Navigating Bicondylar Tibial Plateau Fractures: A Surgical Guide
Key Takeaway
This article provides essential research regarding Navigating Bicondylar Tibial Plateau Fractures: A Surgical Guide. A bicondylar tibial plateau fracture involves both the medial and lateral tibia plateaus. These are classified as Schatzker type V or type VI fractures. Type V affects both condyles without complete dissociation from the shaft, often treated with buttress plates. Type VI involves complete dissociation of the articular segment from the shaft, typically requiring lateral locked or dual plating.
Comprehensive Introduction and Patho-Epidemiology
Bicondylar tibial plateau fractures represent a complex and challenging subset of periarticular lower extremity trauma that tests the limits of orthopedic surgical acumen. These injuries involve both the medial and lateral tibial plateaus, fundamentally disrupting the articular surface, the meniscofemoral ligamentous restraints, and the metadiaphyseal structural integrity of the proximal tibia. In the classic Schatzker classification system, type V and type VI fractures are both considered bicondylar fractures, though they present with distinct morphologic, biomechanical, and prognostic characteristics that dictate entirely different surgical strategies. The management of these injuries requires not only a mastery of osseous fixation but also a profound respect for the precarious soft tissue envelope surrounding the knee joint.
Schatzker type V fractures involve both the medial and lateral condyles without complete dissociation from the underlying tibial diaphysis. These fracture patterns maintain a central pillar of intact metaphyseal bone connecting the intercondylar eminence and articular segment to the shaft. This intact central pillar provides a critical biomechanical foundation, rendering these fractures typically amenable to medial and lateral buttress plate fixation without the profound diaphyseal instability seen in higher-grade injuries. The mechanism of injury often involves a purely axial load with symmetric impaction, leading to a "split-depression" morphology on both sides of the joint while sparing the central metaphysis.

Conversely, Schatzker type VI fractures involve both condyles with complete dissociation of the articular segment from the underlying diaphysis. This metaphyseal-diaphyseal dissociation creates profound instability, as the entire articular block is detached from the tibial shaft, effectively creating a floating knee joint equivalent at the proximal tibia. These highly unstable fractures are typically treated with robust lateral locked plates or dual (lateral and medial) plating constructs to restore the mechanical axis and provide absolute stability to the articular block. The energy required to produce a Schatzker VI fracture is significantly higher, often resulting in severe comminution, profound soft tissue stripping, and a high incidence of acute compartment syndrome.

From an epidemiological standpoint, bicondylar tibial plateau fractures exhibit a classic bimodal distribution. High-energy mechanisms, such as motor vehicle collisions, motorcycle accidents, or falls from significant heights, typically affect younger patients (often males in their third or fourth decades) and are associated with severe soft tissue compromise, diaphyseal extension, and concomitant systemic injuries (polytrauma). Conversely, low-energy mechanisms, such as falls from a standing height, can produce complex bicondylar fracture patterns in elderly patients with osteoporotic bone. In these geriatric cohorts, the bone often fails before the ligaments, leading to severe central articular depression and metaphyseal crushing that complicates screw purchase and construct stability.
Lateral fractures with associated posteromedial fragments should be distinguished from other standard bicondylar types. These specific variants, often captured more accurately by Luo’s three-column classification system, require posteromedial fixation independent from lateral fixation and may be representative of a high-energy fracture-dislocation variant. The Orthopaedic Trauma Association (OTA) and Arbeitsgemeinschaft für Osteosynthesefragen (AO) classification system further categorizes these as 41C fractures. A 41C1 denotes a simple articular and simple metaphyseal fracture; 41C2 indicates a simple articular with a multifragmentary metaphyseal component; and 41C3 represents a multifragmentary articular and multifragmentary metaphyseal fracture. The 41C3 pattern is particularly notorious for its high complication rate, demanding meticulous preoperative planning and execution. The energy imparted during the traumatic event dictates not only the osseous comminution but also the degree of soft tissue envelope destruction, which is often the primary determining factor in the timing and modality of definitive surgical intervention.

Detailed Surgical Anatomy and Biomechanics
A profound understanding of proximal tibial anatomy and knee biomechanics is required to execute precise articular reduction and stable internal fixation. The proximal tibia is characterized by an intricate interplay of osseous morphology, ligamentous restraints, and meniscal load-sharing structures, all of which must be respected and restored to achieve an optimal functional outcome.
Osseous Architecture and Alignment
In the loaded knee, the medial plateau bears approximately 60% to 75% of the physiological load during the normal gait cycle. To accommodate this asymmetric force distribution, the medial plateau is larger, more robust, and morphologically distinct from the lateral plateau. Morphologically, the medial plateau is concave, acting as a stable congruent dish for the medial femoral condyle, whereas the lateral plateau is convex, allowing for the physiologic roll-back mechanism of the knee during flexion. Furthermore, stronger, denser subchondral bone is found on the medial side due to this increased load-bearing requirement. The lateral plateau is anatomically positioned higher than the medial plateau, a critical detail when assessing joint line restoration on intraoperative fluoroscopy.

Restoration of normal lower extremity alignment relies on recreating the native angular relationships of the proximal tibia. The medial proximal tibial angle (MPTA) is 87 degrees relative to the anatomic axis of the tibia (range 85 to 90 degrees). Restoring the MPTA is paramount; failure to do so results in varus or valgus malalignment, which exponentially increases contact stresses in the overloaded compartment and accelerates post-traumatic osteoarthritis. In the sagittal plane, the proximal posterior tibial angle (PPTA) is 81 degrees relative to the anatomic axis of the tibia (range 77 to 84 degrees), representing the native posterior slope of the tibial plateau. Failure to restore this posterior slope can lead to altered knee kinematics, specifically affecting the tensioning of the cruciate ligaments. An iatrogenically increased posterior slope places undue stress on the anterior cruciate ligament (ACL), while a decreased (or reversed) slope stresses the posterior cruciate ligament (PCL).
The metaphyseal flare of the proximal tibia presents unique biomechanical challenges for plate osteosynthesis. The bone transitions from dense cortical diaphyseal bone to thin cortical bone surrounding cancellous metaphyseal bone. In bicondylar fractures, this cancellous bone is often severely impacted, creating massive osseous voids once the articular surface is elevated. These voids must be meticulously filled with structural bone graft or synthetic bone substitutes to provide a mechanical scaffold that prevents secondary subsidence of the articular fragments during the early postoperative rehabilitation phase.
Ligamentous and Meniscal Structures
The soft tissue envelope and ligamentous attachments of the proximal tibia are vital for maintaining knee stability and guiding surgical approaches. The menisci are critical load-sharing and shock-absorbing structures, transmitting up to 50% of the compressive load in extension and up to 85% in 90 degrees of flexion. The medial meniscus is C-shaped and firmly attached to the joint capsule and deep medial collateral ligament, making it less mobile and more prone to tearing during rotational trauma. The lateral meniscus is more circular, covers a larger percentage of the lateral articular surface, and is highly mobile. Preservation of the menisci, particularly the peripheral attachments and root insertions, is paramount during surgical exposure (e.g., via submeniscal arthrotomy) to prevent accelerated post-traumatic osteoarthritis.

The ligamentous anatomy includes the medial collateral ligament (MCL), which originates on the medial femoral epicondyle and inserts broadly on the proximal medial tibia. The lateral collateral ligament (LCL) inserts on the fibular head, alongside the biceps femoris tendon, forming the conjoined tendon. The cruciate ligaments reside within the intercondylar notch; the ACL inserts on the anterior intercondylar area of the tibia, while the PCL inserts on the posterior tibial sulcus. In high-energy bicondylar fractures, avulsion fractures of the cruciate ligament insertions (tibial spine fractures) or frank ligamentous ruptures are common concomitant injuries. The "unhappy triad" equivalent in plateau fractures often involves a lateral plateau depression, an MCL avulsion, and a meniscal tear. These soft tissue lesions must be addressed either acutely during the index procedure or in a staged fashion once osseous stability is achieved.
Furthermore, the iliotibial (IT) band inserts on Gerdy's tubercle on the anterolateral tibia. This robust fascial structure must often be incised or elevated during anterolateral surgical approaches. Careful repair of the IT band and the anterior tibialis fascia is crucial to prevent muscle herniation and restore the lateral tension band effect of the knee. The pes anserinus (conjoined tendons of the sartorius, gracilis, and semitendinosus) inserts on the proximal medial tibia and serves as a critical landmark during posteromedial surgical approaches, often requiring gentle retraction to access the posteromedial osseous column.
Neurovascular Proximity and Risk
The neurovascular anatomy surrounding the proximal tibia dictates the safe zones for surgical dissection, retractor placement, and percutaneous wire or screw placement. The popliteal artery lies directly posterior to the knee capsule, separated from the posterior tibial cortex by only a thin layer of popliteus muscle. As it traverses distally, it passes under the tendinous arch of the soleus muscle and bifurcates into the anterior tibial artery and the tibioperoneal trunk.

The anterior tibial artery passes anteriorly through the proximal interosseous membrane. This anatomical tethering makes the vessel highly susceptible to injury during high-energy proximal tibial fractures, particularly those with significant posterior displacement, shear components, or severe comminution. Ankle-brachial indices (ABIs) and meticulous vascular exams are mandatory in all high-energy bicondylar fractures to rule out occult intimal tears or arterial transections. Any ABI less than 0.9 mandates further investigation with a CT angiogram.
Furthermore, the common peroneal nerve wraps around the fibular neck from posterior to anterior, dividing into the deep and superficial peroneal nerves. This places the nerve at significant risk during posterolateral surgical approaches, fibular head osteotomies, or percutaneous wire insertion in the proximal lateral quadrant. Retractors placed over the posterior aspect of the lateral plateau must be positioned with extreme caution to avoid traction neuropraxia. Iatrogenic peroneal nerve injury results in foot drop, a devastating complication that drastically impairs patient mobility and functional recovery.

Exhaustive Indications and Contraindications
The management of bicondylar tibial plateau fractures is dictated by a complex algorithm encompassing patient-specific factors, fracture morphology, bone quality, and, most importantly, the condition of the surrounding soft tissue envelope. The primary goals of intervention are to restore articular congruity, re-establish the mechanical axis of the lower extremity, ensure joint stability, and allow for early range of motion to nourish the articular cartilage and prevent arthrofibrosis.
Operative and Non-Operative Decision Making
Non-operative management of bicondylar tibial plateau fractures is exceedingly rare in modern orthopedic trauma practice. It is generally reserved for patients who are non-ambulatory at baseline, possess severe medical comorbidities that preclude anesthesia (e.g., recent myocardial infarction, end-stage renal disease with severe coagulopathy), or present with truly non-displaced fracture patterns. It must be noted that a truly non-displaced bicondylar fracture is a biomechanical anomaly; most "non-displaced" patterns on plain films reveal significant occult depression or comminution on CT imaging. In the rare instances where non-operative management is selected, treatment consists of hinged knee bracing, strict non-weight-bearing protocols for 8 to 12 weeks, and serial radiographic surveillance to monitor for secondary displacement or varus collapse.
Operative intervention is the definitive standard of care for the vast majority of Schatzker V and VI fractures. The presence of articular step-off greater than 2 to 3 millimeters, condylar widening exceeding 5 millimeters, varus or valgus malalignment greater than 5 degrees compared to the contralateral limb, and any degree of metaphyseal-diaphyseal instability are absolute indications for surgical fixation. The rationale is clear: articular incongruity leads to altered contact mechanics, focal cartilage overloading, and rapid-onset post-traumatic osteoarthritis. Furthermore, axial malalignment drastically shifts the mechanical axis, creating a vicious cycle of asymmetric loading, hardware failure, and joint destruction.

Soft Tissue Management and Damage Control Orthopedics
The most critical contraindication to immediate definitive internal fixation is a compromised soft tissue envelope. High-energy bicondylar fractures are frequently accompanied by profound soft tissue swelling, fracture blisters (both clear and blood-filled), and impending or frank compartment syndrome. Incising through traumatized, edematous tissue to place bulky metallic plates is a recipe for catastrophic wound dehiscence and deep periprosthetic joint infection.
In these scenarios, the application of a temporary spanning external fixator—a core tenet of Damage Control Orthopedics (DCO)—is the indicated initial procedure. A delta-frame or standard anterior frame spanning the knee joint provides skeletal traction, restores length, reduces capsular tension, and immobilizes the fracture fragments, allowing the soft tissues to resuscitate. Definitive Open Reduction and Internal Fixation (ORIF) is delayed until the soft tissue envelope has adequately recovered, characterized by the resolution of edema, epithelialization of fracture blisters, and the return of normal skin turgor (the "wrinkle sign"). This delay typically ranges from 10 to 21 days. Open fractures and fractures associated with acute compartment syndrome require emergent surgical intervention for irrigation, debridement, and four-compartment fasciotomies, invariably followed by spanning external fixation.

Summary of Indications and Contraindications
| Clinical Scenario | Management Strategy | Rationale and Considerations |
|---|---|---|
| Non-Displaced Fracture | Non-Operative | Exceedingly rare; requires rigid immobilization and serial imaging to ensure no delayed displacement occurs. High risk of secondary collapse. |
| Non-Ambulatory Patient | Non-Operative | Surgical risks (infection, DVT, anesthesia) outweigh functional benefits; focus on pain control and maintaining baseline joint mobility. |
| Articular Step-Off > 2mm | Operative (ORIF) | Restoration of articular congruity is required to minimize the risk of rapid-onset post-traumatic osteoarthritis and restore meniscal function. |
| Condylar Widening > 5mm | Operative (ORIF) | Widening alters meniscal tensioning and joint mechanics, leading to gross coronal instability and cartilage degradation. |
| Mechanical Axis Deviation | Operative (ORIF) | Varus or valgus malalignment drastically shifts load-bearing forces, causing accelerated wear on the overloaded compartment and hardware failure. |
| Open Fractures | Emergent Operative | Immediate irrigation, debridement, and stabilization (via spanning external fixation) to prevent deep infection and osteomyelitis. |
| Compartment Syndrome | Emergent Operative | Emergent four-compartment fasciotomies combined with skeletal stabilization to prevent irreversible ischemic muscle necrosis and nerve death. |
| Severe Soft Tissue Injury | Staged Operative (DCO) | Temporary spanning external fixation until the "wrinkle sign" appears (typically 10-21 days), followed by definitive ORIF to prevent wound necrosis. |
Pre-Operative Planning, Templating, and Patient Positioning
Successful execution of complex bicondylar tibial plateau fracture surgery begins long before the incision is made. Meticulous preoperative planning minimizes intraoperative complications, reduces tourniquet time, limits soft tissue dissection, and optimizes the biomechanical construct of the final fixation. The modern orthopedic surgeon must approach these fractures as a three-dimensional puzzle, requiring advanced imaging and precise tactical mapping.
Advanced Imaging Modalities and Templating
Standard orthogonal radiographs (anteroposterior and lateral) provide the initial assessment of the fracture pattern, overall alignment, and degree of diaphyseal extension. Oblique views can occasionally help delineate specific condylar fragments. However, plain radiography is woefully insufficient for the definitive preoperative planning of bicondylar fractures. The complex overlapping anatomy of the proximal tibia obscures central articular depression and posterior shear fragments.

A high-resolution computed tomography (CT) scan with two-dimensional multiplanar reconstructions (coronal and sagittal) and three-dimensional surface rendering is absolutely mandatory. The CT scan allows the surgeon to map the fracture lines precisely, identify the location and size of articular depression, and recognize specific fragment morphologies. Utilizing Luo’s three-column concept (medial, lateral, and posterior columns), the surgeon can systematically identify which columns are fractured and plan the required surgical approaches. For instance, a posteromedial shear fragment cannot be adequately reduced or stabilized from a standard anterolateral approach; it demands a dedicated posteromedial incision and buttress plating.
Digital templating is the next critical step. Using calibrated CT or radiographic images, the surgeon selects the appropriate plate designs, lengths, and screw trajectories. Templating ensures that raft screws will adequately support the depressed articular segments without penetrating the joint space. It also helps anticipate the volume of bone graft or synthetic void filler required to support the elevated subchondral bone. Anticipating the need for specialized equipment—such as femoral distractors, radiolucent triangles, specific clamp types (e.g., large Weber clamps or Jungbluth clamps), and various biologic adjuncts—is a direct result of comprehensive templating.

Patient Positioning and Operating Room Setup
Patient positioning must facilitate unhindered access to the required surgical approaches while allowing for dynamic intraoperative fluoroscopy. For standard anterolateral and posteromedial approaches, the patient is positioned supine on a fully radiolucent operating table. A bump is placed under the ipsilateral hip to correct natural external rotation, ensuring the patella points directly towards the ceiling. A radiolucent triangle or a sterile bump is placed under the knee to allow for varying degrees of flexion, which relaxes the gastrocnemius muscle and facilitates posterior fragment reduction.
In cases requiring extensive posterior access (e.g., massive posterior shear fractures or complex posterior column comminution), a prone or "floating" position may be utilized. The floating position involves placing the patient in a lateral decubitus orientation, allowing the leg to be rotated internally for posterior access and externally for anterolateral access. Regardless of the position, the C-arm must be positioned on the contralateral side of the table, coming in perpendicular to the limb. The surgeon must confirm that perfect AP and lateral fluoroscopic views of the knee can be obtained effortlessly before prepping and draping. A sterile tourniquet is applied to the proximal thigh, though its use should be minimized to reduce ischemic time and postoperative pain, typically reserved for the critical phases of articular visualization and reduction.

Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of bicondylar tibial plateau fractures is a highly choreographed sequence of exposures, reductions, and fixations. The overarching philosophy is to reconstruct the articular surface anatomically, restore the metaphyseal-diaphyseal relationship, and apply stable internal fixation while respecting the soft tissue biology.
Surgical Approaches: Anterolateral, Posteromedial, and Dual Incisions
The vast majority of bicondylar fractures require a dual-incision technique to address both the medial and lateral columns independently. The anterolateral approach is the workhorse for lateral plateau fractures. The incision is centered over Gerdy's tubercle, extending proximally toward the lateral epicondyle and distally along the anterior crest of the tibia. The iliotibial band is incised, and the anterior tibialis muscle is elevated off the lateral metaphysis. To visualize the articular surface, a submeniscal arthrotomy is performed. The coronary ligaments are incised, allowing the lateral meniscus to be retracted superiorly with stay sutures. This provides direct visualization of the lateral articular depression.
The posteromedial approach is utilized to address medial column and posteromedial shear fragments. The incision is made along the posteromedial border of the proximal tibia, starting at the joint line and extending distally. The saphenous nerve and vein are identified and protected. The deep fascia is incised, and the interval between the medial head of the gastrocnemius (retracted posteriorly) and the pes anserinus (retracted anteriorly) is developed. This provides excellent access to the posteromedial metaphysis. Crucially, the posteromedial approach is an internervous and intermuscular plane that avoids stripping the anterior medial soft tissues, thereby preserving the vascular supply to the medial tibial crest.

Articular Reduction Techniques and Void Management
Reduction typically begins with the medial or posteromedial column. The medial plateau is often a large, non-comminuted fragment that has displaced distally and into varus. Reducing and provisionally fixing the medial fragment to the tibial diaphysis restores the medial cortical read and re-establishes the length and mechanical axis of the tibia. This converts a complex bicondylar fracture into a simpler lateral plateau fracture. Reduction is achieved using large pointed reduction forceps or a femoral distractor placed spanning the knee joint to provide sustained traction and ligamentotaxis.
Once the medial column is provisionally stabilized, attention turns to the lateral articular surface. The lateral plateau often features central depression with a lateral blow-out fragment. The lateral cortex is opened like a book, and the depressed articular segments are elevated from below using bone tamps. Elevation must be performed meticulously, often under direct visualization through the submeniscal arthrotomy and confirmed with fluoroscopy. Once elevated, a massive metaphyseal void is created. This void must be packed tightly with cancellous autograft, allograft, or osteoconductive synthetic cement (e.g., calcium phosphate). Calcium phosphate is particularly advantageous as it provides high initial compressive strength, supporting the articular surface and allowing for earlier mobilization.

Plate Osteosynthesis and Construct Biomechanics
Following articular elevation and void filling, definitive plate osteosynthesis is performed. The medial column is typically stabilized with an under-contoured posteromedial anti-glide or buttress plate. This plate resists the vertical shear forces inherent to the medial plateau during weight-bearing. Because the medial bone is dense, standard non-locking cortical screws are often sufficient to achieve absolute stability.
The lateral column is then stabilized with a pre-contoured periarticular locking plate. The plate is applied to the lateral metaphysis and secured with a combination of non-locking screws (to pull the bone to the plate and restore coronal alignment) and locking screws (to create a fixed-angle construct). A "raft" of subchondral locking screws is placed directly beneath the elevated articular surface. These screws act as a rigid metallic scaffold, preventing secondary subsidence of the articular fragments. In cases of severe Schatzker VI fractures with diaphyseal comminution, the lateral plate must span the comminuted segment, utilizing bridge plating principles to preserve the fracture hematoma and promote secondary bone healing. The combination of a medial buttress plate and a lateral locking plate creates a highly rigid dual-plate construct capable of withstanding physiologic loads.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, bicondylar tibial plateau fractures carry a notoriously high complication rate. The combination of high-energy trauma, tenuous soft tissues, and complex intra-articular mechanics creates a perfect storm for both acute and chronic morbidity.
Infection and Wound Healing Complications
Deep periprosthetic joint infection (PJI) and wound dehiscence are the most feared acute complications, occurring in 5% to 15% of high-energy bicondylar fractures, particularly those associated with open injuries or compartment syndrome. The anterolateral surgical incision is particularly vulnerable due to the thin soft tissue envelope over the proximal tibia. Risk factors include smoking, diabetes, obesity, and premature surgical intervention before soft tissue recovery.
Management of wound necrosis or deep infection requires aggressive and prompt intervention. Superficial dehiscence may be managed with local wound care or negative pressure wound therapy (NPWT). However, deep infections involving the hardware require emergent return to the operating room for radical irrigation and debridement. If the fracture is unhealed and the hardware is stable, the implants are typically retained, and the patient is treated with targeted intravenous antibiotics and potentially local antibiotic beads. Soft tissue defects exposing bone or hardware necessitate rotational flaps (e.g., medial gastrocnemius flap) or free tissue transfer to provide durable coverage. If the hardware is loose or the infection is recalcitrant, the plates must be removed, and stabilization is achieved via a spanning external fixator until the infection is eradicated.

Post-Traumatic Osteoarthritis and Malunion
Post-traumatic osteoarthritis (PTOA) is a frequent long-term complication, occurring in 20% to 40% of patients within 5 to 10 years post-injury. The pathogenesis of PTOA is multifactorial, driven by residual articular incongruity, altered mechanical alignment (varus/valgus malunion), meniscal loss, and the initial chondrocyte apoptosis caused by the traumatic impact itself. Even with an anatomic radiographic reduction, the biologic damage to the cartilage can lead to progressive joint space narrowing and debilitating pain.
Malunion, particularly varus collapse, occurs when the medial column is inadequately fixed or when the patient bears weight prematurely. Varus malalignment drastically increases the contact stresses on the medial compartment, rapidly accelerating cartilage wear. Treatment of symptomatic malunion may require corrective intra-articular or extra-articular osteotomies to realign the mechanical axis and offload the damaged compartment.
Hardware Failure and Salvage Arthroplasty
Hardware failure, such as screw breakage or plate pullout, typically indicates mechanical overload, nonunion, or deep infection. When PTOA becomes end-stage and severely limits the patient's quality of life, salvage Total Knee Arthroplasty (TKA) is indicated. However, post-traumatic TKA is technically demanding and carries higher complication rates than primary TKA for primary osteoarthritis. Challenges include retained hardware (which may require a staged removal), distorted anatomic landmarks, severe bone loss, compromised ligamentous stability, and a scarred, non-compliant soft tissue envelope. Surgeons must often utilize diaphyseal engaging stems, highly constrained polyethylenes (e.g., VVC or hinged designs), and metallic augments to reconstruct the joint successfully.
Summary of Complications
| Complication | Incidence Rate | Primary Etiology | Salvage / Management Strategy |
|---|---|---|---|
| Deep Infection | 5% - 15% | High-energy trauma, premature surgery, poor host factors. | Serial I&D, hardware |
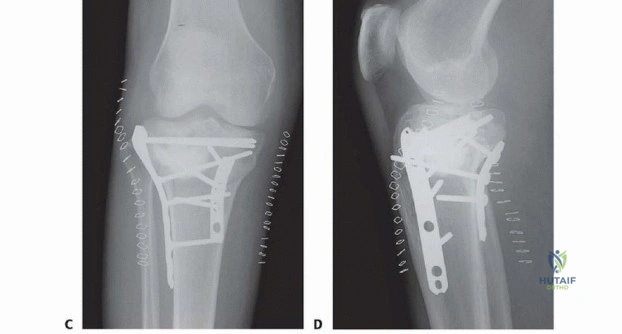
Clinical & Radiographic Imaging Archive

