury. The patterns of knee injury included 56 fractures (29%), 49 ligamentous lesions (25%), and 88 miscellaneous (46%) causes, including bone bruises, wounds, and swelling.
Multi-ligamentous knee injuries can be occult and a detailed examination of the knee should be standard in these patients upon secondary and tertiary surveys.
QUESTION 16 OF 50
Intraoperatively, all patients with sickle cell disease require which of the following:
1
CardiaCrhythm monitoring
2
Oxygen saturation monitoring
3
Active warming
4
Blood pressure monitoring
5
All of the above
The most common intraoperative complications are excessive blood loss (53%), followed by hypothermia (11%). Therefore, patients require extensive monitoring of cardiaCrhythm, blood pressure, temperature, and oxygen saturation. They also need active intraoperative warming, which usually consists of a combination of a warming blanket, humidifier, blood/fluid warmer, and heat lamp
QUESTION 17 OF 50
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. The patient fails an extensive course of physical therapy and is unable to return to baseball. He and his orthopaedic surgeon elect to proceed with surgery. During a repeat evaluation, he has negative sulcus and Beighton sign findings, and radiographs show 5° of glenoid retroversion. What is the most appropriate surgical plan?
---
---


---
---
1
Arthroscopic infraspinatus tenodesis
2
Arthroscopic posterior labral repair
3
Arthroscopic capsular shift and rotator interval closure
4
Posterior glenoid opening-wedge osteotomy
Posterior shoulder instability is a rare form of instability that often presents with pain rather than feelings of instability. It often occurs in young athletes during activities that put the shoulder in an “at-risk position” (flexion, adduction, internal rotation). Repetitive microtrauma can lead to posterior shoulder instability such as seen in football linemen. Swinging a bat or golf club places the lead arm in a flexed, adducted, and internally rotated position, which can lead to posterior translation of the humeral head that is forcibly reduced in follow-through, as seen in this patient. The glenohumeral joint relies on static and dynamic stabilizers. Static stabilizers help prevent instability at the end ranges of motion when the ligaments are taut. Dynamic stabilizers work to prevent subluxation at midranges of motion, at which the ligaments are lax. The rotator cuff is integral as a dynamic stabilizer of the shoulder. It works through a process called concavity compression. The four muscles of the rotator cuff compress the humeral head into the concavity of the glenoid-labrum. This prevents the humeral head from subluxing during the midranges of motion. Of the four rotator cuff muscles, the subscapularis is most important at preventing posterior subluxation. This patient has posterior instability, and various surgical techniques may be indicated depending on findings. Arthroscopic labral repair is indicated for anterior instability. Arthroscopic posterior labral repair is indicated for this patient because he has a posterior labral tear and posterior instability. If a patient has ligamentous laxity (not seen in this scenario because sulcus and Beighton sign findings would be negative), a posterior capsular shift with rotator interval closure is indicated. If a patient has excessive glenoid retroversion (not seen in this scenario with 5 degrees of retroversion), a posterior opening-wedge osteotomy is appropriate. The most common complication seen after arthroscopic posterior labral repair is stiffness, followed by recurrent instability
and degenerative joint disease.
and degenerative joint disease.
QUESTION 18 OF 50
Overall objectives in total knee replacement (TKR) should include all of the following except:
1
Valgus aligned knee
2
Range of motion 0° to 125°
3
Midline tracking patella
4
Collateral ligament balance at full extension and 90°
5
Neutral aligned knee
To have a satisfactory alignment one should have a valgus aligned knee, not a neutral aligned knee. Range of motion should be
0° to 125° with midline tracking patella. The collateral ligament should be balanced at full extension an 90°
0° to 125° with midline tracking patella. The collateral ligament should be balanced at full extension an 90°
QUESTION 19 OF 50
A 12-year-old child with spina bifida paraplegia requires brace management for ankle stability. Which of the following principles applies to brace management in this individual?
1
A shorter lever arm is more effective in limiting pressure.
2
Limbs with mild contractures do better with bracing than flaccid limbs through increased force concentration.
3
Three-point pressure effect works best to prevent the joint from buckling.
4
Four-point pressure effect works best to prevent the joint from buckling.
5
Smaller base support provides increased stability.
Bracing for spina bifida paraplegia provides both support and improved function of the movable limb. An orthosis has value in controlling unstable joints. The three-point pressure effect applies a force above and below the joint to prevent it from buckling. A four-point pressure effect is only required for a two-joint system (this patient has problems only at the ankle). A longer lever arm brace and a brace with a greater area of support provide better stability. Finally, a straighter limb, without contracture, applies less pressure to the brace and lessens overload to the skin.
REFERENCES: Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Bleck EE: Current concepts review: Management of the lower extremities in children who have cerebral palsy. J Bone Joint Surg Am 1990;72:140-144.
Harris MB, Banta JV: Cost of skin care in the myelomeningocele population. J Pediatr Orthop 1990;10:355:361.
REFERENCES: Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Bleck EE: Current concepts review: Management of the lower extremities in children who have cerebral palsy. J Bone Joint Surg Am 1990;72:140-144.
Harris MB, Banta JV: Cost of skin care in the myelomeningocele population. J Pediatr Orthop 1990;10:355:361.
QUESTION 20 OF 50
Which of the following indicates resolution of a postoperative wound infection?
1
C-reactive protein (CRP) has normalized and erythrocyte sedimentation rate (ESR) is improving
2
CRP and ESR remain elevated
3
CRP and ESR are below normal
4
CRP has improved to the same degree as the ESR has improved
5
CRP remains elevated after the ESR has normalized
Khan and associates in a retrospective review found that CRP was more responsive and normalized with resolution of infection, whereas the ESR can remain elevated in the presence of a normal CRP. Since the normal range of ESR and CRP usually begins at 0, a level that is below normal is not likely to be found.
QUESTION 21 OF 50
The development of complex regional pain syndrome (CRPS) following distal radius fracture is associated with what factor?
1
Diabetes
2
Fibromyalgia
3
Nonsurgical fracture management
4
Male gender
CRPS is an uncommon complication following distal radius fractures; its incidence is reported to range between 1% and 37%. Two recent studies have evaluated for risk factors in the development of CRPS following distal radius fractures. Female gender, concomitant fracture of the distal ulna, and surgical treatment were all associated with an increased likelihood of CRPS, as was fibromyalgia. Older age was _identified as conferring both an increased and a decreased risk for CRPS in the two studies._
QUESTION 22 OF 50
of 100
Which procedure(s) would most directly correct the principal deformity shown in Figure 11?

Which procedure(s) would most directly correct the principal deformity shown in Figure 11?
1
Tendo achilles lengthening (TAL)
2
Medializing calcaneal osteotomy and TAL
3
Posterior tibial tendon (PTT) debridement with flexor digitorum longus (FDL) transfer and first tarsometatarsal fusion
4
Lateral column lengthening and spring ligament reconstruction
The radiograph shows a severely abducted forefoot. Lateral column lengthening directly addresses the abducted forefoot by adducting the foot through the talonavicular joint. Spring ligament reconstruction can help to pull the foot out of abduction to some degree, as well.
TAL addresses the equinus deformity that is ever present with acquired flatfoot deformity. A medializing calcaneal osteotomy addresses hindfoot valgus. To address PTT dysfunction, the degenerative PTT is debrided and the FDL is often transferred into its position. A first tarsometatarsal fusion helps to stabilize the medial column. None of these procedures would correct the forefoot abduction seen in the above radiograph.
RECOMMENDED READINGS
20. [Chan JY, Greenfield ST, Soukup DS, Do HT, Deland JT, Ellis SJ. Contribution of Lateral Column Lengthening to Correction of Forefoot Abduction in Stage IIb Adult Acquired Flatfoot Deformity Reconstruction. Foot Ankle Int. 2015 Dec;36(12):1400-11. doi: 10.1177/1071100715596607. Epub 2015 Jul 27. PubMed PMID: 26216884. ](http://www.ncbi.nlm.nih.gov/pubmed/26216884)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26216884)
21. [Deland JT. Adult-acquired flatfoot deformity. J Am Acad Orthop Surg. 2008 Jul;16(7):399-406. Review. PubMed PMID: 18611997. ](http://www.ncbi.nlm.nih.gov/pubmed/18611997)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18611997)
22. [Williams BR, Ellis SJ, Deyer TW, Pavlov H, Deland JT. Reconstruction of the spring ligament using a peroneus longus autograft tendon transfer. Foot Ankle Int. 2010 Jul;31(7):567-77. doi: 10.3113/FAI.2010.0567. PubMed PMID: 20663422. ](http://www.ncbi.nlm.nih.gov/pubmed/20663422)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20663422)
RESPONSES FOR QUESTIONS 12 THROUGH 15
1. T-type fracture
2. Anterior column fracture
3. Anterior wall fracture
4. Posterior wall fracture
5. Posterior column and posterior wall fracture
6. Transverse with posterior wall fracture
For each image set below, please select the correct diagnosis listed above
TAL addresses the equinus deformity that is ever present with acquired flatfoot deformity. A medializing calcaneal osteotomy addresses hindfoot valgus. To address PTT dysfunction, the degenerative PTT is debrided and the FDL is often transferred into its position. A first tarsometatarsal fusion helps to stabilize the medial column. None of these procedures would correct the forefoot abduction seen in the above radiograph.
RECOMMENDED READINGS
20. [Chan JY, Greenfield ST, Soukup DS, Do HT, Deland JT, Ellis SJ. Contribution of Lateral Column Lengthening to Correction of Forefoot Abduction in Stage IIb Adult Acquired Flatfoot Deformity Reconstruction. Foot Ankle Int. 2015 Dec;36(12):1400-11. doi: 10.1177/1071100715596607. Epub 2015 Jul 27. PubMed PMID: 26216884. ](http://www.ncbi.nlm.nih.gov/pubmed/26216884)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/26216884)
21. [Deland JT. Adult-acquired flatfoot deformity. J Am Acad Orthop Surg. 2008 Jul;16(7):399-406. Review. PubMed PMID: 18611997. ](http://www.ncbi.nlm.nih.gov/pubmed/18611997)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/18611997)
22. [Williams BR, Ellis SJ, Deyer TW, Pavlov H, Deland JT. Reconstruction of the spring ligament using a peroneus longus autograft tendon transfer. Foot Ankle Int. 2010 Jul;31(7):567-77. doi: 10.3113/FAI.2010.0567. PubMed PMID: 20663422. ](http://www.ncbi.nlm.nih.gov/pubmed/20663422)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/20663422)
RESPONSES FOR QUESTIONS 12 THROUGH 15
1. T-type fracture
2. Anterior column fracture
3. Anterior wall fracture
4. Posterior wall fracture
5. Posterior column and posterior wall fracture
6. Transverse with posterior wall fracture
For each image set below, please select the correct diagnosis listed above
QUESTION 23 OF 50
A 5-year-old child is bitten by a tick. Which of the following has been shown to aid in management:
1
Prompt tick removal
2
Immediate treatment with doxycycline
3
Immediate treatment with amoxicillin
4
Prompt ELISA testing
5
Steroid administration
Prompt tick removal is recommended because Lyme disease is more likely if the tick is attached for more than 24 hours. Immediate antibiotic administration is not recommended because the incidence of Lyme disease is low after any single tick bite and treatment is equally effective once the disease is diagnosed. Doxycycline is not recommended in children younger than 8
years old because of dental discoloration. Immediate testing for antibodies (ELISA) is not useful because antibodies do not rise for at least several weeks. Steroids are not recommended in this setting.
years old because of dental discoloration. Immediate testing for antibodies (ELISA) is not useful because antibodies do not rise for at least several weeks. Steroids are not recommended in this setting.
QUESTION 24 OF 50
of 100
The most appropriate course of treatment is
The most appropriate course of treatment is
1
extension block splinting.
2
hemi-hamate arthroplasty.
3
implant arthroplasty.
4
volar plate arthroplasty.
- hemi-hamate arthroplasty._
QUESTION 25 OF 50
Time to soft-tissue coverage was not shown to have a statistically significant difference on the rate of infection in the level II study by Pollak et. al
A 38-year-old male suffers the injury shown in Figure A. During operative fixation, free osteoarticular fragments are encountered and reconstruction of these pieces is attempted. Postoperatively, which of the following will have the most beneficial effect on the healing potential of the surviving chondrocytes within these reconstructed articular segments?








































A 38-year-old male suffers the injury shown in Figure A. During operative fixation, free osteoarticular fragments are encountered and reconstruction of these pieces is attempted. Postoperatively, which of the following will have the most beneficial effect on the healing potential of the surviving chondrocytes within these reconstructed articular segments?
1
Gentle compressive loading of the affected joint through early range of motion exercises
2
Strict joint immobilzation for three weeks
3
Shear loading of the affected joint
4
Joint distraction with a spanning external fixator for three weeks
5
Glucosamine chondroitin sulfate supplementation
Figure A demonstrates a comminuted tibial plateau fracture with significant intra-articular involvement. Basic science evidence has demonstrated that post-operative gentle compressive loading may have a positive impact on articular cartilage healing; however, excessive shear loading may be detrimental.
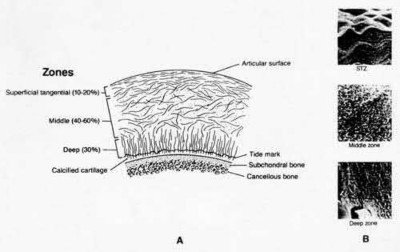
Irrgang et al provide guidelines for rehabilitation following surgical management of articular cartilage lesions of the knee. They state that after articular cartilage repair, exercises to enhance muscle function must be done in a manner which minimizes shear loading of the joint surfaces in the area of the lesion. The authors also discuss the benefits of gentle compressive loading and motion of the joint, and its positive effects on chondrocyte nutrition.
Furthermore, they recommend a period of protected weight bearing as often being necessary, and that this should be followed by progressive loading of the joint.
Illustration A is a diagram showing the different layers of joint cartilage.
When utilizing the pectoralis major tendon as a reference for restoring humeral height during shoulder hemiarthroplasty, at what level cephalad to the proximal edge of the tendon should the top of the prosthesis sit?
Joint stability is critical for successful nonoperative management of posterior wall acetabular fractures. Recent evidence has established that dynamic fluoroscopic stress examination is the best method to determine joint stability in the setting of a posterior wall fracture. The obturator oblique view allows for the best evaluation of hip joint stability during examination for posterior wall fractures.
Grimshaw and Moed retrospectively reviewed the results of patients with posterior wall acetabular fractures managed nonoperatively after evaluation with dynamic fluoroscopic stress tests. At two year follow up, all had good to excellent Merle d’Aubigne clinical scores for hip function and no evidence of post-traumatic hip arthritis on AP pelvis radiographs.
Tornetta retrospectively reviewed his results managing patients with dynamic fluoroscopic stress examination for acetabular fractures which met radiographic nonoperative criteria. Good-to-excellent clinical results were seen in 91% of patients managed nonoperatively.
Tornetta reviewed management of acetabular fractures and Tornetta and Mostafavi separately reviewed management of hip dislocations. In both
articles, emphasis is placed on dynamic examination of posterior wall fractures as instability has been seen with fractures comprising as little as 15% of the posterior wall.
Illustration A demonstrates two fluoroscopic images from a dynamic stress exam of a patient with a posterior wall fracture. The image obtained in the obturator oblique view clearly demonstrates that the femoral head loses congruency with the acetabular dome.
Incorrect Answers:
Answers 1 & 2: Posterior wall fragment size less than 40% was historically used as an indirect measure of stability, however measurements of fragment size may be unreliable and instability has been seen with fractures much smaller than 40%
: A history of hip dislocation was thought to indicate a more unstable fracture. In the level IV study by Grimshaw and Moed, patients with an associated hip dislocation who were stable under stress exam had no significant difference in outcome with nonoperative management.
Answer 5: The iliac oblique view is used to evaluate the anterior wall and posterior column. Displacement or instability of the posterior wall would not be seen with this view
A 64-year-old woman is thrown off a horse, sustaining the injury shown in Figures A and B. She undergoes surgical fixation as seen in Figures C through E. What is the most commonly reported complication of this procedure?
1) Axillary nerve injury
2) Valgus migration of the fracture
3) Nonunion
4) Hardware failure
5) Screw penetration
The patient in the scenario has a 2-part proximal humerus fracture treated with a locking plate as seen in Figures A-E. The most common complication with the use of this implant is screw penetration. The terms screw cut out and penetration are often used interchangeably in the literature with cut out appearing more frequently in reports regarding intertrochanteric fractures.
Owsley et al retrospectively reviewed 53 proximal humerus fractures treated with locking plates and the same post-operative protocol. The most common complication was screw cut out or penetration, followed by varus displacement. They concluded that 3 and 4-part fractures in patients over 60 years have a higher incidence of failure.
Agudelo et al retrospectively reviewed 153 patients at a level-one trauma center treated with proximal humerus locking plates, investigating modes of failure for the implant. They determined that varus malreduction (head-shaft angle
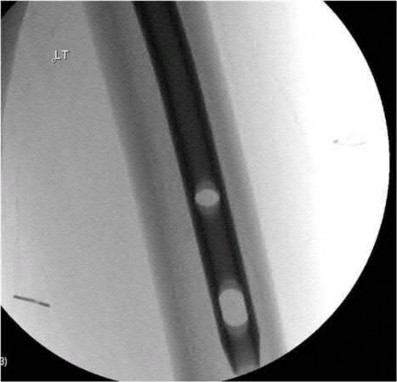
A 25-year-old male sustained a closed midshaft femur fracture following a motor vehicle collision. He is taken to the operating room for supine intramedullary nail fixation of the fracture. Figure A is a lateral fluoroscopic view of the distal femur taken just prior to distal interlocking screw placement. What change in position (with the Carm stationary) would be expected to produce a perfect lateral view of the interlocking hole?
1) Raising the leg
2) Lowering the leg
3) Internal (or external) rotation of the leg
4) Abduction (or adduction) of the leg
5) Fluoroscopic magnification
Interlocking of intramedullary nails using fluoroscopy requires attention to detail. A true lateral of the intramedullary nail is present when "perfect circle" views of interlocking holes are present. Once perfect circles are obtained, the drill can be advanced parallel to the fluoroscopic beam.
Knowledge of the implications of the appearance of the interlocking holes when "perfect circles" are not present can be helpful in minimizing the number of manipulations and fluoroscopic exposure. Widening of the interlocking hole in the proximal-distal direction (as is seen in this case) signifies the need for an adjustment in the abduction/adduction plane. Similarly, widening of the interlocking hole in the anterior-posterior plane signifies the need for an adjustment in the internal/external rotation plane (Answer 3).
Raising or lowering the leg (Answer A and B) should not have major effects of the appearance of the interlocking hole. Similarly, magnification of the C-arm (Answer D) will not affect the appearance. Internal/external rotation will result in widening in the anterior-posterior plane (as this dimension is currently adequate). Abduction or adduction will result in creating "perfect circles" (Answer 4). The position of the leg may hint to which of these is correct. If further widening occurs in the proximal-distal direction, the opposite maneuver will correct to the proper position.
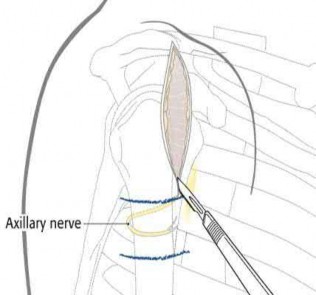
A 46-year-old male is involved in a motor vehicle accident and suffers a proximal humerus fracture. Operative treatment is recommended, and plate fixation is performed through an extended anterolateral acromial approach. Which of the following structures is at increased risk of injury using this surgical exposure compared to the deltopectoral approach?
1) Musculocutaneous nerve
2) Posterior humeral circumflex artery
3) Axillary nerve
4) Cephalic vein
5) Anterior humeral circumflex artery
The anterolateral acromial approach was developed to allow less invasive treatment of proximal humerus fractures. The plane of the avascular anterior
deltoid raphe is utilized, and the axillary nerve is at particular risk of injury and must be identified and protected. With this approach, anterior dissection near the critical blood supply is avoided, substantial muscle retraction is minimized, and the lateral plating zone is directly accessed.
Gardner et al evaluated 23 patients who had acute displaced fractures of the proximal humerus treated with the anterolateral acromial approach and either a locking plate or an intramedullary nail. At one year post-op, there were no axillary nerve deficits, and they found that the approach allowed direct access to the lateral fracture planes for fracture reduction and plate placement or safe nail and interlocking screw placement.
Gardner et al, in another study, performed cadveric dissection using the extended anterolateral acromial approach and measured multiple parameters regarding the axillary nerve. The nerve was predictably found approximately 35 mm from the prominence of the greater tuberosity.
Morgan et al performed a cadaveric study to describe the anatomic insertion point of the deltoid onto the proximal humerus. They found that the deltoid insertion is long and broad, and that placement of 4.5-mm plate would result in detaching 13.5 mm of its insertional footprint. This would leave half of the insertion still attached to the humerus.
Illustration A shows the position of the axillary nerve in relation to the approach.
Which of the following statements is true regarding brake travel time after surgical treatment of complex lower extremity trauma?
1) Brake travel time is significantly increased until 6 weeks after patient begins weight bearing
2) Return of normal brake travel time takes longer after long bone fracture compared to articular fractures
3) Normal brake travel time correlates with improved short musculoskeletal
functional assessment scores
4) Brake travel time is significantly reduced until 8 weeks after patient begins weight bearing
5) Brake travel time returns to normal when weight bearing begins
Brake travel time (BTT) has been shown to be significantly increased until 6 weeks after initiation of weight bearing in both long bone and articular fractures of the right lower extremity.
Egol et al used a computerized driving simulator to compare BTT in three groups of patients; 1)control group, 2)long bone lower extremity fracture group, 3)lower extremity articular fracture group. They concluded that BTT was significantly increased until 6 weeks after initiation of weight bearing in both long bone and articular fractures of the right lower extremity, and that short musculoskeletal functional assessment scores improved with respect to function and other indexes, but did not correlate with improvement in BTT.
An earlier study by Egol et al looked at total brake time as it related to distance traveled by the automobile before braking at 6, 9, and 12 weeks after operative fixation of a right ankle fracture. When compared with controls, braking time was shown to return to normal by 9 weeks post-operatively, and no significant association was found between the functional scores and this normalization.
Giddins et al provide a review of the literature, the law and the views of the major motor insurers related to driving after injury or operations.
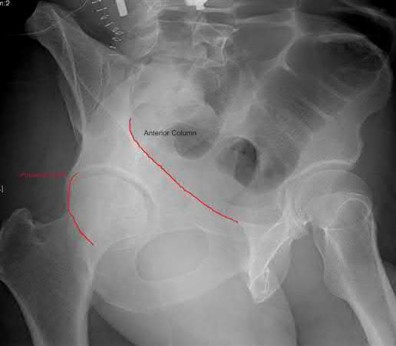
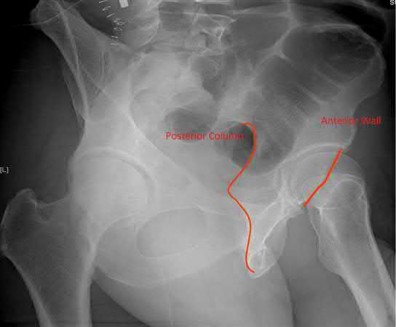
What acetabular component is best appreciated on an obturator oblique radiograph of the pelvis as seen in Figure A?
1) Ilioischial line
2) Posterior column
3) Posterior wall
4) Anterior wall
5) Sacroiliac joint
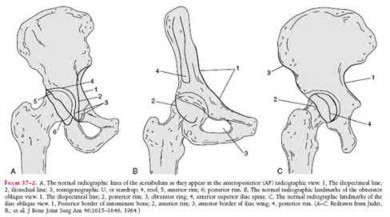
Letournel and Judet developed a schematic representation of the acetabulum as being contained within asymmetric long anterior and short posterior arms of an inverted “Y”.
On the bony pelvis, the ilioischial component becomes that posterior column and the iliopectineal line becomes the anterior column. The Judet-Letournel classification system is based on this scheme. By careful evaluation of landmarks on a standard AP pelvis radiograph, as well as on 45-degree oblique obturator and iliac views, the extent of injury can be determined accurately.
The AP view usually demonstrates the six fundamental landmarks relatively well as seen in illustration A. The obturator oblique view reveals additional information about the anterior column and posterior wall(see illustration A(B),
B). In an obturator oblique view the x-ray beam is centered on and almost perpendicular to the obturator foramen. The iliac oblique view visualizes the posterior column and anterior wall (illustration A(C), C). This view also shows the best detail of the iliac wing as the radiographic beam is roughly perpendicular to the iliac wing. Inclusion of the opposite hip is essential for evaluation of symmetrical contours that may have slight individual variations
and to evaluate the width of the normal articular cartilage in each view in a pelvic series (AP, Judet's) .
Which of the following fractures seen in Figures A through E would be amenable to fixation with a construct using tension band principles?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
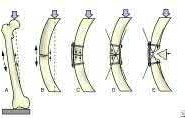
In order for a fracture to be successfully treated with tension band principles the bone must be eccentrically loaded, the construct must be applied on the tensile side, and the opposite cortex must be able to withstand compressive
forces. Of the fractures seen in Figures A-E, the subtrochanteric fracture seen in Figure A best meets the criteria for stabilization according to tension band principles.
Kinast et al retrospectively compared their results with 95 degree blade plate fixation of subtrochanteric fractures utilizing the blade plate as a dynamic tension band. They performed either wide exposure of the fracture site with autogenous bone grafting according to AO technique at the time (group 1), or indirect reduction techniques without bone grafting the medial side as advocated by Mast et al (group 2). The authors found 100% union rates at six months with indirect reduction techniques without bone grafting (group 2), and emphasize the key concepts of preservation of the medial soft tissues and intraoperative pretensioning of the plate.
Illustration A demonstrates the principles of tension band fixation specifically applied to the femur. Within Illustration A, Figure C shows the correct application of a plate along the lateral cortex to resist tensile forces, along with incorrect application of the plate along the medial cortex (Figure D) or in a fracture pattern with an absent opposite cortex (Figure E). Illustration B shows an example of blade plate fixation of a subtrochanteric fracture.
Incorrect Answers:
Answer 2. Figure B demonstrates a comminuted proximal tibia fracture. Although the tibia is eccentrically loaded and an implant applied to anterior cortex could function as a tension band, the posterior comminution would lead to collapse.
Answer 3. Figure C demonstrates a comminuted distal humeral shaft fracture. Again,the comminution prevents application of a tension band construct Answer 4: Figure D shows a valgus impacted proximal humerus fracture.
Eccentric loading is absent for this type of fracture
Answer 5: Figure E demonstrates a comminuted olecranon fracture with extension distal to the coronoid process. Although tension band constructs are commonly used for olecranon fractures, the comminution and distal extension of this fracture would prevent application of a tension band.
Which of the following is an advantage of computer-assisted navigation used to place medullary nail interlocking screws compared to a freehand techinque?
1) Reduced fluoroscopy time
2) More reliable placement of interlocking screws through the nail
3) Reduced procedure time
4) Increased quality of fluoroscopic images
5) Improved accuracy of screw length
Computer-assisted navigation has been shown to reduce radiation exposure for surgeons when performing interlocking of medullary nails compared to freehand technique.
Ricci et al compared two fluoroscopic navigation tracking technologies, optical and electromagnetic versus standard freehand fluoroscopic targeting, in a standardized foam block model for placement of interlocking screws. They found that fluoroscopy time (seconds) and number of fluoroscopy images were significantly less when using the computer-guided systems than for freehand-unguided insertion. Average distance of pin placement from the target in the foam blocks was significantly greater for controls than for each of the navigated systems.
Suhm et al performed a prospective controlled clinical study to compare fluoroscopic guidance with fluoroscopy-based surgical navigation for distal locking of intramedullary implants. The surgical navigation group showed increased procedure time, but equivalent precision with reduced radiation exposure. There was no significant difference in the technical reliability
between both groups.
An 82-year-old nursing home resident falls onto his elbow while rising from a seated position. He has pain and swelling at the elbow without evidence of instability. His radiographs show a comminuted displaced olecranon fracture involving 25% of the articular surface with global osteopenia. Which of the following treatment options has a low risk of complications and a high likelihood of a functional elbow outcome?
1) Cast immobilization in 45 degrees of flexion for 8 weeks
2) Closed reduction and percutaneous pinning
3) ORIF with a tension band construct
4) ORIF with a locking plate
5) Cast immobilization in 90 degrees flexion
The patient in the scenario is a low-demand, elderly patient with a comminuted olecranon fracture. Recent studies have demonstrated good outcomes with
non-operative treatment of olecranon fractures in this patient population.
Hak (jaos'00) reviewed the treatment of olecranon fractures, recommending ORIF for displaced intra-articular fractures, either via tension band wiring or plate osteosynthesis based on fracture pattern and associated ligamentous disruption. For elderly, low-demand, osteoporotic patients, triceps advancement and fragment excision is an option in the case of severely comminuted, osteoporotic patients with a fracture involving
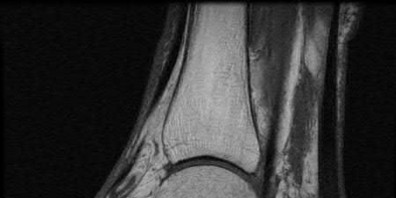
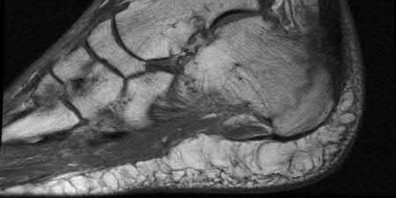
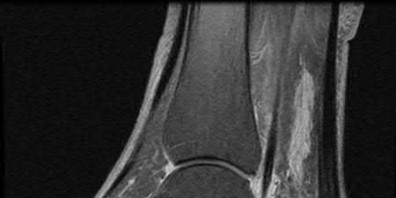
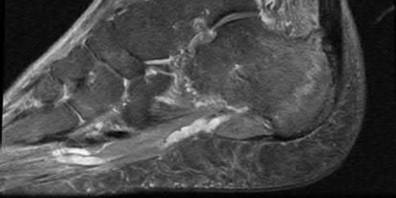
A 47-year-old male presents with a one month history of heel pain after starting marathon training. The heel is tender when squeezed. A foot radiograph is shown in Figure A, and an MRI is obtained which is shown in Figures B and C. What is the most likely diagnosis?
1) Osteomyelitis
2) Acute fracture
3) Subtalar arthritis
4) Achilles tendinitis
5) Stress fracture
The patients history, physical exam, and MRI findings are most consistent with the diagnosis of a stress fracture. Low signal on T1 and increased signal on T2-weighted images is the classic appearance of a stress fracture on magnetic resonance images. Usually the fracture appears as a linear signal band that arises from the cortex of the bone and extends perpendicular to the surface of the bone. Figures A and B show a linear area of enhancement in the posterior aspect of the calcaneus signifying a likely stress reaction from recent overtraining.
Boden et al review the pathogenesis and treatment of stress fractures. With regard to diagnosis, they state that it is primarily clinical, but imaging modalities such as plain radiography, scintigraphy, computed tomography, and magnetic resonance imaging may provide confirmation.
Gehrmann et al review stress fractures of the foot, and state that with regards to calcaneal stress injuries, MRI studies should be obtained for definitive diagnosis when radiographs are negative, and pain persists. With regards to
treatment, they state that these injuries usually heal with activity restrictions, heel-pad inserts, and protected weightbearing for a short period of time.
A 35-year-old right hand dominant man falls from a ladder and sustains the injury seen in Figure A. When discussing the risks and benefits of operative versus nonoperative treatment for his fracture, which of the following is true?
1) No difference in shoulder function
2) Higher risk of nonunion with operative management
3) Higher risk of symptomatic malunion or nonunion with nonoperative management
4) Earlier return to sport with nonoperative management
5) No difference in union rates
Historically, displaced midshaft clavicle fractures, as seen in Figure A, were managed nonoperatively. Recent literature has demonsrated improved outcomes with operative management of these fractures.
Khan et al review current concepts in the management of clavicle fractures. For displaced midshaft clavice fractures, operative treatment seems to result in improved patient and surgeon-based outcomes, decreased rates of malunion and nonunion, and shorter time to union.
Kim and McKee review recent evidence regarding the management of clavicle fractures. For midshaft clavicle fractures, the incidence of nonunion and symptomatic malunion with nonoperative management is higher than
previously believed. They state that risk factors include 100% displacement, comminution, increasing age and female gender.
Incorrect Answers
Answer 1. Recent randomized prospective trials have shown improved short term shoulder function with operative management of displaced midshaft clavicle fractures.
Answer 2. Nonunion rates of 7-15% have been shown with nonoperative management versus 2% with operative fixation
Answer 4. Earlier return to activities has been reported with operative management
Answer 5. As with answer 2, there is a significantly higher rate of nonunion with nonoperative management
Assuming the images represent isolated injuries, which of the following Figures demonstrates a Pipkin II femoral head fracture?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
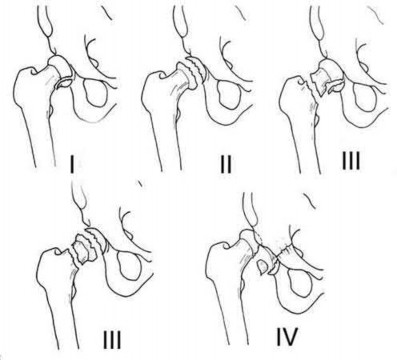
Figure D represents a Pipkin II femoral head fracture, which is defined as a fracture which is superior to the fovea. Differentiation between Pipkin I and Pipkin II fractures can be important, as suprafoveal injuries often require surgical fixation. Illustration A demonstrates the Pipkin fracture types.
Droll et al review femoral head fracture evaluation and treatment. They discuss non-operative indications (typically reserved for Pipkin I injuries) which include an anatomic or near anatomic reduction (
A 20-year-old female presents following a motor vehicle collision with the injuries seen in Figures A and B. She was initially hypotensive and tachycardic however she now has stable vital signs following a 2 liter bolus of saline and 2 units of packed red blood cells. Which of the following would indicate that this patient has occult end-organ hypoperfusion and should be further resuscitated prior to definitive fixation?
1) Heart rate of 80 beats per minute
2) Systolic blood pressure of 120 mmHg
3) Base deficit of -1.8 mEq/L
4) Serum lactate of 5 mmol/Liter
5) Urine output of 40ml/hour
Figure A demonstrates an unstable pelvic fracture and subtrochanteric femur fracture and Figure B shows a scapular body and mutliple rib fractures. These high-energy fractures, along with the patient's initial hypotension and tacchycardia indicate a multiply injured patient in shock. Serum markers such as lactate (normal
An 80-year-old female falls and sustains the fracture seen in Figure A. She is treated with an antegrade cephalomedullary nail. Which of the following led to the complication seen in Figure B?
1) Nail with a lesser radius of curvature
2) Nail with a greater radius of curvature
3) Piriformis entry portal
4) Trochanteric entry portal
5) Lateral decubitus patient position
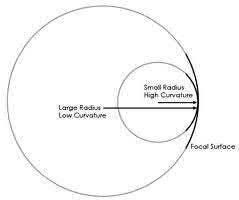
The image in Figure A shows an unstable intertrochanteric fracture and the image in Figure B shows perforation of the anterior cortex of the femur by the intramedullary implant. This complication is due to a mismatch of the curvature of the nail with the anterior bow of the femur, and was likely caused by a nail of a greater radius of curvature (eg, straighter than the femur).
Egol et al measured the radius of curvature for 474 matched cadaveric femurs and found the average anterior radius of curvature to be 120cm (+/- 36cm). In contrast, the radii of curvature for the measured intramedullary nails ranged from 186cm to 300cm, demonstrating that the nails were straighter than the femurs. The authors advocate for a decreased radius of curvature (more curve) for intramedullary nails, especially larger diameter implants designed for fractures about the hip
Ostrum and Levy present a case series of 3 patients with subtrochanteric
fractures who had anterior penetration of the femoral cortex. They state that the mismatch in femoral bow between the bone and the implant is a contributing factor to distal femoral anterior cortex penetration in intramedullary nailing of subtrochanteric fractures.
Simonian et al present 4 iatrogenic femoral neck fractures that occured during a series of 315 femoral nails. The authors attempted to reproduce the iatrogenic fractures with cadaveric femurs and felt that the iatrogenic fractures may be due to a combination of a valgus femoral neck and impingement from the AO insertion jig used at the time.
Harper and Carson examined 14 cadaveric femurs and intramedullary implants at the time. Similar to Egol et al, they found a mismatch between the radius of curvature of the femurs and the intramedullary nails.
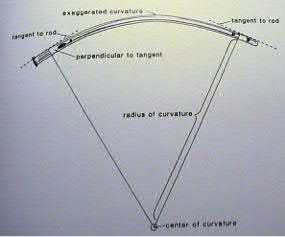
Illustration A shows the difference between a lesser and greater radius of curvature. Illustration B demonstrates how to calculate radius of curvature based on an implant with an exaggerated bow. Illustration C shows the anterior bow of a synthetic femoral model compared with several intramedullary implants.
Bridge plating of the olecranon is MOST appropriate in which of the following clinical scenarios?
1) Fixation of an olecranon osteotomy used for distal humerus surgery in a 24-year-old male
2) Simple transverse olecranon fracture in 33-year-old female
3) Comminuted olecranon fracture in 45-year-old male
4) Severely comminuted proximal olecranon fracture in an osteoporotic 91-year-old female
5) Aphophyseal elbow fracture in 6-year-old male
Bridge plating is most appropriately used for fixation of comminuted fractures which are not able to be fixed anatomically. Of the choices listed above, this would be most appropriate in a comminuted fracture in a 45-year-old male. In contrast, literature shows that severely comminuted, osteoporotic low-demand elderly are best treated with olecranon fracture excision and triceps advancement when possible.
Bailey et al looked at the outcome of plate fixation of olecranon fractures. They concluded that plate fixation is effective for displaced olecranon fractures and leads to good functional outcome. There were low incidence of complications, although 20% did have removal of hardware due to irritation.
Hak et al reviewed the fixation options for olecranon fractures. In their review, they state that comminuted olecranon fractures can be treated by limited-contact dynamic-compression plates. They also supported the use of supplemental bone graft to support comminuted depressed articular fragments. Fragment excision and triceps advancement is appropriate in selected cases in which open reduction seems unlikely to be successful, such as in osteoporotic elderly patients with severely comminuted fractures.
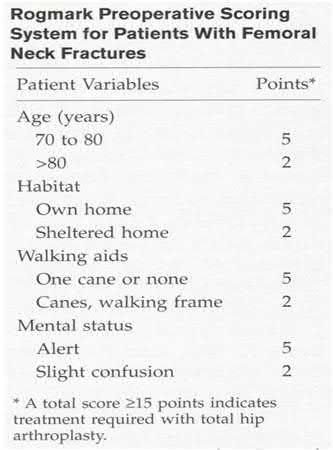
A 75-year-old ambulatory male who lives independently presents with the fracture shown in Figure A. Which of the following is true regarding timing of surgical fixation and post-operative mortality?
1) 30 day mortality is decreased if surgery is delayed 4-7 days
2) 1 year mortality is increased if surgery is delayed greater than 4 days
3) Delay of surgery due to treatment of acute medical comorbidities has no effect on post-operative mortality rates
4) 90 day mortality rate is decreased if surgery is delayed greater than 7 days
5) Timing of surgical fixation has no statistically significant affect on postoperative mortality
Figure A shows a displaced femoral neck fracture.
Moran et al studied 2660 elderly patients who underwent surgical treatment of a hip fracture to determine whether a delay in surgery affects postoperative mortality. The 30-day mortality for patients for whom the surgery had been delayed for more than 4 days was 10.7%, compared to 7.3% in those delayed 1-4 days. The group delayed >4 days also had significantly increased mortality at 90 days and 1 year. Patients who had been admitted with an acute medical comorbidity that required treatment prior to the surgery had a 30-day mortality of 17%, which was nearly 2.5 times greater than that for patients without and acute comorbidity. The study concluded that patients with medical comorbidities that delayed surgery had 2.5 times the risk of death within 30 days after the surgery compared with patients without comorbidities. Mortality was not increased when the surgery was delayed up to four days for patients who were otherwise fit for hip fracture surgery, however, a delay of more than four days significantly increased mortality.
Healy et al examined 120 patients who underwent surgical treatment of 186 displaced femoral neck fractures with either internal fixation, hemiarthroplasty, or total hip arthroplasty. Arthroplasty was associated with more independent living, and was more cost-effective than internal fixation. There was no difference in rates of reoperation or mortality, but arthroplasty produced a longer interval to reoperation or death. They concluded that total hip arthroplasty was the best treatment for displaced fractures of the femoral neck in their series.
Illustration A shows a scoring system developed by Rogmark et al to aid in decision making.
A 35-year-old male suffers an anterior column acetabular fracture during a motor vehicle collision, and subsequently undergoes percutaneous acetabular fixation. Intraoperatively, fluoroscopy is positioned to obtain an obturator oblique-inlet view while placing a supraacetabular screw. Which of the following screw relationships is best evaluated with this view?
1) Intraarticular penetration of the screw
2) Position of the screw cephalad to the sciatic notch
3) Screw starting point at the anterior inferior iliac spine
4) Screw starting point at the gluteal pillar
5) Screw position between the inner and outer tables of the ilium
The obturator oblique-inlet view, as seen in Illustration A, best demonstrates the position of a supra-acetabular screw or pin relative to the tables of the ilium.
Starr et al review their initial results and technique of closed or limited open reduction and percutaneous fixation of acetabular fractures. They defined two groups of patients who may benefit from this technique; elderly patients with multiple comorbidities to facilitate early mobilization and restore hip morphology, and young patients with elementary fracture patterns and multiple associated injuries.
Starr et al describe their operative technique and outcomes for a case series of 3 patients using percutaneous acetabular fixation to augment open reduction of acetabular fractures. The authors state that, for placement of an anterior colum ramus screw, an iliac oblique-inlet (not obturator oblique-inlet) will ensure that the screw is within the medullary canal of the ramus and does not exit anterior or posterior.
Gardner and Nork describe a technique for placement of a large femoral distractor in the supra-acetabular region to compress displaced posterior pelvic ring injuries. They note that the obturator oblique-inlet view is necessary to view the entire length of the pin as well as to ensure that pin remains in bone.
Incorrect answers:
Answer 1: Relationshiop of the screw to the acetabulum is best evaluated with the obturator oblique-outlet view as well as the iliac oblique view
Answer 2: The iliac oblique view is used to ensure the trajectory of the screw is superior to the sciatic notch
Answer 3: The Obturator oblique-outlet view, otherwise known as the "teepee" or "tear drop" view, is used to identify the start for supra-acetabular implant placement
Answer 4: The gluteal pillar is not utilized as a start point when placing supraacetabular fixation, and the obturator oblique-inlet view would not be ideal to visualize this region of the pelvis
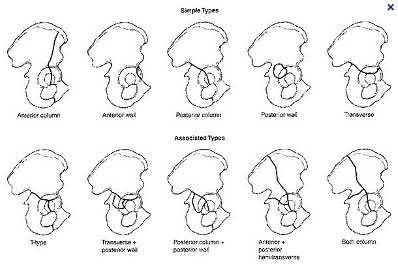
A 74-year-old man falls, sustaining the injury shown in Figures A through C. In surgical planning, what is the best surgical approach to treat this injury?
1) Kocher-Langenbeck
2) Watson-Jones
3) Extended iliofemoral
4) Ilioinguinal
5) Hardinge
Figures A through C depict and AP pelvis and Judet views of a T-type fracture of the right acetabulum. The ilioinguinal approach provides access to the anterior wall and anterior column for fracture fixation, in addition to allowing fixation of the nondisplaced posterior transverse fracture line. The lateral femoral cutaneous nerve (LFCN) is at risk in the superficial part of the dissection. Another option for the approach would be the modified Stoppa, which would also allow excellent access to the anterior column as well as the internal aspect of the iliac wing and quadrilateral plate.
Illustration A shows the five basic and 5 associated acetabular fractures. Incorrect Answers:
Answer 1. Kocher-Langenbeck: access for posterior wall and column fractures
Answer 2. Watson-Jones: anterolateral approach best for the hip, not the anterior column of the acetabulum.
Answer 3. Extended iliofemoral: visualization for both column fractures Answer 5. Hardinge approach: lateral approach for THA
A 28-year-old female is struck by a motor vehicle while crossing the street and suffers the injury seen in Figure A. What technical adjunct could have prevented the operative complication seen in Figure B?
1) Nail of a lesser radius of curvature
2) Nail with a more distal Herzog curve
3) Application of an anterior unicortical plate
4) Nailing while in a hyperflexed position
5) A more distal and medial nail entry site
The patient has a proximal tibia fracture that has been malreduced in procurvatum with anterior translation of the proximal fragment as seen in Figures A and B. Intramedullary nailing of proximal tibia fractures may result in malalignment such as valgus, procurvatum and anterior translation of the proximal fragment.Techniques such as anterior unicortical plating have been described to maintain reduction while placing a locked intramedullary implant.
Nork et al retrospectively review their results using several different intraoperative adjuncts to maintain reduction while nailing proximal tibia fractures including anterior unicortical plates and femoral distractors. They report that, despite high rates of segmental comminution (59.5%) and open fractures (35.1%), acceptable alignment and primary union were achieved in more than 90% of patients.
Dunbar et al describe their technique for application of a provisional unicortical plate through the traumatic wound to maintain reduction during intramedullary nailing of Gustilo-Anderson Type III open tibia fractures. The authors advocate that further soft tissue stripping during plate placement should be avoided, and found excellent results in terms of coronal and sagittal plane alignment for fractures treated with this technique.
Matthews et al review their experience with unicortical plating to maintain reduction during intramedullary nailing of tibia fractures. Similar to the other referenced studies, the authors found the technique assisted with maintaining reduction intraoperatively.
Illustrations A and B demonstrate maintenance of reduction of a proximal tibia fracture using an anterior unicortical plate as a reduction tool during intramedullary nailing.
Incorrect Answers:
Answer 1: Nail of a lesser radius of curvature. Unlike femoral nails, tibial nails are straight to match the coronal/sagittal axis of the tibia and therefore a nail with a lesser radius of curvature (more bend) would not match the anatomy and likely lead to malalignment
Answer 2: Nail with a more distal Herzog curve. The proximal bend for tibial IM nails, known as the Herzog curve, may cause malalignment in proximal tibia fractures due to a phenomenon known as the "wedge effect". Nails with more distal Herzog curves have been implicated in anterior translation of the proximal fragment.
Answer 4: Nailing in a hyperflexed position would cause extension of the proximal fragment due to tension on the extensor mechanism
Answer 5: A more distal and medial entry site would likely lead to further deformity and possible nail cut out through the anterior cortex. A more proximal and lateral entry site is preferred for nailing proximal tibia fractures
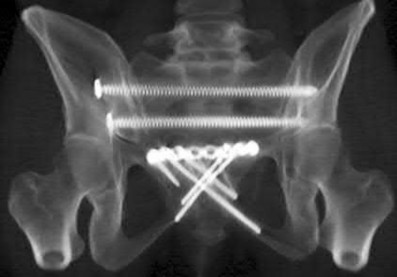
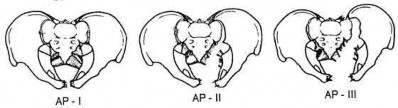
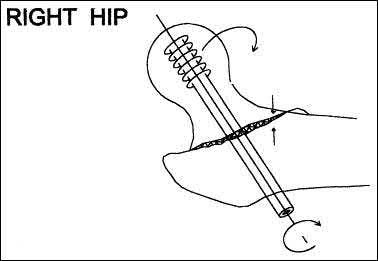
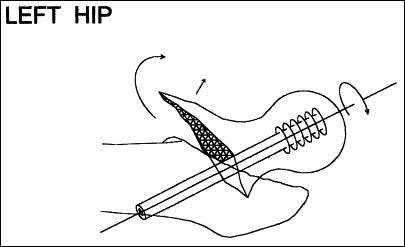
A 32-year-old male sustains an APC-III pelvic ring disruption after a motor vehicle collision. Which of the following imaging techniques best describes the correct utilization of intraoperative flouroscopy for percutaneous iliosacral screw placement across S1?
1) Inlet view helps best guide superior-inferior orientation
2) AP pelvis best guides anterior-posterior screw orientation
3) AP pelvis best guides superior-inferior screw orientation
4) Outlet view best guides anterior-posterior screw orientation
5) Outlet view best guides superior-inferior screw orientation
The outlet view best guides superior-inferior screw orientation during percutaneous S1 screw placement. This is due to the relative forward flexion of the sacrum and pelvis due to pelvic incidence. A lateral sacral view and an inlet pelvis view would best guide anterior-posterior screw orientation.
Routt et al did a review of percutaneous techniques of pelvic surgery. Although anterior pelvic external fixation remains the most common form of percutaneous pelvic fixation, iliosacral screws have the advantage of stabilizing pelvic disruptions directly while diminishing operative blood loss and operative time. They stress importance of a thorough knowledge of pelvic osseous anatomy, injury patterns, deformities, and their fluoroscopic correlations for surgical success.
Routt et al also looked at the complications that can result from percutaneous iliosacral screw placement. Complications ranged from inability for adequate imaging due to patient obesity, L5 nerve root injuries, fixation failure, and sacral nonunions. They support quality triplanar fluoroscopic imaging during iliosacral screw insertions to help accurately reduce injured posterior pelvic rings.
Illustration A is an example of an outlet view image status post anterior pelvic ring plating and percutaneous iliosacral screw. This outlet view allows superior S1 neural foramen visualization to help guide screw placement and avoid nerve injury.
Which of the following methods accurately describes the measurement of tip-apex-distance as it relates to placement of a lag screw in the femoral head?
1) Summation of the distance between the end of the screw and the apex of the femoral head on AP and lateral radiographs
2) Distance from the acetabular teardrop to the tip of the screw on an AP radiograph of the hip
3) Multiplication of the distance between the end of the screw and the apex of the femoral head on AP and lateral radiographs
4) Distance from the center of the lesser trochanter to the tip of the screw on an AP hip radiograph
5) Summation of the distance between the tip of the greater trochanter and end of the screw on AP and lateral hip radiographs
Tip-apex distance (TAD) as it relates to a lag screw in the femoral head is the summation of the distance between the end of the screw and the apex of the femoral head on AP and lateral radiographs, corrected for radiographic magnification of the image. This is shown in Illustration A.
TAD is a useful intraoperative indicator of deep and central placement of the lag screw in the femoral head, regardless of whether a nail or a plate is chosen to fix a fracture. A TAD of 25mm as well as with increasing fracture severity. They concluded that TAD is a valuable consideration for intramedullary devices as well.
Illustrations B and C show a lag screw with an excessive TAD, and subsequent failure of fixation.
Incorrect Answers:
Answers 2-5: TAD is defined as the sum of the distance between the end of the lag screw and the apex of the femoral head on the AP and lateral radiographs, corrected for radiographic magnification of the image.
A 25-year-old man presents one year after undergoing open reduction and internal fixation of the fracture seen in Figure A. Current radiographs demonstrate a united fracture with no evidence of ostenecrosis, subtalar or tibiotalar arthritis. Physical exam is notable for ambulation on the lateral border of the right foot with hindfoot varus, midfoot supination and diminished subtalar motion compared with the contralateral side. Which of the following is an option for reconstruction of this patient's deformity?
1) Total ankle arthroplasty
2) Lateral calcaneus closing wedge osteotomy
3) Calcaneal neck opening wedge osteotomy
4) Talar neck opening medial wedge osteotomy
5) Triple arthrodesis
The most common position of talar neck malunion is varus and this deformity can lock the subtalar and transverse tarsal joints leading to diminished motion and ultimately subtalar arthrosis. Medial opening wedge osteotomy of the talar neck has been described to restore the anatomy of the talus and preserve hindfoot motion.
Daniels et al performed a biomechanical study of hindfoot motion following medial osteotomy and varus malalignment of the talar neck. The authors found a direct correlation between the degree of varus malalignment and diminished forefoot and subtalar motion, and caution against compressive fixation of the medial talus in the presence of comminution.
Monroe and Manoli present a case report of talar neck malunion and describe their technique for osteotomy of the talar neck with insertion of a tricortical iliac crest bone graft to correct the deformity. They found a significant improvement in the AOFAS ankle-hindfoot score and no evidence of
osteonecrosis with follow-up greater than 4 years.
Huang and Cheng retrospectively review their results with anatomic reconstruction of the talar neck in 9 patients who presented a minimum of four weeks after the initial injury with a malreduced or neglected talar neck fracture. They found favorable outcomes with delayed reconstruction as determined by the AOFAS ankle-hindfoot score at an average follow up of 53 months, however note that six patients subsequently developed radiographic hindfoot arthrosis.
Figure A demonstrates a lateral radiograph of a comminuted talar neck fracture with subluxation of the subtalar joint.
Incorrect Answers:
Answer 1: Total ankle arthroplasty is reserved for patients with end-stage tibiotalar arthritis. This patient has an intact and functional tibiotalar joint Answer 2: Lateral calcaneus closing wedge osteotomy would correct some hindfoot varus, however would not address the talar neck deformity leading to diminished motion.
Answer 3: Calcaneal neck opening wedge osteotomy would exacerbate the patient's deformity
Answer 5: Triple arthrodesis would be not be a viable option in a patient with a preserved tibiotalar and subtalar joint.
Which of the following descriptions is true regarding APC-II (anterior-posterior compression) pelvic injuries as classified by Young and Burgess?
1) Pubic symphysis diastasis, intact anterior sacroiliac ligaments, intact sacrotuberous ligament, intact posterior sacroiliac ligaments
2) Pubic symphysis diastasis, torn anterior sacroiliac ligaments, intact sacrotuberous ligament intact posterior sacroiliac ligaments
3) Pubic symphysis diastasis, intact anterior sacroiliac ligaments, torn sacrotuberous ligament, intact posterior sacroiliac ligaments
4) Pubic symphysis diastasis, torn anterior sacroiliac ligaments, torn sacrotuberous ligament, intact posterior sacroiliac ligaments
5) Pubic symphysis diastasis, intact anterior sacroiliac ligaments, torn sacrotuberous ligament, torn posterior sacroiliac ligaments
APC II injuries are unstable injuries and occur as a result of high-energy trauma. Anatomic structures which are injured or torn include the pubic symphysis, anterior iliosacral ligaments, and the sacrotuberous ligaments. The posterior sacroiliac ligaments are spared in APC-II injuries, and differentiate an APC-II injury from an APC-III injury, in which the posterior ligaments are also torn.
Burgess et al review the classifications of pelvic ring disruptions and their association with mortality. They concluded that APC injuries required more blood replacement and were related to death more often than lateral compression, vertical shear, or combined mechanism pelvic injuries.
Tile studied the anatomy of anterior to posterior pelvic ring injuries. Although the anterior structures, the symphysis pubis and the pubic rami, contribute to 40% to the stiffness of the pelvis, clinical and biomechanical studies have shown that the posterior sacroiliac complex is more important to pelvic-ring stability. The posterior sacroiliac ligamentous complex is more important to pelvic-ring stability than the anterior structures and therefore, the classification of pelvic fractures is based on the stability of the posterior lesion.
Illustration A shows the APC classification.
Which of the following deformities is most likely to occur with dynamic hip screw fixation of unstable left sided standard obliquity hip fractures?
1) Posterior spike displacement of the proximal fragment
2) Anterior spike displacement of the proximal fragment
3) Lateral displacement of the proximal fragment relative to the distal fragment
4) Shortening of the proximal fragment relative to the distal fragment
5) Medial displacement of the proximal fragment in relation to the distal fragment
Left-sided unstable intertrochanteric hip fractures are at increased risk of malreduction compared to unstable right-sided fractures fixed with dynamic hip screws. In left-sided fractures the rotational torque imparted to the proximal head and neck fragment can cause loss of reduction leading to potential failures of fixation. With these left sided injuries, the rotational torque can cause an anterior spike, whereas with right-sided injuries the rotational torque causes compression and reduction of the fracture. In addition, if a nail is used for these injuries and the proximal fracture fragment is not being held by the nail itself, this phenomenon can be seen as well.
Mohan et al conducted a study to assess the effect of clockwise rotational torque onto the fracture configuration in unstable and stable intertrochanteric fractures fixed with a dynamic hip screw construct. They found that 11 out of 30 unstable fractures showed an anterior spike (flexion malreduction) in left-sided fixations due to clockwise torque. This malreduction was not present in right-sided or stable fractures.
Illustrations A and B are images from Mohan et al's study showing the rotational affect on the fracture with placement of a dynamic hip screw.
A 45-year-old male sustains a proximal third tibia fracture as an isolated injury and elects to undergo operative treatment with intramedullary nailing. Post-operative radiographs show excessive procurvatum deformity. Which of the following operative techniques would have helped to best avoid the procurvatum deformity?
1) Tibial nailing with increased knee flexion
2) Lateral blocking screw in the proximal fragment
3) Medial blocking screw in the proximal fragment
4) Anterior blocking screw in the proximal fragment
5) Posterior blocking screw in the proximal fragment
Posterior blocking screws in the proximal tibial segement help to avoid tibial procurvatum deformity and malunion. Proximal third tibia fractures are often times difficult to reduce anatomically due to the tendency for both valgus and flexion deformity at the fracture site. The posterior blocking screw helps to eliminate the tendency for the nail to be too posterior and cause the fracture to flex. Blocking screws should be placed on the concavity of the deformity to minimize the procurvatum and valgus deformities of this fracture pattern.
Krettek et al looked at the importance of using blocking screws during intramedullary nailing of metaphyseal fractures using small diameter nails. They found less procurvatum deformity and malunions associated with using of blocking screws and found no complication with their utilization.
Ricci et al reviewed fractures of the proximal third of the tibial shaft treated with intramedullary nails and blocking screws. Their results supported that blocking screws were effective in maintaining alignment of fractures of the proximal third of the tibial shaft treated by intramedullary nailing.
Hiesterman et al review different reduction techniques to avoid malalignment, including the use of a proper starting point and insertion angle, blocking screws, unicortical plates, and a universal distractor.
Illustration A shows a radiograph utilizing posterior proximal and distal blocking screws to prevent procurvatum deformity.
Incorrect Answers:
Grimshaw and Moed retrospectively reviewed the results of patients with posterior wall acetabular fractures managed nonoperatively after evaluation with dynamic fluoroscopic stress tests. At two year follow up, all had good to excellent Merle d’Aubigne clinical scores for hip function and no evidence of post-traumatic hip arthritis on AP pelvis radiographs.
Tornetta retrospectively reviewed his results managing patients with dynamic fluoroscopic stress examination for acetabular fractures which met radiographic nonoperative criteria. Good-to-excellent clinical results were seen in 91% of patients managed nonoperatively.
Tornetta reviewed management of acetabular fractures and Tornetta and Mostafavi separately reviewed management of hip dislocations. In both
articles, emphasis is placed on dynamic examination of posterior wall fractures as instability has been seen with fractures comprising as little as 15% of the posterior wall.
Illustration A demonstrates two fluoroscopic images from a dynamic stress exam of a patient with a posterior wall fracture. The image obtained in the obturator oblique view clearly demonstrates that the femoral head loses congruency with the acetabular dome.
Incorrect Answers:
Answers 1 & 2: Posterior wall fragment size less than 40% was historically used as an indirect measure of stability, however measurements of fragment size may be unreliable and instability has been seen with fractures much smaller than 40%
: A history of hip dislocation was thought to indicate a more unstable fracture. In the level IV study by Grimshaw and Moed, patients with an associated hip dislocation who were stable under stress exam had no significant difference in outcome with nonoperative management.
Answer 5: The iliac oblique view is used to evaluate the anterior wall and posterior column. Displacement or instability of the posterior wall would not be seen with this view
A 64-year-old woman is thrown off a horse, sustaining the injury shown in Figures A and B. She undergoes surgical fixation as seen in Figures C through E. What is the most commonly reported complication of this procedure?
1) Axillary nerve injury
2) Valgus migration of the fracture
3) Nonunion
4) Hardware failure
5) Screw penetration
The patient in the scenario has a 2-part proximal humerus fracture treated with a locking plate as seen in Figures A-E. The most common complication with the use of this implant is screw penetration. The terms screw cut out and penetration are often used interchangeably in the literature with cut out appearing more frequently in reports regarding intertrochanteric fractures.
Owsley et al retrospectively reviewed 53 proximal humerus fractures treated with locking plates and the same post-operative protocol. The most common complication was screw cut out or penetration, followed by varus displacement. They concluded that 3 and 4-part fractures in patients over 60 years have a higher incidence of failure.
Agudelo et al retrospectively reviewed 153 patients at a level-one trauma center treated with proximal humerus locking plates, investigating modes of failure for the implant. They determined that varus malreduction (head-shaft angle
A 25-year-old male sustained a closed midshaft femur fracture following a motor vehicle collision. He is taken to the operating room for supine intramedullary nail fixation of the fracture. Figure A is a lateral fluoroscopic view of the distal femur taken just prior to distal interlocking screw placement. What change in position (with the Carm stationary) would be expected to produce a perfect lateral view of the interlocking hole?
1) Raising the leg
2) Lowering the leg
3) Internal (or external) rotation of the leg
4) Abduction (or adduction) of the leg
5) Fluoroscopic magnification
Interlocking of intramedullary nails using fluoroscopy requires attention to detail. A true lateral of the intramedullary nail is present when "perfect circle" views of interlocking holes are present. Once perfect circles are obtained, the drill can be advanced parallel to the fluoroscopic beam.
Knowledge of the implications of the appearance of the interlocking holes when "perfect circles" are not present can be helpful in minimizing the number of manipulations and fluoroscopic exposure. Widening of the interlocking hole in the proximal-distal direction (as is seen in this case) signifies the need for an adjustment in the abduction/adduction plane. Similarly, widening of the interlocking hole in the anterior-posterior plane signifies the need for an adjustment in the internal/external rotation plane (Answer 3).
Raising or lowering the leg (Answer A and B) should not have major effects of the appearance of the interlocking hole. Similarly, magnification of the C-arm (Answer D) will not affect the appearance. Internal/external rotation will result in widening in the anterior-posterior plane (as this dimension is currently adequate). Abduction or adduction will result in creating "perfect circles" (Answer 4). The position of the leg may hint to which of these is correct. If further widening occurs in the proximal-distal direction, the opposite maneuver will correct to the proper position.
A 46-year-old male is involved in a motor vehicle accident and suffers a proximal humerus fracture. Operative treatment is recommended, and plate fixation is performed through an extended anterolateral acromial approach. Which of the following structures is at increased risk of injury using this surgical exposure compared to the deltopectoral approach?
1) Musculocutaneous nerve
2) Posterior humeral circumflex artery
3) Axillary nerve
4) Cephalic vein
5) Anterior humeral circumflex artery
The anterolateral acromial approach was developed to allow less invasive treatment of proximal humerus fractures. The plane of the avascular anterior
deltoid raphe is utilized, and the axillary nerve is at particular risk of injury and must be identified and protected. With this approach, anterior dissection near the critical blood supply is avoided, substantial muscle retraction is minimized, and the lateral plating zone is directly accessed.
Gardner et al evaluated 23 patients who had acute displaced fractures of the proximal humerus treated with the anterolateral acromial approach and either a locking plate or an intramedullary nail. At one year post-op, there were no axillary nerve deficits, and they found that the approach allowed direct access to the lateral fracture planes for fracture reduction and plate placement or safe nail and interlocking screw placement.
Gardner et al, in another study, performed cadveric dissection using the extended anterolateral acromial approach and measured multiple parameters regarding the axillary nerve. The nerve was predictably found approximately 35 mm from the prominence of the greater tuberosity.
Morgan et al performed a cadaveric study to describe the anatomic insertion point of the deltoid onto the proximal humerus. They found that the deltoid insertion is long and broad, and that placement of 4.5-mm plate would result in detaching 13.5 mm of its insertional footprint. This would leave half of the insertion still attached to the humerus.
Illustration A shows the position of the axillary nerve in relation to the approach.
Which of the following statements is true regarding brake travel time after surgical treatment of complex lower extremity trauma?
1) Brake travel time is significantly increased until 6 weeks after patient begins weight bearing
2) Return of normal brake travel time takes longer after long bone fracture compared to articular fractures
3) Normal brake travel time correlates with improved short musculoskeletal
functional assessment scores
4) Brake travel time is significantly reduced until 8 weeks after patient begins weight bearing
5) Brake travel time returns to normal when weight bearing begins
Brake travel time (BTT) has been shown to be significantly increased until 6 weeks after initiation of weight bearing in both long bone and articular fractures of the right lower extremity.
Egol et al used a computerized driving simulator to compare BTT in three groups of patients; 1)control group, 2)long bone lower extremity fracture group, 3)lower extremity articular fracture group. They concluded that BTT was significantly increased until 6 weeks after initiation of weight bearing in both long bone and articular fractures of the right lower extremity, and that short musculoskeletal functional assessment scores improved with respect to function and other indexes, but did not correlate with improvement in BTT.
An earlier study by Egol et al looked at total brake time as it related to distance traveled by the automobile before braking at 6, 9, and 12 weeks after operative fixation of a right ankle fracture. When compared with controls, braking time was shown to return to normal by 9 weeks post-operatively, and no significant association was found between the functional scores and this normalization.
Giddins et al provide a review of the literature, the law and the views of the major motor insurers related to driving after injury or operations.
What acetabular component is best appreciated on an obturator oblique radiograph of the pelvis as seen in Figure A?
1) Ilioischial line
2) Posterior column
3) Posterior wall
4) Anterior wall
5) Sacroiliac joint
Letournel and Judet developed a schematic representation of the acetabulum as being contained within asymmetric long anterior and short posterior arms of an inverted “Y”.
On the bony pelvis, the ilioischial component becomes that posterior column and the iliopectineal line becomes the anterior column. The Judet-Letournel classification system is based on this scheme. By careful evaluation of landmarks on a standard AP pelvis radiograph, as well as on 45-degree oblique obturator and iliac views, the extent of injury can be determined accurately.
The AP view usually demonstrates the six fundamental landmarks relatively well as seen in illustration A. The obturator oblique view reveals additional information about the anterior column and posterior wall(see illustration A(B),
B). In an obturator oblique view the x-ray beam is centered on and almost perpendicular to the obturator foramen. The iliac oblique view visualizes the posterior column and anterior wall (illustration A(C), C). This view also shows the best detail of the iliac wing as the radiographic beam is roughly perpendicular to the iliac wing. Inclusion of the opposite hip is essential for evaluation of symmetrical contours that may have slight individual variations
and to evaluate the width of the normal articular cartilage in each view in a pelvic series (AP, Judet's) .
Which of the following fractures seen in Figures A through E would be amenable to fixation with a construct using tension band principles?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
In order for a fracture to be successfully treated with tension band principles the bone must be eccentrically loaded, the construct must be applied on the tensile side, and the opposite cortex must be able to withstand compressive
forces. Of the fractures seen in Figures A-E, the subtrochanteric fracture seen in Figure A best meets the criteria for stabilization according to tension band principles.
Kinast et al retrospectively compared their results with 95 degree blade plate fixation of subtrochanteric fractures utilizing the blade plate as a dynamic tension band. They performed either wide exposure of the fracture site with autogenous bone grafting according to AO technique at the time (group 1), or indirect reduction techniques without bone grafting the medial side as advocated by Mast et al (group 2). The authors found 100% union rates at six months with indirect reduction techniques without bone grafting (group 2), and emphasize the key concepts of preservation of the medial soft tissues and intraoperative pretensioning of the plate.
Illustration A demonstrates the principles of tension band fixation specifically applied to the femur. Within Illustration A, Figure C shows the correct application of a plate along the lateral cortex to resist tensile forces, along with incorrect application of the plate along the medial cortex (Figure D) or in a fracture pattern with an absent opposite cortex (Figure E). Illustration B shows an example of blade plate fixation of a subtrochanteric fracture.
Incorrect Answers:
Answer 2. Figure B demonstrates a comminuted proximal tibia fracture. Although the tibia is eccentrically loaded and an implant applied to anterior cortex could function as a tension band, the posterior comminution would lead to collapse.
Answer 3. Figure C demonstrates a comminuted distal humeral shaft fracture. Again,the comminution prevents application of a tension band construct Answer 4: Figure D shows a valgus impacted proximal humerus fracture.
Eccentric loading is absent for this type of fracture
Answer 5: Figure E demonstrates a comminuted olecranon fracture with extension distal to the coronoid process. Although tension band constructs are commonly used for olecranon fractures, the comminution and distal extension of this fracture would prevent application of a tension band.
Which of the following is an advantage of computer-assisted navigation used to place medullary nail interlocking screws compared to a freehand techinque?
1) Reduced fluoroscopy time
2) More reliable placement of interlocking screws through the nail
3) Reduced procedure time
4) Increased quality of fluoroscopic images
5) Improved accuracy of screw length
Computer-assisted navigation has been shown to reduce radiation exposure for surgeons when performing interlocking of medullary nails compared to freehand technique.
Ricci et al compared two fluoroscopic navigation tracking technologies, optical and electromagnetic versus standard freehand fluoroscopic targeting, in a standardized foam block model for placement of interlocking screws. They found that fluoroscopy time (seconds) and number of fluoroscopy images were significantly less when using the computer-guided systems than for freehand-unguided insertion. Average distance of pin placement from the target in the foam blocks was significantly greater for controls than for each of the navigated systems.
Suhm et al performed a prospective controlled clinical study to compare fluoroscopic guidance with fluoroscopy-based surgical navigation for distal locking of intramedullary implants. The surgical navigation group showed increased procedure time, but equivalent precision with reduced radiation exposure. There was no significant difference in the technical reliability
between both groups.
An 82-year-old nursing home resident falls onto his elbow while rising from a seated position. He has pain and swelling at the elbow without evidence of instability. His radiographs show a comminuted displaced olecranon fracture involving 25% of the articular surface with global osteopenia. Which of the following treatment options has a low risk of complications and a high likelihood of a functional elbow outcome?
1) Cast immobilization in 45 degrees of flexion for 8 weeks
2) Closed reduction and percutaneous pinning
3) ORIF with a tension band construct
4) ORIF with a locking plate
5) Cast immobilization in 90 degrees flexion
The patient in the scenario is a low-demand, elderly patient with a comminuted olecranon fracture. Recent studies have demonstrated good outcomes with
non-operative treatment of olecranon fractures in this patient population.
Hak (jaos'00) reviewed the treatment of olecranon fractures, recommending ORIF for displaced intra-articular fractures, either via tension band wiring or plate osteosynthesis based on fracture pattern and associated ligamentous disruption. For elderly, low-demand, osteoporotic patients, triceps advancement and fragment excision is an option in the case of severely comminuted, osteoporotic patients with a fracture involving
A 47-year-old male presents with a one month history of heel pain after starting marathon training. The heel is tender when squeezed. A foot radiograph is shown in Figure A, and an MRI is obtained which is shown in Figures B and C. What is the most likely diagnosis?
1) Osteomyelitis
2) Acute fracture
3) Subtalar arthritis
4) Achilles tendinitis
5) Stress fracture
The patients history, physical exam, and MRI findings are most consistent with the diagnosis of a stress fracture. Low signal on T1 and increased signal on T2-weighted images is the classic appearance of a stress fracture on magnetic resonance images. Usually the fracture appears as a linear signal band that arises from the cortex of the bone and extends perpendicular to the surface of the bone. Figures A and B show a linear area of enhancement in the posterior aspect of the calcaneus signifying a likely stress reaction from recent overtraining.
Boden et al review the pathogenesis and treatment of stress fractures. With regard to diagnosis, they state that it is primarily clinical, but imaging modalities such as plain radiography, scintigraphy, computed tomography, and magnetic resonance imaging may provide confirmation.
Gehrmann et al review stress fractures of the foot, and state that with regards to calcaneal stress injuries, MRI studies should be obtained for definitive diagnosis when radiographs are negative, and pain persists. With regards to
treatment, they state that these injuries usually heal with activity restrictions, heel-pad inserts, and protected weightbearing for a short period of time.
A 35-year-old right hand dominant man falls from a ladder and sustains the injury seen in Figure A. When discussing the risks and benefits of operative versus nonoperative treatment for his fracture, which of the following is true?
1) No difference in shoulder function
2) Higher risk of nonunion with operative management
3) Higher risk of symptomatic malunion or nonunion with nonoperative management
4) Earlier return to sport with nonoperative management
5) No difference in union rates
Historically, displaced midshaft clavicle fractures, as seen in Figure A, were managed nonoperatively. Recent literature has demonsrated improved outcomes with operative management of these fractures.
Khan et al review current concepts in the management of clavicle fractures. For displaced midshaft clavice fractures, operative treatment seems to result in improved patient and surgeon-based outcomes, decreased rates of malunion and nonunion, and shorter time to union.
Kim and McKee review recent evidence regarding the management of clavicle fractures. For midshaft clavicle fractures, the incidence of nonunion and symptomatic malunion with nonoperative management is higher than
previously believed. They state that risk factors include 100% displacement, comminution, increasing age and female gender.
Incorrect Answers
Answer 1. Recent randomized prospective trials have shown improved short term shoulder function with operative management of displaced midshaft clavicle fractures.
Answer 2. Nonunion rates of 7-15% have been shown with nonoperative management versus 2% with operative fixation
Answer 4. Earlier return to activities has been reported with operative management
Answer 5. As with answer 2, there is a significantly higher rate of nonunion with nonoperative management
Assuming the images represent isolated injuries, which of the following Figures demonstrates a Pipkin II femoral head fracture?
1) Figure A
2) Figure B
3) Figure C
4) Figure D
5) Figure E
Figure D represents a Pipkin II femoral head fracture, which is defined as a fracture which is superior to the fovea. Differentiation between Pipkin I and Pipkin II fractures can be important, as suprafoveal injuries often require surgical fixation. Illustration A demonstrates the Pipkin fracture types.
Droll et al review femoral head fracture evaluation and treatment. They discuss non-operative indications (typically reserved for Pipkin I injuries) which include an anatomic or near anatomic reduction (
A 20-year-old female presents following a motor vehicle collision with the injuries seen in Figures A and B. She was initially hypotensive and tachycardic however she now has stable vital signs following a 2 liter bolus of saline and 2 units of packed red blood cells. Which of the following would indicate that this patient has occult end-organ hypoperfusion and should be further resuscitated prior to definitive fixation?
1) Heart rate of 80 beats per minute
2) Systolic blood pressure of 120 mmHg
3) Base deficit of -1.8 mEq/L
4) Serum lactate of 5 mmol/Liter
5) Urine output of 40ml/hour
Figure A demonstrates an unstable pelvic fracture and subtrochanteric femur fracture and Figure B shows a scapular body and mutliple rib fractures. These high-energy fractures, along with the patient's initial hypotension and tacchycardia indicate a multiply injured patient in shock. Serum markers such as lactate (normal
An 80-year-old female falls and sustains the fracture seen in Figure A. She is treated with an antegrade cephalomedullary nail. Which of the following led to the complication seen in Figure B?
1) Nail with a lesser radius of curvature
2) Nail with a greater radius of curvature
3) Piriformis entry portal
4) Trochanteric entry portal
5) Lateral decubitus patient position
The image in Figure A shows an unstable intertrochanteric fracture and the image in Figure B shows perforation of the anterior cortex of the femur by the intramedullary implant. This complication is due to a mismatch of the curvature of the nail with the anterior bow of the femur, and was likely caused by a nail of a greater radius of curvature (eg, straighter than the femur).
Egol et al measured the radius of curvature for 474 matched cadaveric femurs and found the average anterior radius of curvature to be 120cm (+/- 36cm). In contrast, the radii of curvature for the measured intramedullary nails ranged from 186cm to 300cm, demonstrating that the nails were straighter than the femurs. The authors advocate for a decreased radius of curvature (more curve) for intramedullary nails, especially larger diameter implants designed for fractures about the hip
Ostrum and Levy present a case series of 3 patients with subtrochanteric
fractures who had anterior penetration of the femoral cortex. They state that the mismatch in femoral bow between the bone and the implant is a contributing factor to distal femoral anterior cortex penetration in intramedullary nailing of subtrochanteric fractures.
Simonian et al present 4 iatrogenic femoral neck fractures that occured during a series of 315 femoral nails. The authors attempted to reproduce the iatrogenic fractures with cadaveric femurs and felt that the iatrogenic fractures may be due to a combination of a valgus femoral neck and impingement from the AO insertion jig used at the time.
Harper and Carson examined 14 cadaveric femurs and intramedullary implants at the time. Similar to Egol et al, they found a mismatch between the radius of curvature of the femurs and the intramedullary nails.
Illustration A shows the difference between a lesser and greater radius of curvature. Illustration B demonstrates how to calculate radius of curvature based on an implant with an exaggerated bow. Illustration C shows the anterior bow of a synthetic femoral model compared with several intramedullary implants.
Bridge plating of the olecranon is MOST appropriate in which of the following clinical scenarios?
1) Fixation of an olecranon osteotomy used for distal humerus surgery in a 24-year-old male
2) Simple transverse olecranon fracture in 33-year-old female
3) Comminuted olecranon fracture in 45-year-old male
4) Severely comminuted proximal olecranon fracture in an osteoporotic 91-year-old female
5) Aphophyseal elbow fracture in 6-year-old male
Bridge plating is most appropriately used for fixation of comminuted fractures which are not able to be fixed anatomically. Of the choices listed above, this would be most appropriate in a comminuted fracture in a 45-year-old male. In contrast, literature shows that severely comminuted, osteoporotic low-demand elderly are best treated with olecranon fracture excision and triceps advancement when possible.
Bailey et al looked at the outcome of plate fixation of olecranon fractures. They concluded that plate fixation is effective for displaced olecranon fractures and leads to good functional outcome. There were low incidence of complications, although 20% did have removal of hardware due to irritation.
Hak et al reviewed the fixation options for olecranon fractures. In their review, they state that comminuted olecranon fractures can be treated by limited-contact dynamic-compression plates. They also supported the use of supplemental bone graft to support comminuted depressed articular fragments. Fragment excision and triceps advancement is appropriate in selected cases in which open reduction seems unlikely to be successful, such as in osteoporotic elderly patients with severely comminuted fractures.
A 75-year-old ambulatory male who lives independently presents with the fracture shown in Figure A. Which of the following is true regarding timing of surgical fixation and post-operative mortality?
1) 30 day mortality is decreased if surgery is delayed 4-7 days
2) 1 year mortality is increased if surgery is delayed greater than 4 days
3) Delay of surgery due to treatment of acute medical comorbidities has no effect on post-operative mortality rates
4) 90 day mortality rate is decreased if surgery is delayed greater than 7 days
5) Timing of surgical fixation has no statistically significant affect on postoperative mortality
Figure A shows a displaced femoral neck fracture.
Moran et al studied 2660 elderly patients who underwent surgical treatment of a hip fracture to determine whether a delay in surgery affects postoperative mortality. The 30-day mortality for patients for whom the surgery had been delayed for more than 4 days was 10.7%, compared to 7.3% in those delayed 1-4 days. The group delayed >4 days also had significantly increased mortality at 90 days and 1 year. Patients who had been admitted with an acute medical comorbidity that required treatment prior to the surgery had a 30-day mortality of 17%, which was nearly 2.5 times greater than that for patients without and acute comorbidity. The study concluded that patients with medical comorbidities that delayed surgery had 2.5 times the risk of death within 30 days after the surgery compared with patients without comorbidities. Mortality was not increased when the surgery was delayed up to four days for patients who were otherwise fit for hip fracture surgery, however, a delay of more than four days significantly increased mortality.
Healy et al examined 120 patients who underwent surgical treatment of 186 displaced femoral neck fractures with either internal fixation, hemiarthroplasty, or total hip arthroplasty. Arthroplasty was associated with more independent living, and was more cost-effective than internal fixation. There was no difference in rates of reoperation or mortality, but arthroplasty produced a longer interval to reoperation or death. They concluded that total hip arthroplasty was the best treatment for displaced fractures of the femoral neck in their series.
Illustration A shows a scoring system developed by Rogmark et al to aid in decision making.
A 35-year-old male suffers an anterior column acetabular fracture during a motor vehicle collision, and subsequently undergoes percutaneous acetabular fixation. Intraoperatively, fluoroscopy is positioned to obtain an obturator oblique-inlet view while placing a supraacetabular screw. Which of the following screw relationships is best evaluated with this view?
1) Intraarticular penetration of the screw
2) Position of the screw cephalad to the sciatic notch
3) Screw starting point at the anterior inferior iliac spine
4) Screw starting point at the gluteal pillar
5) Screw position between the inner and outer tables of the ilium
The obturator oblique-inlet view, as seen in Illustration A, best demonstrates the position of a supra-acetabular screw or pin relative to the tables of the ilium.
Starr et al review their initial results and technique of closed or limited open reduction and percutaneous fixation of acetabular fractures. They defined two groups of patients who may benefit from this technique; elderly patients with multiple comorbidities to facilitate early mobilization and restore hip morphology, and young patients with elementary fracture patterns and multiple associated injuries.
Starr et al describe their operative technique and outcomes for a case series of 3 patients using percutaneous acetabular fixation to augment open reduction of acetabular fractures. The authors state that, for placement of an anterior colum ramus screw, an iliac oblique-inlet (not obturator oblique-inlet) will ensure that the screw is within the medullary canal of the ramus and does not exit anterior or posterior.
Gardner and Nork describe a technique for placement of a large femoral distractor in the supra-acetabular region to compress displaced posterior pelvic ring injuries. They note that the obturator oblique-inlet view is necessary to view the entire length of the pin as well as to ensure that pin remains in bone.
Incorrect answers:
Answer 1: Relationshiop of the screw to the acetabulum is best evaluated with the obturator oblique-outlet view as well as the iliac oblique view
Answer 2: The iliac oblique view is used to ensure the trajectory of the screw is superior to the sciatic notch
Answer 3: The Obturator oblique-outlet view, otherwise known as the "teepee" or "tear drop" view, is used to identify the start for supra-acetabular implant placement
Answer 4: The gluteal pillar is not utilized as a start point when placing supraacetabular fixation, and the obturator oblique-inlet view would not be ideal to visualize this region of the pelvis
A 74-year-old man falls, sustaining the injury shown in Figures A through C. In surgical planning, what is the best surgical approach to treat this injury?
1) Kocher-Langenbeck
2) Watson-Jones
3) Extended iliofemoral
4) Ilioinguinal
5) Hardinge
Figures A through C depict and AP pelvis and Judet views of a T-type fracture of the right acetabulum. The ilioinguinal approach provides access to the anterior wall and anterior column for fracture fixation, in addition to allowing fixation of the nondisplaced posterior transverse fracture line. The lateral femoral cutaneous nerve (LFCN) is at risk in the superficial part of the dissection. Another option for the approach would be the modified Stoppa, which would also allow excellent access to the anterior column as well as the internal aspect of the iliac wing and quadrilateral plate.
Illustration A shows the five basic and 5 associated acetabular fractures. Incorrect Answers:
Answer 1. Kocher-Langenbeck: access for posterior wall and column fractures
Answer 2. Watson-Jones: anterolateral approach best for the hip, not the anterior column of the acetabulum.
Answer 3. Extended iliofemoral: visualization for both column fractures Answer 5. Hardinge approach: lateral approach for THA
A 28-year-old female is struck by a motor vehicle while crossing the street and suffers the injury seen in Figure A. What technical adjunct could have prevented the operative complication seen in Figure B?
1) Nail of a lesser radius of curvature
2) Nail with a more distal Herzog curve
3) Application of an anterior unicortical plate
4) Nailing while in a hyperflexed position
5) A more distal and medial nail entry site
The patient has a proximal tibia fracture that has been malreduced in procurvatum with anterior translation of the proximal fragment as seen in Figures A and B. Intramedullary nailing of proximal tibia fractures may result in malalignment such as valgus, procurvatum and anterior translation of the proximal fragment.Techniques such as anterior unicortical plating have been described to maintain reduction while placing a locked intramedullary implant.
Nork et al retrospectively review their results using several different intraoperative adjuncts to maintain reduction while nailing proximal tibia fractures including anterior unicortical plates and femoral distractors. They report that, despite high rates of segmental comminution (59.5%) and open fractures (35.1%), acceptable alignment and primary union were achieved in more than 90% of patients.
Dunbar et al describe their technique for application of a provisional unicortical plate through the traumatic wound to maintain reduction during intramedullary nailing of Gustilo-Anderson Type III open tibia fractures. The authors advocate that further soft tissue stripping during plate placement should be avoided, and found excellent results in terms of coronal and sagittal plane alignment for fractures treated with this technique.
Matthews et al review their experience with unicortical plating to maintain reduction during intramedullary nailing of tibia fractures. Similar to the other referenced studies, the authors found the technique assisted with maintaining reduction intraoperatively.
Illustrations A and B demonstrate maintenance of reduction of a proximal tibia fracture using an anterior unicortical plate as a reduction tool during intramedullary nailing.
Incorrect Answers:
Answer 1: Nail of a lesser radius of curvature. Unlike femoral nails, tibial nails are straight to match the coronal/sagittal axis of the tibia and therefore a nail with a lesser radius of curvature (more bend) would not match the anatomy and likely lead to malalignment
Answer 2: Nail with a more distal Herzog curve. The proximal bend for tibial IM nails, known as the Herzog curve, may cause malalignment in proximal tibia fractures due to a phenomenon known as the "wedge effect". Nails with more distal Herzog curves have been implicated in anterior translation of the proximal fragment.
Answer 4: Nailing in a hyperflexed position would cause extension of the proximal fragment due to tension on the extensor mechanism
Answer 5: A more distal and medial entry site would likely lead to further deformity and possible nail cut out through the anterior cortex. A more proximal and lateral entry site is preferred for nailing proximal tibia fractures
A 32-year-old male sustains an APC-III pelvic ring disruption after a motor vehicle collision. Which of the following imaging techniques best describes the correct utilization of intraoperative flouroscopy for percutaneous iliosacral screw placement across S1?
1) Inlet view helps best guide superior-inferior orientation
2) AP pelvis best guides anterior-posterior screw orientation
3) AP pelvis best guides superior-inferior screw orientation
4) Outlet view best guides anterior-posterior screw orientation
5) Outlet view best guides superior-inferior screw orientation
The outlet view best guides superior-inferior screw orientation during percutaneous S1 screw placement. This is due to the relative forward flexion of the sacrum and pelvis due to pelvic incidence. A lateral sacral view and an inlet pelvis view would best guide anterior-posterior screw orientation.
Routt et al did a review of percutaneous techniques of pelvic surgery. Although anterior pelvic external fixation remains the most common form of percutaneous pelvic fixation, iliosacral screws have the advantage of stabilizing pelvic disruptions directly while diminishing operative blood loss and operative time. They stress importance of a thorough knowledge of pelvic osseous anatomy, injury patterns, deformities, and their fluoroscopic correlations for surgical success.
Routt et al also looked at the complications that can result from percutaneous iliosacral screw placement. Complications ranged from inability for adequate imaging due to patient obesity, L5 nerve root injuries, fixation failure, and sacral nonunions. They support quality triplanar fluoroscopic imaging during iliosacral screw insertions to help accurately reduce injured posterior pelvic rings.
Illustration A is an example of an outlet view image status post anterior pelvic ring plating and percutaneous iliosacral screw. This outlet view allows superior S1 neural foramen visualization to help guide screw placement and avoid nerve injury.
Which of the following methods accurately describes the measurement of tip-apex-distance as it relates to placement of a lag screw in the femoral head?
1) Summation of the distance between the end of the screw and the apex of the femoral head on AP and lateral radiographs
2) Distance from the acetabular teardrop to the tip of the screw on an AP radiograph of the hip
3) Multiplication of the distance between the end of the screw and the apex of the femoral head on AP and lateral radiographs
4) Distance from the center of the lesser trochanter to the tip of the screw on an AP hip radiograph
5) Summation of the distance between the tip of the greater trochanter and end of the screw on AP and lateral hip radiographs
Tip-apex distance (TAD) as it relates to a lag screw in the femoral head is the summation of the distance between the end of the screw and the apex of the femoral head on AP and lateral radiographs, corrected for radiographic magnification of the image. This is shown in Illustration A.
TAD is a useful intraoperative indicator of deep and central placement of the lag screw in the femoral head, regardless of whether a nail or a plate is chosen to fix a fracture. A TAD of 25mm as well as with increasing fracture severity. They concluded that TAD is a valuable consideration for intramedullary devices as well.
Illustrations B and C show a lag screw with an excessive TAD, and subsequent failure of fixation.
Incorrect Answers:
Answers 2-5: TAD is defined as the sum of the distance between the end of the lag screw and the apex of the femoral head on the AP and lateral radiographs, corrected for radiographic magnification of the image.
A 25-year-old man presents one year after undergoing open reduction and internal fixation of the fracture seen in Figure A. Current radiographs demonstrate a united fracture with no evidence of ostenecrosis, subtalar or tibiotalar arthritis. Physical exam is notable for ambulation on the lateral border of the right foot with hindfoot varus, midfoot supination and diminished subtalar motion compared with the contralateral side. Which of the following is an option for reconstruction of this patient's deformity?
1) Total ankle arthroplasty
2) Lateral calcaneus closing wedge osteotomy
3) Calcaneal neck opening wedge osteotomy
4) Talar neck opening medial wedge osteotomy
5) Triple arthrodesis
The most common position of talar neck malunion is varus and this deformity can lock the subtalar and transverse tarsal joints leading to diminished motion and ultimately subtalar arthrosis. Medial opening wedge osteotomy of the talar neck has been described to restore the anatomy of the talus and preserve hindfoot motion.
Daniels et al performed a biomechanical study of hindfoot motion following medial osteotomy and varus malalignment of the talar neck. The authors found a direct correlation between the degree of varus malalignment and diminished forefoot and subtalar motion, and caution against compressive fixation of the medial talus in the presence of comminution.
Monroe and Manoli present a case report of talar neck malunion and describe their technique for osteotomy of the talar neck with insertion of a tricortical iliac crest bone graft to correct the deformity. They found a significant improvement in the AOFAS ankle-hindfoot score and no evidence of
osteonecrosis with follow-up greater than 4 years.
Huang and Cheng retrospectively review their results with anatomic reconstruction of the talar neck in 9 patients who presented a minimum of four weeks after the initial injury with a malreduced or neglected talar neck fracture. They found favorable outcomes with delayed reconstruction as determined by the AOFAS ankle-hindfoot score at an average follow up of 53 months, however note that six patients subsequently developed radiographic hindfoot arthrosis.
Figure A demonstrates a lateral radiograph of a comminuted talar neck fracture with subluxation of the subtalar joint.
Incorrect Answers:
Answer 1: Total ankle arthroplasty is reserved for patients with end-stage tibiotalar arthritis. This patient has an intact and functional tibiotalar joint Answer 2: Lateral calcaneus closing wedge osteotomy would correct some hindfoot varus, however would not address the talar neck deformity leading to diminished motion.
Answer 3: Calcaneal neck opening wedge osteotomy would exacerbate the patient's deformity
Answer 5: Triple arthrodesis would be not be a viable option in a patient with a preserved tibiotalar and subtalar joint.
Which of the following descriptions is true regarding APC-II (anterior-posterior compression) pelvic injuries as classified by Young and Burgess?
1) Pubic symphysis diastasis, intact anterior sacroiliac ligaments, intact sacrotuberous ligament, intact posterior sacroiliac ligaments
2) Pubic symphysis diastasis, torn anterior sacroiliac ligaments, intact sacrotuberous ligament intact posterior sacroiliac ligaments
3) Pubic symphysis diastasis, intact anterior sacroiliac ligaments, torn sacrotuberous ligament, intact posterior sacroiliac ligaments
4) Pubic symphysis diastasis, torn anterior sacroiliac ligaments, torn sacrotuberous ligament, intact posterior sacroiliac ligaments
5) Pubic symphysis diastasis, intact anterior sacroiliac ligaments, torn sacrotuberous ligament, torn posterior sacroiliac ligaments
APC II injuries are unstable injuries and occur as a result of high-energy trauma. Anatomic structures which are injured or torn include the pubic symphysis, anterior iliosacral ligaments, and the sacrotuberous ligaments. The posterior sacroiliac ligaments are spared in APC-II injuries, and differentiate an APC-II injury from an APC-III injury, in which the posterior ligaments are also torn.
Burgess et al review the classifications of pelvic ring disruptions and their association with mortality. They concluded that APC injuries required more blood replacement and were related to death more often than lateral compression, vertical shear, or combined mechanism pelvic injuries.
Tile studied the anatomy of anterior to posterior pelvic ring injuries. Although the anterior structures, the symphysis pubis and the pubic rami, contribute to 40% to the stiffness of the pelvis, clinical and biomechanical studies have shown that the posterior sacroiliac complex is more important to pelvic-ring stability. The posterior sacroiliac ligamentous complex is more important to pelvic-ring stability than the anterior structures and therefore, the classification of pelvic fractures is based on the stability of the posterior lesion.
Illustration A shows the APC classification.
Which of the following deformities is most likely to occur with dynamic hip screw fixation of unstable left sided standard obliquity hip fractures?
1) Posterior spike displacement of the proximal fragment
2) Anterior spike displacement of the proximal fragment
3) Lateral displacement of the proximal fragment relative to the distal fragment
4) Shortening of the proximal fragment relative to the distal fragment
5) Medial displacement of the proximal fragment in relation to the distal fragment
Left-sided unstable intertrochanteric hip fractures are at increased risk of malreduction compared to unstable right-sided fractures fixed with dynamic hip screws. In left-sided fractures the rotational torque imparted to the proximal head and neck fragment can cause loss of reduction leading to potential failures of fixation. With these left sided injuries, the rotational torque can cause an anterior spike, whereas with right-sided injuries the rotational torque causes compression and reduction of the fracture. In addition, if a nail is used for these injuries and the proximal fracture fragment is not being held by the nail itself, this phenomenon can be seen as well.
Mohan et al conducted a study to assess the effect of clockwise rotational torque onto the fracture configuration in unstable and stable intertrochanteric fractures fixed with a dynamic hip screw construct. They found that 11 out of 30 unstable fractures showed an anterior spike (flexion malreduction) in left-sided fixations due to clockwise torque. This malreduction was not present in right-sided or stable fractures.
Illustrations A and B are images from Mohan et al's study showing the rotational affect on the fracture with placement of a dynamic hip screw.
A 45-year-old male sustains a proximal third tibia fracture as an isolated injury and elects to undergo operative treatment with intramedullary nailing. Post-operative radiographs show excessive procurvatum deformity. Which of the following operative techniques would have helped to best avoid the procurvatum deformity?
1) Tibial nailing with increased knee flexion
2) Lateral blocking screw in the proximal fragment
3) Medial blocking screw in the proximal fragment
4) Anterior blocking screw in the proximal fragment
5) Posterior blocking screw in the proximal fragment
Posterior blocking screws in the proximal tibial segement help to avoid tibial procurvatum deformity and malunion. Proximal third tibia fractures are often times difficult to reduce anatomically due to the tendency for both valgus and flexion deformity at the fracture site. The posterior blocking screw helps to eliminate the tendency for the nail to be too posterior and cause the fracture to flex. Blocking screws should be placed on the concavity of the deformity to minimize the procurvatum and valgus deformities of this fracture pattern.
Krettek et al looked at the importance of using blocking screws during intramedullary nailing of metaphyseal fractures using small diameter nails. They found less procurvatum deformity and malunions associated with using of blocking screws and found no complication with their utilization.
Ricci et al reviewed fractures of the proximal third of the tibial shaft treated with intramedullary nails and blocking screws. Their results supported that blocking screws were effective in maintaining alignment of fractures of the proximal third of the tibial shaft treated by intramedullary nailing.
Hiesterman et al review different reduction techniques to avoid malalignment, including the use of a proper starting point and insertion angle, blocking screws, unicortical plates, and a universal distractor.
Illustration A shows a radiograph utilizing posterior proximal and distal blocking screws to prevent procurvatum deformity.
Incorrect Answers:
QUESTION 26 OF 50
Which of the following factors is considered to be the strongest predictor of outcome following arthroscopic partial meniscectomy?
1
Patient age
2
Patient body mass index
3
Amount of meniscal resection
4
Location of the meniscal tear
5
Modified Outerbridge cartilage score
DISCUSSION: In a recent evidence-based review of the literature, the only consistent factor predicting outcome after arthroscopic partial meniscectomy was the extent of osteoarthritis as classified by the modified Outerbridge cartilage score at the time of surgery. All other factors listed (ie, location of meniscal tear, patient age, patient BMI, and amount of meniscal resection) were shown to not predict outcome following partial meniscectomy. While not provided as an
hoice, female gender was shown to be a predictor for slower recovery in the short term. The Preferred Respon # 114 is 5.
QUESTION 27 OF 50
Figures 1 and 2 show the radiographs obtained from a 56-year-old man who has been experiencing progressive wrist pain since he felt a pop while throwing a 25-pound bag over his shoulder 6 months ago. Failure to address the injury surgically might lead to progressive arthritic changes in what order?



1
Lunocapitate, radioscaphoid, radial styloid, radiolunate
2
Radioscaphoid, radial styloid, lunocapitate, radiolunate
3
Radial styloid, radioscaphoid, lunocapitate, radiolunate
4
Radial styloid, radioscaphoid, radiolunate, lunocapitate
This patient demonstrates scapholunate dissociation with an associated dorsal intercalated segment instability deformity. Chronic scapholunate ligament tears lead to scapholunate advanced collapse (SLAC) wrist. Watson and Ballet describe SLAC wrist as having a predictable progression of arthritic changes, starting at the radial styloid, progressing to the radioscaphoid joint, and advancing to the lunocapitate joint. Some authors have described the radiolunate joint as being affected in very late-stage _SLAC wrist._
QUESTION 28 OF 50
A 12-year-old child with sickle cell anemia has had pain in the distal femur for 1 day, a temperature of 101.5° F, and a white blood count of 14,000/mm3 . Plain films are unremarkable. Recommended treatment includes:
1
Magnetic resonance imaging of the area
2
Bone scan
3
Needle biopsy of the distal femur
4
Indium labeled white cell scan
5
Intravenous hydration and analgesia
Because the odds are greatly in favor of a noninfectious process, it is appropriate to treat empirically with rehydration and analgesia.
Magnetic resonance imaging would not distinguish between infection and vaso-occlusive crisis. Bone scan would not distinguish between infection and vaso-occlusive crisis.
Needle biopsy is not necessary at this stage since the odds are high (greater than 95%) that the process is not infection. White blood cell scan is not able to distinguish between infection and vaso-occlusive crisis.
Magnetic resonance imaging would not distinguish between infection and vaso-occlusive crisis. Bone scan would not distinguish between infection and vaso-occlusive crisis.
Needle biopsy is not necessary at this stage since the odds are high (greater than 95%) that the process is not infection. White blood cell scan is not able to distinguish between infection and vaso-occlusive crisis.
QUESTION 29 OF 50
A 25-year old right-hand dominant professional baseball pitcher complains of posteromedial right elbow pain that is worsened by throwing. He also reports occasional paresthesias in his small and ring finger after lengthy bullpen sessions. On examination, he is tender along the medial olecranon and complains of pain when extending the elbow >/- 20° of extension. He has negative valgus stress, moving valgus stress, and milking maneuver tests. He is stable to varus stress, chair rise, and lateral pivot shift tests. Radiographs reveal a small osteophyte along the posteromedial border of the olecranon. What is the most likely diagnosis?
1
Valgus extension overload
2
Varus posteromedial rotatory instability (VPMRI)
3
Valgus posterolateral rotatory instability (VPLRI)
4
Olecranon bursitis
The patient has valgus extension overload. This is a spectrum of pathologies, often seen in pitchers, that begins with posteromedial impingement between the medial olecranon and posterior trochlea during forceful elbow extension. As a result, a medial olecranon osteophyte is typically the first notable imaging finding. As pathology increases, there can be progressive damage to the medial collateral ligament (MCL), degeneration of the radiocapitellar articulation, and neuritis of the ulnar nerve. VPMRI is often associated with a large anteromedial coronoid fracture and posterior band MCL rupture. VPLRI occurs when the lateral collateral ligament complex is ruptured. Olecranon bursitis presents with focal swelling or a fluid collection over the posterior aspect of the olecranon.
QUESTION 30 OF 50
A 75-year-old man presents with complaints of shoulder pain, bruising, and weakness following a fall onto his outstretched hand. He underwent an uncomplicated anatomic total shoulder arthroplasty 5 years prior with good range of motion and strength. His current radiographs are shown in Figures 1 and
1
What is the most appropriate next step to restore this patient’s function?
43
2
Rotator cuff repair
3
Revision to reverse total shoulder arthroplasty
4
Physical therapy
5
Latissimus dorsi transfer
The patient's radiographs demonstrate humeral head elevation and anterior translation, suggesting a massive traumatic rotator cuff tear. In this setting, a rotator cuff repair is unlikely to be successful, and a revision to reverse total shoulder arthroplasty is indicated. A latissimus dorsi transfer can address only a portion of the patient's rotator cuff deficiency. Physical therapy may result in some degree of improvement, but this cannot address the joint instability and malalignment. If the shoulder remains in its current position, progressive glenoid loosening would be expected due to the “rocking horse” phenomenon resulting in eccentric glenoid edge loading. Shields and Wiater compared conversion of an anatomic total shoulder to a reverse total shoulder for rotator cuff deficiency with primary reverse total shoulder arthroplasty and found similar American Shoulder and Elbow Surgeons Standardized Shoulder Assessment and visual analog scale pain scores at 2-year follow-up.
QUESTION 31 OF 50
SHOULDER AND ELBOW MCQS FREE 2021





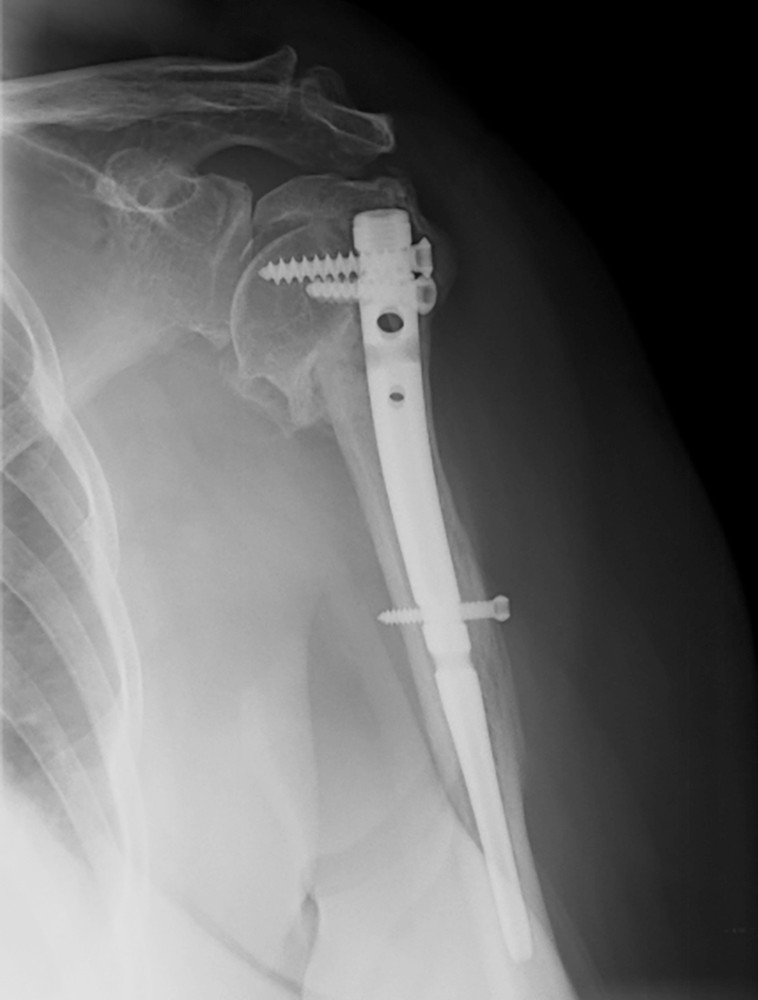


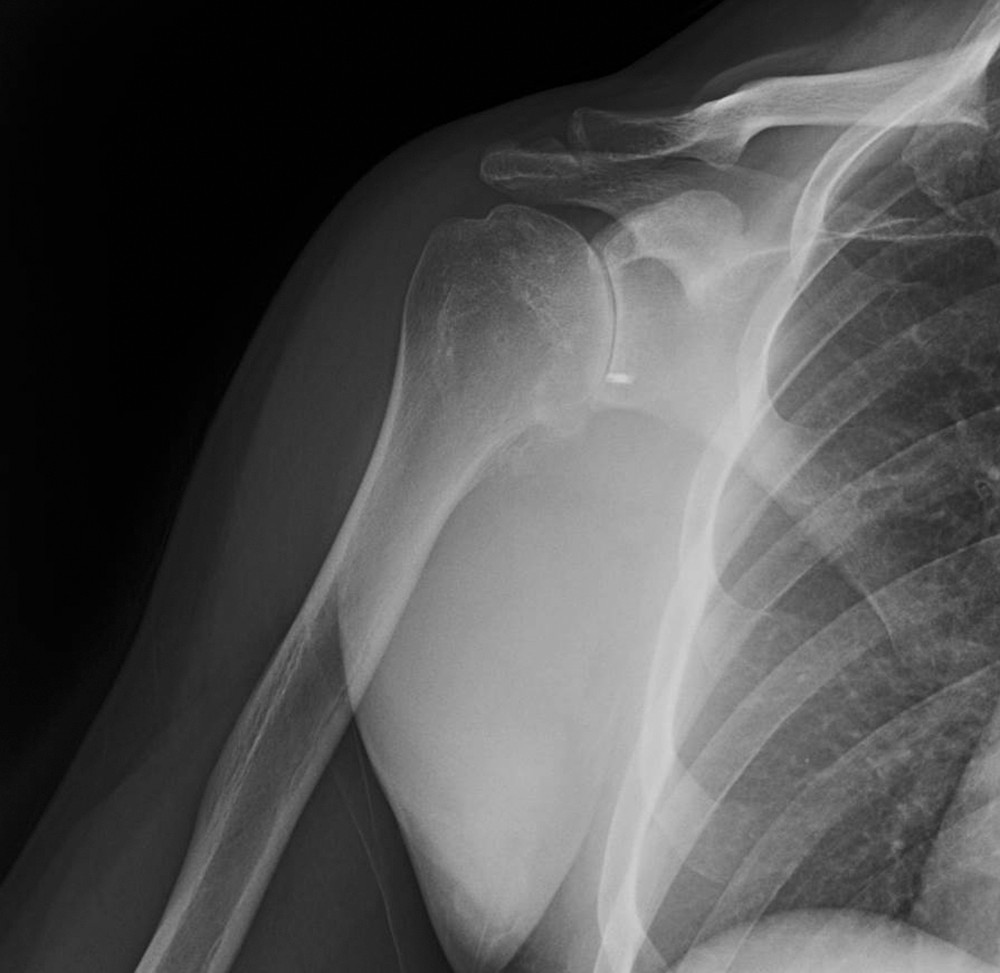



1
Figures 1 and 2 show the current radiographs of a 25-year-old skier who presents 2 weeks after undergoing open reduction and internal fixation (ORIF) of a right elbow fracture dislocation. On examination, he has a well-healed posterior incision without any signs of infection. He expresses mild elbow pain and has limited active and passive range of motion. Neurovascular exam is intact. What is the best next step in treatment?

2
Initiate physical therapy focusing on active-assisted range of motion
3
Revision ORIF
4
Place a hinged external fixator
5
Revision to a total elbow arthroplasty
The patient sustained a complex injury pattern that included a comminuted fracture of the coronoid. This must be identified and distinguished from a simpler olecranon fracture at the time of the initial repair. Loss of the coronoid buttress can lead to residual elbow instability if not addressed. In this situation, the bony stabilization has failed, and an attempt should be made to revise it, with particular attention to stabilizing the coronoid. As in all complex elbow injuries, the status of the collateral ligaments should be assessed, and repaired/reconstructed as needed.
A spanning external fixator can be considered as a secondary option when adequate fixation and stability cannot be achieved, but that would not address the articular incongruity currently present. Total elbow arthroplasty is not indicated due to the patient's age and injury pattern, and physical therapy is unlikely to be successful without a congruently reduced joint.
2
2- When a patient has recurrent anterior shoulder instability, a bony glenoid reconstructive procedure should be considered in which clinical setting?
A. Associated humeral avulsion of the glenohumeral ligament (HAGL)lesion
B. Non-engaging Hill-Sachs lesion
C. Glenoid bone loss of at least 25%
D. Anterior labral periosteal sleeve avulsion (ALPSA) lesion
HAGL lesions may initially be treated without surgery. Recurrent instability in the setting of a HAGL lesion may be treated with a soft-tissue repair. A non- engaging or off-track Hill-Sachs lesion may be treated with an anterior soft- tissue (Bankart) repair. An on-track or engaging Hill-Sachs lesion may be treated by addressing any bony glenoid injury or anterior labral tear plus Hill- Sachs remplissage. An ALPSA lesion may be treated with a soft-tissue procedure, unless it is associated with a glenoid bony defect >25%. A glenoid bony defect >25% is associated with substantially higher risk of recurrent instability and consideration for bony glenoid reconstruction is advised. Consideration of bone augmentation procedures with less severe glenoid bone loss may be considered in higher risk patients, such as collision athletes.
Correct answer : C
3- A 61-year-old right-hand dominant woman falls down the stairs, resulting in a left anteroinferior shoulder dislocation and non- comminuted greater tuberosity fracture. A closed glenohumeral reduction with intravenous sedation is performed in the emergency department. After reduction, the greater tuberosity fragment remains displaced by 2 mm. What is the most appropriate treatment?
A. Open reduction internal fixation with transosseous sutures
B. Arthroscopic fixation using a suture bridge technique
C. Nonsurgical treatment with early passive range of motion
D. Nonsurgical treatment with sling immobilization for 8 weeks
Greater tuberosity fractures and rotator cuff tears associated with a traumatic dislocation are more commonly seen in women >60 years. Greater tuberosity fractures that are displaced <5 mm in the general population and <3 mm in laborers and professional athletes can be treated successfully without surgery. Early passive range of motion is important to avoid stiffness.
Correct answer : C
4- Residual angulation <30° of the humeral shaft after nonoperative fracture treatment has been shown to have what effect on patient reported outcomes?
A. Angulation in the coronal plane has more effect on functional outcomes than in the sagittal plane.
B. Increased angulation corresponds with worse functional outcomes.
C. Angulation >5° in any plane results in an unacceptable cosmetic result.
D. Residual angulation has no correlation with functional outcomes.
Acceptable angulation of humeral shaft fractures for nonoperative treatment is quite generous due to compensatory motion at the shoulder joint. Traditionally, 20° of anterior-posterior and 30° of varus-valgus angulation is acceptable. Indications for surgery have included angulation outside of this range, open fractures, brachial plexus injury, polytrauma, or other factors that preclude functional bracing. Increased amounts of angulation at the conclusion of healing can result in cosmetic dissatisfaction, but this has not been correlated with any specific degree of angulation, as patient factors are a strong influencer. Increased angulation has not been shown to affect functional outcomes within the angulation range previously described.
Correct answer : D
5- A 65-year-old man who underwent an uncomplicated reverse total shoulder arthroplasty (rTSA) to treat rotator cuff arthropathy 2 years ago has a routine follow-up visit in your clinic. A radiograph is shown in Figure 1. He denies shoulder pain, dysfunction, or constitutional symptoms, and his clinical examination findings are benign. Based upon the present radiologic evaluation, what is the next most appropriate step?
A. Revision rTSA
B. Conversion to hemiarthroplasty
C. Continued observation
D. Infection work-up with screening labs and joint aspiration
The patient's radiographs show scapular notching, which is a common complication of reverse shoulder arthroplasty caused by repeated contact between the humeral component and/or medial humerus and the inferior pillar of the scapular neck. Despite this radiographic finding, the patient is doing well clinically and is completely asymptomatic. Therefore, continued observation is appropriate.
Notching can result in creation of particulate debris, causing osteolysis and ultimate implant failure. Therefore, this patient should be monitored with serial radiographs. The overall incidence of notching has been reported to be between 51% and 96%. This nearly ubiquitous finding has been attributed to implant positioning, altered glenoid and humeral anatomy, and duration of implantation. Recent studies have identified that increased lateral offset, increased glenosphere size, and inferior positioning of the base plate can reduce the incidence of scapular notching.
Correct answer : C
6- A healthy 65-year-old woman undergoes anatomic total shoulder arthroplasty to address osteoarthritis (OA). The surgery is uncomplicated. What is the most common indication for future revision?
A. Deep infection
B. Periprosthetic fracture
C. Glenoid component loosening
D. Rotator cuff tear
The most common reason for revision surgery following unconstrained shoulder arthroplasty for glenohumeral OA is loosening of the implant. In most studies that distinguish glenoid from humeral loosening, the glenoid component is more frequently affected. Comprehensive systematic reviews have found that radiographic glenoid loosening can comprise nearly 30% to
40% of all complications following shoulder arthroplasty for non-inflammatory arthritis. Infections, periprosthetic fractures, and rotator cuff tears are uncommon. In the population-based study by Matsen and associates, 10% of the revisions were performed for loosening versus 7% for infection and 7% for rotator cuff tearing.
Correct answer : C
7- An 18-year-old male football player dislocated his elbow during a game. A post-reduction MRI scan is shown in Figure 1. The injury is initially treated non-operatively, but the patient continues to note subjective instability and pain when attempting to push up from a chair. Surgical intervention is planned for repair/reconstruction. What guidance should be provided to the patient and therapist in the early postoperative period?
A. No range-of-motion exercises until 6 weeks postoperative
B. Begin immediate strengthening
C. Avoid valgus stress to elbow
D. Avoid shoulder abduction
The MRI scan shows injuries to both the medial and lateral ligamentous structures of the elbow, with significant widening of the radiocapitellar joint space. The patient’s ongoing symptoms are consistent with posterolateral rotatory instability related to lateral collateral ligament insufficiency. After surgical repair versus reconstruction of the
lateral collateral ligament, it is important to avoid varus stress to the elbow, which can result in failure or loosening of the lateral structures. During shoulder abduction, gravity applies a varus stress to the elbow, and it should be avoided.
Limiting range of motion for the first 6 weeks would result in significant elbow stiffness. Valgus stress should be avoided in the setting of a medial collateral ligament repair or reconstruction. Strengthening is usually delayed until appropriate soft-tissue healing has been achieved.
Correct answer : D
8- When performing reverse shoulder arthroplasty, what factor leads to an increase in the complication indicated by the black arrow in Figure 1?
A. Superior baseplate position on the glenoid
B. Lateralized position of the glenosphere
C. Shorter humeral stem length
D. Larger glenosphere diameter
The image shows scapular notching. Inferior scapular notching is caused by direct mechanical impingement of the humeral bone or humeral prosthesis on the inferior scapular neck. Particulate polyethylene debris may aggravate inferior notching and lead to osteolysis. Impingement-free range of motion (ROM) in all planes is
imperative. Gutiérrez and associates analyzed the factors that affect impingement of the humerus or humeral component against the scapula and the resultant effect on ROM. Varus humeral neck-shaft angle was found to be the most important factor in preventing notching, followed by inferior positioning of the glenosphere, lateral offset of the glenosphere, and increasing size of the glenosphere. Humeral stem length and cementation have not been shown to have an impact on notching.
Correct answer : A
9- A 27-year-old man presents to the emergency department after a fall from a motorcycle. Imaging reveals a displaced glenoid neck fracture, and surgical intervention is planned through a modified Judet approach. What internervous plane is encountered between the infraspinatus and teres minor muscles?
A. Long thoracic nerve and axillary nerve
B. Suprascapular nerve and axillary nerve
C. Suprascapular nerve and long thoracic nerve
D. Spinal accessory nerve and axillary nerve
Surgical indications for scapular fractures are debatable in the literature. Historical indications for extra-articular fractures of the glenoid neck have ranged from 10-25 mm of medial displacement, 25-40⁰ of angular deformity of the glenoid, and a glenopolar angle cut-off of 20-30⁰. While the Judet approach can offer access to the entire scapular body, a modified Judet approach is a more limited approach that allows access to the glenoid neck in the interval
7
between the infraspinatus and teres minor. The infraspinatus is innervated by the suprascapular nerve, whereas the teres minor is innervated by the axillary nerve. The long thoracic nerve innervates the serratus anterior muscle. The spinal accessory nerve innervates the sternocleidomastoid and trapezius muscles.
Correct answer : B
10- What complication following total elbow arthroplasty poses more risk for a 60-year-old man with osteoarthritis than for a man of the same age with rheumatoid arthritis?
A. Aseptic loosening of a linked implant
B. Instability of an unlinked implant
C. Triceps rupture
D. Wound dehiscence
Patients with primary elbow osteoarthritis tend to be active and are often involved in manual occupations that place greater demands on a total elbow implant. Such patients are most often treated with nonprosthetic options because of concerns about prosthetic longevity. As a result, few cases of primary osteoarthritis are included in published studies. However, complications such as stem fracture and aseptic loosening appear to be more common in this population than in any other subgroup, including revision patients. The poor soft-tissue quality associated with rheumatoid arthritis leads to a high-risk ligamentous attenuation and is a general contraindication to use of an unlinked implant. The same poor soft tissue leads to a higher rate of triceps insufficiency and wound dehiscence.
Correct answer : A
11- A 69-year-old woman presents 18 months after undergoing surgical repair of her left proximal humerus fracture. She describes global left shoulder pain with limited range of motion. On examination, she has a well-healed superior shoulder incision without any signs of infection. Active elevation is limited to 45°, and passive range of motion results in crepitus. She expresses difficulty with activities of daily living, such as washing her hair. An AP radiograph of her shoulder is shown in Figure 1. What is the most appropriate step to maximize her function at this time?
A. Physical therapy focusing on supine straight arm raises
B. Removal of intramedullary nail and conversion to hemiarthroplasty
C. Revision open reduction and internal fixation (ORIF) to proximal humerus locking plate
D. Removal of intramedullary nail and conversion to reverse shoulder arthroplasty
The patient had a failed attempt at primary repair of her proximal humerus fracture with subsequent malunion. Because of the position of her greater tuberosity and concern about the status of her rotator cuff on examination, a reverse shoulder prosthesis is the most reliable option to maximize her shoulder function. Given the length of time since her index procedure, additional physical therapy is unlikely to provide significant benefit. A hemiarthroplasty or revision ORIF would have a lower likelihood of success due to the position of the greater tuberosity and presumed rotator cuff compromise.
Correct answer : D
12- Placement of the most distal interlocking screw seen in the radiographs in Figures 1 and 2 poses a risk to the nerve that controls what motor function?
A. Elbow flexion
B. Thumb interphalangeal (IP)
joint extension
C. Index finger proximal IP joint flexion
D. Index finger metacarpophalangeal (MCP) joint abduction
The most distal locking screw in this intramedullary nail construct was placed from anterior to posterior, passing through the distal portion of the biceps and brachialis muscle bellies. The median nerve, along with the brachial artery, is at risk as it lies between these 2 muscles. Malrotation of the nail, producing a more anteromedial starting point for the screw, can lead to a path that intersects with the nerve. Blunt dissection and soft-tissue protection is warranted with this screw placement. Median nerve injury would affect innervations of the flexor digitorum superficialis and profundus to the index finger (among other motors). Although the dissection violates the muscle belly of these 2 elbow flexors, measurable weakness is not typically seen. The radial nerve has already provided function to triceps (elbow extension) proximal to this level and lies sufficiently lateral to be more of a concern with a lateral screw placement (thumb IP extension). The ulnar nerve (index MCP abduction) is further medial at this level and would be at considerably lower risk than the median.
Correct answer : C
13- Figures 1 through 3 are the radiographs of a 40-year-old patient with a history of posterior labral repair who presents with severe pain and stiffness in the shoulder. The pain interferes with activities of daily living and interrupts his sleep at night. He has tried corticosteroid injections, nonsteroidal anti-inflammatory drugs, and activity modification with only temporary benefit. He wishes to discuss definitive treatment options. How can you counsel the patient about treatment with a hemiarthroplasty?
10
A. Functional outcomes and pain relief are inferior to total shoulder arthroplasty.
B. Rates of revision are lower than total shoulder arthroplasty.
C. Hemiarthroplasty avoids problems related to glenoid erosion. D. He can expect long term satisfaction.
The patient has evidence of osteoarthritis with eccentric glenoid wear. Hemiarthroplasty outcomes are worse in patients with eccentric glenoid wear, as compared to those with a concentric joint. Additionally, hemiarthroplasty has been shown to have inferior functional outcomes compared to total shoulder arthroplasty, with low long-term satisfaction rates. Revision rates are equal to or greater than total shoulder arthroplasty at mid to long term follow-up, and glenoid erosion remains a problem.
Correct answer : A
14- In comparing open versus arthroscopic osteocapsular arthroplasty for the treatment of elbow osteoarthritis, what is an advantage of arthroscopic over open treatment?
A. rthroscopic treatment provides better final range of motion than open treatment.
B. Arthroscopic treatment can be safely performed in the presence of prior ulnar nerve transposition.
C. Arthroscopic treatment can be equally effective in both early and advanced elbow osteoarthritis.
D. Arthroscopic treatment allows easy access to both the anterior and posterior compartments of the elbow.
Both arthroscopic and open management of elbow arthritis can be successful. Prior ulnar nerve transposition is a relative contraindication to arthroscopy, unless the nerve is specifically identified and protected intra- operatively. In general, arthroscopic management is indicated for mild to moderate arthritis. In advanced arthritis, there is decreased visualization and an increased risk for neurovascular insult. In contrast, open surgery can be utilized regardless of arthritis severity. Arthroscopy has the advantage of allowing easy access to both the anterior and posterior compartments of the elbow. Cohen and associates has shown better recovery of motion with open osteocapsular arthroplasty (Outerbridge-Kashiwagi procedure) compared with the same technique performed arthroscopically.
Correct answer : D
11
15- A 36-year-old woman dislocated her elbow 6 months ago. The elbow was congruently reduced and rehabilitated. She continues to have a sense of painful clunking in her elbow when she pushes up from a chair with forearm supination, but not pronation. What structure did not heal properly?
A. Posterior band of the medial collateral ligament
B. Anterior band of the medial collateral ligament
C. Radial collateral ligament
D. Lateral ulnar collateral ligament
The patient is showing signs of posterolateral rotatory instability after elbow dislocation. The lateral ulnar collateral ligament is responsible for stabilizing the elbow against this type of instability. The posterior and anterior bands of the medial collateral ligament are primarily resistors of valgus load, with the anterior band being the most significant contributor. The radial collateral ligament does not control the posterolateral rotatory instability described.
Correct answer : D
16- A 36-year-old right-hand dominant butcher presents with a 6-week history of medial elbow pain. On physical examination, she is tender to palpation over the anteroinferior aspect of the medial epicondyle. Pain is reproduced with combined elbow extension/resisted wrist flexion. Nonsurgical treatment of this pathology results in pain relief within one year in what percentage of individuals?
A. 25% to 35%
B. 45% to 55%
C. 65% to 75%
D. 85% to 95%
The patient has medial epicondylitis. Nonsurgical treatment is the hallmark of treatment and has been shown to relieve pain in approximately 90% of cases within one year. Nonsurgical modalities include bracing, physical therapy, nonsteroidal anti-inflammatory medications, activity modification, and injections.
Correct answer : D
12
17- A 55-year-old woman develops posttraumatic arthritis in the elbow following a distal humerus fracture. What is the most likely mid-term (5-
10 years after surgery) complication following semiconstrained total elbow arthroplasty (TEA)?
A. Bushing wear
B. Infection
C. Aseptic component loosening
D. Component fracture
TEA has been described for posttraumatic arthritis of the elbow and typically involves a young patient population with multiple previous operations on the affected elbow. Morrey and Schneeberger found aseptic component loosening to be uncommon (<10% of patients) and usually occurring >10 years after surgery. Prosthetic fracture, usually of the ulnar component, is also a late-term finding. Infection is the most common mode of early failure but usually occurs within the first 5 years and has an overall rate of approximately 5%. Bushing wear has been reported as the most common cause of mechanical TEA failure in this population at intermediate-term follow-up.
correct answer : A
18- A 51-year-old man presents with persistent right shoulder pain several weeks after falling off a roof. On examination, he has pain with palpation over the greater tuberosity, active forward shoulder flexion of
60°, and passive forward shoulder flexion of 160°. He has 2/5 forward flexion and external rotation strength. Initial plain radiographs are unremarkable. A coronal MRI scan of his shoulder is shown in Figure 1. After a thorough discussion, the patient elects to proceed with surgical intervention. During intraoperative assessment, the surgeon contemplates performing a single versus a dual row repair. Currently, what is the consistent difference between the two repair techniques?
A. Dual row repairs result in superior objective clinical outcomes
B. Dual row repairs provide a larger footprint coverage.
C. Single row repairs have a reported higher complete retear rate.
D. Single row repairs have fewer points of tendon fixation.
13
Several investigations continue to elucidate the difference between dual row and single row repairs. Modern dual row repairs involve fixating the rotator cuff tendon along both the medial and lateral aspect of the greater tuberosity as well as linking both points of fixation together. This allows closer restoration of native footprint coverage in comparison with single row repairs. However, doubling the number of implants results in increased healthcare costs without a clear clinical or biomechanical benefit. Several studies report statistically similar outcomes, retear rates, and biomechanical properties between single and dual row repair when the number of suture limbs across the repair site is the same.
correct answer : B
19- Figures 1 and 2 are the radiographs of a 37-year-old left-hand dominant man with left elbow pain and stiffness. He has a history of elbow dislocation as a child but denies any recent injuries. He has an arc of motion of 105° and stable ligaments. He describes crepitus and locking during elbow range of motion. He is an avid Crossfit athlete, intending to return to this activity and improve his range of motion. What is the best treatment?
A. Total elbow arthroplasty (TEA)
B. Ulnohumeral distraction interposition arthroplasty
C. Radial head replacement
D. Arthroscopic or open debridement and capsular release
14
This is a young, high-demand patient with early posttraumatic arthritis of the elbow. A debridement and capsular release has the ability to address his mechanical symptoms, improve his range of motion, and not result in any post- operative functional restrictions. While this may be a temporizing procedure in this patient, it will allow him to return to weight bearing recreational activities in the near term, which is his goal. A TEA would not be indicated based on the patient's age, his degree of arthritis, and his desire to remain active post- operatively. A radial head replacement would not address the patient's ulnohumeral arthritis. Similarly, an ulnohumeral distraction interposition arthroplasty would not address the patient's radiocapitellar arthritis. Both procedures would also require adjustments to his recreational activities post- operatively to prevent progressive failure of the reconstruction.
Correct answer : D
20- Figure 1 is the radiograph of 59-year-old left-hand dominant patient who underwent revision to a reverse total shoulder arthroplasty following a failed open reduction and internal fixation of a proximal humerus fracture. What is a risk factor for the complication shown?
A. Female sex
B. Lateralized component
C. Cemented humeral component
D. Previous surgery
Risk factors for instability after a reverse total shoulder arthroplasty include previous surgery (especially open surgery), loss of humeral tuberosities, inadequate restoration of humeral length,
male sex, BMI >30, and Grammont-style implant. Fixation method for the humeral stem has no impact on instability risk.
Correct answer : D
15
21- Figures 1 through 3 are the radiographs of a 55-year-old woman who fell on her outstretched right arm, resulting in acute elbow pain and swelling. On examination, she has lateral elbow bruising and tenderness, with a mechanical block to forearm supination and pronation. She has no medial tenderness. During surgery through a direct lateral approach, the surgeon observes a completely bare lateral epicondyle and surgical repair is performed, resulting in a stable and congruent joint. Initial postoperative rehabilitation should include
A. 3 weeks of cast immobilization.
B. elbow extension exercises with the forearm supinated. C. elbow extension exercises with the forearm pronated.
D. elbow extension exercises with the forearm in neutral rotation.
Radial head fractures are thought to occur as a result of valgus posterolateral rotary load across the elbow, although the mechanism can certainly vary. Minimally or nondisplaced fractures without any clinical instability or block to motion can often be successfully managed non-surgically. Fractures with >2 mm of displacement or fragments that block motion require surgical repair. A critical aspect during surgery is identifying concomitant injury to the lateral collateral ligament complex (LCL). When encountered, the LCL is most often avulsed from its origin at the lateral epicondyle, resulting in a bare area. After the radial head is either repaired or replaced (Figures 4 and 5), the LCL should
16
be repaired back to its anatomic origin. Postoperatively, the surgeon must communicate to the therapist that elbow extension exercises should be performed with the forearm in pronation as a result of the compromised LCL, as this position places the least stress on the ligamentous repair. Elbow extension exercises in supination or neutral are recommended for compromise of the medial collateral ligament, or combined medial and lateral ligament injury, respectively. Without any medial elbow bruising, swelling, or tenderness, it is unlikely that the patient has an injury to the medial collateral ligament.
Correct answer : C
22- A 78-year-old woman undergoes a reverse total shoulder arthroplasty for cuff tear arthropathy. Her preoperative, 3-month postoperative, and 1- year postoperative radiographs are shown in Figures 1 through 3. What is the cause of the radiographic finding seen here?
17
A. Glenoid component malposition
B. Humeral component malposition
C. Over tensioning of the deltoid
D. Excessive humeral component lateralization
The patient underwent a reverse arthroplasty for cuff tear arthropathy. Her preoperative radiograph shows some superior glenoid wear, which was not corrected at the time of surgery. This has resulted in superior tilt to the glenosphere, which has been identified as a risk factor for scapular notching. This occurs as a result of mechanical impingement between the medial humerus and scapular neck during arm adduction. The Beta angle and reverse shoulder angle have been proposed as measurements that can help identify pathologic glenoid tilt preoperatively. Risk factors for scapular notching include superior tilt of the glenosphere, superior placement of the glenoid baseplate on the glenoid, a 155° humeral implant angle, and incomplete lateralization of the construct.
The humeral component appears well-positioned in this radiograph. Over tensioning of the deltoid and excessive humeral lateralization would risk an acromial stress fracture and could limit shoulder range of motion. This is an inlay humeral stem, which does not lateralize the humerus.
Correct answer : A
23- Figures 1 and 2 are the MRI scans of a 21-year-old swimmer who has had pain in the lateral shoulder for 6 months. It is worse while swimming and with reaching overhead. Twelve weeks of physical therapy and a single corticosteroid injection have failed to improve her symptoms. What is the best next step?
18
A. Arthroscopic superior labrum anterior to posterior (SLAP) repair
B. Arthroscopic rotator cuff repair
C. Arthroscopic Bankart repair
D. Suprascapular nerve decompression
In the MRI scans, the patient has a high-grade tear of the undersurface of the superior rotator cuff. This is known as a partial articular-sided tendon avulsion lesion. This is often seen in overhead athletes and is associated with internal impingement. Given the length of symptoms, failure to respond to nonsurgical treatment, and the high-grade nature of the tear in a young patient, an arthroscopic repair should be performed. The available images do not demonstrate evidence of SLAP tear, Bankart lesion, or suprascapular nerve compression.
Correct answer : B
24- Figure 1 is the intraoperative radiograph of a shoulder hemiarthroplasty for glenohumeral arthritis. A "ream and run" is planned for the glenoid. What can be said about the outcomes of this procedure?
19
A. Activity restrictions are more rigid than after total shoulder arthroplasty. B. Fifty percent of patients require glenoid resurfacing within 2 years.
C. Recovery is faster than a total shoulder arthroplasty. D. Therapy is critical in obtaining a good clinical outco
"Ream and run" shoulder arthroplasty can allow for arthroplasty without the complications of a polyethylene glenoid. Ten-year conversion to total shoulder arthroplasty has been shown in one study to be 12%. Recovery is reported to be slower and requires more rehabilitation than arthroplasty done with glenoid resurfacing. Careful patient selection has been emphasized by the pioneering surgeon.
Correct answer :B
25- Figure 1 is the axial MRI scan of a 45-year-old brick mason who experienced acute right elbow pain after attempting to lift a wheelbarrow. Examination reveals pain and swelling in the antecubital fossa, weakness with forearm supination, and an abnormal hook test. The surgeon performs an anterior repair with two anchors. Three months after surgery, the patient has appropriate strength and range of motion but reports persistent radiating paresthesias along the radial side of the forearm. What is the best next step in management?
A. Exploration of forearm with neurolysis
B. MRI scan of cervical spine C. Revision distal biceps repair D. Observation with nonsteroidal
anti-inflammatory drugs as needed
This is a classic presentation of an acute traumatic distal biceps tendon rupture. In the dominant extremity of a manual laborer, this injury can result in approximately 40% loss of supination strength. Although not required, an MRI scan can confirm
the diagnosis. In general, a single incision anterior or two incision anterior/ posterior repair can be utilized for surgical intervention with similar success rates. Although the percentage of complications is similar between surgical approaches, the type of complications can vary. Anterior only repairs have a
20
higher risk of traction injury to the lateral antebrachial cutaneous nerve (LABC) secondary to the degree of retraction required for exposure in muscular patients. Posterior repairs have a higher risk for radiographic heterotopic bone formation. Fortunately, most LABC injuries are neuropraxias and resolve with observation, but resolution may take up to 6 months. In this case, ongoing observation is appropriate, with surgical exploration being considered only in chronic cases. Patients should be appropriately counseled about this issue prior to surgery.
Correct answer : D
26- When performing an ulnar nerve decompression at the elbow, the surgeon must be aware of the
A. median nerve as it crosses the surgical field 6 cm proximal to the medial epicondyle.
B. medial antebrachial cutaneous nerve as it crosses the field 3 cm distal to the medial epicondyle.
C. anterior antebrachial cutaneous nerve as it crosses the field at the medial epicondyle.
D. posterior antebrachial cutaneous nerve that crosses the field 2 cm distal to the medial epicondyle.
The medial antebrachial cutaneous and medial brachial cutaneous are nerves that can be injured during ulnar nerve decompression at the elbow. The medial antebrachial cutaneous nerve crosses the surgical field at an average of 3.1 cm distal to the medial epicondyle. The medial brachial cutaneous nerve crosses the field 7 cm proximal to the medial epicondyle and arborizes into two to three terminal branches. Because the surgical approach involves dissection on the medial side, the posterior antebrachial cutaneous nerve is distant from the exposure. Although the median nerve potentially can be located in the deep dissection of a submuscular transposition, it is considered distant to an in situ decompression.
Correct answer : B
27- Figures 1 and 2 are the radiographs of a 40-year-old patient who undergoes treatment of the clavicle fracture shown. What is the most likely complication of this intervention?
21
A. Nonunion
B. Acromioclavicular (AC) joint instability
C. Deltoid origin rupture
D. Symptomatic hardware
There have been many prospective and retrospective studies evaluating outcomes after surgical and nonsurgical treatment of displaced middle third clavicle fractures. Surgery results in a lower nonunion rate and higher patient reported outcomes. However, approximately 30% of these patients will have symptoms of hardware irritation and request subsequent plate removal. Nonunion is very low with plate fixation and is more common with nonsurgical treatment. AC joint instability is unlikely to be an issue with middle third clavicle fractures, and there is no evidence of AC malalignment on the images provided. Deltoid origin stripping is necessary for anterior plating, but is much less of an issue with superior plating, as was performed in this patient. Anterior plating is biomechanically inferior to superior plating but may pose a lower risk to neurovascular structures and has the theoretic opportunity to decrease implant irritation, although this has not been clearly demonstrated in the literature.
Correct answer : D
28- Figure 1 is the radiograph of a 54-year-old man who has increasing weakness and numbness in his lateral arm. No prior surgery or injury is reported. What is the most appropriate next diagnostic test?
A. MRI of the shoulder
B. MRI of the cervical spine
C. CT scan of the chest
D. Radiograph of the chest
22
The radiograph reveals a Charcot neuropathic shoulder. The atraumatic destruction of the humeral head is concerning for a neuropathic etiology and warrants MR imaging of the cervical spine to evaluate for the presence of a syrinx. Shoulder arthroplasty in the setting of a neuropathic joint is challenging given the local bone and soft-tissue loss, in addition to the loss of protective sensation. The scant literature on the use of shoulder arthroplasty in these challenging patients reports an improvement in pain but only modest improvements in shoulder function.
Correct answer : B
29- Figure 1 is the radiograph and Figure 2 is the 3-dimensional CT scan of a 55-year-old male patient who fell out of a tree 3 days ago onto his outstretched hand. What is the most appropriate treatment?
A. Lateral ligament repair and radial head replacement
B. Coronoid reconstruction utilizing allograft
C. Open reduction and internal fixation (ORIF) of the coronoid and possible lateral collateral ligament repair
D. ORIF of the coronoid and reconstruction of the medial collateral ligament
The patient presents with a coronoid fracture involving the anteromedial facet. This poses a risk for varus posteromedial rotary instability of the elbow. Appropriate treatment involves coronoid ORIF (this fracture involves the sublime tubercle, so fixing the coronoid will repair the medial collateral ligament) and a repair of the lateral ligament complex. Coronoid reconstruction is not needed with graft because the fracture fragment can be repaired. However, in chronic cases, the coronoid can be reconstructed with autograft
23
olecranon, autograft radial head, or allograft. There is no injury to the radial head, so arthroplasty is not required. Failing to address the lateral ligaments will lead to continued instability.
Correct answer : C
30- A 33-year-old right-hand dominant man presents for evaluation of recurrent right shoulder instability following a fall. He initially sustained a traumatic anterior shoulder dislocation while playing football 12 years ago that was treated with an arthroscopic Bankart repair. He sustained a repeat traumatic dislocation 5 years ago, prompting a revision arthroscopic Bankart repair and capsular shift. His shoulder has been stable until his recent reinjury three months ago. He feels that the shoulder is "sliding out" when he puts his arm in an abducted and externally rotated position. The symptoms remain unchanged despite participating in 2 months of physical therapy. Apprehension/Relocation test is positive. He has full range of motion without weakness. A CT arthrogram reveals 20% loss of bone of the anteroinferior glenoid, no Bankart lesion, and a non-engaging Hill-Sachs. What is the most appropriate treatment?
A. Revision arthroscopic Bankart repair with remplissage
B. Open Bankart repair with capsular shift
C. Transfer of the coracoid to the anterior glenoid
D. Injection of platelet-rich plasma
The history and examination are consistent with recurrent anterior shoulder instability. The patient has significant anteroinferior glenoid bone loss, no identifiable Bankart tear, and a non-engaging Hill Sachs. The glenoid bone deficiency is the most notable contributor to his recurrent instability, and a Latarjet coracoid transfer to the anterior glenoid would most likely provide long-term stability to his shoulder. A remplissage with tenodesis of the infraspinatus into the Hill-Sachs lesion can be helpful if the symptoms are related to engagement of the Hill-Sachs lesion. An open capsular shift and Bankart would not address the bony deficiency. There is no role for PRP in this clinical setting.
Correct answer : C
24
31- What is the most common complication following reverse total shoulder arthroplasty?
A. Scapula spine/acromial fracture
B. Dislocation/instability
C. Implant loosening
D. Periprosthetic fracture
Complications encountered following reverse total shoulder arthroplasty include dislocation, infection, hardware failure, hematoma, neurologic injury, periprosthetic fracture, scapular notching, and acromial/scapular spine fractures. The incidence and risks of these complications are related to the indication for the procedure. Dislocation is the most common complication, with an incidence of 1.5% to 31%. Risk factors associated with postoperative dislocation include male sex, previous shoulder surgery, proximal humeral bone loss, axillary nerve injury, and subscapularis deficiency. Commonly used methods to prevent instability include lateralization of the glenosphere and/or baseplate, eccentric baseplate placement, humeral lateralization or distalization, use of large glenosphere, and increased socket constraint. Correct answer : B
32- A 75-year-old woman with rheumatoid arthritis and a long history of oral corticosteroid use sustains a comminuted intra-articular distal humerus fracture. What is the best surgical option?
A. Open reduction internal fixation (ORIF) with parallel plates B. ORIF with orthogonal plates and iliac crest bone grafting C. Total elbow arthroplasty (TEA)
D. Closed reduction and percutaneous pinning
TEA is the best surgical option. McKee and associates published a multicenter randomized controlled trial comparing ORIF with TEA in elderly patients. TEA resulted in better 2-year clinical functional scores and more predictable outcomes compared with ORIF. TEA was also likely to result in a lower reoperation rate; one-quarter of patients with fractures randomized to ORIF could not achieve stable fixation. Further, Frankle and associates reported a comparative study of TEA versus ORIF in 24 elderly women. TEA outcomes were again superior to ORIF at a minimum of 2 years of follow-up. TEA was especially useful in patients with comorbidities that compromise bone stock, including osteoporosis and oral corticosteroid use. Closed reduction and percutaneous pinning studies have not been published on the adult population. Correct answer : C
25
33- A 17-year-old girl develops chronic posterolateral rotatory instability (PLRI) of the elbow following closed treatment of an elbow dislocation. Advanced imaging reveals incompetence of the lateral collateral ligament complex, and ligament reconstruction is planned. Examination under anesthesia is performed with the forearm in maximal supination and valgus force applied to the elbow, demonstrated in Video 1. As the elbow is brought through a range of motion assessment, the radial head is
A. dislocating posteriorly in extension and reducing in flexion. B. dislocating posteriorly in flexion and reducing in extension. C. dislocating anteriorly in extension and reducing in flexion. D. dislocating anteriorly in flexion and reducing in extension.
PLRI of the elbow is the most common form of chronic elbow instability. The mechanism occurs following a fall onto an outstretched hand, where a valgus force is applied to the elbow and the forearm rotates into progressive supination. This allows the radial head to translate posterior to the capitellum, with progressive injury from lateral to medial sides of the elbow. The pivot shift test is a useful examination maneuver to confirm the presence of PLRI. With the forearm in maximal supination and valgus stress applied to the elbow, the radial head is forced posterior to the capitellum as the elbow is brought into progressive extension, revealing a dimple on the lateral aspect of the elbow. This typically occurs at roughly 30° of flexion. As the elbow is flexed, the radial head reduces.
Correct answer : A
34- Figure 1 is the MRI of a 45-year-old woman with a medical history significant for rheumatoid arthritis who returns to your office with persistent right elbow pain. Her rheumatologist has maximized her disease-modifying anti-rheumatoid drug regimen. She complains of diffuse joint pain and swelling. On examination, she has a pronounced joint effusion, elbow flexion arc of 45°, and crepitus with forearm rotation. Her elbow radiograph reveals preservation of her joint space. What is the most appropriate surgical treatment at this time?
26
A. Total elbow arthroplasty
B. Synovectomy with radial head resection
C. Synovectomy without radial head resection
D. Isolated radial head resection
Rheumatoid arthritis remains a common inflammatory arthropathy that can lead to progressive synovitis of the elbow joint. Patients often present with recalcitrant elbow pain and loss of motion. In the early
stages, the joint space can be fairly well preserved. With progressive synovitis, cartilage destruction leads to symmetric joint space narrowing and joint destruction. For the younger patient with recalcitrant synovitis and a relatively well-preserved joint space, open or arthroscopic synovectomy provides successful improvement for 70% to 80% of patients. In most cases, radial head resection is not required. Synovitis that encircles the radial head and neck can lead to pain and crepitus with forearm rotation. Preserving the radial head prevents the rapid progression of wear at the ulnohumeral joint. A total elbow replacement, while a successful treatment modality for the older, lower demand patient with rheumatoid arthritis, would not be ideal for the younger patient given the significant postoperative restrictions imparted.
Correct answer : C
35- A 15-year-old girl has experienced 6 months of increasing dominant shoulder pain while playing volleyball. Her pain is so significant that she can no longer compete. Examination demonstrates 190° of forward elevation, 110° of external rotation at the side, and internal rotation up the back to T2 bilaterally. She also has 15° of bilateral elbow hyperextension. Load and shift testing demonstrates pain with anterior and posterior drawer tests. She has a large sulcus sign with associated pain. Forward elevation and external rotation strength testing shows 4/5 strength. There is no scapular winging and radiographic findings are normal. What is the best next step?
A. Physical therapy for rotator cuff strengthening
B. Subacromial corticosteroid injection
C. MRI arthrogram
D. Arthroscopic stabilization
27
This patient has multidirectional instability as evidenced by her hyperlaxity and excessive range of motion. Patients with pain after activities often have weak rotator cuff musculature and improve with strengthening of the rotator cuff and proprioceptive retraining. Subacromial injection likely cannot help this patient because it will not treat her underlying motor weakness in the rotator cuff or her dyskinesia. MRI arthrogram is not indicated unless she fails nonsurgical treatment. Arthroscopic stabilization also would be reserved for patients who fail nonsurgical treatment.
Correct answer : A
36- When performing capsular releases during shoulder arthroplasty for the treatment of glenohumeral joint osteoarthritis, what anatomic landmark indicates the location of the axillary nerve as it begins to travel from anterior to posterior?
A. Inferior border of the subscapularis
B. Insertion of the pectoralis major onto the humerus
C. Insertion of the latissimus dorsi tendon onto the humerus
D. Lateral margin of the conjoint tendon
The axillary nerve originates from the posterior cord of the brachial plexus. It passes down the anteroinferior aspect of the subscapularis, courses posteriorly beneath the glenoid and inferior capsule, then wraps around the humerus from posterior to anterior on the deep surface of the deltoid. In the setting of glenoid and humeral head deformity, the inferior border of the subscapularis can be a useful landmark to ensure the nerve is appropriately protected intraoperatively.
Correct answer : A
37- A 24-year-old female rugby player presents after a traumatic shoulder dislocation. She has a history of open Latarjet 3 years ago related to chronic shoulder instability. Her current radiograph and CT scans are shown in Figures 1 through 4. Her shoulder is unstable with abduction and external rotation. Belly press test and axillary nerve function are intact. What is the best surgical option for her?
28
A. Arthroscopic debridement with anteroinferior labral repair and capsular shift
B. Open implant removal and repair of damaged soft-tissue structures
C. Revision anterior glenoid augmentation with iliac crest autograft or distal tibial allograft
D. Open Putti Platt reconstruction
The patient has developed recurrent shoulder instability following a previous Latarjet. Radiographs and CT scans demonstrate resorption of the coracoid graft and failure of hardware. At this point, in a contact athlete with failed hardware and recurrent instability, the most appropriate surgical intervention would be an open procedure with hardware removal and revision bone grafting of the anterior glenoid with iliac crest autograft or distal tibial allograft.
29
Arthroscopic debridement with anteroinferior labral repair and capsular shift and open implant removal and repair of damaged soft-tissue structures are incorrect because an isolated soft-tissue procedure would place the patient at high risk for recurrence. A Putti Platt reconstruction is a nonanatomic reconstruction that has been correlated with progressive glenohumeral arthrosis.
Correct answer : C
38- Figures 1 through 3 are the radiographs and MR arthrogram of a 46- year-old woman who reports bilateral elbow pain over the past 2 years. Pain is diffuse, associated with stiffness, and is worst in the morning. It gradually improves over the course of the day. Physical examination shows a moderate elbow effusion, with tenderness to palpation diffusely around the elbow, but worst in the posteromedial and posterolateral gutters. She lacks 25° of terminal extension bilaterally and has pain with terminal elbow flexion. She has tried anti-inflammatory medication, corticosteroid injections, and physical therapy without improvement in symptoms. What is the best surgical treatment option at this point?
A. Arthroscopic debridement and synovectomy
B. Radial head excision
C. Total elbow arthroplasty
D. Interpositional arthroplasty
30
The patient’s clinical presentation is consistent with inflammatory arthritis. The MRI shows a large effusion with synovitis, particularly around the radial neck. There is bone edema in the proximal ulna, but no evidence of joint destruction, and radiographs reveals maintained joint space. These findings support the diagnosis of early-stage inflammatory arthritis. Because there is no joint destruction, surgical treatment would emphasize preservation of the native elbow joint. Arthroscopic synovectomy has been shown to be very effective in these cases. Referral to a rheumatologist for further workup is also recommended. The other options listed would be considered in the setting of more advanced joint degeneration.
Correct answer : A
39- Figures 1 through 3 are the MRI scans of a 56-year-old woman in good health who reports a 6-month history of shoulder pain and external rotation weakness. Her radiographs are unremarkable. What is the diagnosis?
A. Rotator cuff tear
B. Anteroinferior labral tear
C. Suprascapular nerve compression
D. Quadrilateral space syndrome
31
The images reveal T2-weighted MRI sequences with edema isolated to the infraspinatus. In the absence of a tear in the infraspinatus tendon, the edema is most likely due to compression of the suprascapular nerve in the spinoglenoid notch. As this pathology persists, progressive muscle atrophy and fatty infiltration can result. Compression of the suprascapular nerve in the suprascapular notch would have resulted in edema and weakness in both the supra- and infraspinatus muscles. Compression is commonly caused by cysts from the joint secondary to labral tears. A rotator cuff tear of the infraspinatus is not identified on these images, and there is no history of trauma provided. There is no evidence of an anteroinferior labral tear, nor would this be expected to result in external rotation weakness or MRI abnormality of the infraspinatus. Quadrilateral space syndrome results in compression of the axillary nerve, which supplies the teres minor.
Correcr answer : C
40- A 41-year-old right-hand-dominant man has been treated nonsurgically for right elbow arthritis. His radiographs reveal end-stage ulnohumeral arthritis with complete loss of the joint space. He reports pain during the mid-arc of elbow flexion and extension. During the last 8 years, he has attempted activity modification, medication, physical therapy, and multiple cortisone injections. His symptoms have progressed, resulting in constant pain, loss of a functional range of motion, and an inability to perform many activities of daily living. Secondary to his age and activity demands, he undergoes a soft-tissue interposition arthroplasty of his elbow with an Achilles allograft. Which presurgical finding correlates with elevated risk for postsurgical complications?
A. Inflammatory elbow arthritis
B. A presurgical flexion-extension elbow arc of approximately 50° C. Retained distal humerus hardware on presurgical radiographs D. Evidence of presurgical elbow instability
End-stage posttraumatic or inflammatory elbow arthritis in active, high-demand patients remains difficult to treat. Traditional total elbow arthroplasty is discouraged in this demographic secondary to concerns about implant longevity. Soft-tissue interposition arthroplasty does not necessitate the same activity and weight restrictions for patients after surgery and remains a reasonable salvage procedure. Larson and Morrey published their findings on
38 patients with a mean age of 39 years following soft-tissue interposition arthroplasty for posttraumatic and inflammatory end-stage elbow arthritis. These investigators reported a significant improvement in Mayo Elbow Performance Score in addition to improvement in the flexion-extension arc from 51° to 97° after surgery. They reported worse results and elevated incidence of complications for patients with presurgical elbow instability. Retained hardware from prior surgery was not deemed a contraindication.
Correct answer : D 32
41- Figure 1 is the radiograph of a 12-year-old baseball player who has posterolateral elbow pain with throwing. The area of interest is designated by the black arrow. His range of motion and strength are full. No previous treatment has been provided. What is the most appropriate initial treatment?
A. Elbow arthroscopy with debridement B. Immobilization and rest for 6 weeks C. Corticosteroid injection
D. Open osteochondral autograft transfer
Osteochondritis dissecans of the capitellum is a painful condition that affects immature athletes who undergo repetitive compression of the radiocapitellar joint. Management is based primarily on the integrity of the articular cartilage surface and the stability of the lesion. Nonsurgical treatment is typically selected for patients
with early-grade, stable lesions, and it involves activity modification with
cessation of sports participation. The duration of activity modification is dictated by symptoms, with 3 to 6 weeks of rest followed by return to sport in
3 to 6 months commonly used as a guideline. Strengthening and stretching exercises are commonly incorporated after the pain has subsided. Surgical intervention or corticosteroid injection would not be first-line treatment. Correct answer : B
42- Figures 1 and 2 are the radiographs of a 69-year-old man with a history of treated prostate cancer and hemodialysis-dependent end- stage renal disease who presents to the emergency department with progressively worsening right shoulder pain and stiffness. Laboratory tests reveal a white blood cell count of 17,000, erythrocyte sedimentation rate, 75, and CRP, 10.1. He has a draining sinus located along the anterior shoulder. What is the best next step?
33
A. Arthroscopic irrigation and debridement
B. Admission and IV antibiotics
C. Culture from draining sinus
D. MRI scan with intravenous contrast
The patient's radiographs demonstrate bone loss of the medial humeral head. He has risk factors for both septic arthritis/osteomyelitis, and metastatic cancer, and it is important to understand the extent of his pathology before moving forward with surgical intervention. An MRI scan would assist in the diagnosis and demonstrate the extent of disease/tissue involvement. Administration of IV antibiotics prior to obtaining appropriate cultures would decrease the success rate of treatment in the setting of infection, and mistreat the pathology in the setting of metastasis. Similarly, obtaining cultures from the draining sinus tract would fail to account for the possible tumor diagnosis and may result in inaccurate culture results.
Correct answer : D
43- Figure 1 is the radiograph of a 19-year-old lacrosse player who landed on the apex of his right shoulder in a game 2 weeks ago. Figure 2 represents a comparison view of his uninjured contralateral side. He presents with complaints of right shoulder pain and deformity. Physical examination is negative for rotator cuff pathology or glenohumeral instability. Coracoclavicular distance is increased by 60% on the affected side. What is the best next step in management?
A. Physical therapy
B. Steroid injection
C. Platelet-rich plasma (PRP) injection
D. Operative fixation
34
44- In rotator cuff tear arthropathy with pseudoparalysis, forward elevation of the humerus away from the body is prohibited because of
A. deltoid atony.
B. loss of glenoid concavity.
C. loss of humeral head depression from the biceps tendon. D. loss of compressive force on the humeral head.
The rotator cuff serves as a humeral head compressor that stabilizes the humeral head in the glenoid concavity, so that the deltoid can convert a vertical force into abduction and forward elevation. The deltoid functions normally in patients with chronic rotator cuff arthropathy, so no atony is present. Glenoid concavity can be lost over time as joint degeneration progresses, but this is not the primary mechanism for failure of elevation. The biceps tendon does not serve as a humeral head compressor and does not prevent proximal migration of the shoulder when it is present.
Correct answer : D
45- Figure 1 is the radiograph of a 70-year-old woman with left shoulder pain following a ground-level fall 2 days ago. She reports good function of the shoulder prior to her fall. Examination reveals intact neurovascular status. She elects to undergo an acute reverse shoulder arthroplasty (RSA). How does this intervention compare with other arthroplasty options?
A. RSA results in better outcomes but increased complications compared with hemiarthroplasty.
B. RSA results in better outcomes and similar complications compared with hemiarthroplasty.
C. Acute RSA results in better outcomes than delayed RSA in this demographic.
D. Hemiarthroplasty and RSA have similar outcomes.
RSA has been shown to result in better clinical outcomes with a similar complication rate compared with hemiarthroplasty for the treatment of comminuted proximal humeral fractures in elderly patients. If an RSA is necessary in a delayed fashion to salvage failed nonoperative management, a systematic review and meta-analysis have shown no significant difference in outcomes between acute versus delayed RSA in this patient population. Correct answer : B
35
46- A 45-year-old right-hand dominant woman falls onto an outstretched left hand. Imaging shows a complex elbow dislocation. The postreduction CT scan demonstrates a reduced joint, comminuted radial head fracture, and type I coronoid fracture. Surgical intervention is recommended to address the involved structures. Which component of the intervention adds the most rotational stability?
A. ixation of the coronoid fragment
B. Radial head arthroplasty
C. Repair or reconstruction of the lateral collateral ligament (LCL)
complex
D. Repair or reconstruction of the medial collateral ligament (MCL)
This represents a terrible triad injury, with elbow dislocation, radial head fracture, and coronoid fracture. The LCL complex is typically disrupted in this injury pattern. Repair or reconstruction of this structure provides the greatest increase in rotational stability of the elbow.
Correct answer : C
48- A 68-year-old right-hand dominant woman has experienced progressive right elbow pain and loss of motion for several years. She has failed nonsurgical treatment and elects to undergo a total elbow arthroplasty (TEA). In comparison to a linked prosthesis, an unlinked prosthesis has which reported distinction with extended follow-up?
A. Improved longevity in comparison to the linked prosthesis
B. A significantly larger flexion-extension arc
C. A higher incidence of postsurgical instability
D. Lower frequency of ulnar nerve dysfunction
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants.
Correct answer : C
36
48- A 21-year-old left-hand dominant minor league baseball player presents with a several-month history of pain while throwing. He is most symptomatic during the deceleration phase of his throwing motion. At terminal extension, he notes pain and loss of motion. The patient denies mechanical symptoms. Looking at Figure 1, where is the initial radiographic abnormality most likely to be found in this patient?
A B C D
The patient has evidence of valgus extension overload (VEO). In overhead athletes with VEO, the posteromedial aspect of the olecranon abuts the olecranon fossa during the throwing motion. As a result, osteophyte formation along the medial olecranon is typically the first radiographic abnormality identified. Pain typically occurs during the deceleration phase of throwing, and loss of terminal extension can ultimately develop. As the pathology progresses, osteophytes and loose bodies may be present within the olecranon fossa, and the ulnar collateral ligament can be damaged. Increases in valgus laxity can ultimately cause degenerative changes to the radiocapitellar joint, but this is a secondary phenomenon. Correct answer : B
49- Figures 1 through 3 are the radiographs of a 68-year-old woman with progressive shoulder pain. She has failed all nonoperative modalities and now presents with refractory shoulder pain at night and with any attempted shoulder motion. She lacks the ability to forward elevate or abduct her shoulder >45°. What is the best treatment option?
37
A. Arthroscopic rotator cuff debridement and superior capsular reconstruction
B. Reverse total shoulder arthroplasty
C. Shoulder hemiarthroplasty
D. Total shoulder arthroplasty utilizing a titanium in-growth glenoid component
The patient has cuff tear arthropathy associated with significant pain and poor function. At age 68, a reverse total shoulder arthroplasty is the most reliable option to address her complaints. Arthroscopic debridement with superior capsular reconstruction would be a consideration in a younger patient with an irreparable posterosuperior rotator cuff tear, little to no glenohumeral arthritis, and little to no humeral head elevation. Total shoulder arthroplasty would have a high rate of glenoid component failure and limited function, regardless of the type of glenoid component utilized. Clinical outcomes of reverse total shoulder arthroplasty are superior to hemiarthroplasty in the setting of cuff tear arthropathy.
Correct answer : B
38
50- Figures 1 and 2 are the CT and MRI scans of a patient with shoulder instability. Contrasting these two imaging techniques for decision making in shoulder instability would suggest
A. Both CT and MRI have equivalent cost for the patient.
B. Both CT and MRI have equivalent safety for the patient.
C. Associated soft-tissue damage can be more reliably shown on CT
scans.
D. Two-dimensional CT scans represent better definition of bone loss than two-dimensional MRI scans.
Two-dimensional CT scan is generally accepted as a superior imaging modality for evaluating bone loss in shoulder instability than two-dimensional MRI scan. This advantage is offset by the relatively high radiation dose. Although CT in most situations is less costly, MRI can provide more data regarding associated soft-tissue damage that can be associated with recurrent instability. It should be noted that three-dimensional MRI has recently been shown as equivalent to three-dimensional CT in its ability to identify glenoid bone loss.
Correct answer : D
51- A 43-year-old woman is involved in a motor vehicle collision. She sustains the isolated injury shown in the radiograph in Figure 1. Her neurovascular examination is compromised. What is the most likely deficit?
A. Inability to flex the distal interphalangeal joint of the index finger
B. Positive Froment’s sign
C. Weakness with wrist extension
D. Decreased capillary refill
39
Humeral shaft fractures can be associated with palsy of the radial nerve, which will result in deficits of wrist and finger extension. Most will resolve with observation, consistent with a neuropraxia. Radial nerve palsy is not a contraindication to functional bracing. Distal interphalangeal (IP) joint flexion of the index finger is from the flexor digitorum profundus of the index finger, supplied by the median nerve. Froment's sign results from weakness of the adductor pollicis, which is innervated by the ulnar nerve. In this maneuver, patients compensate with flexion of the IP joint of the thumb (flexor pollicis longus, innervated by the median nerve) when asked to pinch a piece of paper between their thumb and index finger. Vascular injuries are uncommon with isolated humeral shaft fractures.
Correct answer : C
52- Figure 1 is the MR arthrogram of a 24-year old professional baseball pitcher who complains of worsening right elbow pain and decreased pitch velocity over the past 2 months. He was initially managed with rest and forearm strengthening, but continues to complain of medial elbow pain during the long toss portion of his throwing program. What is the most appropriate treatment at this time?
A. Ulnar nerve decompression
B. Common flexor pronator repair
C. Elbow arthroscopy with debridement
D. Medial ulnar collateral ligament reconstruction/repair
The MR arthrogram shows a rupture of the ulnar collateral ligament (UCL) from the ulnar insertion, with the classic T-sign of contrast extravasation. Medial UCL reconstruction, using either ipsilateral palmaris longus or allograft tendon, is
indicated for UCL injuries that fail nonsurgical management. Primary repair has been shown to be successful in select cases, but appropriate patient selection is essential. An arthroscopic elbow debridement would be indicated for early elbow arthritis or intra-articular loose body, which is not demonstrated here. An ulnar nerve decompression would be indicated in the setting of cubital tunnel syndrome, but this patient has no complaints of paresthesias.
Correct answer : D
40
53- A right-hand dominant 45-year-old man sustains an injury to the anterior aspect of his right elbow while trying to lift a heavy load 3 days ago. He has ecchymosis in the anterior and medial elbow regions and has difficulty with resisted forearm supination with the elbow in a flexed position. A diagnosis of an acute distal biceps tendon rupture is made and surgical treatment is chosen. The anatomic relationship of the distal biceps tendon to the median nerve and recurrent radial artery within the antecubital fossa is such that the biceps tendon travels
A. lateral (radial) to the median nerve and posterior (deep) to the recurrent radial artery.
B. lateral (radial) to the median nerve and anterior (superficial) to the recurrent radial artery.
C. medial (ulnar) to the median nerve and posterior (deep) to the recurrent radial artery.
D. medial (ulnar) to the median nerve and anterior (superficial) to the recurrent radial artery.
During surgical repair of a distal biceps tendon rupture, regardless of the surgical approach or technique, an understanding of the regional anatomy is important. The tendon passes distally into the antecubital fossa. The antecubital fossa is defined by the brachioradialis radially and the pronator teres ulnarly. A sheath surrounds the biceps tendon as it passes through the antecubital fossa toward its insertion on the radial tuberosity. The lateral antebrachial cutaneous nerve lies superficially in the subcutaneous tissue of the antecubital fossa. The nerve parallels the brachioradialis. While still superficial, the tendon is contiguous with the lacertus fibrosus that becomes confluent medially with the fascia overlying the flexor-pronator mass. The brachial artery lies just beneath the lacertus fibrosus at the level of the elbow flexion crease. The tendon travels just lateral (radial) to the median nerve within the antecubital fossa and passes posterior (deep) to the recurrent radial artery before it attaches to the radial tuberosity. Full forearm supination allows visualization of the tendinous insertion on the radial tuberosity.
Correct answer : A
41
54- MRI results are shown in Figure 1 for a 22-year-old, right-hand dominant collegiate athlete who reports a 6-month history of progressive weakness in his right arm. He denies any specific traumatic event. He has altered his weight-lifting activities and tried over-the-counter ibuprofen without benefit. No appreciable deformity or atrophy is found on examination of the upper extremities. He demonstrates full active shoulder range of motion, and there is no weakness with abduction in the plane of the scapula. Belly press test findings are normal, but weakness is seen in external rotation with the arm in adduction. He does not demonstrate anterior apprehension, and there is no instability with load and shift testing. Radiographs are unremarkable. What is the best surgical option?
A. Arthroscopic labral debridement and biceps tenodesis
B. Shoulder arthroscopy with undersurface cuff debridement and acromioplasty
C. Cyst decompression at the spinoglenoid notch with possible labral repair
D. Cyst decompression at the suprascapular notch with possible labral repair
This patient’s clinical and MRI findings are consistent with a posterior paralabral cyst with compression of the suprascapular nerve, specifically at the spinoglenoid notch. Compression of the suprascapular nerve can occur at either the suprascapular or spinoglenoid notch. Compression of the nerve at the suprascapular notch affects innervation to both the supraspinatus and infraspinatus muscles, resulting in weakness in both shoulder abduction and external rotation. However, compression at the spinoglenoid notch only affects innervation to the infraspinatus muscle, resulting in isolated weakness in external rotation.
Compression at the spinoglenoid notch often is seen in overhead athletes, and studies have shown associated posterior labral tears (Piatt and associates). Several studies have addressed nonsurgical and surgical treatment options. The treatment decision should focus on the underlying cause (Martin and associates)—in this patient, the cyst. Nonsurgical treatment in the presence of a known lesion has been associated with a higher failure rate than addressing the lesion, which can result in functional improvement (Chen and associates, Cummins and associates). The best response in this scenario is decompression of the cyst at the spinoglenoid notch with possible labral repair.
Correct answer : C 42
55- A 45-year-old woman diagnosed with lateral epicondylitis undergoes an open debridement of the extensor carpi radialis brevis. During surgery, resection extends posterior to the equator of the radiocapitellar joint. Postoperatively, she complains of persistent pain, despite appropriate rehabilitation. What other physical examination finding is she likely to have?
A. Pain with elbow extension in forearm pronation B. Mechanical symptoms when rising from a chair C. Valgus instability
D. Tenderness over the medial collateral ligament (MCL)
Excessive resection of the common extensor origin posterior to the equator of the radiocapitellar joint may lead to iatrogenic lateral collateral ligament (LCL) injury, causing posterior lateral rotatory instability (PLRI). Patients may present with lateral elbow pain, a positive lateral pivot shift test, or mechanical symptoms/subjective instability when pushing up from a chair (positive chair rise test). PLRI is often provoked with combined elbow extension and forearm supination, as the posterior support for the radiocapitellar joint has been lost. Therefore, placing the forearm in pronation during elbow extension places the radiocapitellar joint in a more stable position and is less likely to induce pain or mechanical symptoms. Valgus instability and MCL tenderness would be associated with an MCL injury.
Correct answer : B
56- A 75-year-old man presents with complaints of shoulder pain, bruising, and weakness following a fall onto his outstretched hand. He underwent an uncomplicated anatomic total shoulder arthroplasty 5 years prior with good range of motion and strength. His current radiographs are shown in Figures 1 and 2. What is the most appropriate next step to restore this patient’s function?
43
A. Rotator cuff repair
B. Revision to reverse total shoulder arthroplasty
C. Physical therapy
D. Latissimus dorsi transfer
The patient's radiographs demonstrate humeral head elevation and anterior translation, suggesting a massive traumatic rotator cuff tear. In this setting, a rotator cuff repair is unlikely to be successful, and a revision to reverse total shoulder arthroplasty is indicated. A latissimus dorsi transfer can address only a portion of the patient's rotator cuff deficiency. Physical therapy may result in some degree of improvement, but this cannot address the joint instability and malalignment. If the shoulder remains in its current position, progressive glenoid loosening would be expected due to the “rocking horse” phenomenon resulting in eccentric glenoid edge loading. Shields and Wiater compared conversion of an anatomic total shoulder to a reverse total shoulder for rotator cuff deficiency with primary reverse total shoulder arthroplasty and found similar American Shoulder and Elbow Surgeons Standardized Shoulder Assessment and visual analog scale pain scores at 2-year follow-up.
Correct answer : B
57- Figures 1 and 2 are the MRI arthrograms of a 14-year-old male baseball player who notes medial-sided elbow pain that occurs during the early acceleration phase of throwing. Pain has continued for one year. Pain improves with rest but worsens once he returns to throw. The longest he has rested is 3 months. He has completed a physical therapy program focusing on elbow strengthening and range of motion. He denies mechanical symptoms. Physical examination shows full elbow range of motion, no tenderness, and pain with moving valgus stress test, although there is no instability noted. There is no pain with resisted wrist flexion. What is the best next step?
A. Evaluation of shoulder range of motion and strength
B. Arthroscopic debridement and microfracture
C. Ulnar collateral ligament (UCL) reconstruction
D. UCL repair
44
The patient has a clinical history and physical examination consistent with UCL pathology. In an overhead athlete, deficits in the kinetic chain can contribute to the development of medial elbow pathology due to increased force transmission across the elbow. As a result, it is important to examine the shoulder to ensure that total arc of motion remains equivalent to the contralateral arm. Decreases in total arc of motion, commonly associated with glenohumeral internal rotation deficits (GIRD), can predispose athletes to medial elbow injuries. These shoulder deficits can be addressed with physical therapy. The MRI scan shows a structurally intact UCL, therefore, UCL repair or reconstruction is not indicated. The MRI scans demonstrate no evidence of osteochondral injury, which would be an indication for arthroscopic debridement and microfracture.
Correct answer : A
58- A 42-year-old woman sustains a closed posterior elbow dislocation. A closed reduction is performed, and the elbow appears stable under fluoroscopic examination through a full arc of motion. Initial treatment should consist of
A. early mobilization only.
B. surgical repair of medial and lateral collateral ligaments. C. active motion in a hinged brace from 30° to 120°.
D. application of hinged external fixator with early mobilization.
This is a simple (no associated fracture) elbow dislocation. Such dislocations can be treated with closed reduction followed by mobilization after 5 to 7 days to avoid stiffness, provided the elbow is stable through a full arc of motion at the time of reduction. If the elbow is unstable but has a short arc of stability, then using a hinged brace in the stable arc may be considered. It may be necessary to splint the elbow in pronation if the medial collateral ligament (MCL) is intact and the lateral collateral ligament (LCL) is disrupted, or in supination if the LCL is intact but the MCL disrupted. Surgical repair of the LCL and MCL may be required only if the elbow does not have a stable arc at the time of reduction. If the elbow remains unstable after repair, then application of a hinged external fixator may be considered.
Correct answer : A
45
59- A 40-year-old female recreational basketball player notes pain deep within her shoulder that occurs with activity. Pain began insidiously 6 months previously. She has completed a physical therapy program, and an intra-articular corticosteroid injection provided excellent temporary relief. Physical examination shows symmetric range of motion of her shoulder. She has a positive O'Brien’s active compression test. There is no pain with cross-arm adduction or tenderness to palpation over the acromioclavicular joint. Resisted abduction is nonpainful and strong. MRI shows increased signal in the substance of the superior labrum, low-grade bursal surface fraying of the supraspinatus, and mild degenerative changes within the acromioclavicular joint. What is the best treatment option?
A. Biceps tenodesis
B. Superior labrum anterior to posterior (SLAP) repair
C. Rotator cuff repair
D. Distal clavicle excision
The patient has a clinical history and physical examination consistent with degenerative superior labral pathology, which is supported by the MRI scan. She has failed appropriate nonoperative treatment, and surgical intervention would be indicated. In a middle-aged patient with a degenerative superior labral tear, biceps tenodesis has been shown to have better outcomes and return to sport than SLAP repair. In a young patient with a traumatic superior labral tear, repair would be indicated. The other MRI findings noted are incidental and asymptomatic in this patient. As a result, rotator cuff repair or distal clavicle excision is not indicated.
Correct answer : A
60- A 50-year-old man sustained an external rotation traction injury to his right arm. He felt a pop in the anterior aspect of his shoulder associated with immediate pain and swelling. The MRI scan shows a tear of the subscapularis tendon, as shown in Figures 1 and 2. The arrow points to what anatomic structure?
46
A. Biceps tendon
B. Torn anterior labrum
C. Middle glenohumeral ligament
D. Comma/rotator interval tissue
The anatomic structure labeled is the biceps tendon, which has subluxated medially from the intertubercular groove as a result of disruption of the biceps pulley that occurs with subscapularis tears. The anterior labrum is adjacent to the glenoid and is not normally torn with subscapularis pathology. The middle glenohumeral ligament may appear cord-like, but is shown more medial to the subluxated biceps tendon. The rotator interval tissue, or "comma" tissue, is generally along the upper border of the subscapularis and is pulled toward the coracoid base in subscapularis tears.
Correct answer : A
61- Injuries to what two structures would result in a “floating shoulder"?
A. Clavicle shaft and humeral shaft
B. Scapular body and humeral shaft
C. Rotator cuff and coracoacromial ligament
D. Clavicle shaft and glenoid neck
The superior shoulder suspensory complex (SSSC) is a bone and soft-tissue ring secured to the trunk by superior and inferior bony struts, from which the upper extremity is suspended. The ring is composed of the glenoid process, coracoid process, coracoclavicular ligaments, distal clavicle, acromioclavicular joint, and acromial process. Double lesions of the SSSC are referred to as “floating shoulder” injuries, as in this case in which the injury involves a fractured scapular neck and ipsilateral clavicle fracture. Ipsilateral acromioclavicular dislocation and coracoid fracture is a less common double disruption of the SSSC. Although several case studies have been published on surgical and nonsurgical management of these injuries, no study provides measurable surgical indications beyond the simple presence of the double lesion. This is often referred to as an unstable shoulder girdle. Correct answer : D
47
62- A 25-year old right-hand dominant professional baseball pitcher complains of posteromedial right elbow pain that is worsened by throwing. He also reports occasional paresthesias in his small and ring finger after lengthy bullpen sessions. On examination, he is tender along the medial olecranon and complains of pain when extending the elbow >-
20° of extension. He has negative valgus stress, moving valgus stress, and milking maneuver tests. He is stable to varus stress, chair rise, and lateral pivot shift tests. Radiographs reveal a small osteophyte along the posteromedial border of the olecranon. What is the most likely diagnosis?
A. Valgus extension overload
B. Varus posteromedial rotatory instability (VPMRI) C. Valgus posterolateral rotatory instability (VPLRI) D. Olecranon bursitis
The patient has valgus extension overload. This is a spectrum of pathologies, often seen in pitchers, that begins with posteromedial impingement between the medial olecranon and posterior trochlea during forceful elbow extension. As a result, a medial olecranon osteophyte is typically the first notable imaging finding. As pathology increases, there can be progressive damage to the medial collateral ligament (MCL), degeneration of the radiocapitellar articulation, and neuritis of the ulnar nerve. VPMRI is often associated with a large anteromedial coronoid fracture and posterior band MCL rupture. VPLRI occurs when the lateral collateral ligament complex is ruptured. Olecranon bursitis presents with focal swelling or a fluid collection over the posterior aspect of the olecranon.
Correct answer : A
63- A patient sustains a displaced diaphyseal humerus fracture following a motor vehicle accident. Open reduction internal fixation is indicated due to concomitant lower extremity trauma and is planned through an anterior approach. Which intramuscular interval is exploited during the deep dissection of the mid-humerus in this approach?
A. Lateral head of triceps (radial nerve) and brachialis
(musculocutaneous nerve)
B. Lateral head of the triceps (radial nerve) and biceps brachii
(musculocutaneous nerve)
C. Lateral brachialis (radial nerve) and medial brachialis
(musculocutaneous nerve)
D. Brachialis (musculocutaneous nerve) and coracobrachialis
(musculocutaneous nerve)
48
The anterior approach to the mid-humerus courses along the lateral margin of the biceps brachii. This muscle is swept medially allowing exposure of the brachialis. The brachialis has a dual innervation, with the lateral fibers innervated by the radial nerve and the medial fibers innervated by the musculocutaneous nerve. The humerus is exposed by splitting this muscle in its midline. The lateral head of the triceps resides in the posterior compartment of the arm and is not involved in the anterior approach to the humerus. The interval between brachialis and coracobrachialis is not an internervous plane, as both muscles are supplied by the musculocutaneous nerve.
Correct answer : C
64- Figures 1 and 2 are the current radiographs of a 35-year-old right- hand dominant woman who sustained an acute dislocation to her right elbow after falling from a horse. She underwent a closed reduction and splinting in the emergency department. She describes global elbow pain and difficulty with range of motion. On examination, she has moderate, diffuse elbow swelling with deformity. There are no traumatic wounds, and distally she is neurovascularly intact. Definitive treatment should include
A. repeat closed reduction and casting. B. radial head arthroplasty or fixation. C. radial head excision.
D. arthroscopic loose body removal.
49
This is a young patient who has sustained an elbow dislocation with a radial neck and coronoid fracture to her dominant extremity. Her current radiographs reveal a considerably displaced radial head fragment, along with a small coronoid fracture, and potentially some residual ulnohumeral joint incongruity. A repeat closed reduction is unlikely to be successful, as the radial head is significantly displaced and can block a congruent reduction. Open reduction is required to successfully address this complex injury pattern. Although removal of the radial head can be considered, fixing or replacing the radial head with repair of the lateral collateral ligament is often recommended in the setting of acute trauma to restore adequate stability to the elbow, decrease long-term risk for progressive ulnohumeral arthrosis, and limit sequelae in the setting of an unappreciated longitudinal forearm axis injury.
Correct answer : B
65- Figures 1 and 2 are the radiographs of a 67-year-old woman who underwent shoulder hemiarthroplasty for a proximal humerus fracture dislocation 6 months ago. She now has persistent pain with a pseudoparalytic shoulder. Examination reveals full passive range of motion, but with pain in all directions. Joint aspiration was performed with <50 neutrophils and negative aerobic and anaerobic cultures (anaerobic held for 14 days). What would be her best surgical option for pain relief and improved function?
A. Anatomic total shoulder arthroplasty
B. Revision hemiarthroplasty with allograft prosthetic composite on the humeral side
C. Reverse total shoulder arthroplasty
D. Resection arthroplasty
50
The radiographs provided show lysis of the greater tuberosity and a high-riding humeral head, indicating failure of the rotator cuff. Both anatomic shoulder arthroplasty and revision hemiarthroplasty would suffer from the same functional limitations and risk of instability as the current construct, due to the lack of a functional rotator cuff. Resection arthroplasty is usually reserved for situations of recurrent infection or lack of enough structural bone to allow prosthetic placement. Revision to a reverse total shoulder arthroplasty can bypass the cuff deficiency and treat any component of glenohumeral degeneration and is the best option to reduce pain and improve function in this setting. Correct answer : C
66- A 65-year-old woman has an atraumatic full thickness rotator cuff tear, which is treated successfully with 12 weeks of physical therapy. In discussing future expectations regarding the condition of her rotator cuff, what is the risk of tear progression at 2 years?
A. 0% B. 5%
C. >20% D. >50%
Several studies have demonstrated that degenerative symptomatic rotator cuff tears enlarge over time, which raises some concern regarding treating these injuries nonsurgically. The rate of rotator cuff tear enlargement at 2 years ranges from 20% to 49%, and at 5 years is estimated to be 50%. The risks associated with rotator cuff tear progression includes worsening fatty atrophy and fatty infiltration, decreased tendon pliability, and increased tendon retraction, which can lead to worse clinical outcomes following surgery.
Correct answer : C
67- A 63-year-old right-hand dominant woman has a history of gradually progressive atraumatic right shoulder pain. She describes a constant nagging pain that radiates to her deltoid insertion and difficulty with overhead activities. Her examination and imaging studies confirm a rotator cuff tear. What is the mostly likely initiating anatomic location of her tear?
A. Anterior portion of the supraspinatus tendon adjacent to the biceps tendon
B. 15 mm posterior to the biceps tendon near the supraspinatus/infraspinatus junction
C. Superior portion of the subscapularis tendon
D. 30 mm posterior to the biceps tendon near the supraspinatus/infraspinatus junction
51
Fundamental to understanding the pathogenesis of rotator cuff tears is an appreciation of the likely initiation site of the disease process. Although authors initially postulated that rotator cuff tears originated in the anterior margin of the supraspinatus tendon near the biceps tendon, recent research has challenged this notion. Kim and associates analyzed 360 full-thickness or partial-thickness rotator cuff tears using ultrasonograms. They separated stratified tears based on their anteroposterior size and whether they were partial- or full-thickness tears. The mean width and length of tear size was 16.3 mm and 17 mm, respectively. Histograms showed that the most common tear location for all tears regardless of size was approximately 15 mm posterior to the biceps tendon. This corresponds to the center of the rotator crescent initially described by Burkhart and associates. This location is described as being more susceptible to degeneration secondary to its diminished vascular supply and mechanical properties. The rotator cable is an arch-shaped thick bundle of fibers that is thought to shield the crescent from stress.
Correct answer : B
68- Figures 1 and 2 are the radiograph and MRI scan of a 40-year-old man who fell down a flight of stairs. His upper arm is bruised and painful, and global weakness in the shoulder girdle function is noted. What is the appropriate initial treatment for the acromial finding identified here?
A. Immediate open reduction and internal fixation of the fracture
B. Closed treatment with serial radiographs
C. Fracture fragment excision and deltoid repair
D. Rest, anti-inflammatory medications, and a home exercise program
52
The patient has an os acromiale. The type shown is of the meso-acromion. This is not an acute fracture; well corticated ends are seen on the axillary radiograph, and there is no bone edema on the T2 axial MRI scan. A trial of nonsurgical care that includes rest, ice, and anti-inflammatory medications is recommended. If a patient continues to have symptoms, an arthroscopic evaluation is needed to determine if the os acromiale is mobile and if surgical fixation is appropriate. Correct answer : D
69- A 38-year-old man sustains a terrible triad injury consisting of an elbow dislocation, comminuted and displaced radial head fracture, and a type I coronoid fracture. Intraoperative findings after radial head replacement and lateral collateral ligament complex repair reveal persistent instability consisting of medial opening on valgus stress and posteromedial subluxation of the ulnohumeral and radiocapitellar joints. What is the best next step?
A. Medial collateral ligament repair or reconstruction
B. Reconstruction of the radial collateral ligament
C. Resection of the type I coronoid fracture and capsular repair to the remaining coronoid
D. Open reduction and buttress plating of the coronoid fracture
Terrible triad injuries of the elbow are common, and the management of type I coronoid tip fractures remains controversial. Type I coronoid fractures result in only small changes in elbow kinematics that have been shown to be uncorrected with suture repair. A type I coronoid tip fracture is not amenable to buttress plate fixation. The radial collateral ligament is a component of the lateral collateral ligament complex and has already been repaired. The persistent medial laxity and posteromedial joint subluxation noted is indicative of ongoing instability. The next step would be repair or reconstruction of the medial collateral ligament, which will normally correct the medial instability. Articulated versus static external fixation can be considered if the joint remains unstable despite repair/reconstruction of the damaged stabilizing structures. Correct answer : A
53
70- The fracture seen in Figure 1 is most likely associated with injury to what ligamentous structure?
A. Inferior glenohumeral ligament
B. Acromioclavicular (AC) ligaments
C. Coracoclavicular ligaments
D. Coracoacromial ligament
The radiograph shows an extra-articular distal clavicle fracture lateral to the clavicular attachment point of the coracoclavicular ligaments (conoid and trapezoid). However, unlike a scenario featuring a typical Neer type I fracture, the interval between coracoid and clavicle is clearly widened, and there is marked fracture displacement. This signifies disruption to the coracoclavicular ligaments. The inferior glenohumeral ligament is important to glenohumeral joint stability, but has no effect on the relationship between clavicle and scapula. The AC ligaments are thickenings of the AC joint capsule. They have been shown to be responsible for 90% of anteroposterior stability of the AC joint. The coracoclavicular ligaments are responsible for 77% of stability for superior translation (as in this case). The coracoacromial ligament connects two parts of the scapula (coracoid and acromion) and is part of the arch that supports the rotator cuff.
Correct answer : C
71- What is the most common organism implicated in periprosthetic infection of the shoulder?
A. Methicillin-resistant Staphylococcus aureus (MRSA) B. Cutibacterium acnes
C. Enterococcus species
D. Staphylococcus epidermidis
C acnes is the most common organism recovered in prosthetic shoulder infections (33%), Coagulase-negative Staphylococcus is second (21%), Methicillin-sensitive S aureus (13%), and S epidermidis (10%). MRSA accounts for 5% and Enterococcus species, 1.5%.
Correct answer : B
54
72- Figure 1 is the MR image of a 55-year-old man who sustained an acute traumatic injury to his right shoulder with loss of active range of motion. He was initially evaluated by his primary care physician and treated with physical therapy without success. He was referred to an orthopaedist for surgical consultation 8 weeks after sustaining the injury. The orthopaedic surgeon performs a successful arthroscopic repair but notes poor tendon quality at the repair site. The treating surgeon keeps the patient in a sling full time for 6 weeks without formal therapy. One year after surgery, in comparison to early therapy, this rehabilitation program will likely result in
A. no difference in terminal range of motion.
B. a lower functional outcome score. C. a clinically significant reduction in
passive forward flexion and external rotation.
D. a higher retear rate of the rotator cuff repair.
Historically, orthopaedic surgeons considered early range-of-motion programs following rotator cuff surgery secondary to concerns about potential postsurgical stiffness. Although this may have been a concern with primary open repair, arthroscopic surgery appears to substantially decrease this risk. More recently, investigators are reporting similar results in terms of range of motion, retear rate, and functional outcome scores among patients who undergo early versus delayed rehabilitation programs.
Correct answer : A
73- Stemless shoulder arthroplasty prostheses have recently been suggested as an alternative to traditional stemmed replacement. Advantages of the stemless surgical technique would include
A. better glenoid exposure than with stemmed prostheses.
B. reliable use in four-part proximal humerus fracture reconstruction.
C. use in proximal humeral malunion without the need for an osteotomy. D. improved long-term survivorship profile.
55
Glenoid exposure, while better than with surface replacements, is not improved over traditional stemmed replacements. Metaphyseal comminution would make it unlikely that a stemless implant could be used in most four-part fractures. Stemless replacement does have the unique advantage of allowing placement of a prosthesis in the setting of a proximal humerus malunion without the need for an osteotomy, as the prosthesis is not constrained by the position of the stem. While early results are encouraging, there is no long-term data to suggest that survivorship is increased with stemless arthroplasty. Correct answer : C
74- Figure 1 is the MRI scan of a 25-year-old left-hand dominant minor league pitcher with a 6 month history of progressive left elbow pain during pitching. He fails nonoperative treatment and undergoes surgery to address the problem. What is the most common complication of this procedure?
A. Ulnar nerve neuropraxia
B. Flexor pronator mass avulsion
C. Posterolateral rotatory instability
D. Symptomatic hardware
The MRI scan shows evidence of a medial collateral ligament (MCL) tear. In a patient with a chronic MCL injury that has failed non-operative treatment, MCL reconstruction would be indicated. Initial MCL reconstruction technique involved routine transposition of the ulnar nerve and detachment of the flexor- pronator mass. Subsequent.
technique modifications have been made to minimize complications by avoiding routine ulnar nerve transposition and performing a muscle-splitting approach. Despite these improvements, transient ulnar nerve neuropraxia remains the most common complication, and patients should be counseled about its occurrence pre-operatively. Flexor pronator mass avulsion is more likely with a muscle-detaching approach, but is not more common than ulnar nerve neuropraxia. Posterolateral rotatory instability is a complication of lateral collateral ligament repair or reconstruction, not medial collateral ligament reconstruction. Symptomatic hardware is not a common complication from this procedure
Correct answer : A
56
75- A 35-year-old man presents one week after an acute right shoulder posterior dislocation after being electrocuted. He is evaluated in the emergency department and undergoes closed reduction. The patient reports global right shoulder pain and limited active and passive range of motion. He has mild anterior and lateral bruising. He is distally neurovascularly intact. Current radiographs and an MRI scan are shown in Figures 1 through 3. What is the best next step?
A. Open reduction internal fixation
(ORIF)
B. Sling immobilization in external rotation
C. Bristow-Latarjet
D. Shoulder hemiarthroplasty
The patient has sustained a displaced lesser tuberosity fracture with medial displacement following a posterior shoulder dislocation. Nonoperative management would risk long-term loss of normal subscapularis function, as well as anterior shoulder instability. An ORIF of lesser tuberosity is recommended. The current radiographs do not demonstrate any obvious compromise of glenoid bone stock that would necessitate a coracoid transfer. The humeral head is not compromised; therefore, a hemiarthroplasty is not
indicated. Correct answer : A 57
76- A 51-year-old man sustains the injury shown in the MRI scan in Figures 1 and 2 following a fall. After a thorough discussion regarding risks and benefits, he elects to proceed with surgery. What is the most appropriate surgical treatment for his fracture?
A. Open reduction internal fixation with locking plate
B. Intramedullary (IM) nail
C. Hemiarthroplasty
D. Closed reduction and percutaneous pinning
The patient has sustained a complex proximal humerus fracture with head split component and multiple articular fragments. When the articular surface is significantly compromised, arthroplasty procedures are favored. The only procedure listed that addresses the damaged humeral head is hemiarthroplasty, making it the correct response. Although a possible option, ORIF would be difficult due to the fragmented humeral head, and there would be a high risk for fracture collapse or avascular necrosis. IM nailing will not provide enough control of the fracture pieces, nor will it replace the damaged articular surface. Closed reduction is not an option given the complex nature of the fracture.
Correct answer : C
77- A 68-year-old man presents with chronic progressive right shoulder pain and loss of motion. He has active shoulder elevation of 120° and 5-/5 shoulder forward flexion strength limited by pain. He has exhausted nonsurgical management over the past year and is now interested in surgical intervention. Figure 1 is the preoperative axial CT scan of his shoulder. During surgical reconstruction, the surgeon should anticipate the location of maximal glenoid erosion to be
58
A. posterior. B. superior.
C. posterior inferior. D. posterior superior.
In patients with primary osteo- arthritis of the shoulder, eccent- ric wear on the face of the glenoid is frequently combined with static subluxation of the humeral head. Current studies have clarified that patients with Walch B2 glenoid develop wear along the posterior inferior face of the glenoid and not directly posterior. At the time of shoulder arthroplasty, the eccentric center of rotation must be corrected by soft-tissue, bony, and/or implant
techniques to minimize the risk for poor outcomes. The surgeon should orient
his correction along the posterior inferior to anterior superior plane.
Correct answer : C
78- For humeral shaft fractures, the characteristic most associated with radial nerve palsy is
A. open fracture.
B. distal one-third fracture.
C. proximal one-third fracture. D. comminuted fracture.
Distal third humeral shaft fractures are associated with the highest incidence of radial nerve palsy at 23.6% The classic example is a Holstein Lewis fracture, which is a spiral fracture of the mid-third / distal-third junction. Open fractures are not associated with a higher incidence of radial nerve palsy than closed fractures. Comminution has not been associated with an increase in radial nerve palsy. In fact, transverse and spiral fractures are associated with a higher incidence of radial nerve palsy than comminuted fractures. Proximal humerus fractures have an incidence of only 1.8%.
Correct answer : B
59
79- Figures 1 and 2 are the radiograph and axial CT scan of a 75-year-old woman with diffuse superior shoulder pain 5 months after an uneventful reverse shoulder arthroplasty. She denies trauma, but felt a "pop" when reaching overhead. She had initially done well postoperatively. On physical examination, she has decreased active forward flexion with pain and diffuse superior tenderness along the scapular spine and acromion. There are no signs or symptoms of infection. What is the best next step in management?
A. Application of bone stimulator
B. Open reduction and internal fixation
(ORIF)
C. Physical therapy for deltoid strengthening
D. Sling immobilization for 6 weeks
The radiograph shows a well-positioned reverse total shoulder and the axial CT image demonstrates a minimally displaced fracture through the midacromion. Acromial fracture is a concerning and not uncommon complication that can have devastating effects after reverse shoulder arthroplasty, as function is highly dependent on the deltoid muscle. Fractures can occur at the scapular spine, which may be related to placement of peripheral baseplate screws. Acromial fracture has been reported to occur as early as 1 month postoperatively and as late as 8 years postoperatively. The reported incidence is <8%, and multiple authors note decreases in shoulder elevation and shoulder outcome scores compared with those in patients with reverse shoulder arthroplasty without a fracture. Patients with a fracture can complain of superior shoulder pain that may radiate to the deltoid area and usually report an acute onset of pain or loss of function after initially good clinical progress. The diagnosis can be difficult to determine and is missed on plain radiographs in up to 20% of cases. CT scans are helpful. Treatment is typically nonoperative with sling immobilization for 6 weeks and then
60
advancing activities as tolerated. A bone stimulator and ORIF would not be indicated initially, but could be used if healing does not progress as expected. Continued physical therapy with strengthening would be contraindicated until fracture union is achieved.
Correct answer : D
80- A 76-year-old right-hand dominant woman falls at home, sustaining a displaced 4-part left proximal humerus fracture. When compared with initial treatment with a reverse shoulder arthroplasty, revising a failed open reduction and internal fixation (ORIF) to a reverse shoulder arthroplasty results in
A. higher complication rate.
B. improved functional outcomes. C. lower rates of instability.
D. decreased rate of revision surgery.
When compared to initial treatment with reverse total shoulder arthroplasty, patients who initially undergo ORIF with subsequent revision to reverse total shoulder arthroplasty demonstrate a higher complication rate, increased rate of revision surgery, increased risk of instability, and similar functional outcomes.
Correct answer : A
81- A 45-year-old man with a history of gout in his foot 2 years ago presents with a 3-day history of atraumatic elbow pain. The pain is diffuse, constant, and worse with any movement. Examination shows motion from -20° extension to 90° flexion with pain. There is no erythema around his elbow, but there is mild warmth. He has no fever, and neurovascular examination is unremarkable. Radiographs show an effusion. Serum uric acid level is within normal limits. What is the next diagnostic step?
A. Elbow joint aspiration
B. MRI scan
C. Splint for 2 weeks and repeat examination
D. Sedimentation rate and C-reactive protein level
The patient appears to be experiencing a recurrent gout flare. The best way to confirm the diagnosis is to aspirate the joint and send it for culture, cell count, and crystal examination. This will identify the diagnosis of infection, gout, or pseudogout. An MRI scan will confirm the presence of an effusion, but it will not reveal the cause. A splint may result in pain improvement, but it will not contribute to a diagnosis or definitive treatment. Sedimentation rate and
61
C-reactive protein levels can be elevated in either inflammatory or infectious processes, but these are non-specific and cannot differentiate between the two.
Correct answer : A
82- Figures 1 through 5 are the radiographs and CT scans of a 59-year- old woman who has had 10 years of worsening right shoulder pain. She reports a progression of symptoms, despite multiple corticosteroid injections, nonsteroidal anti-inflammatory drugs, and physical therapy. Her active and passive forward elevation is 100°, external rotation with the arm at the side is 20°, and internal rotation is to L5. What is the best next step?
A. Arthroscopic shoulder debridement
B. Rotator cuff repair
C. Shoulder hemiarthroplasty
D. Total shoulder arthroplasty
62
The patient's radiographs and CT scan show advanced glenohumeral osteoarthritis with posterior humeral head subluxation and mild posterior glenoid erosion (Walch type B2 glenoid). The preferred type of shoulder arthroplasty in this setting remains controversial, as there are data to support both anatomic and reverse total shoulder arthroplasty. There is no significant atrophy of the rotator cuff musculature on sagittal CT to suggest a rotator cuff tear, and a rotator cuff repair is likely contraindicated by the degree of underlying arthritis. A glenohumeral joint debridement would be expected to provide only partial/short-term pain improvement, and is unlikely to be a long- term solution. A shoulder hemiarthroplasty has been shown to result in worse pain relief and functional outcomes than total shoulder arthroplasty in this setting.
Correct answer : D
83- A 23-year-old minor league pitcher describes the insidious onset of posterior shoulder pain during the late cocking phase of his throwing motion. He has gone 6 weeks without throwing, but symptoms quickly returned on return to play. An MR arthrogram of the shoulder reveals fraying of the superior labrum and proximal biceps, and a partial- thickness articular-sided supraspinatus tear (30% tendon thickness). Figure 1 is a representative coronal MRI slice. Clinical examination demonstrates mild weakness of the periscapular muscles, mild superior rotator cuff weakness, and negative instability testing. Internal rotation with the arm in 90⁰ of abduction is 40⁰ in the affected shoulder versus 70⁰ in the contralateral shoulder. What is the best next step?
A. Intra-articular platelet rich plasma (PRP) injection
B. Therapy regimen focused on shoulder range of motion and strengthening
C. Arthroscopic surgery for rotator cuff and labral debridement
D. Arthroscopic surgery for rotator cuff repair and biceps tenodesis
63
Internal impingement is a condition that affects overhead throwing athletes, as the greater tuberosity and articular surface of the rotator cuff contact the posterosuperior glenoid during maximal shoulder abduction and external rotation. The etiology is typically multifactorial, but common contributors include posterior capsular contracture, scapular dyskinesia, and subtle anterior shoulder laxity. Nonoperative management, the mainstay of treatment, includes rest, stretching, scapular strengthening, and proprioception. Results of surgical intervention are variable; therefore, nonoperative measures should be exhausted first. While PRP is currently being investigated as a biologic augmentation in a number of shoulder pathologies, it is not considered first- line treatment.
Correct answer : B
84- A 45-year-old woman with diabetes has a 3-month history of atraumatic left shoulder pain and motion loss. She previously underwent treatment with nonsteroidal anti-inflammatory medication and a home stretching program, experiencing minimal relief of her symptoms. Examination reveals loss of passive external rotation, abduction, and forward elevation without reduction in strength. Radiographs are normal. What is the most appropriate next step?
A. MRI scan with and without contrast
B. Cortisone injection therapy with continued physical therapy (PT) C. Closed manipulation under anesthesia
D. Arthroscopic release with manipulation under anesthesia
The patient's history and physical exam are consistent with adhesive capsulitis, or frozen shoulder. Adhesive capsulitis is most commonly an idiopathic process that results in joint pain and loss of motion from capsular contracture. It is reported to affect approximately 2% to 5% of the general population, typically affecting middle-age women. Secondary causes include previous trauma, as well as associated medical conditions such as diabetes, stroke, and cardiac and thyroid disease. Debate remains as to whether a genetic predisposition for the development of adhesive capsulitis exists, despite the increased frequency noted in twin studies. Although the underlying etiology and pathophysiology are not well understood, the consensus is that synovial inflammation and capsular fibrosis result in pain and joint volume loss. It is hypothesized that in patients with diabetes, an increased rate of glycosylation and cross-linking of the shoulder capsule raises the incidence of frozen shoulder.
The natural history of adhesive capsulitis is spontaneous resolution, therefore, conservative measures are the mainstay of treatment. As the patient has seen little benefit from NSAIDs and a home exercise program, more aggressive intervention is reasonable. In terms of injections, glenohumeral corticosteroid
injection, subacromial corticosteroid injection, and hydrodilation have all 64
demonstrated benefit. Radiographs are usually obtained to exclude other causes of shoulder pain such as glenohumeral arthrosis, malignancy, calcific tendonitis, impingement, and acromioclavicular degeneration. If pain and stiffness persist beyond 6 months, surgical intervention may be considered in the form of closed manipulation or arthroscopic release. Complications of closed manipulation include humerus fracture, glenohumeral dislocation, hematoma, rotator cuff and labral tears, and brachial plexus injury. Arthroscopic release is advocated by some, as it allows for examination of concomitant pathology and controlled release of capsular tissue, with the potential for reduced force when performing the manipulation portion of the procedure. Controversy remains as to whether posterior capsular release should be routinely performed because studies have shown outcomes to be similar with anterior and combined approaches. Therapy should be initiated early after intervention, with some surgeons advocating admission to the hospital with inpatient therapy for pain management and compliance.
Correct answer : B
85- Figures 1 and 2 are the radiographs of a 48-year-old right-hand dominant man who reports progressive pain and stiffness of the elbow. He sustained a fracture dislocation 10 years ago, which was treated with surgical reconstruction. On examination, range of motion is from 40° extension to 110° flexion, with pain at end-range of motion, but no pain through mid-range. A previous corticosteroid injection temporarily improved his pain but did not improve range of motion. The patient elects to undergo an arthroscopic osteocapsular arthroplasty. What structures need to be addressed to improve elbow extension?
65
A. Anterior capsule and osteophytes within anterior compartment
B. Posterior capsule and osteophytes within posterior compartment C. Anterior capsule and osteophytes within posterior compartment D. Posterior capsule and osteophytes within anterior compartment
The patient is young, active, and has evidence of post-traumatic elbow osteoarthritis. His motion is limited by capsular contracture and large osteophytes in the anterior and posterior compartments. He has failed nonoperative treatment, and surgery is indicated to improve his range of motion and function. Arthroscopic osteocapsular arthroplasty allows removal of impinging osteophytes and release of hypertrophied capsule and has been shown to be effective at relieving pain and improving motion in patients with mild to moderate osteoarthritis. Anterior capsular contracture and posterior bony impingement limit extension and must be addressed to improve motion. Posterior capsular contracture and anterior osteophytes limit flexion.
Correct answer : C
86- Figures 1 through 4 are the radiographs of a 47-year-old right-hand dominant man who was involved in an altercation. What is the most appropriate method to address his radial head injury?
66
A. Immobilization followed by functional therapy B. Open reduction and internal fixation (ORIF) C. Radial head excision
D. Radial head arthroplasty
The images demonstrate a comminuted radial head fracture with extension into the radial neck. There is persistent fracture displacement following closed reduction of the elbow. The preferred treatment of radial head fractures with >3 parts in active individuals is radial head arthroplasty. ORIF has higher rates of failure when used for 3- and 4-part fractures. Radial head excision is typically discouraged in the acute setting, as this can contribute to elbow and forearm axis instability.
Correct answer : D
87- A 26-year-old recreational athlete sustained an initial shoulder dislocation 1 year ago and was treated nonsurgically. He recently sustained a second dislocation and is scheduled for surgical repair. Plain radiographs and MRI scans reveal no bony defect. What is the difference in rates of recurrent instability after open versus arthroscopic repair?
A. Recurrence after open surgery is twice that of arthroscopic repair
B. Recurrence after arthroscopic surgery is twice that of open repair
C. Recurrence after arthroscopic repair generally occurs at an earlier time than after open repair
D. There is no difference in recurrence after open and arthroscopic repair
Traditionally, recurrence rates associated with open stabilization procedures have been lower than rates associated with arthroscopic repair. Recent studies show that for patients without significant bone loss, however, the recurrence rate is the same for open and arthroscopic surgeries.
Correct answer : D
88- How does concomitant ulnar nerve pathology affect the outcome of patients treated operatively for medial epicondylitis?
A. Concomitant ulnar nerve pathology has no impact on outcome. B. Concomitant moderate or severe ulnar neuropathy treated with
transposition leads to worse outcomes compared with no ulnar nerve pathology.
C. Concomitant moderate or severe ulnar neuropathy treated with transposition leads to improved outcomes compared with no ulnar nerve pathology.
D. Concomitant mild ulnar neuropathy treated with transposition leads to improved outcomes than no ulnar nerve pathology. 67
89- Figures 1 and 2 are the radiographs of a 64-year-old woman with a history of rheumatoid arthritis (RA) who complains of right elbow pain. She has been treated with tumor necrosis factor-alpha inhibitors and oral corticosteroids for several years. What process is primarily responsible for the radiographic joint destruction?
A. Traumatic insult resulting in complement activation
B. Mutation in the rheumatoid factor gene
C. Osteoblast paracrine signaling resulting in proteolytic collagen degradation
D. Inflammation resulting in a hyperplastic synovial joint lining
RA is a systemic inflammatory disorder marked by erosive arthritis in multiple joints. Elbow involvement is common. The pathologic lesion in RA is pannus, a hyperplastic synovial proliferation that ultimately results in proteoglycan and collagen digestion. Rheumatoid factor mutations, traumatic insults resulting in complement activation, and osteoblast paracrine signaling are not involved in the pathologic process. The Larsen classification assesses the progression of rheumatoid changes in the elbow. Stage I is characterized by osteopenia without joint space narrowing. Stage II indicates joint space narrowing but a normal joint contour. Stage III is marked by joint space loss. This patient has stage IV disease, as seen by the advanced erosive changes with trochlear groove deepening and resulting deformity. Stage V is ankylosis.
Correct answer : D
68
90- Figures 1 through 4 are the radiographs and CT scan of a 63-year-old right-hand dominant man with long- standing left shoulder pain, which now limits his activities of daily living. Examination shows elevation to
150° with markedly limited internal and external rotation. Strength testing is limited by pain. Previous treatments have included physical therapy, steroid injections, and platelet-rich plasma (PRP) injections. An MRI scan shows a partial articular supraspinatus tendon avulsion (PASTA) lesion measuring <50% tendon thickness, a superior labrum anterior to posterior (SLAP) tear, and glenohumeral degeneration with multiple intra-articular loose bodies. What is the best next step?
A. Stem cell injection
B. Arthroscopic rotator cuff repair, biceps tenodesis, and extensive debridement with removal of loose bodies
C. Anatomic total shoulder arthroplasty
D. Reverse shoulder arthroplasty
69
In a patient with end-stage glenohumeral arthritis, the preferred treatment after failing nonoperative treatment would be anatomic shoulder arthroplasty. Recent literature has demonstrated good outcomes even in the setting of partial rotator cuff tears, with or without repair. Stem cell injections are costly and have not been shown to be effective. Arthroscopic treatment may improve pain and function in the short term, but results are unlikely to be long-lasting. Reverse shoulder arthroplasty could be considered; however, there are more long-term studies supporting anatomic total shoulder arthroplasty in this patient population.
Correct answer : C
91- A 75-year-old man sustains an anterior dislocation of his reverse total shoulder arthroplasty. What activity places the arm in the position most commonly associated with instability of a reverse total shoulder arthroplasty?
A. Scratching the opposite shoulder
B. Pushing off ipsilateral chair armrest while standing up
C. Tying shoelaces on the contralateral foot
D. Reaching up to comb hair
Proper soft-tissue tension is critical to prevent instability of a reverse total shoulder. The arm position implicated in reverse total shoulder instability is extension, adduction, and internal rotation, such as pushing out of a chair. The other positions described do not involve extension of the shoulder.
Correct answer : B
92- What is the best way to treat patients with a positive nasal swab for methicillin-resistant Staphylococcus aureus (MRSA) prior to elective shoulder arthroplasty?
A. No treatment is necessary.
B. Apply 5% povidone-iodine solution to each nostril for 10 seconds 1 hour before surgery.
C. Prescribe one week of doxycycline prior to surgery.
D. Apply 2% mupirocin ointment to each nostril on the morning of surgery.
Patients with a positive nasal swab for MRSA can be treated preoperatively with 2% mupirocin to the nares twice daily for 5 days, or 5% povidone-iodine solution to each nostril for 10 seconds per nostril, 1 hour before surgery. S aureus is a gram-positive bacterium capable of both aerobic and anaerobic metabolism. The addition of MRSA and/or methicillin-sensitive S aureus nasal screening, along with a perioperative decolonization protocol, has resulted in a
69% decrease in surgical site infection. It has been shown that prevention programs for staphylococcal periprosthetic joint infections can result in
substantial cost savings. Correct answer : B
70
93- Figure 1 is the clinical photograph of a 22-year-old college pitcher who complains of posterior shoulder pain and feelings of shoulder weakness. He denies shoulder trauma. Evaluation should include
A. CT scan of the shoulder.
B. ultrasonography of the rotator cuff.
C. vascular studies of the upper extremity.
D. electrodiagnostic studies.
The patient has atrophy of the infraspinatus. This would be consistent with either a massive rotator cuff tear or suprascapular neuropathy/compression. Given the
patient's age and the atraumatic onset of symptoms, a significant rotator cuff injury is unlikely, making a suprascapular nerve issue the most likely diagnosis. Electrodiagnostic studies would be most accurate in confirming nerve compression and would aid in localizing the area of compression between the spinoglenoid notch and the suprascapular notch. An MRI scan also would be beneficial to evaluate for any compressive lesion on the nerve, such as a paralabral cyst. Because rotator cuff pathology is unlikely, ultrasonography of the rotator cuff would be of little benefit. CT scan of the shoulder may allow grading of the atrophy of the muscle, but will not be as sensitive for a paralabral cyst/labral tear. Vascular studies would not aid in the diagnosis.
Correct answer : D
94- Figures 1 and 2 are the CT and MRI scans of a 23-year-old man with a history of recurrent anterior shoulder dislocations. He had his first dislocation while in basic training for the military 4 years ago. Since that time, his shoulder has dislocated with less and less provocation, to the point that it now dislocates in his sleep. Examination demonstrates significant apprehension with abduction/external rotation. What is the most appropriate treatment to prevent recurrent shoulder instability?
71
A. Arthroscopic Bankart repair
B. Latarjet
C. Hill-Sachs remplissage
D. Physical therapy
The patient has historical and clinical evidence of significant anterior shoulder instability. The imaging demonstrates significant anteroinferior glenoid bone loss, with a very shallow Hill-Sachs deformity. Patient factors that contribute to recurrent instability
risk include type of sport/activity, age at the time of first dislocation, hyperlaxity, and glenoid bone loss (and/or bipolar bone loss), and these can be utilized to determine if an arthroscopic or open solution is most appropriate. In this patient, restoring glenoid bone stock appears to be the most important variable in stabilizing the shoulder. “Critical” glenoid bone loss has frequently been reported to be >20-25%. In this case, significant bone loss can be suspected from the patient's history, including the number of dislocations, ease of dislocation and reduction, and instability in mid-range of motion.
Correct answer : B
95- How do outcomes and postoperative care of patients undergoing total elbow arthroplasty differ depending on diagnosis?
A. Those performed for inflammatory arthritis have a lower revision rate than those for osteoarthritis.
B. Activity modifications are not required in elbow replacements done for osteoarthritis.
C. Those performed for inflammatory arthritis have a higher failure rate than those for fracture sequelae.
D. Outcomes are similar despite indication.
Over the years, indications for total elbow arthroplasty (TEA) have evolved. With the introduction of better medications for rheumatoid arthritis and other inflammatory arthritides, end-stage arthritis of the elbow from this pathology has become less common. At the same time, there has been increased interest in TEA for treatment of acute distal humerus fractures, and ongoing use for fracture sequelae and osteoarthritis. Fevang and associates found in the Norwegian registry that fracture sequelae led to a 5.8 relative risk of failure
72
compared with inflammatory arthritis. Data from the state of New York found that revision rates for osteoarthritis were 14.7%, whereas those for inflammatory arthritis were only 8.3%. All patients require a 5-lb lifetime lifting limit postoperatively to improve the longevity of the prosthesis.
Correct answer : A
96- Figures 1 through 3 are the MRI scans of a 50-year-old man who sustained a first-time traumatic anterior shoulder dislocation after a fall. What is the most appropriate treatment?
A. Latarjet
B. Rotator cuff repair
C. Bankart repair
D. Superior labrum anterior to posterior (SLAP) repair
Multiple studies have shown that the most common associated injury following traumatic shoulder dislocation (besides anteroinferior labral lesions) are full-thickness rotator cuff tears, especially in patients >40 years of age. Robinson and associates found a
73
33.4% incidence of traumatic rotator cuff tears in this setting. Ro and associates reported rotator cuff tears in 18% of their study population. A level IV systematic review found that patients with rotator cuff tears following shoulder dislocations have more persistent pain and shoulder dysfunction. Rotator cuff repair surgery resulted in improved pain and patient satisfaction compared with those treated nonoperatively.
Correct answer : B
97- A complication associated with using the Morrey approach (triceps reflecting) to implant a semiconstrained total elbow arthroplasty is
A. loss of elbow extensor power. B. implant dislocation.
C. implant malposition.
D. development of heterotopic ossification.
Numerous approaches can be used to implant a total elbow arthroplasty. The Morrey approach identifies, transposes, and protects the ulnar nerve, and then subperiosteally reflects the triceps off the ulna. The sleeve of tissue is very thin distally, and the triceps need to be meticulously repaired at the time of closure. Implant dislocation and malposition are less likely with an extensile approach, and dislocation is unlikely with a semiconstrained implant. The development of heterotopic ossification is unrelated to the surgical approach used for elbow arthroplasty. Correct answer A
98- A 36-year-old recreational athlete feels a pop in his antecubital fossa while lifting weights. He has pain, swelling, and deformity. Representative sagittal and coronal MRI slices are shown in Figures 1 and 2, respectively. What is the most common major complications associated with surgical repair of this structure?
74
A. Symptomatic heterotopic ossification requiring reoperation
B. Brachial artery laceration
C. Deep infection
D. Posterior interosseous nerve palsy
The MRI scan shows a distal biceps tendon rupture with retraction. Tendon rerupture and PIN palsy are the two most common major complications following distal biceps repair surgery. Major complication rates are not found to differ by sex, history of tobacco use, age, exposure type (single versus two
incisions), tear morphology (full versus partial), or type of fixation used.
Correct answer : D
99- Figure 1 is the radiograph of a 21-year-old right-hand dominant patient. Compared with nonoperative treatment, open reduction internal fixation (ORIF) results in
A. lower complication rates. B. lower rates of nonunion. C. increased time to union. D. increased functional
outcome scores.
When comparing operative fixation of displaced clavicle fractures with nonoperative treatment, ORIF results in lower rates of nonunion, faster time to union, and similar outcome scores. There is an increased risk of complication, including infection, neurovascular insult, and the need for additional surgery. Correct answer : B
75
100- What are the components of the lateral ligament complex of the elbow?
A. Radial collateral ligament, lateral ulnar collateral ligament, annular ligament
B. Lateral ulnar collateral ligament (LUCL, anterior and posterior band) and the annular ligament
C. Transverse ligament, radial collateral ligament, lateral ulnar collateral ligament
D. Ulnar collateral ligament (anterior and posterior bands), transverse ligament
The important ligaments on the lateral side of the elbow are thickenings of the capsule. The lateral collateral ligament complex consists of four components: the lateral (radial) collateral ligament (LCL), the LUCL, the accessory LCL, and the annular ligament. The medial collateral ligament complex is a capsular thickening consisting of three components: the anterior band, the posterior band, and the transverse ligament. The LUCL is the most important portion of the lateral ligament in terms of posterolateral rotatory instability.
Correct answer : A
76
77
78
A spanning external fixator can be considered as a secondary option when adequate fixation and stability cannot be achieved, but that would not address the articular incongruity currently present. Total elbow arthroplasty is not indicated due to the patient's age and injury pattern, and physical therapy is unlikely to be successful without a congruently reduced joint.
2
2- When a patient has recurrent anterior shoulder instability, a bony glenoid reconstructive procedure should be considered in which clinical setting?
A. Associated humeral avulsion of the glenohumeral ligament (HAGL)lesion
B. Non-engaging Hill-Sachs lesion
C. Glenoid bone loss of at least 25%
D. Anterior labral periosteal sleeve avulsion (ALPSA) lesion
HAGL lesions may initially be treated without surgery. Recurrent instability in the setting of a HAGL lesion may be treated with a soft-tissue repair. A non- engaging or off-track Hill-Sachs lesion may be treated with an anterior soft- tissue (Bankart) repair. An on-track or engaging Hill-Sachs lesion may be treated by addressing any bony glenoid injury or anterior labral tear plus Hill- Sachs remplissage. An ALPSA lesion may be treated with a soft-tissue procedure, unless it is associated with a glenoid bony defect >25%. A glenoid bony defect >25% is associated with substantially higher risk of recurrent instability and consideration for bony glenoid reconstruction is advised. Consideration of bone augmentation procedures with less severe glenoid bone loss may be considered in higher risk patients, such as collision athletes.
Correct answer : C
3- A 61-year-old right-hand dominant woman falls down the stairs, resulting in a left anteroinferior shoulder dislocation and non- comminuted greater tuberosity fracture. A closed glenohumeral reduction with intravenous sedation is performed in the emergency department. After reduction, the greater tuberosity fragment remains displaced by 2 mm. What is the most appropriate treatment?
A. Open reduction internal fixation with transosseous sutures
B. Arthroscopic fixation using a suture bridge technique
C. Nonsurgical treatment with early passive range of motion
D. Nonsurgical treatment with sling immobilization for 8 weeks
Greater tuberosity fractures and rotator cuff tears associated with a traumatic dislocation are more commonly seen in women >60 years. Greater tuberosity fractures that are displaced <5 mm in the general population and <3 mm in laborers and professional athletes can be treated successfully without surgery. Early passive range of motion is important to avoid stiffness.
Correct answer : C
4- Residual angulation <30° of the humeral shaft after nonoperative fracture treatment has been shown to have what effect on patient reported outcomes?
A. Angulation in the coronal plane has more effect on functional outcomes than in the sagittal plane.
B. Increased angulation corresponds with worse functional outcomes.
C. Angulation >5° in any plane results in an unacceptable cosmetic result.
D. Residual angulation has no correlation with functional outcomes.
Acceptable angulation of humeral shaft fractures for nonoperative treatment is quite generous due to compensatory motion at the shoulder joint. Traditionally, 20° of anterior-posterior and 30° of varus-valgus angulation is acceptable. Indications for surgery have included angulation outside of this range, open fractures, brachial plexus injury, polytrauma, or other factors that preclude functional bracing. Increased amounts of angulation at the conclusion of healing can result in cosmetic dissatisfaction, but this has not been correlated with any specific degree of angulation, as patient factors are a strong influencer. Increased angulation has not been shown to affect functional outcomes within the angulation range previously described.
Correct answer : D
5- A 65-year-old man who underwent an uncomplicated reverse total shoulder arthroplasty (rTSA) to treat rotator cuff arthropathy 2 years ago has a routine follow-up visit in your clinic. A radiograph is shown in Figure 1. He denies shoulder pain, dysfunction, or constitutional symptoms, and his clinical examination findings are benign. Based upon the present radiologic evaluation, what is the next most appropriate step?
A. Revision rTSA
B. Conversion to hemiarthroplasty
C. Continued observation
D. Infection work-up with screening labs and joint aspiration
The patient's radiographs show scapular notching, which is a common complication of reverse shoulder arthroplasty caused by repeated contact between the humeral component and/or medial humerus and the inferior pillar of the scapular neck. Despite this radiographic finding, the patient is doing well clinically and is completely asymptomatic. Therefore, continued observation is appropriate.
Notching can result in creation of particulate debris, causing osteolysis and ultimate implant failure. Therefore, this patient should be monitored with serial radiographs. The overall incidence of notching has been reported to be between 51% and 96%. This nearly ubiquitous finding has been attributed to implant positioning, altered glenoid and humeral anatomy, and duration of implantation. Recent studies have identified that increased lateral offset, increased glenosphere size, and inferior positioning of the base plate can reduce the incidence of scapular notching.
Correct answer : C
6- A healthy 65-year-old woman undergoes anatomic total shoulder arthroplasty to address osteoarthritis (OA). The surgery is uncomplicated. What is the most common indication for future revision?
A. Deep infection
B. Periprosthetic fracture
C. Glenoid component loosening
D. Rotator cuff tear
The most common reason for revision surgery following unconstrained shoulder arthroplasty for glenohumeral OA is loosening of the implant. In most studies that distinguish glenoid from humeral loosening, the glenoid component is more frequently affected. Comprehensive systematic reviews have found that radiographic glenoid loosening can comprise nearly 30% to
40% of all complications following shoulder arthroplasty for non-inflammatory arthritis. Infections, periprosthetic fractures, and rotator cuff tears are uncommon. In the population-based study by Matsen and associates, 10% of the revisions were performed for loosening versus 7% for infection and 7% for rotator cuff tearing.
Correct answer : C
7- An 18-year-old male football player dislocated his elbow during a game. A post-reduction MRI scan is shown in Figure 1. The injury is initially treated non-operatively, but the patient continues to note subjective instability and pain when attempting to push up from a chair. Surgical intervention is planned for repair/reconstruction. What guidance should be provided to the patient and therapist in the early postoperative period?
A. No range-of-motion exercises until 6 weeks postoperative
B. Begin immediate strengthening
C. Avoid valgus stress to elbow
D. Avoid shoulder abduction
The MRI scan shows injuries to both the medial and lateral ligamentous structures of the elbow, with significant widening of the radiocapitellar joint space. The patient’s ongoing symptoms are consistent with posterolateral rotatory instability related to lateral collateral ligament insufficiency. After surgical repair versus reconstruction of the
lateral collateral ligament, it is important to avoid varus stress to the elbow, which can result in failure or loosening of the lateral structures. During shoulder abduction, gravity applies a varus stress to the elbow, and it should be avoided.
Limiting range of motion for the first 6 weeks would result in significant elbow stiffness. Valgus stress should be avoided in the setting of a medial collateral ligament repair or reconstruction. Strengthening is usually delayed until appropriate soft-tissue healing has been achieved.
Correct answer : D
8- When performing reverse shoulder arthroplasty, what factor leads to an increase in the complication indicated by the black arrow in Figure 1?
A. Superior baseplate position on the glenoid
B. Lateralized position of the glenosphere
C. Shorter humeral stem length
D. Larger glenosphere diameter
The image shows scapular notching. Inferior scapular notching is caused by direct mechanical impingement of the humeral bone or humeral prosthesis on the inferior scapular neck. Particulate polyethylene debris may aggravate inferior notching and lead to osteolysis. Impingement-free range of motion (ROM) in all planes is
imperative. Gutiérrez and associates analyzed the factors that affect impingement of the humerus or humeral component against the scapula and the resultant effect on ROM. Varus humeral neck-shaft angle was found to be the most important factor in preventing notching, followed by inferior positioning of the glenosphere, lateral offset of the glenosphere, and increasing size of the glenosphere. Humeral stem length and cementation have not been shown to have an impact on notching.
Correct answer : A
9- A 27-year-old man presents to the emergency department after a fall from a motorcycle. Imaging reveals a displaced glenoid neck fracture, and surgical intervention is planned through a modified Judet approach. What internervous plane is encountered between the infraspinatus and teres minor muscles?
A. Long thoracic nerve and axillary nerve
B. Suprascapular nerve and axillary nerve
C. Suprascapular nerve and long thoracic nerve
D. Spinal accessory nerve and axillary nerve
Surgical indications for scapular fractures are debatable in the literature. Historical indications for extra-articular fractures of the glenoid neck have ranged from 10-25 mm of medial displacement, 25-40⁰ of angular deformity of the glenoid, and a glenopolar angle cut-off of 20-30⁰. While the Judet approach can offer access to the entire scapular body, a modified Judet approach is a more limited approach that allows access to the glenoid neck in the interval
7
between the infraspinatus and teres minor. The infraspinatus is innervated by the suprascapular nerve, whereas the teres minor is innervated by the axillary nerve. The long thoracic nerve innervates the serratus anterior muscle. The spinal accessory nerve innervates the sternocleidomastoid and trapezius muscles.
Correct answer : B
10- What complication following total elbow arthroplasty poses more risk for a 60-year-old man with osteoarthritis than for a man of the same age with rheumatoid arthritis?
A. Aseptic loosening of a linked implant
B. Instability of an unlinked implant
C. Triceps rupture
D. Wound dehiscence
Patients with primary elbow osteoarthritis tend to be active and are often involved in manual occupations that place greater demands on a total elbow implant. Such patients are most often treated with nonprosthetic options because of concerns about prosthetic longevity. As a result, few cases of primary osteoarthritis are included in published studies. However, complications such as stem fracture and aseptic loosening appear to be more common in this population than in any other subgroup, including revision patients. The poor soft-tissue quality associated with rheumatoid arthritis leads to a high-risk ligamentous attenuation and is a general contraindication to use of an unlinked implant. The same poor soft tissue leads to a higher rate of triceps insufficiency and wound dehiscence.
Correct answer : A
11- A 69-year-old woman presents 18 months after undergoing surgical repair of her left proximal humerus fracture. She describes global left shoulder pain with limited range of motion. On examination, she has a well-healed superior shoulder incision without any signs of infection. Active elevation is limited to 45°, and passive range of motion results in crepitus. She expresses difficulty with activities of daily living, such as washing her hair. An AP radiograph of her shoulder is shown in Figure 1. What is the most appropriate step to maximize her function at this time?
A. Physical therapy focusing on supine straight arm raises
B. Removal of intramedullary nail and conversion to hemiarthroplasty
C. Revision open reduction and internal fixation (ORIF) to proximal humerus locking plate
D. Removal of intramedullary nail and conversion to reverse shoulder arthroplasty
The patient had a failed attempt at primary repair of her proximal humerus fracture with subsequent malunion. Because of the position of her greater tuberosity and concern about the status of her rotator cuff on examination, a reverse shoulder prosthesis is the most reliable option to maximize her shoulder function. Given the length of time since her index procedure, additional physical therapy is unlikely to provide significant benefit. A hemiarthroplasty or revision ORIF would have a lower likelihood of success due to the position of the greater tuberosity and presumed rotator cuff compromise.
Correct answer : D
12- Placement of the most distal interlocking screw seen in the radiographs in Figures 1 and 2 poses a risk to the nerve that controls what motor function?
A. Elbow flexion
B. Thumb interphalangeal (IP)
joint extension
C. Index finger proximal IP joint flexion
D. Index finger metacarpophalangeal (MCP) joint abduction
The most distal locking screw in this intramedullary nail construct was placed from anterior to posterior, passing through the distal portion of the biceps and brachialis muscle bellies. The median nerve, along with the brachial artery, is at risk as it lies between these 2 muscles. Malrotation of the nail, producing a more anteromedial starting point for the screw, can lead to a path that intersects with the nerve. Blunt dissection and soft-tissue protection is warranted with this screw placement. Median nerve injury would affect innervations of the flexor digitorum superficialis and profundus to the index finger (among other motors). Although the dissection violates the muscle belly of these 2 elbow flexors, measurable weakness is not typically seen. The radial nerve has already provided function to triceps (elbow extension) proximal to this level and lies sufficiently lateral to be more of a concern with a lateral screw placement (thumb IP extension). The ulnar nerve (index MCP abduction) is further medial at this level and would be at considerably lower risk than the median.
Correct answer : C
13- Figures 1 through 3 are the radiographs of a 40-year-old patient with a history of posterior labral repair who presents with severe pain and stiffness in the shoulder. The pain interferes with activities of daily living and interrupts his sleep at night. He has tried corticosteroid injections, nonsteroidal anti-inflammatory drugs, and activity modification with only temporary benefit. He wishes to discuss definitive treatment options. How can you counsel the patient about treatment with a hemiarthroplasty?
10
A. Functional outcomes and pain relief are inferior to total shoulder arthroplasty.
B. Rates of revision are lower than total shoulder arthroplasty.
C. Hemiarthroplasty avoids problems related to glenoid erosion. D. He can expect long term satisfaction.
The patient has evidence of osteoarthritis with eccentric glenoid wear. Hemiarthroplasty outcomes are worse in patients with eccentric glenoid wear, as compared to those with a concentric joint. Additionally, hemiarthroplasty has been shown to have inferior functional outcomes compared to total shoulder arthroplasty, with low long-term satisfaction rates. Revision rates are equal to or greater than total shoulder arthroplasty at mid to long term follow-up, and glenoid erosion remains a problem.
Correct answer : A
14- In comparing open versus arthroscopic osteocapsular arthroplasty for the treatment of elbow osteoarthritis, what is an advantage of arthroscopic over open treatment?
A. rthroscopic treatment provides better final range of motion than open treatment.
B. Arthroscopic treatment can be safely performed in the presence of prior ulnar nerve transposition.
C. Arthroscopic treatment can be equally effective in both early and advanced elbow osteoarthritis.
D. Arthroscopic treatment allows easy access to both the anterior and posterior compartments of the elbow.
Both arthroscopic and open management of elbow arthritis can be successful. Prior ulnar nerve transposition is a relative contraindication to arthroscopy, unless the nerve is specifically identified and protected intra- operatively. In general, arthroscopic management is indicated for mild to moderate arthritis. In advanced arthritis, there is decreased visualization and an increased risk for neurovascular insult. In contrast, open surgery can be utilized regardless of arthritis severity. Arthroscopy has the advantage of allowing easy access to both the anterior and posterior compartments of the elbow. Cohen and associates has shown better recovery of motion with open osteocapsular arthroplasty (Outerbridge-Kashiwagi procedure) compared with the same technique performed arthroscopically.
Correct answer : D
11
15- A 36-year-old woman dislocated her elbow 6 months ago. The elbow was congruently reduced and rehabilitated. She continues to have a sense of painful clunking in her elbow when she pushes up from a chair with forearm supination, but not pronation. What structure did not heal properly?
A. Posterior band of the medial collateral ligament
B. Anterior band of the medial collateral ligament
C. Radial collateral ligament
D. Lateral ulnar collateral ligament
The patient is showing signs of posterolateral rotatory instability after elbow dislocation. The lateral ulnar collateral ligament is responsible for stabilizing the elbow against this type of instability. The posterior and anterior bands of the medial collateral ligament are primarily resistors of valgus load, with the anterior band being the most significant contributor. The radial collateral ligament does not control the posterolateral rotatory instability described.
Correct answer : D
16- A 36-year-old right-hand dominant butcher presents with a 6-week history of medial elbow pain. On physical examination, she is tender to palpation over the anteroinferior aspect of the medial epicondyle. Pain is reproduced with combined elbow extension/resisted wrist flexion. Nonsurgical treatment of this pathology results in pain relief within one year in what percentage of individuals?
A. 25% to 35%
B. 45% to 55%
C. 65% to 75%
D. 85% to 95%
The patient has medial epicondylitis. Nonsurgical treatment is the hallmark of treatment and has been shown to relieve pain in approximately 90% of cases within one year. Nonsurgical modalities include bracing, physical therapy, nonsteroidal anti-inflammatory medications, activity modification, and injections.
Correct answer : D
12
17- A 55-year-old woman develops posttraumatic arthritis in the elbow following a distal humerus fracture. What is the most likely mid-term (5-
10 years after surgery) complication following semiconstrained total elbow arthroplasty (TEA)?
A. Bushing wear
B. Infection
C. Aseptic component loosening
D. Component fracture
TEA has been described for posttraumatic arthritis of the elbow and typically involves a young patient population with multiple previous operations on the affected elbow. Morrey and Schneeberger found aseptic component loosening to be uncommon (<10% of patients) and usually occurring >10 years after surgery. Prosthetic fracture, usually of the ulnar component, is also a late-term finding. Infection is the most common mode of early failure but usually occurs within the first 5 years and has an overall rate of approximately 5%. Bushing wear has been reported as the most common cause of mechanical TEA failure in this population at intermediate-term follow-up.
correct answer : A
18- A 51-year-old man presents with persistent right shoulder pain several weeks after falling off a roof. On examination, he has pain with palpation over the greater tuberosity, active forward shoulder flexion of
60°, and passive forward shoulder flexion of 160°. He has 2/5 forward flexion and external rotation strength. Initial plain radiographs are unremarkable. A coronal MRI scan of his shoulder is shown in Figure 1. After a thorough discussion, the patient elects to proceed with surgical intervention. During intraoperative assessment, the surgeon contemplates performing a single versus a dual row repair. Currently, what is the consistent difference between the two repair techniques?
A. Dual row repairs result in superior objective clinical outcomes
B. Dual row repairs provide a larger footprint coverage.
C. Single row repairs have a reported higher complete retear rate.
D. Single row repairs have fewer points of tendon fixation.
13
Several investigations continue to elucidate the difference between dual row and single row repairs. Modern dual row repairs involve fixating the rotator cuff tendon along both the medial and lateral aspect of the greater tuberosity as well as linking both points of fixation together. This allows closer restoration of native footprint coverage in comparison with single row repairs. However, doubling the number of implants results in increased healthcare costs without a clear clinical or biomechanical benefit. Several studies report statistically similar outcomes, retear rates, and biomechanical properties between single and dual row repair when the number of suture limbs across the repair site is the same.
correct answer : B
19- Figures 1 and 2 are the radiographs of a 37-year-old left-hand dominant man with left elbow pain and stiffness. He has a history of elbow dislocation as a child but denies any recent injuries. He has an arc of motion of 105° and stable ligaments. He describes crepitus and locking during elbow range of motion. He is an avid Crossfit athlete, intending to return to this activity and improve his range of motion. What is the best treatment?
A. Total elbow arthroplasty (TEA)
B. Ulnohumeral distraction interposition arthroplasty
C. Radial head replacement
D. Arthroscopic or open debridement and capsular release
14
This is a young, high-demand patient with early posttraumatic arthritis of the elbow. A debridement and capsular release has the ability to address his mechanical symptoms, improve his range of motion, and not result in any post- operative functional restrictions. While this may be a temporizing procedure in this patient, it will allow him to return to weight bearing recreational activities in the near term, which is his goal. A TEA would not be indicated based on the patient's age, his degree of arthritis, and his desire to remain active post- operatively. A radial head replacement would not address the patient's ulnohumeral arthritis. Similarly, an ulnohumeral distraction interposition arthroplasty would not address the patient's radiocapitellar arthritis. Both procedures would also require adjustments to his recreational activities post- operatively to prevent progressive failure of the reconstruction.
Correct answer : D
20- Figure 1 is the radiograph of 59-year-old left-hand dominant patient who underwent revision to a reverse total shoulder arthroplasty following a failed open reduction and internal fixation of a proximal humerus fracture. What is a risk factor for the complication shown?
A. Female sex
B. Lateralized component
C. Cemented humeral component
D. Previous surgery
Risk factors for instability after a reverse total shoulder arthroplasty include previous surgery (especially open surgery), loss of humeral tuberosities, inadequate restoration of humeral length,
male sex, BMI >30, and Grammont-style implant. Fixation method for the humeral stem has no impact on instability risk.
Correct answer : D
15
21- Figures 1 through 3 are the radiographs of a 55-year-old woman who fell on her outstretched right arm, resulting in acute elbow pain and swelling. On examination, she has lateral elbow bruising and tenderness, with a mechanical block to forearm supination and pronation. She has no medial tenderness. During surgery through a direct lateral approach, the surgeon observes a completely bare lateral epicondyle and surgical repair is performed, resulting in a stable and congruent joint. Initial postoperative rehabilitation should include
A. 3 weeks of cast immobilization.
B. elbow extension exercises with the forearm supinated. C. elbow extension exercises with the forearm pronated.
D. elbow extension exercises with the forearm in neutral rotation.
Radial head fractures are thought to occur as a result of valgus posterolateral rotary load across the elbow, although the mechanism can certainly vary. Minimally or nondisplaced fractures without any clinical instability or block to motion can often be successfully managed non-surgically. Fractures with >2 mm of displacement or fragments that block motion require surgical repair. A critical aspect during surgery is identifying concomitant injury to the lateral collateral ligament complex (LCL). When encountered, the LCL is most often avulsed from its origin at the lateral epicondyle, resulting in a bare area. After the radial head is either repaired or replaced (Figures 4 and 5), the LCL should
16
be repaired back to its anatomic origin. Postoperatively, the surgeon must communicate to the therapist that elbow extension exercises should be performed with the forearm in pronation as a result of the compromised LCL, as this position places the least stress on the ligamentous repair. Elbow extension exercises in supination or neutral are recommended for compromise of the medial collateral ligament, or combined medial and lateral ligament injury, respectively. Without any medial elbow bruising, swelling, or tenderness, it is unlikely that the patient has an injury to the medial collateral ligament.
Correct answer : C
22- A 78-year-old woman undergoes a reverse total shoulder arthroplasty for cuff tear arthropathy. Her preoperative, 3-month postoperative, and 1- year postoperative radiographs are shown in Figures 1 through 3. What is the cause of the radiographic finding seen here?
17
A. Glenoid component malposition
B. Humeral component malposition
C. Over tensioning of the deltoid
D. Excessive humeral component lateralization
The patient underwent a reverse arthroplasty for cuff tear arthropathy. Her preoperative radiograph shows some superior glenoid wear, which was not corrected at the time of surgery. This has resulted in superior tilt to the glenosphere, which has been identified as a risk factor for scapular notching. This occurs as a result of mechanical impingement between the medial humerus and scapular neck during arm adduction. The Beta angle and reverse shoulder angle have been proposed as measurements that can help identify pathologic glenoid tilt preoperatively. Risk factors for scapular notching include superior tilt of the glenosphere, superior placement of the glenoid baseplate on the glenoid, a 155° humeral implant angle, and incomplete lateralization of the construct.
The humeral component appears well-positioned in this radiograph. Over tensioning of the deltoid and excessive humeral lateralization would risk an acromial stress fracture and could limit shoulder range of motion. This is an inlay humeral stem, which does not lateralize the humerus.
Correct answer : A
23- Figures 1 and 2 are the MRI scans of a 21-year-old swimmer who has had pain in the lateral shoulder for 6 months. It is worse while swimming and with reaching overhead. Twelve weeks of physical therapy and a single corticosteroid injection have failed to improve her symptoms. What is the best next step?
18
A. Arthroscopic superior labrum anterior to posterior (SLAP) repair
B. Arthroscopic rotator cuff repair
C. Arthroscopic Bankart repair
D. Suprascapular nerve decompression
In the MRI scans, the patient has a high-grade tear of the undersurface of the superior rotator cuff. This is known as a partial articular-sided tendon avulsion lesion. This is often seen in overhead athletes and is associated with internal impingement. Given the length of symptoms, failure to respond to nonsurgical treatment, and the high-grade nature of the tear in a young patient, an arthroscopic repair should be performed. The available images do not demonstrate evidence of SLAP tear, Bankart lesion, or suprascapular nerve compression.
Correct answer : B
24- Figure 1 is the intraoperative radiograph of a shoulder hemiarthroplasty for glenohumeral arthritis. A "ream and run" is planned for the glenoid. What can be said about the outcomes of this procedure?
19
A. Activity restrictions are more rigid than after total shoulder arthroplasty. B. Fifty percent of patients require glenoid resurfacing within 2 years.
C. Recovery is faster than a total shoulder arthroplasty. D. Therapy is critical in obtaining a good clinical outco
"Ream and run" shoulder arthroplasty can allow for arthroplasty without the complications of a polyethylene glenoid. Ten-year conversion to total shoulder arthroplasty has been shown in one study to be 12%. Recovery is reported to be slower and requires more rehabilitation than arthroplasty done with glenoid resurfacing. Careful patient selection has been emphasized by the pioneering surgeon.
Correct answer :B
25- Figure 1 is the axial MRI scan of a 45-year-old brick mason who experienced acute right elbow pain after attempting to lift a wheelbarrow. Examination reveals pain and swelling in the antecubital fossa, weakness with forearm supination, and an abnormal hook test. The surgeon performs an anterior repair with two anchors. Three months after surgery, the patient has appropriate strength and range of motion but reports persistent radiating paresthesias along the radial side of the forearm. What is the best next step in management?
A. Exploration of forearm with neurolysis
B. MRI scan of cervical spine C. Revision distal biceps repair D. Observation with nonsteroidal
anti-inflammatory drugs as needed
This is a classic presentation of an acute traumatic distal biceps tendon rupture. In the dominant extremity of a manual laborer, this injury can result in approximately 40% loss of supination strength. Although not required, an MRI scan can confirm
the diagnosis. In general, a single incision anterior or two incision anterior/ posterior repair can be utilized for surgical intervention with similar success rates. Although the percentage of complications is similar between surgical approaches, the type of complications can vary. Anterior only repairs have a
20
higher risk of traction injury to the lateral antebrachial cutaneous nerve (LABC) secondary to the degree of retraction required for exposure in muscular patients. Posterior repairs have a higher risk for radiographic heterotopic bone formation. Fortunately, most LABC injuries are neuropraxias and resolve with observation, but resolution may take up to 6 months. In this case, ongoing observation is appropriate, with surgical exploration being considered only in chronic cases. Patients should be appropriately counseled about this issue prior to surgery.
Correct answer : D
26- When performing an ulnar nerve decompression at the elbow, the surgeon must be aware of the
A. median nerve as it crosses the surgical field 6 cm proximal to the medial epicondyle.
B. medial antebrachial cutaneous nerve as it crosses the field 3 cm distal to the medial epicondyle.
C. anterior antebrachial cutaneous nerve as it crosses the field at the medial epicondyle.
D. posterior antebrachial cutaneous nerve that crosses the field 2 cm distal to the medial epicondyle.
The medial antebrachial cutaneous and medial brachial cutaneous are nerves that can be injured during ulnar nerve decompression at the elbow. The medial antebrachial cutaneous nerve crosses the surgical field at an average of 3.1 cm distal to the medial epicondyle. The medial brachial cutaneous nerve crosses the field 7 cm proximal to the medial epicondyle and arborizes into two to three terminal branches. Because the surgical approach involves dissection on the medial side, the posterior antebrachial cutaneous nerve is distant from the exposure. Although the median nerve potentially can be located in the deep dissection of a submuscular transposition, it is considered distant to an in situ decompression.
Correct answer : B
27- Figures 1 and 2 are the radiographs of a 40-year-old patient who undergoes treatment of the clavicle fracture shown. What is the most likely complication of this intervention?
21
A. Nonunion
B. Acromioclavicular (AC) joint instability
C. Deltoid origin rupture
D. Symptomatic hardware
There have been many prospective and retrospective studies evaluating outcomes after surgical and nonsurgical treatment of displaced middle third clavicle fractures. Surgery results in a lower nonunion rate and higher patient reported outcomes. However, approximately 30% of these patients will have symptoms of hardware irritation and request subsequent plate removal. Nonunion is very low with plate fixation and is more common with nonsurgical treatment. AC joint instability is unlikely to be an issue with middle third clavicle fractures, and there is no evidence of AC malalignment on the images provided. Deltoid origin stripping is necessary for anterior plating, but is much less of an issue with superior plating, as was performed in this patient. Anterior plating is biomechanically inferior to superior plating but may pose a lower risk to neurovascular structures and has the theoretic opportunity to decrease implant irritation, although this has not been clearly demonstrated in the literature.
Correct answer : D
28- Figure 1 is the radiograph of a 54-year-old man who has increasing weakness and numbness in his lateral arm. No prior surgery or injury is reported. What is the most appropriate next diagnostic test?
A. MRI of the shoulder
B. MRI of the cervical spine
C. CT scan of the chest
D. Radiograph of the chest
22
The radiograph reveals a Charcot neuropathic shoulder. The atraumatic destruction of the humeral head is concerning for a neuropathic etiology and warrants MR imaging of the cervical spine to evaluate for the presence of a syrinx. Shoulder arthroplasty in the setting of a neuropathic joint is challenging given the local bone and soft-tissue loss, in addition to the loss of protective sensation. The scant literature on the use of shoulder arthroplasty in these challenging patients reports an improvement in pain but only modest improvements in shoulder function.
Correct answer : B
29- Figure 1 is the radiograph and Figure 2 is the 3-dimensional CT scan of a 55-year-old male patient who fell out of a tree 3 days ago onto his outstretched hand. What is the most appropriate treatment?
A. Lateral ligament repair and radial head replacement
B. Coronoid reconstruction utilizing allograft
C. Open reduction and internal fixation (ORIF) of the coronoid and possible lateral collateral ligament repair
D. ORIF of the coronoid and reconstruction of the medial collateral ligament
The patient presents with a coronoid fracture involving the anteromedial facet. This poses a risk for varus posteromedial rotary instability of the elbow. Appropriate treatment involves coronoid ORIF (this fracture involves the sublime tubercle, so fixing the coronoid will repair the medial collateral ligament) and a repair of the lateral ligament complex. Coronoid reconstruction is not needed with graft because the fracture fragment can be repaired. However, in chronic cases, the coronoid can be reconstructed with autograft
23
olecranon, autograft radial head, or allograft. There is no injury to the radial head, so arthroplasty is not required. Failing to address the lateral ligaments will lead to continued instability.
Correct answer : C
30- A 33-year-old right-hand dominant man presents for evaluation of recurrent right shoulder instability following a fall. He initially sustained a traumatic anterior shoulder dislocation while playing football 12 years ago that was treated with an arthroscopic Bankart repair. He sustained a repeat traumatic dislocation 5 years ago, prompting a revision arthroscopic Bankart repair and capsular shift. His shoulder has been stable until his recent reinjury three months ago. He feels that the shoulder is "sliding out" when he puts his arm in an abducted and externally rotated position. The symptoms remain unchanged despite participating in 2 months of physical therapy. Apprehension/Relocation test is positive. He has full range of motion without weakness. A CT arthrogram reveals 20% loss of bone of the anteroinferior glenoid, no Bankart lesion, and a non-engaging Hill-Sachs. What is the most appropriate treatment?
A. Revision arthroscopic Bankart repair with remplissage
B. Open Bankart repair with capsular shift
C. Transfer of the coracoid to the anterior glenoid
D. Injection of platelet-rich plasma
The history and examination are consistent with recurrent anterior shoulder instability. The patient has significant anteroinferior glenoid bone loss, no identifiable Bankart tear, and a non-engaging Hill Sachs. The glenoid bone deficiency is the most notable contributor to his recurrent instability, and a Latarjet coracoid transfer to the anterior glenoid would most likely provide long-term stability to his shoulder. A remplissage with tenodesis of the infraspinatus into the Hill-Sachs lesion can be helpful if the symptoms are related to engagement of the Hill-Sachs lesion. An open capsular shift and Bankart would not address the bony deficiency. There is no role for PRP in this clinical setting.
Correct answer : C
24
31- What is the most common complication following reverse total shoulder arthroplasty?
A. Scapula spine/acromial fracture
B. Dislocation/instability
C. Implant loosening
D. Periprosthetic fracture
Complications encountered following reverse total shoulder arthroplasty include dislocation, infection, hardware failure, hematoma, neurologic injury, periprosthetic fracture, scapular notching, and acromial/scapular spine fractures. The incidence and risks of these complications are related to the indication for the procedure. Dislocation is the most common complication, with an incidence of 1.5% to 31%. Risk factors associated with postoperative dislocation include male sex, previous shoulder surgery, proximal humeral bone loss, axillary nerve injury, and subscapularis deficiency. Commonly used methods to prevent instability include lateralization of the glenosphere and/or baseplate, eccentric baseplate placement, humeral lateralization or distalization, use of large glenosphere, and increased socket constraint. Correct answer : B
32- A 75-year-old woman with rheumatoid arthritis and a long history of oral corticosteroid use sustains a comminuted intra-articular distal humerus fracture. What is the best surgical option?
A. Open reduction internal fixation (ORIF) with parallel plates B. ORIF with orthogonal plates and iliac crest bone grafting C. Total elbow arthroplasty (TEA)
D. Closed reduction and percutaneous pinning
TEA is the best surgical option. McKee and associates published a multicenter randomized controlled trial comparing ORIF with TEA in elderly patients. TEA resulted in better 2-year clinical functional scores and more predictable outcomes compared with ORIF. TEA was also likely to result in a lower reoperation rate; one-quarter of patients with fractures randomized to ORIF could not achieve stable fixation. Further, Frankle and associates reported a comparative study of TEA versus ORIF in 24 elderly women. TEA outcomes were again superior to ORIF at a minimum of 2 years of follow-up. TEA was especially useful in patients with comorbidities that compromise bone stock, including osteoporosis and oral corticosteroid use. Closed reduction and percutaneous pinning studies have not been published on the adult population. Correct answer : C
25
33- A 17-year-old girl develops chronic posterolateral rotatory instability (PLRI) of the elbow following closed treatment of an elbow dislocation. Advanced imaging reveals incompetence of the lateral collateral ligament complex, and ligament reconstruction is planned. Examination under anesthesia is performed with the forearm in maximal supination and valgus force applied to the elbow, demonstrated in Video 1. As the elbow is brought through a range of motion assessment, the radial head is
A. dislocating posteriorly in extension and reducing in flexion. B. dislocating posteriorly in flexion and reducing in extension. C. dislocating anteriorly in extension and reducing in flexion. D. dislocating anteriorly in flexion and reducing in extension.
PLRI of the elbow is the most common form of chronic elbow instability. The mechanism occurs following a fall onto an outstretched hand, where a valgus force is applied to the elbow and the forearm rotates into progressive supination. This allows the radial head to translate posterior to the capitellum, with progressive injury from lateral to medial sides of the elbow. The pivot shift test is a useful examination maneuver to confirm the presence of PLRI. With the forearm in maximal supination and valgus stress applied to the elbow, the radial head is forced posterior to the capitellum as the elbow is brought into progressive extension, revealing a dimple on the lateral aspect of the elbow. This typically occurs at roughly 30° of flexion. As the elbow is flexed, the radial head reduces.
Correct answer : A
34- Figure 1 is the MRI of a 45-year-old woman with a medical history significant for rheumatoid arthritis who returns to your office with persistent right elbow pain. Her rheumatologist has maximized her disease-modifying anti-rheumatoid drug regimen. She complains of diffuse joint pain and swelling. On examination, she has a pronounced joint effusion, elbow flexion arc of 45°, and crepitus with forearm rotation. Her elbow radiograph reveals preservation of her joint space. What is the most appropriate surgical treatment at this time?
26
A. Total elbow arthroplasty
B. Synovectomy with radial head resection
C. Synovectomy without radial head resection
D. Isolated radial head resection
Rheumatoid arthritis remains a common inflammatory arthropathy that can lead to progressive synovitis of the elbow joint. Patients often present with recalcitrant elbow pain and loss of motion. In the early
stages, the joint space can be fairly well preserved. With progressive synovitis, cartilage destruction leads to symmetric joint space narrowing and joint destruction. For the younger patient with recalcitrant synovitis and a relatively well-preserved joint space, open or arthroscopic synovectomy provides successful improvement for 70% to 80% of patients. In most cases, radial head resection is not required. Synovitis that encircles the radial head and neck can lead to pain and crepitus with forearm rotation. Preserving the radial head prevents the rapid progression of wear at the ulnohumeral joint. A total elbow replacement, while a successful treatment modality for the older, lower demand patient with rheumatoid arthritis, would not be ideal for the younger patient given the significant postoperative restrictions imparted.
Correct answer : C
35- A 15-year-old girl has experienced 6 months of increasing dominant shoulder pain while playing volleyball. Her pain is so significant that she can no longer compete. Examination demonstrates 190° of forward elevation, 110° of external rotation at the side, and internal rotation up the back to T2 bilaterally. She also has 15° of bilateral elbow hyperextension. Load and shift testing demonstrates pain with anterior and posterior drawer tests. She has a large sulcus sign with associated pain. Forward elevation and external rotation strength testing shows 4/5 strength. There is no scapular winging and radiographic findings are normal. What is the best next step?
A. Physical therapy for rotator cuff strengthening
B. Subacromial corticosteroid injection
C. MRI arthrogram
D. Arthroscopic stabilization
27
This patient has multidirectional instability as evidenced by her hyperlaxity and excessive range of motion. Patients with pain after activities often have weak rotator cuff musculature and improve with strengthening of the rotator cuff and proprioceptive retraining. Subacromial injection likely cannot help this patient because it will not treat her underlying motor weakness in the rotator cuff or her dyskinesia. MRI arthrogram is not indicated unless she fails nonsurgical treatment. Arthroscopic stabilization also would be reserved for patients who fail nonsurgical treatment.
Correct answer : A
36- When performing capsular releases during shoulder arthroplasty for the treatment of glenohumeral joint osteoarthritis, what anatomic landmark indicates the location of the axillary nerve as it begins to travel from anterior to posterior?
A. Inferior border of the subscapularis
B. Insertion of the pectoralis major onto the humerus
C. Insertion of the latissimus dorsi tendon onto the humerus
D. Lateral margin of the conjoint tendon
The axillary nerve originates from the posterior cord of the brachial plexus. It passes down the anteroinferior aspect of the subscapularis, courses posteriorly beneath the glenoid and inferior capsule, then wraps around the humerus from posterior to anterior on the deep surface of the deltoid. In the setting of glenoid and humeral head deformity, the inferior border of the subscapularis can be a useful landmark to ensure the nerve is appropriately protected intraoperatively.
Correct answer : A
37- A 24-year-old female rugby player presents after a traumatic shoulder dislocation. She has a history of open Latarjet 3 years ago related to chronic shoulder instability. Her current radiograph and CT scans are shown in Figures 1 through 4. Her shoulder is unstable with abduction and external rotation. Belly press test and axillary nerve function are intact. What is the best surgical option for her?
28
A. Arthroscopic debridement with anteroinferior labral repair and capsular shift
B. Open implant removal and repair of damaged soft-tissue structures
C. Revision anterior glenoid augmentation with iliac crest autograft or distal tibial allograft
D. Open Putti Platt reconstruction
The patient has developed recurrent shoulder instability following a previous Latarjet. Radiographs and CT scans demonstrate resorption of the coracoid graft and failure of hardware. At this point, in a contact athlete with failed hardware and recurrent instability, the most appropriate surgical intervention would be an open procedure with hardware removal and revision bone grafting of the anterior glenoid with iliac crest autograft or distal tibial allograft.
29
Arthroscopic debridement with anteroinferior labral repair and capsular shift and open implant removal and repair of damaged soft-tissue structures are incorrect because an isolated soft-tissue procedure would place the patient at high risk for recurrence. A Putti Platt reconstruction is a nonanatomic reconstruction that has been correlated with progressive glenohumeral arthrosis.
Correct answer : C
38- Figures 1 through 3 are the radiographs and MR arthrogram of a 46- year-old woman who reports bilateral elbow pain over the past 2 years. Pain is diffuse, associated with stiffness, and is worst in the morning. It gradually improves over the course of the day. Physical examination shows a moderate elbow effusion, with tenderness to palpation diffusely around the elbow, but worst in the posteromedial and posterolateral gutters. She lacks 25° of terminal extension bilaterally and has pain with terminal elbow flexion. She has tried anti-inflammatory medication, corticosteroid injections, and physical therapy without improvement in symptoms. What is the best surgical treatment option at this point?
A. Arthroscopic debridement and synovectomy
B. Radial head excision
C. Total elbow arthroplasty
D. Interpositional arthroplasty
30
The patient’s clinical presentation is consistent with inflammatory arthritis. The MRI shows a large effusion with synovitis, particularly around the radial neck. There is bone edema in the proximal ulna, but no evidence of joint destruction, and radiographs reveals maintained joint space. These findings support the diagnosis of early-stage inflammatory arthritis. Because there is no joint destruction, surgical treatment would emphasize preservation of the native elbow joint. Arthroscopic synovectomy has been shown to be very effective in these cases. Referral to a rheumatologist for further workup is also recommended. The other options listed would be considered in the setting of more advanced joint degeneration.
Correct answer : A
39- Figures 1 through 3 are the MRI scans of a 56-year-old woman in good health who reports a 6-month history of shoulder pain and external rotation weakness. Her radiographs are unremarkable. What is the diagnosis?
A. Rotator cuff tear
B. Anteroinferior labral tear
C. Suprascapular nerve compression
D. Quadrilateral space syndrome
31
The images reveal T2-weighted MRI sequences with edema isolated to the infraspinatus. In the absence of a tear in the infraspinatus tendon, the edema is most likely due to compression of the suprascapular nerve in the spinoglenoid notch. As this pathology persists, progressive muscle atrophy and fatty infiltration can result. Compression of the suprascapular nerve in the suprascapular notch would have resulted in edema and weakness in both the supra- and infraspinatus muscles. Compression is commonly caused by cysts from the joint secondary to labral tears. A rotator cuff tear of the infraspinatus is not identified on these images, and there is no history of trauma provided. There is no evidence of an anteroinferior labral tear, nor would this be expected to result in external rotation weakness or MRI abnormality of the infraspinatus. Quadrilateral space syndrome results in compression of the axillary nerve, which supplies the teres minor.
Correcr answer : C
40- A 41-year-old right-hand-dominant man has been treated nonsurgically for right elbow arthritis. His radiographs reveal end-stage ulnohumeral arthritis with complete loss of the joint space. He reports pain during the mid-arc of elbow flexion and extension. During the last 8 years, he has attempted activity modification, medication, physical therapy, and multiple cortisone injections. His symptoms have progressed, resulting in constant pain, loss of a functional range of motion, and an inability to perform many activities of daily living. Secondary to his age and activity demands, he undergoes a soft-tissue interposition arthroplasty of his elbow with an Achilles allograft. Which presurgical finding correlates with elevated risk for postsurgical complications?
A. Inflammatory elbow arthritis
B. A presurgical flexion-extension elbow arc of approximately 50° C. Retained distal humerus hardware on presurgical radiographs D. Evidence of presurgical elbow instability
End-stage posttraumatic or inflammatory elbow arthritis in active, high-demand patients remains difficult to treat. Traditional total elbow arthroplasty is discouraged in this demographic secondary to concerns about implant longevity. Soft-tissue interposition arthroplasty does not necessitate the same activity and weight restrictions for patients after surgery and remains a reasonable salvage procedure. Larson and Morrey published their findings on
38 patients with a mean age of 39 years following soft-tissue interposition arthroplasty for posttraumatic and inflammatory end-stage elbow arthritis. These investigators reported a significant improvement in Mayo Elbow Performance Score in addition to improvement in the flexion-extension arc from 51° to 97° after surgery. They reported worse results and elevated incidence of complications for patients with presurgical elbow instability. Retained hardware from prior surgery was not deemed a contraindication.
Correct answer : D 32
41- Figure 1 is the radiograph of a 12-year-old baseball player who has posterolateral elbow pain with throwing. The area of interest is designated by the black arrow. His range of motion and strength are full. No previous treatment has been provided. What is the most appropriate initial treatment?
A. Elbow arthroscopy with debridement B. Immobilization and rest for 6 weeks C. Corticosteroid injection
D. Open osteochondral autograft transfer
Osteochondritis dissecans of the capitellum is a painful condition that affects immature athletes who undergo repetitive compression of the radiocapitellar joint. Management is based primarily on the integrity of the articular cartilage surface and the stability of the lesion. Nonsurgical treatment is typically selected for patients
with early-grade, stable lesions, and it involves activity modification with
cessation of sports participation. The duration of activity modification is dictated by symptoms, with 3 to 6 weeks of rest followed by return to sport in
3 to 6 months commonly used as a guideline. Strengthening and stretching exercises are commonly incorporated after the pain has subsided. Surgical intervention or corticosteroid injection would not be first-line treatment. Correct answer : B
42- Figures 1 and 2 are the radiographs of a 69-year-old man with a history of treated prostate cancer and hemodialysis-dependent end- stage renal disease who presents to the emergency department with progressively worsening right shoulder pain and stiffness. Laboratory tests reveal a white blood cell count of 17,000, erythrocyte sedimentation rate, 75, and CRP, 10.1. He has a draining sinus located along the anterior shoulder. What is the best next step?
33
A. Arthroscopic irrigation and debridement
B. Admission and IV antibiotics
C. Culture from draining sinus
D. MRI scan with intravenous contrast
The patient's radiographs demonstrate bone loss of the medial humeral head. He has risk factors for both septic arthritis/osteomyelitis, and metastatic cancer, and it is important to understand the extent of his pathology before moving forward with surgical intervention. An MRI scan would assist in the diagnosis and demonstrate the extent of disease/tissue involvement. Administration of IV antibiotics prior to obtaining appropriate cultures would decrease the success rate of treatment in the setting of infection, and mistreat the pathology in the setting of metastasis. Similarly, obtaining cultures from the draining sinus tract would fail to account for the possible tumor diagnosis and may result in inaccurate culture results.
Correct answer : D
43- Figure 1 is the radiograph of a 19-year-old lacrosse player who landed on the apex of his right shoulder in a game 2 weeks ago. Figure 2 represents a comparison view of his uninjured contralateral side. He presents with complaints of right shoulder pain and deformity. Physical examination is negative for rotator cuff pathology or glenohumeral instability. Coracoclavicular distance is increased by 60% on the affected side. What is the best next step in management?
A. Physical therapy
B. Steroid injection
C. Platelet-rich plasma (PRP) injection
D. Operative fixation
34
44- In rotator cuff tear arthropathy with pseudoparalysis, forward elevation of the humerus away from the body is prohibited because of
A. deltoid atony.
B. loss of glenoid concavity.
C. loss of humeral head depression from the biceps tendon. D. loss of compressive force on the humeral head.
The rotator cuff serves as a humeral head compressor that stabilizes the humeral head in the glenoid concavity, so that the deltoid can convert a vertical force into abduction and forward elevation. The deltoid functions normally in patients with chronic rotator cuff arthropathy, so no atony is present. Glenoid concavity can be lost over time as joint degeneration progresses, but this is not the primary mechanism for failure of elevation. The biceps tendon does not serve as a humeral head compressor and does not prevent proximal migration of the shoulder when it is present.
Correct answer : D
45- Figure 1 is the radiograph of a 70-year-old woman with left shoulder pain following a ground-level fall 2 days ago. She reports good function of the shoulder prior to her fall. Examination reveals intact neurovascular status. She elects to undergo an acute reverse shoulder arthroplasty (RSA). How does this intervention compare with other arthroplasty options?
A. RSA results in better outcomes but increased complications compared with hemiarthroplasty.
B. RSA results in better outcomes and similar complications compared with hemiarthroplasty.
C. Acute RSA results in better outcomes than delayed RSA in this demographic.
D. Hemiarthroplasty and RSA have similar outcomes.
RSA has been shown to result in better clinical outcomes with a similar complication rate compared with hemiarthroplasty for the treatment of comminuted proximal humeral fractures in elderly patients. If an RSA is necessary in a delayed fashion to salvage failed nonoperative management, a systematic review and meta-analysis have shown no significant difference in outcomes between acute versus delayed RSA in this patient population. Correct answer : B
35
46- A 45-year-old right-hand dominant woman falls onto an outstretched left hand. Imaging shows a complex elbow dislocation. The postreduction CT scan demonstrates a reduced joint, comminuted radial head fracture, and type I coronoid fracture. Surgical intervention is recommended to address the involved structures. Which component of the intervention adds the most rotational stability?
A. ixation of the coronoid fragment
B. Radial head arthroplasty
C. Repair or reconstruction of the lateral collateral ligament (LCL)
complex
D. Repair or reconstruction of the medial collateral ligament (MCL)
This represents a terrible triad injury, with elbow dislocation, radial head fracture, and coronoid fracture. The LCL complex is typically disrupted in this injury pattern. Repair or reconstruction of this structure provides the greatest increase in rotational stability of the elbow.
Correct answer : C
48- A 68-year-old right-hand dominant woman has experienced progressive right elbow pain and loss of motion for several years. She has failed nonsurgical treatment and elects to undergo a total elbow arthroplasty (TEA). In comparison to a linked prosthesis, an unlinked prosthesis has which reported distinction with extended follow-up?
A. Improved longevity in comparison to the linked prosthesis
B. A significantly larger flexion-extension arc
C. A higher incidence of postsurgical instability
D. Lower frequency of ulnar nerve dysfunction
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants.
Correct answer : C
36
48- A 21-year-old left-hand dominant minor league baseball player presents with a several-month history of pain while throwing. He is most symptomatic during the deceleration phase of his throwing motion. At terminal extension, he notes pain and loss of motion. The patient denies mechanical symptoms. Looking at Figure 1, where is the initial radiographic abnormality most likely to be found in this patient?
A B C D
The patient has evidence of valgus extension overload (VEO). In overhead athletes with VEO, the posteromedial aspect of the olecranon abuts the olecranon fossa during the throwing motion. As a result, osteophyte formation along the medial olecranon is typically the first radiographic abnormality identified. Pain typically occurs during the deceleration phase of throwing, and loss of terminal extension can ultimately develop. As the pathology progresses, osteophytes and loose bodies may be present within the olecranon fossa, and the ulnar collateral ligament can be damaged. Increases in valgus laxity can ultimately cause degenerative changes to the radiocapitellar joint, but this is a secondary phenomenon. Correct answer : B
49- Figures 1 through 3 are the radiographs of a 68-year-old woman with progressive shoulder pain. She has failed all nonoperative modalities and now presents with refractory shoulder pain at night and with any attempted shoulder motion. She lacks the ability to forward elevate or abduct her shoulder >45°. What is the best treatment option?
37
A. Arthroscopic rotator cuff debridement and superior capsular reconstruction
B. Reverse total shoulder arthroplasty
C. Shoulder hemiarthroplasty
D. Total shoulder arthroplasty utilizing a titanium in-growth glenoid component
The patient has cuff tear arthropathy associated with significant pain and poor function. At age 68, a reverse total shoulder arthroplasty is the most reliable option to address her complaints. Arthroscopic debridement with superior capsular reconstruction would be a consideration in a younger patient with an irreparable posterosuperior rotator cuff tear, little to no glenohumeral arthritis, and little to no humeral head elevation. Total shoulder arthroplasty would have a high rate of glenoid component failure and limited function, regardless of the type of glenoid component utilized. Clinical outcomes of reverse total shoulder arthroplasty are superior to hemiarthroplasty in the setting of cuff tear arthropathy.
Correct answer : B
38
50- Figures 1 and 2 are the CT and MRI scans of a patient with shoulder instability. Contrasting these two imaging techniques for decision making in shoulder instability would suggest
A. Both CT and MRI have equivalent cost for the patient.
B. Both CT and MRI have equivalent safety for the patient.
C. Associated soft-tissue damage can be more reliably shown on CT
scans.
D. Two-dimensional CT scans represent better definition of bone loss than two-dimensional MRI scans.
Two-dimensional CT scan is generally accepted as a superior imaging modality for evaluating bone loss in shoulder instability than two-dimensional MRI scan. This advantage is offset by the relatively high radiation dose. Although CT in most situations is less costly, MRI can provide more data regarding associated soft-tissue damage that can be associated with recurrent instability. It should be noted that three-dimensional MRI has recently been shown as equivalent to three-dimensional CT in its ability to identify glenoid bone loss.
Correct answer : D
51- A 43-year-old woman is involved in a motor vehicle collision. She sustains the isolated injury shown in the radiograph in Figure 1. Her neurovascular examination is compromised. What is the most likely deficit?
A. Inability to flex the distal interphalangeal joint of the index finger
B. Positive Froment’s sign
C. Weakness with wrist extension
D. Decreased capillary refill
39
Humeral shaft fractures can be associated with palsy of the radial nerve, which will result in deficits of wrist and finger extension. Most will resolve with observation, consistent with a neuropraxia. Radial nerve palsy is not a contraindication to functional bracing. Distal interphalangeal (IP) joint flexion of the index finger is from the flexor digitorum profundus of the index finger, supplied by the median nerve. Froment's sign results from weakness of the adductor pollicis, which is innervated by the ulnar nerve. In this maneuver, patients compensate with flexion of the IP joint of the thumb (flexor pollicis longus, innervated by the median nerve) when asked to pinch a piece of paper between their thumb and index finger. Vascular injuries are uncommon with isolated humeral shaft fractures.
Correct answer : C
52- Figure 1 is the MR arthrogram of a 24-year old professional baseball pitcher who complains of worsening right elbow pain and decreased pitch velocity over the past 2 months. He was initially managed with rest and forearm strengthening, but continues to complain of medial elbow pain during the long toss portion of his throwing program. What is the most appropriate treatment at this time?
A. Ulnar nerve decompression
B. Common flexor pronator repair
C. Elbow arthroscopy with debridement
D. Medial ulnar collateral ligament reconstruction/repair
The MR arthrogram shows a rupture of the ulnar collateral ligament (UCL) from the ulnar insertion, with the classic T-sign of contrast extravasation. Medial UCL reconstruction, using either ipsilateral palmaris longus or allograft tendon, is
indicated for UCL injuries that fail nonsurgical management. Primary repair has been shown to be successful in select cases, but appropriate patient selection is essential. An arthroscopic elbow debridement would be indicated for early elbow arthritis or intra-articular loose body, which is not demonstrated here. An ulnar nerve decompression would be indicated in the setting of cubital tunnel syndrome, but this patient has no complaints of paresthesias.
Correct answer : D
40
53- A right-hand dominant 45-year-old man sustains an injury to the anterior aspect of his right elbow while trying to lift a heavy load 3 days ago. He has ecchymosis in the anterior and medial elbow regions and has difficulty with resisted forearm supination with the elbow in a flexed position. A diagnosis of an acute distal biceps tendon rupture is made and surgical treatment is chosen. The anatomic relationship of the distal biceps tendon to the median nerve and recurrent radial artery within the antecubital fossa is such that the biceps tendon travels
A. lateral (radial) to the median nerve and posterior (deep) to the recurrent radial artery.
B. lateral (radial) to the median nerve and anterior (superficial) to the recurrent radial artery.
C. medial (ulnar) to the median nerve and posterior (deep) to the recurrent radial artery.
D. medial (ulnar) to the median nerve and anterior (superficial) to the recurrent radial artery.
During surgical repair of a distal biceps tendon rupture, regardless of the surgical approach or technique, an understanding of the regional anatomy is important. The tendon passes distally into the antecubital fossa. The antecubital fossa is defined by the brachioradialis radially and the pronator teres ulnarly. A sheath surrounds the biceps tendon as it passes through the antecubital fossa toward its insertion on the radial tuberosity. The lateral antebrachial cutaneous nerve lies superficially in the subcutaneous tissue of the antecubital fossa. The nerve parallels the brachioradialis. While still superficial, the tendon is contiguous with the lacertus fibrosus that becomes confluent medially with the fascia overlying the flexor-pronator mass. The brachial artery lies just beneath the lacertus fibrosus at the level of the elbow flexion crease. The tendon travels just lateral (radial) to the median nerve within the antecubital fossa and passes posterior (deep) to the recurrent radial artery before it attaches to the radial tuberosity. Full forearm supination allows visualization of the tendinous insertion on the radial tuberosity.
Correct answer : A
41
54- MRI results are shown in Figure 1 for a 22-year-old, right-hand dominant collegiate athlete who reports a 6-month history of progressive weakness in his right arm. He denies any specific traumatic event. He has altered his weight-lifting activities and tried over-the-counter ibuprofen without benefit. No appreciable deformity or atrophy is found on examination of the upper extremities. He demonstrates full active shoulder range of motion, and there is no weakness with abduction in the plane of the scapula. Belly press test findings are normal, but weakness is seen in external rotation with the arm in adduction. He does not demonstrate anterior apprehension, and there is no instability with load and shift testing. Radiographs are unremarkable. What is the best surgical option?
A. Arthroscopic labral debridement and biceps tenodesis
B. Shoulder arthroscopy with undersurface cuff debridement and acromioplasty
C. Cyst decompression at the spinoglenoid notch with possible labral repair
D. Cyst decompression at the suprascapular notch with possible labral repair
This patient’s clinical and MRI findings are consistent with a posterior paralabral cyst with compression of the suprascapular nerve, specifically at the spinoglenoid notch. Compression of the suprascapular nerve can occur at either the suprascapular or spinoglenoid notch. Compression of the nerve at the suprascapular notch affects innervation to both the supraspinatus and infraspinatus muscles, resulting in weakness in both shoulder abduction and external rotation. However, compression at the spinoglenoid notch only affects innervation to the infraspinatus muscle, resulting in isolated weakness in external rotation.
Compression at the spinoglenoid notch often is seen in overhead athletes, and studies have shown associated posterior labral tears (Piatt and associates). Several studies have addressed nonsurgical and surgical treatment options. The treatment decision should focus on the underlying cause (Martin and associates)—in this patient, the cyst. Nonsurgical treatment in the presence of a known lesion has been associated with a higher failure rate than addressing the lesion, which can result in functional improvement (Chen and associates, Cummins and associates). The best response in this scenario is decompression of the cyst at the spinoglenoid notch with possible labral repair.
Correct answer : C 42
55- A 45-year-old woman diagnosed with lateral epicondylitis undergoes an open debridement of the extensor carpi radialis brevis. During surgery, resection extends posterior to the equator of the radiocapitellar joint. Postoperatively, she complains of persistent pain, despite appropriate rehabilitation. What other physical examination finding is she likely to have?
A. Pain with elbow extension in forearm pronation B. Mechanical symptoms when rising from a chair C. Valgus instability
D. Tenderness over the medial collateral ligament (MCL)
Excessive resection of the common extensor origin posterior to the equator of the radiocapitellar joint may lead to iatrogenic lateral collateral ligament (LCL) injury, causing posterior lateral rotatory instability (PLRI). Patients may present with lateral elbow pain, a positive lateral pivot shift test, or mechanical symptoms/subjective instability when pushing up from a chair (positive chair rise test). PLRI is often provoked with combined elbow extension and forearm supination, as the posterior support for the radiocapitellar joint has been lost. Therefore, placing the forearm in pronation during elbow extension places the radiocapitellar joint in a more stable position and is less likely to induce pain or mechanical symptoms. Valgus instability and MCL tenderness would be associated with an MCL injury.
Correct answer : B
56- A 75-year-old man presents with complaints of shoulder pain, bruising, and weakness following a fall onto his outstretched hand. He underwent an uncomplicated anatomic total shoulder arthroplasty 5 years prior with good range of motion and strength. His current radiographs are shown in Figures 1 and 2. What is the most appropriate next step to restore this patient’s function?
43
A. Rotator cuff repair
B. Revision to reverse total shoulder arthroplasty
C. Physical therapy
D. Latissimus dorsi transfer
The patient's radiographs demonstrate humeral head elevation and anterior translation, suggesting a massive traumatic rotator cuff tear. In this setting, a rotator cuff repair is unlikely to be successful, and a revision to reverse total shoulder arthroplasty is indicated. A latissimus dorsi transfer can address only a portion of the patient's rotator cuff deficiency. Physical therapy may result in some degree of improvement, but this cannot address the joint instability and malalignment. If the shoulder remains in its current position, progressive glenoid loosening would be expected due to the “rocking horse” phenomenon resulting in eccentric glenoid edge loading. Shields and Wiater compared conversion of an anatomic total shoulder to a reverse total shoulder for rotator cuff deficiency with primary reverse total shoulder arthroplasty and found similar American Shoulder and Elbow Surgeons Standardized Shoulder Assessment and visual analog scale pain scores at 2-year follow-up.
Correct answer : B
57- Figures 1 and 2 are the MRI arthrograms of a 14-year-old male baseball player who notes medial-sided elbow pain that occurs during the early acceleration phase of throwing. Pain has continued for one year. Pain improves with rest but worsens once he returns to throw. The longest he has rested is 3 months. He has completed a physical therapy program focusing on elbow strengthening and range of motion. He denies mechanical symptoms. Physical examination shows full elbow range of motion, no tenderness, and pain with moving valgus stress test, although there is no instability noted. There is no pain with resisted wrist flexion. What is the best next step?
A. Evaluation of shoulder range of motion and strength
B. Arthroscopic debridement and microfracture
C. Ulnar collateral ligament (UCL) reconstruction
D. UCL repair
44
The patient has a clinical history and physical examination consistent with UCL pathology. In an overhead athlete, deficits in the kinetic chain can contribute to the development of medial elbow pathology due to increased force transmission across the elbow. As a result, it is important to examine the shoulder to ensure that total arc of motion remains equivalent to the contralateral arm. Decreases in total arc of motion, commonly associated with glenohumeral internal rotation deficits (GIRD), can predispose athletes to medial elbow injuries. These shoulder deficits can be addressed with physical therapy. The MRI scan shows a structurally intact UCL, therefore, UCL repair or reconstruction is not indicated. The MRI scans demonstrate no evidence of osteochondral injury, which would be an indication for arthroscopic debridement and microfracture.
Correct answer : A
58- A 42-year-old woman sustains a closed posterior elbow dislocation. A closed reduction is performed, and the elbow appears stable under fluoroscopic examination through a full arc of motion. Initial treatment should consist of
A. early mobilization only.
B. surgical repair of medial and lateral collateral ligaments. C. active motion in a hinged brace from 30° to 120°.
D. application of hinged external fixator with early mobilization.
This is a simple (no associated fracture) elbow dislocation. Such dislocations can be treated with closed reduction followed by mobilization after 5 to 7 days to avoid stiffness, provided the elbow is stable through a full arc of motion at the time of reduction. If the elbow is unstable but has a short arc of stability, then using a hinged brace in the stable arc may be considered. It may be necessary to splint the elbow in pronation if the medial collateral ligament (MCL) is intact and the lateral collateral ligament (LCL) is disrupted, or in supination if the LCL is intact but the MCL disrupted. Surgical repair of the LCL and MCL may be required only if the elbow does not have a stable arc at the time of reduction. If the elbow remains unstable after repair, then application of a hinged external fixator may be considered.
Correct answer : A
45
59- A 40-year-old female recreational basketball player notes pain deep within her shoulder that occurs with activity. Pain began insidiously 6 months previously. She has completed a physical therapy program, and an intra-articular corticosteroid injection provided excellent temporary relief. Physical examination shows symmetric range of motion of her shoulder. She has a positive O'Brien’s active compression test. There is no pain with cross-arm adduction or tenderness to palpation over the acromioclavicular joint. Resisted abduction is nonpainful and strong. MRI shows increased signal in the substance of the superior labrum, low-grade bursal surface fraying of the supraspinatus, and mild degenerative changes within the acromioclavicular joint. What is the best treatment option?
A. Biceps tenodesis
B. Superior labrum anterior to posterior (SLAP) repair
C. Rotator cuff repair
D. Distal clavicle excision
The patient has a clinical history and physical examination consistent with degenerative superior labral pathology, which is supported by the MRI scan. She has failed appropriate nonoperative treatment, and surgical intervention would be indicated. In a middle-aged patient with a degenerative superior labral tear, biceps tenodesis has been shown to have better outcomes and return to sport than SLAP repair. In a young patient with a traumatic superior labral tear, repair would be indicated. The other MRI findings noted are incidental and asymptomatic in this patient. As a result, rotator cuff repair or distal clavicle excision is not indicated.
Correct answer : A
60- A 50-year-old man sustained an external rotation traction injury to his right arm. He felt a pop in the anterior aspect of his shoulder associated with immediate pain and swelling. The MRI scan shows a tear of the subscapularis tendon, as shown in Figures 1 and 2. The arrow points to what anatomic structure?
46
A. Biceps tendon
B. Torn anterior labrum
C. Middle glenohumeral ligament
D. Comma/rotator interval tissue
The anatomic structure labeled is the biceps tendon, which has subluxated medially from the intertubercular groove as a result of disruption of the biceps pulley that occurs with subscapularis tears. The anterior labrum is adjacent to the glenoid and is not normally torn with subscapularis pathology. The middle glenohumeral ligament may appear cord-like, but is shown more medial to the subluxated biceps tendon. The rotator interval tissue, or "comma" tissue, is generally along the upper border of the subscapularis and is pulled toward the coracoid base in subscapularis tears.
Correct answer : A
61- Injuries to what two structures would result in a “floating shoulder"?
A. Clavicle shaft and humeral shaft
B. Scapular body and humeral shaft
C. Rotator cuff and coracoacromial ligament
D. Clavicle shaft and glenoid neck
The superior shoulder suspensory complex (SSSC) is a bone and soft-tissue ring secured to the trunk by superior and inferior bony struts, from which the upper extremity is suspended. The ring is composed of the glenoid process, coracoid process, coracoclavicular ligaments, distal clavicle, acromioclavicular joint, and acromial process. Double lesions of the SSSC are referred to as “floating shoulder” injuries, as in this case in which the injury involves a fractured scapular neck and ipsilateral clavicle fracture. Ipsilateral acromioclavicular dislocation and coracoid fracture is a less common double disruption of the SSSC. Although several case studies have been published on surgical and nonsurgical management of these injuries, no study provides measurable surgical indications beyond the simple presence of the double lesion. This is often referred to as an unstable shoulder girdle. Correct answer : D
47
62- A 25-year old right-hand dominant professional baseball pitcher complains of posteromedial right elbow pain that is worsened by throwing. He also reports occasional paresthesias in his small and ring finger after lengthy bullpen sessions. On examination, he is tender along the medial olecranon and complains of pain when extending the elbow >-
20° of extension. He has negative valgus stress, moving valgus stress, and milking maneuver tests. He is stable to varus stress, chair rise, and lateral pivot shift tests. Radiographs reveal a small osteophyte along the posteromedial border of the olecranon. What is the most likely diagnosis?
A. Valgus extension overload
B. Varus posteromedial rotatory instability (VPMRI) C. Valgus posterolateral rotatory instability (VPLRI) D. Olecranon bursitis
The patient has valgus extension overload. This is a spectrum of pathologies, often seen in pitchers, that begins with posteromedial impingement between the medial olecranon and posterior trochlea during forceful elbow extension. As a result, a medial olecranon osteophyte is typically the first notable imaging finding. As pathology increases, there can be progressive damage to the medial collateral ligament (MCL), degeneration of the radiocapitellar articulation, and neuritis of the ulnar nerve. VPMRI is often associated with a large anteromedial coronoid fracture and posterior band MCL rupture. VPLRI occurs when the lateral collateral ligament complex is ruptured. Olecranon bursitis presents with focal swelling or a fluid collection over the posterior aspect of the olecranon.
Correct answer : A
63- A patient sustains a displaced diaphyseal humerus fracture following a motor vehicle accident. Open reduction internal fixation is indicated due to concomitant lower extremity trauma and is planned through an anterior approach. Which intramuscular interval is exploited during the deep dissection of the mid-humerus in this approach?
A. Lateral head of triceps (radial nerve) and brachialis
(musculocutaneous nerve)
B. Lateral head of the triceps (radial nerve) and biceps brachii
(musculocutaneous nerve)
C. Lateral brachialis (radial nerve) and medial brachialis
(musculocutaneous nerve)
D. Brachialis (musculocutaneous nerve) and coracobrachialis
(musculocutaneous nerve)
48
The anterior approach to the mid-humerus courses along the lateral margin of the biceps brachii. This muscle is swept medially allowing exposure of the brachialis. The brachialis has a dual innervation, with the lateral fibers innervated by the radial nerve and the medial fibers innervated by the musculocutaneous nerve. The humerus is exposed by splitting this muscle in its midline. The lateral head of the triceps resides in the posterior compartment of the arm and is not involved in the anterior approach to the humerus. The interval between brachialis and coracobrachialis is not an internervous plane, as both muscles are supplied by the musculocutaneous nerve.
Correct answer : C
64- Figures 1 and 2 are the current radiographs of a 35-year-old right- hand dominant woman who sustained an acute dislocation to her right elbow after falling from a horse. She underwent a closed reduction and splinting in the emergency department. She describes global elbow pain and difficulty with range of motion. On examination, she has moderate, diffuse elbow swelling with deformity. There are no traumatic wounds, and distally she is neurovascularly intact. Definitive treatment should include
A. repeat closed reduction and casting. B. radial head arthroplasty or fixation. C. radial head excision.
D. arthroscopic loose body removal.
49
This is a young patient who has sustained an elbow dislocation with a radial neck and coronoid fracture to her dominant extremity. Her current radiographs reveal a considerably displaced radial head fragment, along with a small coronoid fracture, and potentially some residual ulnohumeral joint incongruity. A repeat closed reduction is unlikely to be successful, as the radial head is significantly displaced and can block a congruent reduction. Open reduction is required to successfully address this complex injury pattern. Although removal of the radial head can be considered, fixing or replacing the radial head with repair of the lateral collateral ligament is often recommended in the setting of acute trauma to restore adequate stability to the elbow, decrease long-term risk for progressive ulnohumeral arthrosis, and limit sequelae in the setting of an unappreciated longitudinal forearm axis injury.
Correct answer : B
65- Figures 1 and 2 are the radiographs of a 67-year-old woman who underwent shoulder hemiarthroplasty for a proximal humerus fracture dislocation 6 months ago. She now has persistent pain with a pseudoparalytic shoulder. Examination reveals full passive range of motion, but with pain in all directions. Joint aspiration was performed with <50 neutrophils and negative aerobic and anaerobic cultures (anaerobic held for 14 days). What would be her best surgical option for pain relief and improved function?
A. Anatomic total shoulder arthroplasty
B. Revision hemiarthroplasty with allograft prosthetic composite on the humeral side
C. Reverse total shoulder arthroplasty
D. Resection arthroplasty
50
The radiographs provided show lysis of the greater tuberosity and a high-riding humeral head, indicating failure of the rotator cuff. Both anatomic shoulder arthroplasty and revision hemiarthroplasty would suffer from the same functional limitations and risk of instability as the current construct, due to the lack of a functional rotator cuff. Resection arthroplasty is usually reserved for situations of recurrent infection or lack of enough structural bone to allow prosthetic placement. Revision to a reverse total shoulder arthroplasty can bypass the cuff deficiency and treat any component of glenohumeral degeneration and is the best option to reduce pain and improve function in this setting. Correct answer : C
66- A 65-year-old woman has an atraumatic full thickness rotator cuff tear, which is treated successfully with 12 weeks of physical therapy. In discussing future expectations regarding the condition of her rotator cuff, what is the risk of tear progression at 2 years?
A. 0% B. 5%
C. >20% D. >50%
Several studies have demonstrated that degenerative symptomatic rotator cuff tears enlarge over time, which raises some concern regarding treating these injuries nonsurgically. The rate of rotator cuff tear enlargement at 2 years ranges from 20% to 49%, and at 5 years is estimated to be 50%. The risks associated with rotator cuff tear progression includes worsening fatty atrophy and fatty infiltration, decreased tendon pliability, and increased tendon retraction, which can lead to worse clinical outcomes following surgery.
Correct answer : C
67- A 63-year-old right-hand dominant woman has a history of gradually progressive atraumatic right shoulder pain. She describes a constant nagging pain that radiates to her deltoid insertion and difficulty with overhead activities. Her examination and imaging studies confirm a rotator cuff tear. What is the mostly likely initiating anatomic location of her tear?
A. Anterior portion of the supraspinatus tendon adjacent to the biceps tendon
B. 15 mm posterior to the biceps tendon near the supraspinatus/infraspinatus junction
C. Superior portion of the subscapularis tendon
D. 30 mm posterior to the biceps tendon near the supraspinatus/infraspinatus junction
51
Fundamental to understanding the pathogenesis of rotator cuff tears is an appreciation of the likely initiation site of the disease process. Although authors initially postulated that rotator cuff tears originated in the anterior margin of the supraspinatus tendon near the biceps tendon, recent research has challenged this notion. Kim and associates analyzed 360 full-thickness or partial-thickness rotator cuff tears using ultrasonograms. They separated stratified tears based on their anteroposterior size and whether they were partial- or full-thickness tears. The mean width and length of tear size was 16.3 mm and 17 mm, respectively. Histograms showed that the most common tear location for all tears regardless of size was approximately 15 mm posterior to the biceps tendon. This corresponds to the center of the rotator crescent initially described by Burkhart and associates. This location is described as being more susceptible to degeneration secondary to its diminished vascular supply and mechanical properties. The rotator cable is an arch-shaped thick bundle of fibers that is thought to shield the crescent from stress.
Correct answer : B
68- Figures 1 and 2 are the radiograph and MRI scan of a 40-year-old man who fell down a flight of stairs. His upper arm is bruised and painful, and global weakness in the shoulder girdle function is noted. What is the appropriate initial treatment for the acromial finding identified here?
A. Immediate open reduction and internal fixation of the fracture
B. Closed treatment with serial radiographs
C. Fracture fragment excision and deltoid repair
D. Rest, anti-inflammatory medications, and a home exercise program
52
The patient has an os acromiale. The type shown is of the meso-acromion. This is not an acute fracture; well corticated ends are seen on the axillary radiograph, and there is no bone edema on the T2 axial MRI scan. A trial of nonsurgical care that includes rest, ice, and anti-inflammatory medications is recommended. If a patient continues to have symptoms, an arthroscopic evaluation is needed to determine if the os acromiale is mobile and if surgical fixation is appropriate. Correct answer : D
69- A 38-year-old man sustains a terrible triad injury consisting of an elbow dislocation, comminuted and displaced radial head fracture, and a type I coronoid fracture. Intraoperative findings after radial head replacement and lateral collateral ligament complex repair reveal persistent instability consisting of medial opening on valgus stress and posteromedial subluxation of the ulnohumeral and radiocapitellar joints. What is the best next step?
A. Medial collateral ligament repair or reconstruction
B. Reconstruction of the radial collateral ligament
C. Resection of the type I coronoid fracture and capsular repair to the remaining coronoid
D. Open reduction and buttress plating of the coronoid fracture
Terrible triad injuries of the elbow are common, and the management of type I coronoid tip fractures remains controversial. Type I coronoid fractures result in only small changes in elbow kinematics that have been shown to be uncorrected with suture repair. A type I coronoid tip fracture is not amenable to buttress plate fixation. The radial collateral ligament is a component of the lateral collateral ligament complex and has already been repaired. The persistent medial laxity and posteromedial joint subluxation noted is indicative of ongoing instability. The next step would be repair or reconstruction of the medial collateral ligament, which will normally correct the medial instability. Articulated versus static external fixation can be considered if the joint remains unstable despite repair/reconstruction of the damaged stabilizing structures. Correct answer : A
53
70- The fracture seen in Figure 1 is most likely associated with injury to what ligamentous structure?
A. Inferior glenohumeral ligament
B. Acromioclavicular (AC) ligaments
C. Coracoclavicular ligaments
D. Coracoacromial ligament
The radiograph shows an extra-articular distal clavicle fracture lateral to the clavicular attachment point of the coracoclavicular ligaments (conoid and trapezoid). However, unlike a scenario featuring a typical Neer type I fracture, the interval between coracoid and clavicle is clearly widened, and there is marked fracture displacement. This signifies disruption to the coracoclavicular ligaments. The inferior glenohumeral ligament is important to glenohumeral joint stability, but has no effect on the relationship between clavicle and scapula. The AC ligaments are thickenings of the AC joint capsule. They have been shown to be responsible for 90% of anteroposterior stability of the AC joint. The coracoclavicular ligaments are responsible for 77% of stability for superior translation (as in this case). The coracoacromial ligament connects two parts of the scapula (coracoid and acromion) and is part of the arch that supports the rotator cuff.
Correct answer : C
71- What is the most common organism implicated in periprosthetic infection of the shoulder?
A. Methicillin-resistant Staphylococcus aureus (MRSA) B. Cutibacterium acnes
C. Enterococcus species
D. Staphylococcus epidermidis
C acnes is the most common organism recovered in prosthetic shoulder infections (33%), Coagulase-negative Staphylococcus is second (21%), Methicillin-sensitive S aureus (13%), and S epidermidis (10%). MRSA accounts for 5% and Enterococcus species, 1.5%.
Correct answer : B
54
72- Figure 1 is the MR image of a 55-year-old man who sustained an acute traumatic injury to his right shoulder with loss of active range of motion. He was initially evaluated by his primary care physician and treated with physical therapy without success. He was referred to an orthopaedist for surgical consultation 8 weeks after sustaining the injury. The orthopaedic surgeon performs a successful arthroscopic repair but notes poor tendon quality at the repair site. The treating surgeon keeps the patient in a sling full time for 6 weeks without formal therapy. One year after surgery, in comparison to early therapy, this rehabilitation program will likely result in
A. no difference in terminal range of motion.
B. a lower functional outcome score. C. a clinically significant reduction in
passive forward flexion and external rotation.
D. a higher retear rate of the rotator cuff repair.
Historically, orthopaedic surgeons considered early range-of-motion programs following rotator cuff surgery secondary to concerns about potential postsurgical stiffness. Although this may have been a concern with primary open repair, arthroscopic surgery appears to substantially decrease this risk. More recently, investigators are reporting similar results in terms of range of motion, retear rate, and functional outcome scores among patients who undergo early versus delayed rehabilitation programs.
Correct answer : A
73- Stemless shoulder arthroplasty prostheses have recently been suggested as an alternative to traditional stemmed replacement. Advantages of the stemless surgical technique would include
A. better glenoid exposure than with stemmed prostheses.
B. reliable use in four-part proximal humerus fracture reconstruction.
C. use in proximal humeral malunion without the need for an osteotomy. D. improved long-term survivorship profile.
55
Glenoid exposure, while better than with surface replacements, is not improved over traditional stemmed replacements. Metaphyseal comminution would make it unlikely that a stemless implant could be used in most four-part fractures. Stemless replacement does have the unique advantage of allowing placement of a prosthesis in the setting of a proximal humerus malunion without the need for an osteotomy, as the prosthesis is not constrained by the position of the stem. While early results are encouraging, there is no long-term data to suggest that survivorship is increased with stemless arthroplasty. Correct answer : C
74- Figure 1 is the MRI scan of a 25-year-old left-hand dominant minor league pitcher with a 6 month history of progressive left elbow pain during pitching. He fails nonoperative treatment and undergoes surgery to address the problem. What is the most common complication of this procedure?
A. Ulnar nerve neuropraxia
B. Flexor pronator mass avulsion
C. Posterolateral rotatory instability
D. Symptomatic hardware
The MRI scan shows evidence of a medial collateral ligament (MCL) tear. In a patient with a chronic MCL injury that has failed non-operative treatment, MCL reconstruction would be indicated. Initial MCL reconstruction technique involved routine transposition of the ulnar nerve and detachment of the flexor- pronator mass. Subsequent.
technique modifications have been made to minimize complications by avoiding routine ulnar nerve transposition and performing a muscle-splitting approach. Despite these improvements, transient ulnar nerve neuropraxia remains the most common complication, and patients should be counseled about its occurrence pre-operatively. Flexor pronator mass avulsion is more likely with a muscle-detaching approach, but is not more common than ulnar nerve neuropraxia. Posterolateral rotatory instability is a complication of lateral collateral ligament repair or reconstruction, not medial collateral ligament reconstruction. Symptomatic hardware is not a common complication from this procedure
Correct answer : A
56
75- A 35-year-old man presents one week after an acute right shoulder posterior dislocation after being electrocuted. He is evaluated in the emergency department and undergoes closed reduction. The patient reports global right shoulder pain and limited active and passive range of motion. He has mild anterior and lateral bruising. He is distally neurovascularly intact. Current radiographs and an MRI scan are shown in Figures 1 through 3. What is the best next step?
A. Open reduction internal fixation
(ORIF)
B. Sling immobilization in external rotation
C. Bristow-Latarjet
D. Shoulder hemiarthroplasty
The patient has sustained a displaced lesser tuberosity fracture with medial displacement following a posterior shoulder dislocation. Nonoperative management would risk long-term loss of normal subscapularis function, as well as anterior shoulder instability. An ORIF of lesser tuberosity is recommended. The current radiographs do not demonstrate any obvious compromise of glenoid bone stock that would necessitate a coracoid transfer. The humeral head is not compromised; therefore, a hemiarthroplasty is not
indicated. Correct answer : A 57
76- A 51-year-old man sustains the injury shown in the MRI scan in Figures 1 and 2 following a fall. After a thorough discussion regarding risks and benefits, he elects to proceed with surgery. What is the most appropriate surgical treatment for his fracture?
A. Open reduction internal fixation with locking plate
B. Intramedullary (IM) nail
C. Hemiarthroplasty
D. Closed reduction and percutaneous pinning
The patient has sustained a complex proximal humerus fracture with head split component and multiple articular fragments. When the articular surface is significantly compromised, arthroplasty procedures are favored. The only procedure listed that addresses the damaged humeral head is hemiarthroplasty, making it the correct response. Although a possible option, ORIF would be difficult due to the fragmented humeral head, and there would be a high risk for fracture collapse or avascular necrosis. IM nailing will not provide enough control of the fracture pieces, nor will it replace the damaged articular surface. Closed reduction is not an option given the complex nature of the fracture.
Correct answer : C
77- A 68-year-old man presents with chronic progressive right shoulder pain and loss of motion. He has active shoulder elevation of 120° and 5-/5 shoulder forward flexion strength limited by pain. He has exhausted nonsurgical management over the past year and is now interested in surgical intervention. Figure 1 is the preoperative axial CT scan of his shoulder. During surgical reconstruction, the surgeon should anticipate the location of maximal glenoid erosion to be
58
A. posterior. B. superior.
C. posterior inferior. D. posterior superior.
In patients with primary osteo- arthritis of the shoulder, eccent- ric wear on the face of the glenoid is frequently combined with static subluxation of the humeral head. Current studies have clarified that patients with Walch B2 glenoid develop wear along the posterior inferior face of the glenoid and not directly posterior. At the time of shoulder arthroplasty, the eccentric center of rotation must be corrected by soft-tissue, bony, and/or implant
techniques to minimize the risk for poor outcomes. The surgeon should orient
his correction along the posterior inferior to anterior superior plane.
Correct answer : C
78- For humeral shaft fractures, the characteristic most associated with radial nerve palsy is
A. open fracture.
B. distal one-third fracture.
C. proximal one-third fracture. D. comminuted fracture.
Distal third humeral shaft fractures are associated with the highest incidence of radial nerve palsy at 23.6% The classic example is a Holstein Lewis fracture, which is a spiral fracture of the mid-third / distal-third junction. Open fractures are not associated with a higher incidence of radial nerve palsy than closed fractures. Comminution has not been associated with an increase in radial nerve palsy. In fact, transverse and spiral fractures are associated with a higher incidence of radial nerve palsy than comminuted fractures. Proximal humerus fractures have an incidence of only 1.8%.
Correct answer : B
59
79- Figures 1 and 2 are the radiograph and axial CT scan of a 75-year-old woman with diffuse superior shoulder pain 5 months after an uneventful reverse shoulder arthroplasty. She denies trauma, but felt a "pop" when reaching overhead. She had initially done well postoperatively. On physical examination, she has decreased active forward flexion with pain and diffuse superior tenderness along the scapular spine and acromion. There are no signs or symptoms of infection. What is the best next step in management?
A. Application of bone stimulator
B. Open reduction and internal fixation
(ORIF)
C. Physical therapy for deltoid strengthening
D. Sling immobilization for 6 weeks
The radiograph shows a well-positioned reverse total shoulder and the axial CT image demonstrates a minimally displaced fracture through the midacromion. Acromial fracture is a concerning and not uncommon complication that can have devastating effects after reverse shoulder arthroplasty, as function is highly dependent on the deltoid muscle. Fractures can occur at the scapular spine, which may be related to placement of peripheral baseplate screws. Acromial fracture has been reported to occur as early as 1 month postoperatively and as late as 8 years postoperatively. The reported incidence is <8%, and multiple authors note decreases in shoulder elevation and shoulder outcome scores compared with those in patients with reverse shoulder arthroplasty without a fracture. Patients with a fracture can complain of superior shoulder pain that may radiate to the deltoid area and usually report an acute onset of pain or loss of function after initially good clinical progress. The diagnosis can be difficult to determine and is missed on plain radiographs in up to 20% of cases. CT scans are helpful. Treatment is typically nonoperative with sling immobilization for 6 weeks and then
60
advancing activities as tolerated. A bone stimulator and ORIF would not be indicated initially, but could be used if healing does not progress as expected. Continued physical therapy with strengthening would be contraindicated until fracture union is achieved.
Correct answer : D
80- A 76-year-old right-hand dominant woman falls at home, sustaining a displaced 4-part left proximal humerus fracture. When compared with initial treatment with a reverse shoulder arthroplasty, revising a failed open reduction and internal fixation (ORIF) to a reverse shoulder arthroplasty results in
A. higher complication rate.
B. improved functional outcomes. C. lower rates of instability.
D. decreased rate of revision surgery.
When compared to initial treatment with reverse total shoulder arthroplasty, patients who initially undergo ORIF with subsequent revision to reverse total shoulder arthroplasty demonstrate a higher complication rate, increased rate of revision surgery, increased risk of instability, and similar functional outcomes.
Correct answer : A
81- A 45-year-old man with a history of gout in his foot 2 years ago presents with a 3-day history of atraumatic elbow pain. The pain is diffuse, constant, and worse with any movement. Examination shows motion from -20° extension to 90° flexion with pain. There is no erythema around his elbow, but there is mild warmth. He has no fever, and neurovascular examination is unremarkable. Radiographs show an effusion. Serum uric acid level is within normal limits. What is the next diagnostic step?
A. Elbow joint aspiration
B. MRI scan
C. Splint for 2 weeks and repeat examination
D. Sedimentation rate and C-reactive protein level
The patient appears to be experiencing a recurrent gout flare. The best way to confirm the diagnosis is to aspirate the joint and send it for culture, cell count, and crystal examination. This will identify the diagnosis of infection, gout, or pseudogout. An MRI scan will confirm the presence of an effusion, but it will not reveal the cause. A splint may result in pain improvement, but it will not contribute to a diagnosis or definitive treatment. Sedimentation rate and
61
C-reactive protein levels can be elevated in either inflammatory or infectious processes, but these are non-specific and cannot differentiate between the two.
Correct answer : A
82- Figures 1 through 5 are the radiographs and CT scans of a 59-year- old woman who has had 10 years of worsening right shoulder pain. She reports a progression of symptoms, despite multiple corticosteroid injections, nonsteroidal anti-inflammatory drugs, and physical therapy. Her active and passive forward elevation is 100°, external rotation with the arm at the side is 20°, and internal rotation is to L5. What is the best next step?
A. Arthroscopic shoulder debridement
B. Rotator cuff repair
C. Shoulder hemiarthroplasty
D. Total shoulder arthroplasty
62
The patient's radiographs and CT scan show advanced glenohumeral osteoarthritis with posterior humeral head subluxation and mild posterior glenoid erosion (Walch type B2 glenoid). The preferred type of shoulder arthroplasty in this setting remains controversial, as there are data to support both anatomic and reverse total shoulder arthroplasty. There is no significant atrophy of the rotator cuff musculature on sagittal CT to suggest a rotator cuff tear, and a rotator cuff repair is likely contraindicated by the degree of underlying arthritis. A glenohumeral joint debridement would be expected to provide only partial/short-term pain improvement, and is unlikely to be a long- term solution. A shoulder hemiarthroplasty has been shown to result in worse pain relief and functional outcomes than total shoulder arthroplasty in this setting.
Correct answer : D
83- A 23-year-old minor league pitcher describes the insidious onset of posterior shoulder pain during the late cocking phase of his throwing motion. He has gone 6 weeks without throwing, but symptoms quickly returned on return to play. An MR arthrogram of the shoulder reveals fraying of the superior labrum and proximal biceps, and a partial- thickness articular-sided supraspinatus tear (30% tendon thickness). Figure 1 is a representative coronal MRI slice. Clinical examination demonstrates mild weakness of the periscapular muscles, mild superior rotator cuff weakness, and negative instability testing. Internal rotation with the arm in 90⁰ of abduction is 40⁰ in the affected shoulder versus 70⁰ in the contralateral shoulder. What is the best next step?
A. Intra-articular platelet rich plasma (PRP) injection
B. Therapy regimen focused on shoulder range of motion and strengthening
C. Arthroscopic surgery for rotator cuff and labral debridement
D. Arthroscopic surgery for rotator cuff repair and biceps tenodesis
63
Internal impingement is a condition that affects overhead throwing athletes, as the greater tuberosity and articular surface of the rotator cuff contact the posterosuperior glenoid during maximal shoulder abduction and external rotation. The etiology is typically multifactorial, but common contributors include posterior capsular contracture, scapular dyskinesia, and subtle anterior shoulder laxity. Nonoperative management, the mainstay of treatment, includes rest, stretching, scapular strengthening, and proprioception. Results of surgical intervention are variable; therefore, nonoperative measures should be exhausted first. While PRP is currently being investigated as a biologic augmentation in a number of shoulder pathologies, it is not considered first- line treatment.
Correct answer : B
84- A 45-year-old woman with diabetes has a 3-month history of atraumatic left shoulder pain and motion loss. She previously underwent treatment with nonsteroidal anti-inflammatory medication and a home stretching program, experiencing minimal relief of her symptoms. Examination reveals loss of passive external rotation, abduction, and forward elevation without reduction in strength. Radiographs are normal. What is the most appropriate next step?
A. MRI scan with and without contrast
B. Cortisone injection therapy with continued physical therapy (PT) C. Closed manipulation under anesthesia
D. Arthroscopic release with manipulation under anesthesia
The patient's history and physical exam are consistent with adhesive capsulitis, or frozen shoulder. Adhesive capsulitis is most commonly an idiopathic process that results in joint pain and loss of motion from capsular contracture. It is reported to affect approximately 2% to 5% of the general population, typically affecting middle-age women. Secondary causes include previous trauma, as well as associated medical conditions such as diabetes, stroke, and cardiac and thyroid disease. Debate remains as to whether a genetic predisposition for the development of adhesive capsulitis exists, despite the increased frequency noted in twin studies. Although the underlying etiology and pathophysiology are not well understood, the consensus is that synovial inflammation and capsular fibrosis result in pain and joint volume loss. It is hypothesized that in patients with diabetes, an increased rate of glycosylation and cross-linking of the shoulder capsule raises the incidence of frozen shoulder.
The natural history of adhesive capsulitis is spontaneous resolution, therefore, conservative measures are the mainstay of treatment. As the patient has seen little benefit from NSAIDs and a home exercise program, more aggressive intervention is reasonable. In terms of injections, glenohumeral corticosteroid
injection, subacromial corticosteroid injection, and hydrodilation have all 64
demonstrated benefit. Radiographs are usually obtained to exclude other causes of shoulder pain such as glenohumeral arthrosis, malignancy, calcific tendonitis, impingement, and acromioclavicular degeneration. If pain and stiffness persist beyond 6 months, surgical intervention may be considered in the form of closed manipulation or arthroscopic release. Complications of closed manipulation include humerus fracture, glenohumeral dislocation, hematoma, rotator cuff and labral tears, and brachial plexus injury. Arthroscopic release is advocated by some, as it allows for examination of concomitant pathology and controlled release of capsular tissue, with the potential for reduced force when performing the manipulation portion of the procedure. Controversy remains as to whether posterior capsular release should be routinely performed because studies have shown outcomes to be similar with anterior and combined approaches. Therapy should be initiated early after intervention, with some surgeons advocating admission to the hospital with inpatient therapy for pain management and compliance.
Correct answer : B
85- Figures 1 and 2 are the radiographs of a 48-year-old right-hand dominant man who reports progressive pain and stiffness of the elbow. He sustained a fracture dislocation 10 years ago, which was treated with surgical reconstruction. On examination, range of motion is from 40° extension to 110° flexion, with pain at end-range of motion, but no pain through mid-range. A previous corticosteroid injection temporarily improved his pain but did not improve range of motion. The patient elects to undergo an arthroscopic osteocapsular arthroplasty. What structures need to be addressed to improve elbow extension?
65
A. Anterior capsule and osteophytes within anterior compartment
B. Posterior capsule and osteophytes within posterior compartment C. Anterior capsule and osteophytes within posterior compartment D. Posterior capsule and osteophytes within anterior compartment
The patient is young, active, and has evidence of post-traumatic elbow osteoarthritis. His motion is limited by capsular contracture and large osteophytes in the anterior and posterior compartments. He has failed nonoperative treatment, and surgery is indicated to improve his range of motion and function. Arthroscopic osteocapsular arthroplasty allows removal of impinging osteophytes and release of hypertrophied capsule and has been shown to be effective at relieving pain and improving motion in patients with mild to moderate osteoarthritis. Anterior capsular contracture and posterior bony impingement limit extension and must be addressed to improve motion. Posterior capsular contracture and anterior osteophytes limit flexion.
Correct answer : C
86- Figures 1 through 4 are the radiographs of a 47-year-old right-hand dominant man who was involved in an altercation. What is the most appropriate method to address his radial head injury?
66
A. Immobilization followed by functional therapy B. Open reduction and internal fixation (ORIF) C. Radial head excision
D. Radial head arthroplasty
The images demonstrate a comminuted radial head fracture with extension into the radial neck. There is persistent fracture displacement following closed reduction of the elbow. The preferred treatment of radial head fractures with >3 parts in active individuals is radial head arthroplasty. ORIF has higher rates of failure when used for 3- and 4-part fractures. Radial head excision is typically discouraged in the acute setting, as this can contribute to elbow and forearm axis instability.
Correct answer : D
87- A 26-year-old recreational athlete sustained an initial shoulder dislocation 1 year ago and was treated nonsurgically. He recently sustained a second dislocation and is scheduled for surgical repair. Plain radiographs and MRI scans reveal no bony defect. What is the difference in rates of recurrent instability after open versus arthroscopic repair?
A. Recurrence after open surgery is twice that of arthroscopic repair
B. Recurrence after arthroscopic surgery is twice that of open repair
C. Recurrence after arthroscopic repair generally occurs at an earlier time than after open repair
D. There is no difference in recurrence after open and arthroscopic repair
Traditionally, recurrence rates associated with open stabilization procedures have been lower than rates associated with arthroscopic repair. Recent studies show that for patients without significant bone loss, however, the recurrence rate is the same for open and arthroscopic surgeries.
Correct answer : D
88- How does concomitant ulnar nerve pathology affect the outcome of patients treated operatively for medial epicondylitis?
A. Concomitant ulnar nerve pathology has no impact on outcome. B. Concomitant moderate or severe ulnar neuropathy treated with
transposition leads to worse outcomes compared with no ulnar nerve pathology.
C. Concomitant moderate or severe ulnar neuropathy treated with transposition leads to improved outcomes compared with no ulnar nerve pathology.
D. Concomitant mild ulnar neuropathy treated with transposition leads to improved outcomes than no ulnar nerve pathology. 67
89- Figures 1 and 2 are the radiographs of a 64-year-old woman with a history of rheumatoid arthritis (RA) who complains of right elbow pain. She has been treated with tumor necrosis factor-alpha inhibitors and oral corticosteroids for several years. What process is primarily responsible for the radiographic joint destruction?
A. Traumatic insult resulting in complement activation
B. Mutation in the rheumatoid factor gene
C. Osteoblast paracrine signaling resulting in proteolytic collagen degradation
D. Inflammation resulting in a hyperplastic synovial joint lining
RA is a systemic inflammatory disorder marked by erosive arthritis in multiple joints. Elbow involvement is common. The pathologic lesion in RA is pannus, a hyperplastic synovial proliferation that ultimately results in proteoglycan and collagen digestion. Rheumatoid factor mutations, traumatic insults resulting in complement activation, and osteoblast paracrine signaling are not involved in the pathologic process. The Larsen classification assesses the progression of rheumatoid changes in the elbow. Stage I is characterized by osteopenia without joint space narrowing. Stage II indicates joint space narrowing but a normal joint contour. Stage III is marked by joint space loss. This patient has stage IV disease, as seen by the advanced erosive changes with trochlear groove deepening and resulting deformity. Stage V is ankylosis.
Correct answer : D
68
90- Figures 1 through 4 are the radiographs and CT scan of a 63-year-old right-hand dominant man with long- standing left shoulder pain, which now limits his activities of daily living. Examination shows elevation to
150° with markedly limited internal and external rotation. Strength testing is limited by pain. Previous treatments have included physical therapy, steroid injections, and platelet-rich plasma (PRP) injections. An MRI scan shows a partial articular supraspinatus tendon avulsion (PASTA) lesion measuring <50% tendon thickness, a superior labrum anterior to posterior (SLAP) tear, and glenohumeral degeneration with multiple intra-articular loose bodies. What is the best next step?
A. Stem cell injection
B. Arthroscopic rotator cuff repair, biceps tenodesis, and extensive debridement with removal of loose bodies
C. Anatomic total shoulder arthroplasty
D. Reverse shoulder arthroplasty
69
In a patient with end-stage glenohumeral arthritis, the preferred treatment after failing nonoperative treatment would be anatomic shoulder arthroplasty. Recent literature has demonstrated good outcomes even in the setting of partial rotator cuff tears, with or without repair. Stem cell injections are costly and have not been shown to be effective. Arthroscopic treatment may improve pain and function in the short term, but results are unlikely to be long-lasting. Reverse shoulder arthroplasty could be considered; however, there are more long-term studies supporting anatomic total shoulder arthroplasty in this patient population.
Correct answer : C
91- A 75-year-old man sustains an anterior dislocation of his reverse total shoulder arthroplasty. What activity places the arm in the position most commonly associated with instability of a reverse total shoulder arthroplasty?
A. Scratching the opposite shoulder
B. Pushing off ipsilateral chair armrest while standing up
C. Tying shoelaces on the contralateral foot
D. Reaching up to comb hair
Proper soft-tissue tension is critical to prevent instability of a reverse total shoulder. The arm position implicated in reverse total shoulder instability is extension, adduction, and internal rotation, such as pushing out of a chair. The other positions described do not involve extension of the shoulder.
Correct answer : B
92- What is the best way to treat patients with a positive nasal swab for methicillin-resistant Staphylococcus aureus (MRSA) prior to elective shoulder arthroplasty?
A. No treatment is necessary.
B. Apply 5% povidone-iodine solution to each nostril for 10 seconds 1 hour before surgery.
C. Prescribe one week of doxycycline prior to surgery.
D. Apply 2% mupirocin ointment to each nostril on the morning of surgery.
Patients with a positive nasal swab for MRSA can be treated preoperatively with 2% mupirocin to the nares twice daily for 5 days, or 5% povidone-iodine solution to each nostril for 10 seconds per nostril, 1 hour before surgery. S aureus is a gram-positive bacterium capable of both aerobic and anaerobic metabolism. The addition of MRSA and/or methicillin-sensitive S aureus nasal screening, along with a perioperative decolonization protocol, has resulted in a
69% decrease in surgical site infection. It has been shown that prevention programs for staphylococcal periprosthetic joint infections can result in
substantial cost savings. Correct answer : B
70
93- Figure 1 is the clinical photograph of a 22-year-old college pitcher who complains of posterior shoulder pain and feelings of shoulder weakness. He denies shoulder trauma. Evaluation should include
A. CT scan of the shoulder.
B. ultrasonography of the rotator cuff.
C. vascular studies of the upper extremity.
D. electrodiagnostic studies.
The patient has atrophy of the infraspinatus. This would be consistent with either a massive rotator cuff tear or suprascapular neuropathy/compression. Given the
patient's age and the atraumatic onset of symptoms, a significant rotator cuff injury is unlikely, making a suprascapular nerve issue the most likely diagnosis. Electrodiagnostic studies would be most accurate in confirming nerve compression and would aid in localizing the area of compression between the spinoglenoid notch and the suprascapular notch. An MRI scan also would be beneficial to evaluate for any compressive lesion on the nerve, such as a paralabral cyst. Because rotator cuff pathology is unlikely, ultrasonography of the rotator cuff would be of little benefit. CT scan of the shoulder may allow grading of the atrophy of the muscle, but will not be as sensitive for a paralabral cyst/labral tear. Vascular studies would not aid in the diagnosis.
Correct answer : D
94- Figures 1 and 2 are the CT and MRI scans of a 23-year-old man with a history of recurrent anterior shoulder dislocations. He had his first dislocation while in basic training for the military 4 years ago. Since that time, his shoulder has dislocated with less and less provocation, to the point that it now dislocates in his sleep. Examination demonstrates significant apprehension with abduction/external rotation. What is the most appropriate treatment to prevent recurrent shoulder instability?
71
A. Arthroscopic Bankart repair
B. Latarjet
C. Hill-Sachs remplissage
D. Physical therapy
The patient has historical and clinical evidence of significant anterior shoulder instability. The imaging demonstrates significant anteroinferior glenoid bone loss, with a very shallow Hill-Sachs deformity. Patient factors that contribute to recurrent instability
risk include type of sport/activity, age at the time of first dislocation, hyperlaxity, and glenoid bone loss (and/or bipolar bone loss), and these can be utilized to determine if an arthroscopic or open solution is most appropriate. In this patient, restoring glenoid bone stock appears to be the most important variable in stabilizing the shoulder. “Critical” glenoid bone loss has frequently been reported to be >20-25%. In this case, significant bone loss can be suspected from the patient's history, including the number of dislocations, ease of dislocation and reduction, and instability in mid-range of motion.
Correct answer : B
95- How do outcomes and postoperative care of patients undergoing total elbow arthroplasty differ depending on diagnosis?
A. Those performed for inflammatory arthritis have a lower revision rate than those for osteoarthritis.
B. Activity modifications are not required in elbow replacements done for osteoarthritis.
C. Those performed for inflammatory arthritis have a higher failure rate than those for fracture sequelae.
D. Outcomes are similar despite indication.
Over the years, indications for total elbow arthroplasty (TEA) have evolved. With the introduction of better medications for rheumatoid arthritis and other inflammatory arthritides, end-stage arthritis of the elbow from this pathology has become less common. At the same time, there has been increased interest in TEA for treatment of acute distal humerus fractures, and ongoing use for fracture sequelae and osteoarthritis. Fevang and associates found in the Norwegian registry that fracture sequelae led to a 5.8 relative risk of failure
72
compared with inflammatory arthritis. Data from the state of New York found that revision rates for osteoarthritis were 14.7%, whereas those for inflammatory arthritis were only 8.3%. All patients require a 5-lb lifetime lifting limit postoperatively to improve the longevity of the prosthesis.
Correct answer : A
96- Figures 1 through 3 are the MRI scans of a 50-year-old man who sustained a first-time traumatic anterior shoulder dislocation after a fall. What is the most appropriate treatment?
A. Latarjet
B. Rotator cuff repair
C. Bankart repair
D. Superior labrum anterior to posterior (SLAP) repair
Multiple studies have shown that the most common associated injury following traumatic shoulder dislocation (besides anteroinferior labral lesions) are full-thickness rotator cuff tears, especially in patients >40 years of age. Robinson and associates found a
73
33.4% incidence of traumatic rotator cuff tears in this setting. Ro and associates reported rotator cuff tears in 18% of their study population. A level IV systematic review found that patients with rotator cuff tears following shoulder dislocations have more persistent pain and shoulder dysfunction. Rotator cuff repair surgery resulted in improved pain and patient satisfaction compared with those treated nonoperatively.
Correct answer : B
97- A complication associated with using the Morrey approach (triceps reflecting) to implant a semiconstrained total elbow arthroplasty is
A. loss of elbow extensor power. B. implant dislocation.
C. implant malposition.
D. development of heterotopic ossification.
Numerous approaches can be used to implant a total elbow arthroplasty. The Morrey approach identifies, transposes, and protects the ulnar nerve, and then subperiosteally reflects the triceps off the ulna. The sleeve of tissue is very thin distally, and the triceps need to be meticulously repaired at the time of closure. Implant dislocation and malposition are less likely with an extensile approach, and dislocation is unlikely with a semiconstrained implant. The development of heterotopic ossification is unrelated to the surgical approach used for elbow arthroplasty. Correct answer A
98- A 36-year-old recreational athlete feels a pop in his antecubital fossa while lifting weights. He has pain, swelling, and deformity. Representative sagittal and coronal MRI slices are shown in Figures 1 and 2, respectively. What is the most common major complications associated with surgical repair of this structure?
74
A. Symptomatic heterotopic ossification requiring reoperation
B. Brachial artery laceration
C. Deep infection
D. Posterior interosseous nerve palsy
The MRI scan shows a distal biceps tendon rupture with retraction. Tendon rerupture and PIN palsy are the two most common major complications following distal biceps repair surgery. Major complication rates are not found to differ by sex, history of tobacco use, age, exposure type (single versus two
incisions), tear morphology (full versus partial), or type of fixation used.
Correct answer : D
99- Figure 1 is the radiograph of a 21-year-old right-hand dominant patient. Compared with nonoperative treatment, open reduction internal fixation (ORIF) results in
A. lower complication rates. B. lower rates of nonunion. C. increased time to union. D. increased functional
outcome scores.
When comparing operative fixation of displaced clavicle fractures with nonoperative treatment, ORIF results in lower rates of nonunion, faster time to union, and similar outcome scores. There is an increased risk of complication, including infection, neurovascular insult, and the need for additional surgery. Correct answer : B
75
100- What are the components of the lateral ligament complex of the elbow?
A. Radial collateral ligament, lateral ulnar collateral ligament, annular ligament
B. Lateral ulnar collateral ligament (LUCL, anterior and posterior band) and the annular ligament
C. Transverse ligament, radial collateral ligament, lateral ulnar collateral ligament
D. Ulnar collateral ligament (anterior and posterior bands), transverse ligament
The important ligaments on the lateral side of the elbow are thickenings of the capsule. The lateral collateral ligament complex consists of four components: the lateral (radial) collateral ligament (LCL), the LUCL, the accessory LCL, and the annular ligament. The medial collateral ligament complex is a capsular thickening consisting of three components: the anterior band, the posterior band, and the transverse ligament. The LUCL is the most important portion of the lateral ligament in terms of posterolateral rotatory instability.
Correct answer : A
76
77
78
QUESTION 32 OF 50
rfl
I "
Figure 59a Figure 59b
A 12-year-old girl with foot pain who has been diagnosed with hereditary motor sensory neuropathy is seen for the foot deformity shown in Figure 59a. A “block test” is performed and shown in Figure 59b. What is the most appropriate management for this patient?

I "
Figure 59a Figure 59b
A 12-year-old girl with foot pain who has been diagnosed with hereditary motor sensory neuropathy is seen for the foot deformity shown in Figure 59a. A “block test” is performed and shown in Figure 59b. What is the most appropriate management for this patient?
1
Observation
2
Corrective shoes
3
Plantar release with first metatarsal osteotomy and possible tendon transfers
4
Calcaneal osteotomy
5
Triple arthrodesis
DISCUSSION: The hindfoot varus in this individual with a cavovarus deformity is nonstructural as shown by the “block test”. Therefore, surgical procedures directed at correcting the hindfoot deformity are not necessary. Observation is not in order and shoe modifications have not been shown to be effective in managing this problem. The patient is symptomatic; therefore, the treatment of choice is plantar release with first metatarsal osteotomy and possible tendon transfers.
REFERENCES: Paulos L, Coleman SS, Samuelson KM: Pes cavovarus: Review of a surgical approach
using selective soft-tissue procedures. J Bone Joint Surg Am 1980;62:942-953.
McCluskey WP, Lovell WW, Cummings RJ: The cavovarus foot deformity: Etiology and management. Clin Orthop Relat Res 1989;247:27-37.
Ward CM, Dolan LA, Bennett DL, et al: Long-term results of reconstruction for treatment of a flexible
cavovarus foot in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 2008;90:2631-2642.
50 • American Academy of Orthopaedic Surgeons
Figure 60a Figure 60b Figure 60c
REFERENCES: Paulos L, Coleman SS, Samuelson KM: Pes cavovarus: Review of a surgical approach
using selective soft-tissue procedures. J Bone Joint Surg Am 1980;62:942-953.
McCluskey WP, Lovell WW, Cummings RJ: The cavovarus foot deformity: Etiology and management. Clin Orthop Relat Res 1989;247:27-37.
Ward CM, Dolan LA, Bennett DL, et al: Long-term results of reconstruction for treatment of a flexible
cavovarus foot in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 2008;90:2631-2642.
50 • American Academy of Orthopaedic Surgeons
Figure 60a Figure 60b Figure 60c
QUESTION 33 OF 50
of 100
Which image seen during arthroscopic treatment is most likely associated with this patient’s condition?
A
b c
d
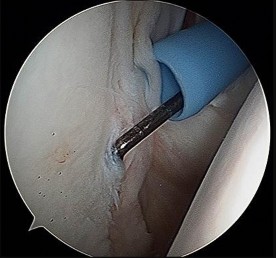


Which image seen during arthroscopic treatment is most likely associated with this patient’s condition?
A
b c
d
1
Figure 10a
2
Figure 10b
3
Figure 10c
4
Figure 10d
This patient’s clinical presentation is consistent with internal impingement accompanied by glenohumeral internal rotation deficit (GIRD). Although throwers may have increased external rotation, their overall arc of motion should be the same as on the nonthrowing side. In comparison, patients with GIRD experience a marked decrease in arc of motion, particularly in internal rotation.
Internal impingement represents a spectrum of findings that can include superior and posterior labral tears, undersurface (articular-sided) tearing of the posterior supraspinatus, posterior glenoid wear, and scar formation of the posterior capsule. Myers and associates demonstrated internal impingement is associated with GIRD, although the latter by itself may be asymptomatic and perhaps a sports-specific adaptation. However, posterior capsular tightness can lead to posterosuperior translation of the humerus during throwing, leading to these injuries. Internal impingement is common among overhead throwing athletes and occurs during the late cocking and early acceleration phases of throwing. Humeral migration during the abducted/externally rotated throwing position results in abutment of the greater tuberosity against the posterosuperior glenoid labrum, which impinges the rotator cuff (Paley and associates).
Pain is often posterior, but symptoms can be vague. Patients may have examination findings consistent with rotator cuff weakness and superior labrum anterior to posterior (SLAP)/biceps involvement. Radiograph findings can be negative, although a Bennett lesion involving hypertrophy and mineralization of the posterior capsular injury may be seen (Wright and Paletta). A CT scan may show glenoid retroversion (Crockett and associates), while MR imaging should be reviewed for a possible partial articular-sided rotator cuff tear, SLAP tear, or increased signal in the posterosuperior labrum or greater tuberosity.
Treatment of this condition should be the focus on therapy, and most cases can be treated nonsurgically. Stretching aimed at the posterior capsule (ie, sleeper stretch) has been reported as effective (Tyler and associates, Litner and associates). Burkhart and associates also demonstrated posterior capsular stretching can help prevent throwing injuries. Because cuff pathology may be present, physical therapy also should include rotator strengthening, scapular stabilization, and addressing of issues related to throwing mechanics (Drakos and associates). Kibler and associates published a comprehensive rehabilitation guideline. Surgical intervention is reserved for those who fail 6 months of nonsurgical treatment and is directed by intra-articular pathology (debridement vs repair of the rotator cuff and labrum) (Braun and associates).
RECOMMENDED READINGS
13. [Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology Part I: pathoanatomy and biomechanics. Arthroscopy. 2003 Apr;19(4):404-20. Review. PubMed PMID: 12671624. ](http://www.ncbi.nlm.nih.gov/pubmed/12671624)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12671624)
14. [Braun S, Kokmeyer D, Millett PJ. Shoulder injuries in the throwing athlete. J Bone Joint Surg Am. 2009 Apr;91(4):966-78. doi: 10.2106/JBJS.H.01341. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/19339585)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19339585)
15. [Crockett HC, Gross LB, Wilk KE, Schwartz ML, Reed J, O'Mara J, Reilly MT, Dugas JR, Meister K, Lyman S, Andrews JR. Osseous adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. Am J Sports Med. 2002 Jan-Feb;30(1):20-6. ](http://www.ncbi.nlm.nih.gov/pubmed/11798991)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11798991)
16. [Drakos MC, Rudzki JR, Allen AA, Potter HG, Altchek DW. Internal impingement of the shoulder in the overhead athlete. J Bone Joint Surg Am. 2009 Nov;91(11):2719-28. doi: 10.2106/JBJS.I.00409. Review. PubMed PMID: 19884449.](http://www.ncbi.nlm.nih.gov/pubmed/19884449)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19884449)
17. [Kibler WB, McMullen J, Uhl T. Shoulder rehabilitation strategies, guidelines, and practice. Orthop Clin North Am. 2001 Jul;32(3):527-38. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/11888148)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11888148)
18. [Lintner D, Mayol M, Uzodinma O, Jones R, Labossiere D. Glenohumeral internal rotation deficits in professional pitchers enrolled in an internal rotation stretching program. Am J Sports Med. 2007 Apr;35(4):617-21. Epub 2007 Feb 9. PubMed PMID: 17293473. ](http://www.ncbi.nlm.nih.gov/pubmed/17293473)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17293473)
19. [Myers JB, Laudner KG, Pasquale MR, Bradley JP, Lephart SM. Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med. 2006 Mar;34(3):385-91. Epub 2005 Nov 22. PubMed PMID: 16303877. ](http://www.ncbi.nlm.nih.gov/pubmed/16303877)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16303877)
20. [Paley KJ, Jobe FW, Pink MM, Kvitne RS, ElAttrache NS. Arthroscopic findings in the overhand throwing athlete: evidence for posterior internal impingement of the rotator cuff. Arthroscopy. 2000 Jan-Feb;16(1):35-40. PubMed PMID: 10627343. ](http://www.ncbi.nlm.nih.gov/pubmed/10627343)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10627343)
21. [Tyler TF, Nicholas SJ, Lee SJ, Mullaney M, McHugh MP. Correction of posterior shoulder tightness is associated with symptom resolution in patients with internal impingement. Am J Sports Med. 2010 Jan;38(1):114-9. doi: 10.1177/0363546509346050. Epub 2009 Dec 4. ](http://www.ncbi.nlm.nih.gov/pubmed/19966099)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19966099)
22. [Wright RW, Paletta GA Jr. Prevalence of the Bennett lesion of the shoulder in major league pitchers. Am J Sports Med. 2004 Jan-Feb;32(1):121-4. PubMed PMID: 14754734. ](http://www.ncbi.nlm.nih.gov/pubmed/14754734)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14754734)
Internal impingement represents a spectrum of findings that can include superior and posterior labral tears, undersurface (articular-sided) tearing of the posterior supraspinatus, posterior glenoid wear, and scar formation of the posterior capsule. Myers and associates demonstrated internal impingement is associated with GIRD, although the latter by itself may be asymptomatic and perhaps a sports-specific adaptation. However, posterior capsular tightness can lead to posterosuperior translation of the humerus during throwing, leading to these injuries. Internal impingement is common among overhead throwing athletes and occurs during the late cocking and early acceleration phases of throwing. Humeral migration during the abducted/externally rotated throwing position results in abutment of the greater tuberosity against the posterosuperior glenoid labrum, which impinges the rotator cuff (Paley and associates).
Pain is often posterior, but symptoms can be vague. Patients may have examination findings consistent with rotator cuff weakness and superior labrum anterior to posterior (SLAP)/biceps involvement. Radiograph findings can be negative, although a Bennett lesion involving hypertrophy and mineralization of the posterior capsular injury may be seen (Wright and Paletta). A CT scan may show glenoid retroversion (Crockett and associates), while MR imaging should be reviewed for a possible partial articular-sided rotator cuff tear, SLAP tear, or increased signal in the posterosuperior labrum or greater tuberosity.
Treatment of this condition should be the focus on therapy, and most cases can be treated nonsurgically. Stretching aimed at the posterior capsule (ie, sleeper stretch) has been reported as effective (Tyler and associates, Litner and associates). Burkhart and associates also demonstrated posterior capsular stretching can help prevent throwing injuries. Because cuff pathology may be present, physical therapy also should include rotator strengthening, scapular stabilization, and addressing of issues related to throwing mechanics (Drakos and associates). Kibler and associates published a comprehensive rehabilitation guideline. Surgical intervention is reserved for those who fail 6 months of nonsurgical treatment and is directed by intra-articular pathology (debridement vs repair of the rotator cuff and labrum) (Braun and associates).
RECOMMENDED READINGS
13. [Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology Part I: pathoanatomy and biomechanics. Arthroscopy. 2003 Apr;19(4):404-20. Review. PubMed PMID: 12671624. ](http://www.ncbi.nlm.nih.gov/pubmed/12671624)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12671624)
14. [Braun S, Kokmeyer D, Millett PJ. Shoulder injuries in the throwing athlete. J Bone Joint Surg Am. 2009 Apr;91(4):966-78. doi: 10.2106/JBJS.H.01341. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/19339585)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19339585)
15. [Crockett HC, Gross LB, Wilk KE, Schwartz ML, Reed J, O'Mara J, Reilly MT, Dugas JR, Meister K, Lyman S, Andrews JR. Osseous adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. Am J Sports Med. 2002 Jan-Feb;30(1):20-6. ](http://www.ncbi.nlm.nih.gov/pubmed/11798991)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11798991)
16. [Drakos MC, Rudzki JR, Allen AA, Potter HG, Altchek DW. Internal impingement of the shoulder in the overhead athlete. J Bone Joint Surg Am. 2009 Nov;91(11):2719-28. doi: 10.2106/JBJS.I.00409. Review. PubMed PMID: 19884449.](http://www.ncbi.nlm.nih.gov/pubmed/19884449)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19884449)
17. [Kibler WB, McMullen J, Uhl T. Shoulder rehabilitation strategies, guidelines, and practice. Orthop Clin North Am. 2001 Jul;32(3):527-38. Review. ](http://www.ncbi.nlm.nih.gov/pubmed/11888148)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11888148)
18. [Lintner D, Mayol M, Uzodinma O, Jones R, Labossiere D. Glenohumeral internal rotation deficits in professional pitchers enrolled in an internal rotation stretching program. Am J Sports Med. 2007 Apr;35(4):617-21. Epub 2007 Feb 9. PubMed PMID: 17293473. ](http://www.ncbi.nlm.nih.gov/pubmed/17293473)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17293473)
19. [Myers JB, Laudner KG, Pasquale MR, Bradley JP, Lephart SM. Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med. 2006 Mar;34(3):385-91. Epub 2005 Nov 22. PubMed PMID: 16303877. ](http://www.ncbi.nlm.nih.gov/pubmed/16303877)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16303877)
20. [Paley KJ, Jobe FW, Pink MM, Kvitne RS, ElAttrache NS. Arthroscopic findings in the overhand throwing athlete: evidence for posterior internal impingement of the rotator cuff. Arthroscopy. 2000 Jan-Feb;16(1):35-40. PubMed PMID: 10627343. ](http://www.ncbi.nlm.nih.gov/pubmed/10627343)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/10627343)
21. [Tyler TF, Nicholas SJ, Lee SJ, Mullaney M, McHugh MP. Correction of posterior shoulder tightness is associated with symptom resolution in patients with internal impingement. Am J Sports Med. 2010 Jan;38(1):114-9. doi: 10.1177/0363546509346050. Epub 2009 Dec 4. ](http://www.ncbi.nlm.nih.gov/pubmed/19966099)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/19966099)
22. [Wright RW, Paletta GA Jr. Prevalence of the Bennett lesion of the shoulder in major league pitchers. Am J Sports Med. 2004 Jan-Feb;32(1):121-4. PubMed PMID: 14754734. ](http://www.ncbi.nlm.nih.gov/pubmed/14754734)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/14754734)
QUESTION 34 OF 50
A 65-year-old woman falls down a couple of stairs at home and has increasing pain in the left hip after prior revision surgery. She is unable to walk and is transferred in for definitive management of her left hip injury. An AP pelvis radiograph is shown in Figure
1
What is an appropriate next test to order?
2
Technetium bone scan
3
CT angiogram of the pelvis
4
Serum metal levels
5
Venous duplex Doppler
The Paprosky acetabular defect classification is a commonly accepted system that helps predict bone defects and guide operative treatment. The classification is reliable and based on the assessment of the AP pelvis radiograph. The classification relies on four individual assessments to determine the type of defect. (1) Superior migration of the center of rotation of the hip represents superior acetabular bone loss; (2) Ischial osteolysis represents bone loss in the posterior column and wall; (3) Teardrop osteolysis describes inferomedial bone loss from the anterior column, medial wall and superior ramus; (4) Position of the acetabular component in relation to Kohler’s line represents anterior column deficiency.
The classification is outlined here: Type I defect, a relatively normal acetabular with minimal deficits. Type II defect, broken into A,B,C with some acetabular defect noted, yet at least 50% direct host bone contact with a hemispherical component can be anticipated. Importantly the anterior and posterior columns remain intact and supportive. IIA has superior and medial bone loss, IIB has an uncontained or segmental defect, IIC has medial bone loss with an intact rim. Type III defect, represented by a severe segmental defect in the acetabular rim that is unable to support early fixation and biologic ingrowth routinely. IIIA defect, >40-60% host bone is in contact with the biologic fixation surface, noted as the “up and out” defect.
17
Typically, migration is >3 cm above the obturator line with moderate ischial lysis, partial destruction of the teardrop, and ilioischial and iliopubic lines intact. IIIB defect, <40% of the host bone will have intimate contact with the ingrowth surface of an acetabular component and is the up and in defect, often associated with a pelvic discontinuity. Extensive ischial osteolysis can be anticipated with destruction of the teardrop and migration of the component medial to the Kohler line. Superior migration will be >3 cm.
The AP pelvis in this case shows an up and in defect that is >3 cm migrated superiorly, making it a type IIIB defect. Due to the acute nature and degree of intrapelvic protrusion, a CT angiogram is warranted and vascular consultation or an intrapelvic approach to the revision may be necessary (Figure 2, angiogram example). The remainder of the options do not pertain to the findings in this particular case.
The classification is outlined here: Type I defect, a relatively normal acetabular with minimal deficits. Type II defect, broken into A,B,C with some acetabular defect noted, yet at least 50% direct host bone contact with a hemispherical component can be anticipated. Importantly the anterior and posterior columns remain intact and supportive. IIA has superior and medial bone loss, IIB has an uncontained or segmental defect, IIC has medial bone loss with an intact rim. Type III defect, represented by a severe segmental defect in the acetabular rim that is unable to support early fixation and biologic ingrowth routinely. IIIA defect, >40-60% host bone is in contact with the biologic fixation surface, noted as the “up and out” defect.
17
Typically, migration is >3 cm above the obturator line with moderate ischial lysis, partial destruction of the teardrop, and ilioischial and iliopubic lines intact. IIIB defect, <40% of the host bone will have intimate contact with the ingrowth surface of an acetabular component and is the up and in defect, often associated with a pelvic discontinuity. Extensive ischial osteolysis can be anticipated with destruction of the teardrop and migration of the component medial to the Kohler line. Superior migration will be >3 cm.
The AP pelvis in this case shows an up and in defect that is >3 cm migrated superiorly, making it a type IIIB defect. Due to the acute nature and degree of intrapelvic protrusion, a CT angiogram is warranted and vascular consultation or an intrapelvic approach to the revision may be necessary (Figure 2, angiogram example). The remainder of the options do not pertain to the findings in this particular case.
QUESTION 35 OF 50
An otherwise healthy 25-year-old man underwent a right anterior cruciate ligament reconstruction with a bone-patellar tendon-bone allograft. Routine preimplantation cultures of the allograft taken by the surgeon were positive for coagulase-negative Staphylococcus 5 days postoperatively. The patient has exhibited no evidence of clinical infection and his postoperative course has been uncomplicated during this time. What is the ideal management of this patient?


1
Observation
2
Oral antibiotics for 6 weeks
3
IV antibiotics for 6 weeks
4
Arthroscopic irrigation and debridement with graft retention
5
Arthroscopic irrigation and debridement with graft removal
DISCUSSION: The incidence of preimplantation positive cultures of musculoskeletal allografts used for anterior cruciate ligament reconstruction has varied between 4.8% and 13.3%. Interestingly, in none of the studies evaluating this issue did any of the patients implanted with a “contaminated” graft develop a clinical infection. The results of the current literature suggest that the treatment of low- virulence organisms is unnecessary if no evidence of clinical infection exists. Preimplantation cultures do not appear to correlate with clinical infection. Therefore, the routine culture of allograft tissue is not recommended.
REFERENCES: Diaz-de-Rada P, Barriga A, Barroso JL, et al: Positive culture in allograft ACL- reconstruction: What to do? Knee Surg Sports Traumatol Arthrosc 2003; 11:219-222.
Guelich DR, Lowe WR, Wilson B: The routine culture of allograft tissue in anterior cruciate ligament reconstruction. Am J Sports Med 2007;35:1495-1499.
Centeno JM, Woolf S, Reid JB III, et al: Do anterior cruciate ligament allograft culture results correlate with clinical infections? Arthroscopy 2007;23:1100-1103.
72 • American Academy of Orthopaedic Surgeons
Figure 87a Figure 87b
REFERENCES: Diaz-de-Rada P, Barriga A, Barroso JL, et al: Positive culture in allograft ACL- reconstruction: What to do? Knee Surg Sports Traumatol Arthrosc 2003; 11:219-222.
Guelich DR, Lowe WR, Wilson B: The routine culture of allograft tissue in anterior cruciate ligament reconstruction. Am J Sports Med 2007;35:1495-1499.
Centeno JM, Woolf S, Reid JB III, et al: Do anterior cruciate ligament allograft culture results correlate with clinical infections? Arthroscopy 2007;23:1100-1103.
72 • American Academy of Orthopaedic Surgeons
Figure 87a Figure 87b
QUESTION 36 OF 50
A 63-year-old woman is seen 10 weeks after sustaining a closed minimally displaced distal radius fracture. She has been in a short-arm cast and reports minimal pain but notes that she is having difficulty using her thumb. An extensor pollicis longus (EPL) tendon rupture is suspected. Which examination finding would confirm lack of EPL function?

1
Positive froment sign with the ulnar palm flat on a table
2
Weak thumb abduction with the dorsal palm flat on a table
3
Inability to flex the thumb with the palm flat on a table
4
Inability to extend the thumb with the palm flat on a table
As many as to 5% of patients with a nondisplaced distal radius fracture experience EPL rupture. The extensor pollicis brevis (EPB) tendon often attaches to the extensor hood and sometimes continues more distally, providing weak metacarpophalangeal extension even in the setting of EPL disruption. However, because of the vector of its pull, the EPB cannot extend the thumb dorsal to the plane of the palm. A positive Froment sign is noted when flexion of the thumb interphalangeal joint with an attempted key pinch is caused by adductor pollicis weakness from ulnar nerve dysfunction. Compression of the median nerve in the carpal tunnel affects the recurrent motor branch of the abductor pollicis brevis, leading to thenar atrophy. The flexor pollicis longus tendon (FPL) is intact so the patient would not have difficulty flexing the thumb with the palm flat.
**Question 42of 100** Figure 1 shows an injury sustained by a 60-year-old man 4 weeks ago. Since that time he has had substantial pain and catching of his finger during attempts at range of motion. What is the most appropriate treatment at this point?
---
1. Tendon debridement
2. Release of the A2 pulley
3. Tendon repair with core sutures
4. Tendon repair with epitendinous sutures
PREFERRED RESPONSE: D
EXPLANATION:
Approximately 70% laceration of the flexor digitorum profundus tendon with active locking is best treated with epitendinous sutures. Performing this procedure under local anesthetic allows for better assessment
of whether the triggering has been resolved. Cyclic loading has been shown to increase with high-grade partial lacerations. Use of core sutures adds little strength to a partial laceration. Debridement alone is reserved for injuries involving less than 60% of the tendon diameter. Release of the A2 wouldcompromise _pulley function._
**Question 42of 100** Figure 1 shows an injury sustained by a 60-year-old man 4 weeks ago. Since that time he has had substantial pain and catching of his finger during attempts at range of motion. What is the most appropriate treatment at this point?
---
1. Tendon debridement
2. Release of the A2 pulley
3. Tendon repair with core sutures
4. Tendon repair with epitendinous sutures
PREFERRED RESPONSE: D
EXPLANATION:
Approximately 70% laceration of the flexor digitorum profundus tendon with active locking is best treated with epitendinous sutures. Performing this procedure under local anesthetic allows for better assessment
of whether the triggering has been resolved. Cyclic loading has been shown to increase with high-grade partial lacerations. Use of core sutures adds little strength to a partial laceration. Debridement alone is reserved for injuries involving less than 60% of the tendon diameter. Release of the A2 wouldcompromise _pulley function._
QUESTION 37 OF 50
Figures 1 through 4 show the radiographs and MRI obtained from a 40-year-old man who has a 6-week history of ring finger pain, redness, and swelling after puncturing the finger with a toothpick. Purulent drainage from the puncture wound site grew _Eikenella corrodens_. The patient was initially treated with oral antibiotics for 10 days and then intravenous (IV) antibiotics for 3 weeks. What is the best next step in treatment?



1
Continued IV antibiotics for 4 weeks
2
Continued oral antibiotics for 6 weeks
3
Bone scan, biopsy, and metastatic work-up
4
Surgical débridement along with antibiotics
This patient has a septic distal interphalangeal joint, which was treated with antibiotics alone. As a result, the patient developed osteomyelitis with bone destruction and abscess. The best way to treat this problem is to perform surgical débridement of bone and soft tissue, along with abscess drainage and an appropriate antibiotic regimen. Antibiotic treatment without surgery would not be successful in eliminating this particular infection. Bone scan with biopsy is not the correct option, because this problem is an infection _and not a tumor, and MRI already has provided enough diagnostic information._
QUESTION 38 OF 50
A tailorâs bunion is an abnormal prominence of the lateral aspect of the 5th metatarsal head. Similar to hallux valgus deformities, tailorâs bunions can be due to a widened intermetatarsal angle between the 4th and 5th metatarsal shafts. The normal 4-5 intermetatarsal angle is:
1
Less than 8°-9°
2
Less than 12°
3
Less than 15°
4
Less than 20°
5
Less than 25°
4-5 intermetarsal angle in normal feet averages 6.2 degrees. Different authors believe an abnormally wide 4-5 intermetatarsal angle to be anything greater than 8°-9°.
QUESTION 39 OF 50
A 24-year-old man has a deep knife wound across the dorsal aspect of his wrist, transecting all of his wrist and finger extensor tendons. How does the surgeon determine which of the proximal tendon stumps in the fourth dorsal compartment is the extensor indicis proprius? ](http://www.orthobullets.com/anatomy/10040/extensor-indicis)Review Topic
1
The tendon runs in a separate compartment.
2
The tendon has a more circular cross section.
3
The tendon has the most distal muscle belly.
4
The tendon is the most radial and superficial.
5
The tendon has two separate slips.
No detailed explanation provided for this question.
QUESTION 40 OF 50
A 24-year-old male sustains the injury seen in Figure A after being thrown from a motorcycle at a high speed. Which of the following fixation methods has been shown to be the most stable fixation construct for this injury?

1
Posterior bridge plating and anterior ring external fixation
2
Percutaneous iliosacral screw and anterior ring external fixation
3
Percutaneous iliosacral screw and anterior ring internal fixation
4
Transiliac screw
5
Two percutaneous iliosacral screws
Figure A shows an APC III injury, which is a rotationally and vertically unstable injury, with damage to the anterior ring, pelvic floor, and posterior ligamentous stabilizing structures.
The referenced study by Sagi et al found that biomechanically, a percutaneous iliosacral screw and anterior ring internal fixation was the most stable construct. In addition, he found no biomechanical support for addition of a second iliosacral screw.
The referenced study by Sagi et al found that biomechanically, a percutaneous iliosacral screw and anterior ring internal fixation was the most stable construct. In addition, he found no biomechanical support for addition of a second iliosacral screw.
QUESTION 41 OF 50
During what phase of the throwing motion is the highest torque measured across the glenohumeral joint?
1
Wind-up
2
Cocking
3
Early acceleration
4
Late acceleration
5
Follow through
Electromyography is used to evaluate muscular firing patterns about the shoulder during the throwing sequence. The rotator cuff muscles and biceps are relatively inactive during the acceleration phase, whereas the pectoralis major, serratus anterior, latissimus dorsi, and subscapularis show highest activity. By contrast, deceleration is accomplished by the rotator cuff musculature and the larger trunk muscles acting in concert to slow down the arm. It is during this phase of follow through that the highest torque is measured secondary to eccentric muscle contraction.
REFERENCES: Jobe FW, Moynes DR, Tibone JE, Perry J: An EMG analysis of the shoulder in pitching: A second report. Am J Sports Med 1984;12:218-220.
Pappas AM, Zawacki RM, Sulliva TJ: Biomechanics of baseball pitching: A preliminary report. Am J Sports Med 1985;13:216-222.
Altcheck DW, Dines DM: Shoulder injuries in the throwing athlete. J Am Acad Orthop Surg 1995;3:159-165.
REFERENCES: Jobe FW, Moynes DR, Tibone JE, Perry J: An EMG analysis of the shoulder in pitching: A second report. Am J Sports Med 1984;12:218-220.
Pappas AM, Zawacki RM, Sulliva TJ: Biomechanics of baseball pitching: A preliminary report. Am J Sports Med 1985;13:216-222.
Altcheck DW, Dines DM: Shoulder injuries in the throwing athlete. J Am Acad Orthop Surg 1995;3:159-165.
QUESTION 42 OF 50
All of the following anomalies are present in patients with ulnar club hand except:
1
Phocomelia
2
Transverse arrest
3
Humeral aplasia
4
Humeral hypoplasia
5
Vertebral dysplasia
Vertebral anomalies are not common in patients with ulnar club hand.
QUESTION 43 OF 50
Of the following signs or findings, which one is most consistent with the diagnosis of cervical radiculopathy?
1
Spurling sign
2
Hoffman sign
3
Clonus
4
Inverted brachioradialis reflex
5
Babinski sign
The Spurling sign is elicited by extending the neck and having the patient rotate his or her head toward the side of the symptoms; reproduction of symptoms, including those of radicular pain,suggests cervical nerve root compression as a contributing factor. The remaining signs and clinical findings are seen with cervical myelopathy. The Hoffman sign is elicited by flicking the terminal phalanx of the third or fourth finger; a positive response is seen as reflex flexion of the terminal phalanx of the thumb. The inverted brachioradialis reflex is seen when the brachioradialis tendon is tapped and a diminished brachioradialis reflex is noted but reflex contraction of the finger flexors is seen.
QUESTION 44 OF 50
of 100
Clinical characteristics of patients who are ideal for a nonsurgical treatment trial (instead of surgery) include
Clinical characteristics of patients who are ideal for a nonsurgical treatment trial (instead of surgery) include
1
absence of neurologic deficits and MSSA infection.
2
normal blood pressure and normal heart rate.
3
negative blood cultures, cocaine abuse
4
normal blood pressure and normal heart rate
- absence of neurologic deficits and MSSA infection.
QUESTION 45 OF 50
According to clinical and biomechanical studies, the most appropriate position for a headless scaphoid compression screw for repair of a scaphoid waist fracture is
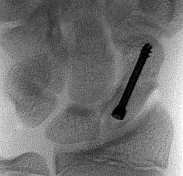
1
retrograde to protect the dorsal blood supply to the scaphoid.
2
retrograde eccentrically in the dorsal scaphoid to avoidtrapezium impingement.
3
deep and centrally placed, respecting the articular surface.
4
anterograde to protect the volar blood supply to the scaphoid.
The position of a scaphoid screw for scaphoid fracture repair (Figure 1) is as critical as the position of a sliding hip screw for intertrochanteric fracture repair. Positioning the screw deep in the center of the densest portion of cancellous bone is beneficial for both of these fracture types.Trumble and associates have shown time to union for scaphoid nonunions to be decreased for centrally placed scaphoid screws. McCallister and associates documented improved biomechanical stability for scaphoid waist fractures repaired with a centrally placed screw vs an eccentrically placed screw. Dodds and associates
---
demonstrated significantly improved biomechanical stability with centrally placed long screws vs centrally placed short screws. The screw may be placed retrograde or antegrade. Although the screw position may be relatively parallel to the radial inclination as the shape of the scaphoid body follows the contour of the radial styloid, screw position should be assessed relative to the scaphoid’s own architecture. Placing the screw in a retrograde fashion can force the treating surgeon to start the screw eccentrically in an attempt to avoid the interference of the trapezium lying over the distal pole of the scaphoid. This may result in noncentral screw placement.
---
demonstrated significantly improved biomechanical stability with centrally placed long screws vs centrally placed short screws. The screw may be placed retrograde or antegrade. Although the screw position may be relatively parallel to the radial inclination as the shape of the scaphoid body follows the contour of the radial styloid, screw position should be assessed relative to the scaphoid’s own architecture. Placing the screw in a retrograde fashion can force the treating surgeon to start the screw eccentrically in an attempt to avoid the interference of the trapezium lying over the distal pole of the scaphoid. This may result in noncentral screw placement.
QUESTION 46 OF 50
The normal porosity of cortical bone is:
1
5%
2
10%
3
20%
4
25%
5
30%
The normal porosity of cortical bone is 10% compared to trabecular bone, which is 50% to 90%. Cortical bone porosity occurs because of the Haversian and Volkman canals and, to a lesser extent, from the osteocyte lacunae and canaliculi.
Trabecular bone is arranged as a series of interconnecting small plates and rods. The porosity may vary between 50% to 90%. This porosity is secondary to the spaces between the trabecular pieces of bone rather than voids in the actual pieces of trabecular bone.
Trabecular bone is arranged as a series of interconnecting small plates and rods. The porosity may vary between 50% to 90%. This porosity is secondary to the spaces between the trabecular pieces of bone rather than voids in the actual pieces of trabecular bone.
QUESTION 47 OF 50
To which of the following long and unbranched molecules does link protein form a bond with G1 domain of aggrecan:
1
Chondroitin 4-sulfate
2
Chondroitin 6-sulfate
3
Keratan sulfate
4
Hyaluronate
5
Dermatan sulfate
Link protein binds to both the G1 domain of aggrecan and the hyaluronate chain forming the aggregan-hyaluronate-link protein complexes referred to as proteoglycan aggregates.
QUESTION 48 OF 50
of 100
Which nerve root contributes to both the sciatic and femoral nerves?
Which nerve root contributes to both the sciatic and femoral nerves?
1
L2
2
L3
3
L4
4
L5
The lumbosacral plexus is formed from the lumbar and sacral roots that are redistributed into the obturator, femoral, and sciatic nerves. The obturator nerve is composed of the L1, L2, and L3 roots. The femoral nerve has contributions from the L3 and L4 roots. The sciatic nerve contains the L4, L5, S1, and lower sacral roots. Therefore, only the L4 root contributes to the femoral and sciatic (via the lumbosacral trunk) nerves, which allows it to innervate the quadriceps and the anterior tibialis muscles.
RECOMMENDED READINGS
32
1. Netter FH. The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. Summit, NJ: Ciba-Geigy; 1991:77-82.
2. [Samudrala S Department Of Neurosurgery University Of Southern California Medical School Los Angeles California And Department Of Neurosurgery University Of Florida Medical School Gainesville Florida, Khoo LT, Rhim SC, Fessler RG. Complications during anterior surgery of the lumbar spine: an anatomically based study and review. Neurosurg Focus. 1999 Dec 15;7(6):e9. PubMed PMID: 16918208. ](http://www.ncbi.nlm.nih.gov/pubmed/16918208)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16918208)
RECOMMENDED READINGS
32
1. Netter FH. The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. Summit, NJ: Ciba-Geigy; 1991:77-82.
2. [Samudrala S Department Of Neurosurgery University Of Southern California Medical School Los Angeles California And Department Of Neurosurgery University Of Florida Medical School Gainesville Florida, Khoo LT, Rhim SC, Fessler RG. Complications during anterior surgery of the lumbar spine: an anatomically based study and review. Neurosurg Focus. 1999 Dec 15;7(6):e9. PubMed PMID: 16918208. ](http://www.ncbi.nlm.nih.gov/pubmed/16918208)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/16918208)
QUESTION 49 OF 50
-A 14-year-old boy has failed physical therapy management for Scheuermann kyphosis, and an extension thoracolumbosacral orthosis brace is recommended. The boy and his parents are told that the brace will force his thoracic spine into normal sagittal alignment and put the anterior vertebral bodies of the thoracic segment into tension, which will induce bone growth and normalization of wedge-shaped vertebrae. What name is associated with this process?
1
Hooke’s law
2
Kirchhoff’s law
3
Wolff’s law
4
Heuter-Volkmann principle
No detailed explanation provided for this question.
QUESTION 50 OF 50
Figure 39 is the radiograph of a 67-year-old woman with rheumatoid arthritis who reports an 8-month history of increasing pain, swelling, and deformity. Anti-inflammatory drugs, orthotics, and extra-depth shoes have failed to provide relief. What is the next most appropriate step in treatment?

1
First metatarsophalangeal joint arthrodesis and lesser metatarsal head resections
2
First metatarsophalangeal joint replacement and lesser metatarsal head resections
3
Keller arthroplasty and lesser metatarsal head resections
4
Distal Chevron osteotomy and lesser metatarsal head resection
5
Lapidus procedure and Weil osteotomies
The patient has a severe rheumatoid forefoot deformity involving all metatarsophalangeal joints. Coughlin and Mann have found that 90% of patients have excellent and good results with combined first metatarsophalangeal fusion and lesser metatarsal head resection. Keller Arthroplasty does not provide a stable platform for walking and is associated with recurrent deformity and pain. The first metatarsophalangeal joint replacement has not been shown to provide reliable long-term results.Osteotomies may be indicated in patients without erosive joint changes. The Lapidus procedure is an arthrodesis of the first tarsometatarsal joint, which would not address the patient’s arthritic first metatarsophalangeal joint.
---
---
