Tumorous Conditions of the Hand: Surgical Excision Guide

Key Takeaway
Tumorous conditions of the hand, such as ganglion cysts, mucous cysts, and epidermoid inclusion cysts, require precise surgical management to minimize recurrence and preserve neurovascular function. This comprehensive guide details evidence-based operative techniques, including open and arthroscopic dorsal ganglion excision, volar ganglion resection, and osteophyte debridement for mucous cysts. Mastery of regional anatomy and meticulous capsular dissection are paramount for optimal postoperative outcomes in hand oncology.
Comprehensive Introduction and Patho-Epidemiology
Tumorous conditions of the hand and wrist encompass a remarkably broad and heterogeneous spectrum of benign neoplastic, non-neoplastic soft-tissue, and osseous lesions. Because the hand is a highly complex, densely packed anatomical structure characterized by minimal subcutaneous tissue and intricate biomechanical tolerances, even diminutive space-occupying lesions can produce profound functional impairment. These masses frequently result in neurovascular compromise, mechanical tendon impingement, and significant cosmetic concern for the patient. The orthopedic surgeon must approach these lesions with a comprehensive understanding of regional microanatomy, intricate carpal biomechanics, and evidence-based surgical oncology principles to ensure complete eradication while preserving maximum hand function.
Ganglions represent the absolute most common cause of focal masses in the hand and wrist, accounting for approximately 50% to 70% of all soft-tissue tumors in this region. These mucin-filled cysts characteristically arise from the synovium of adjacent joints, tendon sheaths, or directly from the substance of the tendons themselves. When originating from the flexor tendon sheath, particularly at the level of the A1 pulley, they may cause mechanical impingement leading to snapping, triggering phenomena, or restricted digital excursion. Although the precise etiology of ganglion cysts remains a subject of intense academic debate, a history of acute trauma or recurrent chronic micro-trauma—often occupational or sports-related—is a frequently reported common denominator. The pathogenesis is widely believed to involve a one-way valve mechanism at the capsular level, allowing synovial fluid to extravasate into the periarticular tissues where it concentrates into a thick, highly viscous, hyaluronic acid-rich mucin.
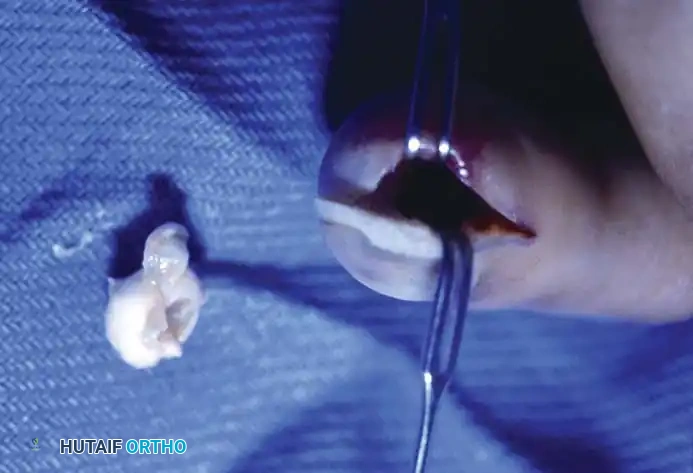
Epidermoid inclusion cysts represent another highly prevalent non-neoplastic tumorous condition, developing from the traumatic implantation of mature epithelial cells into the deep subcutaneous tissues or underlying bone. The clinical history almost universally involves a penetrating wound—such as a needle prick, thorn puncture, or crush injury—to the palm or fingertip occurring several months or even years prior to clinical presentation. Clinically, the patient develops a hard, rubbery, non-tender subcutaneous mass. The distal phalanx is the most common osseous site, where the expanding cyst can cause pressure erosion of the bone, mimicking malignant or infectious destructive processes on standard radiographs.

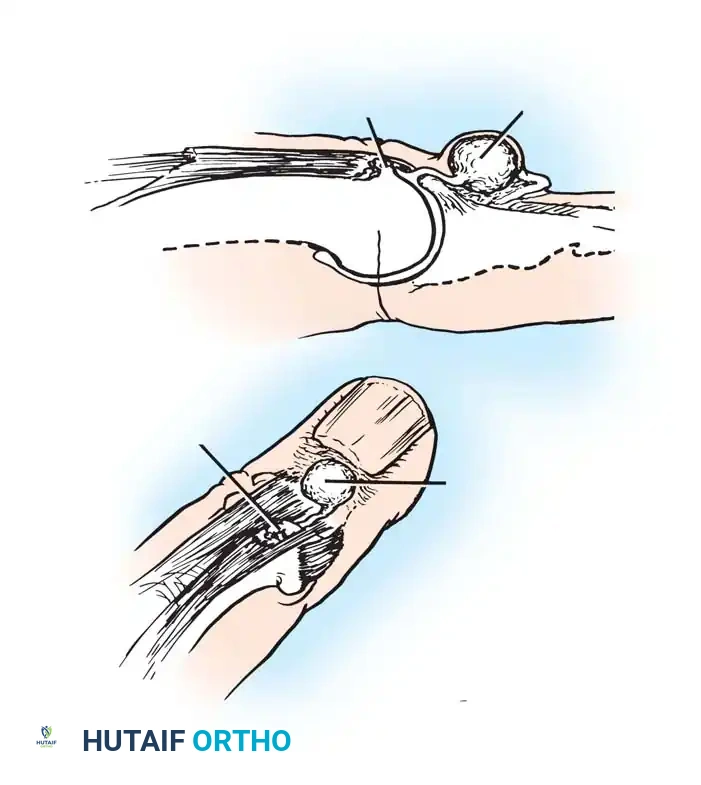
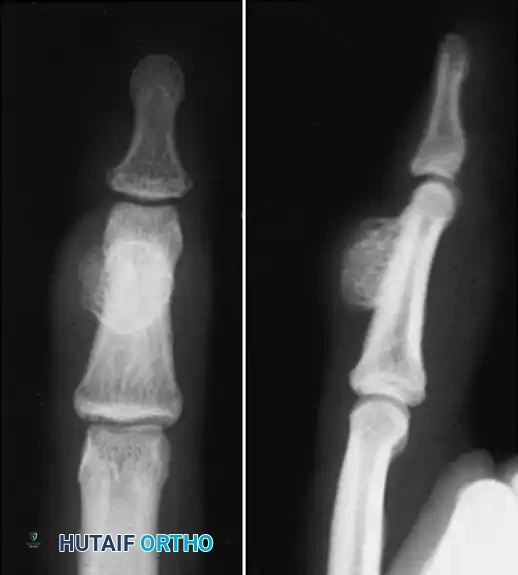
Anteroposterior radiograph demonstrating erosion at the base of the fourth metacarpal and distal capitate.

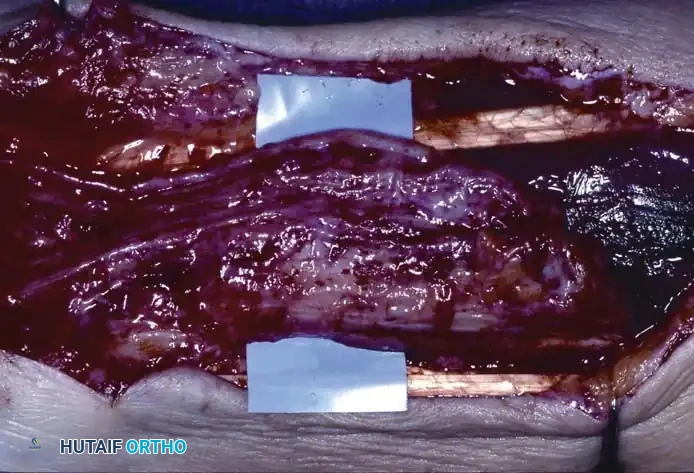
Sagittal section view revealing an intraarticular ganglion bridging the carpometacarpal joint with extensions into the substance of the capitate and fourth metacarpal.
While most ganglions and inclusion cysts are superficial, they can occasionally present within the carpal bones (intraosseous ganglions) or deep within the palmar spaces, leading to secondary compressive neuropathies. Ganglions seldom occur deep in the palm, but when they do, their presence is often heralded not by a visible external mass, but by secondary neurological changes caused by direct mass effect. For instance, cysts arising in or distal to Guyon's canal can cause profound motor neuropathy of the ulnar nerve, leading to intrinsic muscle wasting and clawing.
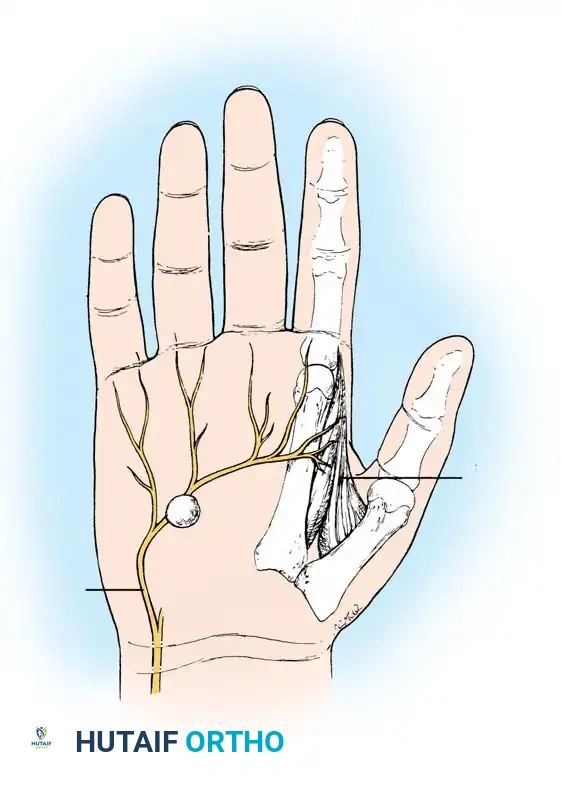
Ganglion in the palm producing pressure on the deep branch of the ulnar nerve, causing severe atrophy of the first dorsal interosseous muscle.

Clinical appearance of an epidermoid inclusion cyst on the index finger following a remote puncture wound.
Detailed Surgical Anatomy and Biomechanics
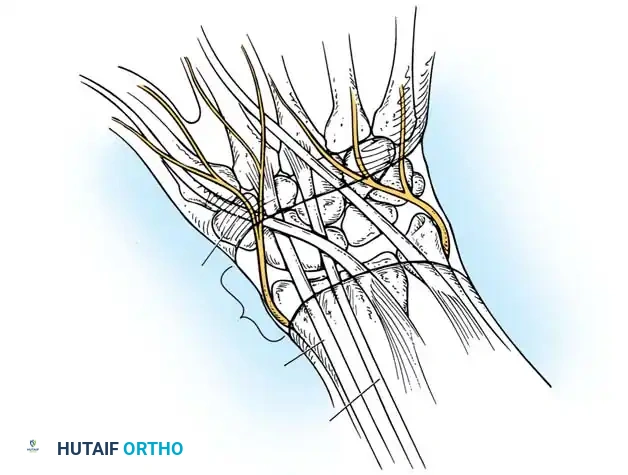
A profound mastery of the surgical anatomy of the hand and wrist is the cornerstone of safe and effective tumor excision. For dorsal wrist ganglions, the anatomical distribution follows a highly predictable pattern, with the most frequent site of origin being the dorsal scapholunate (SL) interosseous ligament. These cysts typically present as firm, smooth, fluctuant, and round masses palpable between the second and fourth extensor tendon compartments. Cysts extending proximally along the extensor tendons may feel less firm, multilocular, and irregular, yet they consistently contain the characteristic slightly yellow, gelatinous, stringy fluid. The surgeon must navigate the extensor retinaculum, meticulously retracting the extensor pollicis longus (EPL) and extensor digitorum communis (EDC) to access the dorsal capsule. Crucially, the terminal sensory fibers of the posterior interosseous nerve (PIN) course along the floor of the fourth compartment; these fibers provide nociceptive innervation to the dorsal capsule and are frequently implicated in the deep, aching pain associated with dorsal ganglions.
Volar wrist ganglions, the second most common presentation, demand an even higher level of anatomical vigilance. These cysts typically arise from the radiocarpal or scaphotrapezial joint and present volarly, just radial to the flexor carpi radialis (FCR) tendon. Their most critical anatomical relationship is with the radial artery, which frequently arborizes around, or even directly through, the lobules of the cyst. The palmar cutaneous branch of the median nerve, which arises approximately 5 cm proximal to the wrist crease and travels between the palmaris longus and FCR, is also at significant risk during volar approaches. Injury to this nerve branch results in a highly morbid, painful neuroma in the proximal palm that can severely limit grip function.
Flexor tendon sheath ganglions and epidermoid inclusion cysts present unique anatomical challenges related to the digital flexor mechanism and the terminal phalangeal pulp. Flexor sheath ganglions most commonly arise at the level of the metacarpophalangeal (MCP) joint flexor skin crease, corresponding to the proximal edge of the A1 pulley. Here, the neurovascular bundles lie in close proximity to the radial and ulnar margins of the pulley and must be protected during excision. Epidermoid cysts of the distal phalanx are intimately associated with the sterile and germinal matrices of the nail bed, as well as the terminal arborizations of the digital nerves. Expanding intraosseous epidermoid cysts can thin the cortical bone of the distal phalangeal tuft to the point of impending pathological fracture, necessitating meticulous curettage and occasionally bone grafting to restore structural integrity.

Biomechanically, the preservation of carpal stability is paramount during the excision of wrist ganglions. The dorsal SL ligament is a critical secondary stabilizer of the scapholunate articulation. While the ganglion stalk frequently originates from this ligament, the surgeon must excise only the capsular tissue and the stalk itself, strictly avoiding the deeper, structurally vital interosseous fibers of the SL ligament. Iatrogenic transection of the dorsal SL ligament can precipitate dorsal intercalated segment instability (DISI), leading to chronic pain, weakness, and eventual radiocarpal arthrosis. Similarly, when resecting volar ganglions, the stout volar radiocarpal ligaments (such as the radioscaphocapitate ligament) must be respected to prevent volar carpal destabilization.
Exhaustive Indications and Contraindications
The decision to proceed with surgical excision of a tumorous condition in the hand requires a careful risk-benefit analysis, taking into account the natural history of the lesion, the patient's symptomatology, and the potential morbidity of the surgical intervention. Ganglions occasionally resolve spontaneously, but recurrence is common when treated by simple rupture or aspiration. Historically, dorsal cysts were ruptured by digital pressure or by striking the flexed wrist with a heavy object (the "Bible bump" treatment). We strongly condemn and do not use this archaic technique, as it predictably leads to recurrence, severe periarticular fibrosis, and potential damage to adjacent osseous and tendinous structures.
Surgical excision remains the gold standard for symptomatic, recurrent, or mechanically disruptive ganglions and solid tumors. Primary indications for surgical intervention include persistent pain that limits activities of daily living, progressive neurological deficit (such as intrinsic wasting from deep palmar ganglions compressing the motor branch of the ulnar nerve), mechanical impingement causing triggering or restricted tendon excursion, and significant patient distress regarding cosmetic appearance or fear of malignancy. For epidermoid inclusion cysts, surgical excision is almost universally indicated to prevent progressive pressure necrosis of the surrounding soft tissues and impending pathological fracture of the distal phalanx.
Contraindications to surgical excision are generally relative and must be weighed against the severity of the patient's symptoms. Absolute contraindications are rare but include active local soft-tissue infection (unless the mass itself is an infected inclusion cyst requiring immediate debridement) and severe peripheral vascular disease that precludes safe tourniquet use or compromises wound healing. A critical relative contraindication for the excision of volar wrist ganglions is an abnormal modified Allen test, indicating inadequate ulnar collateral circulation to the hand. In such cases, the risk of iatrogenic radial artery injury during cyst dissection could lead to catastrophic digital ischemia.
| Parameter | Indications for Surgical Excision | Contraindications for Surgical Excision |
|---|---|---|
| Clinical Symptoms | Intractable pain, aching, or grip weakness; mechanical triggering. | Asymptomatic lesions (relative); patient preference for observation. |
| Neurovascular Status | Compressive neuropathy (e.g., Guyon's canal syndrome, PIN compression). | Failed modified Allen test (absolute for volar ganglions without vascular backup). |
| Pathological Risk | Rapid growth, atypical features on MRI, cortical bone erosion. | Active superficial cellulitis overlying the surgical site. |
| Prior Treatment | Recurrence after multiple aspirations or closed ruptures. | Medical comorbidities precluding safe anesthesia (relative). |
| Cosmesis/Psychological | Severe cosmetic distress; high patient anxiety regarding malignancy. | Unrealistic cosmetic expectations regarding surgical scarring. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is essential for the successful excision of hand tumors. The clinical evaluation must include a detailed history of the mass's onset, growth velocity, and relationship to prior trauma. Physical examination should assess the mass for fluctuance, transillumination (highly suggestive of a fluid-filled ganglion), and mobility relative to underlying tendons and overlying skin. A comprehensive neurological examination is mandatory, particularly assessing two-point discrimination and intrinsic motor function, to rule out occult compressive neuropathies. For volar masses, a modified Allen test must be meticulously performed and documented to confirm the patency of the ulnar artery and the superficial palmar arch.
Imaging modalities play a crucial role in surgical templating, particularly for atypical, recurrent, or deep-seated lesions. While standard orthogonal radiographs are often normal in the setting of soft-tissue ganglions, they are essential to rule out underlying osseous pathology, such as intraosseous ganglions, enchondromas, or the characteristic lytic, expansile lesions with sclerotic margins seen in epidermoid inclusion cysts of the distal phalanx. High-resolution ultrasonography is a cost-effective, dynamic tool for confirming the cystic nature of a mass and mapping its relationship to the radial artery. Magnetic Resonance Imaging (MRI) with and without contrast is reserved for atypical masses, solid tumors lacking transillumination, or suspected intra-articular pathology, providing exquisite detail of the cyst stalk and its capsular origin.



The choice of anesthesia and patient positioning must be tailored to the specific procedure and the patient's physiological status. While many superficial lesions can be excised under local anesthesia with epinephrine (Wide Awake Local Anesthesia No Tourniquet - WALANT), formal excision of deep dorsal or volar wrist ganglions typically requires a regional axillary block or general anesthesia combined with a well-padded pneumatic upper arm tourniquet to ensure a bloodless surgical field. The patient is positioned supine with the operative extremity extended on a radiolucent hand table. The surgeon should utilize loupe magnification (minimum 2.5x to 3.5x) and a headlight to facilitate the meticulous dissection of delicate neurovascular structures and the precise identification of the capsular stalk.
Step-by-Step Surgical Approach and Fixation Technique
The critical, overarching principle of ganglion surgery is the complete, en bloc excision of the cyst complex, definitively including its stalk and a generous margin of the involved joint capsule, without attempting to close the resulting capsular defect. Failure to resect the capsular origin is the primary etiology of postoperative recurrence.
Open Excision of a Dorsal Wrist Ganglion
The dorsal cutaneous branch of the radial nerve and the dorsal branch of the ulnar nerve must be meticulously identified and protected during the superficial dissection to prevent painful postoperative neuromas.
1. Incision and Superficial Dissection: Under tourniquet control, make a transverse incision over the proximal third of the ganglion, following Langer’s lines to optimize cosmetic outcome. Carry the incision through the dermis only. Spread the underlying subcutaneous tissues longitudinally using blunt dissecting scissors (e.g., tenotomy or Stevens scissors) and place delicate retractors.
Initial exposure of the dorsal ganglion, identifying the extensor retinaculum.
- Retinacular Management: Incise the extensor retinaculum directly over the ganglion. Isolate the extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB) tendons, retracting them radially. Dissect the extensor digitorum communis (EDC) tendons to the index finger and retract them, along with the remaining extensor tendons, ulnarward.
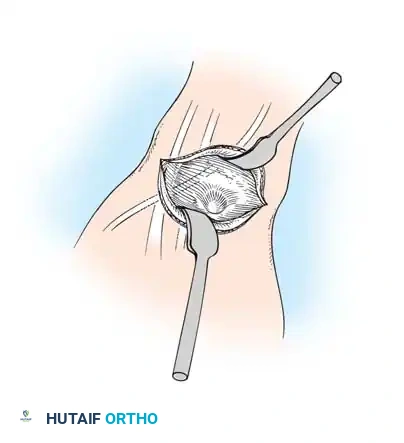
Retraction of the extensor pollicis longus (EPL) and isolation of the cyst.
- Deep Dissection and Stalk Excision: Identify and protect the extensor pollicis longus (EPL) in the proximal portion of the surgical field. Using a combination of sharp and blunt dissection, mobilize the ganglion in its entirety. Trace the stalk down to its capsular origin at the dorsal scapholunate ligament. Excise the cyst along with a 1-cm margin of the dorsal capsule. Do not excise the substance of the scapholunate interosseous ligament itself, as this will cause catastrophic carpal instability.
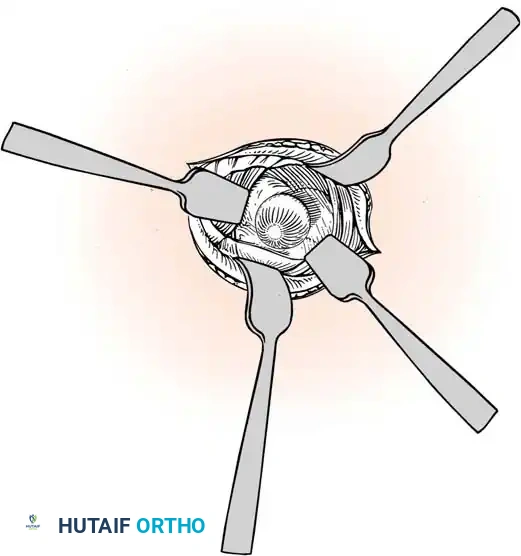
Careful separation of the ganglion from the surrounding extensor tendon sheaths.
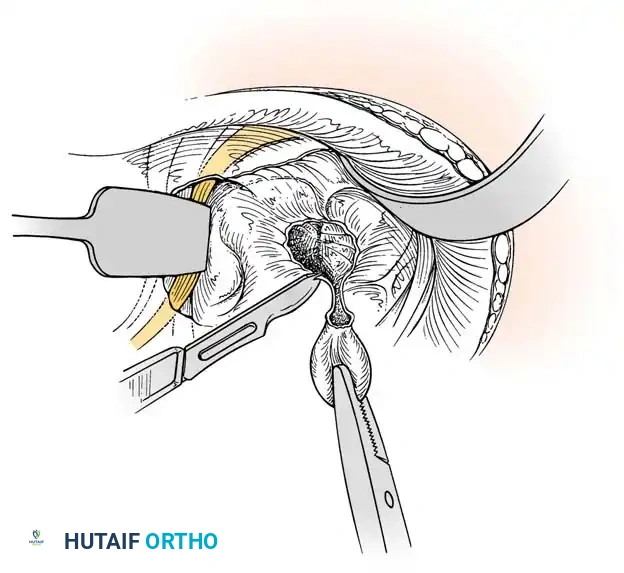
Excision of the ganglion stalk along with a generous margin of the dorsal joint capsule.
- Neurectomy and Closure: Identify the terminal sensory fibers of the posterior interosseous nerve (PIN) at the floor of the fourth compartment. Divide the nerve and gently cauterize the proximal end to denervate the dorsal capsule and reduce postoperative pain. Deflate the tourniquet, irrigate the wound copiously, and obtain meticulous hemostasis using bipolar electrocautery. Do not close the joint capsule. Close the skin with a running, subcuticular 4-0 Monocryl suture.
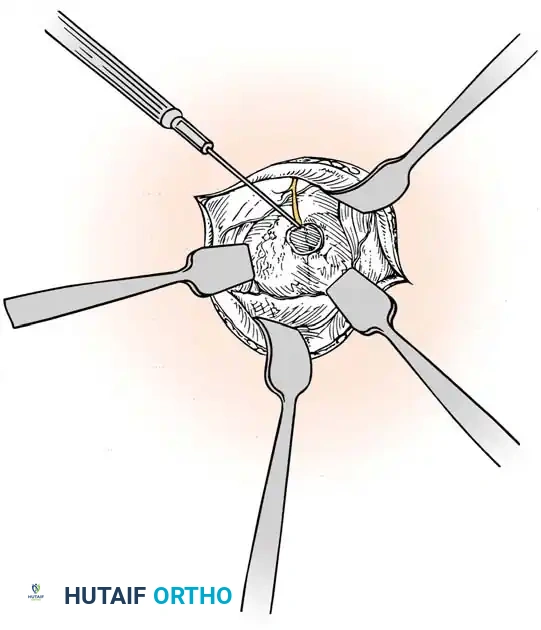
Cauterization of the capsular margins and the terminal branches of the posterior interosseous nerve.
Excision of a Volar Wrist Ganglion
The radial artery frequently arborizes around or directly through the lobules of a volar ganglion. Meticulous dissection under loupe magnification is absolutely mandatory.
1. Exposure: Make a longitudinal or lazy-S incision centered over the ganglion, typically situated just radial to the FCR tendon. Carefully avoid injury to the palmar cutaneous branch of the median nerve.
2. Arterial Mobilization: Dissect the radial artery carefully under loupe magnification. Mobilize the artery and retract it radially using silicone vessel loops. Ligate any small, direct arterial feeding branches to the cyst using fine silk ties or bipolar cautery.
3. Cyst Resection: Dissect the ganglion cyst using blunt and sharp dissection in a proximal-to-distal direction. Carry the dissection down along the stalk to its origin at the radiocarpal or scaphotrapezial joint. Excise the origin with a small portion of the surrounding volar capsule.
4. Hemostasis: Deflate the tourniquet prior to closure to inspect the integrity of the radial artery and ensure complete hemostasis.
Arthroscopic Resection of a Dorsal Wrist Ganglion
Arthroscopic resection has gained immense popularity due to decreased postoperative stiffness, smaller incisions, and the ability to evaluate concomitant intra-articular pathology.
1. Setup and Portals: Apply longitudinal distraction using finger traps attached to the index, long, and ring fingers with 3 to 4 kg of countertraction. Establish standard 3-4 and 4-5 radiocarpal portals. Insert a 2.7-mm arthroscope into the 3-4 portal.
2. Resection: Locate the scapholunate ligament. Direct the arthroscope dorsally to visualize the ganglion stalk or the capsular defect. Introduce a 2.9-mm full-radius shaver through the 4-5 portal. Excise a 1-cm diameter area of the dorsal capsule and the ganglion stalk.
3. Safety Protocol: Stop the capsular resection immediately upon visualization of the extensor tendons to prevent iatrogenic tendon injury. Avoid damaging the intrinsic scapholunate ligament. Convert to an open procedure if complete arthroscopic resection is doubtful.

Excision of Epidermoid Inclusion Cysts
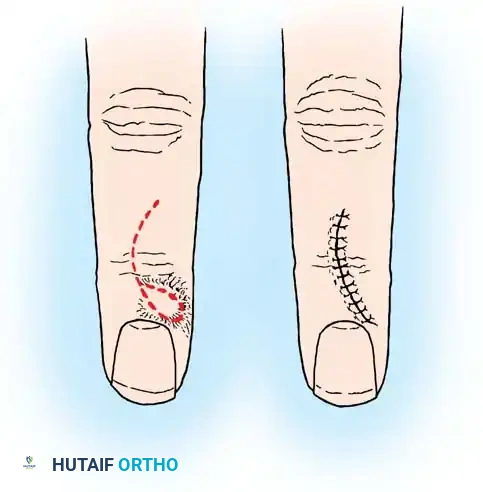
For epidermoid cysts located in the distal phalanx, the surgical approach must prioritize complete removal of the epithelial lining to prevent recurrence.
1. Exposure: Utilize a mid-lateral or palmar-oblique incision over the distal phalanx, avoiding the tactile surface of the fingertip.
2. Osseous Window: If the cyst is intraosseous, elevate a small cortical window using a high-speed burr or fine osteotome.
3. Curettage: Meticulously curette the entire cyst lining from the bony cavity. The cavity may be treated with phenol or a high-speed burr to ensure complete eradication of epithelial cells.
4. Reconstruction: If the remaining cortical shell is critically thin, pack the defect with cancellous allograft or autograft to prevent pathological fracture.


Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the excision of hand tumors carries a distinct profile of potential complications. The most frequently encountered complication following ganglion excision is recurrence. Historically, recurrence rates following simple aspiration and corticosteroid injection have been reported as high as 60% to 70%. Even with formal open excision, recurrence rates range from 4% to 10%, typically resulting from inadequate resection of the capsular stalk or failure to excise a sufficient margin of the adjacent joint capsule. Salvage management for recurrent ganglions involves a wider revision excision, often requiring a more extensive capsulotomy and meticulous identification of multilocular extensions.
Neurological complications, while less frequent, carry significant morbidity. Injury to the dorsal sensory branches of the radial or ulnar nerves during dorsal ganglion excision, or the palmar cutaneous branch of the median nerve during volar excision, can result in the formation of intractable, painful neuromas. Incidence of clinically significant neuroma formation is estimated at 1% to 3%. Salvage management requires prompt recognition; conservative measures include desensitization therapy and gabapentinoids, while refractory cases may necessitate surgical neuroma excision and proximal transposition of the nerve stump into healthy muscle or bone to prevent recurrent irritation.
Vascular complications are predominantly associated with the excision of volar wrist ganglions due to their intimate relationship with the radial artery. Iatrogenic laceration, pseudoaneurysm formation, or complete transection of the radial artery can occur. The incidence of radial artery injury is less than 1% in experienced hands but represents a surgical emergency if collateral circulation is inadequate. Salvage management requires immediate intraoperative microvascular repair or interposition vein grafting. Ligation of the radial artery is only acceptable if a preoperative modified Allen test definitively confirmed robust ulnar dominant collateral flow.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Prevention |
|---|---|---|---|
| Recurrence | 4% - 10% (Open) | Inadequate stalk/capsule excision; failure to identify multilocular cysts. | Revision wide excision; ensure 1-cm capsular margin is taken. |
| Neuroma Formation | 1% - 3% | Iatrogenic injury to superficial sensory nerves (Radial, Ulnar, Palmar Cutaneous). | Loupe magnification; nerve transposition for refractory painful neuromas. |
| Carpal Instability | < 1% | Overzealous resection of the deep intrinsic scapholunate (SL) ligament. | Strict adherence to capsular resection only; potential SL ligament reconstruction if DISI develops. |
| Radial Artery Injury | < 1% | Blind dissection of volar ganglions; failure to mobilize the artery. | Primary microvascular repair; preoperative Allen test is mandatory. |
| Postoperative Stiffness | 5% - 15% | Prolonged immobilization; failure to initiate early active ROM. | Early therapy referral; dynamic splinting; rarely requires surgical arthrolysis. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following the excision of hand and wrist tumors is designed to balance the protection of healing tissues with the prevention of debilitating joint stiffness and tendon adhesions. A phased, progressive approach is essential, particularly for lesions excised in close proximity to the extensor or flexor mechanisms.
Phase I: Immediate Postoperative Period (Days 0 to 14)
Immediately following surgery, the wrist is immobilized in a bulky, sterile compressive dressing reinforced with a well-padded volar plaster or fiberglass splint. For dorsal ganglions, the wrist is splinted in approximately 10 to 15 degrees of mild extension to relieve tension on the dorsal skin incision and capsular defect. For volar ganglions, the wrist is splinted in neutral. Strict elevation of the operative extremity above the level of the heart is mandatory for the first 48 to 72 hours to minimize interstitial edema and mitigate throbbing pain. Patients are instructed to perform active range-of-motion (ROM) exercises of the uninvolved digits, elbow, and shoulder multiple times daily to promote venous and lymphatic return.
Phase II: Early Mobilization and Scar Management (Weeks 2 to 6)
At the 10- to 14-day postoperative mark, the initial surgical dressing and splint are removed, and the surgical site is inspected. Sutures (if non-absorbable) are removed. At this juncture, prolonged rigid immobilization is strictly discontinued to prevent extensor tendon adhesions and capsular contracture. Patients are transitioned to a removable, custom-fabricated thermoplastic wrist splint, to be worn primarily for protection during high-risk activities and at night.
