Revision Total Knee Arthroplasty: Mastering Femoral Bone Loss with Augments and Allografts
Key Takeaway
Join us in the OR for a detailed masterclass on Revision Total Knee Arthroplasty. We'll meticulously address femoral bone loss using metal augments and various grafting techniques. This guide covers comprehensive anatomy, precise planning, granular intraoperative steps, critical pearls, and comprehensive postoperative management, ensuring optimal outcomes for complex knee revisions.
Introduction and Epidemiology
The burden of revision total knee arthroplasty is expanding exponentially within orthopedic surgery. Current epidemiological models project that the number of revision total knee arthroplasty procedures performed will increase at an annual rate of 19.3 percent over the next decade. This surge is driven by the expanding indications for primary arthroplasty in younger, more active demographics, alongside the natural survivorship curve of implants placed in previous decades.
Femoral bone defects are relatively uncommon in primary total knee arthroplasty, typically isolated to severe valgus dysplasia, post-traumatic deformity, or severe rheumatoid arthritis. However, significant femoral bone loss is a ubiquitous challenge in the revision setting. The etiology of this bone loss is multifactorial, encompassing aseptic loosening, particulate-induced osteolysis, periprosthetic joint infection, stress shielding, and iatrogenic bone destruction during the extraction of well-fixed primary components.
To address these defects, modular femoral augments have become an indispensable tool in the revision arthroplasty armamentarium. These augments are highly effective for moderate-sized, uncontained bony defects, allowing the surgeon to maximize bone-to-prosthesis contact while accurately restoring the joint line and the posterior condylar offset.

Pathophysiology of Femoral Bone Loss
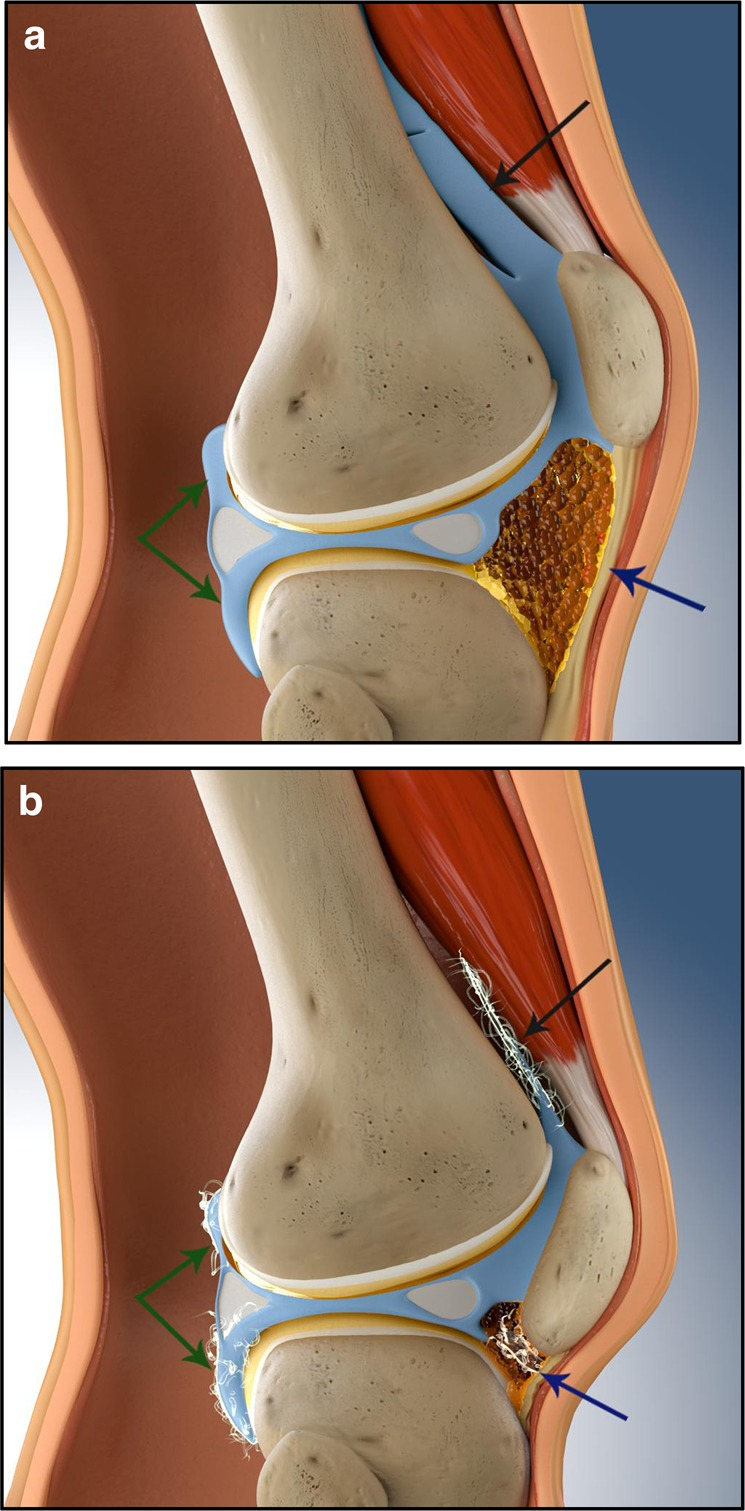
The progressive loss of metaphyseal and epiphyseal bone stock around a failing femoral component fundamentally alters the biomechanical environment of the knee. Polyethylene wear debris generates a macrophage-mediated inflammatory cascade, leading to the activation of osteoclasts and subsequent periprosthetic osteolysis. Furthermore, the presence of a stiff metallic implant alters physiological load transmission, causing stress shielding and localized osteopenia, particularly in the anterior femoral condyles and distal metaphysis. When revision surgery is indicated, the extraction of cemented or porous-coated implants inevitably strips additional cancellous bone, converting contained defects into uncontained, structurally deficient voids that require robust reconstructive strategies.
Surgical Anatomy and Biomechanics
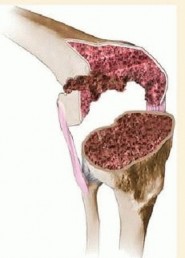
A profound understanding of distal femoral anatomy and knee biomechanics is required to successfully utilize metal augments. The most common forms of bone defects encountered at the time of revision surgery involve the distal and posterior aspects of the femoral condyles.

The distal femur consists of the medial and lateral condyles, which articulate with the tibial plateau, and the anterior trochlear groove, which articulates with the patella. The structural integrity of the metaphyseal flare is critical for the primary stability of a revision femoral component. When metaphyseal bone is compromised, the surgeon must rely on diaphyseal stem engagement to offload the deficient condyles, utilizing augments to fill the remaining epiphyseal voids and provide rotational stability.

Femorotibial Joint Line Restoration
Aside from filling the osseous defect, the primary biomechanical objective in revision knee surgery is the precise restoration of the femorotibial joint line and the posterior condylar offset. The native joint line is typically located 10 to 14 millimeters distal to the medial epicondyle, or approximately 15 millimeters proximal to the fibular head. Proximal migration of the joint line—a common error in revision surgery when distal femoral bone loss is underestimated—results in patella baja, altered patellofemoral kinematics, mid-flexion instability, and decreased extensor mechanism efficiency. Distal femoral augments are utilized specifically to translate the femoral component distally, reconstituting the extension gap and restoring the joint line to its anatomic level.
Biomechanical Properties of Metal Augments
Posterior condylar offset dictates the flexion gap and influences the maximal achievable flexion postoperatively. Failure to restore posterior offset leads to flexion instability and impingement of the posterior tibial margin against the femoral metaphysis. Posterior metal augments lateralize and medialize the condylar geometry to recreate this critical dimension.
Modern improvements in implant design and biomaterials have drastically increased the versatility of metal augments. Traditional titanium and cobalt-chromium augments provide excellent structural support but exhibit a high modulus of elasticity compared to cancellous bone. The advent of highly porous metals, such as tantalum trabecular metal and 3D-printed porous titanium, has revolutionized defect management. These materials boast a high coefficient of friction for initial scratch fit, a modulus of elasticity closely mimicking cancellous bone to minimize stress shielding, and a highly interconnected porosity that facilitates rapid and robust osteointegration in uncemented applications.
Indications and Contraindications
The selection of metal augments versus alternative reconstructive options relies heavily on the precise classification of the bone defect. The Anderson Orthopaedic Research Institute classification system remains the gold standard for evaluating femoral bone defects and guiding surgical intervention.

Anderson Orthopaedic Research Institute Classification
The Anderson Orthopaedic Research Institute classification categorizes defects based on the integrity of the metaphyseal bone and its capacity to support a revision component.
Type 1 defects involve intact metaphyseal bone with minor focal defects that do not compromise component stability. These are typically managed with standard cement application or localized morselized bone grafting.
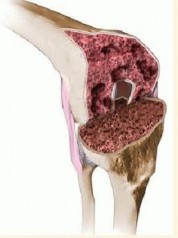
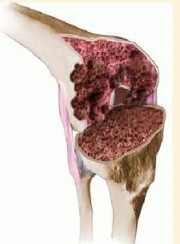
Type 2 defects involve damaged metaphyseal bone with significant cancellous bone loss necessitating structural fill to restore a reasonable joint line level. These defects can involve one condyle (Type 2A) or both condyles (Type 2B). For defects less than 5 millimeters, cement or bone graft is sufficient. For defects greater than 5 millimeters but less than 15 millimeters, metallic augments (distal or posterior) are the treatment of choice.

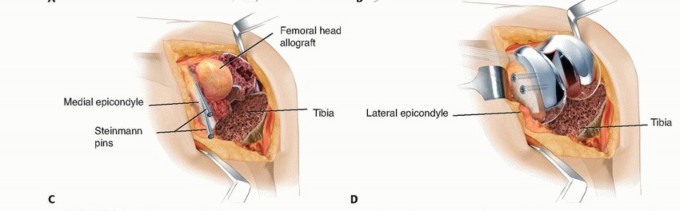
Type 3 defects are characterized by deficient metaphyseal bone that compromises a major portion of either condyle, rendering the metaphysis incapable of supporting the implant. These massive defects require structural allografts, highly porous metaphyseal cones or sleeves, hinged implants, or custom megaprostheses. While augments may still be used in Type 3 defects to fine-tune the joint line, they are insufficient as the sole method of metaphyseal reconstruction.
| Defect Classification | Clinical Presentation | Operative Indication | Alternative Non Operative or Salvage Management |
|---|---|---|---|
| AORI Type 1 | Intact metaphysis, minor focal epiphyseal voids | Cement fill, morselized autograft/allograft | Observation if asymptomatic and implant is well-fixed |
| AORI Type 2A | Unicondylar metaphyseal damage, >5mm defect | Unilateral distal/posterior metal augments | Suppressive antibiotics (if infected and poor surgical candidate) |
| AORI Type 2B | Bicondylar metaphyseal damage, uncontained defects | Bilateral metal augments, diaphyseal stem extension | Knee arthrodesis (salvage for severe extensor mechanism failure) |
| AORI Type 3 | Massive metaphyseal bone loss, absent condyles | Metaphyseal cones/sleeves + augments, structural allograft, tumor prosthesis | Above-knee amputation (salvage for intractable infection/vascular compromise) |
Pre Operative Planning and Patient Positioning
A systematic approach to preoperative planning, intraoperative evaluation, and reconstruction is essential when addressing femoral defects using metal augments. The success of the revision procedure is heavily dependent on anticipating the size and location of bone voids before the first incision is made.
Imaging and Digital Templating
Standard radiographic evaluation must include weight-bearing anteroposterior, lateral, skyline patellar, and full-length standing lower extremity views. The full-length films are critical for determining the mechanical axis, assessing extra-articular deformities, and measuring the diaphyseal bowing of the femur, which dictates the length and trajectory of the revision stem.

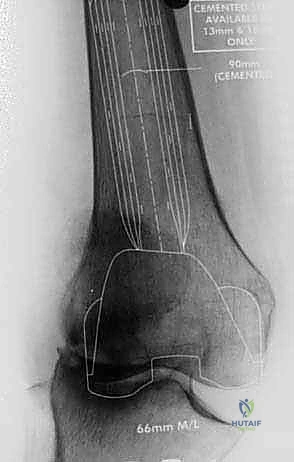
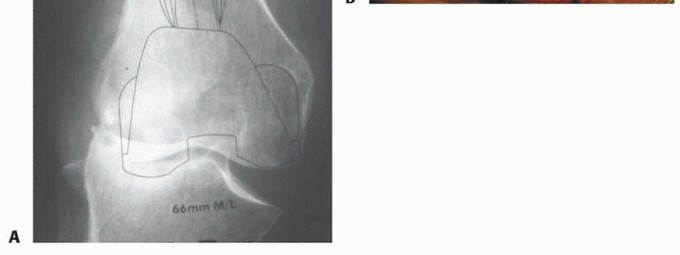
Advanced imaging, particularly computed tomography with metal artifact reduction sequence, provides a three-dimensional understanding of osteolytic lesions that are often obscured by the primary implant on plain radiographs. Digital templating is mandatory. The surgeon must template the anticipated joint line based on contralateral knee radiographs or anatomical landmarks such as the adductor tubercle and fibular head. Templating allows for the estimation of stem diameter, stem length, and the required thickness of distal and posterior augments.

Patient positioning follows standard arthroplasty protocols. The patient is placed supine on a radiolucent operating table to facilitate intraoperative fluoroscopy. A sterile tourniquet may be applied to the proximal thigh, though its inflation is often reserved for the cementation phase to minimize ischemic time. A robust leg holder is utilized to allow hyperflexion of the knee, which is often necessary for component extraction and diaphyseal preparation.
Detailed Surgical Approach and Technique
The surgical approach in revision total knee arthroplasty must balance adequate exposure with the preservation of the extensor mechanism and soft tissue envelope.

Extensile Exposures and Component Explantation
The previous midline skin incision is typically utilized. A standard medial parapatellar arthrotomy is performed. Due to the presence of dense scar tissue and altered joint mechanics, standard exposure may place undue tension on the patellar tendon insertion. The surgeon must maintain a low threshold for extensile measures, such as a quadriceps snip or a tibial tubercle osteotomy, to prevent catastrophic patellar tendon avulsion.
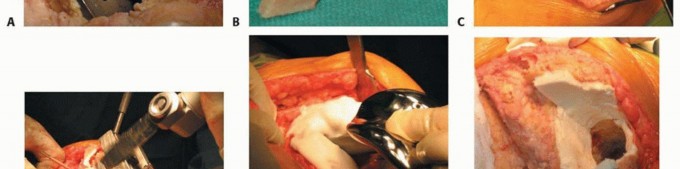
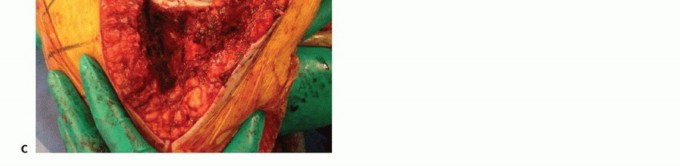
Implant extraction must be meticulous. The interface between the bone and the implant or cement mantle is carefully disrupted using thin, flexible osteotomes, oscillating saws, and ultrasonic extraction devices. The goal is to remove the component with zero additional bone loss. Once the implants are removed, an aggressive synovectomy and debridement of all particulate debris, fibrous tissue, and residual cement are performed to accurately assess the remaining host bone.

Defect Preparation and Gap Balancing
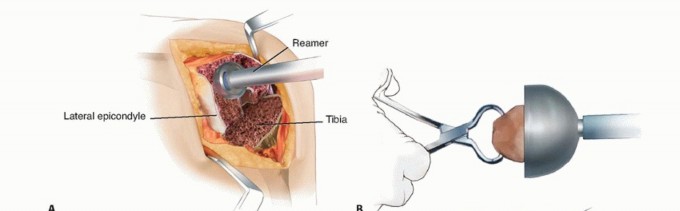
Following debridement, the femoral canal is sequentially reamed to engage the diaphysis. Diaphyseal engagement provides the necessary alignment and initial stability for the revision construct. The femoral trial stem is inserted, and the degree of distal and posterior epiphyseal bone loss is visually and mechanically quantified.

Restoration of the joint line is achieved by referencing the medial epicondyle. If the trial femoral component sits too proximally, the extension gap will be disproportionately large, and the joint line will be elevated. Distal femoral augments (typically available in 5, 10, and 15-millimeter thicknesses) are added to the trial component to translate it distally until the anatomic joint line is achieved and the extension gap is appropriately tensioned against the reconstructed tibia.
Subsequently, the flexion gap is assessed. If the flexion gap is loose or asymmetric, posterior condylar augments are added to the trial component. These augments restore the posterior condylar offset, tension the collateral ligaments in flexion, and prevent anterior translation of the femur on the tibia during deep flexion.
Final Implantation and Fixation Strategy
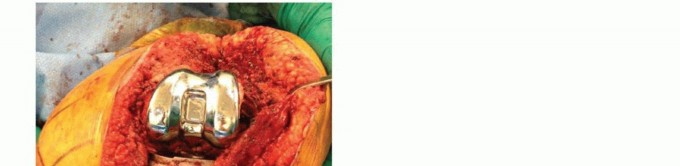
Once the trial components demonstrate optimal tracking, stability, and joint line restoration, the definitive implants are prepared. Modular metal augments are securely fastened to the definitive femoral component using specialized locking screws or Morse taper mechanisms, depending on the manufacturer's design.
The fixation strategy typically involves hybrid cementation. High-viscosity polymethylmethacrylate bone cement is applied to the undersurface of the augments and the metaphyseal portion of the femoral component. The diaphyseal stem is often left uncemented (press-fit) to allow for stress transfer to the diaphysis and facilitate future revisions, although fully cemented stems may be indicated in cases of severe diaphyseal osteopenia. The component is impacted into place, and excess cement is meticulously removed before polymerization is complete.
Complications and Management
Despite meticulous technique, the use of metal augments in revision total knee arthroplasty is associated with specific intraoperative and postoperative complications. The altered biomechanics and compromised soft tissue envelope inherent in revision surgery elevate the risk profile compared to primary arthroplasty.

Joint Line Alteration and Kinematic Failure
The most subtle yet functionally devastating complication is the failure to accurately restore the joint line. Over-augmentation distally can lead to joint line depression, resulting in patella alta and extension deficits. Conversely, under-augmentation leads to joint line elevation, patella baja, and mid-flexion instability. Management requires re-revision with appropriate augment sizing or the use of offset stems to correct the kinematic imbalance.
Aseptic loosening remains a primary mode of failure. While augments fill voids, they do not provide biological fixation unless highly porous metals are utilized without cement. Stress shielding beneath solid titanium augments can lead to progressive localized osteolysis. Periprosthetic joint infection is another major concern, given the increased operative time, larger volume of retained foreign material, and compromised local vascularity.

| Complication | Estimated Incidence | Etiology | Salvage and Management Strategies |
|---|---|---|---|
| Aseptic Loosening | 4 - 8% | Stress shielding, inadequate initial fixation, progressive osteolysis | Re-revision with longer diaphyseal stems, transition to metaphyseal cones/sleeves |
| Periprosthetic Infection | 3 - 7% | Prolonged operative time, extensive dead space, compromised host immunity | Two-stage exchange arthroplasty with articulating antibiotic spacer |
| Joint Line Elevation | 10 - 15% | Underestimation of distal bone loss, failure to use adequate distal augments | Re-revision with thicker distal augments, proximalization of the tibial plateau |
| Periprosthetic Fracture | 2 - 5% | Stress risers at the tip of the diaphyseal stem, aggressive impaction | Open reduction internal fixation with locking plates, or revision to a longer stem bypassing the fracture |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following revision total knee arthroplasty with femoral augments must be tailored to the intraoperative findings, the security of the component fixation, and the integrity of the extensor mechanism.

Early Mobilization and Weight Bearing
In cases where robust diaphyseal press-fit fixation is achieved and the augments are securely cemented to host bone with a competent metaphyseal shell, patients are typically allowed to weight-bear as tolerated immediately postoperatively. Early mobilization is critical to prevent deep vein thrombosis and pulmonary embolism, which have a higher incidence following revision procedures.
If the bone quality is exceedingly poor, or if an extensile exposure such as a tibial tubercle osteotomy was required, weight-bearing may be restricted to toe-touch or partial for the first six weeks. Range of motion exercises are initiated on postoperative day one, utilizing continuous passive motion machines or active-assisted physical therapy. The primary goal in the first two weeks is achieving full extension to prevent flexion contractures, followed by progressive flexion targeting a minimum of 90 degrees by week four.
Summary of Key Literature and Guidelines
The academic literature robustly supports the use of modular metal augments for AORI Type 2 defects in revision total knee arthroplasty. Foundational studies evaluating the survivorship of titanium and cobalt-chromium augments demonstrate excellent mid-to-long-term results, with 10-year survivorship free from aseptic loosening frequently exceeding 90 percent.

Recent biomechanical and clinical investigations have shifted focus toward highly porous metal augments. Trabecular metal augments have shown superior biological fixation potential in uncemented applications, significantly reducing the incidence of radiolucent lines at the augment-bone interface compared to solid metal augments. Furthermore, finite element analysis studies confirm that porous metals exhibit a modulus of elasticity that mitigates stress shielding, preserving the remaining metaphyseal bone stock for potential future revisions. Current consensus guidelines recommend the routine use of modular augments for uncontained defects ranging from 5 to 15 millimeters, emphasizing the critical importance of joint line restoration and diaphyseal offloading to ensure construct longevity.
You Might Also Like