Proximal Tibial Diaphyseal Fracture: High-Energy Trauma Case Study, Clinical & Imaging Diagnostics
Key Takeaway
Diagnosis of high-energy proximal tibial diaphyseal fractures involves a detailed patient history, thorough clinical examination assessing deformity, swelling, and neurovascular status. Initial plain radiographs confirm the fracture, while a CT scan precisely delineates comminution, angulation, and rules out intra-articular extension. This comprehensive approach is crucial for accurate classification and surgical planning.
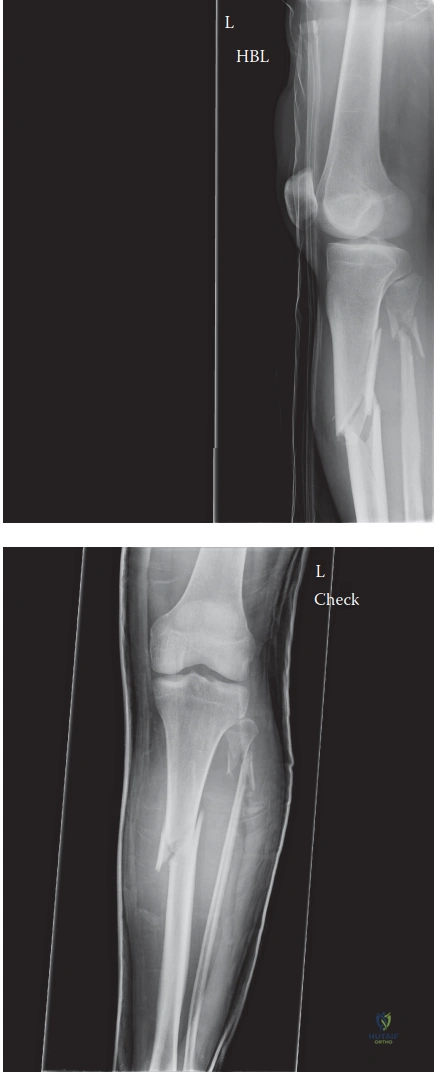
A 38-year-old male presents following a high-velocity motorcycle collision. You are presented with his primary radiographs of the right lower leg. Describe the findings and explain the specific biomechanical reasons why this fracture pattern is prone to malalignment during intramedullary nailing.
Candidate: The radiograph shows a comminuted, proximal third tibial diaphyseal fracture with a butterfly fragment. There is significant shortening and angulation. It is difficult to nail because the proximal segment is wide and the patellar tendon pulls it into extension, often causing apex anterior and valgus malalignment.
Failing to mention the specific anatomical deforming forces (e.g., the quadriceps/patellar tendon pull vs. the pes anserinus) and describing the nail trajectory without explaining the "wedge effect" of the proximal fragment. Candidates often fail to address the risk of intra-articular extension despite the radiographic appearance.
A high-scoring answer identifies the fracture as an AO/OTA 42-B3 pattern. It explains that the proximal fragment is acted upon by the quadriceps mechanism (via the patellar tendon) resulting in apex anterior (procurvatum) angulation, while the pes anserinus and iliotibial band contribute to varus/valgus instability. The candidate must mention the "bell-clapper effect"—where the nail, following the path of least resistance in the wide metaphysis, tracks into the posterior and lateral cortex, cementing the deformity. The candidate should conclude by mandating a CT scan to rule out occult intra-articular extension, which would change the surgical strategy.
You have decided to proceed with an intramedullary nail for this proximal third tibial fracture. Describe your specific intraoperative technical strategy to ensure anatomical reduction and avoid the classic malalignment patterns.
Candidate: I would use a suprapatellar nailing approach with the knee in semi-extension to reduce the deforming force of the extensor mechanism. I would use blocking screws—or Poller screws—placed strategically in the proximal fragment to guide the nail centrally and prevent it from shifting. I would also perform a formal reduction before starting reaming.
Missing the importance of the *order* of operations—specifically, forgetting that the fracture must be reduced prior to nail insertion. Candidates also frequently neglect to specify where exactly to place the Poller screws (e.g., posterior vs. lateral).
Structure the answer: 1. Positioning: Suprapatellar approach in semi-extension (15-20°) to relax the extensor mechanism. 2. Entry Point: Ensure a precise, proximal-anterior starting point. 3. Reduction: Perform reduction *before* reaming using percutaneous clamps. 4. Blocking Screws (Poller Screws): Place them on the concave side of the deformity—posterior to prevent procurvatum and lateral to prevent valgus. 5. Technique: Use a protective cannula to prevent articular cartilage damage and emphasize that the nail follows the blocking screws, essentially "narrowing" the metaphysis to ensure a straight trajectory.
