Full Question & Answer Text (for Search Engines)
Question 1:
Arthroscopic resection/debridement posterior to the midline of the radio- capitellar joint can result in damage to ______ ligament, resulting in ________ instability.
Options:
- Lateral collateral; valgus
- Ulnar collateral; valgus
- Ulnar collateral; posterolateral rotatory
- Annular; posterolateral rotatory
- Lateral collateral; posterolateral rotatory
Correct Answer: Lateral collateral; valgus
Explanation:
Resection posterior to the midpoint of the radiocapitellar joint can result in damage to the lateral collateral ligament and subsequent development of posterolateral rotator instability.
Question 2:
The muscle that flexes the interphalangeal joint of the thumb is innervated by which roots of the brachial plexus:
Options:
- C 5, C 6
- C 5, C 6, C 7
- C 6, C 7, C 8
- C 5, C 6, C 7, C 8, T1
- C 7, C 8, T1
Correct Answer: C 5, C 6
Explanation:
The interphalangeal joint of the thumb is flexed secondary to actions of the flexor pollicis longus (FPL). The FPL is innervated by the anterior interosseous nerve, which is the longest branch of the median nerve. The median nerve is formed by the lateral (roots C 5, C 6, and C 7) and medial (roots C 8 and T1) cords of the brachial plexus.
Question 3:
The anterior interosseous nerve (AIN) originates from the median nerve at what distance from the medial epicondyle:
Options:
- 6 cm distal
- 10 cm proximal
- 6 cm proximal
- 10 cm distal
- At the medial epicondyle
Correct Answer: 6 cm distal
Explanation:
The AIN, the largest branch of the median nerve, originates 5 cm to 8 cm distal to the medial epicondyle from the posteroradial aspect of the median nerve just distal to the proximal border of the superficial head of the pronator teres.
Question 4:
man presents to the emergency department with a 6-week history of difficulty writing and pain after playing tennis. She also reports a recent inability to abduct and adduct her fingers. What is the mechanism of her symptoms:
Options:
- Writers cramp or focal dystonia
- Riche-Cannieu anastamosis
- Martin-Gruber interconnection
- Ulnar neuropathy
- Carpal tunnel syndrome
Correct Answer: Martin-Gruber interconnection
Explanation:
Approximately 17% of the population has a Martin-Gruber interconnection, and 50% of these patients may show additional denervation of normally ulnar nerve-innervated intrinsic muscles. The Martin-Gruber anomaly is a motor neural connection between the anterior interosseous nerve and ulnar nerves that is located adjacent to the ulnar artery in the proximal forearm.
Question 5:
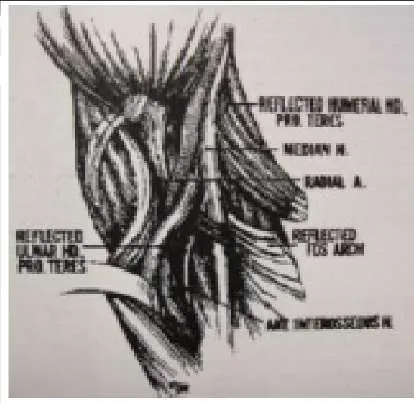
What is the innervation of the indicated muscle in the image (Slide):
Options:
- Median nerve
- Anterior interosseous nerve
- Radial nerve
- Ulnar nerve
- Posterior interosseous nerve
Correct Answer: Median nerve
Explanation:
The arrow in the photograph (Slide) is pointing to the pronator teres â one of the most common sites for compression of the anterior interosseous nerve. The pronator teres is innervated by the median nerve.
Question 6:
Sites of potential compression of the median nerve include all of the following except:
Options:
- Pronator teres
- Transverse carpal ligament
- Pisohamate ligament
- Supracondylar process
- Mass in carpal canal (e.g., lipoma)
Correct Answer: Pisohamate ligament
Explanation:
Around the elbow, the median nerve may be compressed by the pronator teres (causing either anterior interosseous nerve syndrome or pronator syndrome) or the ligament of Struthers originating from a supracondylar process (causing pronator syndrome). In the wrist, the median nerve may be compressed by the transverse carpal ligament or a mass within the carpal canal. The ulnar nerve, not the median nerve, can be compressed by the pisohamate ligament.
Question 7:
What position of the wrist most commonly produces scaphoid fractures:
Options:
- Wrist flexion and radial deviation
- Wrist extension and radial deviation
- Wrist flexion and ulnar deviation
- Wrist extension and ulnar deviation
- C lenched fist and wrist flexion
Correct Answer: Wrist extension and radial deviation
Explanation:
Frykman performed biomechanical studies to evaluate the wrist position in falls that produce scaphoid fractures. The results showed that wrist extension greater than 90° and radial deviation consistently resulted in fracture of the scaphoid.
Question 8:
Which of the following blood vessels supplies the majority of the scaphoid:
Options:
- Superficial palmar branch of the radial artery (volar)
- Radial artery
- Dorsal carpal branch of the radial artery (dorsal)
- Ulnar artery
- 3,4 intracompartmental supra-retinacular artery (3,4-IC SRA)
Correct Answer: Radial artery
Explanation:
Gelberman and Menon used injection studies to demonstrate that the majority of scaphoid blood flow stems from branches of the radial artery entering the scaphoid at the distal pole. Of these, the branch entering the dorsal ridge supplies 70% to 80% of the intraosseous vascularity of the scaphoid bone. The proximal pole is completely dependent on the intraosseous blood supply and is vulnerable to avascular necrosis when fracture disrupts this vascular source.
Question 9:
During a posterior (dorsal) approach to percutaneous screw fixation for a scaphoid fracture, many structures are close to the guidewire insertion location and are at risk for injury. Which of the following structures is the closest to the guidewire insertion location according to a recent cadaveric study:
Options:
- Posterior interosseous nerve
- Extensor digitorum communis to the index
- Extensor indicis proprius
- Extensor carpi radialis brevis
- Extensor digitorum communis to the index and posterior interosseous nerve
Correct Answer: Posterior interosseous nerve
Explanation:
Adamany and colleagues performed a cadaveric study to evaluate the dorsal structures at risk with truly percutaneous headless screw placement for scaphoid fractures. They noted that the posterior interosseous nerve and the extensor digitorum communis to the index finger were an average of 2.2 mm from the guidewire and therefore at greatest risk from this approach.
Question 10:
Which of the following is a concerning risk factor for a dorsal open approach to the scaphoid:
Options:
- Damage to tenous blood supply of the scaphoid
- Difficulty of central screw placement
- Damage to scapho-trapezial-trapezoid joint during the approach
- Damage to the lunatotriquetral (LT) ligament
- njury to the higher rate of infection
Correct Answer: Damage to tenous blood supply of the scaphoid
Explanation:
The dorsal approach is advantageous in obtaining central screw placement. The scapho-trapezial-trapezoid joint is at risk during a volar approach, not a dorsal approach, and infection has not been shown to occur more frequently in one approach over the other. The LT ligament is not seen in either approach. The risk of the open dorsal approach is compromise of the main blood supply to the scaphoid, entering through the dorsal ridge.
Question 11:
A volar approach to the scaphoid is ideal in which of the following fractures:
Options:
- Proximal pole fractures
- Distal pole fractures
- C omminuted scaphoid fractures
- Avascular necrosis of the scaphoid proximal pole
- Scaphoid fracture with associated scapholunate ligament tear
Correct Answer: Distal pole fractures
Explanation:
The volar approach to the scaphoid is optimal in distal pole fractures because it allows direct visualization of the fracture line and exact reduction and fixation. A volar approach is not recommended for fractures or avascular necrosis of the proximal pole, where dorsal screw placement is best. Scapholunate ligament tears are generally repaired from a dorsal approach because the ligament is stoutest dorsally.
Question 12:
Which finger is most commonly involved in a flexor digitorum profundus (FDP) avulsion injury:
Options:
- Index
- Middle
- Ring
- Small
- Thumb
Correct Answer: Ring
Explanation:
An FDP avulsion is caused by forceful extension of the distal interphalangeal (DIP) joint, occurring at the same time as a maximum contraction of the FDP tendon. Jersey finger is often seen in athletes, especially football or rugby players, who commonly get their fingers caught in an opposing playerâ s jersey, thus the name. In most cases, this injury affects the ring finger.
Question 13:
Which type of flexor digitorum profundus (FDP) avulsion is considered the most severe:
Options:
- Type I
- Type II
- Type III
- Type IV
- Type V
Correct Answer: Type I
Explanation:
Type I is the most threatening scenario because the FDP tendon retracts into the palm, and vincular and diffusional blood supply is lost. The sheath may be noncompliant after a few days and may not allow passage of the FDP tendon through the sheath in an attempt to repair the stump to its insertion. Additionally, proximal muscle contracture prevents tendon stump advancement.
Question 14:
When performing pollicization to correct a hypoplastic thumb, the surgeon should rotate the index finger:
Options:
Correct Answer: 150º
Explanation:
After the index finger is rotated 150º, the index finger will be in the ideal location as it mimics the position of where the thumb would have naturally been. This position allows for the greatest amount of grip and pinch strength possible.
Question 15:
For which types of thumb hypoplasia is pollicization the best option:
Options:
- Type I
- Type II
- Type IIIA
- Type IIIB
- Type I, type II, and type IIIA
Correct Answer: Type I
Explanation:
Reconstruction is possible and is therefore the best option for thumb hypoplasia in patients with type I, type II, and type IIIA. These three types of hypoplasia can be corrected because the thumb still has most of the bones and muscles intact. Corrective surgery is necessary to correct weak muscles or a tight web space between the thumb and index finger. When a type IIIB exists, reconstruction is not possible and pollicization must be performed.C orrect Answer: Type I, type II, and type IIIA
Question 16:
What is the most critical step in pollicization to create a normal-looking thumb:
Options:
- Creating skin incisions with skin flaps that will allow a natural first web space
- Shortening of tendons
- Shortening of the index finger metacarpal
- Creating a hyperextended joint when stabilizing the metacarpophalangeal joint to the carpus
- All of the above
Correct Answer: All of the above
Explanation:
It is necessary to create a hand with a natural first web space, shorter tendons that allow for natural movement, a shorter metacarpal that ensures the finger will not grow to an unnatural length, and a hyperextended joint to create the most naturallooking hand possible.
Question 17:
All of the following may be present in a child with type IIIA hypoplasia except:
Options:
- Metacarpophalangeal (MP) joint laxity
- Web space contracture
- Lack of extensor pollicis longus
- Unstable carpometacarpal (C MC ) joint
- Thenar muscle atrophy
Correct Answer: Unstable carpometacarpal (C MC ) joint
Explanation:
Type IIIA hypoplasia includes web space narrowing, thenar atrophy, MP joint laxity, and extrinsic tendon abnormalities. Type IIIA is distinguished from a type IIIB by the fact that a stable C MC joint exists. Because a stable CMC joint exists, a reconstruction is the treatment of choice. When the C MC joint is unstable, as in type IIIB hypoplasia, a pollicization is necessary to restore thumb stability.
Question 18:
The main 3-4 viewing portal for wrist arthroscopy lies in between which two tendons:
Options:
- Extensor pollicis longus (EPL) and extensor carpi radialis brevis (EC RB)
- Extensor digitorum communis (EDC ) and extensor digiti minimi (EDM)
- Abductor pollicis longus (APL) and extensor carpi radialis longus (EC RL)
- EPL and EDC
- Extensor pollicis brevis (EPB) and APL
Correct Answer: EPL and EDC
Explanation:
The 3-4 portal is the main viewing portal and is located between the third and fourth compartment. This portal is bordered by the extensor digitorum communis (EDC ) to the index finger, and the extensor pollicis longus (EPL) can be palpated in the â soft spotâ 1 cm distal to Listers tubercle. This portal is usually the first portal to be made during wrist arthroscopy.
Question 19:
C omplications after wrist arthroscopy occur in what percentage of patients:
Options:
Correct Answer: 5%
Explanation:
The complication rate after routine wrist arthroscopy is between 2% and 5%.
Question 20:
C omplications after wrist arthroscopy occur in what percentage of patients:
Options:
Correct Answer: 5%
Explanation:
The complication rate after routine wrist arthroscopy is between 2% and 5%.
Question 21:
The fracture fragment in Bennettâ s fracture is located in which of the following areas of the hand:
Options:
- Radiopalmar trapezium
- Dorsal thumb metacarpal base
- Ulnopalmar trapezium
- Ulnopalmar thumb metacarpal base
- Radiopalmer lunate
Correct Answer: Radiopalmar trapezium
Explanation:
As an axial load is placed on the thumb tip, it drives the thumb metacarpal (MC ) base in a dorsal-radial direction. As the thumb MC base moves dorsoradially, a fracture is created in the volar, ulnar quadrant of the thumb MC base. Gedda and Moberg describe this as a ligament fracture avulsion. The volar, ulnar quadrant piece usually remains stationary, perhaps migrating a small amount distal the thumb metacarpal base moves dorsoradially, creating a fracture in the volar, ulnar quadrant of the trapezium.C orrect Answer: Ulnopalmar thumb metacarpal base
Question 22:
Which of the following two main soft tissue forces are disrupted by Bennets fracture subluxation:
Options:
- Volar beak (anterior oblique) ligament and extensor pollicis longus
- Volar beak (anterior oblique) ligament and abductor pollicis longus
- Posterior oblique ligament and abductor pollicis brevis
- Dorsal radial ligament and flexor pollicis brevis
- Dorsal radial ligament and abductor pollicis brevis
Correct Answer: Volar beak (anterior oblique) ligament and extensor pollicis longus
Explanation:
The volar, ulnar quadrant piece usually remains stationary due to the volar beak ligament. The thumb metacarpal base tends to sublux dorsoradially due to unopposed pull of the abductor pollicis longus and adductor pollicis. The intact volar beak ligament is usually the counterforce the to these two muscles in the static situation. The extensor pollis longus, flexor pollicis brevis, and abductor pollis longus do not have significant involvement in the Bennettâ s fracture subluxation. Although the dorsal radial ligament is important for carpometacarpal stability, it is not the ligament attached to the fractures fragment.
Question 23:
The greatest amount of step-off that is well-tolerated in a Bennettâ s fracture is:
Options:
- 0 mm
- 1 mm to 2 mm
- 2 mm to 3 mm
- 3 mm to 4 mm
- 4 mm to 5 mm
Correct Answer: 1 mm to 2 mm
Explanation:
Studies by Livesley, Kjaer-Petersen, and others have shown that patients with fractures with more than a 1-mm step-off after reduction were more likely to develop arthritis at the thumb carpometacarpal joint. Although some studies have not shown functional outcome correlating with the presence of arthritis, Oosterbos and De Boer found that all their patients with fair and poor overall results had nonanatomic reductions. Although a cadaveric study by C ullen has shown that a 2-mm step-off may be acceptable, this contrasts with the clinical evidence currently available.
Question 24:
When fracture step-off is greater than the accepted limits, which of the following complications is the most common:
Options:
- Arthritis
- Pain
- Decreased range of motion
- Decreased pinch strength
- All of the above
Correct Answer: All of the above
Explanation:
Studies by Livesley, Kjaer-Petersen, and others have shown that patients with fractures with more than a 1-mm step-off after reduction were more likely to develop arthritis at the thumb carpometacarpal joint. Pain, decreased range of motion, and decreased pinch strength also correlated with these poor outcomes.
Question 25:
C linically, what is the upper limit of acceptable fracture angulation for a fifth metacarpal neck fracture:
Options:
Correct Answer: 70°
Explanation:
Although this is controversial, conservatively treated patients with angulations less than 70° fared well in two prospective studies. Fourteen percent of patients will have a cosmetic deformity, but operatively treated patients exhibited extensor lag and increased rehabilitation times.
Question 26:
In cadaveric models, when does the biomechanics of fifth finger flexion consistently change in relationship to metacarpal neck fracture angulation:
Options:
Correct Answer: 10°
Explanation:
Thirty degrees of angulation is the maximum deformity for acceptable fifth finger grip strength. Ali et al showed that fracture angulation of 30° results in a significant decrease in the distance between the origin and the insertion of the flexor digiti minimi (FDM). This shortening creates more slack in the FDM muscle and more excursion is wasted as muscle shortening prior to the initiation of metacarpophalangeal (MP) flexion.C orrect Answer: 30°
Question 27:
Up to how much angulation can be tolerated in the small finger metacarpal shaft fracture:
Options:
- 0° to 10°
- 11° to 20°
- 21° to 30°
- 31° to 40°
- 41° to 50°
Correct Answer: 41° to 50°
Explanation:
The small finger carpometacarpal joint is mobile, which allows the small finger metacarpal to tolerate deformity better than the fixed index and middle finger rays. Thus, 41° to 50° of angulation can be accommodated by the mobile carpometacarpal joint.
Question 28:
If a metacarpal shaft fracture shortens 4 mm, what will the theoretical amount of extensor lag be at the metacarpophalangeal joint:
Options:
Correct Answer: 14°
Explanation:
For each 2 mm of shortening, a 7° extensor lag exists. Thus, with 4 mm of shortening, there will be a 14° extensor lag at the metacarpophalangeal joint.
Question 29:
In a short oblique metacarpal shaft fracture without comminution or bone loss, what is usual amount of maximal shortening that will occur:
Options:
Correct Answer: 5 mm
Explanation:
In a cadaveric study, shortening beyond 5 mm was prevented by the tethering effect of the transverse metacarpal ligaments and adjacent metacarpals.
Question 30:
Which of the following statements is true regarding metacarpophalangeal joint anatomy:
Options:
- The collateral ligaments are lax in flexion.
- The joint volume is highest in flexion.
- Joint stability is maximal in flexion.
- The metacarpal head is spherical.
- The collateral ligaments originate volar to the axis of flexion.
Correct Answer: Joint stability is maximal in flexion.
Explanation:
The collateral ligaments are lax in extension and tight in flexion. The joint volume is highest in extension. The metacarpal head is cam-shaped. The collateral ligaments originate dorsal to the axis of flexion. Due to the tightening of the collateral ligaments over the cam-shaped metacarpal head in flexion, joint stability is maximized.
Question 31:
Which of the following fracture patterns and mechanisms is incorrectly paired:
Options:
- Transverse fracture-direct blow
- Transverse fracture-axial load on an extended metacarpophalangeal joint
- Comminuted fractures with a butterfly fragment-axial compression and bending
- Spiral fracture-torsion
- Oblique-torsion and axial load
Correct Answer: Transverse fracture-direct blow
Explanation:
Biomechanically and clinically, fracture patterns are often associated with certain types of force. Transverse fractures occur with a direct blow, comminuted fractures occur with axial compression and bending, spiral fractures occur in torsion, and oblique fractures occur with torsion and axial load.
Question 32:
Giant cell tumor of tendon sheath commonly occurs in which of the following age groups:
Options:
- Infants (age 0-1 year)
- Age 1-10 years
- Age 10-20 years
- Age 30-40 years
- Age 60-70 years
Correct Answer: Age 30-40 years
Explanation:
Giant cell tumor of tendon sheath is most commonly found in patients in the fourth through sixth decades; therefore, age 30-40 years is the most appropriate answer choice.
Question 33:
Which of the following clinical features is common in giant cell tumor of tendon sheath:
Options:
- Transillumination
- Erythematous
- Fluctuates in size
- Presents with rapid change in size
- Painless
Correct Answer: Painless
Explanation:
Giant cell tumor of tendon sheath is painless. Giant cell tumor of tendon sheath does not transilluminate, as ganglion cyst does. No overlying skin color changes occur. Giant cell tumor of tendon sheath only increases in size and does not fluctuate like a ganglion cyst; it does not present with a rapid increase in size.
Question 34:
After plain radiographs of giant cell tumor of tendon sheath are obtained, the following imaging study should be obtained:
Options:
- C omputed tomography scan
- Ultrasound
- Magnetic resonance image
- Angiogram
- Bone scan
Correct Answer: Magnetic resonance image
Explanation:
Magnetic resonance imaging provides anatomic detail of the soft tissue mass, helps generate a differential diagnosis, and determines if the mass is unifocal or multifocal and where it originates. Giant cell tumor of tendon sheath is a soft-tissue tumor. Computed tomography is best for bone-based tumors. Ultrasound helps localize lesions but does not provide anatomic detail to help determine the type of mass. Although angiograms are useful for vascular tumors such as renal cell carcinoma or arteriovenous malformations, they are not necessary in the evaluation of a soft tissue mass in the hand with features suggestive of giant cell tumor of tendon sheath. A bone scan is useful when malignant bone tumors are suspected rather than benign soft tissue masses.
Question 35:
Which of the following cell types is not typically found in giant cell tumors of tendon sheath:
Options:
- Multinucleated giant cells
- Histiocytes
- Monocytes
- Polymorphonuclear lymphocytes
- Fibroblasts
Correct Answer: Polymorphonuclear lymphocytes
Explanation:
Multinucleated giant cells, histiocytes, monocytes, and fibroblasts are commonly found in pathologic giant cell tumor of tendon sheath specimens. Polymorphonuclear lymphocytes are typically associated with bacterial infections.
Question 36:
A 25-year-old, right-hand-dominant male truck driver presents to the emergency department (Slide 1, Slide 2). The tip of his left ring finger was amputated in a bicycle accident 2 weeks prior. The amputated piece was â sewn back onâ in the emergency department immediately after the accident, but â turned blackâ over the next week. There is no evidence of infection. He states that the appearance of his finger is embarrassing, and he would like it taken care of as soon as possible. Which of the following procedures is the most appropriate:
Options:
- Local debridement, allow to heal by secondary intention
- Atasoy-Kleinert V-Y advancement flap closure
- Kutler V-Y advancement flap closure
- Moberg flap closure
- Split-thickness hypothenar skin graft
Correct Answer: Atasoy-Kleinert V-Y advancement flap closure
Explanation:
The Atasoy-Kleinert V-Y advancement flap is the best option for transversely oriented fingertip amputations/defects and also for defects with more dorsal than volar tissue loss. The apex of the V is positioned at, or just distal, to the distal interphalangeal join crease on the volar side of the digit. After incising the V marking, the flap is advanced distally to cover the defect, and the incisions are closed in a Y pattern. Local, or chemical, debridement and allowing the resulting defect to heal by secondary intention are a viable option, but the patient stated that he would prefer an aggressive treatment protocol because the appearance of his fingertip is so embarrassing. The Kutler (lateral) V-Y advancement flap is typically used to cover tip defects that demonstrate more volar than dorsal tissue loss. The procedure involves creating V-Y advancement flaps laterally on either side of the affected digit and advancing them toward each other in the midline thereby covering the defect. The Moberg flap is typically used for reconstruction of thumb amputations. This procedure involves the creation of volar tissue flap that includes the neurovascular bundles on either side of the digit. Its use is cautioned in very distal amputations because excess stretch on the vascular pedicles may lead to necrosis at the tip of the flap. Its use is also cautioned in the fingers because of the difference in orientation of the blood supply compared to the thumb. A full-thickness, rather than a split-thickness, skin graft is a viable option to manage this patient. Skin grafts for hand reconstruction should be harvested with the â like replaces likeâ principle in mind, especially when reconstructing the volar skin. Volar hand skin is much thicker and of unique quality when compared with the rest of the body, and therefore, the most appropriate place to harvest a skin graft is the volar surface of the hand.
Question 37:
A 52-year-old, right-hand-dominant watchmaker arrives at the emergency department 30 minutes after the volar soft tissue of his right thumb and index finger was avulsed while using a bandsaw. Physical examination shows 2 cm 3 2 cm wounds involving the distal phalanx of each affected digit. No exposed tendon or bone is present, and no involvement of the joints is noted. The patient requests a treatment option that will retain the most sensation so he can effectively continue in his occupation. Which of the following options is the most appropriate management of this patientâ s wounds:
Options:
- Coverage with cross-finger flaps
- Healing by secondary intention
- Split-thickness skin grafting
- Full-thickness skin grafting
- Radial free forearm flap
Correct Answer: Full-thickness skin grafting
Explanation:
Local flaps such as cross finger flaps are good options but require at least two surgeries (inset then division) and can often result in stiffness secondary to the requisite period of immobilization. In addition, local flaps have lesser return of sensibility than the other techniques listed. Return of tactile sensibility is excellent after healing by secondary intention, but dressing changes for wounds that measure 2 cm 3 2 cm would take months to completely heal. Skin grafting is the next available option with acceptable sensory return. It can be performed during local anesthesia, requires only one operation, and allows for early motion thereby avoiding stiffness. Studies have shown that full-thickness skin grafts recover sensation better than split-thickness skin grafts. A radial forearm flap will be excessively bulky, has unacceptable donor site morbidity in this situation, and results in inadequate sensory recovery.
Question 38:
Which of the following is not considered a part of the triangular fibrocartilage complex:
Options:
- Ulnolunate ligament
- Palmar radioulnar ligament
- Dorsal radioulnar ligament
- Radiolunate ligament
- Ulnotriquetral ligament
Correct Answer: Radiolunate ligament
Explanation:
The triangular fibrocartilage complex is made up of the dorsal and palmar radioulnar ligaments, the meniscal homologue, the articular disk, the ulnolunate, and the ulnotriquetral ligaments. The radiolunate ligament is not part of the complex.
Question 39:
Which of the following arterial branches does not supply the peripheral 25% of the triangular fibrocartilage complex:
Options:
- Dorsal branch of the anterior interosseous artery
- Palmar branch of the anterior interosseous artery
- Dorsal branch of the radial artery
- Dorsal branch of the ulnar artery
- Palmar branch of the ulnar artery
Correct Answer: Dorsal branch of the anterior interosseous artery
Explanation:
The triangular fibrocartilage complex is supplied by both branches of the anterior interosseous artery and the ulnar artery; it is not supplied by the dorsal branch of the radial artery.
Question 40:
Which of the following statements is true:
Options:
- In a wrist with neutral ulnar variance, 20% of the axial load is transmitted across the ulna.
- In a wrist with 2.5 mm ulnar negative variance, 20% of the axial load is transmitted across the ulna.
- In a wrist with 2.5 mm ulnar negative variance, 60% of the axial load is transmitted across the ulna.
- In a wrist with 2.5 mm ulnar positive variance, 600% of the axial load is transmitted across the ulna.
- In a wrist with 2.5 ulnar positive variance, 20% of the axial load is transmitted across the ulna.
Correct Answer: In a wrist with neutral ulnar variance, 20% of the axial load is transmitted across the ulna.
Explanation:
Cadaveric studies have been performed to determine the amount of load across the wrist with various relationships between the radius and ulna lengths. In wrists with neutral ulnar variance (in which the radius and ulna are equal in length), 20% of the load is transmitted across the ulna and 80% is transmitted across the radius. In wrists with negative ulnar variance (in which the ulnar is shorter than the radius), more load is transmitted across the radius and less is transmitted across the ulna. The opposite is true with positive ulnar variance (the ulna is longer than the radius).C orrect Answer: In a wrist with neutral ulnar variance, 20% of the axial load is transmitted across the ulna.
Question 41:
Which of the following parameters is not a determinant of the Palmer classification of triangular fibrocartilaginous complex injuries:
Options:
- Location of the lesion
- Presence of ulnar head chondromalacia
- Presence of lunatotriquetral ligament injury
- Size of the lesion
- Presence of ulnocarpal arthritis
Correct Answer: Size of the lesion
Explanation:
The Palmer classification divides triangular fibrocartilage complex lesions into traumatic and degenerative. Traumatic subclassifications are based on the location of the ligament tear. In the degenerative tear, subclassifications are based on the degree of injury to the triangular fibrocartilage complex and associated chondral and ligamentous injury. Thus, the size of the lesion is not a parameter in the Palmer classification.
Question 42:
What are the components of a Galeazzi fracture-dislocation:
Options:
- Triangular fibrocartilage complex (TFC C ) tear, interosseous membrane tear, and radial shaft fracture
- Ulnar shaft fracture, interosseous membrane tear, and TFC C tear
- Interosseous membrane tear and radial shaft fracture
- TFC C tear and radial shaft fracture
- Wrist radial collateral ligament tear, dorsal intercarpal ligament tear, and ulnar shaft fracture
Correct Answer: Triangular fibrocartilage complex (TFC C ) tear, interosseous membrane tear, and radial shaft fracture
Explanation:
Only one in vitro study examined the soft tissue constraints of the Galeazzi fracture-dislocation pattern. Moore and colleagues performed a radial osteotomy at the pronator teres insertion of nine cadaveric forearms and then sectioned the TFC C and the interosseous membrane in alternating orders. They found that all three structures (TFC C , interosseous membrane, and radialshaft) must be injured to create a radial shortening of more than 10 mm in relationship to the distal ulna.C orrect Answer: Triangular fibrocartilage complex (TFC C ) tear, interosseous membrane tear, and radial shaft fracture
Question 43:
Who are the most common athletes to get medial epicondylitis of the elbow:
Options:
- Tennis players
- Golfers
- Swimmers
- Gymnasts
- Basketball players
Correct Answer: Tennis players
Explanation:
Although medial epicondylitis is called golferâ s elbow, tennis players are more likely to have this condition. Medial epicondylitis can occur in any sport such as baseball pitching, javelin throwing, swimming, and gymnastics in which athletes place a significant valgus flexion force on their elbow.
Question 44:
Indications for replantation include:
Options:
- A crush injury in a patient who smokes
- A sharp amputation of the thumb in a 15-year-old patient
- An ischemia time of 24 hours
- The use of an amputated part that was immersed in warm water for transport
- A single digit amputation proximal to the flexor digitorum superficialis (FDS) insertion
Correct Answer: A sharp amputation of the thumb in a 15-year-old patient
Explanation:
A sharp amputation, particularly of the thumb, is the best indication for replantation. C rushed digits, prolonged ischemia time, poor condition of the severed part, and single digit loss proximal to the FDS insertion on the middle phalanx are relative contraindications to replantation.
Question 45:
An amputation through the wrist is an indication for attempted replantation.
Options:
- True
- False An amputation through the wrist, palm, or forearm is an indication for attempted replantation. The caliber of the vessels and other structures provides a favorable environment for reconstruction. C orrect Answer: True
Correct Answer: True
Question 46:
Care of an amputated part prior to replantation includes:
Options:
- Painting the amputated part with povidone-iodine
- Immersing the amputated part in water
- Placing the amputated part in a warm saline bath
- Wrapping the amputated part with saline-soaked gauze and placing it in a plastic bag on ice
- Putting the amputated part next to the patientâ s body to keep it warm
Correct Answer: Wrapping the amputated part with saline-soaked gauze and placing it in a plastic bag on ice
Explanation:
The appropriate care of an amputated part includes wrapping it in saline- dampened gauze and placing it on ice in a watertight bag. These actions preserve the tissues and slow cellular death until replantation is attempted. The part should not be immersed, painted with povidone- iodine, or kept next to the body.
Question 47:
Replants are monitored by:
Options:
- C olor
- Turgor
- Doppler probes
- Temperature measurements
- All of the above
Correct Answer: All of the above
Explanation:
Monitoring of replanted parts postoperatively is accomplished by clinical checks of color or turgor to indicate blood flow. Additional objective monitoring is performed by using Doppler probes to check flow or by measuring temperature differences between the replanted part as compared to other digits.
Question 48:
C omplications post-replantation include:
Options:
- C old intolerance
- Stiffness
- Excessive laxity of the digit
- A and B only
- All of the above
Correct Answer: A and B only
Explanation:
Complications after replantation include cold intolerance, which may improve over time, and stiffness of the replanted digit, which is generally due to immobility, tendon adhesions, and joint contracture.
Question 49:
Placing some tension on a flexor tendon repair increases the ultimate tensile strength of the repair.
Options:
- True
- False Tension on the repair site of a flexor tendon laceration has been shown experimentally to increase the tensile strength of the repair.
Correct Answer: True
Question 50:
Flexor tendon nutrition is derived from:
Options:
- The vincula
- The pulleys
- Synovial diffusion
- All of the above
- A and C only
Correct Answer: A and C only
Explanation:
Flexor tendon nutrition in the uninjured state is derived via the vincula, which contain blood vessels for nutrition. Injured tendons obtain nutrition via diffusion of synovial fluid. The pulley system does not contribute to flexor tendon nutrition.

 The arrow in the photograph (Slide) is pointing to the pronator teres â one of the most common sites for compression of the anterior interosseous nerve. The pronator teres is innervated by the median nerve.
The arrow in the photograph (Slide) is pointing to the pronator teres â one of the most common sites for compression of the anterior interosseous nerve. The pronator teres is innervated by the median nerve.