Advanced Management of Acetabular Fractures and High-Energy Pelvic Trauma
Key Takeaway
Total hip arthroplasty (THA) is a viable salvage procedure for complex acetabular fractures with poor prognoses, particularly in elderly patients. This approach combines acute fracture fixation with primary arthroplasty, allowing early mobilization. High-energy pelvic ring injuries demand rigorous resuscitative protocols, including pelvic binders, external fixation, and retroperitoneal packing, to mitigate life-threatening hemorrhage before definitive reconstruction.
TOTAL HIP ARTHROPLASTY AS TREATMENT OF ACETABULAR FRACTURE
The management of acetabular fractures has traditionally centered on open reduction and internal fixation (ORIF) to restore articular congruity and preserve the native hip joint. However, total hip arthroplasty (THA) has increasingly been utilized as a primary treatment modality for specific acetabular fractures associated with extremely poor prognoses. This paradigm shift is particularly relevant in the geriatric population, where osteopenia, severe comminution, pre-existing osteoarthritis, and marginal impaction frequently compromise the viability of joint-preserving surgery.
Primary THA in the setting of acute acetabular trauma aims to bypass the prolonged restricted weight-bearing protocols required after isolated ORIF, thereby mitigating the systemic complications of immobility in elderly patients, such as deep vein thrombosis, pulmonary embolism, and decubitus ulcers.
Indications and Patient Selection
The decision to proceed with acute THA rather than isolated ORIF hinges on identifying fracture patterns and patient characteristics that predict a high likelihood of post-traumatic arthritis or fixation failure. Primary indications include:
* Advanced Age: Patients over 65 years with osteopenic or osteoporotic bone.
* Pre-existing Degenerative Joint Disease: Symptomatic osteoarthritis of the affected hip prior to injury.
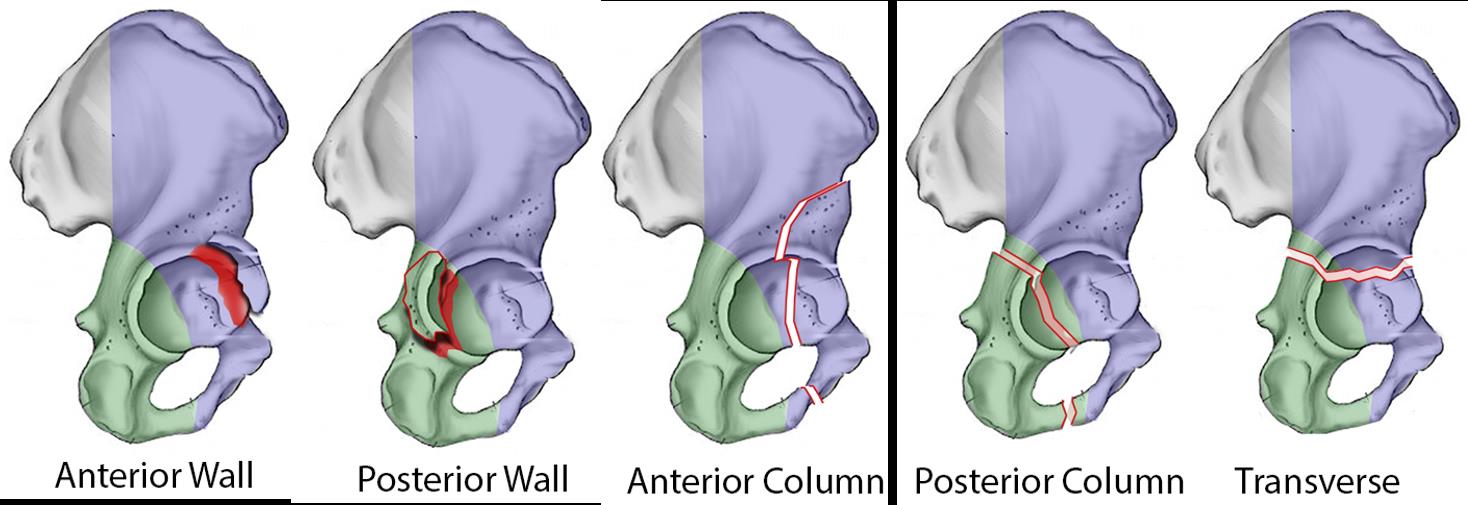
* Severe Articular Comminution: Unreconstructible posterior wall fractures or significant marginal impaction (the "gull sign").
* Femoral Head Damage: Concomitant severe abrasive wear, impaction fractures (Pipkin injuries), or osteochondral defects of the femoral head.
* Pathologic Fractures: Fractures secondary to metastatic disease or severe metabolic bone disorders.
Surgical Warning: Acute THA for acetabular fractures should not be viewed as an "easy way out" of a complex ORIF. The procedure is technically demanding, requiring simultaneous stabilization of the pelvic ring and achieving rigid initial stability of the acetabular component in a compromised bone bed.
Biomechanics and Preoperative Planning
The fundamental biomechanical challenge in acute THA for acetabular fractures is achieving primary stability of the cementless acetabular shell within a discontinuous hemipelvis. The surgical strategy mandates adjunctive fixation of the acetabular fracture—typically with plates, cables, or column screws—followed by multiple screw fixation of a highly porous, multi-hole acetabular cup.
We have successfully utilized this combined technique for the salvage of hip function in older individuals with complex fracture patterns.
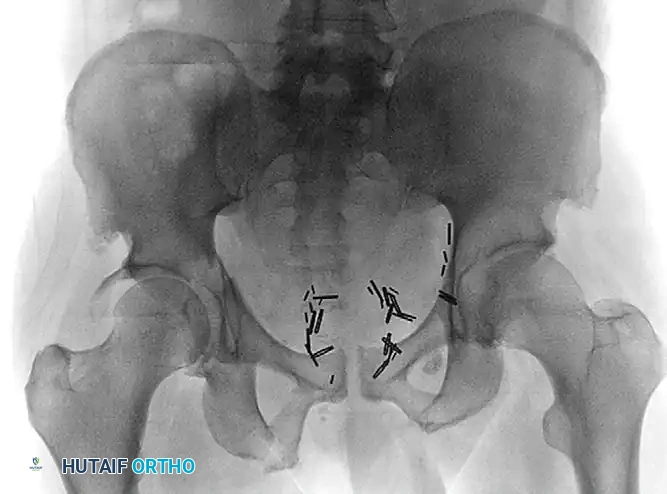
Preoperative anteroposterior (AP) radiograph demonstrating a complex transverse posterior wall fracture in an elderly patient, characterized by significant displacement and articular incongruity.
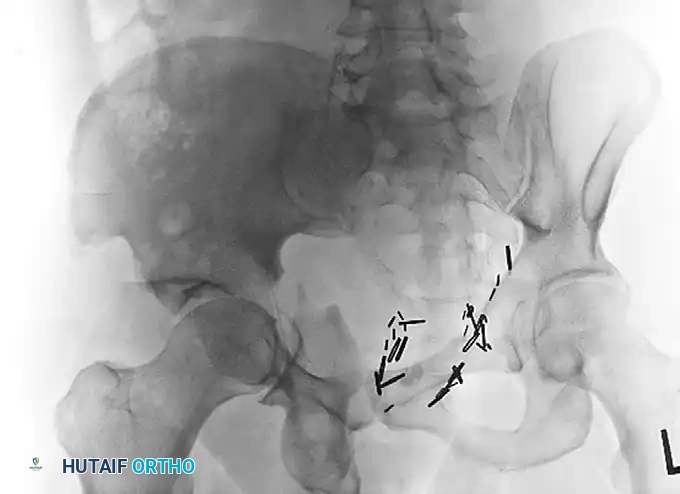
Preoperative Judet oblique radiograph highlighting the extent of posterior column displacement and wall comminution, indicating a poor prognosis for isolated joint preservation.
One primary concern with this technique is the risk that the cementless acetabular component could fail to be adequately incorporated into the healing acetabular bed, leading to aseptic loosening. However, clinical evidence supports the efficacy of this approach. In a landmark series of 57 patients, Mears and Velyvis demonstrated that while the acetabular shells would routinely subside 1 to 3 mm during the initial phase of fracture healing, they typically stabilized thereafter without progressing to clinical failure.
Surgical Approach and Step-by-Step Technique
The choice of surgical approach is critical. Extensile approaches (e.g., extended iliofemoral) should be strictly avoided to minimize the risk of massive soft tissue devitalization, heterotopic ossification, and deep periprosthetic joint infection. A standard Kocher-Langenbeck or a modified posterior approach is generally preferred, as it allows simultaneous access for posterior column/wall fixation and femoral stem implantation.
- Positioning: The patient is placed in the lateral decubitus position on a radiolucent table. Rigid pelvic positioning is essential for accurate assessment of cup anteversion and inclination.
- Exposure: A standard posterior approach to the hip is performed. The sciatic nerve is identified and protected throughout the procedure.
- Fracture Reduction and Fixation: Before any reaming occurs, the acetabular fracture must be reduced and stabilized. This often involves lag screw fixation of the columns and buttress plating of the posterior wall. The hardware must be placed peripherally to avoid interfering with the subsequent hemispherical reaming.
- Acetabular Preparation: The acetabulum is reamed carefully. In osteoporotic bone, line-to-line reaming or minimal under-reaming (1 mm) is preferred to prevent iatrogenic fracture propagation.
- Component Implantation: A highly porous, multi-hole titanium acetabular shell is impacted into place. The cup itself acts as an internal hemispherical plate, bridging the fracture lines.
- Screw Fixation: Multiple screws are placed through the cup into the intact ilium (safe zone), ischium, and pubis to achieve absolute rigid fixation.
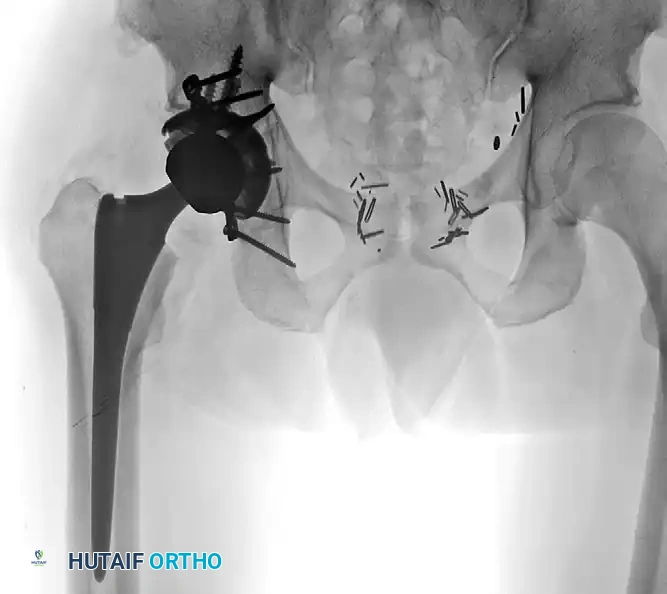
Postoperative AP radiograph illustrating the combined treatment: acute fracture fixation with posterior plating, integrated with a primary total hip arthroplasty utilizing a multi-hole cup and multiple supplementary screws for rigid construct stability.
Delayed THA for Posttraumatic Arthritis
When initial nonoperative management or ORIF fails, patients often develop severe posttraumatic arthritis requiring delayed THA. Total hip arthroplasty performed for posttraumatic arthritis after an acetabular fracture is significantly more complex than primary THA for primary degenerative osteoarthritis.
Surgeons must anticipate:
* Longer Operative Times: Due to the need for hardware removal, altered anatomy, and extensive scar tissue.
* Greater Blood Loss: Increased transfusion requirements are routinely observed.
* Infection Risk: The presence of prior incisions and retained hardware elevates the risk of periprosthetic joint infection.
Each of these operative challenges is magnified in patients who have undergone prior ORIF for their acetabular fractures compared with patients who had initial nonoperative treatment. Despite these technical hurdles, long-term outcomes are highly favorable. The 10-year survivorship of these hips is reported at 97%, which correlates well with a 6% radiographic 10-year loosening rate reported in similar patient populations.
HIGH-ENERGY PELVIC FRACTURES: RESUSCITATION AND RECONSTRUCTION
Fractures of the adult pelvis, exclusive of the acetabulum, generally fall into two distinct epidemiological categories: stable fractures resulting from low-energy trauma (such as ground-level falls in elderly, osteoporotic patients) and unstable fractures caused by high-energy trauma.
Low-energy trauma to the pelvis generally produces stable fractures (e.g., isolated pubic rami fractures) that can be treated symptomatically. These patients require crutch- or walker-assisted ambulation, adequate analgesia, and deep vein thrombosis (DVT) prophylaxis, and the fractures can be expected to heal uneventfully in most cases.
Conversely, high-energy pelvic fractures result in significant morbidity and mortality and demand a multidisciplinary, aggressive approach. The focus of this section is on these high-energy injuries, their management in both the resuscitative and reconstructive phases, and their potential life-threatening complications.
Epidemiology and Associated Injuries
High-energy pelvic fractures result most commonly from motor vehicle accidents, falls from significant heights, motorcycle accidents, automobile-pedestrian encounters, and industrial crush injuries. The pelvis is a highly vascularized ring structure housing critical genitourinary and neurologic anatomy.
The potential complications of high-energy pelvic fractures include:
* Vascular Injuries: Disruption of the presacral venous plexus or branches of the internal iliac artery (e.g., superior gluteal, internal pudendal, or obturator arteries).
* Neurologic Injuries: Traction or crush injuries to the lumbosacral plexus, particularly the L5 and S1 nerve roots in unstable vertical shear or sacral fractures.
* Visceral Injuries: Rupture of the bladder, urethral transection, or bowel perforations.
* Soft Tissue Trauma: Severe degloving injuries (Morel-Lavallée lesions) to the surrounding soft tissues, both open and closed, which severely complicate surgical approaches and increase infection risk.
Reported mortality from severe pelvic fractures ranges from 10% to as high as 50% in earlier series of open pelvic fractures. Risk factors for increased mortality include advanced patient age, a high Injury Severity Score (ISS), associated closed-head or visceral injuries, massive blood loss, profound hypotension, coagulopathy, and the presence of unstable or open pelvic fractures. Early mortality most commonly results from uncontrollable hemorrhage or severe closed-head injury; late mortality typically occurs from sepsis or multiple system organ failure (MSOF).
Acute Resuscitation and Hemorrhage Control
The initial management of a patient with a high-energy pelvic ring injury must strictly adhere to Advanced Trauma Life Support (ATLS) protocols. Hemodynamic instability in the presence of a mechanically unstable pelvic ring is a surgical emergency.
Pelvic Binders and Circumferential Compression
The immediate application of a pelvic orthotic device (pelvic binder or tightly wrapped sheet) is the first-line intervention to apply circumferential pressure in patients with unstable, complex pelvic fractures (e.g., "open book" APC-II or APC-III injuries). By reducing pelvic volume, the binder promotes the tamponade of venous bleeding and stabilizes the fracture ends to prevent clot disruption.
Clinical Pearl: Accurate placement of the pelvic binder is paramount. It must be centered directly over the greater trochanters. One recent study noted that inaccurate placement—specifically above the level of the greater trochanters over the iliac crests—is associated with inadequate fracture reduction and can paradoxically worsen the deformity in certain fracture patterns.
While widely adopted, the literature presents some debate. For instance, Ghaemmaghami et al. did not find that pelvic binders significantly reduced overall hemorrhage or mortality associated with pelvic fractures in their specific cohort, highlighting that binders are a temporizing measure, not a definitive treatment.
External Fixation
Once the patient is in the controlled environment of the operating room, an external fixator can be applied to maintain stability of the pelvis while allowing general surgeons and urologists access to the abdomen and perineum for exploratory laparotomy or diversion procedures.
A significant reduction in transfusion requirements has been reported in patients with unstable pelvic fractures who were treated with immediate external fixation compared with those who did not undergo immediate fixation.
* Anterior Frame: Standard supra-acetabular or iliac crest pins are highly effective for anterior ring disruptions.
* C-Clamp: Injuries with significant posterior displacement (e.g., sacroiliac joint disruptions) may benefit from a C-clamp type of external fixator. This device applies direct compression across the sacroiliac joints and is ideally applied in the operating room when the situation allows.
Angiography versus Preperitoneal Packing
The patient with a pelvic ring injury who exhibits persistent hypotension after circumferential pelvic binding, fluid resuscitation, and ruling out of other sources of bleeding (via FAST exam or chest radiograph) requires immediate intervention for pelvic hemorrhage. Hemorrhage frequently results from the expansive fracture surfaces and the rich network of small venous vessels in the retroperitoneum.
- Angiography and Embolization: Only 5% to 10% of patients with pelvic fractures bleed from major arterial sources that can be identified by angiography and treated with transcatheter embolization. However, higher rates of arterial bleeding in the geriatric population have been noted by Henry et al., making angiography highly relevant in older trauma patients.
- Preperitoneal Pelvic Packing (PPP): More recently, highly favorable results have been reported with direct retroperitoneal packing combined with external fixation. This technique involves a midline suprapubic incision, entering the space of Retzius, and packing laparotomy sponges directly against the bleeding presacral and paravesical venous plexuses.
An algorithm by O’Brien and Dickson has been proposed to navigate the choice between angiography and packing; however, the authors recommended that each institution develop its own protocol, depending heavily on local resources, the immediate availability of an interventional radiologist, and trauma bay facilities. While PPP is highly popular in Europe and has been adopted in major US trauma centers, its universal implementation requires further investigation in the United States, where the structure of trauma care and resource allocation differs.
Management of Open Pelvic Fractures
Open pelvic fractures represent one of the most devastating injuries in orthopedic trauma, with reported mortality rates historically reaching up to 50%. The pathophysiology of this high mortality is twofold:
1. Loss of Tamponade: If the retroperitoneal space is open to the environment (via a perineal, vaginal, or rectal laceration), no natural tamponade effect can occur. Venous bleeding continues unabated, leading to rapid exsanguination.
2. Sepsis: Sepsis caused by massive fecal contamination of the massive pelvic hematoma is a major cause of late mortality.
Management mandates immediate hemorrhage control (packing/binders), aggressive broad-spectrum intravenous antibiotics, and urgent surgical debridement. A diverting colostomy is frequently required if there is any rectal involvement or massive perineal soft tissue loss to prevent continuous contamination of the orthopedic surgical site.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
Whether treating an acetabular fracture with acute THA or managing a reconstructed high-energy pelvic ring injury, postoperative rehabilitation must be meticulously tailored to the stability of the fixation.
For patients undergoing acute THA for acetabular fractures:
* Weight-Bearing: Patients are typically allowed immediate toe-touch or partial weight-bearing, progressing to full weight-bearing by 6 to 8 weeks, depending on the radiographic evidence of fracture consolidation and component stability.
* Precautions: Standard posterior hip precautions are enforced for 6 to 12 weeks to prevent dislocation, particularly given the compromised soft tissue envelope.
* DVT Prophylaxis: Aggressive chemical prophylaxis (e.g., low molecular weight heparin or direct oral anticoagulants) is mandatory for a minimum of 28 to 35 days, given the high risk of venous thromboembolism in pelvic trauma.
Routine clinical and radiographic follow-up at 2 weeks, 6 weeks, 3 months, and 1 year is essential to monitor for component subsidence, heterotopic ossification, and signs of periprosthetic joint infection. Through rigorous adherence to biomechanical principles and multidisciplinary trauma protocols, orthopedic surgeons can significantly reduce the morbidity and mortality associated with these catastrophic injuries.
You Might Also Like