Rheumatoid Tendon Ruptures: An Intraoperative Masterclass in Hand and Wrist Reconstruction

Key Takeaway
This masterclass provides an exhaustive, real-time guide to managing rheumatoid tendon ruptures. We'll meticulously cover comprehensive anatomy, precise preoperative planning, and granular intraoperative execution of extensor and flexor tendon transfers. Emphasis is placed on identifying underlying pathology, meticulous dissection, and salvaging complications, ensuring fellows gain a deep understanding of this challenging reconstructive surgery.
Introduction and Epidemiology
Rheumatoid arthritis is a systemic, progressive autoimmune disorder characterized by chronic synovial inflammation and subsequent joint and soft tissue destruction. Within the hand and wrist, uncontrolled proliferation of the tenosynovium leads to a cascade of joint destruction, ligamentous laxity, subluxation, and ultimately, attritional tendon rupture. The pathogenesis of tendon rupture in the rheumatoid patient is multifactorial, driven by both direct enzymatic degradation from invasive pannus and mechanical attrition against pathologically altered bony prominences.
The advent of disease-modifying antirheumatic drugs and biologic therapies has dramatically altered the epidemiological landscape of rheumatoid arthritis. Historically, up to thirty percent of patients with long-standing rheumatoid arthritis would experience a spontaneous tendon rupture. While modern pharmacological interventions have significantly reduced the incidence of these catastrophic structural failures, attritional ruptures remain a critical challenge in orthopedic surgery, particularly in patients with refractory disease, delayed diagnosis, or non-compliance with medical management.
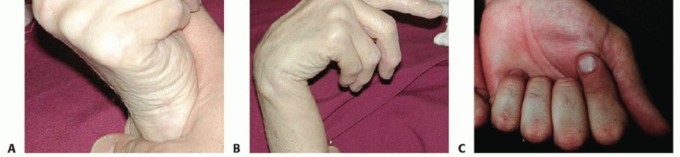
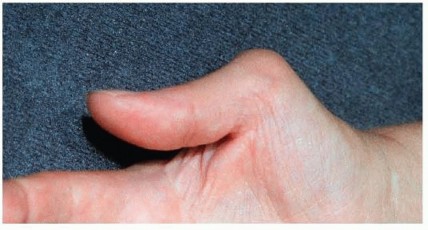
When tendon rupture occurs on the dorsum of the hand or wrist, patients present with an inability to actively extend their digits, severely compromising grip mechanics and hand kinematics. The classic presentation of dorsal tendon rupture follows a sequential ulnar-to-radial pattern, historically termed the Vaughan-Jackson syndrome. This sequence is precipitated by attenuation of the distal radioulnar joint ligaments, leading to dorsal subluxation of the distal ulna. The prominent, often eroded ulnar head acts as an abrasive fulcrum against the overlying extensor tendons, typically beginning with the extensor digiti quinti and progressing radially to involve the extensor digitorum communis of the ring, long, and index fingers.


On the volar aspect of the wrist, attritional flexor tendon ruptures most commonly affect the flexor pollicis longus and the adjacent flexor digitorum profundus to the index or long finger. This specific pattern of volar rupture is known as Mannerfelt syndrome. The mechanical etiology is typically secondary to osteophytic spurring or bony erosion at the scaphotrapezial articulation or the volar radiocarpal joint, which grates against the tendons during active flexion.
The cellular pathophysiology underlying these ruptures involves a complex interplay of cytokines, predominantly tumor necrosis factor alpha and interleukin six, which upregulate matrix metalloproteinases. These enzymes degrade the collagenous extracellular matrix of the tendon substance. Concurrently, the hypertrophic tenosynovium compromises the delicate microvascular supply to the tendon, particularly in watershed zones, rendering the tissue ischemic, friable, and highly susceptible to mechanical shear forces.
Surgical Anatomy and Biomechanics
A thorough understanding of the compartmentalized anatomy of the wrist and the fundamental biomechanics of tendon transfer is paramount for restoring function in the rheumatoid hand. Successful tendon transfer relies on meticulously matching the physiological parameters of the donor muscle to the functional requirements of the recipient tendon.
Dorsal Extensor Compartments
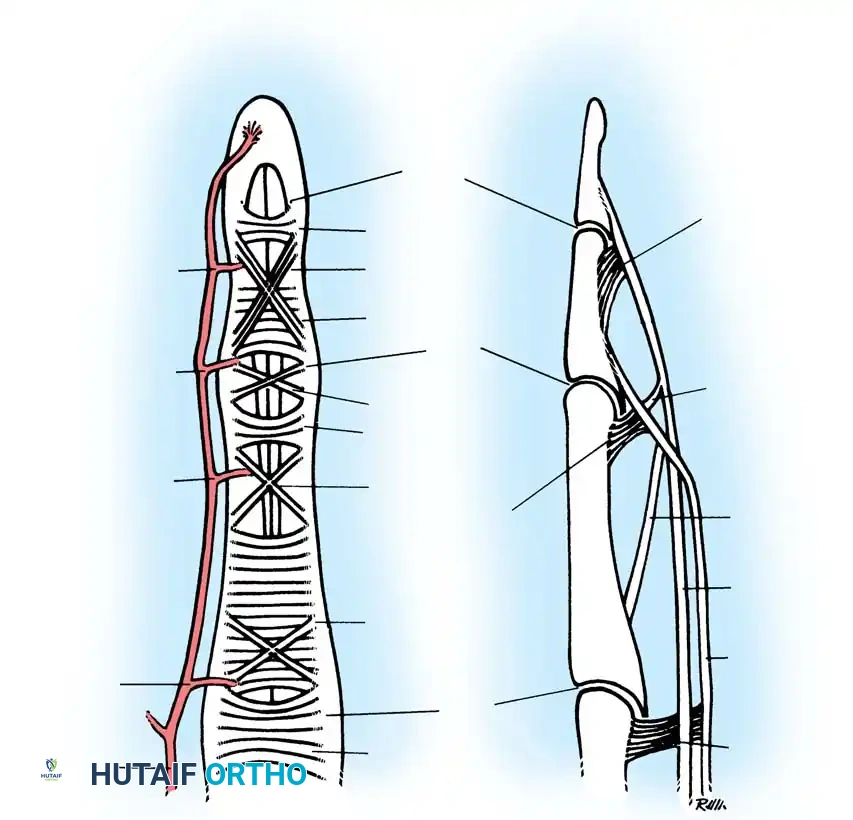
The extensor retinaculum is divided into six distinct fibro-osseous compartments, each lined by tenosynovium susceptible to rheumatoid proliferation. The architectural constraints of these compartments exacerbate the ischemic and mechanical damage caused by tenosynovitis.
The first compartment contains the abductor pollicis longus and extensor pollicis brevis. The abductor pollicis longus frequently presents with multiple slips, predisposing the compartment to critical space reduction and secondary tenosynovitis. The second compartment contains the extensor carpi radialis longus and extensor carpi radialis brevis. These serve as primary wrist extensors and are excellent, robust donor tendons for transfers due to their high force-generating capacity.

The third compartment contains the extensor pollicis longus. It takes an oblique course around Lister's tubercle. The sharp angulation and watershed vascularity make it highly susceptible to spontaneous rupture, both in rheumatoid arthritis and following distal radius fractures. The extensor pollicis longus relies heavily on the intact retinaculum to prevent bowstringing and maintain its moment arm for thumb extension.
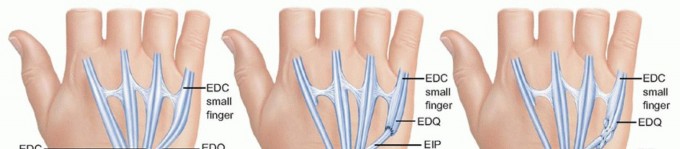
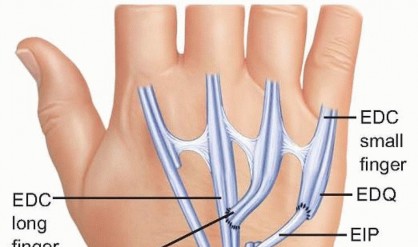
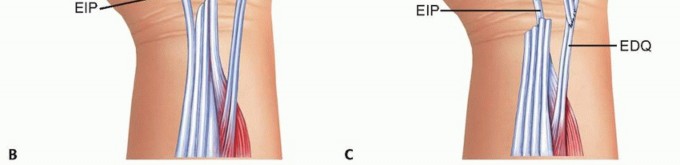
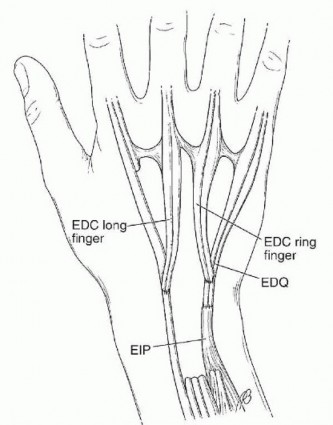
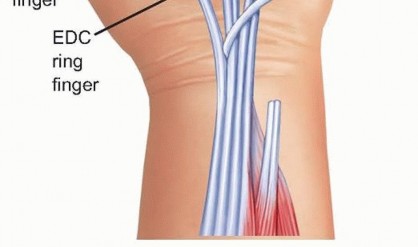
The fourth compartment contains the extensor indicis proprius and the extensor digitorum communis to the digits. The extensor indicis proprius is an independent muscle-tendon unit identifiable by its more distal muscle belly and its position ulnar and deep to the extensor digitorum communis of the index finger. It is a workhorse donor tendon for thumb and digit extension reconstruction.

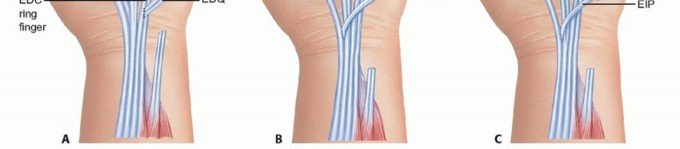
The fifth compartment contains the extensor digiti quinti, which frequently consists of two slips. It lies directly over the distal radioulnar joint, making it the first casualty in Vaughan-Jackson syndrome. The sixth compartment contains the extensor carpi ulnaris, which plays a critical role in dynamic distal radioulnar joint stability. Subluxation of the extensor carpi ulnaris volar to the axis of the wrist transforms it from an extensor to a flexor, contributing to the characteristic radial deviation and volar subluxation of the rheumatoid carpus.
Volar Flexor Anatomy
On the palmar surface, the flexor pollicis longus is the most radial structure entering the carpal tunnel, passing directly over the volar radiocarpal ligaments and the trapeziometacarpal joint. The median nerve, flexor pollicis longus, and the flexor digitorum profundus tendons are tightly packed within the carpal canal. Any bony prominence, particularly from the scaphoid or trapezium, will directly abrade the flexor pollicis longus during the repetitive excursion of thumb flexion.

Principles of Tendon Biomechanics
Tendon transfers must adhere to established biomechanical principles to ensure predictable outcomes. The donor muscle must possess adequate power, typically graded at least four out of five on manual muscle testing, as a transferred muscle will reliably lose one grade of strength postoperatively.
Amplitude, or excursion, is another critical variable. Wrist extensors exhibit approximately thirty-three millimeters of excursion, whereas finger extensors require fifty millimeters, and finger flexors require up to seventy millimeters. When transferring a donor with lesser excursion to a recipient requiring greater excursion, the surgeon must rely on the tenodesis effect of the wrist to augment the effective amplitude.
The line of pull should be as straight as possible. Deviation from a direct vector increases friction, reduces mechanical efficiency, and predisposes the transfer to attenuation or rupture. Furthermore, synergistic transfers are preferred. For example, finger flexion is naturally synergistic with wrist extension; thus, utilizing a wrist extensor to drive finger flexion facilitates easier postoperative cortical re-education.
Indications and Contraindications
Surgical intervention for rheumatoid tendinopathy spans a spectrum from prophylactic tenosynovectomy to complex salvage reconstructions. The decision to proceed with tendon transfer must be integrated into the patient's comprehensive rheumatologic care plan.
The primary indication for tendon transfer is the restoration of lost motor function secondary to complete, irrepairable tendon rupture. Direct primary repair of a rheumatoid tendon rupture is almost universally contraindicated, as the tendon ends are severely degenerated, retracted, and lacking the structural integrity to hold a suture under tension.

Prophylactic surgery is indicated in the presence of tenosynovitis that has been refractory to medical management and local corticosteroid injections for greater than six months. In cases where impending rupture is suspected due to creeping attrition or significant bony prominence, early intervention with tenosynovectomy and skeletal recontouring can prevent the need for subsequent tendon transfers.

Absolute contraindications include active, uncontrolled systemic infection or severe soft tissue compromise over the intended surgical site. Relative contraindications revolve around joint mechanics. A tendon transfer will not move a stiff joint. Passive range of motion must be restored prior to, or concurrently with, the tendon transfer. Severe, uncorrected joint instability, such as an unaddressed caput ulnae or radiocarpal dislocation, will rapidly lead to failure of the transfer due to altered kinematics and recurrent mechanical abrasion.
Operative Versus Non Operative Management Parameters
| Clinical Scenario | Management Strategy | Rationale |
|---|---|---|
| Refractory Tenosynovitis without Rupture | Prophylactic Tenosynovectomy | Prevents enzymatic degradation and ischemic necrosis; preserves native tendon integrity. |
| Isolated EDQ or EDC Rupture | Tendon Transfer (e.g., EIP to EDC) with DRUJ Reconstruction | Restores extension; addressing the DRUJ removes the abrasive fulcrum preventing further sequential ruptures. |
| Multiple Extensor Ruptures (3+ digits) | FDS Transfer via Interosseous Membrane | Local dorsal donors are insufficient; requires robust volar donor to restore mass extension. |
| FPL Rupture (Mannerfelt Syndrome) | FDS Transfer or IP Joint Arthrodesis | Direct repair impossible; arthrodesis preferred if IP joint is severely arthritic; transfer preferred if joint is preserved. |
| Severe Fixed Joint Contracture | Arthrodesis or Arthroplasty | Tendon transfer contraindicated as active motion cannot overcome fixed passive deficits. |
| Poor Soft Tissue Envelope | Flap Coverage Prior to Transfer | Tendon transfers require a well-vascularized, gliding bed to prevent dense adhesion formation. |

Pre Operative Planning and Patient Positioning
Thorough preoperative clinical evaluation is essential to differentiate true tendon rupture from pseudoparalysis caused by joint subluxation, sagittal band rupture, or posterior interosseous nerve palsy. In the rheumatoid hand, volar subluxation of the metacarpophalangeal joints can biomechanically disadvantage the extensor mechanism, mimicking a rupture.

The tenodesis test is a critical diagnostic maneuver. Passive flexion of the wrist should induce passive extension of the digits if the extensor tendons are in continuity. Failure of the digits to extend during passive wrist flexion confirms a discontinuity in the extensor mechanism. Conversely, if the digits extend with wrist flexion but the patient cannot actively extend them, the pathology may lie in the posterior interosseous nerve, though this is rare in isolated rheumatoid presentations without massive synovial cysts at the elbow.

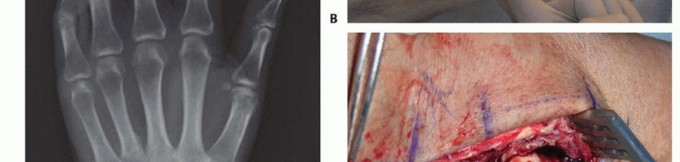
Radiographic evaluation must include standard posteroanterior, lateral, and oblique views of the hand and wrist. The surgeon must scrutinize the distal radioulnar joint for dorsal subluxation of the ulna, the carpus for ulnar translocation and radiocarpal erosion, and the metacarpophalangeal joints for subluxation. Advanced imaging, such as magnetic resonance imaging or high-resolution ultrasonography, can precisely delineate the extent of tenosynovitis and confirm the exact number of ruptured tendons, aiding in donor selection.
Patient Positioning and Operating Room Setup
The patient is positioned supine with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Loupe magnification is highly recommended for meticulous dissection of the tenosynovium and precise tendon weaving.
The surgical field must be prepped and draped to allow visualization of the entire forearm and hand, ensuring the surgeon can assess the tenodesis effect intraoperatively. A sterile marking pen is used to outline the planned incisions, which must be designed to avoid crossing flexion creases at right angles and to preserve broad skin flaps, as rheumatoid skin is notoriously thin and prone to necrosis.

Detailed Surgical Approach and Technique
The surgical execution of tendon transfers in the rheumatoid patient is a multi-stage procedure that demands meticulous attention to soft tissue handling, skeletal stabilization, and biomechanical tensioning. The following sections detail the operative steps for addressing both dorsal and volar ruptures.
Management of the Extensor Mechanism and Vaughan Jackson Syndrome
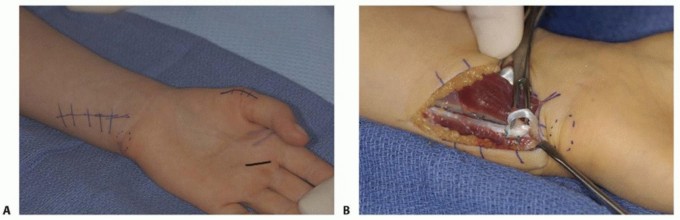
The approach begins with a dorsal longitudinal incision centered over the wrist, extending from the distal third of the forearm to the mid-metacarpal level. The incision may be slightly curved to minimize scar contracture. Full-thickness fasciocutaneous flaps are elevated to expose the extensor retinaculum.

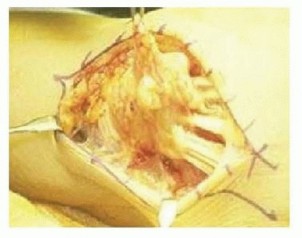
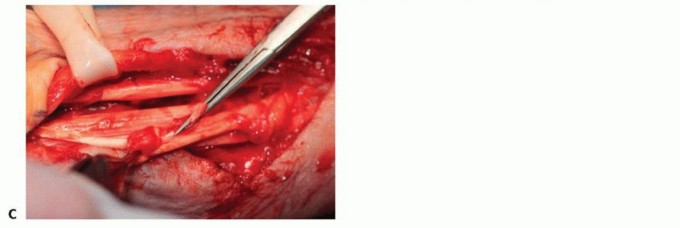
The extensor retinaculum is divided. A common technique involves a step-cut division or reflecting the retinaculum from the ulnar to the radial side, preserving a portion to prevent postoperative bowstringing of the extensor carpi radialis longus and brevis. A radical tenosynovectomy is then performed. The hypertrophic, invasive pannus is meticulously excised from the remaining intact tendons using sharp dissection and rongeurs. Care must be taken to preserve the epitenon wherever possible.
Before addressing the tendon ruptures, the underlying skeletal pathology must be neutralized. In Vaughan-Jackson syndrome, the prominent distal ulna must be addressed to prevent rupture of the transferred tendons. A Darrach procedure (resection of the distal ulna) or a Sauvé-Kapandji procedure (distal radioulnar joint arthrodesis with proximal ulnar pseudoarthrosis) is performed. The Darrach procedure is technically simpler but can lead to ulnar stump instability; thus, careful stabilization of the ulnar stump using the dorsal capsule or a portion of the extensor carpi ulnaris sheath is mandatory.
Tendon Transfer Strategies for Extensor Ruptures
The strategy for reconstruction depends entirely on the number of ruptured tendons.
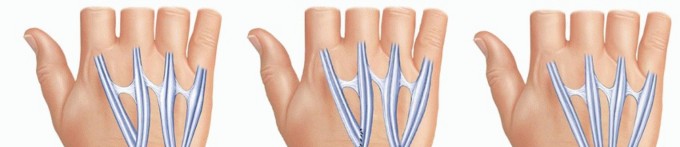
For an isolated extensor digiti quinti rupture, a side-to-side tenodesis is typically sufficient. The distal stump of the extensor digiti quinti is woven into the intact extensor digitorum communis of the ring finger.

When two tendons are ruptured, typically the extensor digiti quinti and the extensor digitorum communis to the ring finger, an independent donor is required. The extensor indicis proprius is the donor of choice. The extensor indicis proprius is identified at the level of the index metacarpophalangeal joint, located ulnar and deep to the extensor digitorum communis. It is transected distally, taking care to repair the extensor hood to prevent an extensor lag of the index finger. The extensor indicis proprius is then withdrawn proximally to the wrist and rerouted towards the ulnar digits.

The transfer is executed using a Pulvertaft weave. The recipient tendons (extensor digiti quinti and ring extensor digitorum communis) are grouped together. The extensor indicis proprius is woven through the recipient tendons at least three times. Tensioning is critical. The transfer must be set tighter than the resting tension of the adjacent intact digits, as the muscle will inevitably stretch and lose some tension postoperatively. The wrist is held in thirty degrees of extension, and the metacarpophalangeal joints are held in zero degrees of extension during the tensioning and suturing process.

For three or more ruptured extensor tendons, local dorsal donors are insufficient. A volar donor must be utilized. The flexor digitorum superficialis of the ring or long finger is highly effective. The flexor digitorum superficialis is harvested at the level of the proximal phalanx through a volar incision, preserving the flexor digitorum profundus and the A2 and A4 pulleys. The tendon is withdrawn into the distal forearm.
Routing the flexor digitorum superficialis to the dorsum can be achieved either subcutaneously around the radial border of the forearm or directly through the interosseous membrane. The interosseous route provides a more
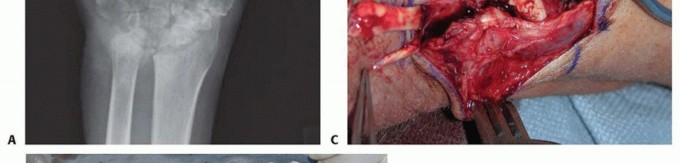
Clinical & Radiographic Imaging





You Might Also Like