Masterclass in Pediatric Radial Head and Neck Fractures: Operative Orthopaedics

Key Takeaway
Pediatric radial neck fractures primarily affect children aged 4 to 14 years, typically occurring through the metaphysis or physis (Salter-Harris types I, II, or IV). Management depends on the degree of angulation. While angulation under 30 to 45 degrees is often managed non-operatively, severe displacement requires closed reduction, percutaneous leverage, intramedullary pinning (Metaizeau technique), or open reduction to restore radiocapitellar alignment and preserve forearm rotation.
ELBOW JOINT FRACTURES AND DISLOCATIONS: RADIAL HEAD AND NECK FRACTURES
Pediatric radial neck fractures represent a unique biomechanical and anatomical challenge in orthopedic traumatology. Unlike adults, in whom radial head fractures predominate, children predominantly sustain fractures of the radial neck. These injuries typically occur in children aged 4 to 14 years. This demographic distribution is primarily due to the ossification timeline of the proximal radius; ossification of the radial head usually does not commence before 5 years of age, making the cartilaginous head highly resilient to trauma, while the metaphyseal neck remains the structural weak point.
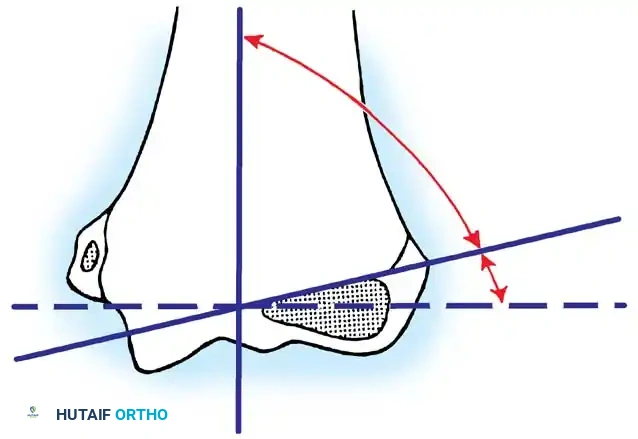
Clinical Pearl: The normal anatomical angulation of the radial neck in children (which can tilt up to 15 degrees laterally) is frequently and erroneously diagnosed as a buckle fracture by inexperienced clinicians. Always compare with contralateral radiographs if the diagnosis is equivocal.
When fractures of the epiphysis of the radial head do occur in children, they are usually Salter-Harris type IV fractures. However, the vast majority of pediatric radial neck fractures occur through the metaphysis. They can also propagate through the physis, producing a metaphyseal spike of bone characteristic of a Salter-Harris type II epiphyseal injury.
Classifications of Radial Neck Fractures
Historically, numerous classifications have been proposed, including those by Vostal, Newman, O’Brien, and Jeffery. In contemporary practice, the Wilkins Classification—which elegantly combines the morphological descriptions of Jeffery and Newman—is the gold standard for guiding surgical decision-making.
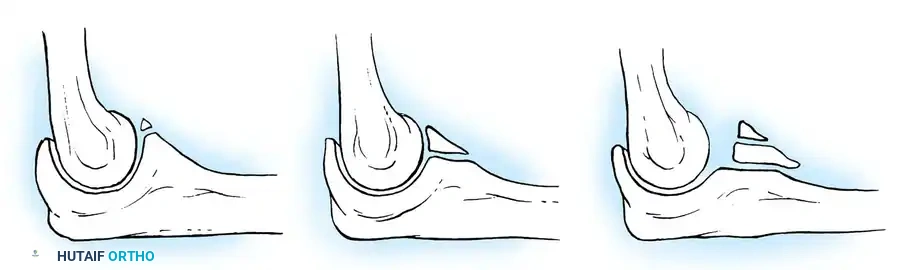
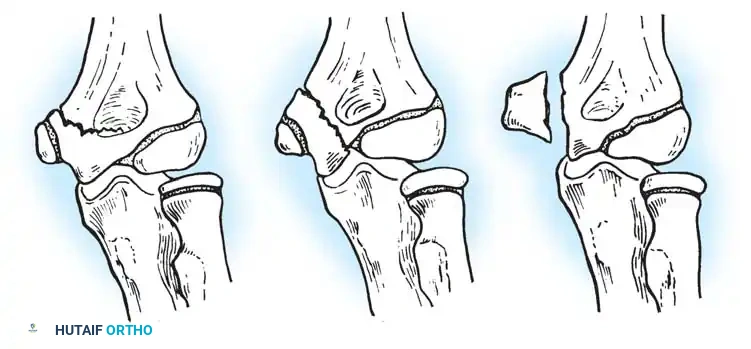
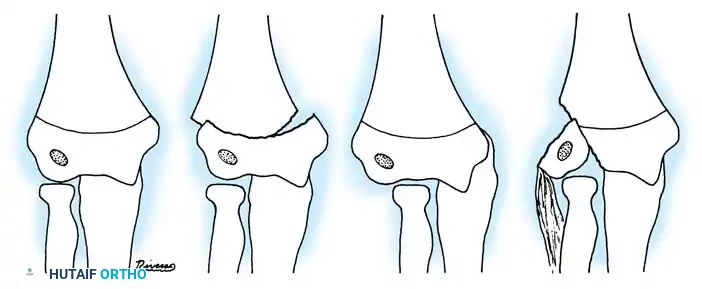
Fig. 33-38 Wilkins classification of radial neck fractures. A, Salter-Harris type II fracture. B, Salter-Harris type IV fracture. C, Salter-Harris type I fracture.
The Wilkins Classification System:
* Type A: Salter-Harris type I and II injuries of the proximal radial epiphyses.
* Type B: Salter-Harris type IV injuries of the proximal radial epiphyses.
* Type C: Fractures involving exclusively the proximal radial metaphysis.
* Type D: Fractures occurring iatrogenically when a dislocated elbow is being reduced.
* Type E: Fractures occurring simultaneously in conjunction with an elbow dislocation.
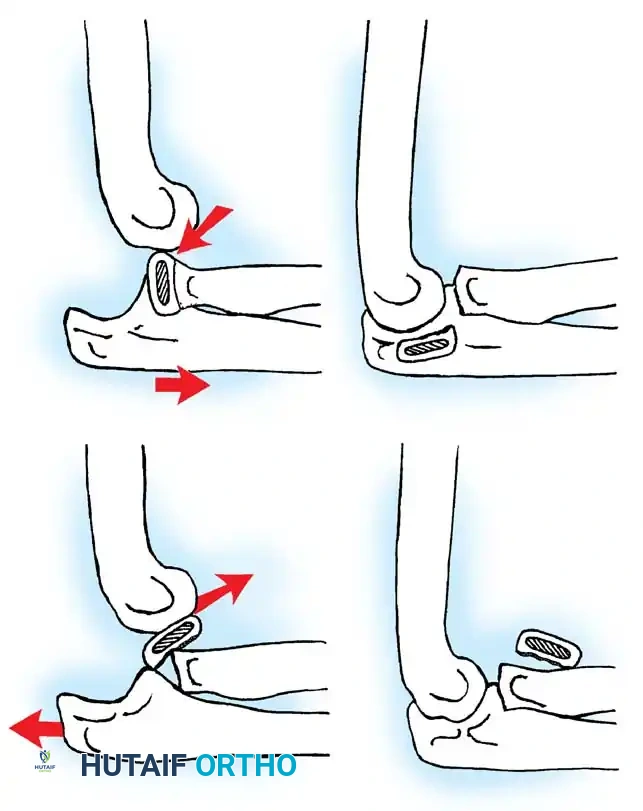
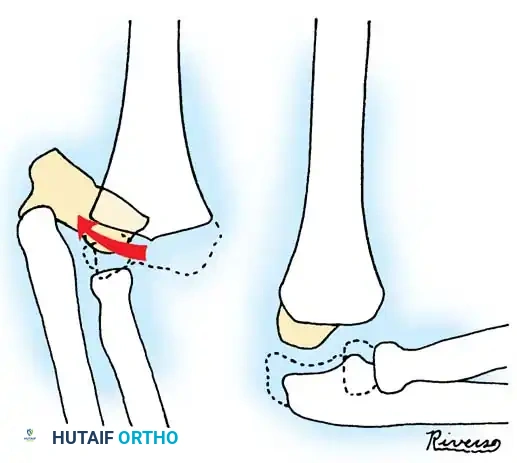
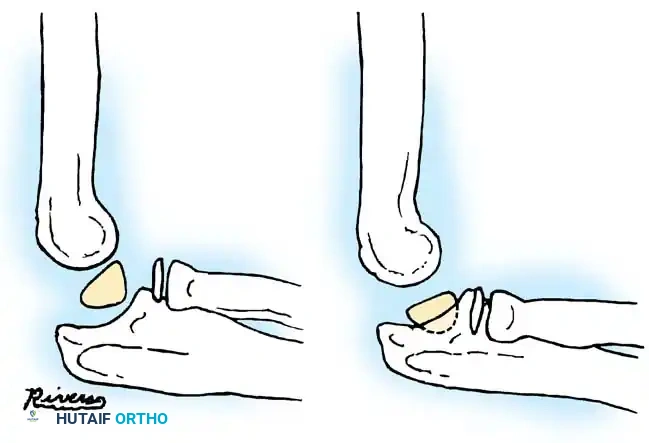
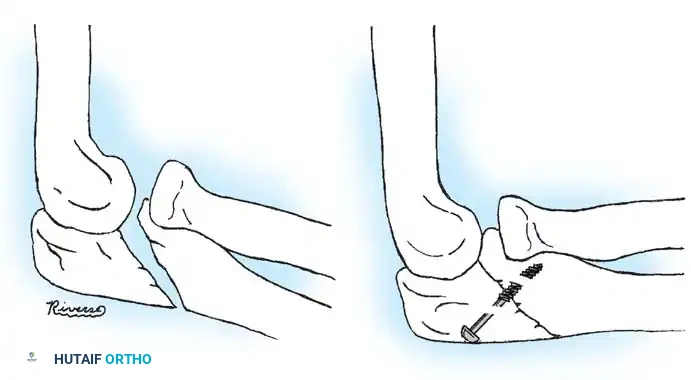
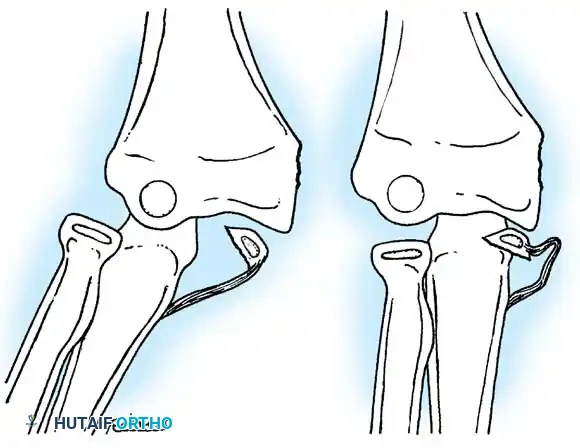
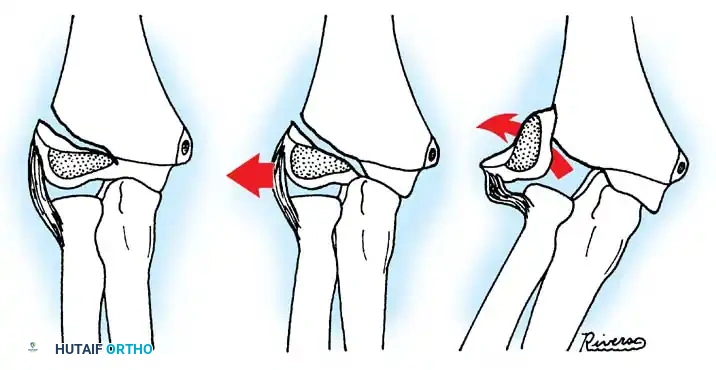
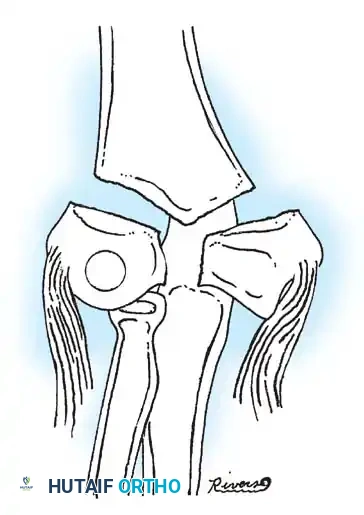
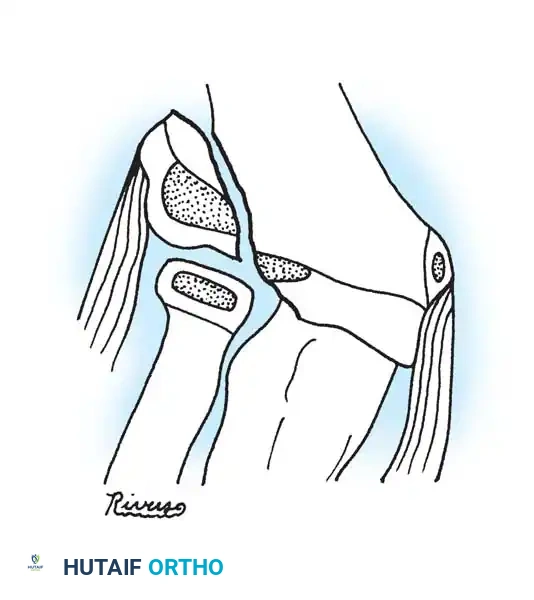
Fig. 33-39 A, Fracture occurring when elbow dislocation is reduced. B, Fractures occurring at time of elbow dislocation.
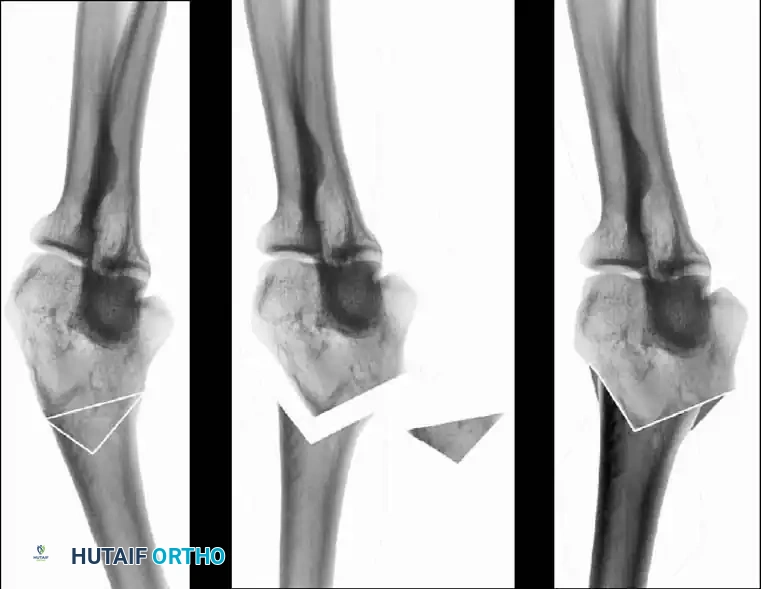
Fractures can present as angulated, translocated (shifted), or totally displaced. In the context of an elbow dislocation, the proximal fragment may become loose within the joint space or trapped, acting as a mechanical block to reduction.
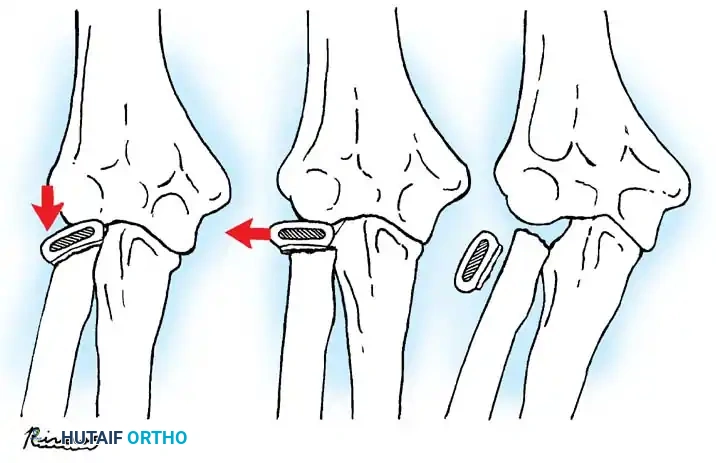
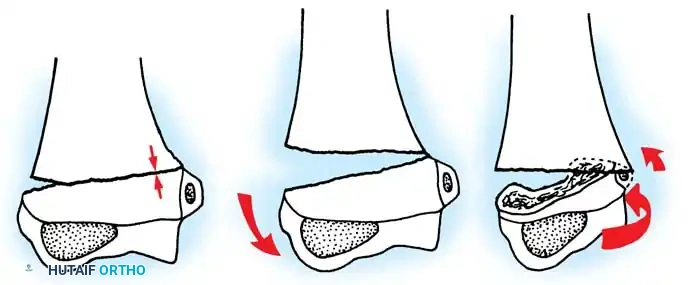
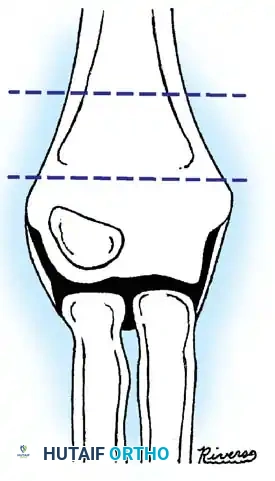
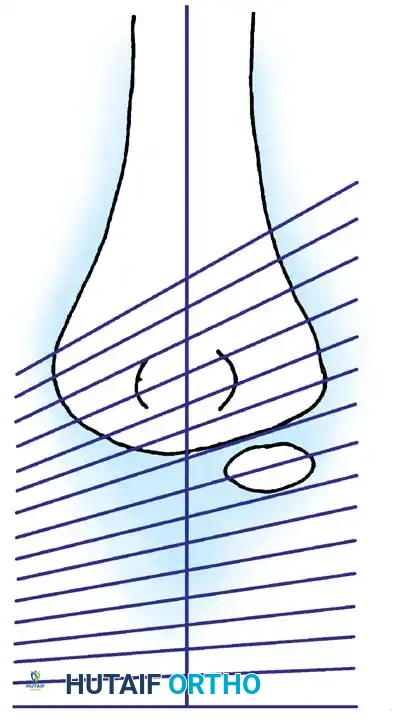
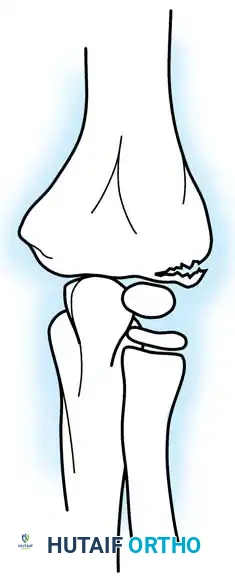
Fig. 33-40 Examples of angulation, translocation, and total displacement of radial neck fractures.
INDICATIONS FOR TREATMENT AND ACCEPTABLE ALIGNMENT
The primary goal of treatment is to restore radiocapitellar alignment to preserve full pronation and supination.
Surgical Warning: Thirty to 45 degrees of residual angulation is generally accepted in closed treatment with satisfactory long-term functional results. Attempting open reduction for angulation less than 45 degrees may introduce unnecessary risks of stiffness, avascular necrosis (AVN), and radioulnar synostosis.
According to Tibone and Stoltz, clinical outcomes are notably inferior in older children approaching skeletal maturity or in patients with associated upper extremity injuries (e.g., medial epicondyle fractures or medial collateral ligament tears). Early intervention is paramount. Steinberg et al. demonstrated that severely displaced fractures achieve superior outcomes following open reduction, whereas moderately displaced fractures perform equally well with closed management.
CLOSED REDUCTION TECHNIQUES
If angulation exceeds 45 degrees, closed reduction should be the first line of intervention. General anesthesia or conscious sedation with fluoroscopic (image intensification) guidance is highly recommended.
The Patterson Technique (Modified by Neher and Torch)
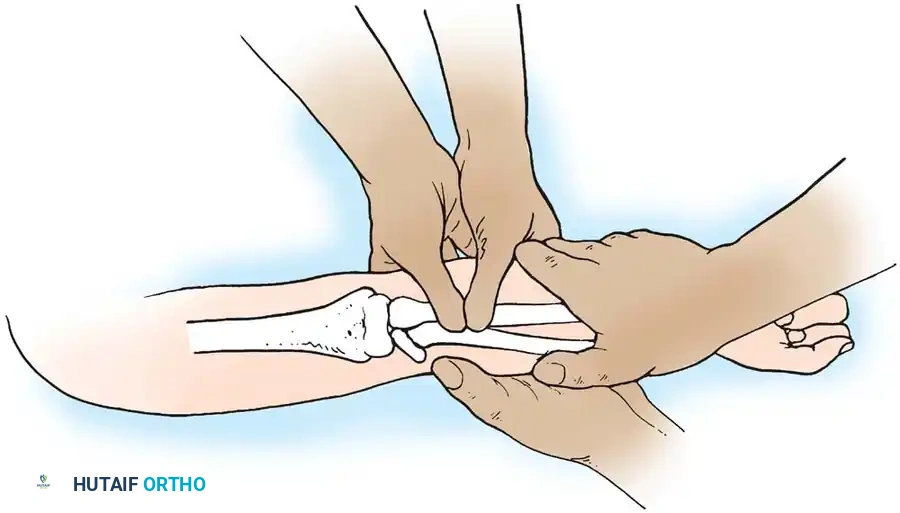
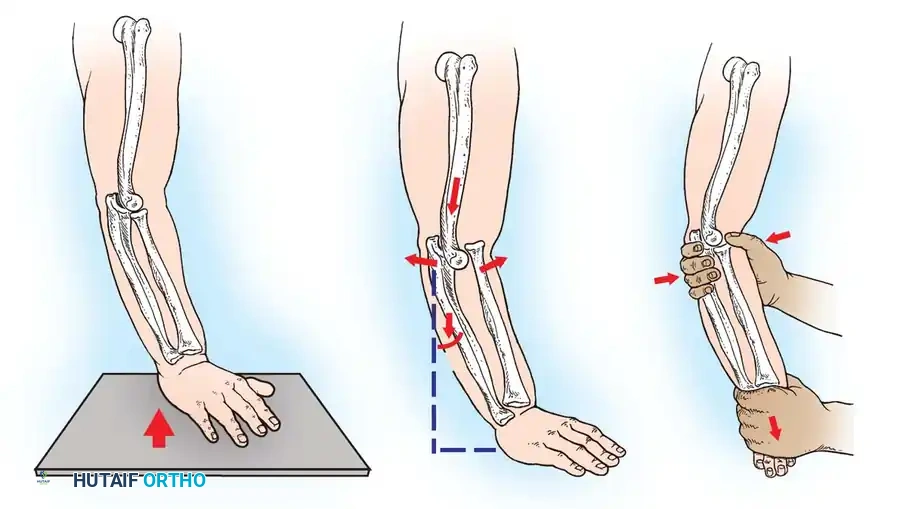
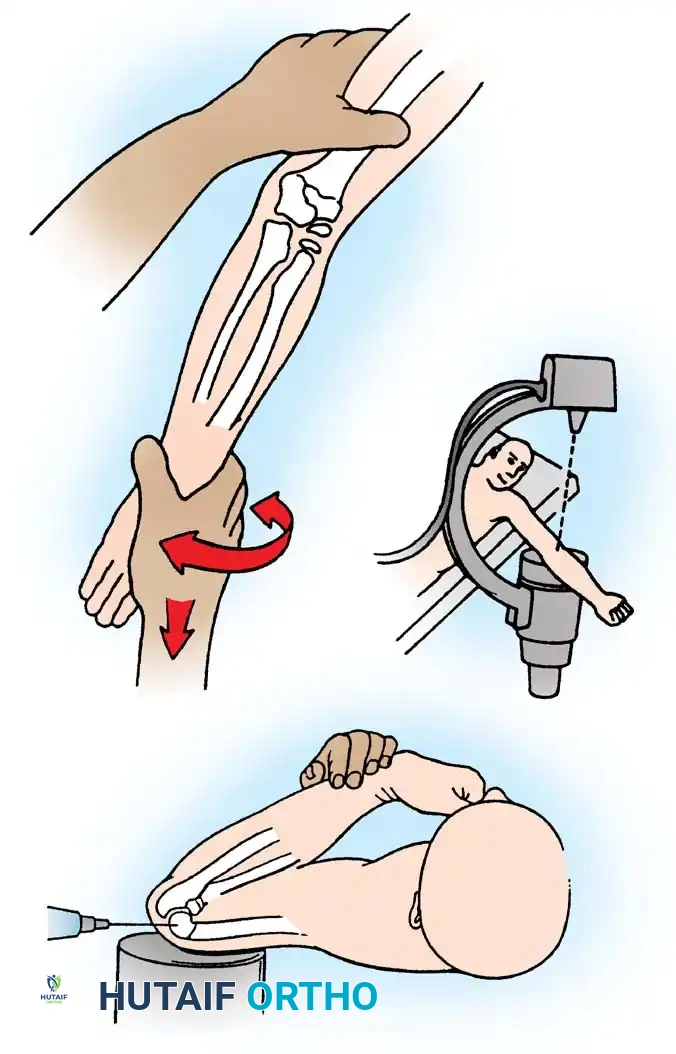
Fig. 33-42 Reduction technique for radial neck fractures.
- Positioning: The patient is placed supine. An assistant firmly stabilizes the distal humerus and the radius distal to the fracture site.
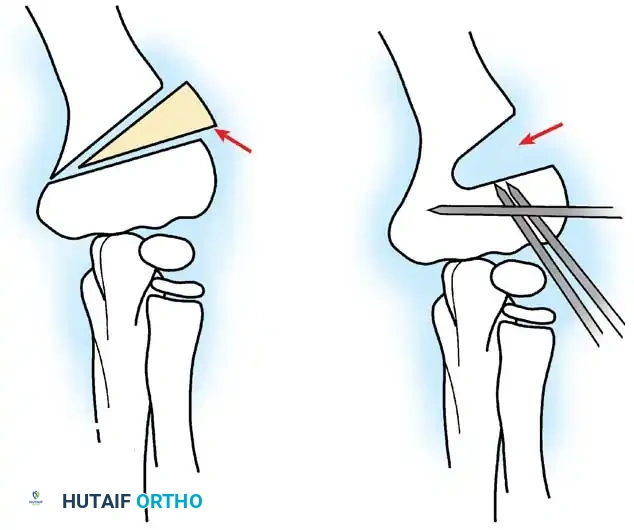
- Maneuver: With the elbow in full extension, the surgeon applies a strong varus stress to the elbow with one hand. This opens the radiocapitellar joint laterally.
- Reduction: Using the thumb of the opposite hand, direct lateral-to-medial pressure is applied over the tilted radial head to lever it back into anatomical alignment.
- Immobilization: The forearm is then placed in 90 degrees of flexion and pronation to lock the reduction.
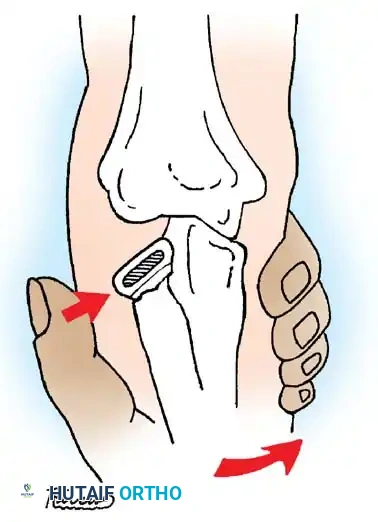
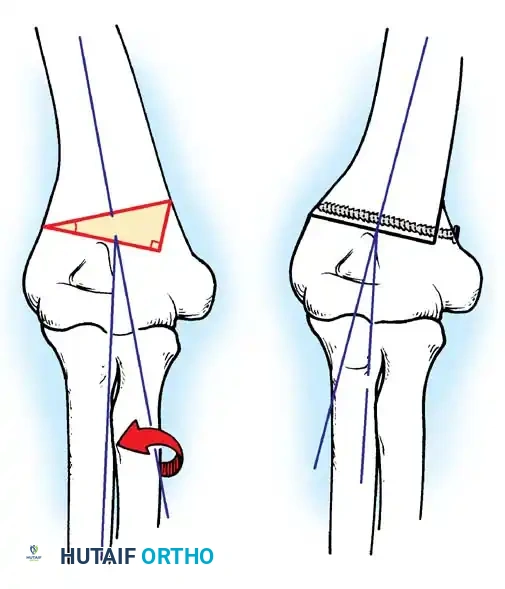
Fig. 33-45 Mechanism of reduction of radial neck fracture.
PERCUTANEOUS AND INTRAMEDULLARY TECHNIQUES
When closed manipulation fails, percutaneous leverage or intramedullary pinning should be utilized before resorting to open reduction.
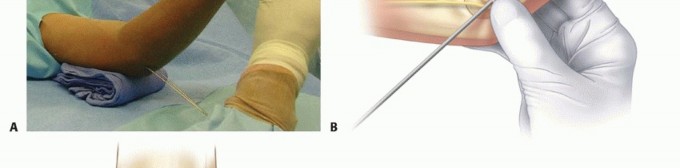
Percutaneous Leverage (Bernstein Technique)
Pesudo et al. and Bernstein et al. popularized the use of a percutaneous pin to manipulate the fracture fragments under fluoroscopy.
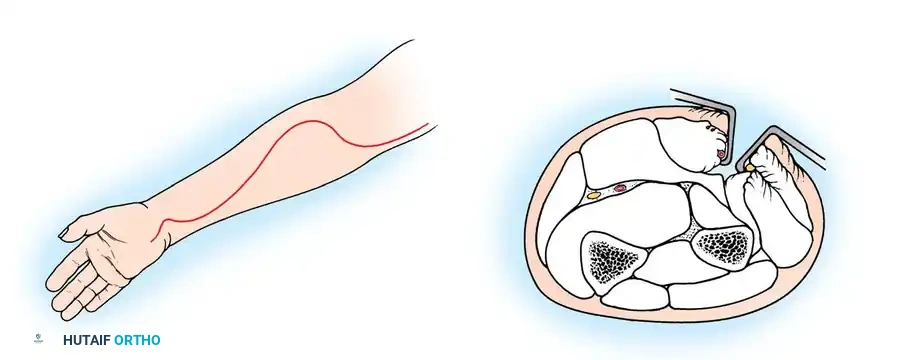
Anatomical Pitfall: During percutaneous reduction, the Kirschner wire must be introduced on the ulnar side of the radius. Introducing the wire laterally risks iatrogenic injury to the deep branch of the radial nerve (posterior interosseous nerve) as it traverses the arcade of Frohse.
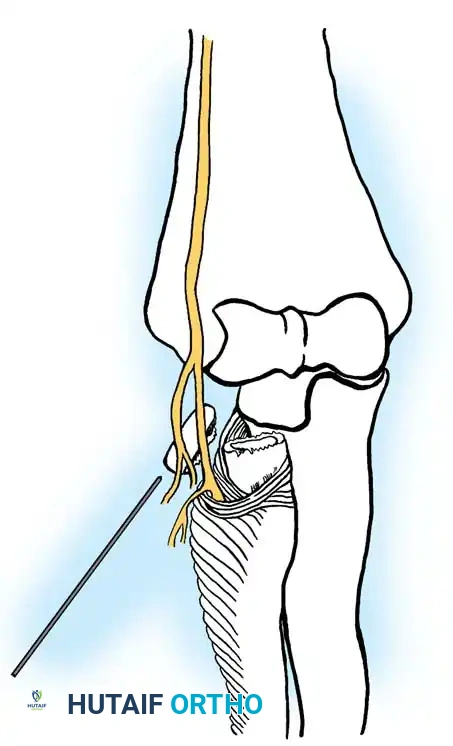
Fig. 33-43 Radial neck fracture in relation to arcade of Frohse.
The Metaizeau Technique (Elastic Stable Intramedullary Nailing)
Gonzalez-Herranz et al. and Metaizeau revolutionized the treatment of displaced radial neck fractures (O’Brien types II and III) using retrograde intramedullary pinning. This technique boasts excellent results in over 94% of cases.
- Entry Point: A small incision is made over the distal lateral radial metaphysis, taking care to protect the superficial radial nerve.
- Pin Preparation: A steel Kirschner wire or titanium elastic nail (TEN) is sharply bent at the distal 1.5 cm.
- Insertion: The wire is advanced retrograde through the medullary canal until the bent tip engages the displaced proximal epiphysis.
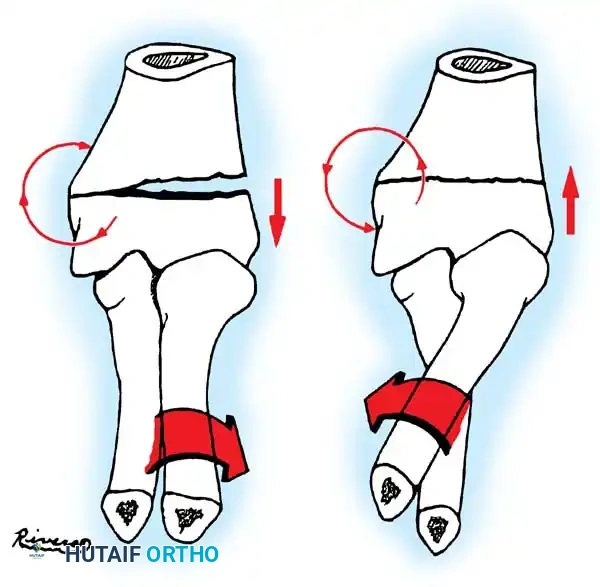
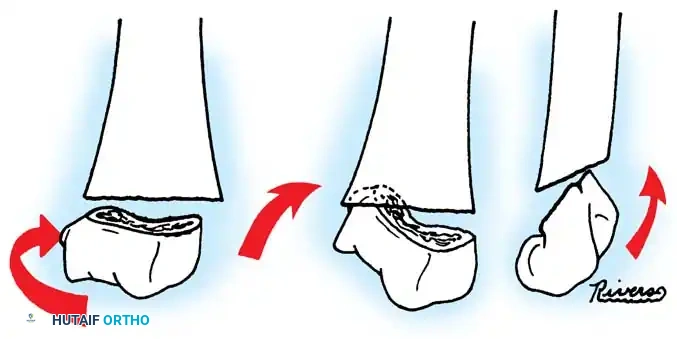
- Reduction: The pin is rotated 180 degrees around its long axis. The bent tip acts as a cam, elevating the radial head and shifting it medially into anatomical position beneath the lateral condyle.

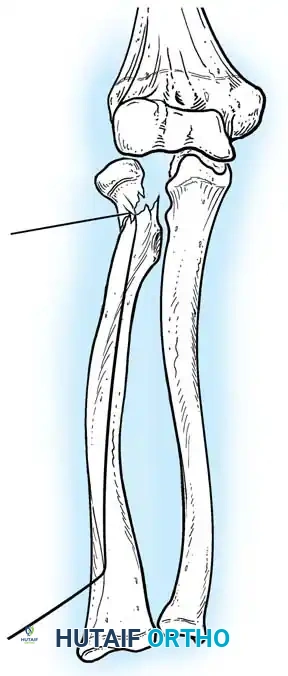
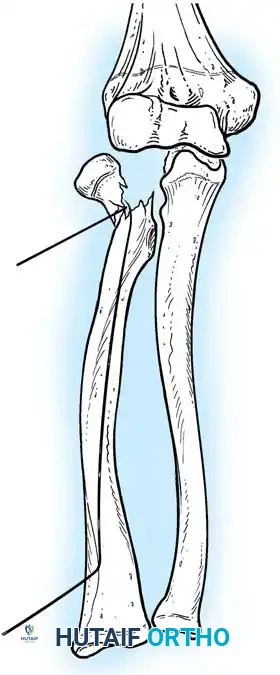
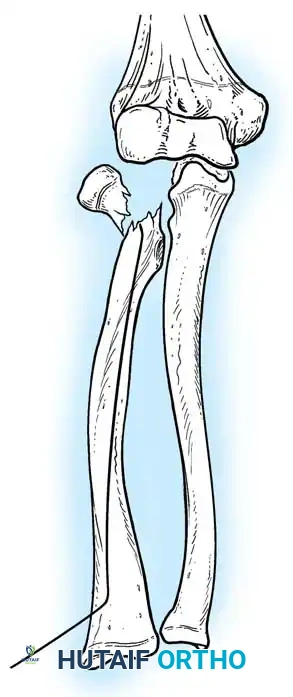
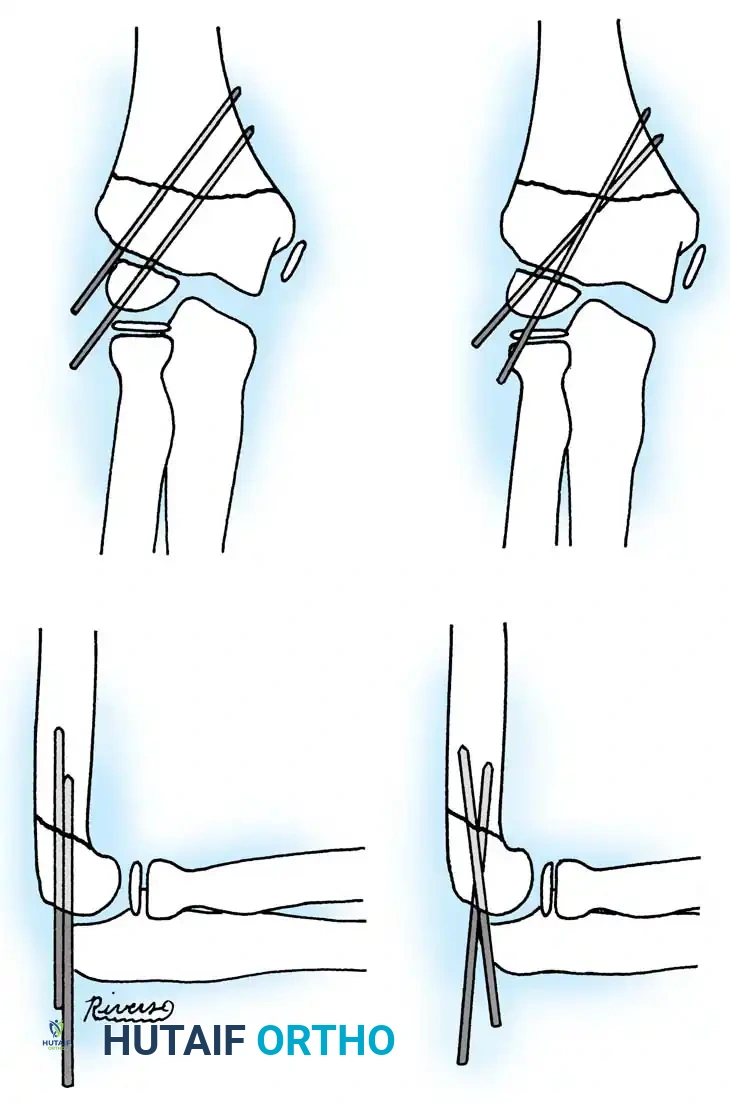
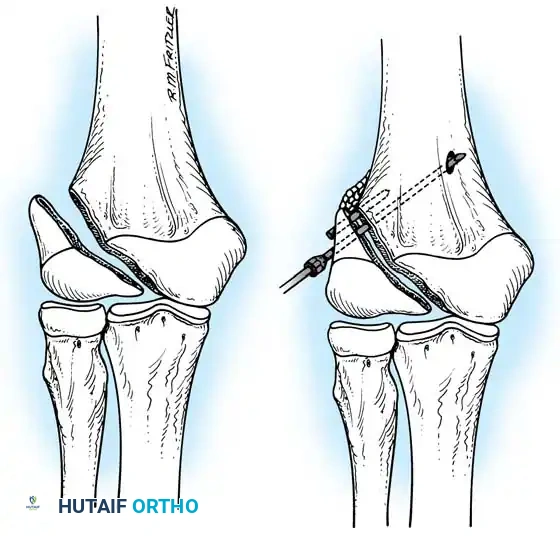
Fig. 33-44 A-D, Reduction of radial head by leverage method and retrograde intramedullary pinning with Kirschner wire.
OPEN REDUCTION AND INTERNAL FIXATION (ORIF)
If closed and percutaneous methods fail to achieve <45 degrees of angulation, open reduction is mandated.
Timing: Surgery must be performed within 5 to 7 days of injury. Delayed surgical intervention drastically increases the risk of myositis ossificans and radioulnar synostosis.
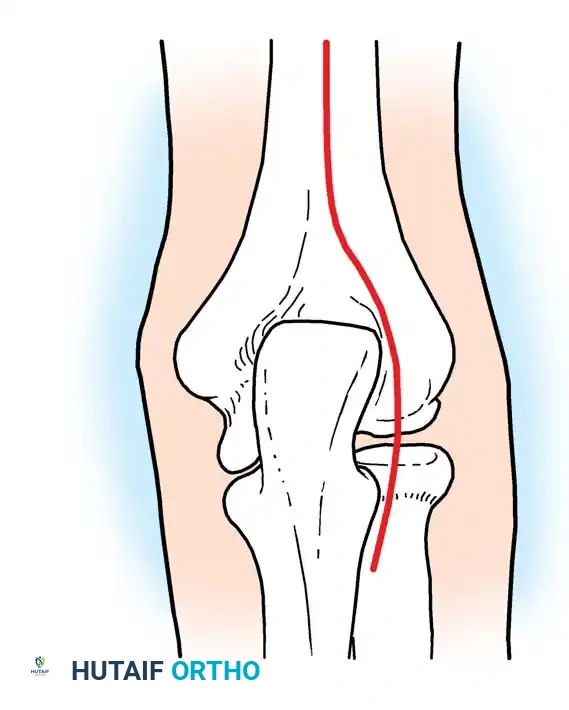
Surgical Approach (Kocher Interval)
- Incision: A lateral Kocher incision is utilized, exploiting the internervous plane between the anconeus (radial nerve) and the extensor carpi ulnaris (posterior interosseous nerve).
- Exposure: The joint capsule is incised anterior to the lateral ulnar collateral ligament (LUCL) to prevent iatrogenic posterolateral rotatory instability (PLRI).
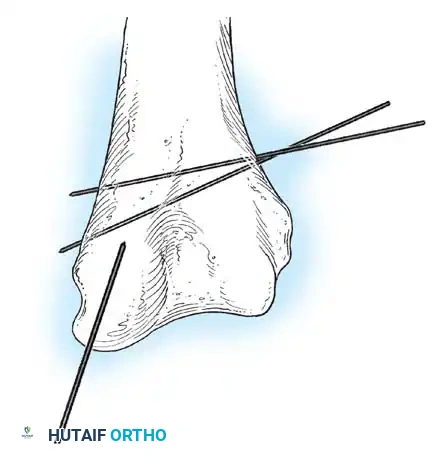
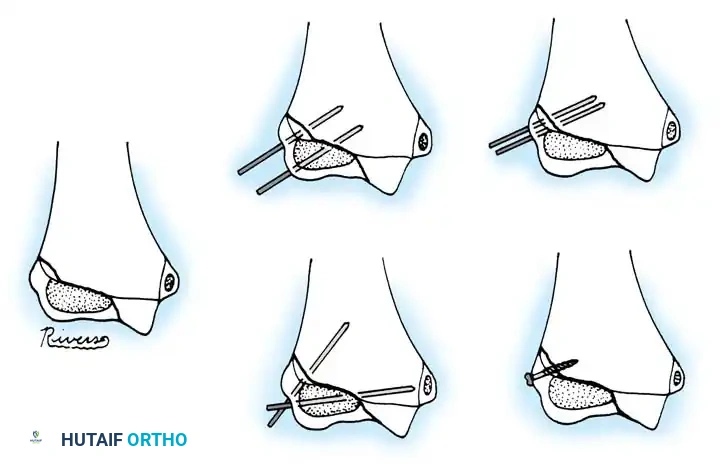
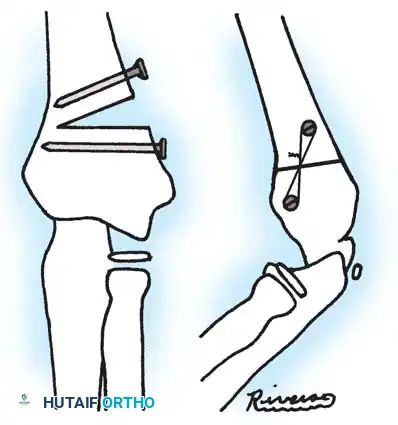
- Fixation: Internal fixation is strictly required; periosteal sutures alone are inadequate. Oblique pins across the fracture are preferred.
Surgical Warning: Avoid transcapitellar (transarticular) wires if possible. While technically easier to insert, they carry a high risk of intraarticular breakage and septic arthritis. Merchan and Fowles both reported significant hardware failure rates with transarticular pinning.
Complications of ORIF
Complications following open reduction are severe and include:
* Loss of pronosupination
* Premature physeal closure
* Nonunion of the radial neck (often due to inadequate fixation)
* Osteonecrosis (AVN) of the radial head due to disruption of the delicate intraosseous blood supply
* Proximal radioulnar synostosis
* Posterior interosseous nerve (PIN) palsy
ADVANCED RECONSTRUCTION: ULNAR OSTEOTOMY FOR CHRONIC DISLOCATIONS
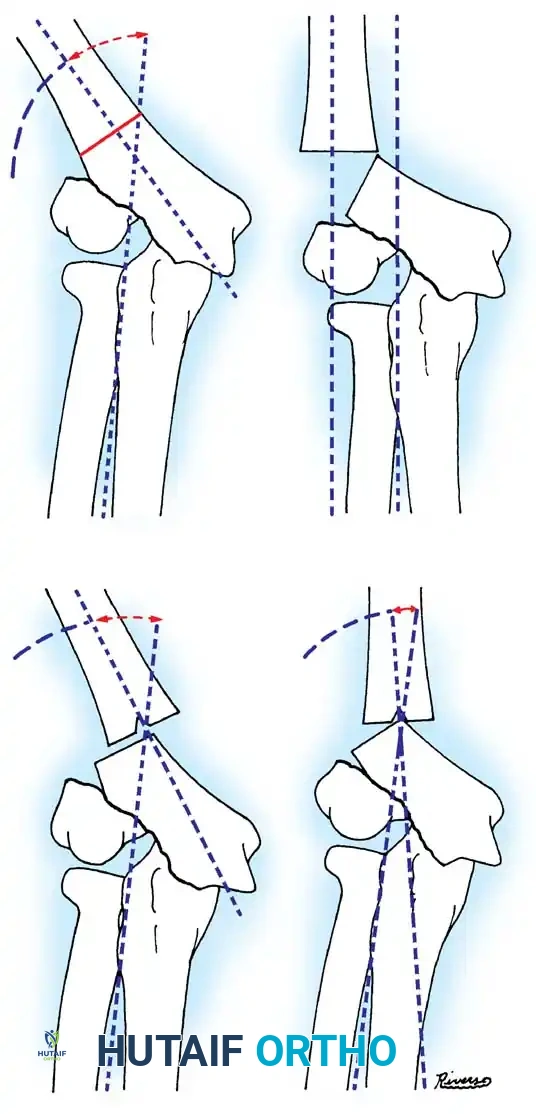
In cases of chronic radial head dislocation (often missed acutely or associated with plastic deformation of the ulna), simple open reduction is insufficient. The Hirayama Technique utilizes an ulnar osteotomy to overcorrect the angular deformity, thereby pulling the radial head back into the joint via the interosseous membrane.
TECHNIQUE 33-5: Osteotomy of the Ulna (Hirayama et al.)
- Preparation: Inflate a pneumatic tourniquet. Make a posterolateral skin incision exposing the radiohumeral joint and proximal third of the ulna. Excise intra-articular scar tissue.
- Osteotomy: Perform a subperiosteal osteotomy of the ulna 5 cm distal to the olecranon.
- Distraction and Angulation: Distract the osteotomy by 1 cm to lengthen the ulna.
- For Anterior Dislocation: Correct by posterior angulation of the ulna.
- For Lateral Dislocation: Correct by medial angulation of the ulna.
- Fixation: Secure the osteotomy with a metal plate bent to approximately 15 degrees. Ensure the radial head rests perfectly within the radial notch of the ulna without excessive radiocapitellar pressure.
- Closure: Approximate the anconeus. Do not repair the annular ligament, as this can restrict rotation.
- Postoperative Care: Apply a plaster splint in 90 degrees of flexion and full supination for 4 weeks, followed by aggressive active range of motion.
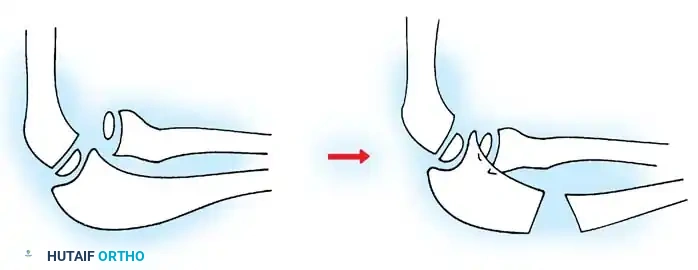
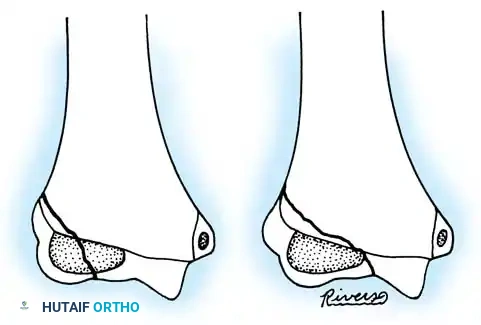
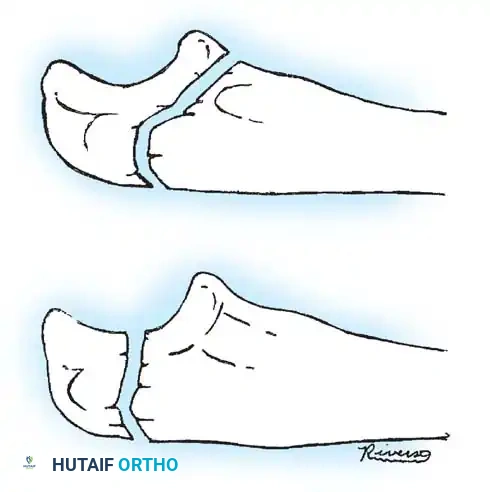
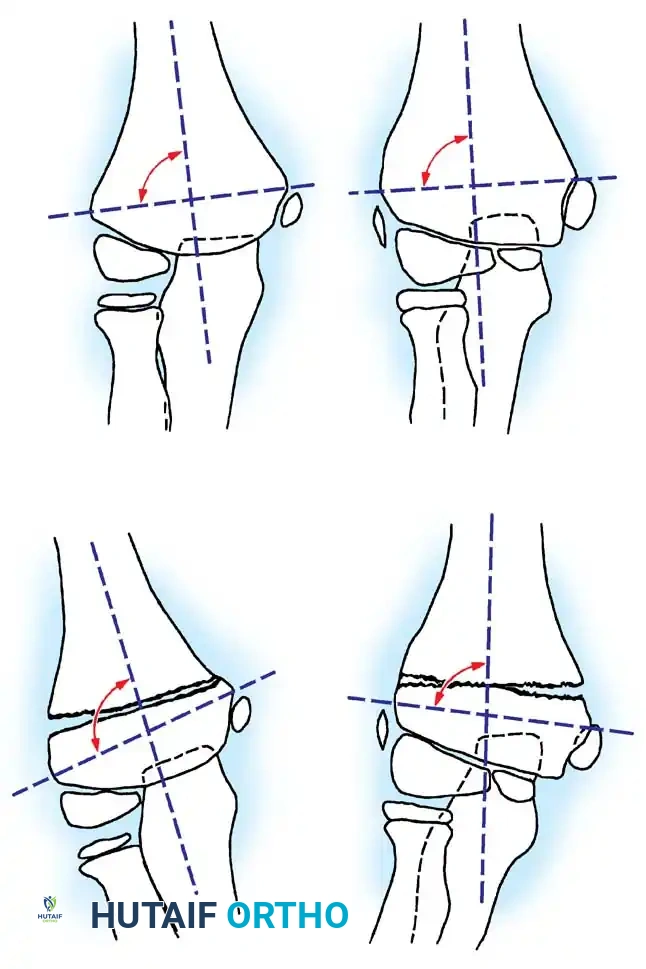
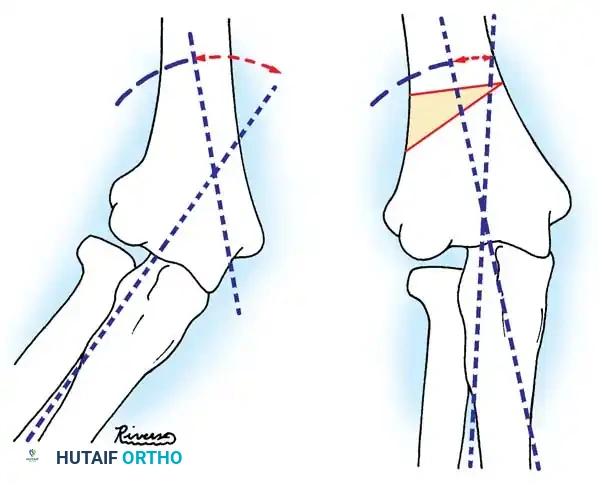
Fig. 33-36 Overcorrection with posterior convexity for anterior dislocation.
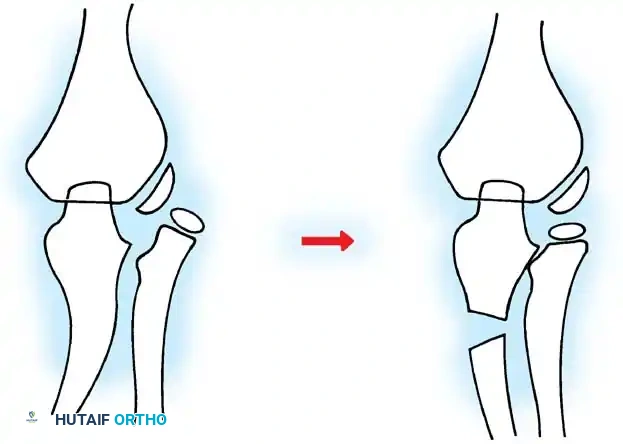
Fig. 33-37 Overcorrection with medial convexity for lateral dislocation.
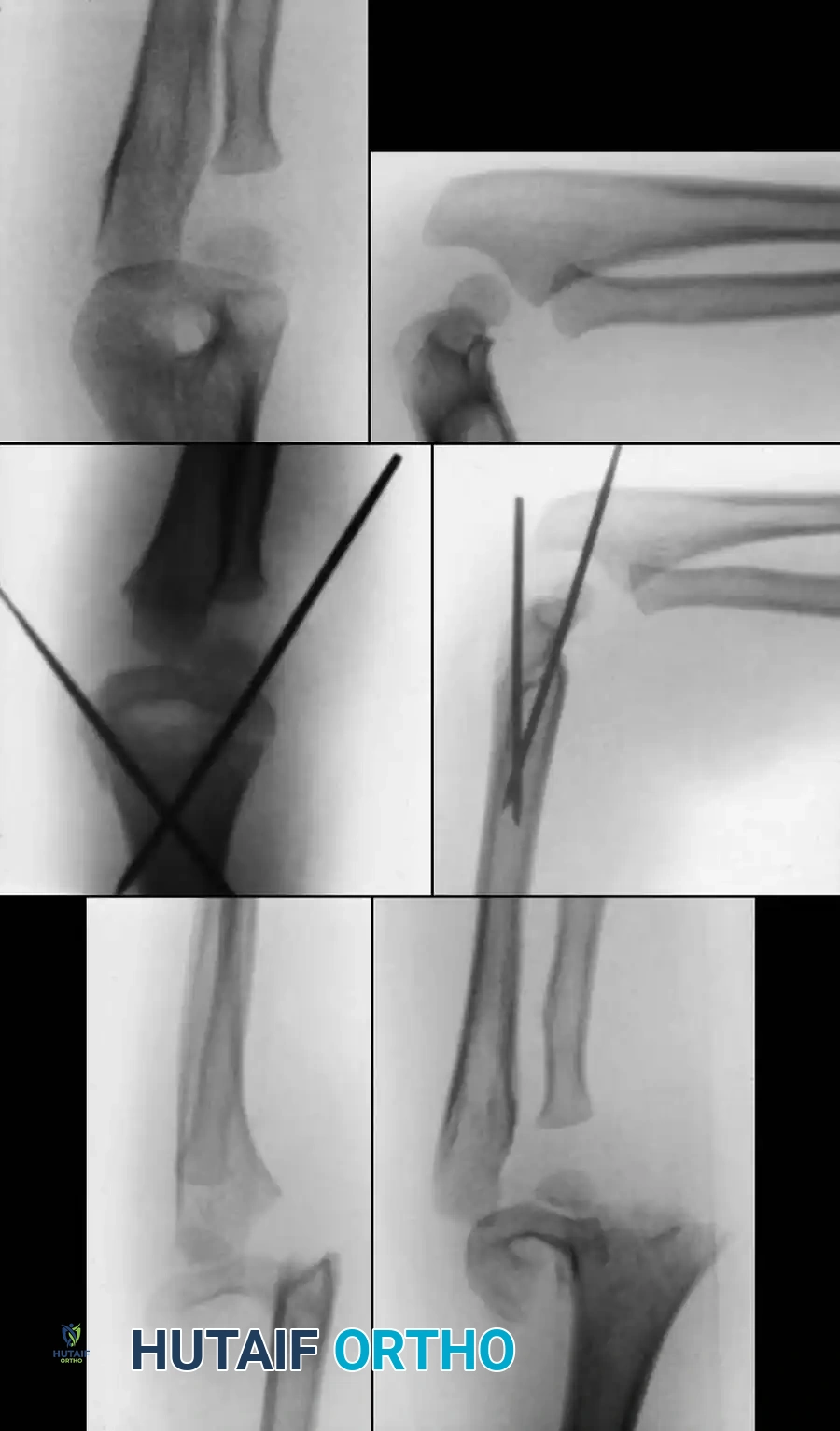
COMPREHENSIVE SURGICAL AND RADIOGRAPHIC ATLAS
The following gallery provides an exhaustive visual reference for the varied presentations, fluoroscopic interventions, and advanced reconstructive techniques associated with pediatric elbow trauma and radial neck fractures.
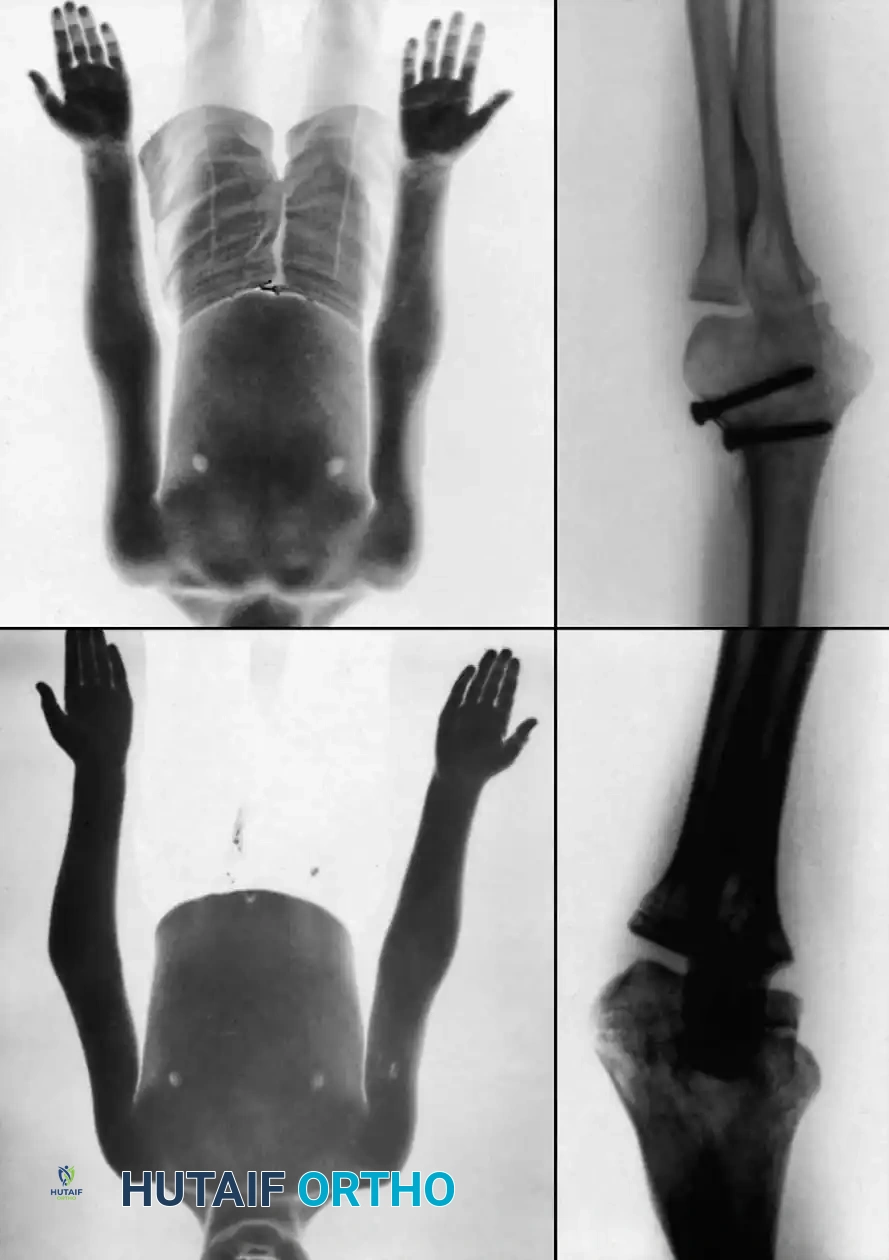
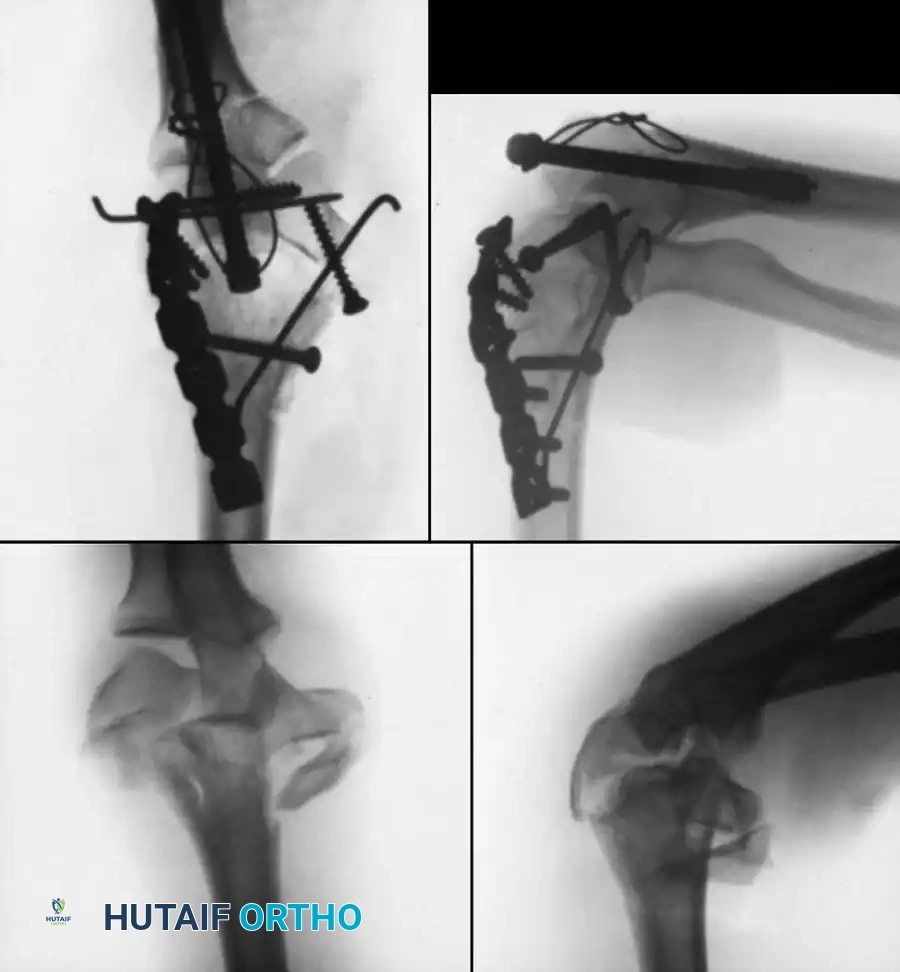
Preoperative Radiographic Evaluation


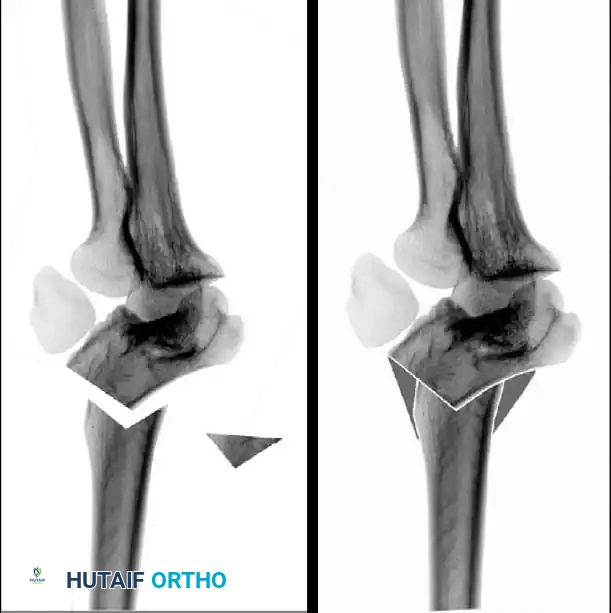
Intraoperative Fluoroscopy and Pin Placement













📚 Medical References
- radial neck fractures in children, J Pediatr Orthop 13:85, 1993.
- Boyd HB, Altenberg AR: Fractures about the elbow in children, Arch Surg 49:213, 1944.
- Cappellino A, Wolfe SW, Marsh JS: Use of a modifi ed Bell Tawse procedure for chronic acquired dislocation of the radial head, J Pediatr Orthop 18:410, 1998.
- Caterini R, Farsetti P, D’Arrigo C, et al: Fractures of the olecranon in children: long-term follow-up of 39 cases, J Pediatr Orthop 11B:320, 2002.
- D’Souza S, Vaishya R, Klenerman L: Management of radial neck fractures in children: a retrospective analysis of one hundred patients, J Pediatr Orthop 13:232, 1993.
- Eastwood DM: Injures to the elbow in childhood—a source of disquiet, J Bone Joint Surg 83B:469, 2001.
- Evans MC, Graham HK:
You Might Also Like