Full Question & Answer Text (for Search Engines)
Question 1:
While he is working, an industrial worker sustains a puncture wound to the plantar aspect of his foot. He suspects the wound was caused by a sharp protruding nail that penetrated his sneaker. The most likely organism to be responsible for a subsequent infection is:
Options:
- Staphylococcus aureus
- Pseudomonas aeruginosa
- Staphylococcus epidermidis
- Streptococcus viridans
- Enterobacter
Correct Answer: Staphylococcus aureus
Explanation:
Although one must be concerned about the possibility of a Pseudomonas infection, the most common organism following puncture injury is staphylococcus aureus. Unless in the setting of diabetes or immune compromise, anaerobic infection rarely occurs.
Question 2:
A 54-year-old woman sustained an injury to her knee 16 months ago. She describes the injury as a dislocation, and she was treated with ligament reconstruction. She has plantarflexion and inversion strength, absent ankle dorsiflexion, and weak eversion. She desires an improvement in the function of the ankle and the ability to comfortably ambulate. The ideal treatment for her is:
Options:
- Ankle arthrodesis in a neutral position
- Intramembranous transfer of the posterior tibial tendon
- Neurolysis of the common peroneal nerve
- Nerve graft of the common peroneal nerve
- Dorsal transfer of the peroneus brevis and longus tendons
Correct Answer: Intramembranous transfer of the posterior tibial tendon
Explanation:
Following peroneal nerve injury, varying degrees of plantarflexion weakness may be present. In the patient with an intact and strong posterior tibial muscle, an intramembranous transfer to the dorsum of the foot may yield positive results with possible active dorsiflexion. Although neurolysis or nerve graft may be considered for selected patients, it is unlikely to yield a satisfactory result at this time following injury.
Question 3:
A 61-year-old man has been treated for type I diabetes for 6 years and presents for evaluation and treatment of an ulcer on the plantar aspect of the forefoot. The ulcer has been present for 4 weeks. The ulcer does not appear infected, claw toe deformities are present, and a posterior tibial pulse is palpable. An important screening test for this patient is:
Options:
- Doppler ultrasound
- 128-MHz tuning fork examination
- C ombined technetium-indium scan
- Semmes-Weinstein monofilament testing
- Transcutaneous oxygen measurements
Correct Answer: Semmes-Weinstein monofilament testing
Explanation:
Although vascular evaluation of all patients with diabetes is important, this patient has a neuropathic plantar ulcer and it is important to assess the extent of neuropathy. The Semmes-Weinstein monofilament is a first-rate screening tool.
Question 4:
The most common complication following medial subtalar dislocation with incarceration of the talus in the extensor brevis muscle is:
Options:
- Avascular necrosis talus
- Ankle arthritis
- Tarsal tunnel syndrome
- Subtalar joint arthritis
- Peroneal tendonitis
Correct Answer: Subtalar joint arthritis
Explanation:
A medial peritalar dislocation is easy to reduce even when the head of the talus is incarcerated in the extensor brevis muscle. Following reduction, stiffness and arthritis of the subtalar joint occurs. Ankle arthritis and tarsal tunnel syndrome may occur following lateral subtalar dislocation.
Question 5:
A patient sustained a fracture of the calcaneus 9 months ago. The fracture was treated with non-weight bearing and cast immobilization. The patient experiences constant pain and is unable to work. On examination, he has limited inversion, eversion motion of the foot, and lateral foot pain. Radiographs are presented. The recommended treatment is:
Options:
- Physical therapy aimed at increasing subtalar joint motion
- Nonsteroidal anti-inflammatory medication and orthotic treatment
- Triple arthrodesis
- Osteotomy of calcaneus and debridement of peroneal tendonitis
- Subtalar arthrodesis
Correct Answer: Subtalar arthrodesis
Explanation:
In the presence of stiffness of the subtalar joint, physical therapy modalities are unlikely to improve the foot function. For the young active worker, an early subtalar arthrodesis is the most reliable procedure to return him to work and an active lifestyle. A triple arthrodesis is contraindicated in the absence of painful transverse tarsal arthritis.
Question 6:
A 44-year-old woman presents with chronic pain in the region of the forefoot. She is unable to wear a shoe with a heel and she has pain in the region of the second toe. On examination, she has swelling of the second toe and painful inflammation of the metatarsophalangeal joint. A clinical picture of her foot is presented. Your initial treatment consists of:
Options:
- Rigid shoe and a toe splint
- C ortisone injection
- Semirigid orthotic support
- Night splinting of the second toe
- Nonsteroidal anti-inflammatory medication and physical therapy treatments
Correct Answer: Rigid shoe and a toe splint
Explanation:
This patient has idiopathic synovitis of the second metatarsophalangeal (MP) joint. This may be associated with hallux valgus or a long second metatarsal, leading to attritional changes in the volar plate and secondary instability of the MP joint. Immobilization of the toe with limitation of dorsiflexion is required. Although cortisone injection may be effective, toe support must be the initial form of treatment.
Question 7:
The most reliable clinical finding of an acute compartment syndrome of the foot is:
Options:
- Absent pulses
- Diminished sensation along the plantar medial foot
- Diminished sensation along the dorsal foot surface
- Marked tense foot swelling and pain
- Pain upon passive dorsiflexion of the toes
Correct Answer: Pain upon passive dorsiflexion of the toes
Explanation:
The most reliable clinical finding of an acute compartment syndrome of the foot is pain upon passive dorsiflexion of the toes. Decreased sensation does not occur commonly and is a late finding, along with changes in perfusion to the foot.
Question 8:
A 9-year-old girl presents for treatment of a calcaneus deformity of the foot that has progressively worsened over the past 3 years. She has a history of poliomyelitis. Upon examination, she has poor plantarflexion, neutral varus and valgus of the hindfoot, and strong dorsiflexion. The preferred treatment for this deformity is:
Options:
- Posterior transfer of the posterior tibial tendon to the fibula
- Posterior transfer of the anterior tibial tendon to the calcaneus
- Posterior transfer of the posterior tibial and peroneal tendons to the calcaneus
- Pantalar arthrodesis
- Ankle arthrodesis in slight plantarflexion
Correct Answer: Posterior transfer of the posterior tibial tendon to the fibula
Explanation:
A calcaneus deformity is ideally treated with posterior transfer of the anterior tibial tendon to the calcaneus. In the presence of calcaneovalgus deformity (which is not present in this child), posterior transfer to the fibula is a better procedure to prevent continued valgus deformity of the ankle.
Question 9:
A 54-year-old woman presents for treatment of leg weakness. She is unable to walk up stairs. She recalls an injury to her ankle while playing tennis 1 year ago. Upon examination, she has poor plantarflexion strength, but excellent dorsiflexion and inversion strength. A magnetic resonance image of her leg is presented. The recommended treatment is:
Options:
- Transfer of the flexor hallucis longus muscle to the calcaneus
- Repair of the Achilles tendon
- Transfer of the anterior tibial tendon to the distal Achilles tendon
- Transfer of the anterior tibial tendon to the calcaneus
- Transfer of the posterior tibial and peroneus brevis tendons to the calcaneus
Correct Answer: Transfer of the flexor hallucis longus muscle to the calcaneus
Explanation:
This patient sustained a rupture of the Achilles tendon that went untreated for 1 year. She has symptomatic weak plantarflexion that may be improved by tendon transfer. Achilles repair is not possible due to the size of the defect. Although transfer of the peroneus brevis muscle or the flexor digitorum longus muscle has been described for correction of plantarflexion weakness, the flexor hallucis longus muscle is stronger and a better transfer.
Question 10:
A 19-year-old collegiate lacrosse player presents for treatment of acute pain along the lateral aspect of the foot. The pain developed during a preseason game 1 week ago. A radiograph is presented. The treatment that will return the athlete to playing competitively with the least likelihood of complications is:
Options:
- Open reduction and internal fixation
- Open reduction and bone grafting
- C ast immobilization and non-weight bearing
- Removable boot immobilization, weight bearing, and pool therapy
- Percutaneous screw fixation
Correct Answer: Percutaneous screw fixation
Explanation:
To rapidly return the competitive athlete to full function, percutaneous screw fixation of an acute fracture or a stress fracture of the fifth metatarsal at the
junction of the metaphysis and diaphysis is preferred treatment. Although nonoperative treatment is associated with fracture healing, the limited function and requirement for immobilization, and possibly limited weight bearing, makes this alternative less appealing in the athlete.
Question 11:
A 19-year-old woman presents for treatment of a painful hallux valgus deformity. In addition to the foot deformity, she has spastic hemiplegic cerebral palsy. A clinical picture of her foot is presented. The recommended treatment is:
Options:
- Distal metatarsal osteotomy
- Proximal metatarsal osteotomy
- Distal metatarsal and proximal hallux phalangeal osteotomy
- Tendon transfer of the adductor hallucis to the abductor hallucis
- Arthrodesis hallux metatarsophalangeal (MP) joint
Correct Answer: Arthrodesis hallux metatarsophalangeal (MP) joint
Explanation:
In patients with spasticity, arthrodesis of the hallux metatarsophalangeal joint is the only reliable means of controlling the hallux and preventing recurrent deformity.
Question 12:
The most common complication of arthrodesis of the proximal interphalangeal (PIP) joint is:
Options:
- Claw toe deformity
- Mallet toe deformity
- Hammer toe deformity
- Curly toe deformity
- Instability of metatarsophalangeal (MP) joint
Correct Answer: Mallet toe deformity
Explanation:
With arthrodesis of the proximal interphalangeal joint (PIP), the long flexor tendon that remains intact flexes the toe at the metatarsophalangeal (MP) joint and also at the distal interphalangeal (DIP) joint, thus the development of a mallet toe deformity.
Question 13:
A 59-year-old woman presents for treatment of a painful hallux valgus deformity. She has a prominent bunion, normal motion of the hallux metatarsophalangeal (MP) joint, and painful callosity under the second MP joint. Radiographs of the foot are presented. The recommended treatment is:
Options:
- Arthrodesis of the hallux MP joint
- Soft tissue release and distal metatarsal osteotomy
- Soft tissue release and proximal metatarsal osteotomy
- Soft tissue release and arthrodesis metatarsocuneiform joint
- Resection arthroplasty of the hallux MP joint
Correct Answer: Arthrodesis of the hallux MP joint
Explanation:
This patient has probable instability of the metatarsocuneiform joint manifested by the overload phenomenon of the second metatarsal. Although this is not a sufficient indication for performing an arthrodesis of the metatarsocuneiform joint (modified Lapidus procedure), other findings of second metatarsal overload, including thickening of the cortex of the second metatarsal and instability of the first metatatarsocuneiform joint, should be looked for in addition to hypermobility of the first ray.
Question 14:
In surgical correction of the adult acquired flatfoot deformity, a medial translational calcaneal osteotomy is often performed in conjunction with additional soft tissue correction medially. One of the proposed biomechanical effects of the osteotomy associated with improvement in the arch of the foot is:
Options:
- Weakening the peroneus brevis tendon
- Tightening the plantar fascia
- Tightening the lateral plantar ligament
- Depression of the first metatarsal axis
- Medial shift of the Achilles tendon
Correct Answer: Medial shift of the Achilles tendon
Explanation:
The medial shift of the calcaneus effectively moves the Achilles tendon, thereby increasing the medial torque on the subtalar joint. The valgus deforming force of the Achilles on the heel is neutralized. The plantar fascia is lengthened, not tightened, by the medial shift of the calcaneus.
Question 15:
One year ago, a patient underwent a triple arthrodesis for management of a severe foot deformity. Although the deformity of her foot is notably improved since the surgery, she has not walked comfortably and the pain is worse than it had been prior to surgery. Upon clinical examination, she is noted to have a fixed supination deformity of the forefoot and callosity under the base of the fifth metatarsal. The recommended management of this problem is:
Options:
- Semirigid orthotic shoe support
- Bracing with a dynamic ankle foot orthoses
- C alcaneal osteotomy
- Excision of the base of the fifth metatarsal
- Revision triple arthrodesis
Correct Answer: Revision triple arthrodesis
Explanation:
This patient underwent a triple arthrodesis that resulted in malunion as demonstrated by the location of the callosity and the fixed forefoot deformity. A calcaneus osteotomy will not correct the midfoot deformity. Nonoperative treatment will not be sufficient in long-term management.
Question 16:
A 28-year-old woman presents for treatment of pain and swelling in the foot. She had twisted her ankle 2 months ago and her initial treatment consisted of limited activity, crutches, and immobilization. Because she has not been able to wean off the crutches, she has pain in the foot radiating to the ankle and distal lateral leg. She has constant pain in the foot and the swelling appears worse than at the time of her injury. C linically, there are multiple areas of tenderness in the foot and ankle that appear swollen and sensitive to examination. The study that would be most helpful to clarify this diagnosis is:
Options:
- Magnetic resonance imaging examination of the ankle
- Weight-bearing radiographs of the ankle and foot
- Ultrasound examination of the ankle ligaments
- Technetium bone scan
- C omputerized axial tomography scan of the ankle and subtalar joint
Correct Answer: Technetium bone scan
Explanation:
This patient appears to have an acute sympathetically mediated pain syndrome. Previously referred to as reflex sympathetic dystrophy, it is essential to make an early diagnosis and initiate treatment. While a lumbar sympathetic block has both diagnostic and therapeutic value, a bone scan is an excellent imaging study for screening and diagnostic purposes in this patient.
Question 17:
A 52-year-old man presents for evaluation and treatment of a painful flatfoot deformity. While playing tennis 2 years ago, he felt a tearing sensation in his foot and ankle. Since that time, he notes that the arch of his foot has become progressively flatter. Upon examination, he has a flatfoot inability to perform a single heel rise and weak inversion strength. He desires to have this deformity corrected. At surgery, the posterior tibial tendon is grossly normal in appearance. The most likely source of his deformity is:
Options:
- Rupture of the Achilles tendon
- Rupture of the peroneus longus tendon
- Rupture of the plantar fascia
- Rupture of the spring ligament
- Rupture of the inferolateral long plantar ligament
Correct Answer: Rupture of the Achilles tendon
Explanation:
A rupture of the spring ligament, the talonavicular capsule, or the deltoid ligament should be looked for in the patient with an acquired flatfoot following trauma. Intratendinous tear of the posterior tibial tendon is also possible.
Question 18:
A 27-year-old man sustained an injury to his foot 2 ½ years ago when a forklift crushed his foot. He sustained a fracture dislocation of the midfoot and was treated with open reduction and internal fixation. His current complaints are burning in the foot associated with numbness over the dorsal foot surface. On examination, he has severe focal sensitivity over the dorsal foot, particularly in the first web space radiating proximally to the ankle. Radiographs demonstrate mild arthritis and anatomic reduction of the tarsometatarsal and midfoot joints. The prognosis for relief of his foot pain at this stage is:
Options:
- Excellent with neuroleptic medication and physical therapy
- Fair regardless of the treatment provided
- Good with treatment for a sympathetically mediated pain syndrome
- Excellent following tarsal tunnel release
- Good with biofeedback and job modification
Correct Answer: Fair regardless of the treatment provided
Explanation:
This patient sustained a crush injury to the foot, and although the dislocation was apparently treated with anatomic reduction, he experiences focal neuritis. It is unlikely that he has a sympathetically mediated pain syndrome, although this should always be considered. The outcome, regardless of treatment, must be guarded for this post-traumatic crush syndrome.
Question 19:
A 34-year-old woman presents for treatment of pain in the hallux. She notes pain upon weight bearing and wearing high-heel shoes. Upon examination, the range of motion of the hallux metatarsophalangeal (MP) joint is 10° dorsiflexion and 30° plantarflexion, with pain upon passive dorsiflexion. Radiographs demonstrate osteophytes over the dorsal surface of the metatarsal head, maintenance of the joint space, and a metatarsal declination angle of 10°. The first metatarsal is elevated above the second metatarsal at the level of the metatarsal neck by 4 mm. The ideal procedure to correct this problem and alleviate pain is:
Options:
- Plantarflexion osteotomy first metatarsal neck
- Plantarflexion osteotomy first metatarsal base
- Dorsiflexion osteotomy first metatarsal neck
- Cheilectomy first metatarsal and dorsiflexion osteotomy hallux proximal phalanx
- Arthrodesis hallux MP joint
Correct Answer: Dorsiflexion osteotomy first metatarsal neck
Explanation:
This patient has mild hallux rigidus with a normal alignment of the first metatarsal. The average elevation of the first metatarsal above the second metatarsal at the level of the metatarsal neck is 7.5 mm, thus, 4 mm is within normal limits. Arthrodesis is not indicated for mild rigidus and osteotomy is indicated only for severe elevation of the first metatarsal. C heilectomy combined with osteotomy of the proximal phalanx (the Moberg osteotomy) is the preferred procedure.
Question 20:
A patient experienced a nondisplaced fracture of the medial and middle cuneiforms. His nonoperative treatment consisted of cast immobilization for 2 weeks with no weight bearing permitted, followed by ambulation as tolerated. He presents for treatment 1 week later with severe swelling in the foot, stiffness of the toes, and limited motion of the hindfoot. The fracture of the cuneiforms appears healed. The ideal management of the stiffness and swelling of the foot is:
Options:
- Application of an intermittent foot pump compression device
- C ontinued cast immobilization and weight bearing as tolerated
- Removable stirrup brace and anti-inflammatory medication
- Deep friction massage combined with acupuncture treatments
- C ast immobilization with frequent changes to monitor swelling
Correct Answer: Application of an intermittent foot pump compression device
Explanation:
Patients who develop swelling of the foot and ankle following trauma and surgery can be effectively treated with application of an intermittent foot pump device. The bladder of the foot pump can be inserted into either a removable boot or cast, or applied to the foot in combination with other methods of rehabilitation. The foot pump is an effective device for decreasing swelling of the foot in association with acute trauma.
Question 21:
A 31-year-old woman presents for treatment of pain in the hallux. She has been experiencing the pain for 2 years. She notes limited motion of the hallux with pain in the joint, particularly when wearing high-heel shoes. She is unable to toe off with running activities. Upon examination, the motion in the hallux metatarsophalangeal (MP) joint is limited in dorsiflexion and radiographs demonstrate mild arthritis of the joint. She requests surgery to correct this disorder. The recommended treatment is:
Options:
- Arthrodesis hallux MP joint
- Plantarflexion osteotomy of the first metatarsal neck
- Plantarflexion osteotomy of the first metatarsal base
- Dorsiflexion osteotomy of the metatarsal neck
- Dorsal cheilectomy metatarsal head
Correct Answer: Dorsal cheilectomy metatarsal head
Explanation:
Cheilectomy is the ideal treatment for correction of mild hallux rigidus. Although elevation of the first metatarsal rarely occurs (metatarsus primus elevatus) as the cause for hallux rigidus, osteotomy of the metatarsal should not be used as the treatment for correction of hallux rigidus with normal alignment of the first metatarsal.
Question 22:
A 17-year-old woman presents for evaluation of a painful hallux valgus deformity. She is unable to wear shoes comfortably, has pain with athletic and daily activities, and notices that the deformity is gradually worsening. Upon clinical examination, she has generalized ligamentous laxity, with motion of the hallux metatarsophalangeal (MP) joint 75° dorsiflexion and 25° plantarflexion. Motion of the first metatarsal is approximately 8° to 10° of combined dorsiflexion and plantarflexion. There is no pain to range of motion of these joints. The hallux valgus angle is 28° and the 1-2 intermetatarsal angle is 12°. The recommended treatment is:
Options:
- Arthrodesis of the first metatarsocuneiform joint (Lapidus)
- Proximal metatarsal osteotomy
- Distal metatarsal osteotomy
- Resection arthroplasty of the MP joint
- Arthrodesis of the hallux MP joint
Correct Answer: Distal metatarsal osteotomy
Explanation:
This adolescent has symptomatic hallux valgus, and surgery is warranted. The motion at the metatarsophalangeal and talometatarsal joints is normal, and there is no evidence of hypermobility despite her generalized ligamentous laxity. Therefore, the modified Lapidus procedure is not indicated. With this deformity, a distal metatarsal osteotomy is ideal.
Question 23:
An 82-year-old woman presents for treatment of a painful second toe deformity. The toe is subluxated at the metatarsophalangeal (MP) joint, and a fixed claw toe deformity is present. Despite severe hallux valgus, and the hallux under riding the second toe, the hallux and bunion are not symptomatic. The procedure that will ideally correct this deformity is:
Options:
- Resection arthroplasty hallux, MP, and proximal interphalangeal joint (PIP) arthroplasty second toe
- Arthrodesis hallux MP joint, MP, and PIP arthroplasty second toe
- Proximal metatarsal osteotomy first metatarsal, MP, and PIP arthroplasty second toe
- Amputation second toe at the MP joint level
- MP and PIP arthroplasty second toe with flexor to extensor tendon transfer
Correct Answer: Amputation second toe at the MP joint level
Explanation:
This elderly patient has a symptomatic second toe deformity only, and surgery to the hallux should be avoided if possible. This is a common clinical problem, and although patients do not readily accept amputation of the toe, it is the preferred procedure because it does not involve reconstruction of the hallux. C orrection of the second toe without amputation will not work unless the hallux deformity is addressed.
Question 24:
A 19-year-old woman had previously been treated for hallux valgus deformity with resection of the medial eminence only. She now presents with severe recurrent deformity of the hallux, with pain. There is neither pain nor crepitus upon range of motion of the hallux metatarsophalangeal (MP) joint. The procedure that will successfully correct the deformity of the hallux and the first metatarsal and maintain motion at the MP joint is:
Options:
- Distal metatarsal osteotomy
- Biplanar distal metatarsal osteotomy
- Arthrodesis of the first talometatarsal joint (modified Lapidus)
- Proximal metatarsal osteotomy
- Double first metatarsal osteotomy
Correct Answer: Double first metatarsal osteotomy
Explanation:
This patient has recurrent hallux valgus with a marked increase in the distal metatarsal articular angle (DMAA). C orrection of this increased DMAA is essential to obtain motion at the metatarsophalangeal joint, and can only be accomplished with a closing wedge type of osteotomy distally. Although a distal biplanar osteotomy may be sufficient, in view of the magnitude of the deformity, a double first metatarsal osteotomy is preferred.
Question 25:
A 63-year-old woman who underwent attempted correction of a hallux valgus deformity 3 years previously presents to the office. She has pain in the hallux from dorsal abutment of the hallux on the shoe. There is no pain in the lesser toes or metatarsals. The recommended procedure to alleviate the irritation of the hallux is:
Options:
- Arthrodesis of the hallux metatarsophalangeal (MP) joint
- Resection arthroplasty of the MP joint (Keller)
- Bone block arthrodesis of the hallux MP joint
- Joint replacement of the hallux MP joint
- Extensor hallucis lengthening
Correct Answer: Extensor hallucis lengthening
Explanation:
This patient had previously undergone resection arthroplasty (Keller) for correction. A common complication of this procedure is a cock-up toe deformity due to insufficiency of the short flexors. This can be corrected with lengthening of the extensor hallucis. If the latter procedure fails, then an arthrodesis can be performed.
Question 26:
A 66-year-old woman has experienced the gradual onset of a flatfoot deformity over the past 10 years. She notes that the condition is bilateral, although worse on one side. Presented are clinical and radiographic images of her condition. This is associated with pain upon ambulation and difficulty with shoe wear. The most likely cause of this flatfoot deformity is:
Options:
- Posterior tibial tendon tear
- Spring ligament tear
- Neuropathy
- Subtalar arthritis
- Tarsometatarsal arthritis
Correct Answer: Tarsometatarsal arthritis
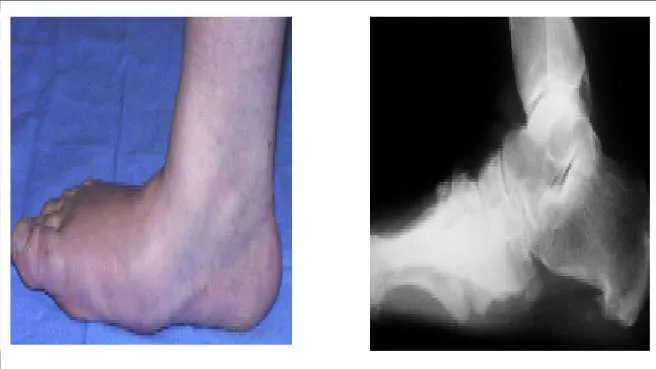
Explanation:
Although posterior tibial tendon insufficiency is a more common cause of adult acquired flatfoot, in this patient the associated clinical and radiographic deformity makes the diagnosis of tarsometatarsal arthritis more likely.
Question 27:
A 66-year-old woman has experienced the gradual onset of a flatfoot deformity over the past 10 years. She notes that the condition is bilateral, although worse on one side. Presented are clinical and radiographic images of her condition. This is associated with pain upon ambulation and difficulty with shoe wear. The most likely cause of this flatfoot deformity is tarsometatarsal arthritis. The initial recommended treatment is:
Options:
- Tarsometatarsal arthrodesis
- Flexor tendon transfer and osteotomy calcaneus
- Triple arthrodesis
- Orthotic arch supports
- C orset type ankle-foot orthosis
Correct Answer: Orthotic arch supports
Explanation:
The initial treatment of idiopathic tarsometatarsal arthritis in the adult is through foot support, shoe modifications, and orthoses. Tarsometatarsal arthrodesis may be required if these treatments fail.
Question 28:
Many materials are used in the production of orthotic arch supports. Plastizote is a material commonly used either alone or in combination. The problem with this material is:
Options:
- It cannot be used in patients with neuropathy.
- It is too hard a material for use with arthritis.
- It is extremely expensive.
- It increases sweating in the foot and is not well tolerated.
- It softens and loses resilience quickly.
Correct Answer: It softens and loses resilience quickly.
Explanation:
Plastizote is a remarkably forgiving material and accommodates well to the foot shape. It is soft, and it loses resilience or sponginess after 6 months. Therefore, plastizote is commonly used in combination with other materials for orthotic support, particularly for the patient with neuropathy.
Question 29:
A 35-year-old man has experienced ankle pain for 7 years. It is associated with giving way and progressive deformity of the foot. He notices that the foot is rolling inward and is becoming flatter. The cause of his condition is:
Options:
- Tarsal coalition
- Subtalar arthritis
- Talonavicular arthritis
- Recurrent ankle sprains
- Rupture spring ligament
Correct Answer: Tarsal coalition
Explanation:
This patient presents with ankle instability and progressively worsening flatfoot, with the hindfoot in valgus. Although a rare condition, this is caused by a talonavicular tarsal coalition, with increasing stress on the ankle likely.
Question 30:
A 14-year-old boy presents for treatment of a painful foot, which has been present for 2 years. He has limited his athletic activities. He has similar symptoms in the opposite foot, although not as severe. On clinical examination, the alignment and appearance of the foot are normal; motion of the foot and ankle is good; and some discomfort is present in the sinus tarsi. Standard radiographs, of which the lateral view is presented, include anteroposterior, lateral, and oblique views. Because the diagnosis is unclear, more imaging studies are required. The next study to obtain is:
Options:
- External oblique views of the foot
- Axial views of the subtalar joint (Harris)
- Oblique views of the subtalar joint (Broden)
- Internal oblique views of the midfoot
- Inclined views of the talonavicular joint (C anale)
Correct Answer: Axial views of the subtalar joint (Harris)
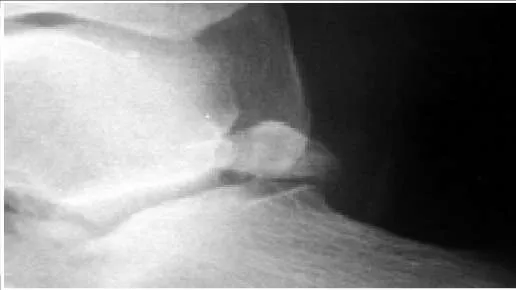
Explanation:
The radiograph demonstrates changes in the subtalar joint suggestive of a middle facet coalition. Note the sclerosis of the joint surface. Although a computed axial tomography scan may be helpful, standard axial views of the subtalar joint (Harris) taken in the plane of the joint are usually diagnostic of tarsal coalition. Motion of the subtalar joint may be normal in the adolescent with a tarsal coalition.
Question 31:
The radiograph of a 22-year-old woman with ankle pain and instability is presented. She has noted this problem for 10 years, and it appears to be worsening. The opposite ankle is not symptomatic. She has not had any previous treatment for foot or ankle problems. The cause of this ankle deformity is most likely to be associated with which of the following conditions:
Options:
- Recurrent ankle instability
- C ongenital bimalleolar dysplasia
- Subtalar fusion
- Talar growth arrest
- Fibular hemimelic syndrome
Correct Answer: Fibular hemimelic syndrome
Explanation:
This patient has a ball and socket ankle, which results from limited motion of the hindfoot during early childhood, either from extensive tarsal coalition, premature hindfoot arthrodesis, or trauma. The condition most commonly associated with a ball and socket ankle is a form of hemimelia of the fibula with lateral ray deficiencies and associated tarsal coalition of which the latter is usually extensive.
Question 32:
The sustentaculum tali is the anatomic roof of which tendon:
Options:
- Posterior tibial
- Flexor digitorum longus
- Flexor digitorum brevis
- Anterior tibial
- Flexor hallucis longus
Correct Answer: Flexor hallucis longus
Explanation:
The sustentaculum tali forms an arch under which the flexor hallucis longus passes. This is of anatomic significance when resecting middle facet tarsal coalition and performing subtalar arthrodesis.
Question 33:
The nerve most likely to be at risk during surgical exposure when performing a triple arthrodesis is the:
Options:
- Sural
- Lateral cutaneous branch superficial peroneal
- Intermediate cutaneous branch superficial peroneal
- Lateral plantar
- Dorsalis pedis
Correct Answer: Sural
Explanation:
The sural nerve has a variable path in the distal leg, but lies immediately adjacent to the peroneal tendons on the lateral side of the foot. The lateral incision used to expose the subtalar and calcaneocuboid joints is adjacent to this nerve.
Question 34:
A 55-year-old man presents for treatment of pain in the Achilles tendon. This has been present for 2 years, but has suddenly become much worse. The pain is approximately 6 cm proximal to the insertion. He is unable to push off during walking and has pain when ascending stairs. C linical examination reveals thickening of the tendon, weakness of the gastrocnemius-soleus, and pain upon squeezing the Achilles tendon. The magnetic resonance image is shown. The diagnosis is:
Options:
- Xanthoma
- Degenerative tendinosis
- C hronic paratendinitis
- Acute rupture
- C hronic rupture
Correct Answer: Degenerative tendinosis
Explanation:
The widening and thickening over a length of the tendon noted clinically and on magnetic resonance image (MRI) is diagnostic of chronic degenerative tendinosis. While paratendinitis may be present simultaneously, limited MRI changes are noted in this condition. Rupture of the tendon may occur and patients with chronic tendinosis should recognize the potential for tendon rupture.
Question 35:
A patient presents for surgical correction of a ruptured Achilles tendon. He recalls injuring his ankle 1 year previously, but did not seek any medical treatment at that time. You plan to repair the tendon, and at surgery, a gap between the tendon ends is noted (Slide). The following procedure is not consistent with an acceptable outcome:
Options:
- V-Y advancement
- Flexor hallucis tendon transfer
- End-to-end repair with the foot positioned in slight equinus
- Flexor digitorum longus tendon transfer
- Fascial turn down flap from musculotendinous junction
Correct Answer: End-to-end repair with the foot positioned in slight equinus
Explanation:
End-to-end repair of a chronic rupture of the Achilles tendon may not be considered if the gap is greater than 2 cm. Equinus positioning is never acceptable. Although each of the other alternatives above may be considered, each has its proponents and potential disadvantages.
Question 36:
You are commencing a repair of an acute rupture of the Achilles tendon that occurred 8 days previously in a 32-year-old recreational tennis player. Fibrillation of the tendon ends is noted. The following is most important to maximize the ultimate outcome of the repair:
Options:
- Resection of the frayed tendon end, and end-to-end apposition
- Incorporation of the plantaris tendon in the repair
- Repair of the tendon with the foot in slight equinus
- Augmentation of the repair with a facial turn down flap
- Repair with the tendon ends at normal resting tension
Correct Answer: Repair with the tendon ends at normal resting tension
Explanation:
Repair of the Achilles tendon at its normal resting length is critical. The frayed tendon ends should not be excised, since this will force a repair with the foot in equinus. The resting tension of the repair can be compared with the position of the opposite limb that should be prepared into the operative field.
Question 37:
A 17-year-old patient presents for evaluation and treatment of pain in the back of her ankle. She is a ballet dancer and has noticed that for the past year, she is unable to assume the pointe position without pain. Upon clinical examination she has full range of motion, excellent strength, normal toe function, and pain with pressure in the posterior ankle. The cause of her pain is:
Options:
- Flexor hallucis longus tendonitis
- Osteochondral defect of the talus
- Anterior tibial tendonitis
- Peroneus longus tendonitis
- Os trigonum syndrome
Correct Answer: Os trigonum syndrome
Explanation:
Posterior ankle impingement is common in ballet dancers. When in the pointe position, maximum plantar flexion of the ankle is present, and pain may occur from impingement in the posterior ankle. Flexor hallucis tendonitis may cause posterior ankle pain, but there is no evidence for this condition here.
Question 38:
The structure that lies immediately medial to the bone prominence in the posterior ankle shown is the:
Options:
- Tibial nerve
- Peroneus longus
- Peroneus brevis
- Posterior tibiofibular ligament
- Flexor hallucis longus
Correct Answer: Flexor hallucis longus
Explanation:
The os trigonum presented in the radiograph may be the cause of posterior ankle impingement. The flexor hallucis longus lies immediately medial to the os and must be protected during excision of this bone.
Question 39:
A 43-year-old construction worker sustained a work-related injury to his foot 7 months ago. He was initially treated with cast immobilization and limited weight bearing. He has lateral foot pain and inability to walk comfortably. He has limited walking endurance. Upon examination, pain is present laterally along the course of the peroneal tendons, and no motion of the subtalar joint is present. The recommendation is:
Options:
- Physical therapy followed by job modification
- Shoe modification and orthotic support
- Nonsteroidal medication, and ankle foot orthoses
- Injection of the peroneal tendons with cortisone
- Subtalar arthrodesis
Correct Answer: Subtalar arthrodesis
Explanation:
A worker who sustains a calcaneus fracture must be returned to the work force as soon as possible. Although these alternatives for treatment may be considered in the patient with limited activity and low demands, the longer the time from injury to salvage surgery with arthrodesis, the less likely it is that the injured worker will ever return to gainful employment. Therefore, subtalar arthrodesis should be performed.
Question 40:
The structure on the side of the metatarsophalangeal joint of the second toe which is marked by the pointer is the:
Options:
- Lumbrical tendon
- Volar plate ligament
- C ollateral ligament
- Interosseous tendon
- Lateral joint capsule
Correct Answer: Volar plate ligament
Explanation:
The structure is the volar plate ligament. This ligament may assume a pathologic role in claw toe deformity and instability of the metatarsophalangeal joint.
Question 41:
A 21-year-old man presents for evaluation of high arches, which have been present his entire life. C urrently, he is experiencing some discomfort with running activities. His brother and mother have high arches. He does not recall any trauma as a child, or any other pertinent childhood musculoskeletal problems. C linical examination reveals a rigid deformity bilaterally. The most common cause for his high arches is:
Options:
- Spina bifida
- Idiopathic cavovarus
- Hereditary sensorimotor neuropathy
- Polio
- Peroneal spastic foot
Correct Answer: Hereditary sensorimotor neuropathy
Explanation:
The most common cause of familial cavovarus foot deformity is hereditary sensorimotor neuropathy (C harcot-Marie-Tooth disease). This is an autosomal dominant condition with variable penetrance. Idiopathic cavus foot is common, but not familial, nor is it associated with this extensive deformity.
Question 42:
A 21-year-old man presents for evaluation of high arches, which have been present his entire life. C urrently, he is experiencing some discomfort with running activities. His brother and mother have high arches. He does not recall any trauma as a child, or any other pertinent childhood musculoskeletal problems. C linical examination reveals a rigid deformity bilaterally. What structure is responsible for plantarflexion of the first metatarsal:
Options:
- Peroneus longus tendon
- Anterior tibial tendon
- Plantar fascia
- Flexor hallucis longus
- Flexor hallucis brevis
Correct Answer: Peroneus longus tendon
Explanation:
The peroneus longus passes under the cuboid to function as a plantar flexor of the first metatarsal. It is a primary deforming force in the development of the cavus foot.
Question 43:
A 22-year-old patient presents for treatment of a painful foot deformity. On examination, a flexible cavovarus deformity is present. The patient has good dorsiflexion foot strength, and eversion strength is weak. A possible tendon transfer that can be used to correct this deformity is:
Options:
- Anterior tibial to middle cuneiform
- Posterior tibial to peroneus longus
- Peroneus longus to peroneus brevis
- Flexor digitorum to posterior tibial
- Posterior tibial to lateral cuneiform
Correct Answer: Peroneus longus to peroneus brevis
Explanation:
Transfer of the strong peroneus longus to the weak peroneus brevis tendon can be considered to improve function and strength of the cavus foot. Posterior tibial tendon transfer is not indicated because dorsiflexion strength is good. Transfer of the anterior tibial tendon is not indicated, although it is contributing to the midfoot varus.
Question 44:
A 56-year-old man presents for treatment of chronic ankle pain. He has noted long-standing pain associated with activities since early adulthood. He does not have any other pertinent musculoskeletal history. C linical and radiographic examinations reveal ankle arthritis. A probable cause for this arthritis and deformity is:
Options:
- Recurrent ankle instability
- Idiopathic osteoarthritis
- Rheumatoid arthritis
- Post traumatic arthritis
- Anterior ankle impingement syndrome
Correct Answer: Recurrent ankle instability
Explanation:
The varus ankle deformity indicates either a chronic hindfoot varus and hindfoot cavus, or chronic recurrent instability of the ankle. If associated with rotatory instability, anterior impingement and eventual arthritis will occur.
Question 45:
When performing fasciotomy of the foot for acute compartment syndrome, the muscle specifically decompressed through medial fasciotomy is:
Options:
- Flexor hallucis brevis
- Quadratus plantae
- Extensor hallucis brevis
- Abductor digiti minimi
- First dorsal interosseous
Correct Answer: Flexor hallucis brevis
Explanation:
Knowledge of the anatomy and pathophysiology of compartment syndrome of the foot is important to plan adequate and correct treatment. The exact number of compartments is not as relevant as the location and ability to decompress the compartment through fasciotomy. The medial compartment contains the abductor hallucis and the flexor hallucis brevis muscles. The quadrates plantae is more posteriorly located and considered to be in a separate calcaneal compartment.
Question 46:
This muscle group demonstrates electrical activity at the time of heel strike:
Options:
- Anterior compartment
- Intrinsic foot muscles
- Lateral compartment
- Deep posterior compartment
- Medial compartment
Correct Answer: Anterior compartment
Explanation:
The anterior muscle compartment, in particular, the anterior tibialis, is active during heel strike, to maintain foot dorsiflexion, and prevent foot drop during heel strike.
Question 47:
A 7-year-old boy presents with bilateral high arches. His parents report that they are having difficulty finding shoes that comfortably fit him. The patient denies any foot pain. The father had similar problems with his feet and was diagnosed with a mild neurologic condition. On exam, the child has bilateral pes cavus with a supple hindfoot. Treatment of the feet at this time should consist of:
Options:
- Soft tissue procedures alone
- Soft tissue procedures and calcaneal osteotomy
- Triple arthrodesis
- Bracing
- Observation
Correct Answer: Soft tissue procedures alone
Explanation:
The child has a supple deformity secondary to C harcot-Marie-Tooth disease that will progress if untreated. Soft tissue procedures, which may consist of claw toe correction, plantar release, and possibly tendon transfer, are recommended for children younger than 8 years old who have a supple hindfoot. The calcaneal osteotomy is reserved for patients with a rigid hindfoot. Triple arthrodesis is a salvage procedure reserved for a fixed, painful foot in older children. Bracing and observation are not preferred options due to the progressive nature of the disease, and the lack of ability to apply corrective forces to the foot in cavus.
Question 48:
A 50-year-old woman presents with pain in the second toe. She describes this as burning and notes swelling of the toe for the past month. Upon examination, there appears to be instability of the toe with a positive dorsal subluxation stress test. The anatomic structure which is responsible for this patientâ s symptoms is:
Options:
- The deep transverse metatarsal ligament
- The second common digital nerve
- The medial collateral ligament of the second metatarsophalangeal joint
- The plantar plate
- The flexor digitorum brevis
Correct Answer: The plantar plate
Explanation:
This patient describes swelling of the toe, which is not associated with an interdigital neuroma. The pain, swelling, and clinical findings suggest a rupture of the plantar plate with early instability and second metatarsophalangeal synovitis.
Question 49:
A 15-year-old boy presents with a 2-year history of pain in the foot associated with a sense stiffness and of giving way of the ankle. Upon examination, pain in the sinus tarsi, slightly decreased subtalar motion, and normal ankle motion with no apparent instability are noted. A lateral foot radiograph is presented. The next radiograph to obtain is:
Options:
- Anteroposterior view of the ankle
- Inversion stress view of the ankle
- Axial view of the hindfoot
- 30° internal oblique view of the foot
- Anteroposterior view of the foot
Correct Answer: Axial view of the hindfoot
Explanation:
This child presents with symptoms suggestive of a tarsal coalition. There is stiffness, and symptoms of ankle discomfort or instability. On the lateral radiograph, there is consolidation of trabeculation under the posterior facet in the shape of a â C â , a typical finding of a middle facet coalition, which should be investigated further with an axial view of the subtalar joint (Harris).
Question 50:
Which ancillary test is not helpful in the diagnosis of C harcot-Marie-Tooth disease (C MT):
Options:
- Electromyography (EMG)
- Nerve conduction velocity (NC V)
- Nerve biopsy
- Muscle biopsy
- Muscle enzymes
Correct Answer: Muscle enzymes
Explanation:
Charcot-Marie-Tooth disease (C MT) is a neuropathic process resulting in muscle atrophy, therefore, muscle enzyme studies will not be helpful. Electromyography (EMG) will confirm the diagnosis by displaying increased amplitude and duration of signals, both of which are indicative of a neuropathic process. Nerve conduction velocity (NC V) will also confirm the diagnosis by displaying decreased motor and sensory conduction velocities. Nerve biopsy can be helpful by showing loss of myelinated fibers and fibrosis. Muscle biopsy will show diffuse atrophy, fibrosis, and adipose tissue within muscle.

 junction of the metaphysis and diaphysis is preferred treatment. Although nonoperative treatment is associated with fracture healing, the limited function and requirement for immobilization, and possibly limited weight bearing, makes this alternative less appealing in the athlete.
junction of the metaphysis and diaphysis is preferred treatment. Although nonoperative treatment is associated with fracture healing, the limited function and requirement for immobilization, and possibly limited weight bearing, makes this alternative less appealing in the athlete.

 The radiograph demonstrates changes in the subtalar joint suggestive of a middle facet coalition. Note the sclerosis of the joint surface. Although a computed axial tomography scan may be helpful, standard axial views of the subtalar joint (Harris) taken in the plane of the joint are usually diagnostic of tarsal coalition. Motion of the subtalar joint may be normal in the adolescent with a tarsal coalition.
The radiograph demonstrates changes in the subtalar joint suggestive of a middle facet coalition. Note the sclerosis of the joint surface. Although a computed axial tomography scan may be helpful, standard axial views of the subtalar joint (Harris) taken in the plane of the joint are usually diagnostic of tarsal coalition. Motion of the subtalar joint may be normal in the adolescent with a tarsal coalition.

 End-to-end repair of a chronic rupture of the Achilles tendon may not be considered if the gap is greater than 2 cm. Equinus positioning is never acceptable. Although each of the other alternatives above may be considered, each has its proponents and potential disadvantages.
End-to-end repair of a chronic rupture of the Achilles tendon may not be considered if the gap is greater than 2 cm. Equinus positioning is never acceptable. Although each of the other alternatives above may be considered, each has its proponents and potential disadvantages.
 Posterior ankle impingement is common in ballet dancers. When in the pointe position, maximum plantar flexion of the ankle is present, and pain may occur from impingement in the posterior ankle. Flexor hallucis tendonitis may cause posterior ankle pain, but there is no evidence for this condition here.
Posterior ankle impingement is common in ballet dancers. When in the pointe position, maximum plantar flexion of the ankle is present, and pain may occur from impingement in the posterior ankle. Flexor hallucis tendonitis may cause posterior ankle pain, but there is no evidence for this condition here.
 A worker who sustains a calcaneus fracture must be returned to the work force as soon as possible. Although these alternatives for treatment may be considered in the patient with limited activity and low demands, the longer the time from injury to salvage surgery with arthrodesis, the less likely it is that the injured worker will ever return to gainful employment. Therefore, subtalar arthrodesis should be performed.
A worker who sustains a calcaneus fracture must be returned to the work force as soon as possible. Although these alternatives for treatment may be considered in the patient with limited activity and low demands, the longer the time from injury to salvage surgery with arthrodesis, the less likely it is that the injured worker will ever return to gainful employment. Therefore, subtalar arthrodesis should be performed.
 The structure is the volar plate ligament. This ligament may assume a pathologic role in claw toe deformity and instability of the metatarsophalangeal joint.
The structure is the volar plate ligament. This ligament may assume a pathologic role in claw toe deformity and instability of the metatarsophalangeal joint.


 This child presents with symptoms suggestive of a tarsal coalition. There is stiffness, and symptoms of ankle discomfort or instability. On the lateral radiograph, there is consolidation of trabeculation under the posterior facet in the shape of a â C â , a typical finding of a middle facet coalition, which should be investigated further with an axial view of the subtalar joint (Harris).
This child presents with symptoms suggestive of a tarsal coalition. There is stiffness, and symptoms of ankle discomfort or instability. On the lateral radiograph, there is consolidation of trabeculation under the posterior facet in the shape of a â C â , a typical finding of a middle facet coalition, which should be investigated further with an axial view of the subtalar joint (Harris).