Schatzker Type VI Tibial Plateau Fracture: Diagnosis & Management in a Collegiate Athlete
Key Takeaway
A Schatzker Type VI tibial plateau fracture is a severe bicondylar knee injury from high-energy valgus impact. Diagnosis involves clinical exam, plain radiographs, and crucial high-resolution CT with 3D reconstructions. This imaging assesses comminution and articular depression, guiding precise surgical planning. MRI identifies soft tissue damage.
Patient Presentation and History
A 28-year-old male collegiate soccer player presented to the emergency department following a high-energy valgus impact injury to his left knee during a competitive match. He was tackled from the lateral side, resulting in his knee being forced into significant valgus and axial compression while his foot remained planted. He reported immediate, excruciating pain, inability to bear weight, and a sensation of the knee giving out or dislocating at the moment of impact. There was rapid onset of swelling.
His past medical history was unremarkable, with no known chronic conditions or prior lower extremity injuries. He denied any allergies. He was a non-smoker and consumed alcohol socially. His primary goal was to return to elite-level soccer competition.
Clinical Examination
On arrival, the patient was in significant pain.
- Inspection: The left knee appeared grossly swollen, tense, and diffusely ecchymotic, particularly on the medial aspect. There was no obvious gross deformity, but the knee was held in approximately 20 degrees of flexion. No open wounds or skin tenting were noted acutely. Effusion was significant.
- Palpation: Diffuse tenderness was elicited around the entire knee joint line, especially over the medial and lateral tibial condyles. The joint was boggy and tense, consistent with a large hemarthrosis. There was no palpable crepitus, but a significant ballottement sign was present. Compartment pressures were assessed clinically and found to be non-concerning acutely.
- Range of Motion: Actively, the patient was unable to move the knee due to pain. Passively, a very limited arc from 10 to 30 degrees of flexion was achieved, met with severe pain and guarding. The end feel was soft and difficult to assess for ligamentous stability in the acute setting due to muscle guarding and pain.
- Neurological Assessment: Distal sensation was intact to light touch in all dermatomes (L2-S1). Motor function was 5/5 for ankle dorsiflexion, plantarflexion, toe extension, and flexion. Specifically, peroneal nerve function (dorsiflexion of ankle and great toe extension) was intact.
- Vascular Assessment: Bilateral dorsalis pedis and posterior tibial pulses were 2+ and symmetric. Capillary refill was brisk in all toes (<2 seconds). Ankle-brachial index was 1.0 on the affected limb. Skin temperature and color were normal.
- Ligamentous Stability: Due to pain and swelling, a comprehensive assessment of ligamentous stability was deferred to the operating room under anesthesia, but gross instability was suspected given the mechanism and fracture pattern on initial imaging.
Imaging and Diagnostics
Plain Radiographs:
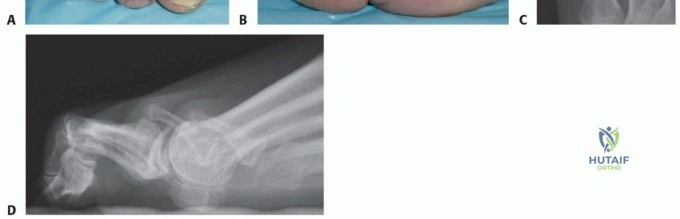
Anteroposterior, Lateral, and Bilateral Oblique views of the left knee were obtained.
* AP View: Demonstrated a comminuted bicondylar tibial plateau fracture with significant depression and lateral displacement of the lateral tibial plateau. There was also a notable fracture line extending medially, involving the medial tibial plateau, with separation of the medial condyle. The metaphyseal-diaphyseal junction appeared disrupted, with extension of fracture lines into the proximal tibial shaft. The fibular head appeared intact.
* Lateral View: Revealed significant posterior tilt of the articular surface and depression of the posterior aspect of both tibial condyles. The overall sagittal alignment of the proximal tibia was distorted.
* Oblique Views: Confirmed the comminution and aided in characterizing the extent of articular depression and displacement of both condyles.
Computed Tomography Scan:
A high-resolution CT scan with 3D reconstructions was immediately performed to thoroughly evaluate the fracture morphology and plan surgical intervention.
* Articular Involvement: Confirmed severe depression and comminution of both the medial and lateral tibial condyles, consistent with a Schatzker Type VI classification, characterized by complete metaphyseal-diaphyseal dissociation. The central articular segments were impacted deeply into the metaphyseal cancellous bone. Coronal and sagittal reformats delineated a large posteromedial shear fragment, which is a critical determinant for surgical approach selection.
Introduction and Epidemiology
Tibial plateau fractures represent a complex spectrum of intra-articular injuries that challenge even the most experienced orthopedic trauma surgeons. The Schatzker classification system categorizes these fractures based on morphology and mechanism, with the Schatzker Type VI representing the most severe variant. This fracture pattern is defined by bicondylar articular involvement coupled with complete dissociation of the tibial metaphysis from the diaphysis. The hallmark of this injury is the profound disruption of both the articular congruity and the mechanical axis of the lower extremity.
Epidemiologically, tibial plateau fractures exhibit a bimodal distribution. Low-energy mechanisms, such as simple falls, typically result in unilateral plateau fractures (often Schatzker I-III) in osteoporotic elderly populations, predominantly females. Conversely, high-energy mechanisms, including motor vehicle collisions, falls from height, and high-velocity athletic trauma, frequently cause complex bicondylar fractures (Schatzker V and VI) in younger, predominantly male patients. In the context of a collegiate athlete, a high-energy valgus or varus force combined with axial loading—often experienced during a tackle with a planted foot—delivers massive kinetic energy to the proximal tibia. This results in severe osseous comminution and devastating concomitant soft tissue envelope injuries.
The management of a Schatzker Type VI fracture in an elite athlete is particularly demanding. The primary surgical objectives are the precise restoration of articular congruity to minimize the risk of post-traumatic osteoarthritis, the re-establishment of normal mechanical alignment (coronal, sagittal, and rotational), and the provision of absolute stability to facilitate early range of motion. Failure to achieve these objectives can lead to career-ending stiffness, chronic instability, and rapid joint degeneration.
Surgical Anatomy and Biomechanics
A profound understanding of proximal tibial anatomy and knee biomechanics is mandatory for the successful reconstruction of a Schatzker VI fracture. The proximal tibia consists of the medial and lateral condyles, separated by the intercondylar eminence.
The medial tibial plateau is larger, concave in the sagittal plane, and possesses thicker, denser subchondral bone. Biomechanically, it bears approximately 60 percent of the load transmitted across the knee joint during normal ambulation. Consequently, fractures involving the medial plateau typically require significantly higher energy to occur and are often characterized by large, non-comminuted shear fragments. The lateral tibial plateau is smaller, convex in the sagittal plane, and extends further proximally than the medial plateau. Its subchondral bone is thinner and more fragile, making it highly susceptible to depression and comminution when subjected to axial and valgus loads.
The soft tissue envelope surrounding the proximal tibia is notoriously tenuous, particularly over the anteromedial aspect where the bone is subcutaneous. The blood supply to the proximal tibia is derived primarily from the anterior tibial artery and the nutrient artery of the tibia, both of which can be compromised by the initial trauma or subsequent surgical dissection. The popliteal artery, tethered proximally at the adductor hiatus and distally at the soleus arch, is highly vulnerable to traction injuries during severe fracture displacement, necessitating rigorous vascular assessment. The common peroneal nerve, winding around the fibular neck, is at risk during varus-producing injuries and lateral surgical approaches.
Biomechanically, the knee is a complex hinge joint that relies on the intricate interplay of osseous geometry, capsuloligamentous structures, and dynamic muscle forces for stability. The menisci deepen the articular surfaces and distribute compressive loads, protecting the underlying articular cartilage. In high-energy plateau fractures, the incidence of concomitant meniscal tears and ligamentous ruptures (particularly the anterior cruciate ligament and medial collateral ligament) is exceedingly high. Surgical reconstruction must restore the mechanical axis—defined by a line drawn from the center of the femoral head to the center of the ankle joint, which should pass just medial to the center of the knee joint—to ensure physiological load distribution and prevent premature articular wear.
Indications and Contraindications
The management of Schatzker Type VI tibial plateau fractures is overwhelmingly operative, given the inherent instability, articular incongruity, and mechanical malalignment associated with these injuries. Non-operative management is reserved strictly for non-ambulatory patients, those with prohibitive medical comorbidities precluding anesthesia, or in cases of severe, uncorrectable soft tissue compromise where surgical intervention would inevitably result in limb loss.
In high-energy trauma, the timing of surgical intervention is dictated by the condition of the soft tissue envelope. The concept of Damage Control Orthopedics is frequently employed. Immediate definitive fixation through a compromised soft tissue envelope carries an unacceptably high risk of wound dehiscence and deep infection. Therefore, initial management often involves the application of a knee-spanning external fixator to restore length, alignment, and rotation, while allowing the soft tissues to recover. Definitive internal fixation is delayed until the resolution of edema, typically indicated by the presence of the wrinkle sign, which usually occurs 10 to 21 days post-injury.
| Parameter | Operative Indications | Non Operative Indications |
|---|---|---|
| Articular Depression | Greater than 2 to 3 millimeters | Less than 2 millimeters (rare in Type VI) |
| Condylar Widening | Greater than 5 millimeters | Minimal widening with intact capsular hinge |
| Mechanical Axis | Coronal or sagittal malalignment greater than 5 degrees | Acceptable alignment maintained in a cast or brace |
| Instability | Clinical or radiographic instability in extension | Stable examination under fluoroscopy |
| Open Fractures | All open fractures require immediate debridement | None |
| Compartment Syndrome | Requires emergent fasciotomy and stabilization | None |
| Patient Status | Medically optimized, ambulatory demand | Non-ambulatory, severe medical comorbidities |
| Soft Tissue Envelope | Resolved edema, positive wrinkle sign | Unresolved severe blistering, active infection |
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful surgical execution. The surgeon must synthesize data from plain radiographs and computed tomography to conceptualize the fracture morphology in three dimensions. The CT scan is invaluable for identifying the location and size of specific articular fragments, particularly the posteromedial and posterolateral shear fragments, which dictate the choice of surgical approaches.
Templating is performed to determine the optimal implant types, lengths, and screw trajectories. For a Schatzker VI fracture, dual plating (medial and lateral) is the gold standard to provide rigid stabilization of both columns. The surgeon must plan the sequence of reduction, typically beginning with the restoration of the articular surface, followed by the reattachment of the metaphysis to the diaphysis. If a posteromedial fragment is present, as is common, a posteromedial approach is planned to buttress this fragment before addressing the lateral side.
The patient is positioned supine on a radiolucent operating table to facilitate unimpeded fluoroscopic imaging in both anteroposterior and lateral planes. A bump may be placed under the ipsilateral hip to correct external rotation and improve access to the lateral aspect of the knee. A sterile tourniquet is applied to the proximal thigh to provide a bloodless surgical field, although its use should be minimized to prevent ischemic complications and postoperative muscle dysfunction, particularly in an athlete. The entire lower extremity is prepped and draped free to allow for intraoperative manipulation and assessment of mechanical alignment. A femoral distractor or external fixator may be sterilized and kept available to assist with joint distraction and visualization of the articular surface.
Detailed Surgical Approach and Technique
The surgical management of a Schatzker VI fracture typically requires a dual-incision approach to adequately visualize and stabilize both the medial and lateral columns. The principle of utilizing two separate incisions—an anterolateral and a posteromedial—is to maintain a wide skin bridge (minimum of 7 centimeters) to prevent catastrophic skin necrosis.
Posteromedial Surgical Approach
The posteromedial approach is generally performed first. The rationale is that the medial column fracture is typically a high-energy shear injury with minimal comminution. Anatomical reduction of the medial column reconstructs the foundational height and alignment of the proximal tibia, providing a stable reference point for the subsequent reconstruction of the highly comminuted lateral column.
An incision is made along the posteromedial border of the proximal tibia, starting at the level of the joint line and extending distally. The superficial dissection identifies and protects the saphenous nerve and vein. The deep fascial interval is developed between the medial head of the gastrocnemius posteriorly and the pes anserinus tendons anteriorly. Retracting the gastrocnemius laterally and posteriorly protects the neurovascular bundle. The popliteus muscle is elevated off the posterior tibia to expose the posteromedial fracture line.
The posteromedial fragment is reduced using pointed reduction forceps. Due to the shear nature of this fragment, it tends to displace distally and posteriorly. Reduction is achieved by applying an anterior and proximal force. Once anatomically reduced, provisional fixation is achieved with Kirschner wires. An under-contoured posteromedial anti-glide plate (typically a 3.5 millimeter pelvic reconstruction plate or a dedicated posteromedial tibial plate) is applied in a buttress mode. The under-contouring ensures that as the plate is compressed to the bone, it applies a dynamic compressive force across the fracture site, resisting the displacing forces of the medial femoral condyle.
Anterolateral Surgical Approach
Following medial stabilization, attention is directed to the anterolateral column. A longitudinal incision is made centered over Gerdy's tubercle, extending proximally to the lateral epicondyle and distally along the anterior compartment musculature. The iliotibial band is incised in line with its fibers. The deep interval is between the iliotibial band and the tibialis anterior muscle. The origin of the tibialis anterior is elevated off the proximal lateral tibia, preserving the periosteum to maximize blood supply to the fracture fragments.
To visualize the articular surface, a submeniscal arthrotomy is performed. The coronary ligaments attaching the lateral meniscus to the tibia are incised, and the meniscus is elevated superiorly using retention sutures. This provides a direct, panoramic view of the lateral articular depression. A femoral distractor, with pins placed in the lateral femoral condyle and the distal tibial shaft, is frequently utilized to distract the joint, unhinging the fracture fragments and facilitating visualization.
Articular Reduction and Metaphyseal Fixation
The depressed lateral articular fragments are carefully elevated using bone tamps introduced through a cortical window created in the lateral metaphysis. The surgeon must meticulously reconstruct the articular congruity, piecing together the cartilaginous fragments like a mosaic. Fluoroscopy is used continuously to confirm the restoration of the joint line in both AP and lateral planes.
Elevation of the depressed articular segments creates a substantial metaphyseal bone void. This void must be rigorously filled to support the articular surface and prevent late subsidence. Options for structural support include autologous bone graft (typically harvested from the iliac crest), allograft cancellous chips, or synthetic calcium phosphate cements. Calcium phosphate cement is particularly advantageous in this setting as it provides immediate high compressive strength, supporting the articular surface during the critical early rehabilitation phase.
Once the articular surface is reconstructed and supported, a pre-contoured lateral proximal tibial locking plate is applied. The plate is positioned to act as a raft, with multiple subchondral locking screws placed immediately distal to the articular surface to support the elevated fragments. The metaphyseal-diaphyseal dissociation is then addressed. Depending on the degree of comminution, the diaphyseal segment of the plate may be fixed using relative stability principles (bridge plating) to preserve the fracture hematoma and promote secondary bone healing via callus formation. The mechanical axis is rigorously checked clinically using a cautery cord from the center of the femoral head to the center of the ankle, ensuring it passes through the center of the knee.
Following definitive fixation, the submeniscal arthrotomy is meticulously repaired to restore the hoop stresses of the meniscus. The wounds are irrigated copiously, and layered closure is performed over a suction drain to minimize postoperative hematoma formation.
Complications and Management
The treatment of Schatzker VI fractures is fraught with potential complications, stemming from both the severe initial trauma and the extensive surgical intervention required. Anticipation, early recognition, and aggressive management of these complications are critical to optimizing patient outcomes.
| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Deep Wound Infection | 5 to 15 percent | Prevention: Delay surgery until soft tissue recovery, meticulous tissue handling, broad skin bridges. Salvage: Aggressive serial surgical debridement, targeted intravenous antibiotics, hardware removal if fracture is healed, soft tissue coverage with rotational or free flaps (e.g., medial gastrocnemius flap). |
| Post Traumatic Osteoarthritis | 20 to 40 percent | Prevention: Anatomic articular reduction, restoration of mechanical axis, stable fixation allowing early motion. Salvage: Non-operative management (NSAIDs, injections, bracing), corrective osteotomy for malalignment, total knee arthroplasty for end-stage disease. |
| Arthrofibrosis and Joint Stiffness | 10 to 20 percent | Prevention: Rigid internal fixation, early continuous passive motion, aggressive physical therapy. Salvage: Intensive physical therapy, manipulation under anesthesia, arthroscopic or open lysis of adhesions, quadriceps snip or V-Y advancement in severe cases. |
| Hardware Failure and Loss of Reduction | 5 to 10 percent | Prevention: Appropriate implant selection (dual plating for bicondylar fractures), adequate bone void filling, strict adherence to weight-bearing restrictions. Salvage: Revision open reduction and internal fixation, augmentation with bone grafting, transition to circular external fixation. |
| Compartment Syndrome | 5 to 10 percent | Prevention: High index of suspicion, serial clinical examinations, avoidance of tight dressings. Salvage: Emergent four-compartment fasciotomy of the lower leg, delayed primary closure or split-thickness skin grafting. |
| Peroneal Nerve Palsy | 1 to 3 percent | Prevention: Careful dissection during the lateral approach, avoidance of excessive traction, proper padding. Salvage: Observation and electromyography at 6 weeks, ankle-foot orthosis for foot drop, nerve exploration or tendon transfers if no recovery by 6 to 12 months. |
Post Operative Rehabilitation Protocols
Rehabilitation following a Schatzker VI fracture in a collegiate athlete is a protracted and highly structured process, requiring close collaboration between the orthopedic surgeon, physical therapist, and athletic trainer. The protocol must balance the need for early motion to prevent arthrofibrosis with the necessity of protecting the articular reconstruction and metaphyseal fixation.
Phase 1: Maximum Protection and Early Motion (Weeks 0 to 6)
The primary goals in this phase are wound healing, edema control, and the restoration of passive range of motion. The patient is strictly non-weight-bearing on the operative extremity. A hinged knee brace is typically locked in extension for ambulation to protect the soft tissues but is unlocked for therapy. Continuous passive motion machines may be utilized immediately postoperatively, aiming for 0 to 90 degrees of flexion within the first two weeks. Patellar mobilization is critical to prevent infrapatellar contracture syndrome. Quadriceps sets and straight leg raises are initiated to prevent profound muscle atrophy.
Phase 2: Progressive Weight Bearing and Active Motion (Weeks 6 to 12)
Radiographic evaluation at 6 weeks dictates the progression of weight-bearing. If callus formation is evident at the metaphyseal-diaphyseal junction and the articular surface remains maintained, the patient is transitioned to toe-touch weight-bearing, progressing to partial weight-bearing (approximately 50 percent of body weight) by week 8 to 10. Active range of motion is aggressively pursued to achieve full extension and functional flexion (greater than 120 degrees). Closed kinetic chain exercises, such as mini-squats and leg presses within a protected range, are introduced to facilitate neuromuscular re-education.
Phase 3: Full Weight Bearing and Strengthening (Months 3 to 6)
Once radiographic union is confirmed (typically around 12 weeks), the patient is cleared for full weight-bearing. The focus shifts to maximizing lower extremity strength, endurance, and proprioception. Advanced closed kinetic chain exercises, stationary cycling, and aquatic therapy are utilized. Isokinetic testing may be employed to identify specific strength deficits compared to the contralateral limb.
Phase 4: Return to Sport Progression (Months 6 to 12+)
For the collegiate athlete, this phase is critical and highly individualized. It involves a progressive transition from linear running to multi-directional agility drills, plyometrics, and sport-specific activities. The athlete must demonstrate symmetric strength (greater than 90 percent of the uninjured limb on isokinetic testing), full dynamic stability, and psychological readiness before being cleared for full contact practice and eventual return to competition. It is imperative to counsel the athlete that maximum medical improvement may take up to 18 months, and a return to pre-injury elite performance levels is not guaranteed following a Schatzker VI fracture.
Summary of Key Literature and Guidelines
The management of complex tibial plateau fractures is continuously evolving, guided by robust biomechanical and clinical research. The foundational principles were established by Schatzker et al. in 1979, who emphasized the necessity of anatomic articular reduction and stable fixation.
The superiority of dual plating over single lateral locked plating for bicondylar fractures has been extensively debated. Biomechanical studies, such as those by Higgins et al., have demonstrated that dual plating provides significantly greater resistance to subsidence under axial loading compared to single lateral locking plates, particularly when a posteromedial fracture line is present. Clinical studies by Barei et al. highlighted the high incidence of posteromedial fragments in bicondylar fractures, mandating the use of a posteromedial approach and buttress fixation to prevent varus collapse.
The Canadian Orthopaedic Trauma Society conducted a landmark multicenter randomized controlled trial comparing open reduction and internal fixation with dual plating versus circular external fixation (Ilizarov method) for severe bicondylar fractures. The study concluded that while both methods achieve satisfactory clinical outcomes, circular external fixation is associated with a lower rate of deep infection and soft tissue complications, whereas internal fixation provides a slightly better restoration of anatomic alignment. In the context of an elite athlete, internal fixation is generally preferred to ensure the most precise articular and mechanical restoration, provided the soft tissue envelope permits safe surgical approaches.
Current guidelines strongly advocate for the use of computed tomography in the preoperative planning of all high-energy tibial plateau fractures to accurately map fracture lines and dictate surgical approaches. Furthermore, the integration of 3D printing and patient-specific instrumentation is emerging as a valuable adjunct in planning complex articular reconstructions, potentially reducing operative time and improving the fidelity of the reduction in challenging cases.
