Full Question & Answer Text (for Search Engines)
Question 1:
Lateral epicondylitis is associated with a tear in the fibers of which muscle:
Options:
- Extensor carpi radialis brevis (EC RB)
- Extensor carpi radialis longus (EC RL)
- Brachioradialis
- Supinator
- Anconeus
Correct Answer: Extensor carpi radialis brevis (EC RB)
Explanation:
Current consensus is that tennis elbow is associated with a strain or microtear of the EC RB origin, which lies beneath the EC RL.
Question 2:
The gold standard for diagnosis of lateral epicondylitis is considered:
Options:
- History and physical examination
- Plain radiographs
- Electromyography
- Magnetic resonance imaging
- Radionuclear bone scan
Correct Answer: History and physical examination
Explanation:
The clinical diagnosis of lateral epicondylitis is supported by specific provocative tests. The gold standard for diagnosis is the history and physical examination. Tenderness on examination is localized to the lateral epicondyle, which can radiate into the forearm; the area of maximum tenderness is approximately 2 mm to 5 mm distal and anterior to the midpoint of the lateral epicondyle. There is usually a history of overuse or of a repetitive activity. The pain is aggravated, with the elbow extended, by resisted wrist and finger extension or with passive finger and wrist flexion.
Question 3:
The amount of time that nonoperative management should be followed for lateral epicondylitis is closest to:
Options:
- 1 day
- 1 week
- 1 month
- 3 months
- 6 months or longer
Correct Answer: 6 months or longer
Explanation:
Ninety to 95% of all patients with tennis elbow respond to nonoperative treatment, and it remains the mainstay for treatment of lateral epicondylitis. Operative treatment may be indicated for debilitating pain in patients without other pathologic causes of pain for whom nonoperative treatment has failed after a reasonable length of time. This time period is usually a minimum of 6 to 12 months.
Question 4:
Extracorporeal shock wave therapy __________ in the treatment of lateral epicondylitis in high-quality trials.
Options:
- Is ineffective
- Is beneficial
- Has not been tested
- Improves short-term pain
- Improves function
Correct Answer: Is ineffective
Explanation:
Current studies have found no benefit of extracorporeal shock wave therapy in the treatment of lateral epicondylitis.
Question 5:
All of the following medications are indicated in the early treatment of frostbite injury except:
Options:
- Ibuprofen
- Tetanus booster
- Antibiotic prophylaxis
- Narcotic pain medications
- Intravenous beta blocker
Correct Answer: Intravenous beta blocker
Explanation:
Peripheral beta-blockade has minimal effect on peripheral vasculature and is not typically used in patients with frostbite injury. Ibuprofen, tetanus booster, antibiotic prophylaxis, and appropriate pain medication are routinely used in the treatment of frostbite injuries.
Question 6:
Orthopedic sequelae of frostbite injury include all of the following except:
Options:
- Joint contractures
- Localized osteoporosis
- Decreased risk of future frostbite injury
- Punched-out subchondral bony lesions
- C old intolerance
Correct Answer: Decreased risk of future frostbite injury
Explanation:
People who have had previous frostbite injuries are at increased risk of thermal injury, whether cold or heat related. Joint contractures, localized osteoporosis, punched-out subchondral bony lesions, and cold intolerance are often present after frostbite injury.
Question 7:
Initial treatment of an acute frostbite injury should include:
Options:
- Rapid rewarming in circulating 34° C to 36° C water
- Rapid rewarming in circulating 40° C to 42° C water
- Rapid rewarming in steam
- Slow rewarming with intermittent 50° C to 55° C water
- Slow rewarming in room air
Correct Answer: Rapid rewarming in circulating 34° C to 36° C water
Explanation:
Rapid rewarming in a 40° C to 42° C circulating water bath is the most effective early treatment of frostbite injury. Slow or fast rewarming in other temperatures and/or rewarming in air is not indicated.
Question 8:
All of the following except _______ increase the risk of frostbite injury.
Options:
- Altitude higher than 17,000 feet
- History of smoking
- Increased humidity
- Prolonged exposure
- Peripheral vascular disease
Correct Answer: Increased humidity
Explanation:
High altitudes, prolonged exposure, and anything that would cause peripheral vasoconstriction increase the risk of frostbite injury. Humidity does not play a significant role in the development of frostbite injury.
Question 9:
Treatment for frostbite injury includes:
Options:
- Limiting active motion of the frostbitten area
- Elevating the frostbitten extremity to reduce edema
- Stopping the rewarming process when there is pain secondary to reperfusion
- Using dry heat
- Massaging the frostbitten area thoroughly to increase perfusion
Correct Answer: Elevating the frostbitten extremity to reduce edema
Explanation:
Treatment of frostbite includes rapid rewarming (even when reperfusion pain occurs), early active motion, elevation, and avoidance of dry heat that can dessicate tissues. Massaging the frostbitten area is not recommended because it may induce additional trauma via shearing forces.
Question 10:
Arthritis of the wrist is estimated to effect what percentage of the U.S. population:
Options:
- Less than 1%
- 3%
- 5%
- 10%
- More than 15%
Correct Answer: 5%
Explanation:
Arthritis of the wrist is estimated to affect 5.3% of the U.S. population, based on radiographic assessments of 4,000 wrists.1 After having rheumatoid arthritis (RA) for 10 years, 90% of patients experience arthritis in their wrist joints.2
Question 11:
The accessory ulnar collateral ligament inserts on the:
Options:
- Proper ulnar collateral ligament
- Lateral bands
- Proximal phalanx
- Volar plate
- Flexor sheath
Correct Answer: Volar plate
Explanation:
The accessory ulnar collateral ligament inserts into the volar plate, whereas the proper collateral inserts into the base of the proximal phalanx.
Question 12:
Which of the following nerves is not a primary articular nerve of the wrist:
Options:
- Posterior interosseous nerve (PIN)
- Lateral antebrachial cutaneous nerve
- Palmar cutaneous branch of the median nerve
- Articular branches from the median nerve
Correct Answer: Palmar cutaneous branch of the median nerve
Explanation:
Fukumoto and colleagues have used Wykeâ s definition to explain primary and accessory innervation of the wrist. Primary articular nerves consist of small nerves that pass to each joint as independent branches of adjacent peripheral nerves. There are three primary articular nerves: the PIN, the lateral antebrachial cutaneous nerve, and the articular branches from the ulnar nerve. Accessory nerves originate from small, twig branches of intramuscular or cutaneous nerves that innervate the skin around the wrist joint. The accessory articular nerves have been identified as the anterior interosseous nerve (AIN), the palmar cutaneous branch of the median nerve, the deep and dorsal branches of the ulnar nerve, and the superficial branch of the radial nerve to the first intercarpal space.
Question 13:
Which of the following nerves provides principal innervation to the central dorsal portion of the wrist:
Options:
- Anterior interosseous nerve (AIN)
- Posterior interosseous nerve (PIN)
- Dorsal branch of the ulnar nerve
- Lateral antebrachial cutaneous nerve
Correct Answer: Posterior interosseous nerve (PIN)
Explanation:
The PIN is found on the deep radial wall of the fourth dorsal compartment, 1.2 cm ulnar to Listerâ s tubercle. As the PIN approaches the radiocarpal joint, it is covered in fascia and gives one branch to the radioscaphoid joint and three to four terminal branches to the intercarpal joints. The PIN is the principal innervation to the central dorsal portion of the wrist. The AIN innervates the radial volar lip of the distal radius. The dorsal branch of the ulnar nerve contributes to innervation of the triangular fibrocartilage complex. The lateral antebrachial cutaneous nerve innervates the thumb carpometacarpal joint and the scaphotrapezotrapezoid joint.
Question 14:
What is the area of innervation of the anterior interosseous nerve (AIN):
Options:
- Radial volar lip of the distal radius
- Triangular fibrocartilage complex (TFC C )
- Dorsal radiocarpal joint
- Thumb carpometacarpal joint
Correct Answer: Radial volar lip of the distal radius
Explanation:
The AIN is a branch of the median nerve. Its muscular innervations include the flexor pollicis longus, the radial half of the flexor digitorum profundus, and the pronator quadratus. The AIN terminates as a sensory branch to the volar radial surface of the distal radius. The TFC C is innervated by components of the ulnar nerve. The dorsal radiocarpal joint is innervated by the posterior interosseous nerve. The thumb carpometacarpal is innervated by the sensory branch of the radial nerve and the lateral antebrachial cutaneous nerve.
Question 15:
When performing complete wrist denervation as described by Wilhem, what pain pathology did not have predictable results:
Options:
- Scaphoid nonunion
- Osteonecrosis of the scaphoid
- Primary radiocarpal arthritis
- Ulnar carpal arthritis
Correct Answer: Ulnar carpal arthritis
Explanation:
In 1983, Ekerot and colleagues reported his results in 48 patients. They used the technique described by Wilhelm but only denervated the radial side of the wrist for patients with scaphoid or lunate pathology. However, the entire wrist was denervated in patients with global degenerative wrist disease or wrist pain with an unknown etiology. Pain relief occurred in only 56% of the patients. They noted the best results occurred in patients with scaphoid nonunion, osteonecrosis of the lunate, and primary radiocarpal arthritis.
Question 16:
What two nerves are resected through a single dorsal incision for wrist denervation:
Options:
- Superficial branch of the radial nerve and posterior interosseous nerve (PIN)
- PIN and the dorsal cutaneous branch of the ulnar nerve
- PIN and anterior interosseous nerve (AIN)
- Superficial branch of the radial nerve and dorsal cutaneous branch of the ulnar nerve
Correct Answer: PIN and anterior interosseous nerve (AIN)
Explanation:
Kupfer and colleagues presented a podium presentation of a single-incision approach to the resection of the PIN and AIN for denervation of the radial side of the wrist. Weinstein and Berger published their results in 2002 with a similar technique. They described a 2-cm long dorsal incision that was 3 to 5 cm proximal to the ulnar head. They then resected a 2-cm segment of the PIN and AIN. In their group of 20 patients, 85% were satisfied with their procedure after an average follow-up of 2.5 years. If failure were to occur, it occurred within the first year.
Question 17:
What muscle is at risk for denervation when a single dorsal incision is used to denervate the radial side of the wrist:
Options:
- Flexor pollicis longus
- Extensor indicis
- Flexor digitorum profundus
- Pronator quadratus
Correct Answer: Flexor pollicis longus
Explanation:
The single dorsal incision approach to wrist denervation involves resection of the posterior interosseous nerve (PIN) and the anterior interosseous nerve (AIN). Distally, the PIN is purely sensory and does not give off motor branches in the vicinity of the wrist joint. The terminal portion of the AIN has both motor and sensory components. A majority of this is motor, and it innervates the pronator quadratus right up to the radiocarpal articulation. Resection of the AIN close to the radiocarpal joint has a high probability of denervating the pronator quadratus. The extensor indicis is usually the last motor branch of the PIN, but this terminal portion of this branch is more than 5 cm proximal from the distal radioulnar joint. The flexor pollicis longus is innervated by the AIN, but motor branches to this muscle are more proximal than branches to the pronator quadratus. The flexor digitorum profundus muscle is innervated by the AIN and ulnar nerve. However, the motor branches are more proximal than the incision for dorsal innervation. C orrect Answer: Pronator quadratus
Question 18:
A 62-year-old man presents with weakness in finger extension in his right hand. He has had the weakness for 1 month but denies any significant traumatic event. The patient maintains an active lifestyle, including golf and tennis. He denies pain or numbness in his hand and is otherwise neurologically intact. Which of the following is the most likely diagnosis:
Options:
- Thoracic outlet syndrome
- Posterior interosseous nerve palsy
- Ulnar nerve palsy
- C arpal tunnel syndrome
- Radial nerve palsy
Correct Answer: Posterior interosseous nerve palsy
Explanation:
Posterior interosseous nerve palsy is described as painless finger drop. This syndrome is commonly associated with trauma to the lateral elbow.
Question 19:
Which of the following are characteristic signs of PIN palsy:
Options:
- Weakness in finger extension
- Pain in dorsum of hand
- Elbow tenderness
- Weakness in finger extension, and elbow tenderness
- Weakness in finger extension, elbow tenderness, and pain in dorsum of hand
Correct Answer: Weakness in finger extension
Explanation:
Painless finger drop is characteristic of posterior interosseous nerve palsy. This syndrome may also involve elbow tenderness in the absence of other clinical findings. Pain in the dorsum of the hand is not associated with this condition because the posterior interosseous nerve contains no sensory component.
Question 20:
What is the most common site of posterior interosseous nerve entrapment:
Options:
- The arcade of Frohse
- The flexor retinaculum
- The first cervical rib
- In the spiral groove of the humerus
- Ligament of Struthers
Correct Answer: The arcade of Frohse
Explanation:
The most common site of posterior interosseous nerve entrapment is at the arcade of Frohse, which is a fibrotendinous ring found within the fibers of the supinator muscle as the posterior interosseous nerve originates from the radial nerve.
Question 21:
Which of the following muscles is innervated by the posterior interosseous nerve:
Options:
- Extensor carpi ulnaris
- Extensor digiti minimi
- Extensor pollicis brevis and longus
- Abductor pollicis longus
- All of the above
Correct Answer: All of the above
Explanation:
The posterior interosseous nerve innervates a number of muscles involved primarily in finger extension, including the extensor carpi ulnaris, extensor digitorum, extensor digiti minimi, extensor pollicis brevis and longus, abductor pollicis longus, and extensor indices.
Question 22:
Posterior interosseous nerve palsy affects finger extension at the metacarpophalangeal and interphalangeal joints.
Options:
- True
- False Only the metacarpophalangeal joints are involved in posterior interosseous nerve palsy, as the muscles of the interphalangeal joints are innervated by the ulnar and median nerves.
Correct Answer: False Only the metacarpophalangeal joints are involved in posterior interosseous nerve palsy, as the muscles of the interphalangeal joints are innervated by the ulnar and median nerves.
Question 23:
A 53-year-old woman presents with bilateral hand numbness and tingling. Her right hand is more affected than her left. The numbness wakes her up at night and is relieved when she shakes her hand. In addition, the patient has had increasing difficulty with fine motor tasks, such as shirt buttoning, over the past 2 to 3 months. Upon close inspection, muscle atrophy is present at the base of her thumbs. Which of the following is the most likely diagnosis:
Options:
- Thoracic outlet syndrome
- Posterior interosseous nerve palsy
- Ulnar nerve palsy
- Carpal tunnel syndrome
- Radial nerve palsy
Correct Answer: Carpal tunnel syndrome
Explanation:
This patient displays the classic signs and symptoms of bilateral carpal tunnel syndrome, which involves median nerve entrapment at the base of the palm. This entrapment leads to numbness and dysesthesias that are worse at night and upon exertion. Pain is typically relieved by shaking the hand. Furthermore, the median nerve innervates several muscles of the hands, and entrapment may lead to muscle atrophy.
Question 24:
All of the following muscles are innervated by the median nerve except:
Options:
- The ulnar two lumbricals (lumbricals III and IV)
- Opponens pollicis
- Abductor pollicis brevis
- Flexor pollicis brevis
- Flexor digitorum profundus to the middle finger
Correct Answer: The ulnar two lumbricals (lumbricals III and IV)
Explanation:
Lumbricals 1 and 2 are innervated by the median nerve, in addition to the opponens pollicis brevis, abductor pollicis brevis, and flexor pollicis brevis.
Question 25:
All of the following are true regarding the transverse carpal ligament except:
Options:
- The transverse carpal ligament attaches medially to the pisiform and hook of hamate.
- The transverse carpal ligament attaches laterally to the scaphoid and trapezium.
- The palmaris longus tendon lies superficially to the transverse carpal ligament.
- All of the above are true
- None of the above are true
Correct Answer: All of the above are true
Explanation:
All of the above statements are true regarding the transverse carpal ligament.
Question 26:
All of the following structures pass through the carpal tunnel except:
Options:
- Motor branch of the median nerve
- Tendon of the flexor pollicis longus
- Palmar cutaneous branch of median nerve
- Tendon of the flexor digitorum profundus
- Tendon of the flexor digitorum sublimes
Correct Answer: Palmar cutaneous branch of median nerve
Explanation:
The palmar cutaneous branch of the median nerve originates proximally to the carpal tunnel and travels superficial to the tunnel.
Question 27:
Dupuytrenâ s contracture characteristically involves which part of the hand:
Options:
- Ulnar side of the hand
- Thumb
- Radial side of the hand
- Extensor tendons
- Web space between the first and second metacarpals
Correct Answer: Ulnar side of the hand
Explanation:
Dupuytrens contracture most frequently involves the ring and small fingers. Although Dupuytrenâ s cords at the thumb have been described, they are rare.
Question 28:
The use of clostridial collagenase for Dupuytrenâ s contracture is performed by:
Options:
- Injecting collagenase into the affected joint
- Injecting collagenase into the Dupuytrenâ s cord
- Performing a subcutaneous wheal injection of collagenase
- Using a patch of collagenase on the skin
- Applying collagenase to the Dupuytrenâ s cords during surgery
Correct Answer: Injecting collagenase into the affected joint
Explanation:
Clostridial collagenase works by breaking the collagen connections. The Dupuytrenâ s cord is ruptured manually; surgery is not necessary.
Question 29:
Dupuytrens cord tissue is characterized by what change from normal:
Options:
- An increase in type II collagen
- A decrease in type III collagen
- An increase of type III collagen
- Abnormal collagen crosslinks
- Increased hyaluronidase
Correct Answer: An increase in type II collagen
Explanation:
Compared to normal palmar fascia, the fibrous bands in Dupuytrenâ s disease have an increased ratio of type III to type I collagen, and an overall increase in the amount of type III collagen.
Question 30:
A 29-year-old man with a remote history of wrist trauma and chronic pain presents with a palpable clunk on radio-ulnar deviation of the wrist. The most sensitive technique for identifying a scapholunate injury is:
Options:
- Plain radiographs
- Magnetic resonance image (MRI)
- Dynamic cineradiography
- Bone scan
- Arthroscopy
Correct Answer: Arthroscopy
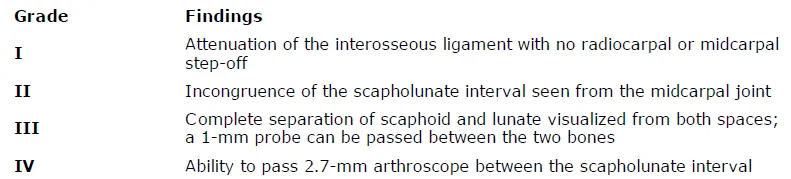
Explanation:
Magnetic resonance imaging is commonly used among patients with concern for ligamentous injuries of the wrist, particularly in the presence of an abnormal physical exam when plain radiographs are normal. However, the sensitivity of MRI has been shown to be less than 40% in comparison with arthroscopy. Arthroscopy has become the gold standard for the diagnosis of ligamentous injuries to the wrist. A classification scheme has been proposed based on both radiocarpal and midcarpal arthroscopic findings.
Question 31:
The radiographic abnormality seen on the lateral radiograph characteristic of scapholunate instability is:
Options:
- Dorsal intercalated segment instability (DISI)
- Volar intercalated segment instability (VISI)
- Terry Thomas sign
- Ring pole sign
- Abnormal Gilulaâ s arcs
Correct Answer: Dorsal intercalated segment instability (DISI)
Explanation:
On a lateral view of the wrist, when the lunate slips into a statically dorsiflexed position greater than 10°, the condition is defined as dorsal intercalated segmental instability (DISI). DISI deformity is also present when the scapholunate angle is greater than 60 degrees (45+/- 15 degrees is normal). The VISI deformity is seen on the lateral radiograph is characteristic of lunotriquetral dissociation. The other signs are seen on the anteroposterior projection.
Question 32:
A 40-year-old woman with radial sided wrist pain for the last 2 years presents to the clinic. Plain radiographs are normal. Because of continued discomfort despite conservative therapies and occasional â clickingâ of the wrist, she is taken to the operating room for diagnostic arthroscopy. At the time, fraying of the membranous portion of the scapholunate (SL) ligament is seen, with mild incongruity from the midcarpal joint. The surgeon is unable to pass a 1-mm probe through the defect. This is most consistent with:
Options:
- Geissler Grade I SL tear
- Geissler Grade II SL tear
- Geissler Grade III tear
- Geissler Grade IV tear
- Scapholunate advanced collapse (SLAC ) wrist
Correct Answer: Geissler Grade I SL tear
Explanation:
Arthroscopy has become the gold standard for the diagnosis of ligamentous injuries to the wrist. A classification scheme has been proposed by Geissler and colleagues, based on both radiocarpal and midcarpal arthroscopic findings (Table). Table. Arthroscopic C lassification of Interosseous Ligament Injury
Question 33:
A 33-year-old woman with a history of a traumatic fall onto her wrist and tenderness over the scapholunate (SL) interval presents to the clinic. Radiographs are normal, and magnetic resonance imaging reveals a partial tear of the SL ligament. The remaining wrist ligaments are normal. If conservative therapy is attempted, then it should consist of:
Options:
- Short arm casting for 2 months
- Activity modification and wrist extension stretching
- Splinting and flexor carpi radialis training
- Splinting and flexor carpi ulnaris training
- C orticosteroid injection into the midcarpal space
Correct Answer: Splinting and flexor carpi radialis training
Explanation:
Conservative management includes a period of splinting and activity modification, followed by proprioception training of the flexor carpi radialis to act as a dynamic scaphoid stabilizer.
Question 34:
Congenital thumb duplication:
Options:
- Should be treated after 2 years of age
- Usually presents bilaterally
- Usually presents in association with other systemic abnormalities
- Often presents with a hypoplastic radial thumb and a dominant-appearing ulnar thumb
- Occurs in approximately 1 out of every 5,000 births
Correct Answer: Often presents with a hypoplastic radial thumb and a dominant-appearing ulnar thumb
Explanation:
Experts recommend treating congenital thumb duplication before the age of 6 months, when the potential for growth and remodeling is greatest. The condition usually presents unilaterally, lacking association with other systemic abnormalities, and usually presents with a hypoplastic radial duplicate and dominant ulnar duplicate.
Question 35:
Complete bifurcation of two distal phalanges articulating with a wide epiphysis of a single proximal phalanx is classified as:
Options:
- Wassel II / IP
- Wassel III / IP
- Wassel IV / MC P
- Wassel IV / IP
- Wassel I/ Distal
Correct Answer: Wassel II / IP
Explanation:
Wassel II (also categorized as IP in the universal classification system) occurs when the duplication begins at the interphalangeal joint of the thumb, resulting in complete bifurcation of two distal phalanges that articulate proximally with a single proximal phalanx.
Question 36:
One of the more common complications of congenital thumb duplication reconstruction is:
Options:
- Weakness of resulting digit
- Paresthesias in resulting digit
- Ulnar deviation at metacarpophalangeal joint and radial deviation at interphalangeal joint
- Nonhealing wound
- Nail splitting
Correct Answer: Ulnar deviation at metacarpophalangeal joint and radial deviation at interphalangeal joint
Explanation:
A Z-deformity, with ulnar deviation at the MC P joint and radial deviation at the IP joint, is one of the most common complications after reconstruction. Weakness, paresthesias, and wound complications are uncommon possible complications.
Question 37:
Ultrasound therapy delivers superficial heat to the tissue and has a penetration depth of 5 mm.
Options:
- True
- False Ultrasound is considered a deep heat modality and does not heat the superficial tissues.
Correct Answer: False Ultrasound is considered a deep heat modality and does not heat the superficial tissues.
Question 38:
Thermal ultrasound is used for all of the following purposes EXC EPT:
Options:
- Increasing capsular extensibility
- Decreasing scar
- Increasing pain threshold
- Reversing Dupuytrenâ s contracture
- Increasing ligament stretch ability
Correct Answer: Reversing Dupuytrenâ s contracture
Explanation:
Thermal uses of ultrasound include increasing pain threshold, decreasing scar, and improving extensibility of the ligaments and joint capsule. Ultrasound has not been shown to have an effect in Dupuytrenâ s contracture.
Question 39:
Phonopheresis is:
Options:
- Delivery of heat to the tissues with a special oval-shaped attachment
- Aspiration of blood with concentration of platelets for re-injection
- Delivery of medicine through the skin using ultrasound
- Using ultrasound in a rapid, deep massage-type application
- Delivery of substimulus auditory waves to the tissue
Correct Answer: Delivery of heat to the tissues with a special oval-shaped attachment
Explanation:
Phonopheresis is delivery of medicine through the skin using ultrasound. Although there is some question as to whether the medications are more effectively absorbed or delivered with ultrasound use, this is a described modality.
Question 40:
Iontophoresis delivers medications such as analgesics or steroids through the skin using an electrical charge.
Options:
- True
- False Iontophoresis uses a direct or galvanic current to drive medications transdermally and is used for scar management and pain control.
Correct Answer: True
Question 41:
Iontophoresis has been effectively used in all of the following EXC EPT:
Options:
- C arpal tunnel syndrome
- Wrist arthritis
- Shoulder/rotator cuff tendinitis
- Lateral epicondylitis
- Medial epicondylitis
Correct Answer: Wrist arthritis
Explanation:
Iontophoresis is effective in soft tissue conditions such as rotator cuff bursitis and lateral epicondylitis.
Question 42:
Types of nerve tissues surrounding the axons include all of the following EXC EPT:
Options:
- Endoneurium
- Hyponeurium
- Perineurium
- Mesoneurium
- Epineurium
Correct Answer: Hyponeurium
Explanation:
The structures surrounding the axons and Schwann cells include the endoneurium, perineurium, and epineurium. The mesoneurium is an adventitial layer in addition.
Question 43:
The Seddon grades of nerve injury include all of the following EXC EPT:
Options:
- Neuropraxia
- Axonotmesis
- Neurotmesis
- Schwann cell disruption
Correct Answer: Schwann cell disruption
Explanation:
Neuropraxic injuries are stretch injuries to the nerve. Axonotmetic injury involves a more severe injury with loss of continuity of axons, and connective tissue elements remain intact. Neurotmesis is a complete nerve discontinuity. Schwann cell disruption occurs in neurotmesis but is not among the grades of Seddon nerve injury.
Question 44:
Younger age is associated with worse outcomes with nerve repair.
Options:
- True
- False Younger age is associated with improved functional outcome after nerve repair, particularly regarding sensory recovery.
Correct Answer: False Younger age is associated with improved functional outcome after nerve repair, particularly regarding sensory recovery.
Question 45:
Optimum conditions for nerve healing after direct repair include:
Options:
- Gapping at suture repair site
- Tension-free repair
- Early motion of extremity
- Preservation of all tissue whether devitalized or viable
- lacing sutures through the endoneurium to increase repair strength
Correct Answer: Tension-free repair
Explanation:
Tension-free repair is the optimal technique to improve the potential for nerve recovery. Gapping, failure to splint to prevent tension on the nerve with motion, and failure to excise scarred or devitalized nerve tissue are impairments to successful nerve repairs. Suture repairs through the deep nerve segments can damage the axons. Sutures should be placed through the epineurium or, in a grouped fascicular repair, through the perineurium around the fascicles.
Question 46:
Gunshot or missile wounds can frequently cause neuropraxic injuries to peripheral nerves.
Options:
- True
- False Missile wounds can cause a blast stretch injury to peripheral nerves and may recover with observation.
Correct Answer: True
Question 47:
The anatomic location of the pathologic lesion of lateral epicondylitis is the:
Options:
- Extensor carpi radialis longus (EC RL)
- Extensor carpi radialis brevis (EC RB)
- Extensor digitorum longus (EDL)
- Extensor digitorum communis (EDC )
- Annular ligament
Correct Answer: Extensor carpi radialis longus (EC RL)
Explanation:
While the EC RL and EDL can sometimes be involved, the primary location of most cases of tennis elbow show characteristic changes at the origin of the EC RB.
Question 48:
Which of the following injectable substances have shown benefit in the treatment of lateral epicondylitis:
Options:
- C orticosteroids
- Autologous blood
- Botulinum toxin
- None of the above
- All of the above
Correct Answer: All of the above
Explanation:
All of these substances have been shown to have efficacy in the treatment of tennis elbow. However, placebo saline injections have also been proven to add some benefit compared to no treatment.
Question 49:
The nerve most at risk during arthroscopic debridement of lateral epicondylitis is the:
Options:
- Ulnar nerve
- Median nerve
- Anterior interosseous nerve
- Posterior interosseous nerve
- Musculocutaneous nerve
Correct Answer: Posterior interosseous nerve
Explanation:
While the ulnar nerve is most at risk during elbow arthroscopy in general, debridement of the lateral capsule posterior to the midpoint of the radiocapitellar joint places the posterior interosseous branch of the radial nerve at risk.
Question 50:
Common concomitant intra-articular pathology that can be found and addressed at arthroscopy for lateral epicondylitis include all of the following, except:
Options:
- Synovial plica
- Loose body
- Synovitis
- Medial epicondylitis
- Chondral lesion
Correct Answer: Medial epicondylitis
Explanation:
While all of the other answers are intra-articular lesions that have been reported in elbow arthroscopies, medial epicondylitis is an extra-articular condition and must be addressed in an open fashion given the proximity of the ulnar nerve.