

Orthopedic Ob Reconstru Review | Dr Hutaif Hip & Knee R -...
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 45-year-old active male undergoes a total hip arthroplasty using a ceramic-on-ceramic bearing. Two years later, he presents with a 'squeaking' sound coming from the hip with deep flexion activities. Radiographs show well-fixed components. What is the most likely etiology of this phenomenon?
Explanation
Question 2
A 68-year-old female is scheduled for a total hip arthroplasty. Preoperative standing and sitting lateral spine-pelvis radiographs demonstrate a change in sacral slope of less than 10 degrees from standing to sitting. Which of the following component positioning strategies is most appropriate given this finding?
Explanation
Question 3
During a posterior-stabilized total knee arthroplasty, the surgeon assesses the gaps with trial components. The knee has a symmetric extension gap that accepts a 10 mm spacer block perfectly. In flexion, the gap is asymmetric, being tight medially and loose laterally. Which of the following is the most appropriate next step in management?

Explanation
Question 4
According to the 2018 Evidence-Based Validated Definition for Periprosthetic Joint Infection, which of the following findings is considered a 'Major Criterion' sufficient for a definitive diagnosis of periprosthetic joint infection (PJI)?
Explanation
Question 5
A 55-year-old male presents with isolated medial compartment osteoarthritis of the right knee. He is being evaluated for a medial unicompartmental knee arthroplasty (UKA). Which of the following physical examination or radiographic findings is an absolute contraindication to a medial UKA?
Explanation
Question 6
A 72-year-old female falls and sustains a periprosthetic femur fracture around her cementless total hip arthroplasty. Radiographs reveal a fracture extending just distal to the tip of the stem. The stem is radiographically loose, but there is excellent proximal and distal bone stock. According to the Vancouver classification, what is the fracture type and the recommended surgical treatment?
Explanation
Question 7
During a revision total hip arthroplasty, you encounter severe acetabular bone loss. Preoperative radiographs demonstrate up and in migration of the cup past Kohler's line, superior migration of 4 cm, and intraoperatively you note destruction of >60% of the acetabular rim, with independent movement of the superior and inferior hemipelvis. What is the most appropriate reconstructive option?
Explanation
Question 8
When performing a direct anterior approach to the hip for total hip arthroplasty, the internervous plane utilized is between the tensor fasciae latae (TFL) and the sartorius superficially. Which two nerves supply these muscles respectively?
Explanation
Question 9
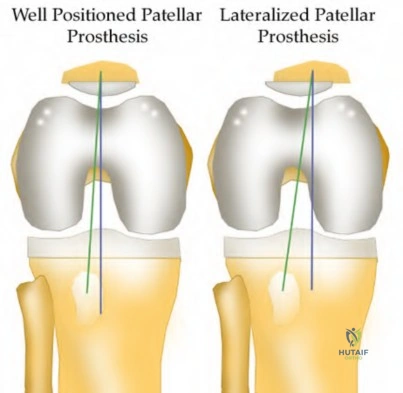
A patient presents with persistent anterior knee pain and a 'clunking' sensation 1 year following a primary total knee arthroplasty. On physical exam, the patella tracks laterally and there is tenderness over the lateral retinaculum. Radiographs and CT scan are obtained. Which of the following component malpositions is most likely responsible for lateral patellar maltracking?
Explanation
Question 10
A surgeon is performing a primary TKA and decides to use the surgical epicondylar axis (SEA) to set the rotation of the femoral component. Which of the following best defines the SEA?
Explanation
Question 11
A 62-year-old male presents with groin pain and a palpable mass 5 years after receiving a metal-on-polyethylene total hip arthroplasty with a large diameter modular cobalt-chromium head on a titanium stem. Serum cobalt levels are significantly elevated while chromium levels are mildly elevated. A metal artifact reduction sequence (MARS) MRI shows a cystic pseudotumor. What is the most likely diagnosis?
Explanation
Question 12
When planning a medial opening wedge high tibial osteotomy (HTO) for isolated medial compartment osteoarthritis in a varus knee, the surgeon intends to shift the mechanical axis to the Fujisawa point. Where is the Fujisawa point located on the tibial plateau?
Explanation
Question 13
According to the classification of cementless femoral stems, a fully porous-coated cylindrical stem relies on which area for its primary mechanical fixation?
Explanation
Question 14
A 70-year-old female presents 6 months post-total knee arthroplasty with an inability to actively extend her knee. Examination reveals a palpable defect at the superior pole of the patella. What is the most appropriate surgical reconstruction option for a chronic quadriceps tendon rupture following TKA with inadequate remaining tissue?
Explanation
Question 15
The wear rate of ultra-high molecular weight polyethylene (UHMWPE) in total hip arthroplasty has been significantly reduced by cross-linking. Which of the following manufacturing steps is required after gamma irradiation to prevent long-term oxidative degradation of the polyethylene?
Explanation
Question 16
In a cruciate-retaining (CR) total knee arthroplasty, the posterior cruciate ligament (PCL) is preserved. If the PCL is left excessively tight during the procedure, what kinematic abnormality is most likely to occur?
Explanation
Question 17
A patient presents with thigh pain 10 years after a cementless total hip arthroplasty. Radiographs demonstrate a continuous radiolucent line of 3 mm with sclerotic margins in Gruen zones 1, 2, 6, and 7. The stem has subsided by 5 mm. What is the most likely mode of failure?
Explanation
Question 18
During a revision total knee arthroplasty, removal of the tibial component reveals a massive contained metaphyseal defect measuring 3 cm deep, but with an intact cortical rim. According to the Anderson Orthopaedic Research Institute (AORI) classification, what type of defect is this, and what is the preferred method of management?
Explanation
Question 19
A 65-year-old patient who underwent a posterior-stabilized total knee arthroplasty 1 year ago complains of a painful 'catch' and an audible pop at the anterior knee when extending the leg from roughly 40 degrees of flexion to full extension. What is the underlying pathomechanics of this condition?
Explanation
Question 20
During primary total knee arthroplasty using a measured resection technique, the surgeon aims to restore the joint line. Which of the following anatomic landmarks is most reliable for approximating the native joint line level if the articular surface is severely distorted?
Explanation
Question 21
A 60-year-old male presents with groin pain 8 years after a metal-on-metal total hip arthroplasty. Lab results show elevated serum cobalt and chromium levels. MRI with MARS (Metal Artifact Reduction Sequence) shows a solid and cystic mass communicating with the joint space. What is the characteristic histological finding in the periprosthetic tissue of this condition?
Explanation
Question 22
During a primary total knee arthroplasty for a severe fixed valgus deformity, the knee is noted to be tight in extension but balanced in flexion. Which of the following lateral structures should be released first to selectively correct the tight extension gap?
Explanation
Question 23
A 75-year-old female sustains a fall 5 years after a cementless THA. Radiographs show a periprosthetic femur fracture occurring around the stem tip. Intraoperative assessment reveals the stem remains firmly fixed in the metaphysis, and the proximal bone stock is adequate. According to the Vancouver classification, what is the fracture type and the standard recommended treatment?
Explanation
Question 24
A 68-year-old female presents with an inability to perform a straight leg raise 3 months following a primary TKA. Examination reveals a palpable gap at the superior pole of the patella. What is the most appropriate surgical management for this complication?
Explanation
Question 25
Which of the following is traditionally considered an absolute contraindication to a medial mobile-bearing unicompartmental knee arthroplasty (UKA)?
Explanation
Question 26
A 65-year-old male complains of a painful catching sensation and an audible "clunk" when extending his knee from a flexed position, 1 year after a posterior-stabilized (PS) TKA. What is the primary etiology of this condition?
Explanation
Question 27
Which surgical approach to the hip is most frequently associated with the risk of iatrogenic injury to the superior gluteal nerve?
Explanation
Question 28
A patient presents with a feeling of the knee "giving way" when descending stairs 1 year post-TKA. On examination, the knee is stable in full extension but has significant anteroposterior laxity at 90 degrees of flexion. Which of the following technical errors during the index surgery is the most likely cause?
Explanation
Question 29
During a primary TKA for a varus osteoarthritic knee, after making the standard measured bone cuts, the knee has a symmetric tight medial gap in both flexion and extension. The lateral gap is well-balanced. Which of the following is the most appropriate next step in soft tissue balancing?
Explanation
Question 30
Tranexamic acid (TXA) is routinely utilized in total joint arthroplasty to minimize perioperative blood loss. What is the cellular mechanism of action of TXA?
Explanation
Question 31
The introduction of highly cross-linked polyethylene (HXLPE) has significantly reduced wear rates and osteolysis in THA. However, the cross-linking process alters the mechanical properties of the material. Which of the following properties is primarily DECREASED by the irradiation process?
Explanation
Question 32
A 45-year-old female with developmental dysplasia of the hip (DDH) presents for THA. Preoperative radiographs show the femoral head is subluxated, with 80% proximal migration relative to the height of the normal true acetabulum. Based on the Crowe classification, what type of dysplasia does she have?
Explanation
Question 33
A 70-year-old female undergoes a right TKA for a severe fixed valgus deformity. Postoperatively in the recovery room, she is noted to have a foot drop and decreased sensation over the dorsum of the right foot. What is the most appropriate initial management?
Explanation
Question 34
According to the classic work by Lewinnek, what is the "safe zone" for the orientation of the acetabular component in total hip arthroplasty to minimize the risk of postoperative dislocation?
Explanation
Question 35
Which of the following statements best describes the surgical principle of true kinematic alignment in total knee arthroplasty?
Explanation
Question 36
A 68-year-old male presents with groin pain 6 years after a primary THA using a large-diameter metal head on a standard titanium alloy stem (metal-on-polyethylene bearing). Radiographs show no component loosening, but an MRI reveals a large cystic mass around the joint. Blood tests show elevated serum cobalt and normal chromium levels. What is the most likely diagnosis?
Explanation
Question 37
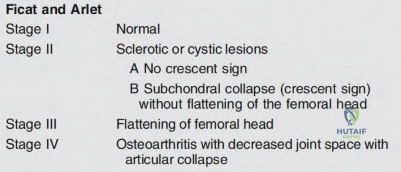
A 35-year-old male presents with right hip pain. MRI confirms avascular necrosis (AVN) of the femoral head. Radiographs show a distinct sclerotic band and cystic changes in the femoral head, but no subchondral collapse or crescent sign. According to the Ficat and Arlet classification, what stage is this, and is core decompression generally indicated?
Explanation
Question 38
In total hip arthroplasty, a single-wedge (flat tapered) titanium cementless stem relies primarily on which of the following mechanisms for its initial mechanical stability?
Explanation
Question 39
A 72-year-old female presents with acute thigh pain and an inability to bear weight after a minor fall, 10 years post-THA. Radiographs demonstrate a fracture around the tip of the well-fixed femoral stem, extending into the diaphysis. The bone stock proximally remains intact. Which principle must be strictly adhered to during the surgical fixation of this fracture?
Explanation
Question 40
During a complex revision TKA, the surgeon notes profound laxity and attenuation of the medial collateral ligament (MCL) such that the knee cannot be balanced coronally in either flexion or extension. The extensor mechanism and posterior capsule remain completely intact. Which level of prosthetic constraint is most appropriate in this scenario?
Explanation
Question 41
In revision total hip arthroplasty (THA), an Extended Trochanteric Osteotomy (ETO) is often planned to remove a well-fixed cementless stem. To ensure successful extraction and subsequent stable fixation of a fully porous-coated cylindrical revision stem, what is the biomechanical principle regarding the length of the ETO fragment?
Explanation
Question 42
A 68-year-old patient with a fused lumbar spine from L2 to the pelvis (pelvic incidence minus lumbar lordosis mismatch) is scheduled for a THA. How does this spinopelvic stiffness affect the optimal acetabular cup positioning to minimize the risk of dislocation?
Explanation
Question 43
A patient with a metal-on-polyethylene (MoP) THA presents 5 years postoperatively with sudden onset groin pain. Blood work reveals serum Cobalt levels significantly higher than Chromium levels. MRI with MARS sequencing shows a solid and cystic pseudotumor around the hip. What is the primary pathophysiologic mechanism for this failure?
Explanation
Question 44
A patient presents with a palpable, painful 'catch' and an audible pop during active extension of the knee from 40 degrees to 30 degrees following a posterior-stabilized (PS) Total Knee Arthroplasty (TKA). What is the most likely etiology?
Explanation
Question 45
Intraoperatively during a primary TKA, the surgeon utilizes spacer blocks and finds that the flexion gap is excessively tight, but the extension gap is perfectly symmetric and balanced. Which of the following is the most appropriate surgical step to correct this kinematic mismatch?
Explanation
Question 46
According to the 2018 International Consensus Meeting (ICM) criteria for Periprosthetic Joint Infection (PJI), which of the following carries the highest diagnostic weight and qualifies as a definitive 'Major' criterion?
Explanation
Question 47
In the manufacturing of highly cross-linked polyethylene (XLPE) for THA, irradiation is used to create cross-links that improve wear resistance. What is the primary biomechanical tradeoff of using a 'remelting' process compared to an 'annealing' process to eliminate free radicals?
Explanation
Question 48
During a total hip arthroplasty, the surgeon utilizes a standard offset stem instead of a high offset stem, inadvertently decreasing the patient's native femoral offset by 15 mm. What is the most likely biomechanical consequence of this error?
Explanation
Question 49
Elevation of the joint line during TKA (often resulting from excessive distal femoral resection and using a thicker polyethylene insert) most commonly leads to which of the following complications?
Explanation
Question 50
A 45-year-old active male with a ceramic-on-ceramic (CoC) THA reports a loud squeaking noise with walking that is socially embarrassing. Which factor is most strongly associated with the etiology of this phenomenon?
Explanation
Question 51
A patient requires a femoral revision THA for aseptic loosening. Radiographs demonstrate extensive metaphyseal bone loss with the diaphyseal cortical bone remaining fully intact for only 3 cm distal to the tip of the current stem. According to the Paprosky femoral defect classification, what type of defect is present?
Explanation
Question 52
Which of the following histological findings is pathognomonic for an Aseptic Lymphocyte-Dominated Vasculitis-Associated Lesion (ALVAL) in the setting of a failed metal-on-metal THA?
Explanation
Question 53
When evaluating a patient for a Unicompartmental Knee Arthroplasty (UKA), which of the following is considered a classic absolute contraindication?
Explanation
Question 54
Following a complete disruption of the extensor mechanism after TKA, a reconstruction utilizing synthetic mesh (e.g., Marlex) is performed. What is the critical recommended postoperative rehabilitation protocol to ensure construct survival?
Explanation
Question 55
In revision TKA for severe AORI Type 2b or 3 metaphyseal bone defects, highly porous metaphyseal titanium cones are increasingly utilized. What is their primary biomechanical and biologic advantage over standard structural allografts?
Explanation
Question 56
Popliteal artery injury is a rare but devastating complication of primary TKA. During which specific surgical maneuver is the artery at the highest risk of direct traumatic injury?
Explanation
Question 57
A 72-year-old patient undergoes a primary TKA for severe valgus deformity. Intraoperatively, the medial collateral ligament (MCL) is found to be severely attenuated and incompetent, preventing varus-valgus stability with standard gap balancing, but the extensor mechanism and soft tissue envelope are otherwise intact. Which level of implant constraint is most appropriate as the next step?
Explanation
Question 58
A 35-year-old female with developmental dysplasia of the hip (DDH) Crowe Type IV is undergoing THA. The surgeon plans to place the acetabular component in the true anatomic hip center. If the leg is lengthened >4 cm without a subtrochanteric shortening osteotomy, which nerve division is most susceptible to traction injury?
Explanation
Question 59
Radiographs of a failed THA demonstrate severe periprosthetic osteolysis. The acetabular component has migrated 4 cm superiorly and 2 cm medially past Kohler's line, and the radiographic teardrop is completely destroyed. Which Paprosky acetabular defect is present?
Explanation
Question 60
A patient presents 8 weeks after a primary TKA with severe stiffness. Despite aggressive, supervised physical therapy, their active and passive range of motion is limited to a painful arc from 15 degrees of extension to 75 degrees of flexion. What is the most appropriate next step in management?
Explanation
Question 61
During a standard Cruciate-Retaining (CR) Total Knee Arthroplasty, what is the primary consequence of an excessive posterior slope cut on the proximal tibia?
Explanation
Question 62
A 65-year-old male with a metal-on-polyethylene total hip arthroplasty (large modular head) presents with insidious groin pain 5 years postoperatively. Blood tests reveal elevated cobalt levels and normal chromium. Aspiration is negative for infection.
What is the most likely diagnosis?
Explanation
Question 63
A 70-year-old female presents with a feeling of instability when going down stairs one year after a primary TKA. Clinical exam reveals stability in full extension and at 90 degrees of flexion, but excessive AP laxity at 30-45 degrees of flexion. Which of the following technical errors is the most likely cause?
Explanation
Question 64
During a complex revision Total Hip Arthroplasty for a well-fixed extensively porous-coated stem, an extended trochanteric osteotomy (ETO) is planned. Which of the following is true regarding the ETO technique?
Explanation
Question 65
In diagnosing Periprosthetic Joint Infection (PJI), the 2018 ICM criteria include Alpha-defensin as a major synovial fluid biomarker. What is the primary cellular source of Alpha-defensin in the context of PJI?
Explanation
Question 66
A 55-year-old female underwent THA with a ceramic-on-ceramic bearing. At her 2-year follow-up, she complains of a loud squeaking noise from her hip when bending to tie her shoes. Which of the following factors is most strongly associated with squeaking in ceramic-on-ceramic THA?
Explanation
Question 67
A 65-year-old man who underwent a Posterior Stabilized (PS) Total Knee Arthroplasty 18 months ago complains of a painful 'catch' or 'pop' when extending his knee from 40 degrees of flexion. Which of the following is the most likely pathophysiologic mechanism for this condition?
Explanation
Question 68
A 78-year-old female sustains a periprosthetic femur fracture 10 years after a cemented THA. Radiographs show a fracture around the tip of the stem with a loose femoral component and poor proximal bone stock, but adequate diaphyseal bone.
What is the most appropriate surgical treatment?
Explanation
Question 69
To reduce polyethylene wear rates in THA, highly cross-linked polyethylene (HXLPE) is widely used. What is the primary purpose of the post-irradiation thermal treatment (melting or annealing) in the manufacturing of HXLPE?
Explanation
Question 70
In a Posterior Stabilized (PS) total knee arthroplasty, what is the primary biomechanical function of the femoral cam and tibial post mechanism?
Explanation
Question 71
Tranexamic acid (TXA) is routinely used to reduce blood loss in total joint arthroplasty. What is the precise mechanism of action of TXA?
Explanation
Question 72
During a primary total hip arthroplasty, the surgeon opts to increase the femoral offset compared to the patient's native anatomy. Assuming the leg length is kept constant, which of the following biomechanical effects is most likely to result from this change?
Explanation
Question 73
A direct anterior approach to the hip utilizes an internervous and intermuscular plane. Which of the following accurately describes this superficial interval?
Explanation
Question 74
A 52-year-old male with isolated medial compartment osteoarthritis is evaluated for a unicompartmental knee arthroplasty (UKA).
Which of the following conditions is considered a strict contraindication to a traditional mobile-bearing UKA?
Explanation
Question 75
A dual mobility cup is often used in revision THA to reduce the risk of dislocation. Which of the following best describes the primary biomechanical principle of a dual mobility construct?
Explanation
Question 76
During TKA, joint line restoration is critical for proper biomechanics. Which of the following is a direct consequence of inadvertently elevating the joint line by more than 8 mm?
Explanation
Question 77
A 62-year-old female presents with a persistently painful, stiff, and swollen knee 1 year after a primary TKA. Inflammatory markers are normal, and aspiration yields fluid with <500 WBCs. She reports a history of a severe skin rash when wearing cheap jewelry. If metal hypersensitivity is suspected, which immunological mechanism is primarily responsible?
Explanation
Question 78
Patellar maltracking is a significant complication following TKA. Which of the following component malpositions is most likely to cause lateral patellar maltracking?
Explanation
Question 79
When planning a primary THA, the surgeon uses the AP pelvis radiograph to assess leg length discrepancy.
Which of the following radiographic landmarks is most reliable for establishing a horizontal reference line for leg length measurement?
Explanation
Question 80
A 68-year-old male sustains a distal femur periprosthetic fracture (Lewis and Rorabeck Type II) directly above a well-fixed PS TKA femoral component. The fracture is displaced. What is the most appropriate management?
Explanation
Question 81
During a measured-resection total knee arthroplasty, the trial components are placed. The knee is found to have a symmetric tight extension gap and a symmetric perfectly balanced flexion gap. Which of the following is the most appropriate next step to balance the knee?
Explanation
Question 82
Which of the following is traditionally considered an absolute contraindication to a fixed-bearing medial unicompartmental knee arthroplasty (UKA)?
Explanation
Question 83
A 65-year-old male with a long-segment lumbar fusion (L2 to Sacrum) presents for a total hip arthroplasty. How does his spinopelvic stiffness affect acetabular dynamics during the transition from standing to sitting?
Explanation
Question 84
In total knee arthroplasty, which of the following femoral component malpositions is most likely to lead to lateral patellar maltracking?
Explanation
Question 85
A surgeon is performing a total hip arthroplasty via the direct anterior (Smith-Petersen) approach. This approach exploits the internervous plane between which two muscle groups?
Explanation
Question 86
A 65-year-old female with a metal-on-polyethylene THA presents with groin pain 5 years post-op. Radiographs show well-fixed components. Aspiration yields sterile fluid with a normal cell count. Serum metal ion testing shows heavily elevated Cobalt with normal Chromium levels. What is the most likely etiology?
Explanation
Question 87
During a cruciate-retaining (CR) total knee arthroplasty trial, the knee is well-balanced in extension, but the anterior tibia lifts off the trial baseplate in deep flexion. What is the most likely cause?
Explanation
Question 88
A 75-year-old female sustains a periprosthetic femur fracture around a cemented polished taper slip stem. Radiographs demonstrate a fracture around the tip of the stem. The stem is radiographically loose, but the proximal bone stock is excellent (Vancouver B2).
What is the gold standard surgical management?
Explanation
Question 89
A patient presents 3 weeks after an uncomplicated primary TKA with acute severe knee pain, erythema, and a large effusion. Synovial fluid analysis reveals a WBC of 45,000 cells/uL with 92% polymorphonuclear neutrophils. Radiographs show perfectly aligned, well-fixed components. What is the best definitive management?
Explanation
Question 90
Pre-operative templating for a primary total hip arthroplasty aims to restore native femoral offset. Failure to restore femoral offset (leaving it decreased) leads to which of the following biomechanical consequences?
Explanation
Question 91
In the manufacturing of modern highly cross-linked polyethylene (HXLPE) for total hip arthroplasty, increasing the radiation dose improves wear resistance but is known to adversely decrease which of the following mechanical properties?
Explanation
Question 92
A patient with a severe 20-degree valgus knee deformity undergoes a primary posterior-stabilized TKA. On post-operative day 1, the patient exhibits a new-onset foot drop and numbness over the first dorsal web space. What is the most appropriate initial step in management?
Explanation
Question 93
Six months following an uncemented total hip arthroplasty, a patient complains of severe sharp groin pain when actively lifting their leg to get into a car. Radiographs reveal an acetabular component that is prominent anteriorly. Which of the following is the most likely diagnosis?
Explanation
Question 94
During a total knee arthroplasty, which of the following surgical steps carries the highest risk of iatrogenic injury to the popliteal artery?
Explanation
Question 95
A surgeon is performing a revision THA for a fractured ceramic femoral head. The femoral stem is well-fixed. After thorough debridement of all ceramic shards, what is the critical step regarding the bearing surface selection?
Explanation
Question 96
During a primary TKA trial reduction, the surgeon notes that the joint is symmetrically loose in full extension and symmetrically loose in 90 degrees of flexion. Which of the following is the most appropriate single intervention?
Explanation
Question 97
Which of the following prophylactic regimens is considered most effective for a patient with a prior history of severe heterotopic ossification undergoing a revision total hip arthroplasty?
Explanation
Question 98
Patellar clunk syndrome is a recognized complication characterized by a fibrosynovial nodule catching in the intercondylar notch. It is most commonly associated with which of the following knee arthroplasty designs?
Explanation
None
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding orthopedic-mcqs-online-ob-20-reconstruction-1a