Partial Scaphoid Excision of Scaphoid Nonunions
Introduction and Epidemiology
Scaphoid fractures represent the most frequently encountered fractures of the carpal bones, accounting for approximately 60% to 70% of all carpal fractures, with an estimated annual incidence of roughly 29 per 100,000 individuals. When recognized acutely and managed with appropriate rigid immobilization or early surgical intervention, these fractures demonstrate robust healing potential, with union rates consistently exceeding 90%. However, the scaphoid is uniquely vulnerable to delayed diagnosis, inadequate initial immobilization, and patient non-compliance, which frequently culminates in the establishment of a scaphoid nonunion.
The standard initial surgical management for an established scaphoid nonunion is open reduction and internal fixation (ORIF) supplemented with bone grafting. Depending on the vascularity of the proximal pole, the presence of avascular necrosis (AVN), and the geometry of the osseous defect, orthopedic surgeons may utilize non-vascularized corticocancellous wedges (e.g., Matti-Russe or Fisk-Fernandez techniques) or vascularized bone grafts (e.g., 1,2-Intercompartmental Supraretinacular Artery [1,2-ICSRA] grafts or medial femoral condyle free flaps). Despite meticulous surgical technique and appropriate rigid internal fixation, failure rates remain stubbornly high. Current literature suggests a failure rate of approximately 15% for scaphoid waist fractures and up to 33% for proximal pole fractures following primary ORIF with bone grafting.
When primary surgical osteosynthesis fails, the orthopedic surgeon is confronted with a profoundly challenging clinical scenario. Revision ORIF with bone grafting in the setting of prior surgical failure carries a daunting nonunion recurrence rate approaching 50%, largely due to compromised local biology, scar tissue formation, and depletion of local vascularized graft options. Historically, silicone replacement arthroplasty was attempted as a salvage maneuver but has been universally abandoned due to catastrophic long-term complications, including severe silicone synovitis, particulate wear debris, implant dislocation, and eventual fragmentation leading to profound carpal destruction.

For patients presenting with chronic, recalcitrant scaphoid nonunions associated with localized posttraumatic arthritic changes—specifically isolated to the distal pole of the scaphoid and the radial styloid—partial scaphoid excision emerges as a highly viable, low-morbidity salvage procedure. Originally popularized by Malerich and colleagues, excising the distal fragment eliminates the source of painful impingement against the radial styloid and the trapezium. Crucially, this technique preserves the proximal fragment to maintain the critical radiolunate articulation, providing a supportive buttress that delays catastrophic carpal collapse while maintaining a functional arc of motion.
Surgical Anatomy and Biomechanics
Osseous Architecture and Articulations
The scaphoid functions as the critical biomechanical link between the proximal and distal carpal rows, effectively acting as a stabilizing tie-rod. It is a complex, boat-shaped bone that is almost entirely enveloped in articular cartilage (approximately 80% of its surface area), articulating with the scaphoid fossa of the radius proximally, the lunate and capitate ulnarly, and the trapezium and trapezoid distally. Because it lacks any significant tendinous insertions, its stability and kinematic behavior rely entirely on its complex three-dimensional geometry and its robust intrinsic and extrinsic ligamentous attachments, most notably the scapholunate interosseous ligament (SLIL), the radioscaphocapitate (RSC) ligament, and the scaphotrapezial-trapezoid (STT) ligament complex.

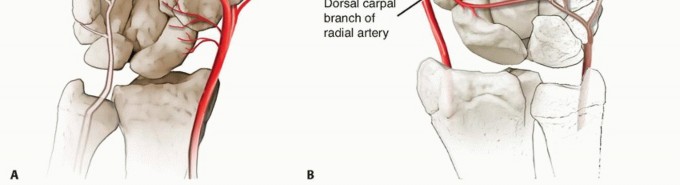
Vascular Supply
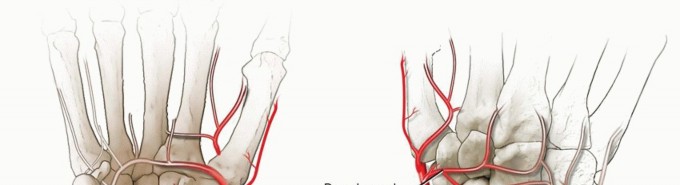
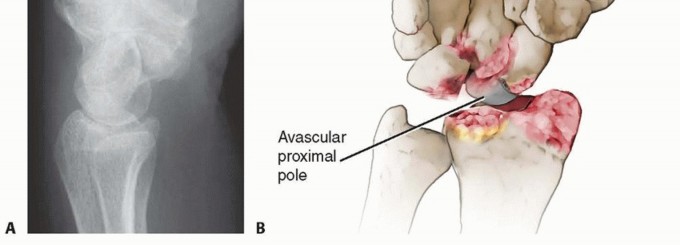
The vascular anatomy of the scaphoid is the primary determinant of its healing capacity and the fundamental pathogenesis of nonunion. As classically described by Gelberman, the predominant arterial supply enters the scaphoid via the dorsal ridge, located distal to the scaphoid waist. These vessels, which are terminal branches of the radial artery, perfuse the proximal pole in a retrograde fashion. A minor volar vascular contribution supplies only the distal 20% to 30% of the bone. Consequently, fractures at the scaphoid waist or proximal pole disrupt this tenuous intraosseous vascular network, placing the proximal fragment at an exceptionally high risk for avascular necrosis (AVN) and subsequent structural collapse.
Carpal Kinematics and Pathomechanics
The scaphoid acts as an essential stabilizing strut that dictates synchronous carpal motion. When this strut is compromised by a nonunion, the normal kinematic linkage between the proximal and distal carpal rows is abolished. The distal scaphoid fragment, driven by the compressive forces exerted by the trapezium and trapezoid during axial loading, tends to flex palmarly and pronate. Conversely, the proximal fragment remains tethered to the lunate via the intact SLIL. As the distal scaphoid flexes, the lunate extends, resulting in the classic dorsal intercalated segment instability (DISI) deformity.

Over time, this uncoupled motion and the resultant scaphoid foreshortening reduce overall carpal height and drastically alter the contact mechanics of the radiocarpal and midcarpal joints. The flexed, pronated distal scaphoid fragment causes abnormal, concentrated point-loading against the radial styloid, initiating the predictable cascade of scaphoid nonunion advanced collapse (SNAC). Partial excision of this distal fragment directly addresses this abnormal point-loading, alleviating radioscaphoid impingement. By leaving the proximal pole in the scaphoid fossa, the lunate remains supported, preventing the capitate from migrating proximally into the radiocarpal joint.

Indications and Contraindications
Patient selection is paramount when considering partial scaphoid excision. This procedure is strictly a salvage operation; it is not a first-line treatment for acute fractures or simple nonunions that are amenable to anatomical reconstruction and bone grafting. It is designed to provide predictable pain relief while preserving a functional arc of motion in a very specific subset of symptomatic patients.
Appropriate Surgical Candidates
The ideal candidate for distal scaphoid excision is a patient with a chronic scaphoid waist nonunion who has failed previous internal fixation, or a low-demand patient who presents with a long-standing, neglected nonunion and early degenerative changes. Specifically, the arthritic changes must be localized strictly to the articulation between the distal scaphoid fragment and the radial styloid (early SNAC Stage I or Stage II). Furthermore, the proximal scaphoid fragment must possess an intact cartilaginous surface articulating with the scaphoid fossa of the radius to ensure continued radiocarpal congruity post-resection.

Contraindications to Distal Excision
Absolute contraindications include advanced midcarpal arthritis, specifically capitolunate degeneration (SNAC Stage III). If the capitate has migrated proximally and is articulating abnormally with the lunate, excising the distal scaphoid will fail to relieve the patient's midcarpal pain, necessitating a more extensive salvage procedure such as a proximal row carpectomy (PRC) or a four-corner arthrodesis. Additionally, inflammatory arthropathies (e.g., rheumatoid arthritis), active wrist infections, severe untreated carpal instability (gross radiocarpal subluxation), and an arthritic or fragmented proximal scaphoid pole represent absolute contraindications.
Operative Versus Non Operative Management
| Clinical Scenario | Recommended Management Strategy | Biomechanical & Clinical Rationale |
|---|---|---|
| Asymptomatic Chronic Nonunion | Non-Operative (Observation) | Low-demand or elderly patients with incidental findings may remain asymptomatic for years; surgical intervention risks introducing iatrogenic morbidity and stiffness. |
| Symptomatic Nonunion (No Arthritis) | Operative (ORIF + Bone Graft) | Joint preservation is the primary goal. Restoring scaphoid anatomy and length prevents the progression to DISI and subsequent SNAC arthritis. |
| Failed ORIF + Radioscaphoid Arthritis | Operative (Partial Scaphoid Excision) | Targeted salvage procedure. Eliminates distal fragment impingement while preserving midcarpal kinematics, maintaining a functional range of motion and acceptable grip strength. |
| Advanced SNAC (Capitolunate Arthritis) | Operative (PRC or 4-Corner Fusion) | Partial excision is insufficient. Complete midcarpal reconstruction or arthrodesis is necessary to address the diffuse degenerative changes and proximal capitate migration. |
Pre Operative Planning and Patient Positioning
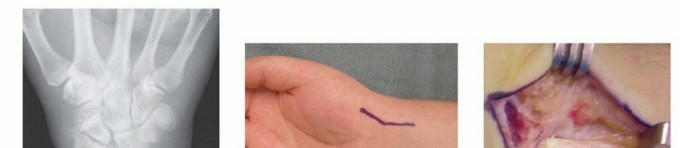
Radiographic Evaluation
Comprehensive imaging is critical for preoperative templating and staging of the SNAC wrist. A standard wrist series including posteroanterior (PA), lateral, oblique, and dedicated scaphoid (ulnar deviation) views must be obtained. The PA view allows for the assessment of carpal height ratio and the presence of radial styloid beaking or sclerosis. The lateral view is essential for evaluating the radiolunate angle (>15 degrees extension indicates DISI) and identifying the presence of dorsal intercalated segment instability.

Advanced cross-sectional imaging is routinely indicated. A non-contrast computed tomography (CT) scan with 1mm fine cuts and sagittal/coronal reconstructions precisely defines the fracture morphology, the volumetric size of the distal fragment, and the extent of cystic resorption or sclerosis at the nonunion interface. CT is highly sensitive for detecting subtle osteophyte formation at the radial styloid or midcarpal joint that might preclude isolated distal pole excision. Magnetic resonance imaging (MRI) may be utilized to assess the viability of the proximal pole; however, in the context of a planned distal excision, the biological viability of the proximal fragment is secondary to the structural integrity of its articular cartilage.

Patient Setup and Anesthesia
The procedure is typically performed under regional anesthesia (supraclavicular or axillary brachial plexus block) combined with intravenous sedation, though general anesthesia may be utilized based on patient comorbidities and anesthesiologist preference.
The patient is positioned supine on the operating table with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm (typically inflated to 250 mmHg) to ensure a bloodless surgical field. The limb is prepped and draped in standard sterile fashion. Intraoperative fluoroscopy (mini C-arm) is positioned either parallel or perpendicular to the hand table, ensuring unimpeded access for orthogonal imaging throughout the procedure to confirm complete excision of the distal fragment.

Detailed Surgical Approach and Technique
Partial scaphoid excision of the distal fragment is most commonly performed via a volar (modified Russe) approach, which provides direct, extensile access to the distal pole and the scaphotrapezial-trapezoid (STT) joint while minimizing iatrogenic disruption to the critical dorsal vascular supply of the proximal pole.
Superficial Dissection and Internervous Planes
A longitudinal or slightly curvilinear incision is made over the volar aspect of the wrist, centered directly over the flexor carpi radialis (FCR) tendon. The incision extends from the distal wrist crease proximally for approximately 4 to 5 centimeters.

Subcutaneous tissues are bluntly dissected. Extreme vigilance must be maintained during this superficial exposure to identify and protect the palmar cutaneous branch of the median nerve (PCBMN), which typically lies just ulnar to the FCR tendon, and the superficial sensory branches of the radial nerve, which arborize radially. The FCR tendon sheath is incised longitudinally, and the tendon is retracted ulnarly. This maneuvers protects the median nerve and exposes the deep floor of the FCR sheath, which is subsequently incised to reveal the underlying volar radiocarpal capsule.
Capsulotomy and Deep Exposure
A longitudinal or T-shaped capsulotomy is performed through the volar radiocarpal ligaments. The radioscaphocapitate (RSC) ligament crosses directly over the waist of the scaphoid and is a primary volar stabilizer of the carpus. Depending on the exact location of the nonunion, the RSC ligament may need to be carefully mobilized or partially incised. If incised, it is imperative that the RSC is meticulously repaired during closure to prevent postoperative ulnar translation of the carpus.
Once the capsule is reflected, the scaphoid nonunion is visualized. The nonunion site is often obscured by dense fibrous tissue, hypertrophic synovium, or cartilaginous debris. A rongeur or small curette is used to clear this interposing tissue, clearly defining the pathological interface between the proximal and distal fragments.
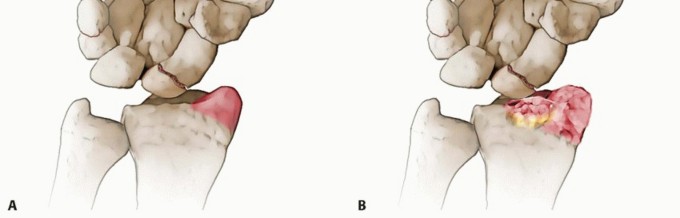
Excision of the Distal Fragment
The distal fragment is grasped with a towel clip or a robust tenaculum. Because the distal fragment articulates with the trapezium and trapezoid, its ligamentous tethers (including the STT joint capsule and ligaments) must be sharply divided. A scalpel or a small periosteal elevator is used to carefully detach these capsular reflections, taking care not to damage the articular surface of the trapezium or trapezoid.
Using a combination of sharp dissection, small osteotomes, and rongeurs, the distal fragment is excised in its entirety. It is critical to utilize intraoperative fluoroscopy to ensure that no osseous fragments remain that could impinge upon the radial styloid or the trapezium during wrist mobilization. Once the fragment is removed, the proximal fragment is visually and mechanically inspected. The proximal fragment is left in situ within the scaphoid fossa of the radius. Its stability is assessed; typically, the intact scapholunate interosseous ligament provides sufficient stability to prevent displacement or extrusion of the proximal pole.

Radial Styloidectomy (Optional but Recommended)
In cases where there is radiographic or direct visual evidence of radioscaphoid impingement or early degenerative changes on the radial styloid (styloid beaking), a concomitant radial styloidectomy is highly recommended. Using a small osteotome or a motorized burr under constant irrigation, the tip of the radial styloid is resected. Care must be taken not to resect more than 3 to 4 millimeters of the styloid to avoid compromising the origin of the radioscaphocapitate ligament, which could lead to iatrogenic carpal instability and ulnar slide of the carpus.
Closure
Following thorough irrigation and meticulous hemostasis (achieved after tourniquet deflation), the volar wrist capsule is repaired using non-absorbable or slowly absorbable braided sutures (e.g., 2-0 or 3-0 Ethibond or Vicryl). A robust capsular repair, particularly of the RSC ligament, is essential to restore the volar stabilizing structures of the wrist. The FCR sheath is loosely approximated to prevent tendon bowstringing, and the skin is closed with subcutaneous and subcuticular sutures.
Complications and Management
While partial scaphoid excision is designed as a low-morbidity salvage procedure, it fundamentally alters the biomechanics of the wrist. Surgeons must counsel patients appropriately regarding postoperative expectations, particularly concerning grip strength and the potential for long-term carpal degradation.
Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Etiology / Clinical Presentation | Salvage Strategy |
|---|---|---|---|
| Progressive Carpal Collapse (SNAC) | 15 - 25% | Altered kinematics leading to progressive capitolunate degeneration over time. Presents as recurrent deep midcarpal wrist pain. | Proximal Row Carpectomy (PRC) or Four-Corner Arthrodesis. |
| Persistent Impingement Pain | 5 - 10% | Incomplete excision of the distal fragment or retained osteophytes on the trapezium/radial styloid. | Revision excision, aggressive arthroscopic debridement, or completion radial styloidectomy. |
| Decreased Grip Strength | > 80% (Expected) | Loss of the scaphoid strut alters the moment arms of extrinsic flexors and wrist stabilizers. | Physical therapy, functional adaptation. Grip strength usually plateaus at 70-80% of the contralateral side. |
| Neuroma Formation | 2 - 5% | Iatrogenic injury or traction neuropraxia to the palmar cutaneous branch of the median nerve or superficial radial nerve. | Desensitization therapy, gabapentinoids. Surgical excision and nerve burying into the pronator quadratus for recalcitrant cases. |
The most significant long-term concern is the inexorable progression of carpal instability. Because the scaphoid no longer bridges the proximal and distal rows, the lunate may progressively rotate into a more severe DISI posture, leading to abnormal loading of the capitate. Routine radiographic surveillance at annual intervals is recommended to monitor for these midcarpal changes.
Post Operative Rehabilitation Protocols
The postoperative rehabilitation following distal scaphoid excision is generally more accelerated than that following ORIF and bone grafting, as there is no requirement to wait for osseous union. The focus shifts rapidly from protection to the restoration of functional kinematics.
Phase I: Immobilization (Weeks 0 to 2)
Immediately postoperatively, the wrist is immobilized in a bulky, well-padded short-arm volar splint to allow for soft tissue healing and to protect the capsular repair. Digital range of motion is encouraged immediately in the recovery room to prevent extrinsic tendon adhesions and reduce dependent edema. The patient is instructed to keep the extremity strictly elevated above heart level.
Phase II: Early Mobilization (Weeks 2 to 6)
At the two-week postoperative visit, sutures are removed, and the surgical wound is inspected. The patient is transitioned to a custom-molded thermoplastic wrist orthosis. Supervised physical therapy is initiated, focusing on active and active-assisted range of motion of the radiocarpal and midcarpal joints. Emphasis is placed on the "dart-thrower's motion" (radial extension to ulnar flexion), which minimizes stress on the SLIL while maximizing functional recovery. Pronation and supination exercises are also incorporated. The orthosis is worn between exercise sessions and at night.
Phase III: Strengthening and Return to Activity (Weeks 6 to 12)
By six weeks, the orthosis is gradually weaned for daytime activities. Progressive resistance exercises are introduced to rebuild grip and pinch strength, compensating for the altered carpal biomechanics. Patients are typically able to return to light duty or activities of daily living by 8 weeks, with full, unrestricted heavy manual activity permitted by 12 weeks, depending on their functional recovery, proprioceptive control, and pain levels.
Summary of Key Literature and Guidelines
The academic foundation for partial scaphoid excision rests on several key biomechanical and clinical studies. Malerich et al. (1999) provided a seminal review of distal scaphoid resection for scaphoid nonunion, demonstrating that excising the distal fragment reliably relieves pain associated with STT or radioscaphoid impingement while preserving a functional arc of motion. Their cohort demonstrated high patient satisfaction rates, particularly in lower-demand individuals, establishing the procedure as a viable alternative to total wrist arthrodesis.
Subsequent biomechanical studies have elucidated why this procedure is successful as a temporizing or definitive salvage option. By removing the distal pole, the abnormal point-loading forces on the radial styloid are eliminated. Furthermore, leaving the proximal pole in the scaphoid fossa prevents the capitate from migrating proximally into the radiocarpal joint, a complication frequently seen after complete scaphoid excision without concomitant intercarpal arthrodesis.
Current orthopedic guidelines reserve partial scaphoid excision for a very specific niche: the symptomatic patient with a chronic distal or waist nonunion, failed previous osteosynthesis, and localized early degenerative changes (SNAC I/II), who wishes to avoid the prolonged immobilization and altered kinematics associated with total wrist arthrodesis, four-corner fusion, or proximal row carpectomy. When patient selection is rigorous and surgical execution is meticulous, distal scaphoid excision provides a reliable, durable improvement in quality of life.
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
You Might Also Like