High-Energy Schatzker Type VI Tibial Plateau Fracture: A Case Study with Neurovascular Compromise
Key Takeaway
A Schatzker Type VI tibial plateau fracture from high-energy trauma presents with gross deformity, severe pain, and critical neurovascular deficits like peroneal nerve palsy and diminished ABI. X-rays and CT scans with 3D reconstructions are crucial to confirm complex bicondylar comminution, articular depression, and metaphyseal-diaphyseal dissociation, guiding urgent orthopedic management.
Patient Presentation and History
A 35-year-old male presented to the emergency department following a high-energy motor vehicle collision (MVC). He was the unrestrained driver involved in a head-on collision at approximately 50 mph, experiencing direct impact to the lateral aspect of his left knee against the dashboard. Paramedics reported significant deformity and ecchymosis of the left knee at the scene.
On arrival, the patient reported immediate, severe, excruciating pain in his left knee, rendering him unable to bear any weight. He denied loss of consciousness but reported transient numbness and paresthesia in his left foot and ankle immediately after the impact, which had partially resolved. There were no other overt injuries reported in the primary survey by the trauma team, though secondary survey was ongoing.
AMPLE History:
* Allergies: No known drug allergies (NKDA).
* Medications: None.
* Past Medical/Surgical History: Healthy, no prior surgeries, no chronic medical conditions.
* Last Meal: Approximately 3 hours prior to injury.
* Events: Detailed as above.
Social History: Non-smoker, occasional alcohol use. Employed as a construction worker, indicating a high functional demand.
Biomechanics of the Injury Mechanism
The mechanism of injury in this presentation—a high-energy dashboard impact—is classic for complex proximal tibia trauma. The biomechanical forces involved typically combine a massive axial load with a varus or valgus bending moment, depending on the exact position of the limb at the time of impact. In an unrestrained driver, the knee is often flexed at approximately 90 degrees. Upon collision, the kinetic energy is transferred directly through the patellofemoral joint and into the tibial plateau.
The lateral condyle of the tibia is morphologically convex and structurally weaker than the larger, concave medial condyle. Consequently, an axial load combined with a valgus moment frequently results in depression and cleavage of the lateral plateau. However, in high-energy scenarios exceeding the structural threshold of the proximal tibial metaphysis, the energy propagates transversely and distally, resulting in metaphyseal-diaphyseal dissociation—the hallmark of a Schatzker Type VI fracture. The reported transient neurological symptoms and high-energy mechanism immediately elevate the index of suspicion for profound structural and neurovascular disruption.
Clinical Examination Findings
Upon focused orthopedic examination after primary and secondary surveys by the trauma team, the following was noted:
General: Patient was alert, oriented, and hemodynamically stable. Pain localized to the left knee.
Left Lower Extremity:
* Inspection: Gross deformity of the left knee, with significant swelling and ecchymosis extending from the distal thigh to the proximal calf. There was a large, tense effusion. Skin integrity was compromised with a large, non-blanchable blister developing laterally over the tibial plateau, approximately 3x2 cm, and impending fracture blisters around the anterolateral aspect. No open wounds were noted initially. The limb appeared subtly shortened and in slight valgus angulation.
* Palpation: Markedly tender globally around the knee joint, particularly over the lateral and medial tibial condyles. Palpable crepitus was elicited with gentle manipulation. The patella was ballotable, confirming a significant hemarthrosis. Distal pulses (dorsalis pedis and posterior tibial) were present but faintly palpable compared to the contralateral limb; capillary refill was sluggish at 3-4 seconds. Compartments of the lower leg felt firm but not tense on initial examination.
* Range of Motion (ROM): Actively and passively severely limited due to pain and guarding. Estimated active ROM was 0-10 degrees of flexion. Attempts at passive ROM were met with extreme pain.
* Neurological Assessment:
* Peroneal Nerve: Weakness in ankle dorsiflexion (grade 3/5) and great toe extension (grade 3/5). Sensory deficit noted in the first web space and dorsum of the foot. This represented a concerning partial peroneal nerve palsy.
* Tibial Nerve: Intact motor function (plantarflexion grade 5/5) and sensation in the sole of the foot.
* Femoral Nerve: Intact motor and sensory function.
* Vascular Assessment: Distal pulses were weak. Ankle-Brachial Index (ABI) was performed bilaterally. Left ABI was 0.82, right ABI was 1.0. The diminished ABI raised significant concern for a popliteal artery injury, despite palpable pulses.
* Ligamentous Stability: Due to extreme pain, guarding, and gross swelling, a comprehensive assessment of ligamentous stability was deferred. However, gross instability was noted with gentle varus stress in extension, suggesting significant lateral collateral ligament (LCL) or posterolateral corner (PLC) involvement, or severe bone loss.
* Associated Injuries: No obvious hip or ankle injuries detected on clinical examination. Spine was stable to palpation.
Given the high-energy mechanism, gross deformity, significant soft tissue compromise, neurological deficit, and concerning vascular compromise, an emergent multidisciplinary approach was immediately initiated.
Advanced Soft Tissue and Compartment Evaluation
The soft tissue envelope in the proximal tibia is notoriously unforgiving. The anteromedial surface of the tibia is subcutaneous, providing minimal muscular coverage to absorb traumatic forces or support wound healing following surgical incisions. In this patient, the presence of a non-blanchable, blood-filled fracture blister laterally signifies a Tscherne Grade III closed soft tissue injury. This indicates extensive muscle contusion, severe skin damage, and subcutaneous degloving (a localized Morel-Lavallée lesion).
Furthermore, the firm compartments of the lower leg necessitate hyper-vigilance for acute compartment syndrome (ACS). The proximal tibia fractures, particularly high-energy bicondylar variants, are highly associated with ACS due to massive hematoma formation within the tight fascial compartments of the calf. While the compartments were "firm but not tense" initially, the presence of a partial peroneal nerve palsy complicates the clinical picture. Ischemic neuropathy from elevated anterior or lateral compartment pressures can mimic a direct traumatic stretch injury to the common peroneal nerve at the fibular neck. Serial clinical examinations every two hours, and potentially continuous intra-compartmental pressure monitoring using a slit-catheter or Stryker needle technique, are mandatory. A delta pressure (Diastolic Blood Pressure minus Compartment Pressure) of less than 30 mmHg would dictate emergent four-compartment fasciotomies.
Neurovascular Anatomy and Pathology
The diminished ABI of 0.82 is a critical finding. The popliteal artery is rigidly tethered proximally at the adductor hiatus and distally at the soleal arch. As it traverses the popliteal fossa, it lies in direct proximity to the posterior capsule of the knee joint and the proximal posterior tibia. In high-energy bicondylar fractures, particularly those with a significant posteromedial shear fragment or posterior translation of the tibial shaft, the popliteal artery is at extreme risk for intimal tearing, thrombosis, or complete transection. The trifurcation (anterior tibial artery, posterior tibial artery, and peroneal artery) is equally vulnerable. The anterior tibial artery, as it passes anteriorly through the proximal interosseous membrane, is frequently compromised in severe proximal tibia fractures.
The common peroneal nerve courses around the fibular neck, making it highly susceptible to traction injuries during severe varus or valgus deforming forces, or direct contusion from lateral impact. The grade 3/5 weakness in the extensor hallucis longus (EHL) and tibialis anterior, combined with sensory blunting in the deep peroneal nerve distribution (first web space), suggests an axonotmesis or neurapraxia.
Imaging and Diagnostics
To delineate the complex osseous architecture and address the suspected vascular compromise, a comprehensive imaging protocol was executed.
Radiographic and Tomographic Evaluation
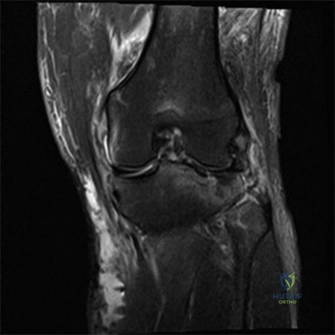
Standard trauma radiographs, including Anteroposterior (AP), Lateral, and bilateral oblique views of the left knee, were obtained. The AP radiograph demonstrated a severe bicondylar tibial plateau fracture with significant depression of the lateral articular surface and a vertical split extending through the medial condyle. Crucially, the fracture lines extended distally into the tibial diaphysis, completely separating the articular block from the shaft—confirming a Schatzker Type VI pattern. The lateral view revealed posterior subluxation of the tibial plateau relative to the femoral condyles, a highly unstable configuration.
Given the complexity of the fracture and the necessity for precise preoperative templating, a non-contrast Computed Tomography (CT) scan of the knee with 2D multiplanar reconstructions (sagittal and coronal) and 3D surface rendering was performed.
The CT scan is the gold standard for evaluating tibial plateau fractures. It allows for the precise mapping of articular comminution, the depth of joint depression, and the orientation of major fracture fragments. In this case, the CT scan revealed:
1. A severely comminuted and depressed lateral plateau, with the central articular segment impacted 18 mm distally into the metaphyseal cancellous bone.
2. A large, displaced posteromedial fragment. This fragment is critical; it represents the primary restraint to posterior subluxation of the knee and must be anatomically reduced and buttressed to prevent late varus collapse.
3. Extensive metaphyseal comminution with a "blow-out" of the lateral cortex.
4. Complete metaphyseal-diaphyseal dissociation with a 15-degree valgus and 10-degree apex anterior angulation.
Computed Tomography Angiography
Due to the abnormal ABI (0.82) and the high-energy mechanism, a CT Angiogram (CTA) of the left lower extremity with bilateral runoff was emergently obtained. The CTA is highly sensitive and specific for detecting arterial injuries such as intimal flaps, pseudoaneurysms, and occlusions.
The CTA revealed an intimal flap in the distal popliteal artery, just proximal to the trifurcation, causing a non-flow-limiting stenosis (approximately 40% narrowing). Distal runoff to the foot was preserved via the posterior tibial and peroneal arteries, though the anterior tibial artery showed focal vasospasm as it traversed the interosseous membrane. Vascular surgery was immediately consulted. Given the preservation of distal flow and the absence of an expanding hematoma or complete occlusion, the consensus was for close observation, avoidance of systemic anticoagulation due to the risk of compartment syndrome and surgical bleeding, and emergent stabilization of the fracture to prevent further vascular intimal damage from mobile osseous fragments.
Differential Diagnosis
In the context of high-energy knee trauma presenting with gross instability and neurovascular compromise, the differential diagnosis must encompass severe fracture patterns and catastrophic soft tissue disruptions. The following table outlines the primary differential diagnoses considered during the initial evaluation.
| Differential Diagnosis | Key Clinical Features | Radiographic and Advanced Imaging Findings | Management Implications |
|---|---|---|---|
| Schatzker Type VI Tibial Plateau Fracture | Severe pain, gross deformity, metaphyseal-diaphyseal dissociation, high risk of compartment syndrome and neurovascular injury. | Bicondylar fracture lines extending into the diaphysis. Complete separation of the articular block from the tibial shaft. | Requires staged management (Damage Control Orthopedics). Temporizing spanning external fixation followed by definitive dual-plate ORIF. |
| Knee Dislocation (KD) with Periarticular Fracture | Extreme multidirectional instability, "dimple sign" (irreducible posterolateral dislocation), very high incidence of popliteal artery complete transection. | Asymmetric joint spaces, frank tibiofemoral dislocation (often spontaneously reduced prior to imaging), avulsion fractures (e.g., Segond fracture, fibular head avulsion). | True surgical emergency if vascularly compromised. Requires immediate reduction, potential vascular bypass, and spanning external fixation. Ligamentous reconstruction is staged months later. |
| Distal Femur Fracture (AO/OTA 33-C3) | Swelling proximal to the joint line, shortened and externally rotated limb, palpable distal femoral fragments in the suprapatellar pouch. | Intra-articular fracture of the distal femur with metaphyseal comminution. Often shows a "Hoffer's" coronal plane fracture (Hoffa fragment). | Requires surgical fixation, typically with a lateral locking plate or retrograde intramedullary nail. High risk of stiffness and post-traumatic arthrosis. |
| Proximal Tibia Fracture-Dislocation (Moore Classification) | Severe subluxation of the tibia relative to the femur, often with massive ligamentous avulsions rather than purely articular depression. | Coronal split fractures, entire condyle avulsions, or rim avulsions indicating massive capsuloligamentous failure. | High risk of popliteal artery tethering. Requires careful reduction and often necessitates simultaneous bony fixation and acute ligamentous repair/reconstruction. |
Surgical Decision Making and Classification
The fracture was classified as a Schatzker Type VI, AO/OTA 41-C3.3, and a Tscherne Grade III closed soft tissue injury.
Damage Control Orthopedics versus Early Total Care
The paradigm of treatment for high-energy tibial plateau fractures has evolved significantly. Historically, Early Total Care (ETC)—involving immediate open reduction and internal fixation (ORIF) through extensive exposures—was attempted. This approach yielded disastrous complication rates, including deep infection, wound dehiscence, and amputation rates approaching 20-80% in the presence of severe soft tissue injury.
Consequently, the modern standard of care for a Schatzker VI fracture with a Tscherne III soft tissue envelope is Damage Control Orthopedics (DCO). DCO operates on the principle of staging the definitive intervention to allow the local soft tissue envelope to recover and the systemic inflammatory response syndrome (SIRS) to abate. The initial "first hit" of the trauma primes the patient's immune system; a prolonged, massive definitive surgery immediately upon presentation acts as a "second hit," potentially precipitating acute respiratory distress syndrome (ARDS), multiple organ dysfunction syndrome (MODS), and catastrophic local wound failure.
The surgical plan was formulated as a two-stage approach:
1. Stage One: Emergent application of a knee-spanning external fixator. This achieves immediate restoration of mechanical axis length, alignment, and rotation (restoring the "tube"). Crucially, it stabilizes the osseous fragments, mitigating ongoing trauma to the popliteal artery intimal flap, reducing pain, and allowing for aggressive elevation and soft tissue resuscitation.
2. Stage Two: Definitive ORIF, to be performed 10 to 21 days post-injury, contingent upon the resolution of soft tissue swelling, the re-epithelialization of fracture blisters, and the appearance of the "wrinkle sign" (return of normal skin turgor).
Non-operative management was entirely contraindicated given the intra-articular step-off, metaphyseal-diaphyseal dissociation, and neurovascular risk.
Surgical Technique and Intervention
Stage One Temporizing External Fixation
The patient was taken emergently to the operating room. General anesthesia was induced, and the patient was positioned supine on a radiolucent Jackson table. A thorough examination under anesthesia (EUA) confirmed gross multidirectional instability of the knee.
A modular, joint-spanning external fixator was applied. The strategic placement of pins is paramount; they must be positioned outside the anticipated zones of future definitive surgical incisions (anterolateral and posteromedial approaches).
Two 5.0 mm half-pins were placed in the anterior distal femur, approximately 15 cm proximal to the joint line, taking care to remain strictly in the sagittal plane to avoid tethering the vastus lateralis or medialis, which could impede future knee flexion. Two 5.0 mm half-pins were placed in the anterior tibial diaphysis, distal to the fracture zone.
Under fluoroscopic guidance, longitudinal traction was applied to restore limb length and correct the metaphyseal-diaphyseal dissociation. A slight varus force was applied to correct the valgus deformity, and the external fixator bars were tightened. Fluoroscopy confirmed restoration of the mechanical axis and distraction of the joint space, which relies on ligamentotaxis to partially reduce the major articular fragments. The pin sites were dressed with chlorhexidine-impregnated sponges. Post-application, the distal pulses remained palpable, and the ABI was re-checked, improving slightly to 0.88, suggesting that restoring length relieved some kinking of the popliteal artery.
Soft Tissue Resuscitation Phase
Over the next 14 days, the patient remained admitted. The limb was strictly elevated above the level of the heart. The fracture blisters were left intact to serve as a sterile biologic dressing; as they evolved, they were carefully unroofed and treated with silver sulfadiazine cream. Deep vein thrombosis (DVT) prophylaxis was initiated with low-molecular-weight heparin (LMWH) 24 hours post-external fixation, balancing the risk of DVT against the risk of compartment syndrome. The partial peroneal nerve palsy remained stable, with no progression of motor weakness, and serial compartment checks remained negative for ACS.
By day 14, the swelling had subsided significantly, the fracture blisters had epithelialized, and a positive "wrinkle sign" was present. The patient was cleared for definitive Stage Two ORIF.
Stage Two Definitive Open Reduction and Internal Fixation
The definitive reconstruction of a Schatzker VI fracture requires meticulous preoperative planning. The goal is anatomic reduction of the articular surface, restoration of the mechanical axis, and stable internal fixation allowing for early range of motion, all while respecting the precarious soft tissue envelope.
Positioning and Preparation
The patient was positioned supine on a radiolucent flat top table. A bump was placed under the ipsilateral hip to internally rotate the leg to a neutral position. A sterile tourniquet was applied to the proximal thigh but not inflated, held in reserve for catastrophic bleeding, as tourniquet ischemia can exacerbate soft tissue compromise. The external fixator was prepped into the sterile field and subsequently removed.
Surgical Approaches
A dual-incision technique was utilized to address both the medial and lateral columns independently, avoiding the disastrous soft tissue stripping associated with a single extensile anterior approach.
- Posteromedial Approach: The medial column must be addressed first. The posteromedial fragment is the keystone of the knee; if left unreduced, the femur will subluxate posteriorly and into varus. An 8 cm longitudinal incision was made along the posteromedial border of the proximal tibia. The saphenous nerve and vein were identified and protected anteriorly. The interval between the medial head of the gastrocnemius (retracted posteriorly) and the pes anserinus (retracted anteriorly) was developed. The popliteus muscle was partially elevated off the posterior tibia to expose the fracture apex.
- Anterolateral Approach: An S-shaped incision was made, starting proximal to Gerdy's tubercle, extending distally along the anterior crest of the tibialis anterior muscle. Full-thickness fasciocutaneous flaps were elevated. A submeniscal arthrotomy was performed; the coronary ligament was incised, and the lateral meniscus was elevated and tagged with non-absorbable sutures to expose the depressed articular surface.
Reduction and Fixation Sequence
The posteromedial fragment was reduced directly using a ball-spiked pusher and pointed reduction forceps. Anatomic reduction was confirmed fluoroscopically and by direct palpation of the posterior cortical read. A 3.5 mm pre-contoured posteromedial buttress plate was applied in an anti-glide fashion to neutralize the vertical shear forces.
Attention was then turned to the lateral side. The lateral metaphyseal wall was opened like a book to access the depressed central articular fragments. Using bone tamps, the articular surface was carefully elevated to match the contour of the medial plateau and the femoral condyles. The resulting massive metaphyseal void was filled with a structural calcium phosphate bone cement and cancellous allograft to support the elevated cartilage and prevent subsidence.
The lateral wall was closed, and a 3.5 mm proximal tibia lateral anatomic locking plate was applied. The plate was slid submuscularly down the diaphysis. Proximal fixation was achieved with multiple raft screws placed directly subchondrally to support the articular elevation. Distal fixation to the diaphysis was achieved with a combination of locking and non-locking cortical screws, restoring the metaphyseal-diaphyseal continuity.
Closure
The meniscal coronary ligament was repaired using the previously placed tagging sutures. The iliotibial band and anterior tibial fascia were closed meticulously. Subcutaneous tissues and skin were closed with minimal tension. Due to the high risk of wound breakdown, an incisional Negative Pressure Wound Therapy (iNPWT) dressing was applied over the anterolateral incision at -125 mmHg to reduce edema and promote perfusion.
Post Operative Protocol and Rehabilitation
The postoperative rehabilitation following a complex bicondylar tibial plateau fracture is prolonged and requires a delicate balance between protecting the fixation and preventing joint stiffness.
Phased Recovery and Weight Bearing Progression
Phase I: Immediate Postoperative (Weeks 0-2)
* Weight Bearing: Strict Non-Weight Bearing (NWB) on the operative extremity.
* Immobilization: The knee is placed in a hinged knee brace locked in full extension to protect the soft tissues and prevent flexion contractures.
* Range of Motion: Passive Range of Motion (PROM) is initiated immediately via a Continuous Passive Motion (CPM) machine, starting at 0-30 degrees and advancing 10 degrees daily as tolerated. Early ROM is critical for cartilage nutrition and preventing intra-articular adhesions.
* Medical Management: Continuation of DVT prophylaxis (e.g., Apixaban or Enoxaparin) for a minimum of 28 days. Strict elevation.
Phase II: Early Rehabilitation (Weeks 2-6)
* Wound Care: Sutures removed at 2-3 weeks. iNPWT discontinued.
* Weight Bearing: Continued strict NWB. The articular cartilage and structural bone graft require a minimum of 8-12 weeks to consolidate sufficiently to withstand axial loading.
* Range of Motion: Progression to Active-Assisted Range of Motion (AAROM). Goal is to achieve 0-90 degrees of flexion by week 6.
* Strengthening: Isometric quadriceps sets, straight leg raises (in brace), and patellar mobilizations are emphasized.
Phase III: Intermediate Rehabilitation (Weeks 6-12)
* Weight Bearing: Radiographic evaluation at 6-8 weeks to assess bridging callus and maintenance of articular reduction. If satisfactory, initiate Touch-Down Weight Bearing (TDWB) with crutches.
* Range of Motion: Goal is full ROM (0-120+ degrees).
* Strengthening: Introduction of closed kinetic chain exercises (e.g., stationary bicycle with low resistance) once cleared for partial weight bearing.
Phase IV: Advanced Rehabilitation (Months 3-6+)
* Weight Bearing: Progressive transition to Full Weight Bearing (FWB) by 10-12 weeks, guided by clinical and radiographic healing.
* Strengthening: Aggressive lower extremity strengthening, proprioceptive training, and gait mechanics normalization.
* Return to Work: For a construction worker, return to heavy manual labor may take 6 to 9 months, and permanent restrictions (e.g., kneeling, heavy carrying) may be required depending on the degree of residual post-traumatic arthrosis.
Clinical Pearls and Pitfalls
The management of Schatzker Type VI fractures is fraught with potential complications. Mastery of these injuries requires adherence to several critical surgical and clinical principles.
Strategic Considerations for Bicondylar Fractures
Pearls:
* Respect the Soft Tissue Envelope: The timing of definitive surgery is dictated entirely by the soft tissues, not the bone. Operating through fracture blisters or massive edema guarantees wound dehiscence and deep infection. The "wrinkle sign" is your most reliable indicator for surgical readiness.
* The Posteromedial Fragment is the Keystone: Always address the medial/posteromedial column first. Anatomic reduction of this fragment restores the medial cortical read
