High-Yield Orthopedic Board Review MCQs

High-Yield Orthopedic Board Review MCQs
This module contains 50 advanced orthopedic multiple-choice questions meticulously developed to mirror the American Board of Orthopaedic Surgery (ABOS) Part I and AAOS OITE examinations. These questions are comprehensively derived from the clinical teaching case: Orthopaedic Board Review MCQs: High-Yield Practice Questions.
Comprehensive Exam
00:00
Start Quiz
Question 1
A 72-year-old female sustains a displaced femoral neck fracture after a mechanical fall. The primary blood supply at risk of disruption, which leads to a high incidence of avascular necrosis of the femoral head in this injury pattern, originates directly from which of the following arteries?
Explanation
Correct Answer: A. Medial circumflex femoral artery
Avascular necrosis (AVN) of the femoral head is a major complication following displaced femoral neck fractures. The primary blood supply to the adult femoral head is derived from the medial circumflex femoral artery (MCFA), specifically its lateral epiphyseal branches. Displaced fractures disrupt this retinacular blood supply. The MCFA is a branch of the profunda femoris artery. The artery of the ligamentum teres provides a negligible amount of blood in adults, and the lateral circumflex femoral artery primarily supplies the anterior portion of the femoral neck and greater trochanter.
Question 2
A 5-year-old boy falls from monkey bars and sustains an extension-type supracondylar humerus fracture. On presentation to the emergency department, his hand is pale and pulseless, but he has normal capillary refill and warm fingers. What is the most appropriate next step in management?
Explanation
Correct Answer: B. Closed reduction and percutaneous pinning, followed by vascular reassessment
A pulseless hand in the setting of a pediatric supracondylar humerus fracture is a vascular emergency, often due to kinking, spasm, or entrapment of the brachial artery over the proximal fracture fragment. The immediate and most appropriate next step is urgent closed reduction and percutaneous pinning. In the majority of cases, anatomic reduction relieves the tension on the neurovascular bundle and restores perfusion. If the hand remains pulseless and poorly perfused (white/cold) after reduction, open exploration is indicated. CT angiography delays definitive treatment and is not indicated in the acute setting.
Question 3
A 13-year-old obese male presents with a 3-week history of left knee pain and a limp. He denies any recent trauma or systemic symptoms. On examination, as the left hip is passively flexed, it obligatorily deviates into external rotation. Radiographs of the knee are unremarkable. Which of the following is the most likely underlying pathophysiology of his condition?
Explanation
Correct Answer: B. Shear failure through the hypertrophic zone of the physis
The clinical vignette describes Slipped Capital Femoral Epiphysis (SCFE), which classically presents in obese adolescents with a painful limp, referred knee pain, and obligate external rotation of the hip during flexion. The underlying pathophysiology of SCFE involves mechanical shear failure through the hypertrophic zone of the physis (growth plate) due to increased mechanical stress (obesity) and hormonal changes during the adolescent growth spurt. Avascular necrosis of the epiphysis describes Legg-Calvé-Perthes disease, which typically affects younger children (ages 4-8).
Question 4
A 14-year-old male presents with vague anterior knee pain and intermittent catching. Radiographs reveal an osteochondral lesion consistent with osteochondritis dissecans (OCD). Based on the most common location for this pathology, which specific anatomical site is most likely affected?
Explanation
Correct Answer: A. Lateral aspect of the medial femoral condyle
Osteochondritis dissecans (OCD) of the knee most commonly affects the lateral aspect of the medial femoral condyle (accounting for approximately 70-80% of cases). It is thought to result from repetitive microtrauma leading to subchondral bone ischemia and subsequent fragmentation of the overlying articular cartilage and bone. The classic radiographic finding is a crescent-shaped radiolucency. The lateral femoral condyle is the second most common site.
Question 5
A 9-year-old African American boy with homozygous hemoglobin SS disease presents with a 4-day history of fever, localized distal femoral pain, and an inability to bear weight. Blood cultures and a bone aspirate are obtained. While Staphylococcus aureus remains a common pathogen, this patient is at uniquely high risk for osteomyelitis caused by which of the following encapsulated, gram-negative bacilli?
Explanation
Correct Answer: C. Salmonella typhimurium
Patients with sickle cell disease are functionally asplenic and have a uniquely high risk of osteomyelitis caused by Salmonella species, an encapsulated, gram-negative bacillus. While Staphylococcus aureus is still the most common overall cause of osteomyelitis in this population, the incidence of Salmonella is disproportionately high compared to the general population. Microinfarctions in the bowel wall are thought to allow Salmonella to translocate into the bloodstream and seed infarcted bone.
Question 6
A 68-year-old male presents with insidious onset of right hip pain 14 months after a primary total hip arthroplasty. Inflammatory markers are mildly elevated. Joint aspiration yields a synovial fluid leukocyte count of 4,500 cells/μL with 75% neutrophils. Cultures grow a coagulase-negative, Gram-positive coccus that forms biofilms. Which of the following organisms is most likely responsible?
Explanation
Correct Answer: B. Staphylococcus epidermidis
Prosthetic joint infections (PJIs) are most commonly caused by coagulase-negative staphylococci, particularly Staphylococcus epidermidis, especially in delayed or late-onset presentations (3-24 months post-op). S. epidermidis is a normal skin commensal that possesses a unique ability to adhere to orthopedic implants and form a protective glycocalyx biofilm. This biofilm makes the bacteria highly resistant to host immune responses and systemic antibiotics. S. aureus is coagulase-positive and typically presents more acutely.
Question 7
A 74-year-old female presents with chronic right shoulder pain and an inability to actively elevate her arm above 45 degrees. Radiographs demonstrate severe glenohumeral joint space narrowing and superior migration of the humeral head, articulating with the acromion. A reverse total shoulder arthroplasty (RTSA) is planned. The biomechanical advantage of this prosthesis relies primarily on the function of which of the following muscles to achieve active elevation?
Explanation
Correct Answer: C. Deltoid
Reverse total shoulder arthroplasty (RTSA) is indicated for rotator cuff tear arthropathy, where a massive, irreparable rotator cuff tear leads to superior migration of the humeral head and pseudoparalysis. The RTSA design reverses the normal anatomy by placing a glenosphere on the glenoid and a concave cup on the humerus. This medializes and distalizes the center of rotation, significantly increasing the moment arm and resting tension of the deltoid muscle. This allows the deltoid to initiate and maintain active shoulder elevation even in the absence of a functional supraspinatus.
Question 8
A 45-year-old construction worker experiences acute low back pain radiating down the lateral aspect of his left leg to the dorsum of his foot. Examination reveals a positive straight leg raise test on the left. He demonstrates 3/5 strength in ankle dorsiflexion and great toe extension. The Achilles and patellar reflexes are symmetric and 2+. Which of the following nerve roots is most likely compressed?
Explanation
Correct Answer: C. L5
A posterolateral disc herniation at the L4-L5 level typically impinges the traversing L5 nerve root. The L5 nerve root provides motor innervation to the extensor hallucis longus (EHL, great toe extension), tibialis anterior (ankle dorsiflexion), and gluteus medius (hip abduction). It provides sensory innervation to the lateral calf and the dorsum of the foot. The L4 root (affected by L3-L4 herniation) mediates the patellar reflex, and the S1 root (affected by L5-S1 herniation) mediates the Achilles reflex and ankle plantarflexion.
Question 9
A 32-year-old manual laborer presents with chronic, progressive dorsal wrist pain and decreased grip strength. He denies any specific acute trauma. Radiographs reveal sclerosis and fragmentation of the lunate. Which of the following anatomical variants is most frequently associated with the development of this condition?
Explanation
Correct Answer: B. Negative ulnar variance
Kienböck's disease is the eponym for avascular necrosis of the lunate. It is strongly associated with negative ulnar variance, a condition where the distal ulna is abnormally short relative to the distal radius. This anatomical variant alters the biomechanics of the radiocarpal joint, leading to increased shear forces and mechanical loading specifically on the lunate, predisposing it to microfracture and subsequent vascular compromise.
Question 10
A 28-year-old male is struck by a motor vehicle and sustains a severely displaced, high-energy Schatzker VI tibial plateau fracture. Twelve hours post-admission, he complains of excruciating leg pain that is out of proportion to the injury and not relieved by intravenous opioids. Which of the following is the most sensitive early clinical finding for the suspected complication?
Explanation
Correct Answer: C. Pain with passive stretch of the involved compartment muscles
Acute compartment syndrome is a devastating complication of high-energy fractures, particularly tibial plateau and tibial shaft fractures. The earliest and most sensitive clinical sign is pain out of proportion to the injury, specifically exacerbated by passive stretch of the muscles within the involved compartment. The classic "5 Ps" (pain, pallor, pulselessness, paresthesias, paralysis) are often taught, but pallor, pulselessness, and paralysis are late signs indicating irreversible tissue ischemia and muscle necrosis.
Question 11
A 5-year-old boy falls from monkey bars and sustains a Gartland type III supracondylar humerus fracture. On presentation to the emergency department, his hand is pale and pulseless, but he has brisk capillary refill and normal motor function of the hand. What is the most appropriate next step in management?
Explanation
Correct Answer: Closed reduction and percutaneous pinning, followed by reassessment of the pulse
In a pulseless but well-perfused (pink, brisk capillary refill) hand following a displaced supracondylar humerus fracture, the initial step is urgent closed reduction and percutaneous pinning. Often, the brachial artery is kinked, tethered over the proximal fracture fragment, or in spasm, and anatomic reduction restores the pulse. If the hand remains pulseless and becomes poorly perfused (white/ischemic) after reduction, open exploration of the brachial artery is indicated. CT angiography delays definitive treatment and is not indicated in the acute setting of a pulseless, pink hand.
Question 12
A 72-year-old female undergoes a reverse total shoulder arthroplasty (RTSA) for severe rotator cuff tear arthropathy. Which of the following best describes the biomechanical alteration achieved by this implant design to restore active shoulder elevation?
Explanation
Correct Answer: Medialization and distalization of the center of rotation to increase the deltoid moment arm and tension
The reverse total shoulder arthroplasty (RTSA) is designed to compensate for a deficient rotator cuff. By placing the glenosphere on the native glenoid and the concave articular surface on the humerus, the center of rotation is medialized and distalized compared to the native anatomy. This significantly increases the moment arm of the deltoid muscle and tensions its fibers, allowing the deltoid to act as the primary elevator of the shoulder without the need for a functioning supraspinatus to provide a compressive fulcrum.
Question 13
A 22-year-old male falls onto an outstretched hand and sustains a proximal pole scaphoid fracture. He is counseled that he is at high risk for avascular necrosis (AVN) and nonunion. Which of the following best describes the primary arterial supply to the scaphoid that explains this risk?
Explanation
Correct Answer: Blood supply enters distally via branches of the radial artery and flows in a retrograde fashion to the proximal pole
The scaphoid receives its primary blood supply (70-80%) from the dorsal carpal branch of the radial artery, which enters the bone distally at the dorsal ridge and flows in a retrograde fashion to supply the proximal pole. Fractures at the waist or proximal pole disrupt this retrograde flow, isolating the proximal fragment from its blood supply. This places the proximal pole at a high risk for avascular necrosis and nonunion, often necessitating surgical intervention.
Question 14
A 45-year-old male presents with a "foot drop" and numbness over the dorsum of his foot. To differentiate between a compressive common peroneal neuropathy at the fibular head and an L5 radiculopathy from an L4-L5 disc herniation, weakness in which of the following muscles would most specifically point to an L5 radiculopathy?
Explanation
Correct Answer: Tibialis posterior
Both the common peroneal nerve and the L5 nerve root innervate the tibialis anterior, extensor hallucis longus (EHL), extensor digitorum brevis (EDB), and peroneus longus. However, the tibialis posterior is innervated by the tibial nerve, which receives its primary motor contributions from the L4 and L5 nerve roots. Therefore, weakness in foot inversion (tibialis posterior function) in the setting of a foot drop indicates a lesion proximal to the sciatic bifurcation, specifically an L5 radiculopathy, rather than an isolated common peroneal nerve palsy.
Question 15
A 13-year-old overweight boy presents with a 3-week history of left knee pain and a limp. On examination, as his left hip is passively flexed, it obligatorily goes into external rotation. Radiographs reveal a widening of the left proximal femoral physis. Which of the following is the most appropriate definitive management?
Explanation
Correct Answer: In situ single screw fixation of the proximal femoral epiphysis
The patient's presentation is classic for a Slipped Capital Femoral Epiphysis (SCFE). The obligate external rotation with passive hip flexion is a hallmark clinical sign. The standard of care for a stable SCFE is in situ fixation, typically with a single cannulated screw placed centrally into the epiphysis. This prevents further slippage and promotes premature physeal closure. Closed reduction is contraindicated as it significantly increases the risk of avascular necrosis.
Question 16
A 32-year-old male sustains a high-energy closed tibial plateau fracture. Twelve hours later, he develops severe leg pain out of proportion to the injury, exacerbated by passive stretch of the toes. Which of the following pathophysiological mechanisms is the primary initiator of the tissue ischemia in this condition?
Explanation
Correct Answer: Venous outflow obstruction leading to increased intracompartmental pressure and subsequent collapse of the capillary bed
Acute compartment syndrome occurs when increased pressure within a closed fascial space compromises tissue perfusion. The cascade begins with increased tissue pressure (from edema or hematoma) that exceeds venous pressure, leading to venous outflow obstruction. This further increases intracompartmental pressure, eventually exceeding capillary perfusion pressure. This causes capillary collapse and severe tissue ischemia. Arterial inflow is typically maintained until very late stages, which is why distal pulses are usually present even in severe compartment syndrome.
Question 17
A 15-year-old boy presents with a painful mass around his distal femur. Radiographs show a destructive, mixed lytic and sclerotic lesion in the metaphysis with a "sunburst" periosteal reaction and a Codman triangle. Biopsy confirms the most likely diagnosis. Which of the following histologic findings is required for this diagnosis?
Explanation
Correct Answer: Production of osteoid by malignant mesenchymal cells
The clinical and radiographic presentation is classic for conventional osteosarcoma. The defining histologic feature required for the diagnosis of osteosarcoma is the production of osteoid (unmineralized bone matrix) directly by malignant mesenchymal cells. Small round blue cells are characteristic of Ewing sarcoma, malignant cartilage is seen in chondrosarcoma, and giant cells are the hallmark of Giant Cell Tumor of bone.
Question 18
A 68-year-old male presents with a chronically painful total knee arthroplasty, 2 years post-operatively. Aspiration yields a synovial fluid white blood cell count of 45,000 cells/μL with 90% neutrophils. Cultures grow a coagulase-negative Staphylococcus. Which of the following characteristics of this organism makes eradication difficult without implant removal?
Explanation
Correct Answer: Formation of a polysaccharide glycocalyx biofilm
Coagulase-negative staphylococci (e.g., S. epidermidis) are a leading cause of chronic prosthetic joint infections. Their primary virulence factor in this setting is the ability to adhere to the implant surface and produce a polysaccharide glycocalyx, forming a dense biofilm. This biofilm protects the bacteria from the host immune system and systemic antibiotics, typically necessitating surgical removal of the implant (e.g., two-stage revision) for definitive cure.
Question 19
A 42-year-old weekend warrior sustains an acute Achilles tendon rupture while playing tennis. He elects for non-operative management. The Achilles tendon is most vulnerable to rupture in a specific watershed zone. Where is this zone located relative to the calcaneal insertion?
Explanation
Correct Answer: 2 to 6 cm proximal to the calcaneal insertion
The Achilles tendon has a watershed area of relative hypovascularity located approximately 2 to 6 cm proximal to its insertion on the calcaneus. This decreased blood supply, combined with repetitive mechanical stress, makes this specific region the most common site for degenerative tendinopathy and acute ruptures.
Question 20
A 35-year-old manual laborer presents with chronic dorsal wrist pain. Radiographs reveal sclerosis and fragmentation of the lunate, with proximal migration of the capitate and a negative ulnar variance. This represents Lichtman Stage IIIb Kienböck's disease. Which of the following biomechanical factors is most strongly associated with the development of this condition?
Explanation
Correct Answer: Negative ulnar variance
Kienböck's disease is avascular necrosis of the lunate. It is strongly associated with negative ulnar variance (where the ulna is shorter than the radius at the distal articular surface). This anatomic variant leads to increased shear and compressive forces transmitted from the radius directly to the lunate, predisposing it to microfracture, vascular compromise, and subsequent osteonecrosis. Joint leveling procedures (e.g., radial shortening osteotomy) are often utilized to offload the lunate in early stages.
Question 21
A 5-year-old boy is brought to the emergency department after falling from monkey bars. He sustained a completely displaced extension-type supracondylar humerus fracture. His hand is pink and well-perfused, but he is unable to make an "OK" sign with his thumb and index finger. Which of the following structures is most likely injured, and what is its typical anatomical course at the elbow?
Explanation
Correct Answer: A
The inability to make an "OK" sign indicates an injury to the anterior interosseous nerve (AIN), which innervates the flexor pollicis longus and the flexor digitorum profundus to the index finger. AIN neuropraxia is the most common nerve injury associated with extension-type supracondylar humerus fractures. The AIN is a motor branch of the median nerve, which passes between the humeral and ulnar heads of the pronator teres muscle in the proximal forearm.
Question 22
A 24-year-old female soccer player undergoes anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. The surgeon aims to anatomically reconstruct the anteromedial (AM) and posterolateral (PL) bundles. Which of the following best describes the biomechanical function and tensioning pattern of the native ACL bundles?
Explanation
Correct Answer: C
The anterior cruciate ligament (ACL) consists of two distinct functional bundles named for their tibial insertion sites: the anteromedial (AM) and posterolateral (PL) bundles. The AM bundle is tightest in flexion and is the primary restraint to anterior tibial translation. The PL bundle is tightest in extension and is the primary restraint to rotatory loads, which is clinically evaluated by the pivot shift test.
Question 23
A 13-year-old obese male presents with a 2-week history of left groin pain and a limp. He is currently unable to bear weight on the affected limb. Radiographs reveal a slipped capital femoral epiphysis (SCFE). He undergoes urgent in situ percutaneous pinning. Which of the following factors is most strongly associated with the development of avascular necrosis (AVN) of the femoral head in this patient?
Explanation
Correct Answer: C
The Loder classification categorizes Slipped Capital Femoral Epiphysis (SCFE) into stable and unstable based on the patient's ability to bear weight (with or without crutches). An "unstable" SCFE is defined by the inability to bear weight and carries a significantly higher risk of avascular necrosis (AVN) of the femoral head (up to 47%) compared to stable SCFE, where the AVN rate is typically less than 10%. While slip angle and BMI are important factors in the disease process, stability is the primary prognosticator for AVN.
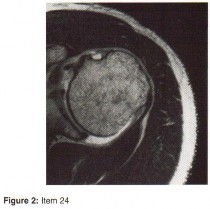
Question 24
A 32-year-old male sustains a closed, spiral fracture of the distal third of the humeral shaft (Holstein-Lewis fracture) after an arm-wrestling match. On examination, he has a wrist drop and absent sensation over the dorsal first web space. What is the most appropriate initial management for this patient's neurologic deficit?
Explanation
Correct Answer: B
Primary radial nerve palsy in the setting of a closed humeral shaft fracture is generally treated observationally with closed reduction and functional bracing (e.g., Sarmiento brace). The majority of these injuries (up to 90%) represent neuropraxia or axonotmesis and will recover spontaneously over 3 to 4 months. Immediate surgical exploration is indicated for open fractures, associated vascular injury, or if the nerve palsy develops after a closed reduction attempt (secondary palsy), which suggests nerve entrapment in the fracture site.
Question 25
A 6-year-old boy is diagnosed with Legg-Calvé-Perthes disease. His orthopedic surgeon explains that his prognosis depends heavily on the extent of epiphyseal involvement. According to the lateral pillar (Herring) classification, which radiographic finding during the fragmentation stage is associated with the worst prognosis?
Explanation
Correct Answer: B
The Herring lateral pillar classification is utilized during the fragmentation stage of Legg-Calvé-Perthes disease to determine prognosis based on the height of the lateral portion of the capital femoral epiphysis. Group A has no lateral pillar involvement. Group B has >50% lateral pillar height maintained. Group C has <50% lateral pillar height maintained and is associated with the worst prognosis, often leading to aspherical congruency or incongruency of the hip joint and early-onset osteoarthritis.
Question 26
A 45-year-old male undergoes an open reduction and internal fixation of a proximal humerus fracture via a deltopectoral approach. Postoperatively, he has profound weakness in shoulder abduction and numbness over the lateral aspect of the shoulder. The injured nerve exits the axilla through a specific anatomic space. What are the borders of this space?
Explanation
Correct Answer: A
The patient has an iatrogenic axillary nerve injury. The axillary nerve and the posterior circumflex humeral artery exit the axilla posteriorly through the quadrilateral space. The borders of the quadrilateral space are: superiorly the teres minor (viewed posteriorly) or subscapularis (viewed anteriorly), inferiorly the teres major, medially the long head of the triceps, and laterally the surgical neck of the humerus.
Question 27
A 68-year-old female with severe varus gonarthrosis is undergoing a total knee arthroplasty. After making the initial bone cuts, the surgeon notes that the knee is tight medially in both flexion and extension. Which of the following structures should be released first to balance the knee?
Explanation
Correct Answer: B
In a varus knee, medial tightness in both flexion and extension requires a sequential medial release to achieve a balanced gap. The standard sequence begins with the removal of medial osteophytes, which often provides significant correction. If still tight, the next step is the release of the deep medial collateral ligament (dMCL). If further release is needed, the posteromedial capsule and semimembranosus are released, followed by the superficial MCL (sMCL), and finally the pes anserinus if absolutely necessary.
Question 28
A 55-year-old female presents with severe, long-standing carpal tunnel syndrome. She has profound thenar atrophy. During an open carpal tunnel release, the surgeon must be careful to avoid injuring the recurrent motor branch of the median nerve. Which of the following muscles is innervated by this specific branch?
Explanation
Correct Answer: C
The recurrent motor branch of the median nerve, often referred to as the "million dollar nerve," innervates the three thenar muscles: the opponens pollicis, the abductor pollicis brevis (APB), and the superficial head of the flexor pollicis brevis (FPB). The adductor pollicis, deep head of the FPB, and interossei are innervated by the deep branch of the ulnar nerve.
Question 29
A 72-year-old male complains of bilateral calf and thigh pain that occurs after walking two blocks. The pain is relieved when he sits down or leans forward on a shopping cart. He denies pain when riding a stationary bicycle. His pedal pulses are 2+ bilaterally. Which of the following pathophysiologic mechanisms is the primary cause of his symptoms?
Explanation
Correct Answer: B
The patient's symptoms are classic for neurogenic claudication secondary to lumbar spinal stenosis. The relief of symptoms with lumbar flexion (e.g., leaning on a shopping cart, riding a bicycle) occurs because flexion increases the cross-sectional area of the spinal canal, relieving pressure on the neural elements. The primary degenerative changes causing central canal stenosis are facet joint hypertrophy, ligamentum flavum hypertrophy, and bulging of the intervertebral disc. Vascular claudication would cause pain with any exertion (including cycling) and is relieved by rest alone, not postural changes.
Question 30
A 4-year-old boy presents with a 3-day history of fever, irritability, and refusal to bear weight on his right leg. Laboratory studies show an elevated CRP and ESR. MRI reveals marrow edema in the distal femoral metaphysis with a small subperiosteal abscess. What anatomical feature of the pediatric long bone makes the metaphysis the most common site for acute hematogenous osteomyelitis?
Explanation
Correct Answer: B
In children, acute hematogenous osteomyelitis most commonly affects the metaphysis of long bones. The terminal branches of the nutrient artery loop near the physis and empty into large, dilated venous sinusoids. The sluggish, turbulent blood flow in these sinusoids creates an ideal environment for bacterial deposition and proliferation. Furthermore, there is a relative lack of active phagocytic cells in this specific region, further contributing to the susceptibility to infection.
Question 31
A 6-year-old boy falls from a swing and sustains an extension-type supracondylar humerus fracture. Radiographs show that the distal fracture fragment is displaced posterolaterally. Based on this specific displacement pattern, which nerve is at the highest risk of injury from the proximal fracture fragment?
Explanation
Correct Answer: Anterior interosseous nerve
In extension-type supracondylar humerus fractures, the direction of distal fragment displacement dictates which neurovascular structures are at risk from the sharp proximal fragment. When the distal fragment displaces posterolaterally, the proximal fragment is directed anteromedially. This anteromedial spike places the median nerve (specifically its anterior interosseous branch) and the brachial artery at the highest risk of injury. Conversely, if the distal fragment displaces posteromedially, the proximal fragment is directed anterolaterally, placing the radial nerve at risk. The anterior interosseous nerve (AIN) is the most commonly injured nerve overall in pediatric supracondylar humerus fractures.
Question 32
A 13-year-old obese male presents with acute-on-chronic left hip pain. He is unable to bear weight on the affected limb, even with the assistance of crutches. Radiographs confirm a slipped capital femoral epiphysis (SCFE). According to the Loder classification, what is the most significant prognostic implication of his inability to bear weight?
Explanation
Correct Answer: Increased risk of avascular necrosis (AVN)
The Loder classification categorizes slipped capital femoral epiphysis (SCFE) into stable and unstable based on the patient's ability to bear weight. An unstable SCFE is defined by the inability to ambulate with or without crutches. This distinction is critical because it carries significant prognostic value regarding the development of avascular necrosis (AVN). Unstable SCFE has a high rate of AVN, historically reported between 24% and 47%, due to the acute disruption of the retinacular vessels supplying the femoral head. Stable SCFE, where the patient can bear weight, has an AVN rate of nearly 0%.
Question 33
A 35-year-old carpenter presents with insidious onset of dorsal wrist pain, swelling, and decreased grip strength. Radiographs demonstrate sclerosis and collapse of the lunate. Which of the following radiographic anatomic variants is most classically associated with the pathogenesis of this condition?
Explanation
Correct Answer: Negative ulnar variance
The patient's presentation and radiographic findings are diagnostic of Kienböck's disease, which is avascular necrosis (osteonecrosis) of the lunate. The etiology is multifactorial, involving both vascular and mechanical factors. Mechanically, negative ulnar variance (where the distal ulna is shorter than the distal radius) is classically associated with Kienböck's disease. This anatomic variant leads to increased shear forces and abnormal load transmission across the radiolunate joint, predisposing the lunate to microtrauma, vascular compromise, and subsequent osteonecrosis. Joint leveling procedures, such as a radial shortening osteotomy, are often utilized in early stages to unload the lunate.
Question 34
A 74-year-old female with a massive, irreparable rotator cuff tear and severe glenohumeral osteoarthritis undergoes a reverse total shoulder arthroplasty (RTSA). Which of the following best describes the primary biomechanical advantage provided by this specific implant design to restore active forward elevation?
Explanation
Correct Answer: Medialization and distalization of the center of rotation
The reverse total shoulder arthroplasty (RTSA), based on the Grammont design principles, fundamentally alters the biomechanics of the shoulder to compensate for a deficient rotator cuff. By placing a glenosphere on the native glenoid and a concave cup on the proximal humerus, the center of rotation is medialized and distalized. Medialization decreases the torque on the glenoid component (reducing loosening risk) and recruits more deltoid muscle fibers for elevation. Distalization tensions the deltoid muscle, significantly increasing its moment arm and allowing it to act as the primary elevator of the arm in the absence of a functioning supraspinatus.
Question 35
A 14-year-old boy presents with a painful, swollen distal femur. Radiographs reveal a destructive metaphyseal lesion with a "sunburst" periosteal reaction. Biopsy confirms high-grade intramedullary osteosarcoma. A germline mutation in which of the following tumor suppressor genes is most classically associated with a hereditary predisposition to this malignancy?
Explanation
Correct Answer: RB1
Osteosarcoma is the most common primary malignant bone tumor in children and adolescents. While most cases are sporadic, there are well-known genetic predispositions. A germline mutation in the RB1 (retinoblastoma) tumor suppressor gene is classically associated with hereditary retinoblastoma, and these patients have a significantly increased risk (up to 500-fold) of developing secondary malignancies, most notably osteosarcoma. Another critical genetic association is the TP53 mutation, seen in Li-Fraumeni syndrome, which also heavily predisposes individuals to osteosarcoma.
Question 36
A 48-year-old male presents with a right-sided foot drop and radiating leg pain. Examination reveals 3/5 strength in ankle dorsiflexion and great toe extension. To clinically differentiate a compressive L5 radiculopathy from a common peroneal nerve palsy, the examiner should test the strength of which of the following movements?
Explanation
Correct Answer: Ankle inversion
Differentiating an L5 radiculopathy from a common peroneal nerve palsy is a classic clinical challenge, as both conditions cause foot drop (weakness in ankle dorsiflexion and great toe extension). The key to differentiating them lies in testing muscles innervated by the L5 nerve root that travel via a different peripheral nerve. Ankle inversion is primarily controlled by the tibialis posterior muscle, which is innervated by the tibial nerve (L4, L5). In an L5 radiculopathy, ankle inversion will be weak. In a common peroneal nerve palsy, the tibial nerve is unaffected, so ankle inversion strength will be preserved. Ankle eversion (peroneus longus/brevis) is innervated by the superficial peroneal nerve and would be weak in both conditions.
Question 37
A 24-year-old male sustains a displaced fracture of the proximal pole of the scaphoid. He is counseled regarding the high risk of avascular necrosis and nonunion. The unique vulnerability of the proximal pole is primarily due to the scaphoid's intraosseous blood supply, which classically follows which of the following patterns?
Explanation
Correct Answer: Enters the dorsal ridge distally and flows retrogradely
The scaphoid has a tenuous and unique blood supply that predisposes it to avascular necrosis (AVN) and nonunion, particularly following proximal pole fractures. The primary blood supply (70-80%) comes from the dorsal carpal branch of the radial artery, which enters the scaphoid at the dorsal ridge near the waist and distal pole. From there, the intraosseous blood flow is retrograde (distal to proximal) to supply the proximal pole. A fracture at the waist or proximal pole disrupts this retrograde flow, leaving the proximal fragment ischemic.
Question 38
A 45-year-old male sustains an acute Achilles tendon rupture while playing tennis. The rupture occurred in the classic "watershed" region of the tendon, which is known to have a precarious blood supply. Approximately how far proximal to the calcaneal insertion is this hypovascular zone located?
Explanation
Correct Answer: 2 to 6 cm
The Achilles tendon is the largest and strongest tendon in the body, but it is highly susceptible to rupture, most commonly occurring in a specific hypovascular zone. This "watershed" area is located approximately 2 to 6 cm proximal to the tendon's insertion on the calcaneus. The blood supply to the tendon comes from the musculotendinous junction proximally and the osseotendinous junction distally, leaving this mid-substance region relatively ischemic and prone to degenerative changes and subsequent acute rupture during eccentric loading.
Question 39
A 40-year-old male sustains a high-energy bicondylar tibial plateau fracture. Preoperative computed tomography (CT) reveals a large, displaced posteromedial coronal shear fragment. To achieve direct visualization and apply a buttress plate to this specific fragment, which of the following surgical approaches is most appropriate?
Explanation
Correct Answer: Posteromedial approach
Bicondylar tibial plateau fractures often involve a posteromedial coronal shear fragment (Moore Type I). This fragment cannot be adequately reduced or stabilized via a standard anterolateral approach. A dedicated posteromedial approach is required. This approach typically utilizes the interval between the medial head of the gastrocnemius (which is retracted laterally) and the pes anserinus tendons (which are retracted medially or anteriorly). This allows for direct visualization of the posteromedial cortex and the application of an anti-glide or buttress plate to counteract the deforming shear forces.
Question 40
A 12-year-old male basketball player presents with anterior knee pain that worsens with jumping and running. Physical examination reveals point tenderness localized strictly to the inferior pole of the patella, with no tenderness at the tibial tubercle. Radiographs demonstrate fragmentation and sclerosis at the inferior patellar pole. What is the most likely diagnosis?
Explanation
Correct Answer: Sinding-Larsen-Johansson syndrome
Sinding-Larsen-Johansson (SLJ) syndrome is an osteochondrosis or traction apophysitis occurring at the inferior pole of the patella, where the proximal patellar tendon originates. It is common in active adolescents aged 10-14 years and presents with activity-related anterior knee pain and localized tenderness at the inferior patellar pole. Radiographs often show fragmentation or calcification at this site. It is clinically distinct from Osgood-Schlatter disease, which is a similar traction apophysitis but occurs distally at the insertion of the patellar tendon on the tibial tubercle.
Question 41
A 72-year-old female sustains a displaced femoral neck fracture after a mechanical fall. The surgeon opts for a hemiarthroplasty rather than internal fixation due to the high risk of avascular necrosis. The primary blood supply to the femoral head, which is disrupted in this injury, is a direct branch of which of the following arteries?
Explanation
Correct Answer: A (Profunda femoris artery)
The primary blood supply to the adult femoral head is derived from the medial circumflex femoral artery (MCFA), specifically its lateral epiphyseal branch. The MCFA is typically a direct branch of the profunda femoris artery (deep artery of the thigh), although anatomical variants exist where it branches directly from the common femoral artery. Displaced femoral neck fractures disrupt this critical extracapsular arterial ring and the ascending cervical branches, leading to a high rate of avascular necrosis (AVN) and nonunion, which is why arthroplasty is often preferred in the elderly population. The obturator artery provides the artery of the ligamentum teres, which supplies a negligible amount of blood to the adult femoral head.
Question 42
A 13-year-old obese male presents with a 3-week history of left knee pain and a limp. On physical examination, as the left hip is passively flexed, it obligatorily rotates externally. Radiographs confirm a slipped capital femoral epiphysis (SCFE). Which of the following best describes the biomechanical failure and anatomical zone involved in this condition?
Explanation
Correct Answer: B (Failure through the hypertrophic zone of the physis due to shear stress)
Slipped capital femoral epiphysis (SCFE) is characterized by the displacement of the proximal femoral epiphysis relative to the metaphysis. Biomechanically, this occurs due to excessive shear stress across the physis, often exacerbated by obesity and the relatively vertical orientation of the physis during the adolescent growth spurt. Histologically, the mechanical failure occurs specifically through the hypertrophic zone of the physis. This zone lacks the structural integrity of the adjacent zones because the chondrocytes are enlarged and the extracellular matrix is relatively sparse, making it the weakest link under shear loading.
Question 43
A 24-year-old male is struck by a motor vehicle, sustaining a highly comminuted fracture of the proximal fibula. He subsequently develops a foot drop and numbness over the dorsum of his foot. Which of the following muscles will most likely demonstrate normal strength on physical examination?
Explanation
Correct Answer: D (Tibialis posterior)
The patient has sustained an injury to the common peroneal nerve, which wraps around the fibular neck and is highly susceptible to injury in proximal fibula fractures. The common peroneal nerve bifurcates into the deep and superficial peroneal nerves. The deep peroneal nerve innervates the anterior compartment of the leg (tibialis anterior, extensor hallucis longus, extensor digitorum longus), responsible for ankle dorsiflexion. The superficial peroneal nerve innervates the lateral compartment (peroneus longus and brevis), responsible for ankle eversion. The tibialis posterior is located in the deep posterior compartment of the leg and is innervated by the tibial nerve. Therefore, its function (plantarflexion and inversion) will remain intact.
Question 44
A 5-year-old boy falls from monkey bars and presents with a grossly deformed elbow. The hand is pale and pulseless, but capillary refill is 2 seconds. Radiographs show a Gartland type III extension-type supracondylar humerus fracture. The patient is taken emergently to the operating room. After closed reduction and percutaneous pinning, the hand remains pink and warm with brisk capillary refill, but the radial pulse is still not palpable. What is the most appropriate next step in management?
Explanation
Correct Answer: C (Observation and admission for close neurovascular monitoring)
The management of a "pink, pulseless" hand following the reduction of a pediatric supracondylar humerus fracture is a classic board scenario. The initial absence of a pulse is often due to kinking, spasm, or tethering of the brachial artery over the proximal fracture fragment. If, after anatomical reduction and stabilization, the hand becomes well-perfused (pink, warm, capillary refill < 2 seconds) but the pulse remains impalpable, the standard of care is close observation. The collateral circulation around the pediatric elbow is robust enough to maintain viability. Immediate vascular exploration is indicated only for a "white, pulseless" hand that does not improve after reduction.
Question 45
A 68-year-old male presents with increasing pain and stiffness in his right knee, 14 months after a primary total knee arthroplasty. Inflammatory markers are elevated, and a joint aspiration yields a synovial fluid white blood cell count of 45,000 cells/μL with 90% neutrophils. Cultures grow a coagulase-negative Staphylococcus. Which of the following characteristics of this organism is the primary reason for its virulence in prosthetic joint infections?
Explanation
Correct Answer: B (Ability to form a polysaccharide glycocalyx biofilm)
Coagulase-negative staphylococci, such as Staphylococcus epidermidis, are the most common pathogens in delayed prosthetic joint infections (PJIs). Their primary virulence factor is the ability to adhere to polymer and metal surfaces and produce a thick polysaccharide glycocalyx, forming a biofilm. This biofilm protects the bacteria from the host's immune system (e.g., phagocytosis) and significantly decreases the penetration and efficacy of systemic antibiotics. This is why definitive treatment of chronic PJIs typically requires surgical removal of the hardware (e.g., two-stage exchange arthroplasty) rather than antibiotics alone.
Question 46
A 72-year-old female undergoes a reverse total shoulder arthroplasty (RTSA) for severe rotator cuff tear arthropathy. By reversing the normal anatomical concavity and convexity of the glenohumeral joint, this implant alters the biomechanics of the shoulder. Which of the following best describes the primary biomechanical advantage of this prosthesis?
Explanation
Correct Answer: B (It medializes and distalizes the center of rotation, increasing the moment arm of the deltoid)
The reverse total shoulder arthroplasty (RTSA) was designed by Paul Grammont specifically for patients with a deficient rotator cuff. By placing a convex glenosphere on the native glenoid and a concave cup on the proximal humerus, the center of rotation of the shoulder joint is medialized and distalized. This biomechanical shift significantly increases the moment arm of the deltoid muscle and recruits more of its anterior and posterior fibers to assist in elevation. Consequently, the deltoid can compensate for the absent supraspinatus, allowing the patient to actively elevate the arm.
Question 47
A 35-year-old manual laborer presents with chronic, progressive dorsal wrist pain and decreased grip strength. Radiographs reveal sclerosis and fragmentation of the lunate, consistent with Kienböck's disease. Which of the following anatomical variants is most strongly associated with the development of this condition?
Explanation
Correct Answer: B (Negative ulnar variance)
Kienböck's disease is avascular necrosis of the lunate. While the exact etiology is multifactorial (involving vascular anatomy and trauma), it is strongly associated with negative ulnar variance. Negative ulnar variance occurs when the distal ulna is shorter than the distal radius. This anatomical configuration alters the biomechanics of the wrist, leading to increased shear stress and load transmission directly across the radiolunate joint. Over time, this repetitive microtrauma can compromise the tenuous blood supply to the lunate, precipitating osteonecrosis. Joint leveling procedures (e.g., radial shortening osteotomy) are often performed to unload the lunate in early stages of the disease.
Question 48
A 45-year-old male presents with severe lower back pain radiating down the lateral aspect of his left leg to the dorsum of his foot. MRI reveals a large paracentral disc extrusion at the L4-L5 level. Physical examination is most likely to reveal weakness in which of the following actions, and a diminished reflex in which tendon?
Explanation
Correct Answer: B (Weakness in great toe extension; normal reflexes)
In the lumbar spine, a paracentral disc herniation typically impinges on the traversing nerve root. Therefore, an L4-L5 paracentral herniation will compress the L5 nerve root. The L5 nerve root provides motor innervation primarily to the extensor hallucis longus (EHL), responsible for great toe extension, and the tibialis anterior (ankle dorsiflexion). Sensory loss would be noted over the first dorsal web space. Unlike the L4 root (patellar reflex) and the S1 root (Achilles reflex), there is no reliable primary deep tendon reflex associated with the L5 nerve root; thus, reflexes typically remain normal.
Question 49
A 38-year-old male is admitted after sustaining a high-energy Schatzker type VI tibial plateau fracture. Twelve hours post-injury, he complains of severe, unrelenting leg pain that is out of proportion to the injury and not relieved by intravenous opioids. Passive stretch of the toes elicits excruciating pain. If compartment pressures are measured, which of the following thresholds is most widely accepted as an absolute indication for emergent four-compartment fasciotomy?
Explanation
Correct Answer: C (Delta pressure (Diastolic blood pressure - Compartment pressure) < 30 mmHg)
Acute compartment syndrome is a surgical emergency characterized by increased pressure within a closed fascial space, compromising tissue perfusion. While absolute compartment pressures were historically used (e.g., > 30 mmHg), the "delta pressure" is now recognized as a much more accurate and reliable indicator, as it accounts for the patient's systemic perfusion pressure. A delta pressure (Diastolic Blood Pressure minus Compartment Pressure) of less than 30 mmHg is the widely accepted threshold that indicates inadequate capillary perfusion, necessitating emergent fasciotomy to prevent irreversible muscle and nerve necrosis.
Question 50
A 9-year-old African American boy with homozygous sickle cell disease (HbSS) presents with a 4-day history of fever, chills, and severe pain in his right thigh. Blood cultures and a subperiosteal aspirate grow a non-lactose fermenting, Gram-negative motile bacillus that produces hydrogen sulfide. Which of the following pathophysiological mechanisms best explains this patient's unique susceptibility to this specific organism?
Explanation
Correct Answer: A (Impaired splenic macrophage function and reticuloendothelial blockade)
The organism described is Salmonella species, which is uniquely a common cause of osteomyelitis in patients with sickle cell disease (though S. aureus remains the most common overall). Patients with sickle cell disease experience recurrent vaso-occlusive crises, leading to microinfarctions of the spleen and eventual autosplenectomy by early childhood. This loss of splenic function severely impairs the reticuloendothelial system's ability to clear encapsulated organisms and intravascular bacteria. Furthermore, microinfarctions in the bowel wall allow Salmonella to translocate into the bloodstream, where the defective splenic macrophages fail to clear the bacteremia, allowing the bacteria to seed areas of ischemic bone.
You Might Also Like