Compartment Syndromes and Volkmann Contracture: A Master Surgical Guide
Key Takeaway
Acute compartment syndrome is a surgical emergency characterized by elevated intracompartmental pressure that compromises tissue perfusion. Left untreated, it progresses to irreversible muscle and nerve necrosis, culminating in Volkmann ischemic contracture. This guide details the pathophysiology, critical anatomical compartments of the upper extremity, diagnostic criteria, and step-by-step surgical techniques for emergent fasciotomy and the management of established contractures.
INTRODUCTION AND HISTORICAL CONTEXT
Acute compartment syndrome (ACS) of the upper extremity represents a catastrophic orthopedic emergency. It is defined by a critical increase in interstitial pressure within a closed osseofascial space, leading to microvascular compromise, tissue ischemia, and ultimately, irreversible myoneural necrosis. If unrecognized or inadequately treated, ACS progresses to the devastating clinical entity known as Volkmann ischemic contracture—a permanent, fibrotic deformity of the affected musculature.
First described by Richard von Volkmann in 1881, the ischemic contracture was initially attributed to tight bandages. Today, modern orthopedic surgery recognizes that any condition decreasing compartment volume or increasing compartment content can precipitate this ischemic cascade.
PATHOPHYSIOLOGY AND BIOMECHANICS
The fundamental biomechanical failure in compartment syndrome is the disruption of the local arteriovenous gradient. As intracompartmental pressure (ICP) rises, it eventually surpasses the intravascular pressure of the venules and capillaries.
- The Ischemic-Edema Cycle: As described by Eaton and Green, increased interstitial pressure causes capillary collapse, impeding local blood flow. The resulting local tissue ischemia leads to cellular hypoxia, failure of the Na+/K+ ATPase pump, and subsequent intracellular swelling. This local edema further increases intracompartmental pressure, creating a vicious, self-propagating cycle of ischemia.
- Critical Pressure Thresholds: In a classic canine model, muscle necrosis was definitively shown to occur when tissue pressure rises to within 20 mm Hg below the diastolic blood pressure. Currently, a $\Delta$P (Diastolic Blood Pressure minus Intracompartmental Pressure) of less than 30 mm Hg is the universally accepted threshold for emergent surgical intervention.
- Tissue Ischemia Tolerance: The tolerance of tissue to prolonged hypoxia varies strictly by histological type:
- Muscle Tissue: Functional impairment manifests after 2 to 4 hours of ischemia. Irreversible functional loss and myonecrosis occur after 4 to 12 hours.
- Nerve Tissue: Peripheral nerves are highly sensitive to ischemia. Abnormal function (paresthesias) appears after just 30 minutes. Irreversible functional loss (axonotmesis/neurotmesis) occurs after 12 to 24 hours.
Clinical Pearl: The presence of palpable distal pulses does not rule out acute compartment syndrome. Arterial inflow continues long after capillary perfusion has ceased. Waiting for the loss of a pulse is waiting for irreversible necrosis.
ETIOLOGY
While fractures (particularly supracondylar humerus and both-bone forearm fractures) are the most common precipitants, ACS can occur in the absence of fracture.
- Traumatic Causes: Direct trauma, crushing injuries of the upper arm, shoulder dislocations, and avulsion of the triceps muscle.
- Iatrogenic Causes: Prolonged pneumatic tourniquet use, arterial punctures/arteriography, and tight circumferential casting. Intravenous regional anesthesia (Bier block) has also been implicated, particularly when hypertonic saline is used to dilute the anesthetic agent.
- Neonatal Causes: Compartment syndrome has been documented in neonates resulting from intrauterine malposition or strangulation of the extremity by the umbilical cord.
- Chronic Exertional Compartment Syndrome (CECS): Though rare in the upper extremity compared to the leg, CECS of the first dorsal interosseous muscle and the volar forearm has been reported, most frequently in professional motorcyclists and elite rowers.
SURGICAL ANATOMY OF THE UPPER EXTREMITY COMPARTMENTS
A profound understanding of the cross-sectional anatomy is mandatory for adequate surgical decompression.
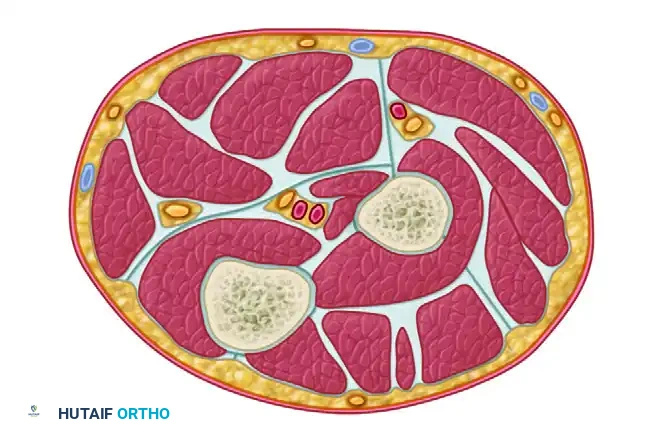
The Forearm Compartments
The forearm is divided into three primary compartments, though the volar compartment is functionally subdivided into superficial and deep spaces.
- Superficial Volar Compartment: Contains the pronator teres (PT), flexor carpi radialis (FCR), palmaris longus (PL), flexor carpi ulnaris (FCU), and flexor digitorum superficialis (FDS).
- Deep Volar Compartment: Contains the flexor digitorum profundus (FDP), flexor pollicis longus (FPL), and pronator quadratus. This compartment is the most severely affected in forearm ACS due to its proximity to the interosseous membrane and unyielding fascial borders.
- Dorsal Compartment: Contains the extensor digitorum communis (EDC), extensor digiti minimi (EDQ/EDM), extensor carpi ulnaris (ECU), and the deep outcropping muscles (abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, extensor indicis proprius).
- Mobile Wad of Henry: Contains the brachioradialis (BR), extensor carpi radialis longus (ECRL), and extensor carpi radialis brevis (ECRB).
Cross section through the upper third of the forearm demonstrating the critical spatial relationships of the superficial and deep volar compartments, the dorsal compartment, and the mobile wad.
The Hand Compartments
The hand contains 10 distinct fascial compartments that must be evaluated during a severe crush injury.
- Interosseous Compartments (7): Four dorsal interosseous and three volar interosseous compartments.
- Thenar Compartment: Contains the abductor pollicis brevis, flexor pollicis brevis, and opponens pollicis.
- Hypothenar Compartment: Contains the abductor digiti minimi, flexor digiti minimi, and opponens digiti minimi.
- Adductor Compartment: Contains the adductor pollicis.
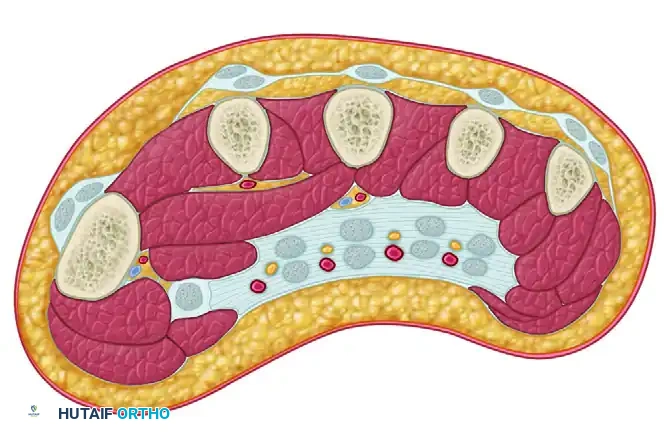
Cross section through the hand illustrating the dorsal and volar interosseous compartments, the adductor compartment to the thumb, and the thenar/hypothenar compartments.
The Digit Compartments
Acute compartment syndrome of the intrinsic muscles of the hand and digits can result in severe contracture. The digits are compartmentalized by strong fascial septa.
- Cleland Ligament: Dorsal to the neurovascular bundle.
- Grayson Ligament: Volar to the neurovascular bundle.
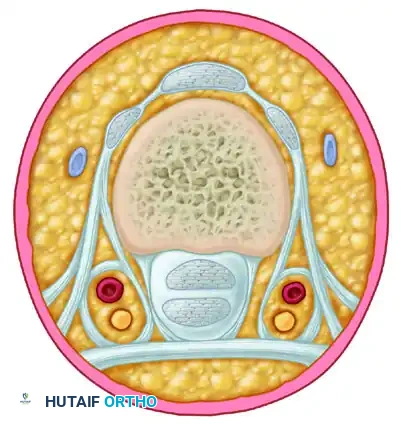
Cross section through the finger demonstrating the compartmentalization created by Cleland and Grayson ligaments around the neurovascular bundle.
CLINICAL DIAGNOSIS
The diagnosis of ACS is primarily clinical, supplemented by invasive pressure monitoring in obtunded or polytrauma patients.
- Pain out of proportion: The earliest and most reliable indicator.
- Pain with passive stretch: Exquisite pain upon passive extension of the digits (stretching the ischemic volar flexors) is the hallmark sign of deep volar compartment ischemia.
- Palpable tenseness: The compartment feels "wood-like."
- Paresthesia: Indicates early nerve ischemia (median/ulnar nerves).
- Paralysis and Pulselessness: Late, ominous signs indicating irreversible damage.
Surgical Warning: Do not rely on capillary refill or distal pulses. If a patient has a clinically obvious compartment syndrome, proceed directly to the operating room. Delaying for pressure measurements in a clinically obvious case constitutes surgical negligence.
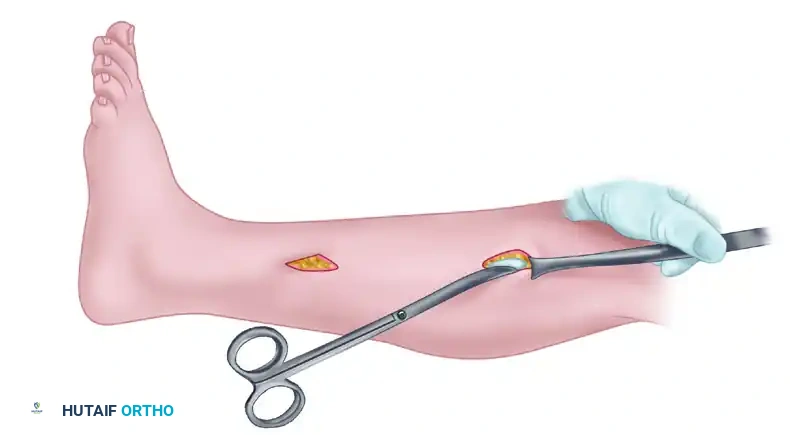
ACUTE SURGICAL MANAGEMENT: FASCIOTOMY
The absolute indication for fasciotomy is a clinical diagnosis of ACS or a $\Delta$P < 30 mm Hg in an unresponsive patient.
Forearm Fasciotomy (Volar and Dorsal Approaches)
Positioning: Supine, arm extended on a hand table. A sterile tourniquet is applied but strictly uninflated unless catastrophic hemorrhage occurs, as tourniquet inflation exacerbates ischemia.
Step 1: The Volar Approach (Extended Henry)
1. Incision: Begin proximal to the elbow joint on the medial aspect of the arm. Cross the antecubital fossa obliquely to avoid flexion contractures. Extend the incision down the volar forearm, curving ulnarly at the wrist, and crossing the carpal tunnel in line with the fourth ray.
2. Superficial Release: Divide the subcutaneous tissues. Identify and protect the medial antebrachial cutaneous nerve. Incise the lacertus fibrosus (bicipital aponeurosis) completely, as this is a major point of proximal compression.
3. Fascial Decompression: Longitudinally incise the superficial fascia over the FCU and FDS.
4. Deep Compartment Release: Retract the superficial flexors (FDS) and the neurovascular bundle radially. Expose the deep compartment (FDP and FPL). Incise the deep fascia overlying these muscles. If the muscle bellies remain tight, perform careful epimysiotomies.
5. Carpal Tunnel Release: Divide the transverse carpal ligament to decompress the median nerve, which is frequently compressed by swelling from the forearm.
Step 2: The Dorsal Approach
1. Incision: A straight longitudinal incision from the lateral epicondyle to the midline of the wrist.
2. Fascial Decompression: Incise the dorsal fascia longitudinally. Identify the interval between the EDC and ECRB to decompress the mobile wad and the dorsal compartment simultaneously.
Hand and Digit Fasciotomy
Hand Decompression:
1. Dorsal Incisions: Make two longitudinal incisions over the second and fourth metacarpals. Retract the extensor tendons to access and release the dorsal and volar interosseous fascial compartments.
2. Thenar/Hypothenar Incisions: Make a longitudinal incision along the radial border of the first metacarpal for the thenar compartment, and along the ulnar border of the fifth metacarpal for the hypothenar compartment.
Digit Decompression:
1. Make mid-axial incisions along the ulnar side of the index, middle, and ring fingers, and the radial side of the thumb and small finger.
2. Release the fascia, taking care to protect the neurovascular bundles situated between Grayson and Cleland ligaments.
MANAGEMENT OF ESTABLISHED VOLKMANN CONTRACTURE
If ACS is missed, the necrotic muscle is gradually replaced by dense, inelastic fibrous tissue. The classic Volkmann contracture presents with elbow flexion, forearm pronation, wrist flexion, metacarpophalangeal (MCP) joint extension, and interphalangeal (IP) joint flexion.
The infarct typically forms an ellipsoid shape, with the most severe necrosis at the center of the deep volar compartment (FDP and FPL). The median and ulnar nerves are frequently tethered and compressed within this fibrotic mass.
Muscle Sliding Operation of Flexors (Max Page Procedure)
For established, moderate Volkmann contracture where some functional muscle remains, a muscle sliding operation is indicated to restore digit extension and wrist position.
Surgical Steps:
1. Incision: Extensive volar incision from the medial epicondyle to the wrist.
2. Neurolysis: Identify the ulnar nerve proximally at the cubital tunnel. Perform a meticulous neurolysis and anterior transposition. Identify and decompress the median nerve throughout the forearm, freeing it from the fibrotic muscle bed.
3. Muscle Release: Elevate the common flexor origin from the medial epicondyle. Release the origins of the PT, FCR, PL, FCU, and FDS.
4. Deep Release: Subperiosteally elevate the FDP from the ulna and the FPL from the radius.
5. Sliding: Allow the entire flexor-pronator mass to slide distally (typically 2 to 3 cm). This distal migration relieves the flexion contracture at the wrist and digits.
6. Fixation/Closure: The muscle mass is not sutured to bone but allowed to heal in its new, distally advanced position. The wrist and digits are splinted in extension.
Established Intrinsic Muscle Contractures of the Hand
Ischemia of the intrinsic muscles leads to an intrinsic-plus hand deformity (MCP flexion, PIP/DIP extension).
Surgical Management (Intrinsic Release):
1. Approach: Dorsal longitudinal incisions over the metacarpals.
2. Release: Identify the lateral bands of the extensor mechanism. Resect the oblique fibers of the intrinsic wing expansions (Littler's release) to allow PIP joint flexion while preserving the transverse fibers for MCP joint flexion.
3. Adducted Thumb: Severe contracture of the adductor pollicis requires release of its origin from the third metacarpal or a Z-plasty of the first web space to restore thumb opposition and grasp.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Acute Fasciotomy Management:
* Wound Care: Fasciotomy wounds must never be closed primarily. Apply a negative pressure wound therapy (NPWT/VAC) dressing at 75-100 mm Hg to manage exudate and reduce edema.
* Second Look: Return to the operating room at 48-72 hours for a second look, debridement of any definitively necrotic muscle (which appears dark, non-contractile, and does not bleed when cut), and possible delayed primary closure.
* Coverage: If the wound cannot be closed without tension by day 5-7, apply a split-thickness skin graft (STSG).
* Splinting: Splint the hand in a functional position (wrist extended 30 degrees, MCPs flexed 70 degrees, IP joints fully extended) to prevent secondary contractures.
Post-Contracture Reconstruction Management:
* Following a muscle slide procedure, the extremity is immobilized in a long-arm cast with the wrist and digits in maximum corrected extension for 4 weeks.
* Aggressive, supervised occupational therapy is initiated immediately upon cast removal, focusing on passive stretching and active tendon gliding to maximize the functional excursion of the advanced muscle mass.
===
📚 Medical References
- Compartment syndrome of the arm—a complication of the pneumatic tourniquet, J Bone Joint Surg 65A:270, 1983.
- Greenwald AS, Boden SD, Goldberg VM, et al: Bone-graft substitutes: facts, fi ctions, and applications, J Bone Joint Surg 83A:98, 2001.
- Hankin FM, Papadopoulos S: A sterile pneumatic tourniquet for surgical procedures about the elbow, Orthop Rev 17:1240, 1988.
- Heiple KG, Goldberg VM, Powell AE, et al: Biology of cancellous bone grafts, Orthop Clin North Am 18:179, 1987.
- Henderson MS: Nonunion in fractures: the massive bone graft, JAMA 81:463, 1923.
- Henry MO: Homografts in orthopedic surgery, J Bone Joint Surg 30A:70, 1948.
- Hirota K, Hashimoto H, Kabara S, et al: The relationship between pneumatic tourniquet time and the amount of pulmonary emboli in patients undergoing knee
You Might Also Like