Surgical Correction of First Metatarsal Malunion
Key Takeaway
First metatarsal malunion frequently presents with transfer metatarsalgia, altered forefoot biomechanics, and multiplanar deformities. Successful surgical correction demands a meticulous understanding of the first metatarsal's vascular supply to prevent avascular necrosis. This guide details the step-by-step execution of corrective osteotomies, including the 'broomstick' technique, emphasizing precise anatomical alignment, rigid internal fixation, and strategic postoperative rehabilitation to restore optimal weight-bearing distribution and functional range of motion.
Comprehensive Introduction and Patho-Epidemiology
The first ray is a highly complex, dynamic biomechanical unit responsible for bearing approximately one-third of the body's weight during the stance phase of gait. Surgical interventions for hallux valgus and other first ray pathologies, such as proximal or distal chevron osteotomies, Scarf osteotomies, and basilar closing wedge osteotomies, carry an inherent and well-documented risk of complications, including nonunion, delayed union, and malunion. Malunion of the first metatarsal is a particularly devastating complication that typically presents as a rigid, multiplanar deformity. The most common manifestations involve dorsal elevation (dorsiflexion malunion), excessive iatrogenic shortening, residual varus or valgus angulation, or a combination of these pathological states.
These anatomical alterations fundamentally disrupt the normal weight-transfer mechanism of the forefoot. Iatrogenic elevation or excessive shortening of the first metatarsal head effectively offloads the first ray, transferring pathological ground reaction forces laterally to the lesser metatarsals. This biomechanical failure inevitably results in transfer metatarsalgia, the development of intractable plantar keratoses (IPKs) beneath the second and third metatarsal heads, and severe, debilitating forefoot pain. The patho-epidemiology of this condition suggests that while the overall incidence of malunion following primary hallux valgus surgery is relatively low (ranging from 1% to 5% depending on the specific procedure and surgeon volume), the functional impairment it causes is disproportionately high.
Corrective surgery for a first metatarsal malunion is technically demanding and requires a profound understanding of forefoot biomechanics, meticulous preoperative planning, and strict adherence to vascular safe zones. The surgeon must navigate compromised soft tissue envelopes, altered bony architecture, and the presence of prior hardware. The primary goal of reconstruction is not merely radiographic realignment, but the restoration of the first ray's weight-bearing capacity to alleviate lateral column overload. Failure to respect the tenuous vascularity of the previously operated first metatarsal can lead to the catastrophic complication of avascular necrosis (AVN) of the metatarsal head, which often necessitates salvage procedures such as first metatarsophalangeal (MTP) joint arthrodesis.
Furthermore, the chronicity of the malunion plays a significant role in the pathophysiology of the surrounding soft tissues. Long-standing dorsal elevation leads to contracture of the dorsal capsuloligamentous structures and attenuation of the plantar plate and flexor apparatus. Consequently, purely osseous correction is rarely sufficient; the reconstructive surgeon must be prepared to perform concomitant soft tissue releases or augmentations to restore dynamic stability to the first MTP joint. Understanding this interplay between altered bone morphology and soft tissue adaptation is the cornerstone of successful revision forefoot surgery.
Detailed Surgical Anatomy and Biomechanics
The biomechanical integrity of the human foot relies heavily on the "windlass mechanism" originally described by Hicks. As the hallux dorsiflexes during the terminal stance phase of gait, the plantar fascia is wound around the first metatarsal head, elevating the medial longitudinal arch, plantarflexing the first metatarsal, and locking the midtarsal joints to create a rigid lever for propulsion. A dorsiflexion malunion or significant shortening of the first metatarsal directly sabotages this mechanism. The shortened or elevated first ray cannot engage the ground appropriately, preventing the necessary tensioning of the plantar fascia and resulting in a functionally incompetent medial column.
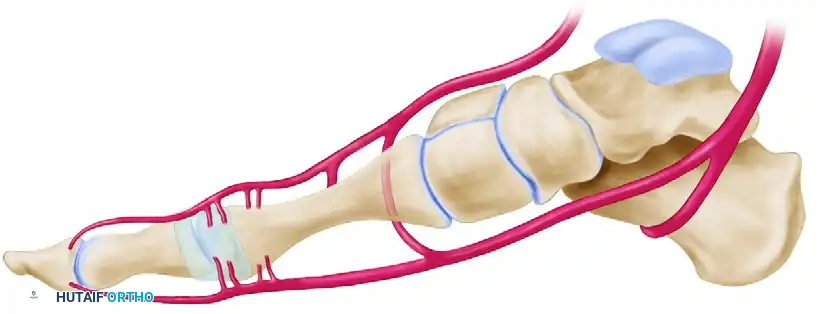
The vascular supply to the first metatarsal head is delicate, highly complex, and exceptionally susceptible to iatrogenic injury during corrective osteotomies and capsular releases. A thorough comprehension of the extraosseous and intraosseous arterial networks is mandatory for any reconstructive foot and ankle surgeon. The primary blood supply to the first metatarsal head is derived from the first dorsal metatarsal artery (FDMA), the first plantar metatarsal artery (FPMA), and the superficial branch of the medial plantar artery. These vessels give rise to a rich network of pericapsular perforators that enter the metatarsal head distally. The principal nutrient artery, conversely, enters the lateral aspect of the metatarsal shaft proximally, supplying the medullary canal.
The site of a cortical osteotomy must remain strictly within the interval between the pericapsular perforators distally and the nutrient artery proximally. Violation of this safe zone significantly increases the risk of osteonecrosis. The surgeon must conceptualize this safe zone in three dimensions, recognizing that prior surgical dissection may have already compromised a portion of this collateral network.
From a dorsal perspective, the relationship between the osteotomy site, the nutrient artery, and the distal pericapsular perforators becomes highly apparent. The first dorsal metatarsal artery and its branching network are especially vulnerable to overpenetration of the lateral cortex by an oscillating saw during the osteotomy cut. Surgeons must exercise extreme caution when breaching the lateral cortex, utilizing a retractor or a controlled drill-hole technique to protect these vital dorsal and lateral structures.
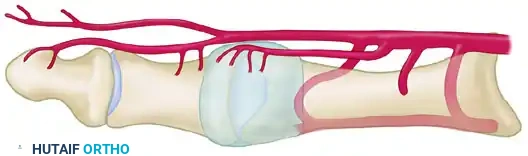
When a lateral capsular release is indicated to correct residual deformity or contracture, it must be executed with absolute precision. The safe zone for a lateral capsular release spares all perforators entering the metatarsal head proximally and all perforators entering the proximal phalanx distally. This is achieved as long as the capsulotomy is performed strictly in line with the metatarsophalangeal (MTP) joint in the coronal plane. Deviating proximally into the metatarsal neck region during a lateral release is a well-documented cause of iatrogenic AVN.

Exhaustive Indications and Contraindications
The decision to proceed with surgical correction of a first metatarsal malunion must be based on a comprehensive evaluation of the patient's symptoms, functional demands, and the failure of exhaustive conservative management. The primary indication for surgery is persistent, debilitating pain that limits activities of daily living. This pain is most frequently localized not just to the first MTP joint, but to the lesser metatarsal heads due to transfer lesions. Patients will often present with thick, painful calluses beneath the second and third metatarsal heads, and an antalgic gait characterized by lateral weight shifting.
Conservative management must be attempted and documented prior to surgical intervention. This includes the use of custom-molded orthoses with a first ray cut-out to allow the first metatarsal to plantarflex, combined with a metatarsal pad placed proximal to the lesser metatarsal heads to offload the transfer lesions. Rocker-bottom shoe modifications, wide toe-box footwear, and activity modification are also essential first-line treatments. Only when these modalities fail to provide adequate relief, and the patient's quality of life remains significantly impaired, should surgical reconstruction be entertained.
Contraindications to surgical correction are both systemic and local. Absolute contraindications include active deep infection, severe peripheral arterial disease (e.g., Ankle-Brachial Index < 0.5 or non-palpable pulses without adequate collateral flow on Doppler), and active Charcot neuroarthropathy. Relative contraindications include poorly controlled diabetes mellitus (HbA1c > 8.0%), heavy tobacco use (which exponentially increases the risk of nonunion and wound breakdown), and profound osteoporosis, which may preclude adequate hardware fixation. Furthermore, patient compliance is paramount; a patient who cannot adhere to a strict non-weight-bearing protocol postoperatively is a poor candidate for complex osteotomy reconstruction.
| Clinical Parameter | Indication for Surgery | Relative Contraindication | Absolute Contraindication |
|---|---|---|---|
| Pain Profile | Refractory transfer metatarsalgia | Mild, intermittent pain | Asymptomatic radiographic malunion |
| Vascular Status | Intact pulses, ABI > 0.9 | ABI 0.5 - 0.9, microvascular disease | ABI < 0.5, active ischemic rest pain |
| Soft Tissue | Healed, pliable surgical scars | Thin, atrophic skin, prior dehiscence | Active ulceration, cellulitis, osteomyelitis |
| Bone Quality | Normal trabecular density | Moderate osteopenia | Severe osteoporosis precluding fixation |
| Patient Factors | Compliant, realistic expectations | Smoker (unwilling to quit), obesity | Non-compliant, severe psychiatric illness |
Pre-Operative Planning, Templating, and Patient Positioning
Patients presenting with a suspected malunion require a highly structured and comprehensive clinical and radiographic evaluation. Clinical assessment begins with a detailed gait analysis. The surgeon must observe for an antalgic gait, avoidance of first ray loading during the terminal stance phase, and a compensatory lateral weight shift. The plantar aspect of the foot must be thoroughly inspected for hyperkeratotic lesions beneath the lesser metatarsal heads, which are the hallmark physical finding of a functionally shortened or elevated first ray. Range of motion (ROM) of the first MTP joint must be assessed for stiffness, crepitus, and pain, differentiating between intra-articular pathology (such as concurrent degenerative joint disease) and extra-articular capsular contracture.
Standard weight-bearing radiographs are non-negotiable and form the foundation of preoperative planning. An Anteroposterior (AP) view is utilized to evaluate the intermetatarsal angle, the hallux valgus/varus angle, and the relative metatarsal lengths. The Lateral view is critical for assessing sagittal plane alignment; dorsal elevation of the first metatarsal head is frequently identified by measuring the first metatarsal declination angle or Meary's angle. The Sesamoid Axial view is indispensable for determining the position of the sesamoid apparatus relative to the crista, identifying subluxation, joint space narrowing, or arthritic changes that might dictate an arthrodesis rather than a joint-sparing osteotomy. In cases of complex, multiplanar deformities, a weight-bearing Cone-Beam CT (CBCT) scan is highly recommended to accurately map the Center of Rotation of Angulation (CORA) and assess bone stock.
Preoperative templating is mandatory to determine the exact location, angle, and type of corrective osteotomy required. The surgeon must calculate the required degree of plantarflexion, lengthening, and transverse plane correction. If distraction osteogenesis is planned, the exact length of the required regenerate bone must be calculated by comparing the malunited first metatarsal to the contralateral normal foot, or by utilizing standard metatarsal parabola templates. Hardware selection—whether utilizing locking plates, intramedullary devices, or external fixators—should be finalized during this templating phase, with backup options readily available in the operating room.
Patient positioning is critical for optimal surgical execution. The patient is placed supine on a radiolucent operating table to allow for unencumbered intraoperative fluoroscopy. A small bump is placed under the ipsilateral hip to internally rotate the leg, bringing the foot into a neutral, vertical position. A pneumatic thigh tourniquet is typically utilized to maintain a bloodless surgical field, though it should be deflated prior to final closure to ensure adequate perfusion of the capital fragment and soft tissue flaps. Prophylactic intravenous antibiotics are administered 30 minutes prior to inflation of the tourniquet.
Step-by-Step Surgical Approach and Fixation Technique
The "Broomstick" Osteotomy
The "broomstick" osteotomy is a highly versatile, multiplanar corrective technique designed specifically to address complex malunions of the first metatarsal. By utilizing a meticulously drilled semicircular arc rather than a straight saw cut, the surgeon can rotate and translate the capital fragment in multiple planes simultaneously, while minimizing further bone loss and functional shortening.
- Exposure and Preparation: Utilize a dorsal or dorsomedial longitudinal incision, carefully incorporating or excising the previous surgical scar to prevent narrow skin bridges. Perform a meticulous dissection, strictly preserving the dorsal sensory nerves (medial dorsal cutaneous nerve) and the critical vascular structures outlined previously. Expose the malunion site subperiosteally, but critically limit the stripping of the capital fragment to the absolute minimum required for the osteotomy. Aggressive distal stripping is a primary cause of postoperative AVN.
- The Unicortical Drill Arc: Utilize a 2-mm drill bit (or a 1.5-mm K-wire on a wire driver to minimize thermal necrosis and bone loss). Create a precise semicircle of unicortical holes extending from the dorsal cortex to the plantar cortex. This arc should be positioned adjacent to, or directly within, the previous osteotomy site, encompassing an arc of approximately 150 degrees. The use of multiple small drill holes rather than an immediate saw cut prevents the saw blade from skiving, significantly reduces thermal osteonecrosis, and preserves maximal bone stock.
- Osteotome Connection: Connect the unicortical drill holes using only the corner of a 5-mm or 6-mm sharp, straight, thin osteotome. Use the osteotome strictly as a cutting edge to break the cortical bridges between the drill holes. Crucial Step: Do not penetrate the lateral cortex with the osteotome at this stage. Premature penetration can lead to uncontrolled propagation of the fracture line into the diaphysis or the articular surface, compromising the entire reconstruction.
- Completion of the Osteotomy: Return to the 2-mm drill bit. Make numerous holes in the lateral cortex by passing the drill through the newly created unicortical osteotomized semicircle. Complete the osteotomy using a thin (4 mm wide) blade on a small power oscillating saw. This staged, drill-assisted technique significantly reduces the amount of shortening compared to a standard freehand saw cut.
- Multiplanar Deformity Correction:
- Sagittal Plane (Elevation): Manually rotate the metatarsal head plantarward until the dorsal cortex of the capital (distal) fragment is positioned inferior (plantar) to the dorsal cortex of the shaft (proximal) fragment. This maneuver slightly plantarflexes the first metatarsal head, restoring its ability to assume the appropriate weight-bearing load.
- Coronal/Transverse Plane (Varus/Valgus): If the capital fragment has healed in varus or valgus, reverse the deformity until the capital fragment is reduced to normal anatomical alignment with the shaft.
- The "broomstick" configuration allows the capital fragment to pivot smoothly like a ball-and-socket, enabling simultaneous correction of all planes of deformity without the need for complex closing or opening wedges.
- Internal Fixation: Once anatomical alignment is achieved and temporarily held with reduction forceps or provisional K-wires, definitive internal fixation is applied. Modern fixation typically involves low-profile, titanium locking plates contoured to the new dorsal or medial anatomy. Alternatively, multiple small fragment cortical screws (e.g., 2.0 mm or 2.4 mm) can be utilized if the bone stock is robust. Interfragmentary wires are technically difficult to utilize in this confined location but are not strictly contraindicated if rigid compression can be achieved.
Distraction Osteogenesis for Severe Shortening
When the first metatarsal is excessively shortened (typically >8-10 mm) and simple plantarflexion cannot restore the weight-bearing parabola, distraction osteogenesis is indicated. This technique utilizes a unilateral, single-plane external fixator. Following a low-energy corticotomy utilizing a multiple drill-hole and osteotome technique (to preserve the endosteal blood supply), the fixator is applied. After a latency period of 7 to 10 days to allow for early callus formation, gradual distraction is applied at a rate of 1 mm per day in divided increments (0.25 mm every 6 hours) until the anatomical length of the first metatarsal is restored. Once length is achieved, the fixator is locked, and the bone is allowed to consolidate, a phase that can take several months.
Lesser Metatarsal Osteotomies (Weil Procedures)
In cases where lengthening the first metatarsal is contraindicated or technically unfeasible, the surgeon may elect to perform shortening osteotomies of the lesser metatarsals to restore the metatarsal parabola. The Weil osteotomy—an intra-articular, oblique shortening osteotomy of the metatarsal neck—is the standard procedure. While technically straightforward and associated with reliable bone healing due to the large cancellous surface area, it carries significant risks, including the dreaded "floating-toe" deformity caused by intrinsic muscle imbalance, persistent metatarsalgia, and marked overall forefoot shortening.
Complications, Incidence Rates, and Salvage Management
The surgical correction of a first metatarsal malunion is fraught with potential complications, even in the hands of experienced foot and ankle surgeons. The most devastating complication is avascular necrosis (AVN) of the first metatarsal head. The incidence of AVN is highly variable, ranging from 0% to upwards of 75% in historical literature, heavily dependent on the degree of soft tissue stripping and violation of the vascular safe zones. Early AVN may be managed conservatively with prolonged offloading, but advanced collapse with secondary degenerative joint disease inevitably requires a first MTP joint arthrodesis.
Nonunion or delayed union of the corrective osteotomy is another significant concern, particularly given the often-sclerotic nature of the malunited bone and the compromised local vascularity. The incidence of nonunion ranges from 2% to 10%. Management of an aseptic nonunion requires revision surgery with rigid internal fixation, meticulous debridement of the nonunion site, and the application of autologous bone graft (e.g., from the proximal tibia or calcaneus) or orthobiologics to stimulate osteogenesis.
Iatrogenic hallux varus is a distressing complication often resulting from over-resection of the medial eminence, excessive lateral capsular release, or over-tightening of the medial capsule during the index bunionectomy. It presents with medial deviation of the great toe, intrinsic minus deformity, and subluxation of the sesamoid apparatus.

Correction of a rigid or long-standing hallux varus often requires a salvage procedure if soft tissue reconstruction (e.g., extensor hallucis brevis transfer or split extensor hallucis longus transfer) is no longer viable due to joint contracture or advanced arthrosis. In older, lower-demand patients, a Keller resection arthroplasty or a first MTP joint arthrodesis may be indicated to restore a plantigrade, braceable foot and eliminate pain.

| Complication | Estimated Incidence | Primary Pathophysiology | Salvage / Management Strategy |
|---|---|---|---|
| Avascular Necrosis (AVN) | 2% - 15% | Violation of vascular safe zones, excessive stripping | NWB if early; 1st MTP Arthrodesis if collapsed |
| Nonunion / Delayed Union | 2% - 10% | Inadequate fixation, thermal necrosis, smoking | Revision ORIF with autologous bone grafting |
| Recurrent Transfer Metatarsalgia | 10% - 20% | Inadequate plantarflexion of 1st MT during correction | Custom orthotics; Weil osteotomies of lesser rays |
| Iatrogenic Hallux Varus | 1% - 5% | Over-resection of medial eminence, lateral overtightening | Soft tissue transfer; Arthrodesis; Keller arthroplasty |
| Hardware Prominence / Pain | 5% - 15% | Thin dorsal soft tissue envelope | Hardware removal after radiographic consolidation |
Phased Post-Operative Rehabilitation Protocols
The postoperative protocol following the correction of a first metatarsal malunion must be meticulously tailored to the rigidity of the internal fixation, the patient's body habitus, bone quality, and anticipated compliance. A generic, one-size-fits-all approach is inappropriate and risks catastrophic failure of the reconstruction.
Phase 1: Immediate Postoperative Period (Weeks 0-2)
The primary goals during this phase are wound healing, edema control, and protection of the osteotomy site. The patient is typically placed in a well-padded, short-leg splint in the operating room. Strict elevation of the operative extremity above the level of the heart is mandatory for the first 72 to 96 hours to minimize swelling and prevent wound dehiscence. The patient must remain strictly non-weight-bearing (NWB) utilizing crutches, a knee scooter, or a walker. At the 10-to-14-day mark, the patient returns to the clinic for suture removal and initial postoperative radiographs to confirm the maintenance of alignment.
Phase 2: Intermediate Protection Phase (Weeks 2-6)
Depending on the stability of the construct and the bone quality assessed intraoperatively, the patient is transitioned into either a short-leg fiberglass cast or a rigid controlled ankle motion (CAM) boot. In cases of tenuous fixation, poor bone stock, or extensive multiplanar correction (such as a large structural bone graft), strict NWB status must be maintained. If a highly rigid locking plate construct was achieved in healthy bone, the surgeon may permit touchdown or heel-touch weight-bearing in the CAM boot. Active range of motion of the ankle and lesser toes is encouraged to prevent stiffness, but the first MTP joint is generally protected from aggressive manipulation during this early healing phase.
Phase 3: Consolidation and Early Mobilization (Weeks 6-12)
At 6 to 8 weeks postoperatively, repeat radiographs are obtained to assess for trabecular bridging across the osteotomy site. Full, unprotected weight-bearing in standard footwear is only permitted when union of the osteotomy is apparent both clinically (absence of pain on palpation and loading) and radiographically (bridging trabeculae across three out of four cortices). Once clinical union is achieved, aggressive physical therapy focusing on first MTP joint dorsiflexion and plantarflexion must commence. Manual therapy, scar mobilization, and intrinsic foot muscle strengthening are critical to restoring the windlass mechanism.
Phase 4: Long-Term Rehabilitation (Weeks 12+)
Patients must be explicitly counseled that the final range of motion and maximal medical improvement are often not reached until 12 to 18 months postoperatively. Soft tissue remodeling, resolution of deep postoperative edema, and the return of normal gait mechanics are gradual processes. The patient must be informed prior to surgery that permanent loss of some metatarsophalangeal joint motion is highly probable due to capsular scarring and altered joint mechanics from the initial surgery and the revision. However, they should be reassured that overall foot function, the resolution of transfer metatarsalgia, and overall pain levels should be significantly improved.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of first metatarsal malunions is guided by several foundational principles established in landmark orthopedic literature. The concept of the windlass mechanism, originally detailed by Hicks in 1954, remains the biomechanical cornerstone for understanding why first ray malunions fail and cause lateral column overload. Restoring the ability of the first metatarsal to plantarflex and engage the ground during terminal stance is the primary objective of any reconstructive effort.
The vascular anatomy of the first metatarsal, thoroughly mapped by Shereff et al., dictates the surgical safe zones utilized today. Their cadaveric studies definitively demonstrated the vulnerability of the dorsal and lateral intraosseous blood supply, leading to the modern consensus that aggressive soft tissue stripping and poorly placed lateral capsular releases are the primary drivers of iatrogenic avascular necrosis.
Regarding surgical techniques, the utilization of distraction osteogenesis for severe first metatarsal shortening was popularized by Hurst and Nunley. Their work demonstrated that while technically demanding and requiring prolonged external fixation, gradual distraction restores the anatomical length and the metatarsal parabola without sacrificing the native anatomy of the lesser rays. For multiplanar deformities without severe shortening, the "broomstick" or dome-shaped osteotomies have been championed in the literature for their ability to provide infinite centers of rotation, allowing for simultaneous correction in the sagittal, coronal, and transverse planes without the inherent shortening associated with traditional closing wedge osteotomies.
Clinical guidelines emphasize a stepwise approach to management: exhaustive conservative care must precede surgical intervention. When surgery is indicated, the surgeon must meticulously plan the correction using CORA principles, respect the compromised vascular envelope, and choose a fixation construct robust enough to withstand the immense ground reaction forces experienced by the first ray during gait. Salvage procedures, such as first MTP arthrodesis, remain a highly reliable fallback and should be openly discussed with the patient as a potential primary or secondary option in cases of severe joint arthrosis or bone loss.
