Full Question & Answer Text (for Search Engines)
Question 1:
When counseling a patient concerning the treatment of an acute Achilles tendon rupture, which of the following is true:
Options:
- The relative risk of rerupture is 10 times greater in patients treated nonoperatively.
- The relative risk of infection is five times greater in patients treated operatively.
- The relative risk of complications in the operative group is twice as high as those treated nonoperatively.
- The relative risk of rerupture is equal between the operative and nonoperative treatment.
- The relative risk of rerupture is two times higher with nonoperative treatment.
Correct Answer: The relative risk of rerupture is 10 times greater in patients treated nonoperatively.
Explanation:
This meta-analysis showed: Operative versus nonoperative (pooled rates):
Question 2:
Following open repair of an Achilles tendon rupture, which of the following is true:
Options:
- C asting alone has a lower risk or rerupture compared to casting followed by functional bracing.
- C asting alone has a higher rate of rerupture compared to casting followed by functional bracing.
- There is a higher complication rate in the group treated by casting followed by functional bracing compared to casting alone.
- C asting alone has a lower rerupture rate and complication rate compared to casting followed by functional bracing.
- C asting followed by functional bracing has an unacceptable rerupture rate.
Correct Answer: C asting alone has a lower risk or rerupture compared to casting followed by functional bracing.
Explanation:
This meta-analysis showed: Postoperative splinting: cast alone compared with cast followed by functional bracing Rerupture Cast alone 5.0% (7/140) (relative risk 2.04) Cast followed by functional bracing 2.3% (3/133) Complications (adhesions, infection, disturbed sensibility): Cast alone 35.7% (50/140) (relative risk 1.88) Cast followed by functional bracing 19.5% (26/133)
Question 3:
Which of the following is the most useful symptom or sign of a foot compartment syndrome:
Options:
- Numbness in the lateral plantar nerve distribution
- Weakness of toe extension (interossei muscles)
- Decreased capillary refill
- Severe pain
- Weakness of ankle plantarfexion
Correct Answer: Severe pain
Explanation:
Pain out of proportion to injury is the most reliable indicator of a foot compartment syndrome. Foot compartment syndromes can be difficult to diagnose compared to compartment syndromes of the leg. In the leg, one can rely on motor and nerve testing while motor testing in the foot is difficult secondary to the pain from the injury. The severe pain is usually out of proportion to injury. Pain suggestive of compartment syndrome includes: Unremitting pain Pain not responsive to increasing doses of narcotics Pain that is so severe the patient cannot lie still or cooperate with the examiner
Question 4:
Which of the following is the most useful sign in diagnosing a foot compartment syndrome:
Options:
- Numbness in the lateral plantar nerve distribution
- Numbness in the medial plantar nerve distribution
- Weakness with toe dorsiflexion
- Weakness when testing ankle plantarflexion
- Severe pain with passive toe flexion
Correct Answer: Severe pain with passive toe flexion
Explanation:
Pain with passive stretch is a reliable sign in compartment syndrome of the leg, foot, and ankle. In Myersonâ s study, he found that pain with passive stretch was present in 86% of patients when those intrinsic muscles of the foot were stretched.
Question 5:
Which of the following compartments are most commonly involved (increased tissue pressure) in compartment syndrome of the foot:
Options:
- Superficial
- Medial
- C alcaneal
- Adductor
- First interosseus
Correct Answer: C alcaneal
Explanation:
The calcaneal compartment is most commonly involved in foot compartment syndromes. Approximately 5% to 10% of calcaneus fractures are complicated by a compartment syndrome. The cancellous bone of the calcaneus may have significant bleeding. Swelling of the hindfoot can be severe.
Question 6:
Which of the following is the most commonly accepted number of foot compartments:
Options:
- Three
- Five
- Eight
- Nine
- Twelve
Correct Answer: Nine
Explanation:
The foot can be divided into nine distinct compartments. A. C alcaneal compartment 1. Quadratus plantae 2. Posterior tibial nerve, artery, and vein 3. Lateral plantar nerve, artery, and vein 4. Medial plantar nerve (variable) *Remember that the calcaneal compartment may communicate with the posterior tibial compartment. A. Interosseiâ (four separate compartments) B. Adductor muscle C . Medial 1. Flexor hallucis brevis 2. Abductor hallucis D. Lateral 1. Abductor digiti minimi 2. Flexor digiti minimi E. Superficial 1. Flexor digitorum brevis 2. Lumbricals (four) 3. Flexor digitorum longus 4. Medial plantar nerve (variable)
Question 7:
Which of the following structures is in the calcaneal compartment of the foot:
Options:
- Flexor hallucis
- Abductor digiti minimi
- Flexor digitorum longus
- Quadratus plantae
- Flexor digiti minimi
Correct Answer: Quadratus plantae
Explanation:
The foot can be divided into nine distinct compartments. A. C alcaneal compartment 1. Quadratus plantae 2. Posterior tibial nerve, artery, and vein 3. Lateral plantar nerve, artery, and vein 4. Medial plantar nerve (variable) *Remember that the calcaneal compartment may communicate with the posterior tibial compartment. B. Interosseiâ (four separate compartments) C . Adductor muscle D. Medial 1. Flexor hallucis 2. Abductor hallucis E. Lateral 1. Abductor digiti minimi 2. Flexor digiti minimi F. Superficial 1. Flexor digitorum brevis 2. Lumbricals (four) 3. Flexor digitorum longus 4. Medial plantar nerve (variable)
Question 8:
Which of the following structures is in the medial compartment of the foot:
Options:
- Abductor digiti minimi
- Flexor digiti minimi
- Abductor hallucis
- Flexor digitorum brevis
- Flexor digitorum longus
Correct Answer: Abductor hallucis
Explanation:
The foot can be divided into nine distinct compartments. A. C alcaneal compartment 1. Quadratus plantae 2. Posterior tibial nerve, artery, and vein 3. Lateral plantar nerve, artery, and vein 4. Medial plantar nerve (variable) *Remember that the calcaneal compartment may communicate with the posterior tibial compartment. B. Interossei (four separate compartments) C . Adductor muscle D. Medial 1. Flexor hallucis 2. Abductor hallucis E. Lateral 1. Abductor digiti minimi 2. Flexor digiti minimi F. Superficial 1. Flexor digitorum brevis 2. Lumbricals (four) 3. Flexor digitorum longus 4. Medial plantar nerve (variable)
Question 9:
Which of the following foot compartments communicates with the deep posterior tibial compartment:
Options:
- Medial
- Lateral
- Adductor
- C alcaneal
- Superficial
Correct Answer: C alcaneal
Explanation:
The foot can be divided into nine distinct compartments. A. C alcaneal compartment 1. Quadratus plantae 2. Posterior tibial nerve, artery, and vein 3. Lateral plantar nerve, artery, and vein 4. Medial plantar nerve (variable) *Remember that the calcaneal compartment may communicate with the posterior tibial compartment. B. Interosseiâ (four separate compartments) C . Adductor muscle D. Medial 1. Flexor hallucis 2. Abductor hallucis E. Lateral 1. Abductor digiti minimi 2. Flexor digiti minimi F. Superficial 1. Flexor digitorum brevis 2. Lumbricals (four) 3. Flexor digitorum longus 4. Medial plantar nerve (variable)
Question 10:
A 45-year-old man has severe, unremitting pain after sustaining a displaced calcaneus fracture. He is immobilized in a bulky compression dressing with plaster splints. After removing his dressing, he is noted to have marked swelling with no resolution of his pain. The next step in management is:
Options:
- Ice and elevation
- Ice, elevation, and an increase in pain medication
- Application of a foot pump
- Epidural block for pain control
- Measurement of the calcaneal compartment tissue pressure
Correct Answer: Measurement of the calcaneal compartment tissue pressure
Explanation:
The patient has the most reliable finding in foot compartment syndromesâ unremitting pain that is out of proportion to injury. When patients have unremitting pain following removal of a compression dressing, the compartment pressures should be measured to determine if a compartment syndrome is present. If the tissue pressure is within 30 mm Hg of the diastolic pressure, the pressures are above 30 mm Hg, and a neurological deficit is present, a compartment syndrome has occurred and the patient should undergo an emergency fasciotomy.
Question 11:
A 45-year-old man has severe, unremitting pain after sustaining a displaced calcaneus fracture. His hindfoot is swollen. The calcaneal compartment tissue pressure is 47 mm Hg. His diastolic pressure is 70 mm Hg. The next step in management is:
Options:
- Ice and elevation
- Ice, elevation, and an increase in pain medication
- Application of a foot pump
- Epidural block for pain control
- Emergent release of the foot compartments
Correct Answer: Emergent release of the foot compartments
Explanation:
The patient has the most reliable finding in foot compartment syndromesâ unremitting pain that is out of proportion to injury. When patients have unremitting pain following removal of a compression dressing, the compartment pressures should be measured to determine if a compartment syndrome is present. If the tissue pressure is within 30 mm Hg of the diastolic pressure, the pressures are above 30 mm Hg, and a neurological deficit is present, a compartment syndrome has occurred and the patient should undergo an emergency fasciotomy.
Question 12:
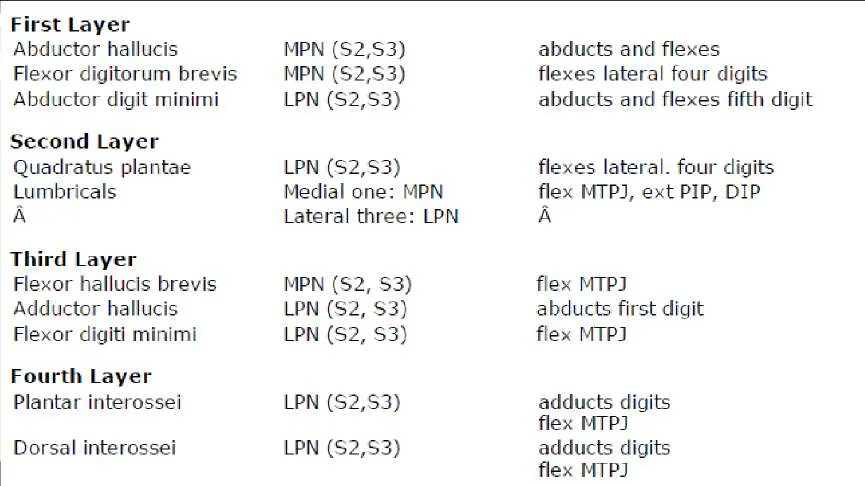
Which of the following groups of muscles are located in the first layer of the foot muscles:
Options:
- Abductor hallucis, flexor digitorum brevis, quadratus plantae
- Flexor hallucis brevis, adductor hallucis, flexor digiti, minimi
- Abductor, hallucis, flexor digitorum brevis, abductor digiti minimi
- Quadratus plantae, lumbricals
- Abductor hallucis, quadratus plantae, lumbricals
Correct Answer: Abductor hallucis, flexor digitorum brevis, quadratus plantae
Explanation:
The muscles of the foot and their innervations are as follows: Abbreviations: MPN=medial plantar nerve, LPN=lateral plantar nerve, MTPJ=metatarsophalangeal joint, PIP=proximal interphalangeal joint, and DIP=distal interphalangeal joint.
Question 13:
Which of the following muscles are in the second layer of the foot:
Options:
- Abductor hallucis, flexor digitorum brevis, abductor digiti minimi
- Abductor hallucis, quadratus plantae
- Flexor hallucis brevis, abductor hallucis, flexor digiti minimi
- Quadratus plantae, lumbricals
- Plantar interossei, dorsal interossei
Correct Answer: Quadratus plantae, lumbricals
Explanation:
The muscles of the foot and their innervations are as follows: Abbreviations: MPN=medial plantar nerve, LPN=lateral plantar nerve, MTPJ=metatarsophalangeal joint, PIP=proximal interphalangeal joint, and DIP=distal interphalangeal joint.
Question 14:
Which of the following groups of muscles are in the third layer of the foot:
Options:
- Abductor hallucis, flexor digitorum brevis, abductor digiti minimi
- Quadratus plantae, lumbricals
- Flexor hallucis brevis, adductor hallucis, flexor digiti minimi
- Flexor hallucis brevis, quadratus plantae, abductor digiti minimi
- Dorsal interossei, plantar interossei
Correct Answer: Flexor hallucis brevis, adductor hallucis, flexor digiti minimi
Explanation:
The muscles of the foot and their innervations are as follows: Abbreviations: MPN=medial plantar nerve, LPN=lateral plantar nerve, MTPJ=metatarsophalangeal joint, PIP=proximal interphalangeal joint, and DIP=distal interphalangeal joint.
Question 15:
Which of the following muscles are innervated by the medial plantar nerve:
Options:
- Abductor digiti minimi
- Adductor hallucis, flexor digitorum brevis
- Abductor hallucis, flexor digitorum brevis, flexor hallucis brevis, medial lumbrical
- Adductor hallucis, flexor digiti minimi, plantar interossei
- Plantar interossei, dorsal interossei
Correct Answer: Abductor hallucis, flexor digitorum brevis, flexor hallucis brevis, medial lumbrical
Explanation:
The muscles of the foot and their innervations are as follows: Abbreviations: MPN=medial plantar nerve, LPN=lateral plantar nerve, MTPJ=metatarsophalangeal joint, PIP=proximal interphalangeal joint, and DIP=distal interphalangeal joint.
Question 16:
Which of the following is true of interdigital neuromas:
Options:
- Interdigital neuromas are a benign neoplasm of the Schwann cell
- Interdigital neuromas most commonly occur in the second web space
- Numbness is a common finding in interdigital neuromas
- Interdigital neuromas most commonly occur in the third web space
- There is an equal incidence of interdigital neuromas in men and women
Correct Answer: Interdigital neuromas are a benign neoplasm of the Schwann cell
Explanation:
Discussion Important core knowledge of interdigital neuroma (Morton's syndrome) includes: A. Etiology-neither a neuroma nor a tumor; most likely degenerative from repetitive trauma from the transverse intermetatarsal ligament. 1. Pathology-most commonly perineural fibrosis B. Most common in the third web space (about 80%) 1. Medial branch of the lateral plantar nerve joins the lateral branch of medial plantar curve C . More common in women than men D. Presentation 1. Paresthesias, dysesthesias, burning sensation 2. Diffuse symptoms in forefoot 3. Pain is relieved by massaging the foot 4. Numbness occurs as a late finding E. Physical examination 1. Tenderness to direct pressure in the web space 2. Tenderness with forefoot compression
Question 17:
Which of the following structures can cause chronic impingement-type posterior ankle pain athletes:
Options:
- Flexor digitorum longus
- Posterior tibialis
- Gastrocnemius soleus complex
- Peroneus longus
- Peroneus quartus
Correct Answer: Peroneus quartus
Explanation:
Discussion Posterior impingent can be caused by anomalous muscles. The most common is the peroneus quartus. Here are some important points. Posterior ankle impingement-compression of the talus and surrounding soft tissues between the tibia and calcaneus A. C ause-forced or repetitive plantar flexion of the foot B. Occurs in dancers and athletes C . Presentation-pain in the medial or lateral aspect of the ankle posteriorly with activities, especially plantar flexion D. Physical examination-tenderness medial or lateral to the Achilles tendon E. Diagnosis is difficult to make and often missed because of the following: 1. Symptoms are reproduced by plantar flexion of the ankle 2. Injections can be performed to see if the injection relieves the symptoms Anomalous muscles about the ankle A. Most common is the peroneus quartus (prevalence of the muscle between 7% and 22%) 1. Arises from peroneus brevis and inserts into retrotrochlear eminence of the calcaneus B. Peroneocalcaneus internus (1%) 1. Arises from the fibula and inserts into under surface of sustentaculum tali C . Long accessory to the long flexors or quadratus plantae (1%-8%) D. Tibiocalcaneus internus E. Accessory soleus
Question 18:
Which of the following may cause impingement-type posterior ankle pain in dancers?
Options:
- Gastrocnemius-soleus complex
- Posterior tibialis
- Peroneus longus
- Peroneus brevis
- Flexor hallucis longus
Correct Answer: Flexor hallucis longus
Explanation:
Discussion Posterior ankle impingement caused by compression of the talus and surrounding soft tissues between the tibia and calcaneus. In dancers, symptoms may be caused by a low lying or enlarged flexor hallucis longus muscle. A. Cause forced or repetitive plantar flexion of the foot B. Occurs in dancers and athletes C . Presentation â pain in the medial or lateral aspect of the ankle posteriorly with activities, especially plantar flexion D. Physical examination â tenderness medial or lateral to the Achilles tendon E. Diagnosis is difficult to make and often missed 1. Symptoms are reproduced by plantar flexion of the ankle 2. Injections can be performed to see if the injection relieves the symptoms Causes of posterior impingement: A. Os trigonum B. Enlarged lateral process of the talus Enlarged posterior process of the calcaneus Posterior intermalleolar ligament Soft tissue impingement Loose bodies Ganglia Low lying flexor hallucis longus muscle body Anomalous muscle bodies
Question 19:
Which of the following statements about the gait cycle is true:
Options:
- The swing phase is longer than the stance phase and lasts for 62% of the cycle.
- From heel rise to toe-off, the tibia goes into external rotation.
- At heel strike, the anterior tibialis muscle is quiescent.
- At toe-off, the gastroc-soleus complex is eccentric contracting.
- From heel strike to toe-off, the transverse tarsal joint unlocks.
Correct Answer: From heel rise to toe-off, the tibia goes into external rotation.
Explanation:
Discussion Because gait cycle questions are common on examinations, remember the following points: Stance phase: 62% of cycle Swing phase: 38% of cycle Muscle firing Electromyography findings during gait cycle: Muscle Activity Heel strike Anterior tibialis Gastroc-soleus Eccentric contraction Quiet Foot flat Anterior tibialis Gastroc-soleus Quiet Eccentric contraction Heel-off Gastroc-soleus C oncentric contraction Toe-off Gastroc-soleus C oncentric contraction Subtalar joint Heel strike to foot flat: Three important points Eversion of the subtalar joint Unlocking of the transverse tarsal joint Internal rotation of the tibia Heel rise to toe-off Inversion of the subtalar joint Locking of the transverse tarsal joint External rotation of the tibia
Question 20:
Which of the following statements describes the subtalar joint during walking:
Options:
- Heel strike to toe-off: Internal rotation of the tibia
- Heel strike to toe-off: Unlocking if transverse tarsal joint
- Heel strike to toe-off: Eversion of the subtalar joint
- Heel rise to toe-off: Eversion of the subtalar joint
- Heel rise to toe-off: Locking of the transverse tarsal joint
Correct Answer: Heel rise to toe-off: Eversion of the subtalar joint
Explanation:
Discussion Because gait cycle questions are common on examinations, remember these points: Stance phase: 62% of cycle Swing phase: 38% of cycle Muscle firing Electromyography findings during gait cycle: Muscle Activity Heel strike Anterior tibialis Gastroc-soleus Eccentric contraction Quiet Foot flat Anterior tibialis Gastroc-soleus Quiet Eccentric contraction Heel-off Gastroc-soleus C oncentric contraction Toe-off Gastroc-soleus C oncentric contraction Subtalar joint Heel strike to foot flat: Three important points Eversion of the subtalar joint Unlocking of the transverse tarsal joint Internal rotation of the tibia Heel rise to toe-off Inversion of the subtalar joint Locking of the transverse tarsal joint External rotation of the tibia
Question 21:
Which of the following tendons is the main inverter of the hind foot:
Options:
- Peroneus longus tendon
- Peroneus brevis tendon
- Flexor hallucis longus tendon
- Flexor digitorum longus tendon
- Posterior tibial tendon
Correct Answer: Posterior tibial tendon
Explanation:
p class="subHeader"> Discussion The posterior tibial tendon is the main inverter of the hindfoot. To conduct a sensitive test for posterior tibial tendon function, ask a patient to perform a single leg rise and observe if the hindfoot inverts. Patients with no posterior tibial tendon function are unable to invert the hindfoot on single leg rise.
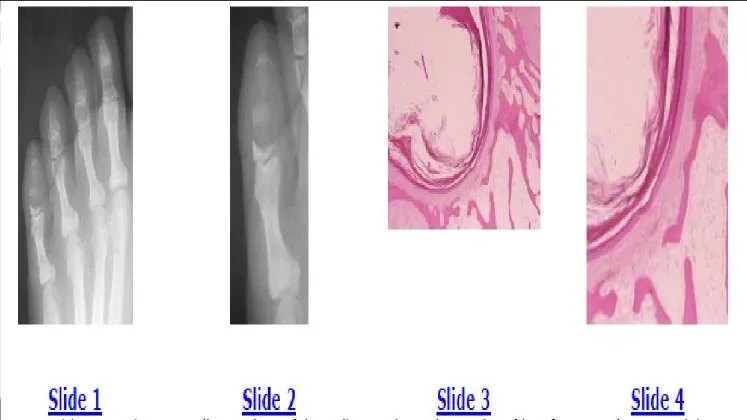
Question 22:
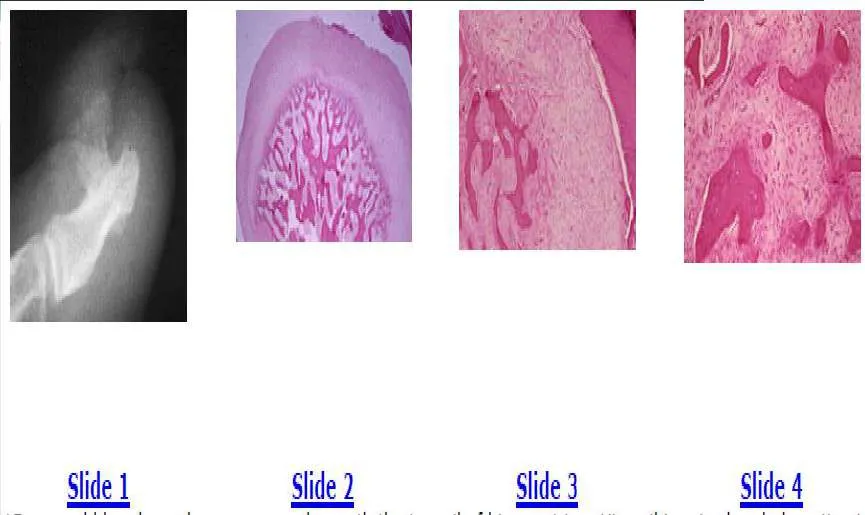
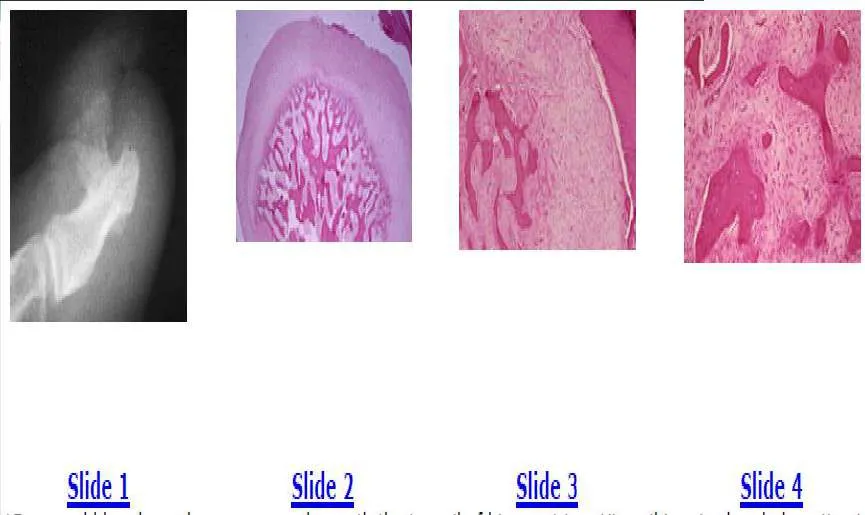
Slide 1 Slide 2 Slide 3 Slide 4 A 35-year-old woman has a swollen and painful small toe. The radiographs of her foot are shown in Slides 1 and 2, and biopsy specimens in Slides 3 and 4. The most likely diagnosis is:
Options:
- Enchondroma
- Plasmacytoma
- C hondromyxoid fibroma
- C hondroblastoma
- Epidermoid inclusion cyst
Correct Answer: Enchondroma
Explanation:
The radiographs show an expansile, lytic destructive lesion, which has replaced the distal and middle phalanxes of the little toe. The biopsy specimen shows the squamous epithelium of the skin with keratin production extending into the medullary cavity of the bone. The patient has an epidermoid inclusion cyst. These cysts are usually secondary to trauma. The treatment should be curettage and grafting.C orrect Answer: Epidermoid inclusion cyst
Question 23:
A 35-year-old woman has a swollen and painful small toe. The radiographs of her foot are shown in Slides 1 and 2, and biopsy specimens are shown in Slides 3 and 4. The most appropriate treatment would be:
Options:
- C urettage with or without grafting
- Toe amputation
- External beam irradiation
- C urettage and external beam irradiation
- Toe amputation and chemotherapy
Correct Answer: C urettage with or without grafting
Explanation:
The radiographs show an expansile, lytic destructive lesion, which has replaced the distal and middle phalanxes of the little toe. The biopsy specimen shows the squamous epithelium of the skin with keratin production extending into the medullary cavity of the bone. The patient has an epidermoid inclusion cyst. These cysts are usually secondary to trauma. The treatment should be curettage and grafting.
Question 24:
Which of the following statements about plantar fasciitis is true:
Options:
- Occurs in men more often than in women
- Bilateral involvement is rare
- Normal thickness of the plantar fascia is 15 mm
- Plantar fascia supports the medial longitudinal arch
- Plantar fascia inserts at the base of the metatarsals
Correct Answer: Plantar fascia supports the medial longitudinal arch
Explanation:
Discussion Plantar fasciitis: General features Most common cause of heel pain Frequently occurs in athletes Men and women affected equally Symptoms are bilateral in 10% of patients C linical findings Pain on the bottom of the heel Pain is worse with first steps in the morning Pain is worse with weight bearing after sitting Pain is worse with activities of daily living Tenderness over the plantar fascia Pain is worsened by dorsiflexion of the toes Plantar fascia Broad, thick structure that originates from the medial calcaneal tuberosity and inserts on the plantar plates of the metatarsalphalangeal joints and proximal phalanges Supports the medial longitudinal arch Although the etiology of plantar fasciitis is not known, one theory is excessive stress on the plantar fascia causes micro tears Biopsies show fibroblastic proliferation and chronic granulomatous tissue The fascia can be as thick as 15 mm (3 mm is normal)
Question 25:
Which of the following statements describes the results of extracorporeal shock wave therapy for chronic plantar fasciitis:
Options:
- No improvement in pain scores occurred at 4 or 12 weeks.
- No improvement in pain scores occurred at 4 weeks, but significant improvement occurred at 12 weeks.
- Pain scores significantly improved at 4 and 12 weeks.
- Pain scores improved, but function did not improve.
- Although pain scores improved, less than 50% of the patients were satisfied.
Correct Answer: Pain scores significantly improved at 4 and 12 weeks.
Explanation:
Discussion In a recent study in Orthopaedics, Furia showed that a significant improvement in pain and function scores occurred in patients who had plantar fasciitis treated with extracorporeal shock wave therapy. Approximately 80% of the patients were satisfied with the treatment and would have the shock wave treatment again. Results Pain Visual Analog Scale (VAS) Pre-treatment VAS 9.2 standard deviation (SD) 0.7 Post-treatment VAS (4 weeks) 3.4 SD 1.9 (P<.05) Post-treatment VAS (12 weeks) 2.4 SD dev 1.8 (P<.05) RAND Score Physical functioning Pre-treatment 40.4 SD 1.3 Post-treatment (4 weeks) 91.5 SD 11.5 (P<.05) Post-treatment (12 weeks) 91.5 SD 10.6 (P<.05) RAND Score Pain Pre-treatment 3.3 SD dev 1.1 Post-treatment (4 weeks) 88.6 SD 16 (P<.05) Post-treatment (12 weeks) 90.0 SD 11.6 (P<.05) Patient satisfaction At 4 and 12 weeks post treatment, 49 (82%) patients were satisfied, and all patients would undergo the procedure again.
Question 26:
A 40-year-old man has pain in his foot after minor trauma. A radiograph is shown in Slide 1 and biopsy specimens are shown in Slides 2 and 3. The most likely diagnosis is:
Options:
- Low-grade chondrosarcoma
- High-grade chondrosarcoma
- Enchondroma
- C hondroblastoma
- C hondromyxoid fibroma
Correct Answer: Enchondroma
Explanation:
The radiograph shows a lucent lesion in the proximal phalanx of the second toe and expansion of the proximal phalanx. The bone is expanded with a thin periosteal rim. Faint calcifications are also seen within the medullary cavity. This radiographic appearance is characteristic of an enchondroma. The low-power hematoxylin and eosin stain shows abundant blue hyaline matrix and a paucity of cells. The high-power hematoxylin and eosin stain shows the small dark and uniform nuclei present in enchondromas. No pleomorphism or nuclear atypia are present.
Question 27:
A 40-year-old man has pain in his foot after minor trauma. A radiograph is shown in Slide 1 and biopsy specimens are shown in Slides 2 and 3. Which of the following would be the most appropriate treatment:
Options:
- Curettage and bone grafting
- Wide resection and allograft reconstruction
- Toe amputation
- External beam irradiation
- C urettage, cement augmentation, and external beam irradiation
Correct Answer: Curettage and bone grafting
Explanation:
The radiograph shows a lucent lesion in the proximal phalanx of the second toe and expansion of the proximal phalanx. The bone is expanded with a thin periosteal rim. Faint calcifications are also seen within the medullary cavity. This radiographic appearance is fairly characteristic of an enchondroma. The low-power hematoxylin and eosin stain shows abundant blue hyaline matrix and a paucity of cells. The high-power hematoxylin and eosin stain shows the small dark and uniform nuclei present in enchondromas. No pleomorphism or nuclear atypia are present.
Question 28:
A 40-year-old man has pain in his foot after minor trauma. A radiograph is shown in Slide 1 and biopsy specimens are shown in Slides 2 and 3. Which of the following best describes this condition:
Options:
- Benign bone tumor
- Low-grade malignant bone tumor
- High-grade malignant bone tumor
- Benign reactive lesion (non-neoplastic)
- Metabolic condition
Correct Answer: Benign bone tumor
Explanation:
The radiograph shows a lucent lesion in the proximal phalanx of the second toe and expansion of the proximal phalanx. The bone is expanded with a thin periosteal rim. Faint calcifications are also seen within the medullary cavity. This radiographic appearance is fairly characteristic of an enchondroma. The low-power hematoxylin and eosin stain shows abundant blue hyaline matrix and a paucity of cells. The high-power hematoxylin and eosin stain shows the small dark and uniform nuclei present in enchondromas. No pleomorphism or nuclear atypia are present.
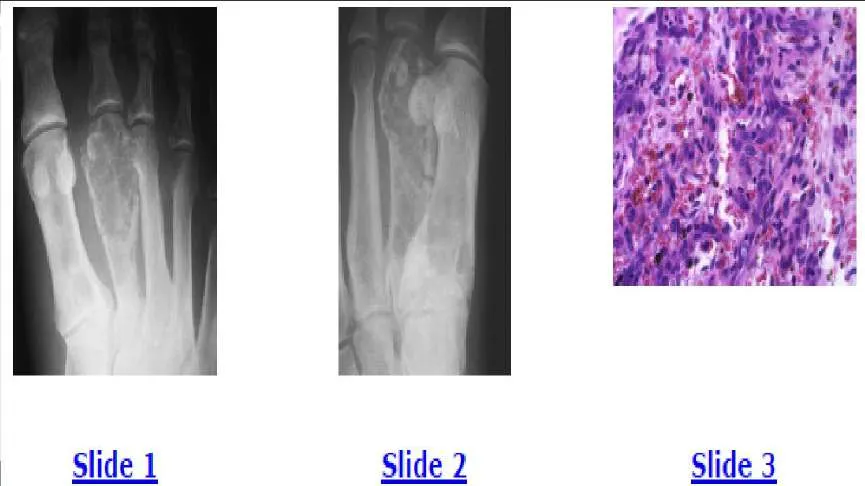
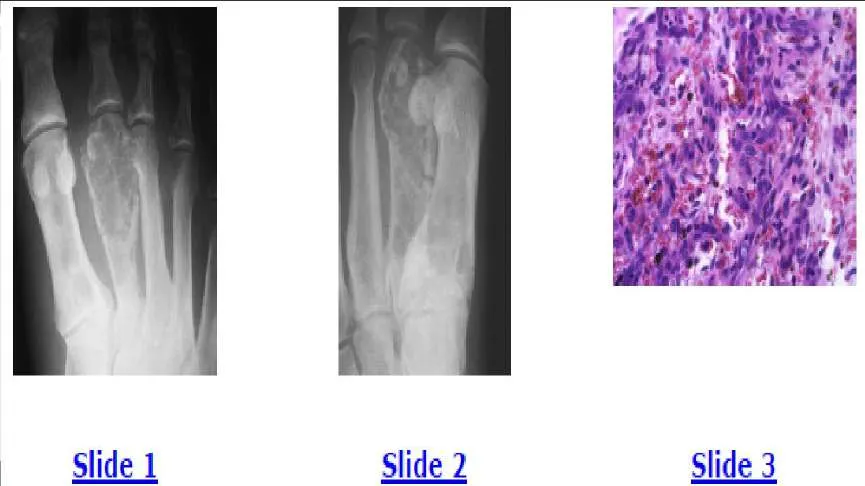
Question 29:
A 35-year-old man has experienced foot pain for 6 months. The anteroposterior and oblique radiographs are shown in Slides 1 and 2, and a biopsy specimen is shown in Slide 3. The most likely diagnosis is:
Options:
- Metastatic adenocarcinoma
- Multiple myeloma
- Eosinophilic granuloma (Langerhans cell histiocytosis)
- Aneursymal bone cyst
- Hemangioendothelioma
Correct Answer: Hemangioendothelioma
Explanation:
The radiographs show lytic destructive lesions in the first and second metatarsals. Malignant vascular tumors, such as hemangioendothelioma, characteristically manifest as multiple lytic lesions in the same extremity in young patients. The biopsy shows vasoformative cells, which are trying to form blood vessels. The correct diagnosis is hemangioendothelioma of bone, which is a low-grade malignancy with a low risk of pulmonary metastases. Patients are typically treated with external beam irradiation. This patient opted for below-knee amputation. He could have also been treated with irradiation.
Question 30:
A 35-year-old man has foot pain for 6 months. The anteroposterior and oblique radiographs are shown in Slides 1 and 2, and a biopsy specimen is shown in Slide 3. Which of the following treatments is the most appropriate:
Options:
- Preoperative chemotherapy and wide resection
- Wide resection and external beam irradiation
- C hemotherapy and external beam irradiation
- Wide resection alone
- External beam irradiation alone
Correct Answer: External beam irradiation alone
Explanation:
The radiographs show lytic destructive lesions in the first and second metatarsals. Malignant vascular tumors, such as hemangioendothelioma, characteristically manifest as multiple lytic lesions in the same extremity in young patients. The biopsy shows vasoformative cells, which are trying to form blood vessels. The correct diagnosis is hemangioendothelioma of bone, which is a
low-grade malignancy with a low risk of pulmonary metastases. Patients are typically treated with external beam irradiation. This patient opted for below-knee amputation. He could have also been treated with irradiation.
Question 31:
A 35-year-old man has foot pain for 6 months. The anteroposterior and oblique radiographs are shown in Slides 1 and 2, and a biopsy specimen is shown in Slide 3. The etiology of this condition is most likely:
Options:
- Benign neoplasm
- Low-grade malignant neoplasm
- High-grade malignant neoplasm
- Post-traumatic
- Infectious
Correct Answer: Low-grade malignant neoplasm
Explanation:
The radiographs show lytic destructive lesions in the first and second metatarsals. Malignant vascular tumors, such as hemangioendothelioma, characteristically manifest as multiple lytic lesions in the same extremity in young patients. The biopsy shows vasoformative cells, which are trying to form blood vessels. The correct diagnosis is hemangioendothelioma of bone, which is a low-grade malignancy with a low risk of pulmonary metastases. Patients are typically treated with external beam irradiation. This patient opted for below-knee amputation. He could have also been treated with irradiation.
Question 32:
Which of the following medications is an effective alternative to intravenous vancomycin for the treatment of severe soft tissue infections caused by methicillin-resistant Staphylococcus aureus (MRSA):
Options:
- C iprofloxacin
- Dicloxacillin
- Linezolid
- Gentamicin
- C lindamycin
Correct Answer: Linezolid
Explanation:
Oral linezolid (600 mg twice a day) is an effective oral alternative to intravenous vancomycin. Below is a summary of a recent prospective, randomized study showing the efficacy of linezolid. Staphylococcus aureus complicates soft tissue and skin infections. Approximately 30% of S aureus infections are methicillinresistant. Although vancomycin has been the treatment of choice for MRSA, linezolid inhibits bacterial protein synthesis by blocking formation of the 70S initiation complex and can be administered orally, which is an advantage over vancomycin. This is a single-center study of adult patients. Investigators randomized 60 patients with S aureus (culture proven) to intravenous vancomycin or oral linezolid. The median length of therapy was 10 days. Seven patients in the vancomycin group required amputation, whereas no amputations were performed in the linezolid group. The median length of hospital stay was shorter in the linezolid group, and outpatient therapy was $100 per day less expensive (approximately $6,500 was saved on the hospital stay). A higher clinical cure rate (94%) was reported with the linezolid group compared to 84% with vancomycin. Linezolid is given orally, 600 mg every 12 hours, and it is well tolerated. No adverse effects were reported in this study. Other studies have had similar results. This is an important study for orthopedic surgeons because the number of patients presenting with MRSA infections is increasing. Athletes may be at an increased risk for the infection because of the potential for spread in locker rooms. This can be a limb-threatening infection and must be taken seriously.
Question 33:
The mechanism of action of linezolid is:
Options:
- Inhibition of cell wall synthesis
- Inhibition of ribonucleic acid synthesis
- Inhibition of deoxyribonucleic acid synthesis
- Inhibition of the 70S initiation complex
- Inhibition of protein prehylation
Correct Answer: Inhibition of cell wall synthesis
Explanation:
Oral linezolid (600 mg twice a day) is an effective oral alternative to intravenous vancomycin. Below is a summary of a recent prospective, randomized study showing the efficacy of linezolid. Staphylococcus aureus complicates soft tissue and skin infections. Approximately 30% of S aureus infections are methicillinresistant. Although vancomycin has been the treatment of choice for methicillin- resistant S aureus (MRSA), linezolid inhibits bacterial protein synthesis by blocking formation of the 70S initiation complex and can be administered orally, which is an advantage over vancomycin. This is a single-center study of adult patients. Investigators randomized 60 patients with S aureus (culture proven) to intravenous vancomycin or oral linezolid. The median length of therapy was 10 days. Seven patients in the vancomycin group required amputation, whereas no amputations were performed in the linezolid group. The median length of hospital stay was shorter in the linezolid group, and outpatient therapy was $100 per day less expensive (approximately $6,500 was saved on the hospital stay). A higher clinical cure rate (94%) was reported with the linezolid group compared to 84% with vancomycin. Linezolid is given orally, 600 mg every 12 hours, and it is well tolerated. No adverse effects were reported in this study. Other studies have had similar results. This is an important study for orthopedic surgeons because the number of patients presenting with MRSA infections is increasing. Athletes may be at an increased risk for the infection because of the potential for spread in locker rooms. This can be a limb-threatening infection and must be taken seriously.
Question 34:
A 25-year-old minor league baseball player has a severe soft tissue infection on the sole of his foot. The infection has not responded to oral cephalexin. There is 4 cm of surrounding erythema and induration, and a small amount of exudate can be expressed. The most likely organism is:
Options:
- Streptococcus
- Staphyloccus aureus
- Methicillin-resistant S aureus (MRSA)
- Corynebacterium
- Enteroccocus
Correct Answer: Methicillin-resistant S aureus (MRSA)
Explanation:
Staphylococcus aureus complicates soft tissue and skin infections. Approximately 30% of S aureus infections are methicillinresistant. Although vancomycin has been the treatment of choice for MRSA, linezolid inhibits bacterial protein synthesis by blocking formation of the 70S initiation complex and can be administered orally, which is an advantage over vancomycin. This is a single-center study of adult patients. Investigators randomized 60 patients with S aureus (culture proven) to intravenous vancomycin or oral linezolid. The median length of therapy was 10 days. Seven patients in the vancomycin group required amputation, whereas no amputations were performed in the linezolid group. The median length of hospital stay was shorter in the linezolid group, and outpatient therapy was $100 per day less expensive (approximately $6,500 was saved on the hospital stay). A higher clinical cure rate (94%) was reported with the linezolid group compared to 84% with vancomycin. Linezolid is given orally, 600 mg every 12 hours, and it is well tolerated. No adverse effects were reported in this study. Other studies have had similar results. This is an important study for orthopedic surgeons because the number of patients presenting with MRSA infections is increasing. Athletes may be at an increased risk for the infection because of the potential for spread in locker rooms. This can be a limb-threatening infection and must be taken seriously.
Question 35:
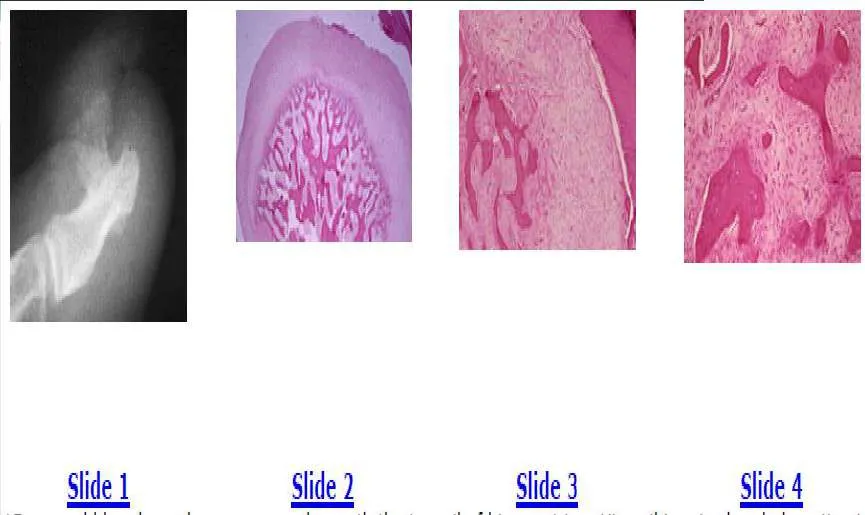
A 15-year-old boy has a large mass underneath the toenail of his great toe. His nail is raised and ulceration is present. The plain radiograph is shown in Slide 1, and biopsy specimens are shown in Slides 2, 3, and 4. The most likely diagnosis is:
Options:
- Low-grade osteosarcoma
- High-grade osteosarcoma
- Fibrosarcoma
- Parosteal osteosarcoma
- Subungual exostosis
Correct Answer: Subungual exostosis
Explanation:
The plain radiograph shows a large bone lesion arising from the dorsal surface of the distal phalanx. This radiographic appearance is characteristic of a subungual exostosis. Osteochondromas do not occur in the distal phalanx, and there is no communication between the lesion and the medullary cavity.
The biopsy specimens show the new bone formation and a fibroblastic stroma, which can be confused with osteosarcoma. The diagnosis is subungual exostosis and the treatment is simple excision.
Question 36:
A 15-year-old boy has a large mass underneath the toenail of his great toe. His nail is raised and ulceration is present. The plain radiograph is shown in Slide 1, and biopsy specimens are shown in Slides 2, 3, and 4. Which of the following is the best form o treatment:
Options:
- Toe amputation
- Preoperative chemotherapy followed by toe amputation
- External beam irradiation
- External beam irradiation and chemotherapy
- Simple excision
Correct Answer: Simple excision
Explanation:
The plain radiograph shows a large bone lesion arising from the dorsal surface of the distal phalanx. This radiographic appearance is characteristic of a subungual exostosis. Osteochondromas do not occur in the distal phalanx, and there is no communication between the lesion and the medullary cavity. The biopsy specimens show the new bone formation and a fibroblastic stroma, which can be confused with osteosarcoma. The diagnosis is subungual exostosis and the treatment is simple excision.
Question 37:
A 15-year-old boy has a large mass underneath the toenail of his great toe. His nail is raised and ulceration is present. The plain radiograph is shown in Slide 1, and biopsy specimens are shown in Slides 2, 3, and 4. Which of the following best describes this condition:
Options:
- Low-grade malignancy
- High-grade malignancy
- Inactive benign neoplasm
- Aggressive benign neoplasm
- Benign reactive condition (non-neoplastic)
Correct Answer: Benign reactive condition (non-neoplastic)
Explanation:
The plain radiograph shows a large bone lesion arising from the dorsal surface of the distal phalanx. This radiographic appearance is characteristic of a subungual exostosis. Osteochondromas do not occur in the distal phalanx, and there is no communication between the lesion and the medullary cavity.
The biopsy specimens show the new bone formation and a fibroblastic stroma, which can be confused with osteosarcoma. The diagnosis is subungual exostosis and the treatment is simple excision.
Question 38:
Deep infection following open reduction internal fixation (ORIF) for tibial pilon fractures is most commonly associated with:
Options:
- Open fractures
- Postoperative wound dehiscence
- Anterior incision
- Medial and lateral plating
- Low energy injury
Correct Answer: Postoperative wound dehiscence
Explanation:
Deep infection following ORIF of pilon fractures is correlated with postoperative wound dehiscence or skin slough but not with the presence of an open fracture in a series of 60 pilon fractures treated by ORIF.
Question 39:
Polyglycolide screws used for fixation of ankle fractures:
Options:
- Are associated with a higher rate of sterile effusion than polylactide screws
- Are associated with a lower rate of sterile effusion than polylactide screws
- Are not associated with sterile effusion
- Provide more rigid fixation than polylactide screws
- Do not resorb over time
Correct Answer: Are associated with a higher rate of sterile effusion than polylactide screws
Explanation:
Polyglycolide screws have a high incidence of sterile effusions as a result of rapid hydrolysis; polylactide screws showed no soft tissue reactions.
Question 40:
The most effective fixation technique that will ensure adequate visualization (imaging) of avascular necrosis changes following talar neck fracture is:
Options:
- Fixation with 0.062-inch K-wires
- C losed reduction
- Fixation with stainless steel mini-fragment screws
- Fixation with titanium screws
- Fixation with a stainless steel locking plate
Correct Answer: Fixation with 0.062-inch K-wires
Explanation:
High-quality magnetic resonance images of the talus can consistently be obtained in the presence of titanium screws in contrast to images obtained with stainless steel implants. Magnetic resonance imaging is better than plain radiographs at assessing the volume of talar avascular necrosis.
Question 41:
Treatment of significant loss of height and posttraumatic arthritis following nonoperative treatment of calcaneus fractures should include:
Options:
- Subtalar distraction bone block arthrodesis
- Corrective osteotomy
- Tibiotalocalcaneal arthrodesis
- Custom Arizona ankle brace with heel lift
- Custom orthotics with lateral heel posting
Correct Answer: Subtalar distraction bone block arthrodesis
Explanation:
Management of late loss of height following calcaneus fracture is best addressed by a distraction arthrodesis of the subtalar joint using a wedge- shaped structural bone graft.
Question 42:
Incisions made through blood-filled fracture blisters have:
Options:
- A lower risk of wound healing problems than clear fluid-filled fracture blisters
- No increased risk of wound healing problems than through normal skin
- The same ability to heal as clear fluid-filled fracture blisters
- A higher risk of wound healing problems than clear fluid-filled fracture blisters
- Should be left open to heal by secondary intention
Correct Answer: A higher risk of wound healing problems than clear fluid-filled fracture blisters
Explanation:
Biopsies of the edge of fracture blisters following ankle fracture show that blood-filled blisters represent a deeper injury than clear fluid-filled blisters. The dermis of clear blisters still showed some epithelial cells remaining, while the dermis of blood blisters showed no epithelial cells. Therefore, blood-filled blisters are more difficult to heal.
Question 43:
The plantar ecchymosis sign is:
Options:
- An indication of possible compartment syndrome
- An indication of possible compartment syndrome
- An indication of possible Lisfranc fracture or sprain
- Described as a sign of plantar fascia rupture
- Requires immediate fasciotomy
Correct Answer: An indication of possible compartment syndrome
Explanation:
The plantar ecchymosis sign is described as an ecchymotic area on the plantar midfoot that is indicative of possible injury to the plantar tarsometatarsal ligaments.
Question 44:
The joint contact area of the second tarsometatarsal joint after Lisfranc dislocation diminishes the greatest with:
Options:
- Dorsolateral subluxation of the second metatarsal
- Dorsal subluxation of the second metatarsal
- Lateral subluxation of the second metatarsal
- Medial subluxation of the second metatarsal
- Plantar subluxation of the second metatarsal
Correct Answer: Dorsolateral subluxation of the second metatarsal
Explanation:
Minor degrees of displacement not apparent on plain radiographs lead to significant decrease in the contact area of the second tarsometatarsal joint. Dorsolateral subluxation of the second tarsometatarsal joint suffers a loss of contact area more severely than pure dorsal or lateral subluxation. Just 3 mm of dorsolateral subluxation causes a 38% loss of contact area.
Question 45:
The â fleck signâ in midfoot injuries is a result of avulsion of the:
Options:
- Lisfranc ligament that extends from the first metatarsal base to the second metatarsal base
- Lisfranc ligament that extends from the middle cuneiform to the first metatarsal base
- Lisfranc ligament that extends from the medial cuneiform to the first metatarsal base
- Lisfranc ligament that extends from the medial cuneiform to the second metatarsal base
- Lisfranc ligament that extends from the lateral cuneiform to the third metatarsal base
Correct Answer: Lisfranc ligament that extends from the first metatarsal base to the second metatarsal base
Explanation:
The fleck sign was described as an avulsion of the ligament that runs from the medial cuneiform to the base of the second metatarsal, the so-called Lisfranc ligament. It is considered pathognomonic for a tarsometatarsal injury.
Question 46:
Delayed unions and nonunions of base of fifth metatarsal fractures have been demonstrated to heal by:
Options:
- Prolonged cast immobilization and non-weight bearing
- Pulsed electromagnetic fields
- C ontinued use of a fracture boot with protected weight- bearing
- Injection of demineralized bone matrix
- Rigid carbon fiber shoe inserts
Correct Answer: Pulsed electromagnetic fields
Explanation:
Nine delayed unions and nonunions of the proximal fifth metatarsal were treated with pulsed electromagnetic fields. All fractures healed in a mean of 4 months (follow-up 39 months, no refractures).
Question 47:
The main blood supply to the talar body is from the:
Options:
- Peroneal artery
- Dorsalis pedis artery
- Artery of the tarsal canal
- Artery of the sinus tarsi
- 1st dorsal metatarsal artery
Correct Answer: Artery of the tarsal canal
Explanation:
The main blood supply to the body of the talus is the artery of the tarsal canal, which is a branch off the posterior tibial artery. The dorsalis pedis and the artery of the sinus tarsi supply the talar head.
Question 48:
The strongest hardware configuration for fixation of talar neck fractures is:
Options:
- Two crossed screws from distal to proximal
- Two parallel screws inserted from distal to proximal
- One large screw from posterior to anterior
- Two parallel screws from posterior to anterior
- One oblique screw from distal to proximal
Correct Answer: Two parallel screws inserted from distal to proximal
Explanation:
Biomechanical cadaveric testing of several screw configurations showed two parallel screws from proximal to distal as the strongest fixation. The screws can be inserted either open or percutaneously. All screw configurations were stronger than K-wire configurations.
Question 49:
The maximal joint reactive force in the ankle is approximately:
Options:
- Two times body weight
- Three times body weight
- Five times body weight
- Seven times body weight
- Eight times body weight
Correct Answer: Five times body weight
Explanation:
Stauffer and colleagues quantified ankle joint reactive force to be approximately 5 times body weight. This is a significant concern for prosthetic ankle arthroplasty because the implant surface area is relatively small over which these forces must be spread out.
Question 50:
According to Sandersâ computed tomography (C T) classification for calcaneus fractures, a Sanders III fracture has:
Options:
- One fracture line in the posterior facet
- Two fracture lines in the posterior facet
- Three fracture lines in the posterior facet
- Four fracture lines in the posterior facet
- Five fracture lines in the posterior facet
Correct Answer: Two fracture lines in the posterior facet
Explanation:
The Sanders C T classification is determined on coronal C T scans of the calcaneus at the level where the posterior facet is widest. A Sanders I is a nondisplaced fracture; Sanders II consists of a single fracture line splitting the posterior facet into two main fragments; Sanders III has two fracture lines with three main posterior facet fragments; and a Sanders IV has four or more articular fragments present.
 The muscles of the foot and their innervations are as follows: Abbreviations: MPN=medial plantar nerve, LPN=lateral plantar nerve, MTPJ=metatarsophalangeal joint, PIP=proximal interphalangeal joint, and DIP=distal interphalangeal joint.
The muscles of the foot and their innervations are as follows: Abbreviations: MPN=medial plantar nerve, LPN=lateral plantar nerve, MTPJ=metatarsophalangeal joint, PIP=proximal interphalangeal joint, and DIP=distal interphalangeal joint.
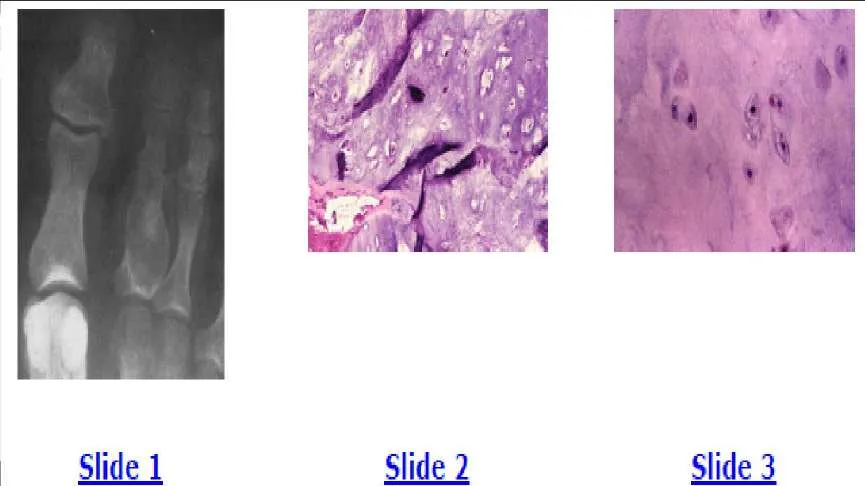
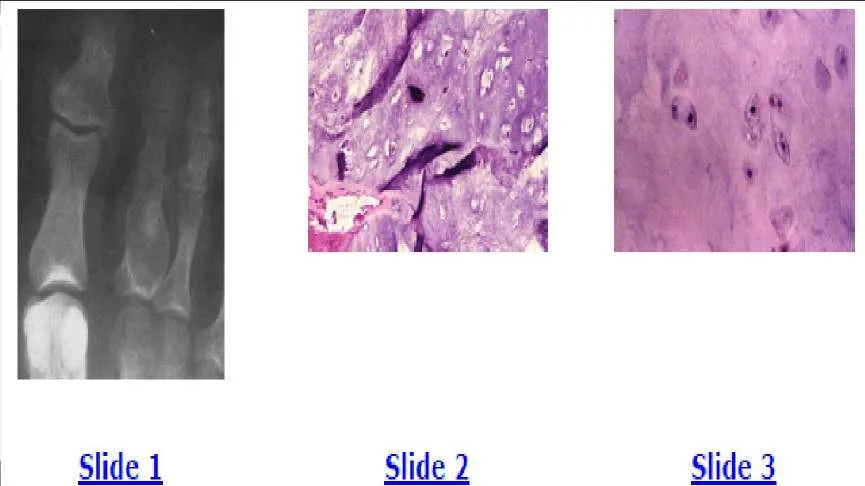 The radiograph shows a lucent lesion in the proximal phalanx of the second toe and expansion of the proximal phalanx. The bone is expanded with a thin periosteal rim. Faint calcifications are also seen within the medullary cavity. This radiographic appearance is fairly characteristic of an enchondroma. The low-power hematoxylin and eosin stain shows abundant blue hyaline matrix and a paucity of cells. The high-power hematoxylin and eosin stain shows the small dark and uniform nuclei present in enchondromas. No pleomorphism or nuclear atypia are present.
The radiograph shows a lucent lesion in the proximal phalanx of the second toe and expansion of the proximal phalanx. The bone is expanded with a thin periosteal rim. Faint calcifications are also seen within the medullary cavity. This radiographic appearance is fairly characteristic of an enchondroma. The low-power hematoxylin and eosin stain shows abundant blue hyaline matrix and a paucity of cells. The high-power hematoxylin and eosin stain shows the small dark and uniform nuclei present in enchondromas. No pleomorphism or nuclear atypia are present.
 low-grade malignancy with a low risk of pulmonary metastases. Patients are typically treated with external beam irradiation. This patient opted for below-knee amputation. He could have also been treated with irradiation.
low-grade malignancy with a low risk of pulmonary metastases. Patients are typically treated with external beam irradiation. This patient opted for below-knee amputation. He could have also been treated with irradiation.
 The biopsy specimens show the new bone formation and a fibroblastic stroma, which can be confused with osteosarcoma. The diagnosis is subungual exostosis and the treatment is simple excision.
The biopsy specimens show the new bone formation and a fibroblastic stroma, which can be confused with osteosarcoma. The diagnosis is subungual exostosis and the treatment is simple excision.
 The biopsy specimens show the new bone formation and a fibroblastic stroma, which can be confused with osteosarcoma. The diagnosis is subungual exostosis and the treatment is simple excision.
The biopsy specimens show the new bone formation and a fibroblastic stroma, which can be confused with osteosarcoma. The diagnosis is subungual exostosis and the treatment is simple excision.