High-Energy Schatzker Type VI Tibial Plateau Fracture: Clinical Case Study & Diagnostics

Key Takeaway
Diagnosing a high-energy Schatzker Type VI tibial plateau fracture involves detailed clinical assessment, observing presentation, deformity, and neurovascular status. Comprehensive imaging, including X-rays and CT with 3D reconstructions, is vital. These diagnostics accurately characterize articular depression, comminution, and condylar widening, essential for precise classification and surgical planning.
Patient Presentation and History
A 42-year-old male presented to the Level I Trauma Center Emergency Department following a high-energy motor vehicle collision. The patient was the restrained driver of a sedan involved in a high-speed, head-on impact with a stationary object. Extrication time was approximately twenty minutes. The reported mechanism of injury involved a direct impact of the lateral aspect of the left knee and proximal tibia against the dashboard, combined with significant axial loading transmitted through the floorboard.
Upon initial presentation, the patient complained of severe, intractable pain localized to the left knee and proximal leg, accompanied by gross deformity and an absolute inability to bear weight on the affected extremity. The pre-hospital emergency medical services personnel had appropriately applied a rigid long-leg splint with the limb in full extension and administered intravenous fentanyl, which provided minimal analgesic relief.
The initial Advanced Trauma Life Support primary survey revealed a patent airway, bilateral breath sounds, and hemodynamic stability. There was no reported loss of consciousness, and the Glasgow Coma Scale score was 15. The secondary survey identified the left lower extremity injury as the primary site of trauma, with no other immediate life-threatening thoracic, abdominal, or pelvic injuries identified.
The patient’s past medical history was notable only for essential hypertension, which was well-controlled on a daily low-dose angiotensin-converting enzyme inhibitor. He denied any history of smoking, alcohol abuse, or illicit drug use, which is a favorable prognostic indicator for bone healing and soft tissue recovery. His occupation as a heavy manual laborer necessitates a high functional demand, thereby prioritizing a treatment strategy aimed at achieving an anatomic articular reduction and stable mechanical alignment to facilitate a return to demanding physical activities.
The high-energy nature of the mechanism immediately raises the index of suspicion for severe articular comminution, metaphyseal-diaphyseal dissociation, and profound soft tissue envelope compromise, characteristic of complex bicondylar tibial plateau fractures. The combination of axial load and valgus or varus moments dictates the specific fracture pattern, which in this case, presented as a catastrophic failure of both the medial and lateral columns of the proximal tibia.
Clinical Examination Findings
The initial orthopedic assessment prioritized the evaluation of the neurovascular status and the integrity of the soft tissue envelope, followed by a meticulous examination of the osseous structures once the patient was hemodynamically stabilized and appropriately positioned in the trauma bay.
Soft Tissue Inspection
Inspection revealed a gross deformity of the left knee joint characterized by significant global swelling, predominantly localized to the proximal third of the tibia. Extensive ecchymosis was evident circumferentially, with pronounced tracking along the lateral and posterolateral aspects of the leg. The skin overlying the proximal tibia appeared taut and shiny, demonstrating early effacement of the normal skin creases, indicative of substantial underlying edema and hematoma formation.
At the time of initial presentation, no fracture blisters (either clear fluid-filled or blood-filled) were observed; however, the soft tissue envelope was classified as a Tscherne Grade II closed injury, given the severe soft tissue contusion and impending risk of further swelling. A meticulous 360-degree inspection of the limb confirmed the absence of any open wounds, lacerations, or punctate lesions that would necessitate classification as an open fracture. The overall limb alignment demonstrated a clinically apparent valgus deformity combined with slight leg length shortening, secondary to the proximal tibial articular collapse and metaphyseal impaction.
Palpation and Compartment Assessment
Palpation elicited marked circumferential tenderness over the proximal tibia, with maximal points of tenderness corresponding to the medial and lateral joint lines and the tibial tubercle. Gentle manipulation of the limb produced palpable crepitus, definitively confirming gross bony instability. A massive, tense knee effusion was present, highly suggestive of a lipohemarthrosis resulting from the intra-articular fracture and marrow extravasation.
Given the high-energy mechanism and the degree of swelling, a rigorous clinical assessment for acute compartment syndrome was performed. The anterior, lateral, superficial posterior, and deep posterior compartments of the leg were palpated. Initially, the compartments were soft and compressible, lacking the classic "wood-like" tension associated with elevated intracompartmental pressures. Furthermore, passive stretch of the digits (specifically passive plantarflexion of the hallux and toes to assess the anterior compartment, and passive dorsiflexion to assess the deep posterior compartment) did not elicit pain out of proportion to the underlying fracture. Despite these initial reassuring findings, the high risk associated with Schatzker Type VI fractures mandated serial clinical examinations every two hours.
Range of Motion and Stability
Range of motion testing was grossly restricted and deferred due to the severity of the injury. The knee was held in an obligate position of approximately 10 to 15 degrees of flexion to maximize the intra-articular volume and minimize capsular tension. Any attempt at passive range of motion elicited severe guarding and apprehension. Active motion, including a straight leg raise, was impossible due to pain, loss of the extensor mechanism mechanical advantage secondary to the fracture, and gross instability. Varus and valgus stress testing was contraindicated in the acute setting to prevent further soft tissue stripping and neurovascular compromise.
Neurological and Vascular Status
A detailed neurological examination of the distal extremity was conducted to assess for potential traction injuries or direct contusions to the peripheral nerves.
Assessment of the common peroneal nerve revealed mild motor weakness. Dorsiflexion of the ankle (tibialis anterior function, deep peroneal nerve) was graded at 4/5, and eversion of the foot (peroneus longus and brevis function, superficial peroneal nerve) was also graded at 4/5. Sensation in the first dorsal web space (deep peroneal nerve distribution) remained intact. These findings were consistent with a mild neuropraxia, likely secondary to a traction injury over the fibular head during the initial valgus deforming force, rather than a complete nerve transection.
Assessment of the tibial nerve demonstrated full 5/5 motor strength for ankle plantarflexion (gastrocnemius-soleus complex) and foot inversion (tibialis posterior). Sensation over the plantar aspect of the foot was completely intact.
Vascular assessment confirmed the presence of palpable, strong, and symmetric femoral, popliteal, dorsalis pedis, and posterior tibial pulses. Capillary refill time in the digits was brisk, at less than two seconds. There were no audible bruits or palpable thrills. Given the robust clinical vascular examination, an immediate Ankle-Brachial Index measurement or CT angiography was deferred, though the threshold for these modalities remained low if any changes in perfusion were detected. The proximity of the popliteal artery to the posterior cortex of the proximal tibia makes it highly susceptible to injury, particularly in fracture patterns involving posterior translation or severe comminution.
Imaging and Diagnostics
Following the initial clinical stabilization and primary survey, a comprehensive multimodality imaging protocol was initiated to precisely define the fracture morphology, quantify articular depression, and formulate a definitive preoperative plan.
Plain Radiographic Evaluation
An initial trauma series of radiographs of the left knee was obtained, including standard anteroposterior, lateral, and bilateral oblique projections.
The anteroposterior radiograph demonstrated a complex, comminuted, bicondylar fracture of the proximal tibia. There was clear evidence of metaphyseal-diaphyseal dissociation, the hallmark of a Schatzker Type VI injury. The lateral tibial plateau exhibited significant articular depression and widening, characteristic of a high-energy valgus impaction force. The medial plateau demonstrated a vertical shear fracture line extending into the metaphysis, indicating a failure of the medial column.
The lateral radiograph confirmed the extensive comminution and provided a preliminary assessment of the posterior articular slope. A significant joint effusion was visible, displacing the suprapatellar fat pad. The normal anatomical posterior slope of the tibial plateau was disrupted, with evidence of posterior cortical comminution and potential posterior subluxation of the articular fragments. The oblique views further delineated the degree of articular step-off and the extent of the metaphyseal fracture lines extending distally into the tibial diaphysis.
Advanced Computed Tomography
While plain radiographs are essential for initial diagnosis, two-dimensional imaging consistently underestimates the true severity of articular comminution and depression in complex tibial plateau fractures. Therefore, a dedicated high-resolution Computed Tomography scan of the left knee with fine 1-millimeter axial cuts, supplemented by sagittal, coronal, and three-dimensional volumetric reconstructions, was obtained.
The CT scan proved critical for operative planning. The axial images allowed for precise mapping of the articular fracture lines, confirming a highly comminuted lateral plateau with a central zone of severe depression measuring approximately 14 millimeters. The coronal reconstructions clearly visualized the metaphyseal-diaphyseal dissociation and quantified the varus/valgus angular deformity.
Crucially, the CT scan identified a distinct posteromedial shear fragment. The recognition of this posteromedial fragment is of paramount importance; failure to adequately buttress this specific fragment during surgical fixation inevitably leads to postoperative varus collapse and catastrophic failure of the construct. The three-dimensional reconstructions provided a spatial understanding of the fracture fragments, allowing the surgical team to mentally "reduce" the fracture and plan the optimal trajectories for lag screws and the precise placement of periarticular locking plates.
Preoperative Templating
Utilizing the digital imaging and communications in medicine data from the CT scan, digital preoperative templating was performed. This process involved superimposing calibrated templates of various anatomical locking plates over the reconstructed images. Templating facilitated the selection of appropriate plate lengths, ensuring adequate diaphyseal fixation distal to the most inferior fracture line. It also allowed for the anticipation of specific screw trajectories to capture critical articular fragments, particularly in the highly comminuted lateral plateau, while avoiding intra-articular screw penetration.
Differential Diagnosis
The presentation of a high-energy traumatic knee injury with gross deformity and inability to bear weight necessitates a broad differential diagnosis. While the clinical and radiographic findings in this case definitively point to a complex tibial plateau fracture, it is imperative to distinguish this specific pattern from other severe periarticular injuries that present similarly but require vastly different management algorithms.
| Diagnosis | Clinical Features | Radiographic Hallmarks | Management Implications |
|---|---|---|---|
| Schatzker Type VI Tibial Plateau Fracture | Severe pain, gross swelling, valgus/varus deformity, metaphyseal instability. High risk of compartment syndrome. | Bicondylar involvement with complete metaphyseal-diaphyseal dissociation. Articular depression and widening. | Requires staged management: initial spanning external fixation followed by delayed definitive dual plating once soft tissues permit. |
| Schatzker Type V Tibial Plateau Fracture | Similar to Type VI but often less profound metaphyseal instability. Medial and lateral joint line tenderness. | Bicondylar fracture without complete metaphyseal-diaphyseal dissociation. The metaphysis remains attached to the diaphysis. | May still require dual plating, but the intact metaphyseal-diaphyseal continuity slightly alters the biomechanical demands of the fixation construct. |
| Distal Femur Fracture (AO/OTA Type 33-C) | Deformity proximal to the joint line. Shortening of the thigh. Knee effusion if intra-articular. | Supracondylar or intercondylar fracture lines of the distal femur. Tibial plateau remains intact. | Requires distal femoral locking plates or retrograde intramedullary nailing. Soft tissue envelope concerns differ from proximal tibia. |
| Traumatic Knee Dislocation (KD) with Periarticular Fracture | Extreme instability in multiple planes. High incidence of popliteal artery injury and peroneal nerve palsy. | Gross malalignment of the tibiofemoral joint. Often associated with avulsion fractures (e.g., Segond sign, fibular head avulsion). | True surgical emergency requiring immediate reduction. High priority for CT angiography to rule out vascular disruption. |
Surgical Decision Making and Classification
The management of high-energy tibial plateau fractures represents one of the most challenging paradigms in orthopedic trauma. The decision-making process is dictated not only by the osseous morphology but, more importantly, by the condition of the surrounding soft tissue envelope.
Fracture Classification Systems
Accurate classification is essential for guiding treatment and predicting prognosis. This injury was classified using three distinct systems:
- Schatzker Classification: Classified as a Type VI. This denotes a bicondylar fracture with complete dissociation of the metaphysis from the diaphysis. It represents the highest energy pattern in this system, associated with severe soft tissue compromise and a high complication rate.
- AO/OTA Classification: Classified as a 41-C3. This indicates a complete articular fracture (C) of the proximal tibia (41) with multifragmentary articular and metaphyseal comminution (3).
- Luo's Three-Column Classification: Based on axial CT imaging, the proximal tibia is divided into medial, lateral, and posterior columns. This fracture involved all three columns (a three-column fracture), specifically highlighting the presence of the posteromedial fragment, which dictates the necessity for a posterior or posteromedial surgical approach.
Damage Control Orthopedics
The traditional approach of "Early Total Care" (immediate open reduction and internal fixation) for high-energy Schatzker VI fractures has historically been associated with unacceptably high rates of devastating complications, including deep soft tissue infection, wound dehiscence, and osteomyelitis, often leading to amputation. The fragile soft tissue envelope, already traumatized by the initial impact and subsequent swelling, cannot tolerate the additional surgical insult of extensive incisions and periosteal stripping in the acute setting.
Therefore, the principle of "Damage Control Orthopedics" was strictly applied. The immediate goal was not definitive articular reduction, but rather restoration of limb length, alignment, and stability to protect the soft tissues and allow the edema to subside. The decision was made to proceed urgently to the operating room for the application of a knee-spanning external fixator.
Definitive open reduction and internal fixation would be delayed until the soft tissue envelope demonstrated sufficient recovery. Clinical indicators of readiness for definitive surgery include the resolution of pitting edema, the return of normal skin turgor, and the appearance of the "wrinkle sign" (epithelial wrinkling upon joint manipulation or skin pinching), which typically occurs 10 to 21 days post-injury.
Surgical Technique and Intervention
The surgical management of this complex injury was executed in a staged, biphasic manner, adhering strictly to the principles of soft tissue preservation and biomechanically sound osseous fixation.
Phase One Spanning External Fixation
The patient was taken to the operating room within 12 hours of presentation. Under general anesthesia, a thorough examination under anesthesia was deferred to avoid exacerbating the soft tissue injury.
A bridging, knee-spanning external fixator was constructed. The primary objective during pin placement was to remain strictly outside the anticipated zones of future surgical incisions for definitive plating.
Two 5.0-millimeter Schanz pins were placed in the anterior diaphysis of the femur, utilizing a minimally invasive percutaneous technique. Care was taken to ensure these pins were placed proximal to the suprapatellar pouch to avoid inadvertent intra-articular penetration. Distally, two 5.0-millimeter Schanz pins were placed in the anteromedial face of the tibial shaft, sufficiently distal to the fracture zone and the anticipated distal extent of the definitive medial plate.
Manual traction was applied to restore limb length and correct the gross valgus deformity. Multi-planar fluoroscopy confirmed the restoration of the mechanical axis and the provisional alignment of the metaphyseal-diaphyseal junction. The external fixator frame, utilizing carbon fiber rods and multi-pin clamps, was then rigidly tightened. The pin sites were dressed meticulously, and the limb was elevated.
Phase Two Definitive Fixation
Fourteen days post-injury, clinical examination revealed significant improvement in the soft tissue envelope. The swelling had dramatically subsided, the ecchymosis was resolving, and a positive wrinkle sign was present over the anterolateral and posteromedial aspects of the proximal tibia. The patient was cleared for definitive open reduction and internal fixation.
Surgical Approaches
Given the bicondylar nature of the fracture and the presence of a distinct posteromedial fragment identified on the preoperative CT scan, a dual-incision approach was mandatory. Attempting to address a Schatzker VI fracture through a single anterior midline incision requires excessive soft tissue stripping and invariably fails to adequately reduce and buttress the posterior columns.
The patient was positioned supine on a radiolucent Jackson table. A bump was placed under the ipsilateral hip to internally rotate the leg, facilitating access to the posteromedial corner. A sterile tourniquet was applied to the proximal thigh but not inflated, reserving it for potential excessive hemorrhage.
1. Posteromedial Approach:
The posteromedial approach was executed first. This is biomechanically critical, as restoring the medial column provides a stable foundation against which the lateral plateau can be reduced. An incision was made along the posteromedial border of the proximal tibia. The saphenous nerve and vein were identified and protected. The pes anserinus was retracted anteriorly, and the medial head of the gastrocnemius was retracted posteriorly, exposing the posteromedial fracture fragment.
2. Anterolateral Approach:
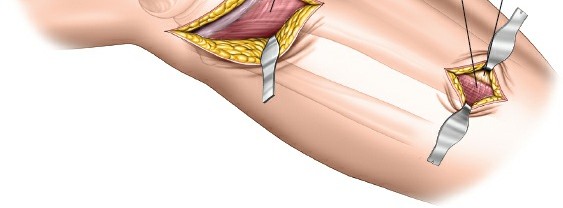
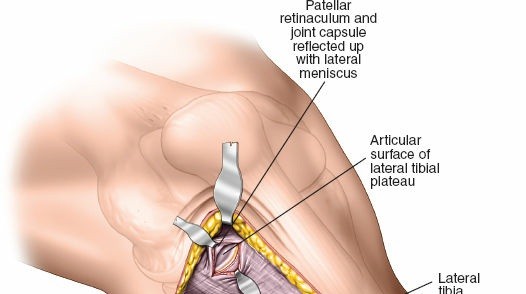
Following the medial column stabilization, a standard anterolateral approach was performed. An incision was made centered over Gerdy's tubercle, extending proximally toward the lateral epicondyle and distally along the anterior tibial crest. The iliotibial band was incised in line with its fibers. The anterior compartment musculature was elevated subperiosteally off the lateral tibia. A submeniscal arthrotomy was performed, sharply dissecting the coronary ligaments to elevate the lateral meniscus, providing direct visualization of the depressed articular surface.
Articular Reduction and Grafting
Through the anterolateral arthrotomy, the severe central articular depression was visualized. The lateral cortical fracture fragment (often referred to as the "trapdoor") was hinged open like a book. Utilizing bone tamps introduced through the metaphyseal fracture window, the depressed articular segments were carefully elevated to restore the joint line congruity, referencing the intact portions of the plateau and the femoral condyles.
Elevation of these chronically depressed fragments inevitably creates a substantial metaphyseal bone void. To support the elevated articular surface and prevent postoperative subsidence, this void must be filled. In this case, a structural allograft combined with a synthetic calcium phosphate bone cement was utilized. The calcium phosphate provides high early compressive strength, allowing for more aggressive early rehabilitation while the allograft incorporates over time.
Once the articular surface was anatomically restored and grafted, the lateral cortical "trapdoor" was closed, and provisional fixation was achieved with multiple smooth Kirschner wires placed subchondrally.
Biomechanical Fixation Construct
The definitive fixation required a robust, load-bearing construct capable of neutralizing the complex deforming forces across the metaphyseal-diaphyseal junction.
Medial Column Fixation:
Through the posteromedial approach, the vertical shear fragment was reduced anatomically using a large pointed reduction forceps. A 3.5-millimeter pre-contoured posteromedial anti-glide plate was applied. This plate functions in a buttress mode, neutralizing the vertical shear forces that drive the medial plateau distally and into varus. Non-locking cortical screws were utilized to lag the plate to the bone, maximizing the buttress effect.
Lateral Column Fixation:
Through the anterolateral approach, a 3.5-millimeter proximal tibial anatomical locking compression plate was applied. This plate acts as a neutralization plate for the lateral column and provides a fixed-angle construct to bridge the metaphyseal-diaphyseal dissociation. Multiple proximal locking screws were inserted parallel to the joint line in a "rafting" configuration to support the elevated articular surface. The distal portion of the plate was secured to the tibial diaphysis utilizing a combination of locking and non-locking screws, ensuring at least three bicortical points of fixation distal to the most inferior fracture line.
Intraoperative fluoroscopy, encompassing true anteroposterior, lateral, and oblique views, confirmed anatomic articular reduction, restoration of the mechanical axis, and appropriate hardware placement without intra-articular penetration. The wounds were irrigated copiously and closed in layers over closed-suction drains.
Post Operative Protocol and Rehabilitation
The postoperative rehabilitation protocol for a Schatzker Type VI tibial plateau fracture is prolonged and requires a delicate balance between protecting the surgical fixation and preventing debilitating joint stiffness.
Acute Postoperative Phase
Immediately postoperatively, the limb was placed in a hinged knee brace locked in full extension to protect the soft tissue repairs and the fracture construct. The closed-suction drains were removed on postoperative day two.
Deep vein thrombosis prophylaxis was initiated immediately, utilizing low-molecular-weight heparin, and continued for a minimum of four weeks, given the high risk associated with major lower extremity trauma and prolonged immobility. Intravenous antibiotics (first-generation cephalosporin) were administered for 24 hours postoperatively.
Pain management utilized a multimodal approach, including scheduled acetaminophen, non-steroidal anti-inflammatory drugs (once hemostasis was assured and renal function verified), gabapentin for neuropathic pain modulation, and judicious use of opioid analgesics for breakthrough pain.
Intermediate and Late Rehabilitation
Weight Bearing:
Strict non-weight bearing status on the operative extremity was enforced for a total of 10 to 12 weeks. The complex articular comminution and metaphyseal dissociation require substantial time for preliminary callus formation and osseous integration of the bone graft before they can withstand axial loading forces. Premature weight-bearing is the leading cause of hardware failure and articular subsidence.
Range of Motion:
Despite the weight-bearing restrictions, early range of motion is critical to prevent arthrofibrosis and nourish the articular cartilage. Continuous Passive Motion machines were initiated on postoperative day two, starting from 0 to 30 degrees and advancing 10 degrees daily as tolerated. Active-assisted and passive range of motion exercises under the guidance of a physical therapist were emphasized. The goal was to achieve a minimum of 90 degrees of flexion by week four and full extension immediately.
Strengthening and Return to Function:
Isometric quadriceps and hamstring strengthening (e.g., straight leg raises, quad sets) were initiated immediately. Progressive resistance exercises were delayed until radiographic evidence of fracture consolidation was observed, typically around the 12-week mark.
Following the 12-week non-weight bearing period, a progressive partial weight-bearing protocol was initiated, advancing by 25% of body weight weekly, transitioning to full weight-bearing by week 16, contingent upon clinical and radiographic healing. Return to heavy manual labor for this patient was anticipated to take a minimum of 6 to 9 months, and he was counseled regarding the high likelihood of permanent functional limitations and the risk of post-traumatic osteoarthritis.
Clinical Pearls and Pitfalls
The management of high-energy tibial plateau fractures is fraught with potential complications. Adherence to established principles is paramount for optimizing outcomes.
Clinical Pearls:
* Respect the Soft Tissue Envelope: The condition of the soft tissues dictates the timing of surgery. Applying the principles of Damage Control Orthopedics with a temporary spanning external fixator significantly reduces the risk of devastating wound complications.
* Identify the Posteromedial Fragment: Rigorous evaluation of the preoperative CT scan is required to identify coronal plane fractures. The posteromedial fragment must be specifically addressed and buttressed; failure to do so is a primary cause of postoperative varus collapse.
* Utilize the Three-Column Concept: Moving beyond simple AP/Lateral plain films and utilizing Luo's three-column CT classification ensures that all unstable segments of the proximal tibia are recognized and mechanically neutralized.
* Meticulous Submeniscal Arthrotomy: Direct visualization of the articular surface is essential for accurate reduction. Fluoroscopy alone is insufficient for judging the congruity of the lateral plateau.
Clinical Pitfalls:
* Operating Through Compromised Skin: Performing definitive open reduction through swollen, blistered, or ecchymotic skin dramatically increases the risk of deep infection and wound dehiscence. Patience is a surgical virtue in these injuries.
* Missing Compartment Syndrome: High-energy proximal tibia fractures carry a high risk of compartment syndrome. Relying solely on the presence of palpable pulses is a critical error; pain out of proportion and pain with passive stretch are the earliest and most reliable clinical indicators.
* Inadequate Metaphyseal Fixation: In Schatzker VI fractures, the metaphyseal-diaphyseal dissociation requires robust, rigid fixation. Using plates that are too short or failing to achieve adequate bicortical purchase distal to the fracture lines will lead to mechanical failure.
* Iatrogenic Peroneal Nerve Injury: Excessive traction during the anterolateral approach or improper placement of retractors around the fibular head can convert a mild neuropraxia into a permanent devastating nerve palsy. Careful dissection and protection of the common peroneal nerve are mandatory.
You Might Also Like