Vascularized Bone Grafting of Avascular Scaphoid Nonunions

Introduction and Epidemiology
Scaphoid fractures represent a significant proportion of all carpal bone fractures, accounting for approximately 60% of all such injuries. Despite appropriate initial management, which often involves cast immobilization or percutaneous fixation, nonunions occur in up to 15% of scaphoid fractures. The clinical implications of a scaphoid nonunion are substantial, often leading to chronic wrist pain, weakness, reduced range of motion, and a predictable progression towards degenerative changes, collectively termed scaphoid nonunion advanced collapse (SNAC) wrist. The progression to SNAC wrist typically initiates at the radioscaphoid articulation, characterized clinically by specific tenderness at the radial styloid-scaphoid interface.
The etiology of scaphoid nonunion is multifactorial, frequently stemming from delayed diagnosis and treatment, inadequate immobilization, significant fracture displacement, or involvement of the proximal pole. A critical predisposing factor, particularly for recalcitrant nonunions, is the development of avascular necrosis (AVN) of the proximal scaphoid pole. This compromised vascularity significantly impedes bone healing, necessitating specialized reconstructive strategies such as vascularized bone grafting. The rationale for vascularized bone grafting in these challenging cases is to introduce a viable, biologically active graft with an intact blood supply, thereby enhancing osteogenesis, improving graft incorporation, and potentially reversing or preventing AVN of the proximal fragment.
The economic burden and impact on patient quality of life further underscore the importance of effective management strategies for scaphoid nonunions. Early identification of risk factors and appropriate surgical intervention are paramount to preserving wrist function and preventing long-term degenerative sequelae.
FIG 1 • A. Tenderness at the anatomic snuffbox is a classic finding of scaphoid nonunion. B. The radial styloid-scaphoid interface is the earliest site of degenerative change in scaphoid nonunions, and patients will often display tenderness at that location. C. The distal pole of the scaphoid is palpable at the base of the thumb on the palmar aspect of the wrist. Tenderness is a consistent finding in scaphoid nonunion.
Surgical Anatomy and Biomechanics
A thorough understanding of scaphoid anatomy, particularly its intricate vascular supply and biomechanical role, is fundamental to the successful management of scaphoid nonunions. The scaphoid, due to its unique anatomical position and blood supply, is inherently prone to nonunion and avascular necrosis.
Scaphoid Vascularity
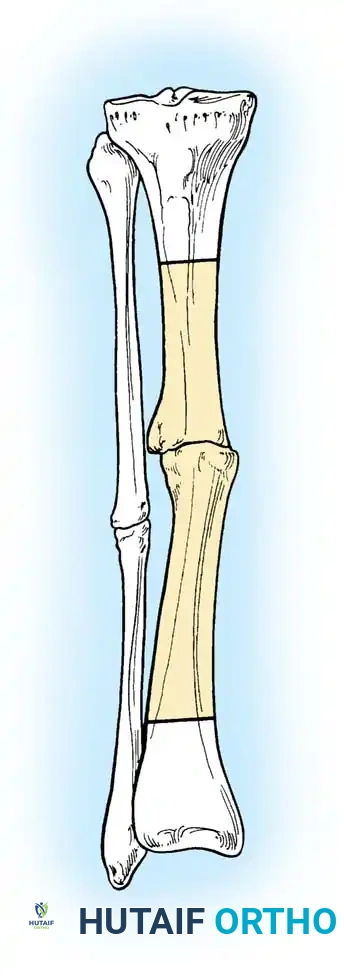
The scaphoid’s blood supply is predominantly retrograde, traversing in a distal-to-proximal direction. The primary arterial supply emanates from branches of the radial artery, specifically the superficial palmar branch, the dorsal carpal branch, and the palmar carpal branch. The dorsal carpal branch of the radial artery provides the dominant supply, giving rise to numerous intraosseous vessels that penetrate the dorsal ridge of the scaphoid and supply approximately 70-80% of the bone, including the critical proximal pole. The palmar carpal branch contributes supply to the distal tubercle and a smaller portion of the waist.
A significant vulnerability arises from the fact that the intraosseous vessels traverse the scaphoid to supply the proximal pole. Unlike other carpal bones, the scaphoid lacks significant soft tissue attachments over much of its surface, meaning its blood supply largely relies on these intrinsic vessels. Consequently, a fracture through the scaphoid waist can disrupt the primary blood supply to the proximal pole, leading to ischemia and avascular necrosis. Studies indicate that in approximately 30% of scaphoids, there is either a single, tenuous, or no vascular channel definitively reaching the proximal pole, further predisposing this segment to AVN following fracture.
The concept of vascularized bone grafting relies on harvesting bone with an attached, identifiable vascular pedicle. Several sources of vascularized bone graft have been identified, primarily from the distal radius, leveraging its robust arterial network. Animal studies involving vascularized bone grafts have unequivocally demonstrated a significant increase in local blood flow and osteogenic activity compared to nonvascularized grafts, providing a strong biological rationale for their application in avascular nonunions.

FIG 2 • Diagram illustrating the intrinsic blood supply to the scaphoid, highlighting the critical distal-to-proximal retrograde flow.
Scaphoid Biomechanics and Kinematics
The scaphoid plays a pivotal role in carpal kinematics, acting as a link between the proximal and distal carpal rows. It contributes to both dart-thrower's motion and the stability of the wrist. A nonunion of the scaphoid disrupts this intricate kinematic chain, leading to altered load transmission across the carpus. This instability can manifest as a dorsal intercalated segmental instability (DISI) pattern, where the lunate extends dorsally. Over time, abnormal stresses on the radioscaphoid and midcarpal joints lead to progressive degenerative arthritis, starting at the radial styloid and subsequently involving the scaphocapitate and lunocapitate articulations. This degenerative cascade is precisely what vascularized bone grafting aims to prevent or halt by achieving durable union and restoring carpal stability.
The presence of a humpback deformity, frequently associated with scaphoid nonunions, exacerbates abnormal kinematics and predisposes to progressive carpal collapse. Surgical reconstruction must not only achieve union but also restore scaphoid length and alignment to normalize wrist mechanics.
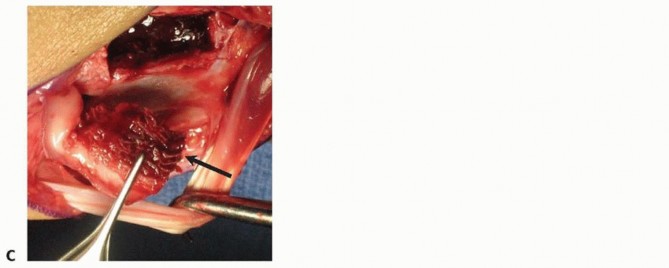
FIG 3 • Lateral radiographic view demonstrating the "humpback" deformity often associated with scaphoid nonunion and its impact on carpal alignment.
Indications and Contraindications
Vascularized bone grafting (VBG) is a specialized technique reserved for complex scaphoid nonunions, particularly those where conventional non-vascularized grafting has failed or is unlikely to succeed. Careful patient selection is crucial for optimizing outcomes.
Indications for Vascularized Bone Grafting
The primary indications for VBG stem from the compromised biological environment often found in recalcitrant scaphoid nonunions. These include:
- Proximal pole avascular necrosis (AVN): This is arguably the most compelling indication. When significant AVN of the proximal fragment is evident on MRI or CT, a VBG provides a direct vascular supply to enhance healing.
- Established scaphoid nonunion with bone loss and/or carpal collapse: When there is significant bone loss at the nonunion site, necessitating a structural graft, a vascularized graft can improve structural integrity and healing potential. Carpal collapse, often manifested as a dorsal intercalated segmental instability (DISI) pattern, indicates chronic instability that requires robust reconstruction.
- Failed conventional non-vascularized bone grafting: Cases where previous attempts with non-vascularized grafts have failed to achieve union, especially in the presence of AVN, often warrant a VBG.
- Large scaphoid cysts at the nonunion site: Cysts indicate a poor biological environment; a vascularized graft can stimulate healing and fill the defect.
- Revision surgery for scaphoid nonunion: In complex revision scenarios, a VBG offers enhanced biological potential for successful union.
- Significant smoking history or other comorbidities affecting bone healing: While not an absolute indication, a VBG may be considered in patients with factors known to impede bone healing, given its superior biological activity.

FIG 4 • Coronal T1-weighted MRI demonstrating findings consistent with avascular necrosis of the proximal scaphoid pole, a primary indication for vascularized bone grafting.
Contraindications for Vascularized Bone Grafting
While VBG offers significant advantages, certain conditions may contraindicate its use:
- Severe degenerative arthritis of the wrist (SNAC wrist Grade III or IV): If there is advanced arthritis involving the midcarpal or radiocarpal joints beyond the initial radioscaphoid interface, a scaphoid reconstruction may not significantly improve symptoms or function, and wrist salvage procedures (e.g., proximal row carpectomy, four-corner fusion, total wrist arthrodesis) may be more appropriate.
- Active infection: Any active infection in the wrist is an absolute contraindication, requiring eradication before any reconstructive surgery.
- Poor overall patient health or severe comorbidities: Patients with conditions that preclude major surgery or compromise graft viability (e.g., severe peripheral vascular disease, uncontrolled diabetes, poor nutritional status) may not be suitable candidates.
- Unrealistic patient expectations: Patients must understand the potential for prolonged rehabilitation and the possibility of persistent symptoms or the need for further surgery.
- Extensive bone loss rendering reconstruction impossible: In rare cases of extreme scaphoid destruction, reconstruction might not be feasible, making salvage procedures the only option.
- Insufficient vascular pedicle for graft harvest: Preoperative assessment may reveal an inadequate or compromised vascular supply at the donor site, preventing safe graft harvest.
Summary of Operative vs Non Operative Indications
| Indication Type | Operative Indications for Vascularized Bone Grafting | Non-Operative or Alternative Surgical Indications |
|---|---|---|
| Primary Indication | Proximal pole AVN confirmed on MRI/CT. | Non-displaced, stable nonunions without AVN (trial of immobilization or non-vascularized grafting). |
| Bone Loss/Deformity | Significant bone loss, humpback deformity, or DISI pattern requiring structural support. | Minimal bone loss, stable alignment (non-vascularized grafting). |
| Revision Surgery | Failed previous non-vascularized grafting, especially with AVN. | First-time intervention for simple nonunion without AVN. |
| Patient Factors | High-demand patients, smokers, or those with comorbidities affecting healing (relative indication). | Low-demand patients, significant comorbidities precluding surgery (conservative management). |
| Arthritis | None or early SNAC (Grade I/II). | Advanced SNAC (Grade III/IV) (salvage procedures: PRC, 4CF, arthrodesis). |
Pre Operative Planning and Patient Positioning
Preoperative planning for scaphoid nonunion with vascularized bone grafting is an intricate process demanding meticulous attention to clinical, radiographic, and technical details to ensure optimal outcomes. This comprehensive approach is paramount for patient safety and surgical efficacy.
Clinical and Radiographic Assessment
Clinical Evaluation: A thorough patient history is indispensable, focusing on the mechanism of injury, the initial management, any prior surgical interventions, and the chronology of symptoms. Critical elements include pain characteristics (location, intensity, aggravating factors), functional limitations (grip strength, range of motion deficits, impact on activities of daily living), and identification of co-morbidities such as smoking, diabetes, or metabolic bone disease that may impede bone healing. Physical examination must delineate areas of localized tenderness, classically the anatomic snuffbox and scaphoid tubercle (Fig 1), and often the radial styloid-scaphoid interface in cases with early degenerative changes. Assessment of wrist range of motion (flexion, extension, radial and ulnar deviation, forearm pronation/supination) and comparative grip strength provide baseline functional data. A detailed neurovascular assessment of the entire upper extremity, including Allen's test, is imperative to ensure adequate collateral circulation, especially given the planned manipulation of radial artery branches.
Radiographic Imaging: A multimodal imaging strategy is crucial for precise nonunion characterization:
- Plain Radiographs: Standard wrist series including posteroanterior (PA) with ulnar deviation, lateral, oblique (45° pronated oblique), and dedicated scaphoid views are the initial cornerstone. These films provide initial insights into the presence of nonunion, fracture pattern, displacement, degree of bone loss, presence of cystic changes, and identification of a dorsal intercalated segmental instability (DISI) pattern or "humpback" deformity. Measurements such as the scapholunate angle (>60°) and radiolunate angle (>15°) are critical for assessing carpal collapse. Early signs of radioscaphoid arthrosis, such as radial styloid beaking, are carefully documented.

FIG 5 • Preoperative plain radiograph (PA view) of a wrist revealing a scaphoid waist nonunion with evidence of proximal pole sclerosis and a widened fracture gap. - Computed Tomography (CT) Scan: Fine-cut CT scans (typically 0.625mm or 1mm slices) with multiplanar reconstructions (coronal, sagittal, axial) are indispensable. This modality offers superior detail regarding the nonunion site, extent of sclerosis, presence and size of cystic lesions, and precise quantification of bone loss. It is critical for confirming the absence of bridging trabeculae across the nonunion and for a definitive assessment of the overall scaphoid morphology, allowing for three-dimensional appreciation of any associated deformity. This information guides graft sizing and contouring.
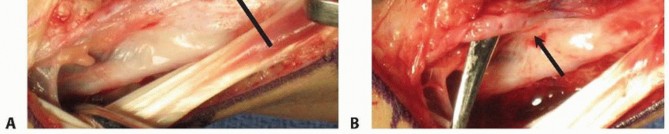
FIG 6 • Coronal CT reconstruction demonstrating a sclerotic proximal pole and a distinct nonunion gap in a chronic scaphoid fracture, with associated cystic changes. - Magnetic Resonance Imaging (MRI): While CT excels in bone detail, MRI provides invaluable information regarding the vascularity of the scaphoid fragments, particularly the proximal pole. Low signal intensity on T1-weighted images and high signal intensity on T2-weighted or STIR sequences within the proximal pole marrow cavity are highly suggestive of avascular necrosis (AVN). MRI also helps to identify associated soft tissue pathology or degenerative changes not readily apparent on plain films or CT.

FIG 4 • Coronal T1-weighted MRI demonstrating findings consistent with avascular necrosis of the proximal scaphoid pole, characterized by low signal intensity, a primary indication for vascularized bone grafting. - Arteriography/Angiography: Preoperative angiography is not routinely performed for all vascularized bone grafts but may be considered in specific circumstances. These include cases with a history of prior wrist surgery that could have altered the regional vascular anatomy, suspected vascular anomalies, or when utilizing free vascularized grafts where recipient vessel identification is paramount. Doppler ultrasound mapping can be a non-invasive adjunct for identifying the precise course of specific radial artery branches.
Graft Selection and Donor Site Considerations
The selection of the appropriate vascularized bone graft is tailored to the specific anatomical and biological requirements of the scaphoid nonunion. Key considerations include:
- Location of the Nonunion: Proximal pole and waist nonunions with significant AVN often benefit from dorsally based grafts. Volar nonunions or those with primarily volar bone loss may favor volar-based grafts.
- Extent of Bone Loss: Grafts requiring significant structural support to bridge a defect or correct a deformity (e.g., humpback) will require a larger corticocancellous segment.
- Surgeon Preference and Experience: Familiarity with a particular graft harvest technique influences selection.
The most common donor sites are local pedicled grafts from the distal radius, capitalizing on its robust arterial supply:
- 1,2-Intercompartmental Supraretinacular Artery (1,2-ICSRA) Graft (Dorsal Radius): This pedicled graft, based on the 1,2-ICSRA (a branch of the radial artery originating between the first and second extensor compartments), offers a reliable vascular supply and provides excellent structural support. It is highly versatile for proximal pole AVN and waist nonunions with humpback deformity. Its predictable anatomy and cortical inclusion make it suitable for screw fixation.

FIG 7 • Anatomical dissection showing the 1,2-intercompartmental supraretinacular artery (1,2-ICSRA) pedicle coursing proximally along the dorsal radius, providing the vascular supply for this graft. - Dorsal Radial Artery (DRA) Graft (Zaidemberg Graft): This graft, also from the dorsal distal radius, is based on a smaller perforator from the dorsal branch of the radial artery, typically emerging near the first dorsal compartment. It provides a smaller, predominantly cancellous graft, often preferred for filling smaller defects, stimulating osteogenesis in non-structural defects, or augmenting other grafts.
- Pronator Quadratus (PQ) Pedicled Graft (Volar Radius): Harvested from the volar aspect of the distal radius, this graft maintains a vascular pedicle from the pronator quadratus artery (a branch of the anterior interosseous artery). It is particularly advantageous for volar bone defects or nonunions requiring a volar approach, offering both structural and biological contribution.

FIG 8 • Illustration of the pronator quadratus pedicled graft harvest from the volar aspect of the distal radius, depicting the muscle flap and its vascularized bone island.
Graft Sizing: The precise size and shape of the graft are determined by preoperative templating using CT images to accurately match the scaphoid defect and facilitate optimal anatomical restoration.
Operating Room Setup and Patient Positioning
Operating Room Configuration: The operating room must be meticulously prepared. A stable hand table is essential, allowing unhindered access to the entire forearm and wrist. A C-arm image intensifier is mandatory for intraoperative radiographic assessment of reduction and fixation. Standard wrist surgical instrumentation, including small osteotomes, rongeurs, curettes, and a high-speed burr, should be readily available. Cannulated headless compression screw sets (e.g., Herbert, Acutrak, Barouk) of various lengths and diameters are required. High-magnification surgical loupes (2.5x to 4.0x) are strongly recommended for precise dissection and preservation of the delicate vascular pedicle. A Doppler probe for intraoperative vascular assessment can be invaluable.
Patient Positioning: The patient is positioned supine on the operating table. The affected arm is abducted and placed on a stable hand table, ensuring unimpeded access to both the dorsal and volar aspects of the distal forearm and wrist. This flexibility is critical for simultaneous graft harvest and scaphoid exposure if two surgical fields are to be utilized. A pneumatic tourniquet is applied to the upper arm, and the limb is prepared and draped in a sterile fashion from the elbow to the fingertips. The draping should allow for full pronation and supination of the forearm to facilitate optimal exposure and graft delivery.
Detailed Surgical Approach and Technique
The surgical technique for vascularized bone grafting of scaphoid nonunions demands meticulous attention to detail, from careful debridement to precise graft harvest, anatomical reduction, and stable fixation. The choice of surgical approach (dorsal or volar) and specific graft type is dictated by the characteristics of the nonunion, the extent of bone loss, the presence of avascular necrosis, and surgeon preference.
General Principles of Nonunion Debridement and Preparation
Irrespective of the chosen approach or graft, several fundamental principles must be rigorously adhered to when preparing the nonunion site:
- Surgical Exposure: Adequate surgical exposure of the nonunion site is paramount. This requires carefully planned incisions and soft tissue dissection to visualize the entire nonunion, associated cysts, and surrounding carpal anatomy while protecting neurovascular structures.
- Fibrous Tissue Excision: All interposing fibrous tissue at the nonunion site must be meticulously excised. This typically involves using a fine scalpel, curettes, and small rongeurs to create a clear surgical field.
- Sclerotic Bone Debridement: Sclerotic bone, indicative of avascularity and poor healing potential, must be thoroughly debrided until healthy, punctate bleeding cancellous bone is exposed on both the proximal and distal scaphoid fragments. A high-speed burr is often employed for this purpose, alongside fine curettes and osteotomes. Any associated intramedullary cysts are also curetted extensively. This biological preparation creates an optimal environment for graft incorporation.

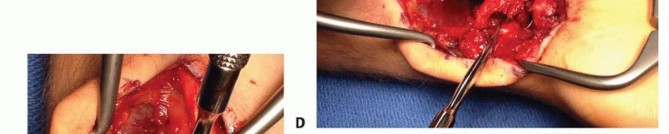
FIG 9 • Intraoperative view showing meticulous debridement of the nonunion site, removing fibrous tissue and sclerotic bone until viable, bleeding bone is exposed on both scaphoid fragments. - Correction of Deformity: If a "humpback" deformity (increased scapholunate angle, volar flexion of the distal fragment) or significant carpal collapse (DISI) is present, the scaphoid must be anatomically reduced and its length and alignment restored. This often necessitates gentle longitudinal distraction of the wrist (e.g., with a mini-distractor or Finger Traps) and direct manipulation of the scaphoid fragments. Temporary K-wires can be used to maintain the corrected alignment while the graft is prepared and inserted.
- Recipient Bed Preparation: A precisely shaped trough or cavity is prepared within the debrided scaphoid fragments to perfectly accommodate the harvested vascularized bone graft. The recipient bed must maximize bone-to-bone contact to facilitate healing and ensure that the vascular pedicle can lie without tension or compression.
Dorsal Approach to the Scaphoid and Graft Harvest (1,2-ICSRA)
The dorsal approach is widely utilized for scaphoid waist and proximal pole nonunions, particularly those with a "humpback" deformity, as it offers direct visualization for deformity correction and allows access to the reliable 1,2-ICSRA graft.
Surgical Exposure of the Scaphoid
- Incision: A dorsal longitudinal or slightly curvilinear incision is made over Lister's tubercle, centered over the scaphoid, extending approximately 4-6 cm proximally from the wrist crease and 2-3 cm distally.
- Extensor Compartment Access: The subcutaneous tissues are carefully dissected. Lister's tubercle is identified. The extensor pollicis longus (EPL) tendon (third dorsal compartment) is released from its groove and retracted ulnarly. This exposes the floor of the second dorsal compartment (extensor carpi radialis longus and brevis, ECRL/ECRB tendons).
- Capsulotomy: A longitudinal capsulotomy is performed between the second and third extensor compartments to expose the dorsal aspect of the scaphoid and the radioscaphoid articulation. Care is taken to protect the posterior interosseous nerve (PIN), which usually terminates in the dorsal wrist capsule. A portion of the dorsal intercarpal ligament may need to be incised or released to gain adequate access to the nonunion site.

FIG 10 • Dorsal approach to the wrist, showing exposure of the scaphoid nonunion site between the second and third extensor compartments after retraction of the EPL tendon.
Harvest of the 1,2-ICSRA Graft
- Separate Incision (Optional): While a single incision can be used, a slightly more radial or separate, shorter curvilinear incision just radial to the dorsal midline of the distal radius, extending approximately 4-5 cm proximally from the radial styloid, is often preferred for graft harvest to optimize pedicle length and mobility.
- Pedicle Identification: Dissection proceeds deep to the extensor retinaculum, between the first (abductor pollicis longus, APL; extensor pollicis brevis, EPB) and second (ECRL, ECRB) dorsal compartments. The 1,2-ICSRA typically emerges from the radial artery at or just distal to the level of the radial styloid and runs proximally within the periosteum and overlying fascial envelope of the distal radius. This artery, along with its venous concomitants, is meticulously identified and carefully dissected proximally as far as necessary to achieve adequate pedicle length and mobility for rotation to the scaphoid, while preserving its integrity. Magnification (loupes) is highly recommended.

FIG 11 • Intraoperative image demonstrating the meticulous harvest of a 1,2-ICSRA vascularized bone graft from the dorsal distal radius, with careful preservation of the vascular pedicle. - Bone Island Harvest: Once the pedicle is adequately mobilized, a rectangular or trapezoidal corticocancellous bone graft is precisely harvested from the dorsal aspect of the distal radius, ensuring the entire vascular pedicle remains attached to the bone island. The dimensions of the graft are precisely tailored to the preoperatively templated scaphoid defect, typically measuring 1.0-1.5 cm in length, 0.5-0.8 cm in width, and 3-5 mm in thickness, utilizing a small osteotome or oscillating saw. The donor site defect on the radius can be filled with cancellous bone graft or bone substitute if desired, though it often heals spontaneously.
Graft Insertion and Fixation
- Recipient Site Preparation: The scaphoid nonunion site, previously debrided and aligned, is now ready to receive the graft. A precise trough is created to ensure a snug fit.
- Graft Placement: The vascularized graft is carefully transferred to the scaphoid nonunion site. The pedicle must be handled with utmost gentleness, ensuring it is not twisted, kinked, or subjected to excessive tension or compression. The graft is positioned to bridge the defect, restore scaphoid length, and correct any deformity. Confirm vascularity with a handheld Doppler.
- Internal Fixation: Rigid internal fixation is critical. This is most commonly achieved with cannulated headless compression screws (e.g., Herbert, Acutrak, Barouk screws). A guide wire is carefully placed across the scaphoid nonunion, traversing the vascularized graft and engaging both the proximal and distal scaphoid fragments. Intraoperative fluoroscopy confirms ideal guide wire position, reduction, and screw trajectory. The screw provides interfragmentary compression, enhancing stability and promoting union. K-wires may be used as an alternative or adjunct in specific cases.
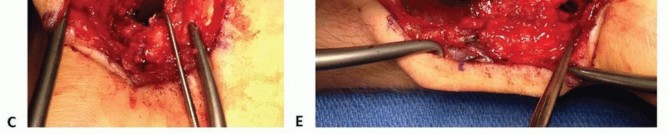
FIG 12 • Post-operative radiograph showing a scaphoid nonunion united with a 1,2-ICSRA vascularized bone graft and fixed with a headless compression screw providing interfragmentary compression.

FIG 13 • Different angle post-operative radiograph demonstrating the well-seated vascularized graft and robust internal fixation. - Closure: The dorsal wrist capsule and extensor retinaculum are repaired. The EPL tendon is repositioned. The skin and subcutaneous tissues are closed in layers, ensuring no pressure on the vascular pedicle. A bulky soft dressing and a long arm thumb spica splint are applied.
Volar Approach to the Scaphoid and Graft Harvest (Pronator Quadratus)
The volar approach is indicated for scaphoid nonunions, particularly those involving the waist or distal pole, with significant volar bone loss, or when a dorsal approach is less advantageous. The pronator quadratus (PQ) pedicled graft is a reliable option from this approach.
Surgical Exposure of the Scaphoid
- Incision: A curved incision is made along the radial border of the flexor carpi radialis (FCR) tendon, extending from the distal forearm across the wrist crease to the thenar eminence.
- Dissection: The FCR sheath is incised, and the FCR tendon is retracted ulnarly. The radial artery and its branches are carefully identified and retracted radially, protecting them from injury. The median nerve, typically lying ulnar to the FCR, is also identified and protected. The radial sensory nerve branches must also be protected during skin incision.
- Capsulotomy: A longitudinal capsulotomy is performed over the scaphoid, carefully incising the radioscaphocapitate and short radiolunate ligaments if necessary, taking care to preserve any radial artery branches supplying the scaphoid distally.
Harvest of the Pronator Quadratus Pedicled Graft
- Exposure of PQ: The pronator quadratus muscle is exposed on the volar aspect of the distal radius after retracting the FCR tendon and radial artery.
- Pedicle Identification: The vascular pedicle to the pronator quadratus, typically branches from the anterior interosseous artery or sometimes directly from the radial artery, is identified and carefully dissected.
- Bone Island Harvest: A rectangular corticocancellous graft is harvested from the volar aspect of the distal radius, maintaining its attachment to a flap of pronator quadratus muscle and its vascular pedicle. The size and shape are customized to the scaphoid defect. The entire flap, including bone and muscle, is then gently mobilized and rotated into the scaphoid nonunion site.

FIG 8 • Illustration of the pronator quadratus pedicled graft harvest from the volar aspect of the distal radius, depicting the muscle flap and its vascularized bone island. (This image might be repetitive with a previous entry, ensuring careful image placement and numbering)
Graft Insertion and Fixation
- Preparation of Recipient Site: The scaphoid nonunion is debrided as per the general principles, and the fragments are reduced. A precisely sized trough is created to accept the PQ graft.
- Graft Placement: The PQ flap with its attached bone is meticulously rotated and seated into the scaphoid defect, ensuring the vascular pedicle is not compromised.
- Internal Fixation: Rigid internal fixation, typically with a headless compression screw, is performed. The volar approach often facilitates placement of a volar-to-dorsal screw, which may be beneficial biomechanically. Fluoroscopy is used to confirm accurate reduction and hardware placement.
- Closure: The FCR sheath, wrist capsule, and skin are closed in layers. A volar long arm thumb spica splint is applied.
Other Vascularized Grafts and Fixation Considerations
Dorsal Radial Artery (DRA) Graft (Zaidemberg Graft)
The Zaidemberg graft is another dorsally harvested vascularized graft, but its pedicle arises from a smaller perforator of the dorsal branch of the radial artery. It provides a smaller, more cancellous graft, less structural but rich in osteogenic cells. It is suitable for filling smaller defects or supplementing other grafts. The harvest technique is similar to the 1,2-ICSRA, emphasizing careful microdissection of the pedicle.
Free Vascularized Bone Grafts
In cases of massive scaphoid bone loss, failed previous attempts, or when local pedicled grafts are deemed insufficient, free vascularized bone grafts may be considered. Common donor sites include the medial femoral condyle (which provides a vascularized cancellous graft with excellent osteogenic potential) or a free fibula graft (for larger structural defects). These grafts necessitate microvascular anastomosis to suitable recipient vessels in the forearm (e.g., radial artery and concomitant veins), requiring specialized microvascular surgical expertise.
Fixation Principles
Irrespective of the graft type or surgical approach, rigid internal fixation is paramount for achieving successful union. Headless compression screws are preferred due to their ability to provide axial compression across the nonunion site, minimize implant prominence, and allow for earlier rehabilitation. The screw should ideally be centrally placed within the scaphoid, crossing the graft and engaging both the proximal and distal scaphoid fragments. This interfragmentary compression is crucial for stability and promoting bone healing. K-wires may be used for temporary reduction or as definitive fixation in specific situations, but they generally require longer immobilization periods. The primary objective of fixation is to create a stable biomechanical environment that optimizes the biological potential of the vascularized graft.
Complications and Management
Despite meticulous surgical technique, complications can arise following vascularized bone grafting for scaphoid nonunions. Prompt recognition and appropriate management are crucial for salvage and optimizing functional outcomes.
Intraoperative and Early Postoperative Complications
- Pedicle Compromise: This is the most critical intraoperative and early postoperative concern, directly impacting graft viability. Kinking, stretching, tension, compression, or direct iatrogenic injury to the vascular pedicle can lead to graft ischemia and failure. Management: Intraoperatively, meticulous handling, adequate soft tissue release, and gentle retraction are paramount. Direct visualization under magnification and intraoperative assessment of pedicle flow (e.g., with a handheld Doppler probe or observation of capillary refill) are essential. If compromise is suspected, immediate exploration and release of any constricting structures are necessary.
- Hemorrhage and Hematoma: Meticulous hemostasis throughout the procedure is required. Postoperative hematoma formation can cause significant pain, swelling, and potentially compromise the vascular pedicle by extrinsic compression. Management: Careful attention to hemostasis, judicious use of electrocautery, and prophylactic drain placement in selected cases can mitigate risk. Evacuation of a significant hematoma may be necessary.
- Infection: Superficial or deep wound infection can occur, potentially compromising graft integration. Management: Superficial infections typically respond to oral antibiotics. Deep infections require aggressive surgical debridement, irrigation, cultures, and targeted intravenous antibiotic therapy. In severe cases, graft removal may be unavoidable, leading to persistent nonunion.
- Nerve Injury: Injury to sensory nerve branches (e.g., superficial radial nerve branches during dorsal exposure) is a risk, leading to numbness, dysesthesia, or painful neuroma formation. Motor nerve injury (e.g., posterior interosseous nerve terminal branches during dorsal approach, anterior interosseous nerve during volar approach) is less common but more debilitating. Management: Meticulous dissection, clear identification, and protection of all anatomical structures are imperative. Neuromas may require surgical excision or neurolysis.
- Hardware-related Issues: Malpositioning of screws or K-wires can result in intra-articular penetration, adjacent tendon irritation, impingement, or inadequate fixation leading to instability. Management: Intraoperative fluoroscopy is critical for confirming proper reduction and hardware placement. If malposition is identified postoperatively and is symptomatic or detrimental to union, revision of hardware may be required.
Late Complications and Salvage Strategies
- Persistent Nonunion: This is the most significant long-term complication, occurring if the graft fails to incorporate, or if the scaphoid fragments do not achieve bony union. Factors contributing include inadequate debridement, unstable fixation, graft ischemia (especially if pedicle compromise was subtle), patient non-compliance, and continued smoking. Management: Re-evaluation with serial CT scans is essential to confirm persistent nonunion. If symptomatic and progressive, revision surgery may involve repeat debridement, re-grafting (potentially with a different vascularized graft or free vascularized microvascular flap), and more robust fixation.
- Avascular Necrosis of Proximal Pole (Recurrence or Persistence): Despite vascularized grafting, the proximal pole may fail to revascularize or sustain its blood supply, leading to continued collapse and fragmentation. Management: Similar to persistent nonunion, revision with another vascularized graft or consideration of wrist salvage procedures if significant degenerative changes are progressing rapidly.
- Degenerative Arthritis (SNAC Wrist Progression): Even with successful union, if preoperative carpal alignment was not fully restored or significant chondral damage was already present, progressive degenerative arthritis can occur. Management: For early SNAC changes, conservative management with activity modification, NSAIDs, and corticosteroid injections. For advanced stages (SNAC III/IV), wrist salvage procedures such as proximal row carpectomy (PRC), four-corner fusion (4CF), or total wrist arthrodesis may be required.
- Donor Site Morbidity: Pain, nerve injury (e.g., superficial radial nerve neuroma at the dorsal distal radius harvest site), prominent scarring, or subtle weakness (e.g., if a significant portion of pronator quadratus is taken) can occur. Management: Symptomatic treatment, nerve blocks, or surgical neurolysis/neurectomy if severe intractable pain from a neuroma is present.
- Malunion/Deformity Recurrence: Failure to fully correct a pre-existing "humpback" deformity or to restore scaphoid length adequately can lead to ongoing
Clinical & Radiographic Imaging


You Might Also Like