Hemi-Hamate Autograft Reconstruction for Unstable PIP Dorsal Fracture-Dislocations

Key Takeaway
Join us in the OR for a masterclass on hemi-hamate autograft reconstruction of unstable PIP dorsal fracture-dislocations. We'll meticulously cover patient assessment, preoperative planning, precise surgical technique from incision to fixation, and critical postoperative care. Learn to restore joint stability and function, avoiding common pitfalls and ensuring optimal patient outcomes in complex hand trauma.
Alright, fellows, gather 'round. Welcome to the operating theater. Today, we're tackling a challenging injury: an unstable dorsal Proximal Interphalangeal (PIP) joint fracture-dislocation requiring a hemi-hamate autograft reconstruction. This procedure demands precision, a thorough understanding of hand anatomy, and meticulous technique. Our goal is to restore the critical cup-shaped geometry of the middle phalanx base and re-establish the palmar plate attachment, thereby regaining joint stability and enabling early, functional range of motion.
Understanding the Unstable PIP Joint: Anatomy and Pathogenesis
Let’s begin with a quick review of the anatomy and biomechanics of the PIP joint, which is crucial for understanding why these injuries occur and how to fix them. The PIP joint is a complex hinge articulation, designed to provide over 95 degrees of flexion while maintaining concentric reduction of its articular surfaces.
Anatomy of the PIP Joint and Its Stabilizers
The PIP joint consists of the head of the proximal phalanx and the base of the middle phalanx. Its stability relies on a delicate balance of static and dynamic stabilizers:
- Static Stabilizers:
- Palmar Plate (Volar Plate): This is a thick, fibrocartilaginous structure located on the palmar aspect of the joint. It prevents hyperextension and provides a crucial attachment point for the accessory collateral ligaments. Its strong distal insertion onto the palmar lip of the middle phalanx is key.
- Collateral Ligaments: These include the proper collateral ligaments and the accessory collateral ligaments. The proper collateral ligaments originate from the sides of the proximal phalanx head and insert onto the palmar-lateral aspects of the middle phalanx base. They are taut in flexion and lax in extension. The accessory collateral ligaments originate more volarly and insert onto the palmar plate.
- Cup-shaped Geometry of the Middle Phalanx: The concave articular surface of the middle phalanx base acts like a "hook" wrapping around the convex head of the proximal phalanx, preventing dorsal translation.
- Dynamic Stabilizers:
- Extensor Tendon Mechanism: The central slip inserts onto the dorsal base of the middle phalanx, providing active extension.
- Flexor Tendon Mechanism: The flexor digitorum superficialis (FDS) inserts into the middle phalanx, contributing to flexion and also exerting a dorsalizing force if its insertion is disrupted or the palmar plate is compromised.
Fracture Patterns and Instability
PIP joint fracture-dislocations typically present with distinct patterns:
- Palmar Lip Fracture-Dislocations: This is our focus today. It involves a fracture of the palmar lip of the middle phalanx, leading to dorsal subluxation or dislocation of the middle phalanx on the proximal phalanx head.
- Mechanism: Several forces encourage this dorsal migration. The extensor tendon lifts the middle phalanx, and the distal FDS insertion can lever the middle phalanx dorsally, especially when the primary restraints are compromised.
- Restraints Lost: In these injuries, both primary restraints to dorsal subluxation are disrupted: the palmar plate is no longer attached, and the critical cup-shaped geometry of the middle phalangeal palmar lip is lost. The remaining articular surface often slopes dorsally, actively encouraging the middle phalanx to ride up and over the proximal phalangeal head.
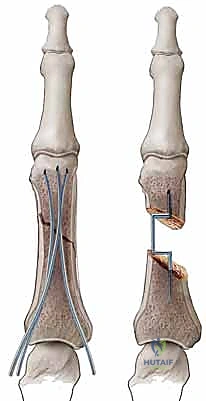
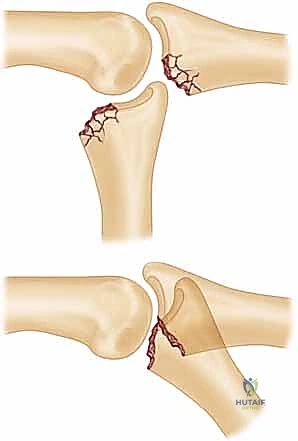
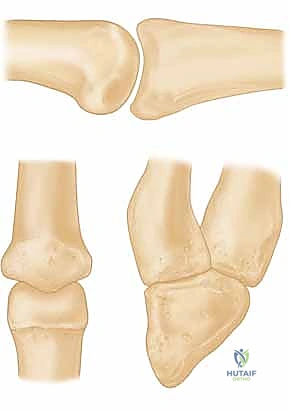
* FIG 1 • A. Unstable PIP fracture-dislocation. The upward pull of the central tendon insertion and the distal superficialis insertion pull and push the middle phalanx up and over the proximal phalangeal head. The only forces preventing dorsal subluxation are the middle phalanx palmar lip and the palmar plate, both of which are lost in an unstable PIP palmar lip fracture.
*
* FIG 1 • B. PIP instability after a fracture. A direct relation exists between the amount of middle phalanx palmar lip destroyed by the fracture and the resultant PIP joint stability. Articular damage in excess of 50% of the joint surface always renders the joint unstable, whereas fractures involving less than 30% usually are stable. Tenuous fractures (ie, those with articular damage of 30% to 50% of the joint surface), must be assessed with lateral radiographs. If the joint will not stay reduced with less than 30 degrees of flexion, it must be classified as “unstable.”
* Dorsal Lip Fracture-Dislocations: These involve a fracture of the dorsal lip of the middle phalanx with palmar subluxation of the middle phalanx. Treatment is complicated by the need to re-establish continuity of the extensor tendon insertion.
* Pilon Fractures: These are severe injuries involving a loss of continuity of both dorsal and palmar cortical margins of the middle phalangeal articular surface. The base of the middle phalanx is often highly comminuted and impacted. These are typically managed with traction and early motion.
Classification of PIP Fractures: Stable vs. Unstable
We classify PIP fractures as "stable" or "unstable."
* Stable fractures maintain concentric joint reduction throughout the full range of motion (ROM).
* Unstable fractures sublux or dislocate at some point in the motion arc.
* A critical threshold: When 42% or more of the palmar articular surface is damaged, the joint always exhibits dorsal instability. In the clinical setting, even as little as 30% articular surface involvement can render the joint unstable.
Pathogenesis of Palmar Lip Fractures
The middle phalangeal palmar lip fracture associated with unstable dorsal PIP fracture-dislocations is typically created by one of two mechanisms:
- Avulsion Fractures:
- Mechanism: These result from PIP joint hyperextension and traction through the palmar plate attachment.
- Characteristics: The fracture fragment is typically not comminuted and involves less than 30% of the articular surface.
- Stability: These injuries are usually stable and rarely require surgical intervention. If unstable, osteosynthesis with lag screws is often possible due to the lack of comminution and substantial fragment size.
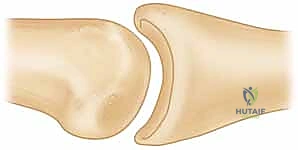
* FIG 2 • A. Avulsion fracture. Avulsion fractures usually are caused by a forced PIP joint hyperextension. The fragment is not comminuted and involves less than 30% of the joint surface. The PIP joint is most often stable.
* Impaction Shear Fracture-Dislocations:
* Mechanism: These are caused by a longitudinally applied load to the tip of the finger with the PIP joint slightly flexed, such as a "jammed finger" from a mishandled ball catch. The force drives the middle phalanx into and over the proximal phalanx head.
* Characteristics: This results in a middle phalangeal palmar lip fracture that is highly comminuted, with fragments often deeply impacted into the soft metaphyseal bone. Up to 80% of the joint surface can be involved.
* Stability: The joint reduction is often unstable.
*

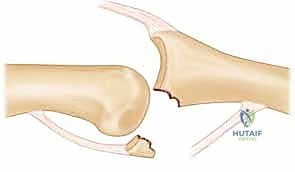
* FIG 2 • B. Impaction shear fracture. This type of PIP fracture-dislocation is caused by a longitudinal load to the joint. The fracture fragments are comminuted and impacted into the middle phalanx. The joint reduction often is unstable.
Patient History and Physical Findings
When evaluating these patients, a thorough assessment is paramount.
Clinical Evaluation
- History: Patients typically present with a history of recent trauma, often a "jamming" injury to the finger. They will complain of pain, swelling, and deformity at the PIP joint.
- Inspection: Carefully inspect the affected finger.
- Look for obvious deformity, swelling, and ecchymosis.
- Assess alignment in the coronal plane. Lateral deviation suggests asymmetric compression of articular fragments, which can lead to varus or valgus angulation.
- Assess alignment in the sagittal plane. A lack of colinearity between the middle and proximal phalanx suggests persistent joint subluxation or dislocation.
- Palpate the joint for tenderness and stability.
- Range of Motion: Attempt gentle active and passive range of motion, noting any instability or crepitus.
- Neurovascular Status: Always assess digital nerve sensation and capillary refill to rule out associated neurovascular compromise, although it's rare in these injuries.
- Associated Injuries: Disruption of the terminal extensor tendon, leading to a mallet finger deformity, often occurs in association with unstable dorsal PIP fracture-dislocations. This must be identified preoperatively as it requires concurrent treatment.
Imaging and Other Diagnostic Studies
Plain radiographs are the mainstay of diagnosis.
- Posteroanterior (PA) and Lateral Views: These are essential.
- On the lateral radiograph, carefully inspect the quality of the reduction. The remaining articular cartilage on the middle phalanx base must be in full contact with the proximal phalanx head. Any dorsal gap between the two surfaces – a "V" sign – indicates persistent instability and must be corrected.
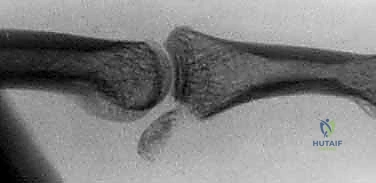
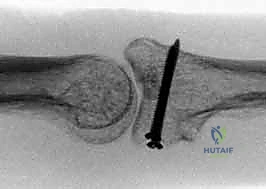
* FIG 4 • Unstable PIP palmar lip fracture-dislocation. Extensive damage has occurred to the palmar lip of the middle phalanx, but the dorsal cortical margin and a small amount of dorsal articular cartilage remain intact. Even slight dorsal subluxation can be detected by looking for a V-shaped gap between the middle and proximal phalanges.
*
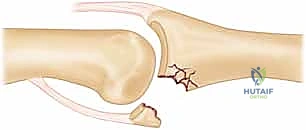
* FIG 4 • Unstable PIP palmar lip fracture-dislocation (continued). Note the "V" sign indicating persistent dorsal subluxation.
* Determine the percentage of joint surface fractured. This is critical for predicting joint reduction stability:
* Less than 30%: Reduction is usually stable. The middle phalanx almost always remains concentrically reduced throughout a full ROM.
* 30% to 50%: Reduction is tenuous. The middle phalanx may or may not subluxate dorsally when the PIP joint is extended. If any subluxation is noted on the lateral radiograph with the PIP joint fully extended, flex the joint to 30 degrees and repeat the lateral radiograph. If it still subluxes, it's unstable.
* Over 50%: The PIP joint is inherently unstable, and surgical intervention is almost always required.
* On the PA view, inspect for asymmetric compression of middle phalanx articular fragments, which could lead to varus or valgus angulation.
* Stress Radiographs: If stability is questionable, stress radiographs (e.g., in extension and 30 degrees of flexion) can help confirm instability.
* CT or MRI: Rarely necessary for acute, obvious unstable PIP dorsal fracture-dislocations. Plain radiographs usually suffice. However, for chronic cases or those with significant comminution where surgical planning requires a clearer 3D understanding of fragment size and impaction, a CT scan can be beneficial. MRI is generally reserved for soft tissue injuries like collateral ligament ruptures or palmar plate avulsions without significant bony involvement.
Nonoperative Management
Nonoperative management is reserved for stable fractures.
- Stable PIP Fracture-Dislocations (Less than 30% articular involvement):
- If the joint does not hyperextend and the lateral radiograph in full extension confirms concentric reduction, buddy tape the fingers and allow early ROM.
- If the joint hyperextends, some flexion must be maintained for 3 weeks to allow fracture fragments to consolidate and restore palmar plate continuity. Apply a dorsal blocking splint that prevents PIP hyperextension but allows full active flexion.
- Tenuous PIP Fracture-Dislocations (30% to 50% articular involvement):
- This requires careful thought, patient cooperation, and meticulous follow-up.
- The primary treatment goal is to maintain joint reduction while the palmar fragments consolidate and restore the cup-shaped geometry.
- Joint reduction must be achievable with less than 30 degrees of flexion, and the palmar fragments must fall into a position that will restore the palmar lip.
- If concentric reduction is achieved, an extension block treatment (splints or pins) may be employed.
- If the joint will not stay reduced with less than 30 degrees of flexion, the joint is unstable and must be treated surgically.
- Unstable PIP Fracture-Dislocations (Over 50% articular involvement):
- These rarely can be managed nonoperatively. All restraints to dorsal subluxation are lost. Surgical intervention is almost always required to rebuild the cup-shaped geometry of the middle phalanx base and reattach the palmar plate.
- Non-operative treatment for unstable fractures has a high failure rate, leading to chronic subluxation, accelerated articular wear, and poor long-term functional outcomes. When the middle phalanx rides dorsally, PIP flexion occurs by "hinging" at the fracture margin, leading to proximal phalanx articular cartilage wear while the undamaged middle phalanx surface remains unused.
Surgical Management: Hemi-Hamate Autograft Reconstruction
Today, we're performing a hemi-hamate osteochondral autograft. This is a robust solution for specific, unstable PIP fracture-dislocations.
Indications for Hemi-Hamate Autograft
- Unstable PIP dorsal fracture-dislocations where the middle phalanx dorsal cortex remains intact. This is critical, as the dorsal cortex provides a stable platform for graft integration.
- Failed previous treatments such as traction, external fixation devices, extension block splinting, or palmar plate arthroplasty. Hemi-hamate arthroplasty is a valuable salvage procedure.
- Chronic PIP dorsal dislocations are also amenable to this technique, provided there is enough intact cartilage on both sides of the joint. Specifically, undamaged cartilage must be present on the palmar 50% of the proximal phalanx head and on at least a small rim of the middle phalanx dorsal articular surface.
Contraindications
- Significant pre-existing degenerative arthritis of the PIP joint. In such cases, a PIP arthrodesis or total joint arthroplasty may be a more appropriate solution.
- Extensive comminution or loss of the dorsal cortical margin of the middle phalanx, which precludes stable graft integration.
- Active infection.
- Insufficient cartilage on the proximal phalanx head or dorsal middle phalanx rim.
Preoperative Planning
Before we scrub in, let's review our plan.
- Anesthesia: We'll be using a regional block in combination with general anesthesia for patient comfort and optimal intraoperative conditions. This allows for a bloodless field with the tourniquet, while also providing excellent postoperative pain control.
- Radiograph Review: I've meticulously reviewed the radiographs. We've assessed the extent of articular surface damage, confirmed joint instability, and evaluated the quality of the remaining articular cartilage. We've also confirmed the dorsal cortex of the middle phalanx is intact, which is a key indication for this procedure.
- Antibiotics: Our patient has received perioperative intravenous antibiotics, typically a first-generation cephalosporin, as per protocol.
- Tourniquet Application: An upper arm tourniquet has been applied. This is preferred over a forearm tourniquet, which can put pressure on the flexor muscles and cause excessive finger flexion, hindering exposure. We'll inflate it once we're draped and ready.
- Hair Removal: The dorsum of the hand, specifically around the fourth and fifth carpometacarpal (CMC) joints, has been shaved to facilitate the hemi-hamate graft harvest.
- Coronal Plane Assessment: I've assessed the finger for any pre-existing radial or ulnar deviation. If coronal plane angulation is observed, we must remember to level the middle phalangeal joint surface during fracture site preparation and graft placement to prevent residual deformity.
- Mallet Finger Check: We've re-examined the patient for any associated mallet finger injury. If the terminal extensor tendon has been damaged, we will plan to include a DIP extension splint in the postoperative regimen.
- Fluoroscopy Setup: A mini C-arm is essential for this procedure. The fluoroscopy unit will be positioned to allow easy intraoperative imaging in both PA and lateral views without disrupting our sterile field. Ensure the image intensifier is draped appropriately.
Patient Positioning
Let's get our patient positioned correctly.
- Supine Position: The patient is supine on the operating table.
- Hand Table: The affected arm is extended onto a radiolucent hand table. This provides a stable, sterile working surface and allows for unimpeded fluoroscopic imaging.
- Lead Hand: We will use a lead hand to position the hand palm up with the fingers extended for the PIP joint approach. Remember, we will need to remove the lead hand intermittently to facilitate use of fluoroscopy. For the hamate harvest, the hand will be positioned palm down or slightly pronated.
Intraoperative Execution: The Masterclass
Now, let’s begin the surgery. We'll start with the PIP joint exposure and fracture site preparation.
I. PIP Joint Exposure and Fracture Site Preparation
Our approach to the PIP joint will be through a Brunner incision. This provides excellent visualization of the fracture, the pulley system, and the neurovascular bundles, while minimizing scar contracture.
- Incision:
- Fellow 1, please hand me a #15 blade. We will make a Brunner incision on the palmar aspect of the affected finger, from the base of the finger (proximal phalanx level) distally to the DIP flexor crease. Observe how the zig-zag pattern crosses the flexion creases at an angle, preventing contracture.

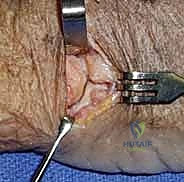
* *TECH FIG 1 • A. Brunner incision. The incision is made
Additional Intraoperative Imaging & Surgical Steps








REFERENCES
-
Graft donor site aching discomfort was noted only rarely in three patients. The remaining patients were asymptomatic.
-
Motion
-
ROM in the PIP averaged 85 degrees (range 65 degrees to 100 degrees).
-
Most patients had a slight PIP flexion contracture that averaged 9 degrees (range 0 degrees to 25 degrees).
-
The ROM of the MP joint averaged 90 degrees (range 75 degrees to 100 degrees), and the motion at the DIP joint averaged 60 degrees (range 35 degrees to 80 degrees).
-
Stability
-
Two of 12 patients demonstrated slight dorsal subluxation on the lateral radiograph, but neither patient had symptoms or functional problems.
-
One of the two patients with dorsal subluxation also demonstrated 20 degrees of ulnar instability, but she was not symptomatic from this abnormality.
-
An apparent articular surface step-off between the graft and native middle phalanx cartilage commonly is observed. This phenomenon is caused by the greater thickness of the cartilage on the graft compared to the middle phalanx cartilage.
-
All grafts united, as demonstrated by bridging trabeculae.
-
None of the grafts demonstrated sclerosis that suggested osteonecrosis.
-
Graft reabsorption was not observed.
-
Our experience with PIP hemi-hamate arthroplasty is too short to definitively determine the ultimate fate of the transferred articular cartilage.
-
Early results do not suggest that autograft will lead to excessive rates of cartilage degeneration causing symptomatic posttraumatic changes.
-
No patients developed infection, and no patients required subsequent surgery.
-
Dorsal subluxation was noted in 2 of 12 patients. One was believed to have been caused by an incompetent palmar plate. The other case of dorsal subluxation was attributed to a graft that was not appropriately contoured to restore the cup-shaped geometry of the middle phalanx base.
-
Eaton RG, Malerich MM. Volar plate arthroplasty for the proximal interphalangeal joint: a ten year review. J Hand Surg Am 1980;5:260–268.
-
Freeland AE, Benoist LA. Open reduction and internal fixation method for fractures at the proximal interphalangeal joint. Hand Clin 1994;10:239–250.
-
Hamilton SC, Stern PJ, Fassler PR, et al. Mini-screw fixation for the treatment of proximal interphalangeal joint dorsal fracturedislocations. J Hand Surg Am 2006;8:1349–1354.
-
Hastings H, Capo J, Steinberg B, et al. Hemicondylar hamate replacement arthroplasty for proximal interphalangeal joint fracture-dislocations. Abstract. Presented at the 54th annual meeting of The American Society for Surgery of the Hand, September 3–5, 1999, Boston, MA.
-
Hastings H II, Carroll C IV. Treatment of closed articular fractures of the metacarpophalangeal and proximal interphalangeal joints. Hand Clin 1988;4:503–527.
-
Hastings J II, Hamlet WP. Critical assessment of PIP joint stability after palmar lip fractures dislocations. Abstract. Presented at the 56th Annual Meeting of The American Society for Surgery of the Hand, October 3–6, 2001, Baltimore, MD.
-
Inanami H, Ninomiya S, Okutsu I, et al. Dynamic external finger fixator for fracture-dislocation of the proximal interphalangeal joint. J Hand Surg Am 1993;18:160–194.
-
Jupiter JB, Sheppard JE. Tendon wire fixation of avulsion fractures in the hand. Clin Orthop Relat Res 1987;214:113–120.
-
Kiefhaber TR, Stern PJ. Fracture-dislocations of the proximal interphalangeal joint. J Hand Surg Am 1998;23:368–380.
-
Krakauer JD, Stern PJ. Hinged device for fracture involving the proximal interphalangeal joint. Clin Orthop Relat Res 1996;327:29–37.
-
McElfresh EC, Dobyns JH, O’Brien ET. Management of fracture-dislocations of the proximal interphalangeal joints by extension-block splinting. J Bone Joint Surg Am 1972;54:1705–1711.
-
Morgan JP, Gordon DA, Klug MS, et al. Dynamic digital traction for unstable comminuted intra-articular fracture-dislocations of the proximal interphalangeal joint. J Hand Surg Am 1995; 20:565–573.
-
Schenck RR. Dynamic traction and early passive movement for fractures of the proximal interphalangeal joint. J Hand Surg Am 1986;11:850–858.
-
Viegas SF. Extension block pinning for proximal interphalangeal joint fracture-dislocations: preliminary report of a new technique. J Hand Surg Am 1992;17:896–901.
-
Williams RMM, Hastings H II, Kiefhaber TR. PIP fracturedislocations treatment technique: use of a hemi-hamate resurfacing arthroplasty. Tech Hand Up Extrem Surg 2002;6:185–192.
-
Williams RMM, Kiefhaber TR, Sommerkamp TG, et al. Treatment of unstable dorsal proximal interphalangeal fracture/dislocations using a hemi-hamate autograft. J Hand Surg Am 2003;28:856–865.
You Might Also Like