Fasciotomy for Chronic Exertional Compartment Syndrome: Surgical Masterclass
Key Takeaway
Chronic exertional compartment syndrome (CECS) requires precise surgical decompression when conservative measures fail. This guide details the single-incision fasciotomy for the anterior and lateral compartments, and the double-incision approach for the posterior compartments. Mastery of these techniques, including meticulous identification of the superficial peroneal nerve and complete fascial release, is essential for restoring biomechanical function and preventing neurovascular compromise in high-demand athletes.
INTRODUCTION TO CHRONIC EXERTIONAL COMPARTMENT SYNDROME (CECS)
Chronic exertional compartment syndrome (CECS) is a debilitating condition characterized by exercise-induced pain, swelling, and occasionally neurologic impairment in the lower extremity. Unlike acute compartment syndrome, which is a surgical emergency driven by trauma, CECS is a reversible ischemic process. It occurs when the volume of skeletal muscle expands by up to 20% during strenuous activity, overwhelming the non-compliant osseofascial boundaries of the leg compartments.
When conservative management—such as activity modification, orthotics, and physical therapy—fails to provide relief, surgical decompression via fasciotomy becomes the gold standard of treatment. The primary goal of operative intervention is the complete release of the restricting fascia to normalize intracompartmental pressures during exertion, thereby restoring microvascular perfusion and eliminating ischemic pain.
This comprehensive guide details the two primary surgical approaches for lower extremity CECS: the Single-Incision Fasciotomy for the anterior and lateral compartments (as described by Fronek et al.), and the Double-Incision Fasciotomy for the posterior compartments (as described by Rorabeck).
PREOPERATIVE EVALUATION AND INDICATIONS
Diagnostic Criteria
The diagnosis of CECS is heavily reliant on dynamic intracompartmental pressure (ICP) monitoring. The modified Pedowitz criteria remain the standard for diagnosing CECS. Surgery is indicated if one or more of the following pressure thresholds are met using a slit-catheter or solid-state transducer system:
* Pre-exercise (Resting) Pressure: $\ge$ 15 mm Hg
* 1-Minute Post-exercise Pressure: $\ge$ 30 mm Hg
* 5-Minute Post-exercise Pressure: $\ge$ 20 mm Hg
Surgical Indications
- Confirmed elevated intracompartmental pressures correlating with the patient's exertional pain.
- Failure of a minimum of 3 to 6 months of non-operative management.
- Presence of fascial hernias associated with localized pain and elevated pressures.
- Neurologic symptoms (e.g., paresthesias in the distribution of the superficial peroneal nerve) during exertion.
💡 Clinical Pearl
Always evaluate the patient for concurrent pathologies, such as medial tibial stress syndrome (MTSS), tibial stress fractures, or popliteal artery entrapment syndrome, as these can mimic or coexist with CECS.
SINGLE-INCISION FASCIOTOMY FOR CHRONIC ANTERIOR AND LATERAL COMPARTMENT SYNDROME
The anterior and lateral compartments are the most frequently affected in CECS. The single-incision technique, popularized by Fronek et al., provides excellent visualization for the release of both compartments while minimizing soft tissue morbidity and cosmetic deformity.
Applied Surgical Anatomy
- Anterior Compartment: Contains the tibialis anterior, extensor hallucis longus (EHL), extensor digitorum longus (EDL), and peroneus tertius muscles. The neurovascular bundle consists of the deep peroneal nerve and the anterior tibial artery.
- Lateral Compartment: Contains the peroneus longus and peroneus brevis muscles. The superficial peroneal nerve (SPN) courses through this compartment before piercing the lateral fascia to become subcutaneous, typically in the distal third of the leg.
Patient Positioning and Preparation
- Positioning: Place the patient supine on the operating table. A bump may be placed under the ipsilateral hip to internally rotate the leg slightly, bringing the anterolateral aspect of the leg into optimal view.
- Tourniquet: Apply a proximal thigh tourniquet. While some surgeons prefer to operate without a tourniquet to assess muscle viability and hemostasis dynamically, using one provides a bloodless field, which is critical for identifying the superficial peroneal nerve.
- Preparation: Standard sterile prep and drape from the toes to the mid-thigh.
Surgical Technique (Fronek et al.)
1. Incision Strategy
The approach depends on the presence or absence of a muscular hernia.
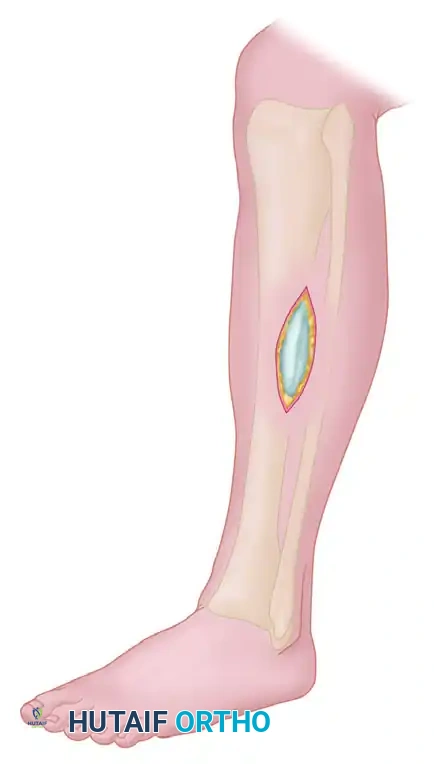
Scenario A: No Fascial Hernia Present
Make a 5-cm longitudinal incision halfway between the fibula and the tibial crest in the midportion of the leg. This central placement allows access to both the anterior and lateral compartments via a single skin window.
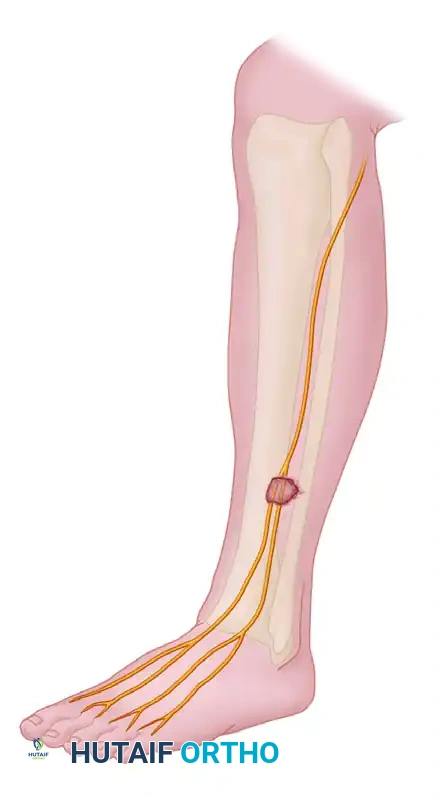
Scenario B: Fascial Hernia Present
If a muscular hernia is present—often located at the exit point of the superficial peroneal nerve—center the incision directly over the fascial defect.
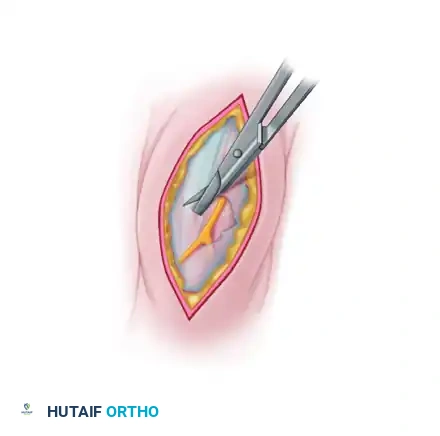
2. Deep Dissection and Nerve Identification
Carefully dissect through the subcutaneous tissues. Meticulous hemostasis is required.
* Identify the superficial peroneal nerve as it exits the lateral compartment fascia.
* Identify the anterolateral intermuscular septum, which divides the anterior and lateral compartments.
* If a fascial defect (hernia) is present, use scissors to enlarge the defect across the intermuscular septum to gain access to both compartments.
🚨 Surgical Warning
Do not repair muscular hernias. Attempting to close a fascial defect in the setting of CECS will acutely decrease compartment volume, potentially precipitating an iatrogenic acute compartment syndrome. The hernia will resolve functionally once the compartment is fully decompressed.
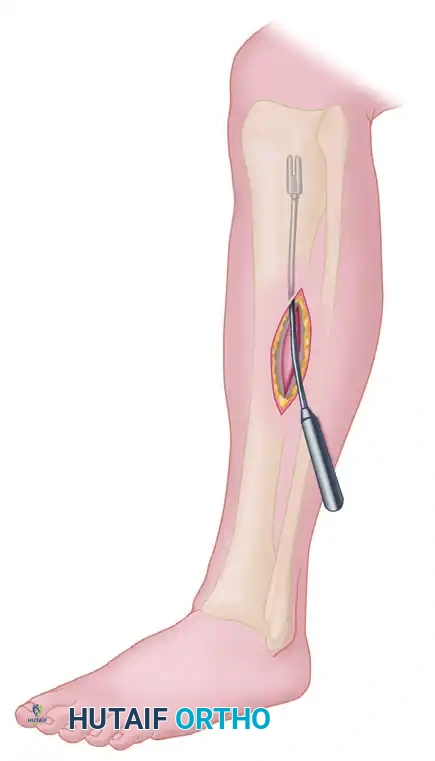
3. Anterior Compartment Release
- Incise the anterior compartment fascia transversely for a few millimeters to create a starting point.
- Pass a fasciotome (or long Metzenbaum scissors) into the anterior compartment.
- Direct the instrument proximally and distally in line with the anterior tibial muscle. Ensure the release extends from the proximal tibial flare down to the extensor retinaculum.

4. Lateral Compartment Release
- Identify the lateral compartment fascia, ensuring the superficial peroneal nerve is protected and retracted gently.
- Run the fasciotome proximally and distally, strictly posterior to the superficial peroneal nerve, in line with the fibular shaft.
- The release must extend proximally to the fibular head and distally to the lateral malleolus.


5. Closure
- Deflate the tourniquet and achieve meticulous hemostasis. Hematoma formation is a primary cause of postoperative pain and scarring.
- Irrigate the wounds copiously with sterile saline.
- Close the skin and subcutaneous tissue only. Never close the fascia.
- Apply a sterile, mildly compressive dressing.
DOUBLE-INCISION FASCIOTOMY FOR CHRONIC POSTERIOR COMPARTMENT SYNDROME
Involvement of the deep and superficial posterior compartments is less common than anterolateral CECS but presents a unique surgical challenge. The deep posterior compartment is notoriously difficult to decompress fully due to its deep anatomical location and the overlying soleus muscle. The double-incision technique, described by Rorabeck, ensures complete release while protecting the saphenous neurovascular bundle.
Applied Surgical Anatomy
- Superficial Posterior Compartment: Contains the gastrocnemius, soleus, and plantaris muscles. The sural nerve courses superficially over this compartment.
- Deep Posterior Compartment: Contains the tibialis posterior, flexor digitorum longus (FDL), and flexor hallucis longus (FHL). The neurovascular bundle consists of the tibial nerve and the posterior tibial artery and vein. This compartment is tightly bound by the tibia, fibula, interosseous membrane, and the deep transverse fascia.
Patient Positioning
- Positioning: Place the patient supine with the hip externally rotated and the knee slightly flexed ("frog-leg" position). Alternatively, the lateral decubitus position can be utilized depending on surgeon preference.
- Tourniquet: Apply a proximal thigh tourniquet.
Surgical Technique (Rorabeck)
1. Incision Strategy
Make two separate longitudinal incisions on the medial aspect of the leg, approximately 1 cm posterior to the posteromedial border of the tibia.
* Proximal Incision: Approximately 5 to 7 cm in length, located in the proximal third of the leg.
* Distal Incision: Approximately 5 to 7 cm in length, located in the distal third of the leg.
Using two incisions rather than one massive longitudinal incision significantly reduces wound healing complications and cosmetic morbidity while still allowing for complete fascial release under direct or semi-direct visualization.
2. Superficial Dissection and Neurovascular Protection
- In the proximal incision, carefully dissect through the subcutaneous fat to identify the saphenous vein and the saphenous nerve.
- Gently mobilize and retract these structures anteriorly to prevent iatrogenic injury. Damage to the saphenous nerve can result in painful neuromas and medial foot numbness.
3. Superficial Posterior Compartment Release
- Identify the investing fascia of the superficial posterior compartment (overlying the medial head of the gastrocnemius and the soleus).
- Incise the fascia longitudinally. Use long scissors or a fasciotome to extend the release proximally to the tibial plateau and distally toward the musculotendinous junction of the Achilles tendon.
- Verify the release by passing a finger along the length of the compartment.
4. Deep Posterior Compartment Release
This is the most critical and technically demanding step of the procedure.
* Retract the superficial posterior compartment musculature (gastrocnemius and soleus) posteriorly.
* Identify the deep transverse fascia, which covers the flexor digitorum longus (FDL) and the tibialis posterior.
* Detaching the Soleal Bridge: In the proximal aspect of the leg, the soleus muscle takes origin from the posteromedial tibia (the soleal bridge). To fully expose and release the proximal extent of the deep posterior compartment, this soleal bridge must be partially detached or elevated from the tibia.
* Once the deep fascia is exposed, incise it longitudinally.
* Extend the release distally through the second incision, ensuring the fascia over the FDL and tibialis posterior is completely divided down to the level of the medial malleolus.
🔪 Surgical Pitfall
Failure to release the proximal third of the deep posterior compartment (by neglecting to detach the soleal bridge) is the most common cause of recurrent posterior CECS. Ensure the release extends fully behind the medial tibial crest.
5. Closure
- Deflate the tourniquet and obtain strict hemostasis. The deep posterior compartment is highly vascular, and unrecognized bleeding can lead to severe postoperative hematomas.
- Irrigate the wounds thoroughly.
- Close the subcutaneous tissues and skin. Leave the fascia open.
- Apply a sterile, bulky, mildly compressive dressing.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management following fasciotomy for CECS is designed to promote early mobility, prevent fascial scarring (which can lead to recurrence), and safely return the athlete to high-demand activities.
Phase 1: Immediate Postoperative (Weeks 0-2)
- Weight-Bearing: Patients are typically allowed to weight-bear as tolerated immediately postoperatively with the use of crutches for support.
- Wound Care: Keep the surgical dressings clean and dry. Sutures or staples are removed at 10 to 14 days.
- Mobility: Encourage immediate active and passive range of motion (ROM) of the ankle and toes to prevent tendon adhesions and promote venous return.
- Edema Control: Elevation and ice are critical during the first 72 hours to manage swelling.
Phase 2: Early Rehabilitation (Weeks 2-6)
- Physical Therapy: Initiate formal physical therapy focusing on restoring full ankle ROM, particularly dorsiflexion and plantarflexion.
- Strengthening: Begin isometric strengthening of the anterior, lateral, and posterior musculature. Progress to isotonic exercises as pain allows.
- Cardiovascular Fitness: Patients may begin low-impact cardiovascular activities, such as stationary cycling or deep-water running, once the incisions are fully healed.
Phase 3: Return to Sport (Weeks 6-12)
- Progression: Introduce impact activities gradually. Begin with a walk-jog progression on a soft surface (e.g., a treadmill or track).
- Sport-Specific Training: Incorporate plyometrics, cutting, and sport-specific drills by weeks 8 to 10.
- Clearance: Full return to competitive sports is generally permitted between 8 and 12 weeks postoperatively, provided the patient is pain-free, has full strength, and demonstrates no signs of recurrent compartment syndrome.
COMPLICATIONS AND MANAGEMENT
While fasciotomy for CECS is highly successful (with success rates exceeding 85% for the anterior/lateral compartments), complications can occur.
- Nerve Injury: The superficial peroneal nerve (in anterolateral releases) and the saphenous nerve (in posterior releases) are at highest risk. Injury can result in numbness, paresthesias, or painful neuromas. Meticulous surgical technique and direct visualization are paramount.
- Recurrence: Recurrence of symptoms is most commonly due to an incomplete fascial release, particularly at the proximal or distal extents of the compartments, or failure to release the deep posterior compartment adequately. Revision surgery may be required.
- Hematoma and Seroma: Inadequate hemostasis after tourniquet deflation can lead to hematoma formation, which increases the risk of infection and excessive scarring.
- Infection: Superficial wound infections are managed with oral antibiotics, while deep infections may require surgical debridement.
- Cosmetic Concerns: Patients should be counseled preoperatively about the risk of visible scarring and the potential for persistent, asymptomatic muscle herniation through the fascial defect.
CONCLUSION
Surgical management of Chronic Exertional Compartment Syndrome via single- or double-incision fasciotomy is a highly effective intervention for athletes and active individuals failing conservative care. A profound understanding of lower extremity cross-sectional anatomy, precise identification of neurovascular structures, and an uncompromising approach to complete fascial release are the cornerstones of surgical success. By adhering to the techniques outlined by Fronek and Rorabeck, orthopedic surgeons can reliably restore limb biomechanics, alleviate ischemic pain, and facilitate a safe return to high-level physical exertion.
📚 Medical References
- Chronic compartment syndrome: diagnosis, management, and outcomes, Am J Sports Med 13:162, 1985.
- Fraipont MJ, Adamson GJ: Chronic exertional compartment syndrome, J Am Acad Orthop Surg 11:268, 2003.
- Fronek J, Mubarak SJ, Hargens AR, et al: Management of chronic exertional anterior compartment syndrome of the lower extremity, Clin Orthop Relat Res 220:217, 1987.
- Gelberman RH, Garfi n SR, Hergenroeder PT, et al: Compartment syndromes of the forearm: diagnosis and treatment, Clin Orthop Relat Res 161:252, 1981.
- Gershuni DH, Gosink BB, Hargens AR, et al: Ultrasound evaluation of the anterior musculofascial compartment of the leg following exercise, Clin Orthop Relat Res 167:185, 1982.
- Giannotti G, Cohn SM, Brown M: Utility of near-infrared spectroscopy in the diagnosis of lower extremity compartment syndrome, J Trauma 48:396, 2000.
- Hargens AR, Schmidt DA, Evans KL, et al: Quantitation of skeletal-muscle necrosis in a model compartment syndrome, J Bone Joint Surg 63A:631, 1981.
- Treatment of Biceps Brachii
You Might Also Like


