Volar Wedge Bone Grafting & Internal Fixation for Scaphoid Nonunions: An Intraoperative Masterclass

Key Takeaway
Welcome to the OR, fellows. Today, we're tackling a symptomatic scaphoid nonunion with volar wedge bone grafting and internal fixation. This masterclass will guide you through meticulous preoperative planning, precise anatomical dissection, careful nonunion débridement, anatomical reduction, and secure hardware placement, emphasizing critical surgical pearls and potential pitfalls for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Scaphoid nonunions represent one of the most unforgiving and biomechanically devastating pathologies encountered in hand and upper extremity surgery. This is not merely a delayed healing of a carpal fracture; it is a complex, progressive biomechanical collapse that demands profound anatomical knowledge and meticulous surgical execution. The scaphoid is the most frequently fractured carpal bone, accounting for up to 70% of all carpal fractures. Despite advances in immobilization and early percutaneous fixation, approximately 5% to 10% of these fractures fail to achieve osseous union, progressing to a defined nonunion after a period of six months. The failure to heal is rarely a matter of simple biology; it is almost always a combination of precarious vascularity, persistent mechanical instability, and delayed clinical recognition.
The pathogenesis of a scaphoid nonunion is driven by three primary culprits. First, delayed diagnosis or inadequate initial immobilization remains a massive contributing factor. Because acute scaphoid fractures often present with mild swelling and are frequently misdiagnosed as routine wrist sprains, patients may not seek appropriate treatment during the critical early window of osteogenesis. If a fracture remains mobile for the first four weeks, the fracture hematoma dissipates, and the highly organized process of primary bone healing is disrupted, causing the nonunion rate to skyrocket. Second, the anatomical location of the fracture plays a decisive role. Fractures occurring at the proximal pole are notoriously difficult to heal due to the retrograde intraosseous blood supply, which we will detail in the anatomy section. Finally, initial displacement of greater than 1mm indicates a disruption of the surrounding stabilizing ligaments and periosteum, drastically increasing the shear forces across the fracture site and preventing creeping substitution.

The natural history of an untreated scaphoid nonunion is not benign; it is a predictable, unrelenting march towards debilitating radiocarpal and midcarpal arthrosis. This progressive degenerative cascade is formally termed Scaphoid Nonunion Advanced Collapse (SNAC). As the scaphoid fails, it can no longer serve as the vital mechanical linkage between the proximal and distal carpal rows. The distal scaphoid fragment tends to flex along with the trapezium and trapezoid, while the proximal fragment extends with the lunate, driven by the intact scapholunate interosseous ligament. This divergent rotation creates a classic "humpback" deformity, leading to a Dorsal Intercalated Segment Instability (DISI) pattern. Over time, the abnormal kinematics cause point-loading and cartilage wear, beginning at the radial styloid (SNAC I), progressing to the radioscaphoid joint (SNAC II), and ultimately involving the capitolunate articulation (SNAC III).
Our primary surgical objective with volar wedge bone grafting and internal fixation is to intervene decisively before this degenerative cascade becomes irreversible. By addressing the humpback deformity, we are not just achieving radiographic union; we are fundamentally restoring the native carpal kinematics. The volar approach allows us to directly access the site of maximal bone loss—which is almost universally on the volar aspect of the scaphoid in these flexion deformities—and insert a structural corticocancellous wedge. This graft acts as a biological strut, forcing the scaphoid out of its collapsed state, restoring its anatomical length, and correcting the lateral intrascaphoid angle. Coupled with rigid headless compression screw fixation, this masterclass technique provides the mechanical stability and osteoconductive scaffold necessary to eradicate the nonunion and preserve wrist function for decades.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches the skin, the operating surgeon must possess a three-dimensional mastery of scaphoid and radiocarpal anatomy. The scaphoid is a unique osteological entity; nearly 80% of its surface area is covered by hyaline articular cartilage. This extensive cartilaginous shell is essential for its role as the universal joint of the wrist, articulating with the radius, lunate, capitate, trapezium, and trapezoid. However, this leaves only a minimal footprint for vascular ingress and ligamentous attachment. The scaphoid functions biomechanically as an intercalated tie-rod, bridging the proximal and distal carpal rows. It must withstand massive compressive and shear forces during routine activities, making it highly susceptible to fracture during an axial load, such as a fall on an outstretched hand (FOOSH) with the wrist in extension and ulnar deviation.

Vascularity is the absolute crux of scaphoid survival and fracture healing. The arterial supply is notoriously tenuous, exhibiting a retrograde flow pattern that is highly vulnerable to disruption. Approximately 70% to 80% of the scaphoid's intraosseous blood supply is derived from the dorsal scaphoid branches of the radial artery. These vessels enter the bone through a narrow non-articular ridge on the dorsal-radial aspect of the scaphoid waist and flow proximally. Consequently, a fracture through the waist or proximal pole physically severs this intraosseous network, leaving the proximal fragment dependent on diffusion or rendering it entirely avascular. The remaining 20% to 30% of the blood supply enters volarly at the distal tubercle via branches of the superficial palmar arch. While this volar supply reliably nourishes the distal pole, it is insufficient to support a fractured proximal pole, underscoring why proximal pole nonunions have such a high rate of avascular necrosis (AVN).
Understanding the complex ligamentous tethers surrounding the scaphoid is paramount for both exposure and postoperative stability. During the volar approach, the surgeon will directly encounter the stout volar extrinsic ligaments, primarily the radioscaphocapitate (RSC) ligament and the long radiolunate (LRL) ligament. The RSC acts as a vital fulcrum for the scaphoid waist, preventing abnormal palmar subluxation. The LRL stabilizes the lunate and the proximal scaphoid pole. A critical surgical pearl during the capsulotomy is to preserve as much of the LRL and the proximal origin of the RSC as possible. Overzealous release of these volar stabilizers can lead to iatrogenic instability of the proximal pole, making subsequent screw fixation and anatomical reduction exponentially more difficult. Dorsally, the dorsal intercarpal (DIC) and dorsal radiocarpal (DRC) ligaments provide further stability, though they are generally undisturbed during a purely volar approach.
The neurovascular topography of the volar wrist dictates our surgical window. The approach utilizes the internervous and intermuscular plane of the flexor carpi radialis (FCR) tendon. Distally, as the FCR sheath is opened, the surgeon must be acutely aware of the volar superficial branch of the radial artery, which often crosses the surgical field and typically requires ligation to achieve adequate exposure of the scaphotrapezial (ST) joint. Ulnar to the FCR lies the palmaris longus (if present) and, deep to it, the median nerve. The median nerve and the digital flexor tendons must be meticulously retracted ulnarly and protected with blunt retractors throughout the procedure to prevent catastrophic traction neuropraxia. Proximally and radially, the main trunk of the radial artery must be identified and protected, particularly during the harvesting of the distal radius bone graft.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of a successful outcome in scaphoid nonunion surgery. The volar wedge bone grafting technique is specifically indicated for symptomatic scaphoid waist nonunions that demonstrate a flexion collapse, commonly referred to as a "humpback" deformity. Clinically, these patients present with chronic, deep-seated radial wrist pain, diminished grip strength, and restricted wrist extension. Radiographically, the indication is solidified by the presence of a lateral intrascaphoid angle greater than 45 degrees or a height-to-length ratio that indicates significant volar bone loss. Furthermore, this procedure is highly indicated when there is an associated Dorsal Intercalated Segment Instability (DISI) deformity, as the volar wedge acts as a structural strut to restore the scaphoid's length, thereby realigning the lunate and correcting the carpal collapse.
A mandatory prerequisite for utilizing a non-vascularized distal radius autograft is the presence of viable bone in both the proximal and distal scaphoid fragments. The biological capacity of the proximal pole must be confirmed preoperatively. If the proximal pole demonstrates punctate bleeding intraoperatively (the "paprika sign") and preoperative MRI confirms adequate perfusion, a non-vascularized structural graft is highly appropriate. However, if the proximal pole is entirely sclerotic, fragmented, or demonstrates overt avascular necrosis (AVN) on gadolinium-enhanced MRI, a standard non-vascularized wedge graft is relatively contraindicated, as it will likely fail to incorporate. In such scenarios, the surgeon must pivot to a vascularized bone graft (e.g., 1,2-Intercompartmental Supraretinacular Artery [1,2-ICSRA] graft or a free medial femoral condyle graft).
Absolute contraindications for this specific joint-preserving procedure include the presence of advanced degenerative changes. If the patient has progressed to SNAC Stage II (radioscaphoid arthrosis) or Stage III (capitolunate arthrosis), attempting to reconstruct the scaphoid is futile and will not alleviate the patient's pain. In these advanced stages, salvage procedures such as a Proximal Row Carpectomy (PRC) or a Scaphoid Excision and Four-Corner Fusion are indicated. Additionally, active local or systemic infection, severe osteopenia that precludes rigid screw fixation, and profound patient non-compliance regarding postoperative immobilization serve as strict contraindications to this technically demanding reconstruction.
To ensure clarity for surgical decision-making, the following table delineates the precise indications and contraindications for volar wedge bone grafting with internal fixation.
| Category | Specific Clinical/Radiographic Criteria |
|---|---|
| Primary Indications | Symptomatic scaphoid waist nonunion (> 6 months duration). |
| Presence of a "humpback" flexion deformity (Volar bone loss). | |
| Lateral intrascaphoid angle > 45 degrees. | |
| Associated DISI deformity requiring carpal realignment. | |
| Confirmed viability of the proximal pole (No AVN). | |
| Relative Contraindications | Proximal pole nonunion with a very small (< 20%) proximal fragment. |
| Mild, early radioscaphoid arthrosis (SNAC I - requires careful patient counseling). | |
| Tobacco use (Requires strict cessation protocol prior to surgery). | |
| Absolute Contraindications | Advanced carpal collapse with SNAC II or SNAC III arthrosis. |
| Established Avascular Necrosis (AVN) of the proximal pole. | |
| Active local or systemic infection. | |
| Inability to comply with strict postoperative rehabilitation protocols. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is what separates an adequate surgeon from a master surgeon. The evaluation begins with a rigorous imaging protocol. Standard posteroanterior (PA), lateral, and specialized scaphoid views (45- and 60-degree pronated oblique views) are mandatory to assess the fracture orientation, degree of displacement, and the presence of any early degenerative spurring at the radial styloid. However, plain radiographs are insufficient for precise surgical templating. A high-resolution Computed Tomography (CT) scan, reformatted in the true sagittal and coronal planes of the scaphoid, is the gold standard. The CT scan allows the surgeon to accurately measure the volumetric bone void, calculate the exact lateral intrascaphoid angle, and template the required dimensions of the corticocancellous wedge graft needed to restore anatomical length.
Furthermore, assessing the vascular status of the proximal pole is a critical preoperative step. While intraoperative assessment of bleeding bone is the ultimate test, a preoperative Magnetic Resonance Imaging (MRI) scan without and with intravenous gadolinium contrast provides invaluable predictive data. A proximal pole that enhances with contrast indicates viable intraosseous microcirculation, validating the plan for a non-vascularized volar wedge graft. Conversely, a dark, non-enhancing proximal pole on T1-weighted fat-suppressed contrast images signals avascular necrosis, prompting a shift in the surgical plan toward a vascularized bone graft. The MRI is also useful for ruling out concomitant soft tissue injuries, such as tears of the scapholunate interosseous ligament or triangular fibrocartilage complex (TFCC).
Graft selection and fixation strategy must be finalized before entering the operating theater. For a volar wedge, the ipsilateral distal radius is the preferred donor site. It offers a reliable source of structurally sound corticocancellous bone, is accessible within the same surgical field, and avoids the significant donor site morbidity associated with iliac crest bone harvesting. Regarding fixation, the advent of cannulated, headless compression screws has revolutionized scaphoid nonunion management. The surgeon must choose between a fully threaded, variable-pitch screw (e.g., Acutrak), which offers excellent compression across smaller fragments, or a smooth-shanked screw (e.g., Herbert), which provides robust absolute compression but requires larger fragment sizes to avoid thread bridging. We typically template for a screw length that will engage the dense subchondral bone of the proximal pole without penetrating the radiocarpal joint.
Anesthesia and patient positioning are optimized for surgical efficiency and patient safety. The procedure is typically performed under a regional brachial plexus block (supraclavicular or axillary), supplemented with deep intravenous sedation or light general anesthesia. This ensures profound intraoperative muscle relaxation and excellent postoperative pain control. The patient is positioned supine with the affected upper extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. The arm is exsanguinated with an Esmarch bandage, and the tourniquet is inflated to 250 mmHg. The entire upper extremity, from fingertips to mid-arm, is prepped and draped in a standard sterile fashion. Although the primary plan utilizes a distal radius graft, the ipsilateral iliac crest is often prepped and draped as a contingency, should a larger or more robust structural graft be required unexpectedly.
Step-by-Step Surgical Approach and Fixation Technique
The execution of the volar wedge bone grafting technique requires absolute precision. We begin with a curvilinear incision over the volar aspect of the wrist. The incision starts proximally over the flexor carpi radialis (FCR) tendon, approximately 3-4 cm proximal to the wrist crease, and extends distally, gently curving across the wrist flexion creases to terminate at the base of the thenar eminence, safely avoiding the palmar cutaneous branch of the median nerve.

Superficial dissection is carried down through the subcutaneous tissue to identify the FCR tendon sheath. Using a #15 blade, the superficial fascia of the FCR sheath is incised longitudinally. The FCR tendon is then mobilized and retracted radially. Deep to the FCR, the surgeon will encounter the floor of the tendon sheath, which is sharply divided. At this juncture, the volar superficial branch of the radial artery is frequently encountered traversing the field; it is carefully isolated, ligated, and divided to prevent troublesome bleeding and to allow unimpeded access to the deep carpal structures.
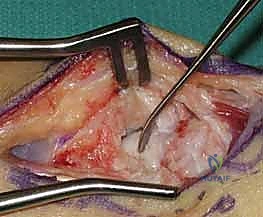
Deep dissection requires meticulous protection of the neurovascular structures. The median nerve and the digital flexor tendons are gently retracted ulnarly using a blunt Wheatlander or a Ragnell retractor. The deep volar radiocarpal capsule is now exposed. A longitudinal or H-shaped capsulotomy is performed over the scaphoid. It is a critical surgical pearl to preserve the integrity of the long radiolunate (LRL) ligament and the proximal portion of the radioscaphocapitate (RSC) ligament to prevent iatrogenic destabilization of the proximal pole. The capsular flaps are tagged with fine sutures for later repair.

With the capsule open, the scaphoid nonunion site is brought into direct view. The nonunion is often obscured by fibrous scar tissue and a pseudarthrosis. Using a combination of a sharp dental pick, small curettes, and a high-speed burr, the fibrous tissue is meticulously debrided. The sclerotic bone ends of both the proximal and distal fragments must be resected back to healthy, bleeding, cancellous bone. The appearance of punctate bleeding—the "paprika sign"—confirms the viability of the fragments. Once debrided, the true extent of the volar bone void and the humpback deformity becomes glaringly apparent.
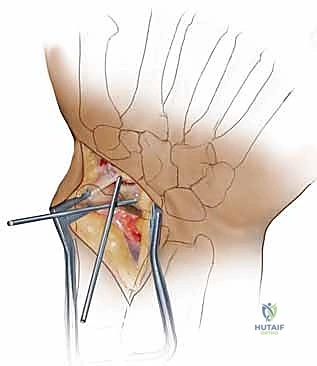
Correction of the humpback deformity is the most crucial biomechanical step. Two 0.045-inch Kirschner wires (K-wires) are inserted as joysticks: one into the distal scaphoid fragment and one into the proximal fragment. By applying an extension moment to the distal joystick and a flexion moment to the proximal joystick, the scaphoid is hinged open volarly. This maneuver restores the anatomical length of the scaphoid, corrects the lateral intrascaphoid angle, and simultaneously realigns the lunate out of its DISI posture. The resulting trapezoidal void on the volar aspect of the scaphoid is then precisely measured using a sterile caliper to determine the exact dimensions required for the bone graft.
Attention is then turned to the distal radius for graft harvest. Through the proximal extent of our existing incision, the pronator quadratus is elevated off the volar aspect of the distal radius. A cortical window is mapped out based on the caliper measurements. Using an oscillating saw and fine osteotomes, a corticocancellous wedge is carefully harvested. The surgeon must ensure the structural integrity of the cortical face of the graft while capturing a robust volume of underlying cancellous bone.

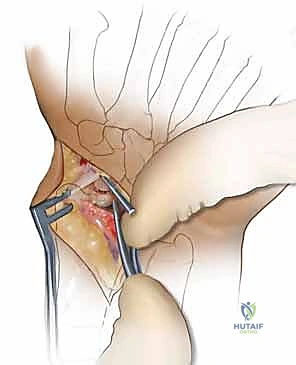
The harvested graft is meticulously shaped on the back table using a rongeur or a fine burr to perfectly match the dimensions of the scaphoid defect. The graft is then press-fit into the volar void with the cortical surface facing volarly to act as a structural buttress, and the cancellous portion facing the medullary canal to promote osteogenesis. The joysticks are relaxed, allowing the native ligamentous tension to compress the scaphoid fragments against the newly inserted wedge graft, locking it securely in place.

Rigid internal fixation is then achieved. A 0.035-inch guidewire for the cannulated headless compression screw is introduced from the distal scaphoid tubercle, directed proximally, dorsally, and ulnarly, aiming for the absolute central axis of the proximal pole. The trajectory is verified in multiple planes using intraoperative fluoroscopy. Achieving a central position in the proximal pole is statistically correlated with higher union rates and superior biomechanical pull-out strength.

Once the guidewire trajectory is confirmed, the length is measured. The outer cortex of the distal scaphoid is over-drilled to allow the screw head to countersink beneath the articular cartilage. The appropriate length headless compression screw is then advanced over the wire. As the variable pitch threads engage, the surgeon will visually and fluoroscopically observe robust compression of the distal fragment, the intercalated wedge graft, and the proximal fragment into a single, rigid construct.

The final step involves a rigorous fluoroscopic examination to ensure anatomical reduction, proper screw length without joint penetration, and solid compression. The joysticks and guidewire are removed. The volar capsule is meticulously repaired using 3-0 or 4-0 absorbable sutures to restore radiocarpal stability. The pronator quadratus is allowed to fall back over the radial donor site, and the FCR sheath and skin are closed in layers. A sterile dressing and a well-molded volar thumb spica splint are applied before the tourniquet is deflated.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, scaphoid nonunion surgery carries a significant risk profile. The most dreaded complication is persistent nonunion, which occurs in approximately 10% to 20% of cases, even with structural grafting and rigid internal fixation. Persistent nonunion is typically the result of inadequate debridement of necrotic bone, failure to achieve absolute mechanical stability, or unrecognized preoperative avascular necrosis of the proximal pole. When a nonunion persists, the patient will continue to experience pain and progressive weakness. Salvage management in the setting of a failed volar wedge graft depends on the viability of the proximal pole; if viable, a revision with a vascularized bone graft and exchange hardware may be attempted. If the proximal pole is necrotic, salvage shifts toward a Proximal Row Carpectomy (PRC) or a Scaphoid Excision and Four-Corner Fusion.
Hardware complications are also a notable concern. Headless compression screws can back out or be left proud during initial insertion, leading to impingement and rapid destruction of the articular cartilage in the radioscaphoid or scaphotrapezial joints. The incidence of symptomatic hardware prominence ranges from 5% to 8%. Furthermore, if the screw is placed eccentrically rather than down the central axis of the scaph
