This mock exam provides 50 randomized questions derived from Arab Board and FRCS databanks to perfectly simulate testing environments.
Score: 0%
Advanced Orthopedic Mock Exam (Set 0B101D)
High-Yield Simulation: This randomly generated exam contains exactly 50 high-yield multiple-choice questions curated from the Arab Orthopaedic Board and FRCS databanks. Optimize your learning: Use "Exam Mode" for timed pressure, or switch to "Study Mode" for instant explanations.
QUESTION 1 OF 50
Which of the following is most commonly associated with the use of bisphosphonates in the setting of
metastatic breast cancer?
1
Reduction of skeletal-related events by 30% to 40%
2
Jaw osteonecrosis in 15% of patients
3
Pain improvement in 20% of patients
4
Acceleration of hypercalcemic symptoms and signs
5
Accelerated bone destruction
Bisphosphonate therapy in breast cancer patients is indicated for the correction of hypercalcemia and the prevention of cancer treatment-induced bone loss. Bisphosphonates reduce metastatic bone pain in at least 50% of patients and can reduce the frequency of skeletal-related events by 30% to 40%. Osteonecrosis of the jaw could occur in up to 2.5% of breast cancer patients during longterm bisphosphonate therapy.
QUESTION 2 OF 50
Slide 1
A patient presents for surgical correction of a ruptured Achilles tendon. He recalls injuring his ankle 1 year previously, but did not seek any medical treatment at that time. You plan to repair the tendon, and at surgery, a gap between the tendon ends is noted (Slide). The following procedure is not consistent with an acceptable outcome:
1
V-Y advancement
2
Flexor hallucis tendon transfer
3
End-to-end repair with the foot positioned in slight equinus
4
Flexor digitorum longus tendon transfer
5
Fascial turn down flap from musculotendinous junction
End-to-end repair of a chronic rupture of the Achilles tendon may not be considered if the gap is greater than 2 cm. Equinus positioning is never acceptable. Although each of the other alternatives above may be considered, each has its proponents and potential disadvantages.
QUESTION 3 OF 50
A 47-year-old man is seen in consultation in the ICU after being admitted and treated emergently for a dissecting aortic aneurysm. Current examination reveals generalized weakness of the lower extremities with a significant decrease in pain and temperature sensation from approximately the waist down.Proprioception is maintained. What is the most likely diagnosis at this time?
1
Anterior cord syndrome
2
Central cord syndrome
3
Brown-Sequard syndrome
4
Posterior cord syndrome
5
Spinal shock
Incomplete cord syndromes include anterior cord syndrome, Brown-Sequard syndrome,central cord syndrome, and posterior cord syndrome. The anterior cord syndrome involves a variable loss of motor function and pain and/or temperature sensation, with preservation of proprioception as seen in this patient. The Brown-Sequard syndrome involves an ipsilateral loss of proprioception and motor function, with contralateral loss of pain and temperature sensation. The posterior cord syndrome is a rare injury and is characterized by preservation of motor function, sense of pain and light touch, with loss of proprioception and temperature sensation below the level of the lesion. The central cord syndrome is characterized with greater motor weakness in the upper extremities than in the lower extremities. The pattern of motor weakness shows greater distal involvement in the affected extremity than proximal muscle weakness.
Spinal shock is the period of time, usually 24 hours, after a spinal injury characterized by absent reflexes, flaccidity, and loss of sensation below the level of the injury.
QUESTION 4 OF 50
A 27-year-old man presents to the emergency department with an ankle fracture. CT scans note anteromedial marginal impaction.
Which radiograph (Figures A-E) would best correlate with this finding?
1
Figure A
2
Figure B
3
Figure C
4
Figure D
5
Figure E
This patient has anteromedial marginal impaction seen on CT scans. This is characteristic of a supination-adduction ankle fracture (Figure D).
In the Lauge-Hansen classification, ankle fractures are classified into supination-adduction (SA), supination-external rotation, pronation-abduction, pronation-external rotation. Certain considerations exist when treating SA fractures with marginal impaction: (1) An anteromedial approach will aid in visualizing and reducing the impaction (instead of standard medial approach).
(2) Disimpaction of the articular fragment and possibly bone grafting of the resulting defect may be necessary rather than simple percutaneous fixation.
McConnell et al. reviewed marginal plafond impaction in supination adduction injuries. Supination-adduction injuries comprised 5% of 500 fractures (44 fractures), and 42% (8 fractures) of these had marginal impaction.
Illustration A is another example of a SA fracture depicting vertical fracture of the medial malleolus in association with marginal impaction of the plafond
(arrow). Illustration B is an axial CT showing increased density at the level of the subchondral bone, characteristic of anteromedial marginal impaction.
Illustration C is a coronal CT showing showing articular depression of the impacted segment and tibiotalar incongruity.
Incorrect Answers:
Answer 1: Figure A shows a pronation-abduction ankle fracture. Answer 2: Figure B shows a talar body fracture.
Answer 3: Figure C shows a pronation-external rotation ankle fracture Answer 5: Figure E shows a supination-external rotation ankle fracture. Marginal impaction is not characteristic of these injuries.
QUESTION 5 OF 50
Which of the following describes the inheritance pattern of Marfanâs syndrome:
1
Autosomal recessive
2
Autosomal dominant
3
X-linked recessive
4
X-linked dominant
5
Sporadic
Structural defects are usually transmitted by an autosomal-dominant pattern. In contrast, with metabolic or enzyme deficiencies, the condition is usually transmitted in an autosomal-recessive pattern.
Remember the major autosomal-dominant conditions: Achondroplasia
Spondyloepiphyseal dysplasia
Multiple epiphyseal dysplasia
Marfan's syndrome Ehlers-Danlos syndrome Osteogenesis imperfecta (I, IV) Multiple hereditary exostosis Polydactyly
QUESTION 6 OF 50
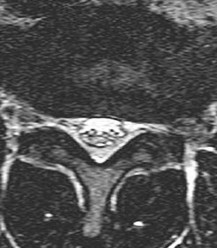
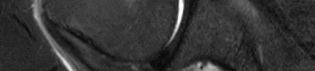
of 100 Figure 5 is a T2-weighted MR image of a 26-year-old man who has had left leg pain for 3 months that has failed nonsurgical treatment. Surgical decompression is planned. Which approach would provide the most direct ability to perform surgical decompression?
1
Posterior midline approach
2
Retroperitoneal approach
3
Far lateral approach
4
Transpsoas approach
The MR image shows a far lateral disk herniation impinging on the exiting nerve root lateral to the exiting foramen. This is reached most directly with a far lateral (Wiltse) approach. This is a posterior paramedian approach that uses the interval between the paraspinal muscles (multifidus and longissimus) and arrives onto the facet joints. The intertransverse membrane can then be released, exposing the far lateral disk herniation. A posterior midline approach will allow easy access to the spinal canal, which is medial to the disk herniation, and will not allow for easy disk removal without the need for a facetectomy, which would destabilize the level. An anterior approach would not allow for access to the far lateral disk herniation, nor would a traditional retroperitoneal or newer transpsoas approach.
RECOMMENDED READINGS
[Wiltse LL, Spencer CW. New uses and refinements of the paraspinal approach to the lumbar spine. Spine (Phila Pa 1976). 1988 Jun;13(6):696-706. PubMed PMID: 3175760. ](http://www.ncbi.nlm.nih.gov/pubmed/3175760)[View](http://www.ncbi.nlm.nih.gov/pubmed/3175760)[ ](http://www.ncbi.nlm.nih.gov/pubmed/3175760)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/3175760)
[Epstein NE. Evaluation of varied surgical approaches used in the management of 170 far-lateral lumbar disc herniations: indications and results. J Neurosurg. 1995 Oct;83(4):648-56. PubMed PMID: 7674015. ](http://www.ncbi.nlm.nih.gov/pubmed/7674015)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/7674015)
QUESTION 7 OF 50
What structure is considered the single most important soft-tissue restraint to anterior-posterior stability of the sternoclavicular joint?
1
Posterior capsular ligament
2
Anterior capsular ligament
3
Interclavicular ligament
4
Intra-articular disk
5
Subclavius tendon
In a cadaver ligament sectioning study, the posterior capsular ligament was considered the most important structure for anterior-posterior stability of the sternoclavicular joint. The anterior capsular ligament also helps prevent anterior displacement but not to the same degree as the posterior ligament. The interclavicular ligament provides little support for anteroposterior translation.
REFERENCES: Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Rockwood CA Jr, Matsen FA III, Jobe CM: Gross Anatomy of the Shoulder. Philadelphia, PA, WB Saunders, 1998.
QUESTION 8 OF 50
of 100
Figures 1 and 2 are the MRI scans of the spine of a 20-year-old college football player who complains of severe right arm pain after making a tackle. He has numbness of the right thumb and index finger but has 5/5 strength in both arms, and his neurological examination is otherwise unremarkable. You counsel the patient that he can return to play when/if
1
nonoperative care has a higher chance than surgery of allowing him to be able to return to play.
2
he is asymptomatic with normal range of motion and a negative neurological examination.
3
he is not likely to be able to return to football.
4
after surgical decompression.
■ The patient has sustained a herniated disk, which is likely causing his radicular symptoms. The patient does not have significant weakness or myelopathic symptoms, and initial treatment should be nonoperative. However, Hsu found that surgical treatment is shown to result in a better chance of returning to play in National Football League players. Regardless the treatment, the patient should not be allowed to return to play until he is asymptomatic with normal range of motion and a negative neurological examination.
QUESTION 9 OF 50
Secondary ossification of the elbow
1
Occurs over a two-year period
2
Occurs more rapidly in males
3
Proceeds in a predictable fashion through skeletal maturity
4
Is not important for the orthopedist to understand
5
Is complete by age 10
Secondary ossification is very imprtant in managing fractures. It begins at age 1-2 and is complete by 14 years girls and 16 years in boys.
QUESTION 10 OF 50
Iontophoresis has been effectively used in all of the following EXC EPT:
1
C arpal tunnel syndrome
2
Wrist arthritis
3
Shoulder/rotator cuff tendinitis
4
Lateral epicondylitis
5
Medial epicondylitis
Iontophoresis is effective in soft tissue conditions such as rotator cuff bursitis and lateral epicondylitis.
QUESTION 11 OF 50
of 100
What is the most likely diagnosis?
1
Desmoid tumor
2
High-grade pleomorphic sarcoma
3
Synovial sarcoma
4
Extraskeletal Ewing sarcoma
- Desmoid tumor_
QUESTION 12 OF 50
A 16-year-old female swimmer reports several episodes of atraumatic glenohumeral instability that occur with different arm positions. Examination reveals generalized ligamentous laxity and a positive sulcus sign, and her shoulder can be subluxated both anteriorly and posteriorly. Initial management should consist of
1
a strengthening program for the rotator cuff and scapular muscles.
2
arthroscopic thermal capsulorrhaphy.
3
an inferior capsular shift.
4
a glenoid osteotomy.
5
a Putti-Platt repair.
The patient has multidirectional instability (MDI). It has been reported that a high percentage of patients with MDI respond to a properly structured exercise program that is continued for at least 3 to 6 months. If nonsurgical management fails to provide relief, stabilization with an inferior capsular shift procedure has been effective in a high percentage of patients. Unidirectional repairs, such as the Putti-Platt procedure, are unsuitable for correcting MDI. Thermal capsulorrhaphy has been reported to have a very high failure rate
(greater than 50%) for treating MDI.
REFERENCES: Burkhead WZ Jr, Rockwood CA Jr: Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am 1992;74:890-896.
Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Pollock RG, Owens JM, Flatow EL, et al: Operative results of the inferior capsular shift procedure for multidirectional instability of the shoulder. J Bone Joint Surg Am
2000;82:919-928.
Miniaci A, Birnie J: Thermal capsular shrinkage for treatment of multidirectional instability of the shoulder. J Bone Joint Surg Am 2003;85:2283-2287.
QUESTION 13 OF 50
A 62-year-old man falls on his porch and sustains an elbow injury. A radiograph is provided in Figure A. Which of the following is the best treatment?
1
Closed reduction and long arm casting
2
Early motion with a hinged elbow brace
3
Open reduction internal fixation with a tension band construct
4
Open reduction internal fixation with a plate
5
Fragment excision and advancement of the triceps tendon
The radiograph shows an olecranon fracture with articular comminution and depression of a large intra-articular fragment. This pattern is best treated with plate fixation to support the articular reduction.
Bailey et al reviewed 25 cases of olecranon fractures (simple and comminuted fracture patterns) treated with plate fixation. All 25 went on to union. There were no major complications reported. Twenty percent of patients underwent hardware removal at a later date for prominence.
Hak et al review the treatment options available for olecranon fractures. Simple intra-articular fractures without comminution are suitable for tension band fixation. Comminution of the articular surface is an indication for plate fixation and may benefit from bone graft to support depressed articular segments. Osteoporotic patients or fractures with severe comminution may do better with fragment excision and advancement of the triceps.
QUESTION 14 OF 50
of 100 A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
1
Midsubstance tear of the lateral ulnar collateral ligament
2
Proximal avulsion of the ulnar collateral ligament
3
Proximal avulsion of the lateral ulnar collateral ligament
4
Distal bony avulsion of the ulnar collateral ligament from the sublime tubercle
DISCUSSION:
Classic posterior elbow dislocations result from a posterolateral rotatory mechanism, whereby the hand is fixed (typically on the ground) while the weight of the body creates a valgus and external rotation moment on the elbow. This results first in tearing of the lateral collateral ligament that proceeds medially through the anterior and posterior joint capsules, ending with potential involvement of the ulnar collateral ligament (but this is not universal). McKee and associates assessed the lateral soft-tissue injury pattern of elbow dislocations
with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding. Midsubstance
tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
QUESTION 15 OF 50
With the use of perineural catheters, improvement in all of the following outcomes can be anticipated except:
1
Lower pain scores
2
NarcotiCsparing effect
3
Reduced incidence of nausea and vomiting
4
Increased sleep disturbances
5
Shortened length of stay
Double blind placebo controlled randomized trials the use of perineural catheters led to improved pain scores, decreased narcotiCusage and narcotiCrelated side effects, and fewer sleep disturbances.
Length of stay was shortened by the use of perineural catheters as compared to epidural or IV PCA analgesia in several studies. In pilot studies, the use of perineural catheters in carefully selected patients allowed ambulatory total shoulder arthroplasty and single day admissions for total hip arthroplasty and total knee arthroplasty
QUESTION 16 OF 50
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow. The athlete undergoes repair of the injury, and postsurgical radiographs are shown in Figures 1 and
1
At his first postsurgical visit, he reports no pain but describes weakness in his hand and decreased sensation over his lateral forearm. Upon examination, he has decreased 2-point discrimination over the lateral forearm and an inability to actively extend his thumb and fingers at the metacarpophalangeal joints. He can extend at the finger interphalangeal joints. He can extend his wrist weakly, and it deviates radially as he extends. His distal sensation is intact. Considering his examination findings, which two nerves are injured?




2
PIN and radial nerve
3
PIN and lateral antebrachial cutaneous nerve (LABCN)
4
Median nerve and LABCN
5
Radial nerve and LABCN
This patient had an eccentric muscle contraction (muscle lengthening while contracting) of his biceps muscle while trying to stop a defender from getting around him. This in turn caused failure of the distal biceps tendon, as evidenced by pain in the antecubital fossa, lack of elbow supination strength, and his positive biceps active test finding (supination/pronation of the forearm showing no motion of the biceps muscle belly). Eccentric contractors have the highest potential for building strength but also are at highest risk for injury. Concentric (muscle shortening with contraction), isometric (no change in muscle length with contracture), and isokinetic (constant velocity of muscle contraction with a variable force) do not describe the mechanism detailed. The loss of distal biceps attachment will result in loss of elbow supination strength in flexion (the biceps is the only supinator to cross the
elbow) while still retaining elbow flexion (albeit weakened) because of the other elbow flexors (brachioradialis and brachialis). Consequently, treatment should be anatomic repair of the distal biceps insertion, which can be performed with a 2-incision or 1-incision technique. Although all of the listed complications have been reported with these techniques, LABC neuropraxia is by far the most common. Radiographs show that this athlete’s injury was repaired using a 1-incision technique with a cortical fixation device and a radial bone tunnel. This technique has gained favor because of its decreased incidence of heterotopic ossification and radioulnar synostosis compared with the 2-incision technique. The most troubling complication for most surgeons is the development of a posterior interosseous nerve (PIN) palsy, which this patient clearly demonstrates in addition to the more common LABCN upon postsurgical examination. Because the LABCN injury is typically a neuropraxia from retraction, a period of observation is indicated. PIN injury can result from excessive traction during surgical exposure or from entrapment by the fixation button. Considering the anatomy of the PIN, successful recovery of the nerve typically progresses based on the distance from the origin of the nerve to the muscle indicated. The extensor indicis proprius (EIP) muscle is the most distal muscle innervated and can be expected to recover last. First to return would be the EDC
followed by the ECU, EDQ, and, finally, the EIP.
---
QUESTION 17 OF 50
The disadvantages of a complete arthroscopiCrepair of a rotator cuff include all of the following except:
1
Complete arthroscopiCrepair limits some suture configuration options in the tendon.
2
Postoperative pain is increased.
3
Complete arthroscopiCrepair is technically difficult to perform.
4
Complex instrumentation is required.
5
Operative time is longer.
ArthroscopiCrepair techniques generally require the use of suture anchors and limit some suture configuration options in the tendon. Complete arthroscopiCrepair is technically difficult, requires significantly greater and more complex instrumentation, and has a potentially longer operative time. However, it decreases postoperative pain
QUESTION 18 OF 50
Which of the following can be an inhibitor of physiologiCcalcification in bone:
1
Type I collagen
2
Large proteoglycans
3
Matrix vesicles
4
Phosphoproteins
5
Bone sialoprotein
Large proteoglycans, pyrophosphate, adenosine triphosphate, and citrate all act as inhibitors of physiologiCcalcification of bone. Note the role of promoters and inhibitors:
Apatite nucleation and growth
Promoters
Type I collagen Bone sialoprotein Matrix vesicles Phosphoproteins Proteolipids Biglycan
Inhibitors
Large proteoglycans Pyrophosphate Adenosine triphosphate Citrate
Mineral proliferation
Regulators
Osteocalcin Phosphoproteins Proteoglycans
QUESTION 19 OF 50
A 42-year-old woman has a 3-week history of acute lower back pain with radiation into the left lower extremity. There is no history of trauma and no systemic symptoms are noted. Examination reveals a positive straight leg test at 25 degrees on the left side. Motor testing reveals mild weakness of the gluteus maximus and weakness of the gastrocnemius at 3/5. Sensory examination reveals decreased sensation along the lateral aspect of the foot. Knee reflex is intact; however, the ankle reflex is absent. MRI scans show a posterolateral disk herniation. The diagnosis at this time is consistent with a herniated nucleus pulposus at what level?
1
L1-2
2
L2-3
3
L3-4
4
L4-5
5
L5-S1
The patient’s history and examination findings are consistent with a lumbar disk herniation at the L5-S1 level. Weakness of the gastrocnemius and gluteus maximus are consistent with an S1 lumbar radiculopathy. Nerve root tension signs are also
consistent with a disk herniation at L5-S1, which typically affects the traversing S1 nerve root.
QUESTION 20 OF 50
Figure 1 Figure 2
A 43-year-old woman has had a 2-year history of ankle pain. Her ankle pain is associated with swelling, decreased activities, and limited range of motion. Upon examination, diffuse warmth and swelling of the ankle are noted. Radiographs and a clinical picture are presented. The most likely diagnosis is:
1
Rheumatoid arthritis
2
Gout
3
Septic arthritis
4
Synovial sarcoma
5
Pigmented villonodular synovitis (PVNS)
Although pigmented villonodular synovitis (PVNS), infection, or gout may cause inflammatory changes on both sides of the ankle joint, the most likely cause of this inflammatory arthropathy is rheumatoid arthritis. Note the cystic changes, the synovial hypertrophy, and the joint inflammation.
QUESTION 21 OF 50
Which of the following features is true of congenital scoliosis but not infantile idiopathic scoliosis:
1
Bracing has been shown to decrease progression.
2
The age of onset is before 3 years old.
3
The thoracic curve may be convex to either the left side or the right in either curve type.
4
The rib-vertebral angle difference predicts the risk of worsening.
5
Vertebrae are abnormally formed from birth.
In congenital scoliosis, the vertebrae are abnormally formed from birth. The vertebrae are normal at birth in infantile idiopathic scoliosis.
Age of onset is before age 3 in both types of scoliosis.
The thoracic curve may be convex to the left slide or the right side in either curve type. In infantile idiopathic scoliosis, it is most commonly convex to the left.
The rib-vertebral angle difference (angle between the apical vertebral endplate and the rib on the convexity minus the rib on the concavity) greater than 20° predicts an increased risk of worsening in infantile idiopathic scoliosis but not in congenital scoliosis.
Bracing has not been shown to affect infantile idiopathic scoliosis.
QUESTION 22 OF 50
-The ability of compressed cortical bone to resist greater applied force in the longitudinal plane than in the transverse plane is an illustration of what material property?
1
Yield strength
2
Elastic modulus
3
Viscoelasticity
4
Anisotropy
No detailed explanation provided for this question.
QUESTION 23 OF 50
Which of the following structures is the most important restraint to posterior subluxation of the glenohumeral joint when positioned in 90 degrees of flexion and internal rotation?
1
Subscapularis muscle and tendon
2
Supraspinatus muscle and tendon
3
Middle glenohumeral ligament
4
Inferior glenohumeral ligament
5
Coracohumeral ligament
The posterior band of the inferior glenohumeral ligament is the most important restraint to posterior subluxation of the glenohumeral ligament with the shoulder in 90 degrees of flexion and internal rotation. With the shoulder in external rotation, the subscapularis is an important stabilizer to posterior subluxation. When the shoulder is in neutral rotation, the coracohumeral ligament is the primary stabilizer. The middle glenohumeral ligament functions primarily to resist anterior translation of the shoulder in the midrange of abduction. The supraspinatus muscle and tendon have relatively little contribution to anterior and posterior translation of the glenohumeral joint.
REFERENCES: Blasier RB, Soslowsky LJ, Malicky DM, Palmer ML: Posterior glenohumeral subluxation: Active and passive stabilization in a biomechanical model. J Bone Joint Surg Am 1997;79:433-440.
Flatow EL, Warner JI: Instability of the shoulder: Complex problems and failed repairs: Part I. Relevant biomechanics, multidirectional instability, and severe glenoid loss. Instr Course Lect 1998;47:97-112.
QUESTION 24 OF 50
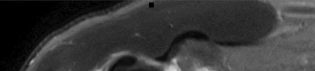
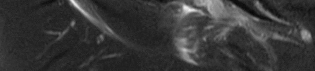
A 30-year-old firefighter sustained a longitudinal pulling injury to the arm while attempting to move a heavy object during a fire. Figure 45 shows an MRI scan of the elbow. Initial management should consist of**
1
rest and a sling followed by a gradual return to activities.
2
physical therapy and extension-block bracing.
3
repair of the biceps tendon to the brachialis muscle.
4
repair of the common flexor origin.
5
anatomic repair of the distal biceps tendon.
Because the MRI scan shows a complete rupture of the distal biceps tendon, the preferred treatment is anatomic repair of the tendon to the radial tuberosity either with the use of suture anchors or transosseous sutures through a two-incision technique. Several studies have documented superior results with anatomic repair of the distal biceps tendon when compared with results of nonsurgical management or repair of the tendon by attachment to the brachialis muscle. Patients undergoing anatomic repair of the distal biceps tendon through a two-incision technique typically regain a functional range of motion and nearly normal strength.
REFERENCES: D’Alessandro DF, Shields CL Jr, Tibone JE, Chandler RW: Repair of distal biceps tendon ruptures in athletes. Am J Sports Med 1993;21:114-119.
Boyd JB, Anderson LD: A method for reinsertion of the distal biceps brachii tendon. J Bone Joint Surg Am 1961;43:1041-1043.
Morrey BF, Askew LJ, An KN, Dobyns JH: Rupture of the distal tendon of the biceps brachii: A biomechanical study. J Bone Joint Surg Am 1985;67:418-421.
Failla JM, Amadio PC, Morrey BF, Beckenbaugh RD: Proximal radioulnar synostosis after repair of distal biceps brachii rupture by the two-incision technique: Report of four cases. Clin Orthop 1990;253:133-136.
QUESTION 25 OF 50
Schwannomas are differentiated from neurofibromas by all of the following except:
1
Ease of excision
2
Eccentric location on the nerve
3
Absence of fascicles
4
Presence of schwann cells
5
None of the above
Schwann cells contribute to schwannoma and neurofibroma.
QUESTION 26 OF 50
In the anterior cruciate ligament (ACL)-deficient knee, which of the following variables has the highest correlation with the development of arthritis?
1
Duration of time since the injury
2
Patient age
3
Additional ligament injury
4
Degree of laxity
5
Meniscal integrity
Ample evidence supports an increased rate of degenerative arthritis in the ACL-deficient knee. Several variables play a role in the development of the arthritis, but the integrity of the meniscus has been shown to be the single most important factor.
REFERENCES: O’Brien WR: Degenerative arthritis of the knee following anterior cruciate ligament injury: Role of the meniscus. Sports Med Arthroscopy Rev 1993;1:114-118.
Fetto JF, Marshall JL: The natural history and diagnosis of anterior cruciate ligament insufficiency. Clin Orthop 1980;147:29-38.
McDaniel WJ Jr, Dameron TB Jr: The untreated anterior cruciate ligament rupture. Clin Orthop 1983;172:158-163.
QUESTION 27 OF 50
of 100
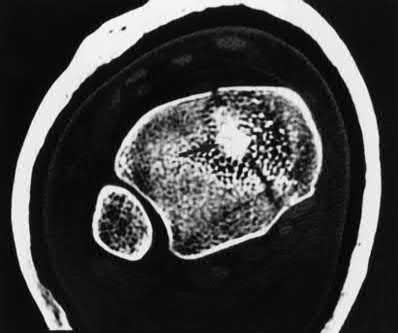
Chemotherapy for this condition is
1
contraindicated when pathology is benign.
2
associated with a high risk for subsequent myelodysplastic syndrome.
3
provides dramatic survival benefits.
4
provides modest survival benefits.
This patient has a dedifferentiated liposarcoma within a preexisting atypical lipomatous tumor. The imaging demonstrates a large fatty mass with increased internal septations proximally (the atypical lipomatous tumor) and a solid enhancing mass distally (the dedifferentiated portion). A biopsy reveals a high-grade liposarcoma. The other diagnostic responses do not reflect sarcomatous transformation of the lesion.
Surgical treatment of a high-grade sarcoma involves wide surgical resection. Radiation decreases local recurrence but does not clearly influence overall survival. The role of chemotherapy in high-grade soft-tissue sarcomas remains investigational; there is a modest (8%-15%) associated improvement in overall survival.
Intramuscular lipomas and atypical lipomatous tumors are treated with marginal resection alone. Radiation therapy for soft-tissue sarcomas may be given before or after surgery. When administered before surgery, patients have a higher wound complication rate but better long-term function attributable to lower rates of lymphedema, fibrosis, and contractures.
RECOMMENDED READINGS
1. [Schlieman M, Smith R, Kraybill WG. Adjuvant therapy for extremity sarcomas. Curr Treat Options Oncol. 2006 Nov;7(6):456-63. Review. PubMed PMID: 17032558.](http://www.ncbi.nlm.nih.gov/pubmed/17032558)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/17032558)
2. [Yang JC, Chang AE, Baker AR, Sindelar WF, Danforth DN, Topalian SL, DeLaney T, Glatstein E, Steinberg SM, Merino MJ, Rosenberg SA. Randomized prospective study of the benefit of adjuvant radiation therapy in the treatment of soft tissue sarcomas of the extremity. J Clin Oncol. 1998 Jan;16(1):197-203. PubMed PMID: 9440743.](http://www.ncbi.nlm.nih.gov/pubmed/9440743)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/9440743)
3. Soft tissue tumors. In: Damron TA, ed. _Orthopaedic Surgery Essentials: Oncology and Basic Science_. Philadelphia, PA: Lippincott Williams and Wilkins; 2008:87-92
QUESTION 28 OF 50
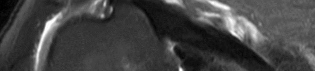
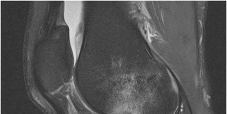
Figure 1 is the MRI scan of a 35-year-old female soccer player who injured her knee during a game. Given the findings of the scan, physical examination is most likely to reveal
1
grade 2 pivot shift.
2
positive Thessaly test.
3
positive quadriceps active test.
4
positive dial test at 30°.
---
---
DISCUSSION:
The MRI scan clearly reveals bone bruises in the mid lateral femoral condyle and posterior tibial plateau. These MRI findings are commonly associated with acute anterior cruciate ligament injuries. Therefore, the preferred answer would be a positive pivot shift examination. A positive posterior drawer and positive quad active test are associated with posterior cruciate ligament injuries. A positive dial test would be suggestive of a posterolateral instability of the knee.
QUESTION 29 OF 50
of 100
Contracture of which structure causes hammertoe deformity?
1
Extensor digitorum longus tendon
2
Extensor digitorum brevis tendon
3
Flexor digitorum longus tendon
4
Flexor digitorum brevis tendon
A patient with a flexible hammertoe deformity has the deformity while standing, but practically no deformity when seated with the foot in equinus. The metatarsophalangeal joint is not involved. The deformity is created by contracture of the flexor digitorum longus tendon.
RECOMMENDED READINGS
[Coughlin MJ. Lesser toe abnormalities. Instr Course Lect. 2003;52:421-44. Review. PubMed PMID: 12690869.](http://www.ncbi.nlm.nih.gov/pubmed/12690869)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/12690869)
Couglin MJ. Lesser toe deformities. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. Vol 1. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:363-464.
QUESTION 30 OF 50
A 56-year-old woman sustains a type IIIB open tibial shaft fracture. She undergoes irrigation and debridement and intramedullary nailing with flap coverage 24 hours later. Cultures are taken pre-debridement and post-debridement. She develops a surgical site infection at 6 weeks, which requires removing the hardware and placing
show
Commented [1]:
an external fixator. Deep cultures are most likely to pathogens found in
1
pre-debridement cultures.
2
post-debridement cultures.
3
neither debridement culture.
4
anaerobic specimens.
One study found only 8% of organisms grown on pre-debridement cultures eventually caused infection; 7% of cases with negative pre-debridement cultures became infected. Of cases that did become infected, pre-debridement cultures grew the infecting organism only 22% of the time. Post-debridement cultures were more accurate in predicting infection. However, of cases that became infected, the infecting organism was present on post-debridement cultures only 42% of the time. It is concluded that pre-debridement and post-debridement bacterial cultures from open fracture wounds are of essentially no value. It is recommended that they not be done.
In another study, before any interventions were performed, initial aerobic and anaerobic cultures of the wounds of 117 consecutive open extremity fractures grades I through III were obtained. The results of these cultures were correlated with the development of a wound infection. If an infection occurred, the organism grown from the infected wound was compared with any organism grown from the primary wound cultures. Of the initial cultures, 76% (89/117) did not demonstrate any growth, while the other 24% (28/117) only grew skin flora. There were only 7 (6%) wound infections, and 71% (5/7) initially did not grow any organisms. Of the isolates that grew from the initial cultures, none were the organisms that eventually led to
47
wound infections. The use of primary wound cultures in open extremity injuries has no value in the management of patients suffering from infections after long bone open extremity fractures.
QUESTION 31 OF 50
of 100 A 26-year-old mixed martial arts fighter sustains a posterolateral elbow dislocation. The primary stabilizers of the elbow joint are the
1
radiocapitellar joint, the posterior band of the medial collateral ligament, and the annular ligament.
2
ulnohumeral joint, the anterior band of the medial collateral ligament, and the lateral ulnar collateral ligament.
3
radiocapitellar joint, the anterior band of the medial collateral ligament, and the radial collateral ligament.
4
ulnohumeral joint, the anterior band of the medial collateral ligament, and the posterior band of the medial collateral ligament.
DISCUSSION:
The primary stabilizers of the elbow are the ulnohumeral joint, the lateral collateral ligament (lateral epicondyle to the crista supinatoris), and the anterior band of the medial collateral ligament (anterior inferior medial epicondyle to the sublime tubercle). Secondary stabilizers are the radial head, the common flexor and
extensor origins, and the joint capsule. The muscles that cross the elbow joint act as dynamic stabilizers.
QUESTION 32 OF 50
Which statement regarding the peroneal tendon(s) is incorrect:
1
The peroneus longus tendon attaches to the first metatarsal.
2
The peroneus brevis tendon is a plantarflexor of the ankle.
3
The peroneus brevis tendon has muscle attached to the tendon at a level lower than the peroneus longus tendon.
4
The peroneus longus tendon lies anterior to the peroneus brevis tendon at the level of the distal fibula.
5
There are two separate retinacular sheaths for the peroneal tendons distal to the tip of the fibula.
The peroneus brevis tendon plantarflexes and everts the foot and ankle. The peroneus longus tendon plantarflexes the foot, is a mild evertor of the foot, and plantarflexes the first metatarsal. The peroneus brevis tendon is prone to tears or splits at the level of the distal fibula and lies anterior to the peroneus longus tendon at this level.
QUESTION 33 OF 50
Which of the following promotes physiologiCcalcification at the level of apatite nucleation and growth:
1
Matrix vesicles
2
Large proteoglycans
3
Pyrophosphates
4
Adenosine triphosphate
5
Citrate
Matrix vesicles are important in the initiation of mineralization of collagen. They promote apatite nucleation and growth of the crystals. Large proteoglycans, pyrophosphates, adenosine triphosphate, and citrate are all inhibitors.
Note the role of promoters and inhibitors: Apatite nucleation and growth Promoters
Type I collagen Bone sialoprotein Matrix vesicles Phosphoproteins Proteolipids Biglycan
Inhibitors
Large proteoglycans Pyrophosphate Adenosine triphosphate Citrate
Mineral proliferation
Regulators
Osteocalcin Phosphoproteins Proteoglycans
QUESTION 34 OF 50
Figures 1 through 3 are the radiographs of a 65-year-old man with long-standing shoulder pain who has had acute worsening shoulder pain over the past three months following a fall. He is unable to raise his arm in forward elevation >90° and has failed nonsurgical treatments including physical therapy. What is the most predictable way to reverse pseudoparalysis?
64
1
Reverse shoulder arthroplasty (RSA)
2
Superior capsular reconstruction
3
Rotator cuff repair
4
Lower trapezius muscle transfer
The radiographs reveal a high-riding humeral head with an acromiohumeral interval of 1 mm. This indicates a chronic long-standing rotator cuff tear. There is further evidence of arthritic change with grade 4 Hamada findings. The only surgery with predictable outcomes for massive tear, high-riding humeral head and severe arthritis is RSA. 65
QUESTION 35 OF 50
An 18-year-old female Marine Corps recruit enters basic training. Her enlistment history and physical examination showed that she was an elite high school cross country runner. What is her most significant risk factor for a femoral or pelvic stress fracture during basic training?
1
Running mileage during the 2 months prior to basic training
2
Self-rated fitness
3
Running frequency during the 2 months prior to basic training
4
No menstrual bleeding during the year prior to basic training
5
Race/ethnicity
DISCUSSION: Approximately 5% of female recruits incur a stress fracture during the 13 weeks of Marine Corps basic training. Approximately 40% of these were femoral or pelvic stress fractures that were more severe than in civilian athletes or male military recruits. Only women who reported no menses during the previous year had a greater likelihood of femoral or pelvic stress fractures than did women who reported 10 to
12 menses. The referenced study did not find a statistically significant increase in risk of stress fracture in those recruits who had lesser menstrual irregularities in the year prior to recruit training, but there was a trend toward increased risk of stress fracture.
REFERENCES: Shaffer RA, Rauh MJ, Brodine SK, et al: Predictors of stress fracture susceptibility in young female recruits. Am J Sports Med 2006;34:108-115.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of
Orthopaedic Surgeons, 2004, pp 273-283.
QUESTION 36 OF 50
Figures below demonstrate the radiographs obtained from a 35-year-old woman with end-stage
debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. A further work-up reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MRI with MARS. Revision THA is recommended. The most common complication following revision of a failed metal-on- metal hip arthroplasty is
1
infection.
2
instability.
3
loosening.
4
periprosthetic fracture.
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on- metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child- bearing age. The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cellcounts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
QUESTION 37 OF 50
Risk factors for peroneal nerve palsy after total knee replacement (TKR) include all of the following except:
1
Severe valgus deformity
2
Flexion contracture
3
Epidural anethesia
4
Previous lumbar laminectomy and valgus osteotomy
5
Increased flexion gap
Severe valgus deformity, flexion contracture, and epidural anesthesia are risk factors associated with peroneal nerve palsy following TKR. Previous lumbar laminectomy and previous valgus osteotomy of the tibia also increase a patientâs chance of peroneal nerve palsy
QUESTION 38 OF 50
An 11-year-old boy stepped on a nail and sustained a puncture to the right forefoot 6 days ago. He was wearing tennis shoes at the time of injury. Treatment in the emergency department consisted of local debridement and tetanus prophylaxis; a radiograph was negative for foreign body, chondral defect, or fracture. He was discharged with a 3-day prescription of amoxicillin and clavulanate. The patient now has increasing pain and tenderness at the puncture site. What is the best course of action?
1
Change the antibiotic to ciprofloxacin
2
Initiate gentamicin
3
Resume the prescription for amoxicillin and clavulanate
4
Observation and follow-up in 48 hours
5
Surgical debridement
The initial treatment consisting of oral antibiotics was appropriate but with progressive symptoms, surgical debridement is necessary. Ciprofloxacin is contraindicated in children, and at this stage, oral antibiotics are inadequate. Intravenous antibiotics may be necessary, but surgical debridement is paramount. Failure to respond to the initial management precludes further observation.
REFERENCES: Riegler HP, Routson T: Complications of deep puncture wounds of the foot.
J Trauma 1979;19:18-22.
Green NE: Musculoskeletal infections in children: Part IV. Pseudomonas infections of the foot following puncture wounds. Instr Course Lect 1983;32:43-46.
QUESTION 39 OF 50
-is the radiograph of a 52-year-old right-hand dominant man who fell while skiing. He was initially treated at a mountainside clinic where he was placed in a sling. He now reports moderate shoulder pain but has no other complaints. What is the most appropriate management?
1
Hemiarthroplasty
2
Total shoulder arthroplasty
3
Open reduction and internal fixation
4
Sling for 6 to 8 weeks followed by mobilization
5
Sling followed by early mobilization within 2 to 3 weeks
No detailed explanation provided for this question.
QUESTION 40 OF 50
of 100
Which principle of fracture fixation should be considered when performing plate fixation of both shaft fractures for this patient?
1
Compression plating on the compression side of the bone
2
Compression plating on the tension side of the bone
3
Bridge plating
4
Insertion of 4.5-mm rather than 3.5-mm screws
This patient sustained comminuted fractures of the radius and ulna. The radial and ulnar artery pulses are palpable at the wrist, and perfusion to the hand is adequate. Consequently, angiography may not provide useful information. The most appropriate next step is to measure forearm compartment pressures.
A forearm compartment pressure measurement higher than 30 mm Hg, or within 20 mm Hg of the diastolic blood pressure, is concerning for compartment syndrome. There are 4 muscle compartments in the forearm: deep volar, superficial volar, mobile wad, and dorsal. Release of the volar compartments should include the carpal tunnel and may effectively decrease pressures in the dorsal and mobile wad compartments.
Compression plating of diaphyseal radius and ulna fractures is appropriate for management of simple fracture patterns. Compression permits the creation of a near-zero strain environment conducive to primary bone healing. Compression plates are conceptually most effective when placed on the tension side of bone. To minimize strain, there should be at least 6 cortices of screw purchase proximal and distal to the fracture. In most cases, 3.5-mm plate and screws are preferred. Larger, 4.5-mm implants may be more likely to propagate fracture lines in the event of device removal.
Severely comminuted shaft fractures are currently treated with the intention to optimize rather than minimize strain by use of a load-sharing implant. A 2% to 10% strain environment is conducive to callus formation and can be created with bridge plating; insertion of fewer screws that are more widely spaced, and use of either a flexible implant material (eg, titanium) or locked plate. A locked intramedullary nail device can also be used to create a controlled-strain environment; however, angulation and rotation of the fracture can be more difficult to control. Temporary external fixation is considered in the event of severe soft-tissue loss and/or fracture contamination.
RECOMMENDED READINGS
21. Schulte LM, Meals CG, Neviaser RJ. Management of adult diaphyseal both-bone forearm fractures. J Am Acad Orthop Surg. 2014 Jul;22(7):437-46. doi: 10.5435/JAAOS-22-07-437. Review. PubMed PMID: 24966250.
22. Prasarn ML, Ouellette EA. Acute compartment syndrome of the upper extremity. J Am Acad Orthop Surg. 2011 Jan;19(1):49-58. Erratum in: J Am Acad Orthop Surg. 2011 May;19(5):50A. PubMed PMID: 21205767.
23. Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology. J Bone Joint Surg Br. 2002 Nov;84(8):1093-110. Review. PubMed PMID: 12463652.
QUESTION 41 OF 50
If an orthopaedic surgeon receives royalties from a company for his or her participation in the design and development of a product, and uses that same product for the care of his or her patients, what is the orthopaedic surgeon's obligation?
1
Obligated to disclose only the fact that he or she was involved in the design and development
2
Obligated to disclose only the company relationship if there is a state law requiring it
3
Obligated to disclose his or her full relationship with the company, including the fact that he or she receives royalties
4
No obligation to disclose this private matter to the patient
5
Avoid this situation because it should not exist since he or she cannot use such a product
#
**
The AAOS has a specific code of ethics and professionalism that addresses this issue: "When an orthopaedic surgeon receives anything of value, including royalties, from a manufacturer, the orthopaedic surgeon must disclose this fact to the patient." It is derived from a broader document developed by the American Medical Association, and is applicable to all physicians. At present, this is an ethical issue receiving greater federal scrutiny. This issue has had a greater effect on the public's perception of the integrity of the orthopaedic profession.
QUESTION 42 OF 50
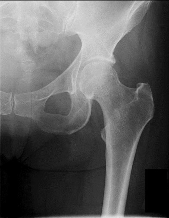
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. Further workup confirms an anterosuperior tear of the acetabular labrum and prominence of the acetabulum. What is the most likely location of a chondral injury associated with these findings? ---
1
Posterosuperior acetabulum
2
Posteroinferior acetabulum
3
Femoral head above the fovea
4
Femoral head below the fovea
This clinical scenario describes a patient with FAI attributable to pincer (acetabular) deformity. This form of FAI, which involves prominence of the anterosuperior acetabular lip, may be more common among women. Decreased range of motion and pain occur secondary to the abutment of the femoral head against the acetabular labrum and rim. Hip flexion, combined with adduction and internal rotation, recreates this contact and causes pain, but CAM or pincer etiology remains unknown. The differential diagnosis of hip pain in a young athlete includes femoral neck stress reaction/fracture, sacroiliac arthritis, intra-articular loose body, trochanteric bursitis, osteitis pubis, and hernia. No information presented in this scenario suggests any of these causes. Diagnosis of FAI is best performed via MR imaging, with an arthrogram increasing the sensitivity and specificity for labral pathology. Ultrasonography may be useful in the diagnosis of dysplasia or for dynamic assessment of a snapping hip, but ultrasonography is not commonly used to diagnose labral pathology. Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result in a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has _important functions for hip stability and maintenance of the suction seal of the joint._
QUESTION 43 OF 50
Which of the following elbow injuries as found in Figures A-E best characterizes the radiographic "double-arc" sign?
1
Figure A
2
Figure B
3
Figure C
4
Figure D
5
Figure E
Figure C and Illustration A (below) demonstrate the radiographic "double-arc" finding.
McKee et al described a unique "shear fracture of the distal articular surface of the humerus" which involved coronal fractures of the capitellum and a portion of the trochlea. He described the characteristic radiographic finding as the "double-arc sign" which represents the subchondral bone of the displaced capitellum and lateral trochlea ridge.
Incorrect Answers:
Figure A shows a radial head fracture. Figure B shows an elbow dislocation.
Figure D shows a pediatric lateral condyle fracture.
Figure E shows a pediatric medial epicondyle apophyseal avulsion fracture.
QUESTION 44 OF 50
Internal impingement is characterized by which of the following anatomic lesions?
1
Subscapularis tear
2
Bursal-sided rotator cuff tear
3
Articular-sided rotator cuff tear
4
Tight anterior capsule
5
Laxity of the posterior capsule
DISCUSSION: Internal impingement is characterized by articular-sided partial-thickness rotator cuff tears and superior glenoid labral tears. The capsule is characterized by laxity anteriorly and tightness posteriorly.
Scientific References
: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, p 82.
Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I:
Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Figure 27
QUESTION 45 OF 50
Which of the following areas results in latitudinal physeal enlargement:
1
Proliferative zone
2
Provisional calcification zone
3
Reserve zone
4
HypertrophiCzone
5
Perichondrial ring of La Croix
The perichondrial ring of La Croix is the source of cells which differentiate into chondrocytes and results in latitudinal physeal enlargement.
The other answers refer to specifiCgrowth plate zones which have functions. The reserve zone is for matrix production and storage. The proliferative zone is for matrix production and cellular proliferation. The hypertrophiCzone contains the zone of maturation, degeneration, and provisional calcification.
QUESTION 46 OF 50
of 100
A 69-year-old patient with diabetes has had acute-onset back pain and difficulty with ambulation for several hours. Evaluation reveals a temperature of 38.3°C, a white blood cell (WBC) count of 14000/µL (reference range [rr], 4500-11000/µL), C-reactive protein (CRP) level of 120 mg/L (rr, 0.08-3.1 mg/L), erythrocyte sedimentation rate of 130 mm/h (rr, 0-20 mm/h), normal rectal examination findings, and normal sensation to light touch. Motor function testing of the lower extremities reveals 3/5 ankle dorsiflexion and 4/5 plantar flexion strength bilaterally. An MR image reveals a large epidural abscess from L1-5. What is the most appropriate treatment at this time?
1
Medical management with intravenous (IV) antibiotics and observation
2
CT-guided aspiration of the abscess before initiating antibiotics
3
Surgical decompression and IV antibiotics
4
Blood cultures and re-evaluation in 24 hours
Epidural abscess is a serious and potentially disastrous condition. Although medical management is effective in some situations, surgical decompression is considered urgent with the presence of a neurological deficit. Medical management can be considered in the case of a neurologically intact patient, particularly when the microorganism has been identified. If medical management is chosen, careful observation and serial examination for neurologic deterioration is required. Surgical decompression is indicated if a patient's neurologic status worsens or if medical management failure is noted. Additionally, diabetes, a CRP level higher than 115 mg/L, WBC higher than 12500/µL , and bacteremia have proven predictive of medical treatment failure. This patient would be a better candidate for urgent surgical decompression and subsequent IV antibiotics than for medical management.
RECOMMENDED READINGS
[Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[View ](http://www.ncbi.nlm.nih.gov/pubmed/24231778)[Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24231778)
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
[24373683/. ](http://www.ncbi.nlm.nih.gov/pubmed/24373683)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/24373683)
CLINICAL SITUATION FOR QUESTIONS 96 AND 97
Figures 96a and 96b are the CT scans of a 32-year-old man who was thrown from his motorcycle. He has humeral shaft and femoral shaft fractures. A secondary survey reveals substantial tenderness to his lower thoracic spine. He is awake and alert and his movement is limited by pain secondary to the extremity fractures. He is otherwise neurologically intact.
A B
QUESTION 47 OF 50
A 25-year-old football player sustained an injury to his ankle 2 months ago. He has ankle pain upon dorsiflexion and external rotation. A radiograph demonstrates widening of the tibiofibular syndesmosis and a 3-mm space between the medial talus and the medial malleolus. The recommended treatment is:
1
Open reduction and internal fixation of a high fibula fracture
2
Reconstruction with peroneus brevis followed by aggressive rehabilitation of the ankle
3
Repair of the high ankle sprain with syndesmosis screw
4
Arthrodesis of the tibiofibular syndesmosis
5
Ankle arthroscopy, synovectomy, and repair of the deltoid ligament
It is imperative that any diastasis of the tibiofibular joint is repaired to prevent the late sequelae (e.g., arthritis), particularly in the athlete. Arthroscopy is not sufficient, other than evaluation for additional joint pathology, and syndesmosis arthrodesis would
rarely be indicated for this condition. There is no evidence of a high fibula fracture, although this must be a concern and should always be considered.
QUESTION 48 OF 50
When elevating the arm, the ratio of scapulothoracic to glenohumeral motion over the total range of motion is best described as
1
1:2, and in the first 30 degrees the ratio is 1:5.
2
1:2, and in the first 30 degrees the ratio is variable.
3
2:1, and in the first 30 degrees the ratio is variable.
4
2:1, and in the first 30 degrees the ratio is 3:1.
5
highly variable and no definitive statement can be made about the ratios.
The ratio of scapulothoracic to glenohumeral motion with elevation has been shown to vary depending on what portion of elevation is examined, how much load is on the arm, and the technique used to measure increments of elevation. However, almost every study shows that the ratio of scapulothoracic to glenohumeral motion is 1:2 for the contributions over a full range of elevation to 170 degrees. In the first 30 degrees of elevation, there is significant variability in the ratio, and there may be significant variability up to around 60 degrees.
REFERENCES: Inman VT, Saunders JR, Abbott LC: Observations of the function of the shoulder joint. Clin Orthop 1996;330:3-12.
Freedman L, Munro RH: Abduction of the arm in the scapular plane: Scapular and glenohumeral movements. J Bone Joint Surg Am 1966;18:1503.
QUESTION 49 OF 50
of 100
A 30-month-old boy underwent open reduction of his right hip to address developmental hip dysplasia. The reduction was performed through an anterior approach, and a shortening femoral osteotomy was not performed. Four months after surgery, hip radiographs reveal absence of ossification of the femoral epiphysis and fragmentation of the ossific nucleus. What is the likely cause of this complication?
1
Intraoperative damage to the medial femoral circumflex artery
2
Intraoperative damage to the lateral femoral circumflex artery
3
Excessive pressure on the femoral head after reduction
4
Incarceration of the acetabular labrum in the reduction
The incidence of pediatric hip dysplasia is approximately 1 per 100 live births, with hip dislocation present in 1 in 1000 births. Two surgical approaches primarily are used for surgical reduction in the dislocated pediatric hip: the modified medial approach as described by Weinstein and the
anterior Smith-Peterson approach. The Weinstein modification of the Ludloff approach exploits the interval between the pectineus muscle and the femoral neurovascular bundles rather than the interval between the pectineus and the adductor longus and brevis. The modified “bikini” anterior Smith-Peterson approach passes between the sartorius and tensor fascia lata superficially and between the rectus and gluteus medius during deep dissection.
When using the medial approach, the neurovascular bundle is particularly at risk, including the medial circumflex femoral vessels that supply blood to the femoral head ossific nucleus. Damage to this structure increases risk for osteonecrosis of the femoral head. Unlike the anterior approach, the medial approach does not allow for the performance of a capsulorrhaphy, poses higher risk for postprocedure redislocation, and is less useful in children of walking age. Identification of the ligamentum teres during deep dissection assists in localization of the true bony acetabulum.
The anatomic structure primarily at risk during the anterior approach is the lateral femoral cutaneous nerve. Excessive traction or transection of this structure will result in numbness in the proximal lateral thigh. This surgical approach allows for identifying and addressing all potential impediments to reduction: the redundant capsule, hypertrophic labrum, hypertrophic ligamentum teres, pulvinar, iliopsoas tendon, and transverse acetabular ligament. In older children who undergo open reduction with periacetabular osteotomy without a concomitant proximal femoral shortening osteotomy, reduction may be accompanied by increased pressure on the femoral head which, in turn, may result in secondary osteonecrosis of the femoral head.
RECOMMENDED READINGS
1. Karol LA. Developmental dysplasia of the hip. In: Song KM, ed. _Orthopaedic Knowledge Update: Pediatrics 4_. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2011:159-167.
2. [Vitale MG, Skaggs DL. Developmental dysplasia of the hip from six months to four years of age. J Am Acad Orthop Surg. 2001 Nov-Dec;9(6):401-11. Review. PubMed PMID: 11730331. ](http://www.ncbi.nlm.nih.gov/pubmed/11730331)[View Abstract at](http://www.ncbi.nlm.nih.gov/pubmed/11730331)[ ](http://www.ncbi.nlm.nih.gov/pubmed/11730331)[PubMed](http://www.ncbi.nlm.nih.gov/pubmed/11730331)
3. Weinstein SL, Ponseti IV. Congenital dislocation of the hip. J Bone Joint Surg Am. 1979 Jan;61(1):119-
[24/. PubMed PMID: 759421. ](http://www.ncbi.nlm.nih.gov/pubmed/759421)[View Abstract at PubMed](http://www.ncbi.nlm.nih.gov/pubmed/759421)
4. Olszewski DC, Karol LA. The medial Ludloff open reduction in developmental dysplasia of the hip before the age of walking. Operative Techniques in Orthopaedics. 2013;23:109-114.
QUESTION 50 OF 50
A 47-year-old woman has a painful bunion of the right foot, and shoe wear modifications have failed to provide relief. Examination reveals a severe hallux valgus with dorsal subluxation of the second toe. Radiographs are shown in Figures 14a and 14b. The most appropriate management should include
1
hallux metatarsophalangeal arthrodesis.
2
custom orthotics.
3
Chevron osteotomy with second toe correction.
4
Keller resection arthroplasty with second toe correction.
5
proximal metatarsal osteotomy with second toe correction.
The radiographs do not show significant arthrosis of the hallux metatarsophalangeal joint; therefore, arthrodesis is unnecessary. Orthotics will not correct the deformity. A distally based osteotomy will not achieve sufficient correction of the incongruity of deformity, and a Keller resection is not indicated in the younger population. The treatment of choice is a proximal metatarsal osteotomy with second toe correction.
REFERENCE: Mann RA, Rudicel S, Graves SC: Repair of hallux valgus with a distal soft-tissue procedure and proximal metatarsal osteotomy: A long-term follow-up. J Bone Joint Surg Am 1992;74:124-129.