AAOS & ABOS Sports Medicine MCQs (Set 4): Knee Ligament & Meniscal Injuries | Board Review

Key Takeaway
This high-yield question set, Set 4, prepares you for AAOS/ABOS Sports Medicine exams. It focuses on the diagnosis, classification, and management of knee ligament injuries, meniscal tears, and patellofemoral instability, providing essential practice for board certification.
AAOS & ABOS Sports Medicine MCQs (Set 4): Knee Ligament & Meniscal Injuries | Board Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 15-year-old diver has had persistent, activity-related low back pain for the past 2 months. He denies any history of trauma. Examination reveals that the pain is localized to the lumbosacral junction, and there are no radicular symptoms. The pain is worse with back extension. Neurologic examination is normal, as are AP, lateral, and oblique radiographs of the lumbosacral spine. Further evaluation should include
Explanation
Question 2
A 23-year-old college basketball player reports persistent lateral ankle pain after sustaining an inversion injury 6 months ago. Examination reveals pain over the anterolateral ankle, absence of swelling, and no clinical instability. Management consisting of vigorous physical therapy fails to provide relief, and a intra-articular corticosteroid injection provides only temporary relief. Radiographs obtained at the time of injury and subsequent AP and varus stress views are normal. A recent MRI scan fails to show any abnormalities. Management should now include
Explanation
Question 3
Which of the following tissues used for anterior cruciate ligament (ACL) reconstruction has the highest maximum load to failure?
Explanation
Question 4
Creatine is currently being used by athletes as a dietary supplement in an attempt to enhance performance. What is the physiologic basis for its use?
Explanation
Question 5
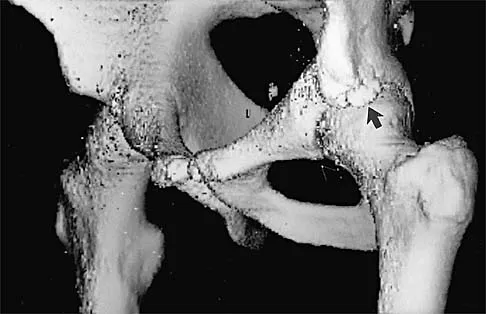
A 16-year-old high school football player sustains an injury to the left hip. The avulsed fragment identified by the arrow in Figure 34 represents the origin of which of the following structures?
Explanation
Question 6
Which of the following methods of meniscal repair has the highest load to failure strength?
Explanation
Question 7
Figure 35 shows the lateral radiograph of a 15-year-old basketball player who felt a dramatic pop in his knee when landing after a lay-up. The patient reports that he cannot bear weight on the injured extremity. Management should consist of
Explanation
Question 8
A 52-year-old man has pain in the sternal area after landing on his right shoulder in a fall from his bicycle. In addition, he reports that he had difficulty swallowing and breathing immediately after the fall, but the symptoms resolved. A CT scan reveals a posterior sternoclavicular dislocation. Initial management should include
Explanation
Question 9
What nerve is at greatest risk of harm from the portal shown in Figure 36?
Explanation
Question 10
In the majority of patients with chronic anterior cruciate ligament (ACL)-deficient knees, analysis of the gait pattern during level walking will most likely reveal which of the following changes?
Explanation
Question 11
Glenohumeral inferior stability in the adducted shoulder position is primarily a function of the
Explanation
Question 12
A 20-year-old football player has repeated episodes of heat cramps during summer training sessions. A deficiency of what electrolyte is most responsible for heat cramps?
Explanation
Question 13
Figure 37 shows the radiograph of a 23-year-old football player who sustained a blow to the anterior aspect of his shoulder. Examination reveals pain and limited rotation. He is unable to flex the arm above the shoulder. Management should include which of the following studies?
Explanation
Question 14
A 21-year-old football player had severe pain and immediate swelling in the left anteromedial chest wall while bench pressing near maximal weights several days ago. Examination at the time of injury revealed a mass on the anteromedial chest wall. Follow-up examination now reveals decreased swelling, and axillary webbing is observed. The patient has weakness to adduction and forward flexion. The injured muscle originates from the
Explanation
Question 15
A 24-year-old baseball pitcher reports pain over the posterior aspect of his shoulder that occurs only during throwing. He notes that the discomfort is greatest during the late cocking and early acceleration phases. Examination reveals localized tenderness with palpation over the external rotators and posterior glenoid. Radiographs are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
Question 16
What percent of the adult human meniscus is vascularized?
Explanation
Question 17
A 30-year-old man who participates in recreational sports reports the spontaneous onset of intermittent pain and swelling about the right knee. Examination reveals a 3+ effusion, with a range of motion of 10 degrees to 60 degrees. He has mild diffuse tenderness but no instability. MRI scans and an arthroscopic view are shown in Figures 39a through 39c. Management should consist of
Explanation
Question 18
Figure 40 shows the plain radiograph of a 30-year-old woman who has had a long history of standing bilateral anterior knee pain and a sense of patellar instability without frank dislocation. Nonsurgical management consisting of anti-inflammatory drugs and physical therapy has failed to provide relief. Examination reveals full range of motion of both knees, with moderate patellofemoral crepitance. Patellar apprehension and patellar grind tests are positive. The Q-angle measures 20 degrees. Management should now consist of
Explanation
Question 19
A 24-year-old runner who underwent an allograft reconstruction of the anterior cruciate ligament (ACL) 3 years ago now reports anterior knee pain. Examination reveals no swelling or effusion, and the patient has full motion. A Lachman test and a pivot-shift test are negative. Palpation reveals tenderness on the patellar tendon and at the inferior pole of the patella. AP and lateral radiographs are shown in Figures 41a and 41b. Management should consist of
Explanation
Question 20
What is the most common mechanism of injury that produces turf toe?
Explanation
Question 21
A 68-year-old man embarks on a 24-week strength training program. He trains at 80% of his single repetition maximum for both the upper and lower extremities. Which of the following changes can be anticipated?
Explanation
Question 22
A 26-year-old ballet dancer reports posterolateral ankle pain, especially with maximal plantar flexion. Examination reveals maximal tenderness just posterior to the lateral malleolus, and symptoms are heightened with forced passive plantar flexion. Radiographs are shown in Figures 42a and 42b. What is the most likely cause of the patient's symptoms?
Explanation
Question 23
A 23-year-old soccer player sustains a grade III complete posterior cruciate ligament (PCL) tear after colliding with another player. In reconstructing the PCL, it is optimal to reconstruct the
Explanation
Question 24
Figure 43 shows the lateral radiograph of a patient who underwent anterior cruciate ligament reconstruction. Based on the tunnel placement shown in the radiograph, evaluation of postoperative knee range of motion will most likely show
Explanation
Question 25
A 10-year-old soccer player has bilateral heel pain and reports that the pain is worse during and immediately after sports. Examination reveals that the calcaneal tuberosities are painful to palpation bilaterally. What is the most likely diagnosis?
Explanation
Question 26
A 10-year-old male Tanner stage 1 soccer player sustains a complete anterior cruciate ligament (ACL) tear. Which of the following surgical techniques minimizes the risk of iatrogenic growth arrest in this patient?
Explanation
Question 27
A 25-year-old male sustains an anterior knee dislocation. After closed reduction in the emergency department, his foot is warm with palpable dorsalis pedis pulses. His ankle-brachial index (ABI) is 0.8. What is the most appropriate next step in management?
Explanation
Question 28
A 45-year-old female experiences a popping sensation in her posterior knee while descending stairs. MRI demonstrates a complete medial meniscus posterior root tear. Biomechanically, this injury is most equivalent to which of the following conditions?
Explanation
Question 29
A 22-year-old male presents with a knee injury after a tackling collision. The dial test demonstrates 15 degrees of increased external rotation at 30 degrees of knee flexion compared to the contralateral side, but symmetric external rotation at 90 degrees. This finding indicates an isolated injury to which structure?
Explanation
Question 30
Which type of medial collateral ligament (MCL) tear has the lowest intrinsic healing potential and most frequently requires surgical repair if conservative management fails?
Explanation
Question 31
During an ACL reconstruction, arthroscopic evaluation of the posteromedial compartment reveals a longitudinal tear at the meniscocapsular junction of the posterior horn of the medial meniscus. This specific pathology is commonly referred to as a:
Explanation
Question 32
A 6-year-old child presents with a painless snapping knee. MRI demonstrates a lateral meniscus covering the entire tibial plateau. Arthroscopy reveals hypermobility of the posterior horn with an absent coronary ligament. Which discoid meniscus variant is this?
Explanation
Question 33
During a double-bundle posterior cruciate ligament (PCL) reconstruction, the anterolateral bundle is biomechanically optimized when tensioned and fixed at what angle of knee flexion?
Explanation
Question 34
A 22-year-old athlete presents with recurrent instability 1 year after an ACL reconstruction. Radiographs reveal that the femoral tunnel was placed vertically at the 12 o'clock position in the intercondylar notch. What is the most likely clinical consequence of this tunnel malposition?
Explanation
Question 35
A 30-year-old runner presents with a palpable, tender mass along the lateral joint line of the knee. MRI shows a multiloculated cystic structure associated with the lateral meniscus. This condition is most strongly associated with which type of meniscal tear?
Explanation
Question 36
A 24-year-old female athlete tears her anterior cruciate ligament (ACL) while playing soccer. During surgical reconstruction, the surgeon specifically aims to restore the posterolateral (PL) bundle. Biomechanically, restoring the PL bundle is most critical for controlling which of the following specific motions?
Explanation
Question 37
A 32-year-old male undergoes a posterior cruciate ligament (PCL) reconstruction. The surgeon opts for an open tibial inlay technique rather than a traditional transtibial tunnel technique. The primary biomechanical and anatomical advantage of the inlay technique is:
Explanation
Question 38
A 55-year-old woman feels a pop in her posterior knee while deep squatting. MRI reveals an extruded medial meniscus and a complete defect at the posterior horn root. Biomechanically, an unrepaired complete medial meniscus posterior root tear is equivalent to:
Explanation
Question 39
A 22-year-old football player sustains an isolated grade III medial collateral ligament (MCL) injury. Which specific location or characteristic of the MCL tear has the highest risk of failing nonoperative management?
Explanation
Question 40
A 27-year-old male presents with chronic knee instability. Physical examination demonstrates 15 degrees of increased external rotation at 30 degrees of knee flexion compared to the contralateral side. At 90 degrees of flexion, the external rotation is symmetric bilaterally. This Dial test finding indicates an isolated injury to which structure?
Explanation
Question 41
Radiographs of a 19-year-old skier's acutely injured knee show a Segond fracture. This pathognomonic avulsion fracture of the anterolateral proximal tibia is highly associated with an anterior cruciate ligament (ACL) tear. Which specific structure avulses to cause this fracture?
Explanation
Question 42
During arthroscopy on a 20-year-old patient, a longitudinal tear of the medial meniscus is identified. The healing potential of a meniscal repair depends heavily on vascular supply. In an adult, what portion of the medial meniscus is considered well-vascularized (the red-red zone)?
Explanation
Question 43
A patient complains of a severe loss of terminal knee extension 4 months after an anterior cruciate ligament (ACL) reconstruction. A lateral radiograph in full extension shows the entire tibial tunnel is placed anterior to the Blumensaat line. This non-anatomic placement is most likely to result in:
Explanation
Question 44
A 30-year-old male sustains a knee dislocation (KD-III) in a high-velocity accident. After closed reduction, distal pulses are palpable but the ankle-brachial index (ABI) is measured at 0.8. What is the most appropriate next step in management?
Explanation
Question 45
A 29-year-old runner presents with a palpable, firm mass along the lateral joint line of the knee. MRI reveals a multiloculated parameniscal cyst. This finding is most strongly associated with which type of meniscal tear?
Explanation
Question 46
Surgical reconstruction of the posterolateral corner (PLC) of the knee aims to restore its three primary static stabilizers. These structures include the lateral collateral ligament, the popliteus tendon, and the:
Explanation
Question 47
A 9-year-old boy (Tanner stage 1) sustains a mid-substance anterior cruciate ligament (ACL) tear and experiences recurrent instability. To minimize the risk of iatrogenic growth arrest, which surgical management is most appropriate?
Explanation
Question 48
Following an anterior cruciate ligament (ACL) reconstruction using a hamstring autograft, the graft undergoes a biological process known as ligamentization. During this process, the graft is mechanically at its weakest during which postoperative timeframe?
Explanation
Question 49
The posterior cruciate ligament (PCL) consists of two functional bundles. What is the tensioning pattern of these bundles throughout the knee's range of motion?
Explanation
Question 50
A 10-year-old girl presents with painless snapping in her lateral knee. MRI reveals a complete discoid lateral meniscus without any evidence of tearing. What is the most appropriate management for this patient?
Explanation
Question 51
The posterior oblique ligament (POL) is a key static stabilizer of the posteromedial corner of the knee. The POL is most effective at resisting valgus stress and internal tibial rotation at what degree of knee flexion?
Explanation
Question 52
Proponents of double-bundle anterior cruciate ligament (ACL) reconstruction argue that it more accurately restores native knee kinematics compared to single-bundle reconstruction. Specifically, biomechanical studies suggest double-bundle reconstruction provides superior control of:
Explanation
Question 53
A 40-year-old male undergoes a subtotal medial meniscectomy for an irreparable bucket-handle tear. Biomechanically, the loss of the medial meniscus primarily leads to which of the following alterations in knee joint contact mechanics?
Explanation
Question 54
Female athletes demonstrate a significantly higher incidence of noncontact anterior cruciate ligament (ACL) injuries compared to males. Which of the following is an established intrinsic risk factor for ACL tears in the female athletic population?
Explanation
Question 55
During a traumatic knee dislocation, the popliteal artery is exceptionally vulnerable to traction injury due to its rigid tethering within the popliteal fossa. Proximally, it is tethered by the adductor hiatus. Distally, the artery is tightly anchored by which anatomical structure?
Explanation
Question 56
A 12-year-old female soccer player with wide-open physes sustains a complete anterior cruciate ligament (ACL) rupture. She experiences recurrent instability despite bracing and physical therapy. When planning surgical reconstruction, which of the following techniques minimizes the risk of growth arrest and angular deformity?
Explanation
Question 57
A 24-year-old professional football player sustains a direct blow to the proximal tibia with the knee flexed, resulting in a posterior cruciate ligament (PCL) injury. Which bundle of the PCL is the primary restraint to posterior tibial translation at 90 degrees of knee flexion?
Explanation
Question 58
A 30-year-old skier sustains a twisting injury to his knee. On physical examination, the dial test demonstrates 20 degrees of increased external rotation at 30 degrees of knee flexion compared to the contralateral side. At 90 degrees of flexion, the external rotation is symmetric to the normal knee. What is the most likely diagnosis?
Explanation
Question 59
A 22-year-old athlete presents with a locked knee after a deep squat. MRI reveals a "double PCL sign" on the sagittal T2-weighted sequence.
What is the most appropriate management for this pathology?
Explanation
Question 60
When comparing bone-patellar tendon-bone (BPTB) autografts and hamstring autografts for primary ACL reconstruction, patients receiving a BPTB autograft have a statistically higher risk of which of the following postoperative complications?
Explanation
Question 61
An 18-year-old high school hockey player sustains an acute, isolated Grade III medial collateral ligament (MCL) tear during a game. Physical examination reveals gapping in 30 degrees of flexion with a firm endpoint in full extension. What is the most appropriate initial management?
Explanation
Question 62
A 22-year-old football player sustains a direct blow to the proximal tibia while his knee is flexed. Exam shows a posterior sag sign and +2 posterior drawer at 90 degrees of flexion, but no varus/valgus instability. Dial test is symmetric at 30 and 90 degrees. What is the most appropriate initial management?
Explanation
Question 63
Biomechanical studies have demonstrated that a complete radial tear of the medial meniscus posterior root results in contact pressures most similar to which of the following conditions?
Explanation
Question 64
A 28-year-old woman is 6 months status post anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. She complains of anterior knee pain and a painful clunk at terminal extension. She lacks 10 degrees of full extension compared to the contralateral knee. What is the most likely cause of her symptoms?
Explanation
Question 65
During clinical examination of a knee with a suspected multiligamentous injury, the dial test demonstrates 20 degrees of increased external rotation compared to the contralateral side at 30 degrees of knee flexion. At 90 degrees of knee flexion, the external rotation is symmetric to the normal side. This physical examination finding is most consistent with:
Explanation
Question 66
A 30-year-old skier sustains an acute grade III medial collateral ligament (MCL) tear at its tibial insertion. Which of the following factors is most strongly associated with failure of non-operative management for this specific injury pattern?
Explanation
Question 67
When evaluating the vascular supply of the menisci for potential repair, the peripheral blood supply predominantly arises from which of the following arteries?
Explanation
Question 68
A 24-year-old male presents to the emergency department after a high-speed motorcycle accident. His knee is grossly unstable in multiple planes, and a knee dislocation is suspected. The Ankle-Brachial Index (ABI) is calculated to be 0.85. What is the most appropriate next step in management?
Explanation
Question 69
A 12-year-old boy (Tanner stage II) sustains a midsubstance ACL rupture. He has significant growth remaining. Which of the following surgical techniques is most appropriate to minimize the risk of growth arrest or angular deformity?
Explanation
Question 70
The anterior cruciate ligament (ACL) consists of two main functional bundles. Which of the following best describes the biomechanical behavior of the anteromedial (AM) and posterolateral (PL) bundles during knee range of motion?
Explanation
Question 71
A 32-year-old male presents for evaluation of a failed ACL reconstruction. Imaging reveals widening of the femoral and tibial bone tunnels, measuring 16 mm and 15 mm, respectively. What is the most appropriate surgical approach?
Explanation
Question 72
A 10-year-old child presents with a painful clunking lateral knee. MRI demonstrates a Wrisberg variant of a discoid lateral meniscus. This specific variant is characterized by which of the following anatomical features?
Explanation
Question 73
An AP radiograph of a 22-year-old skier's acutely injured knee demonstrates an elliptic bony avulsion fragment just distal to the lateral tibial plateau. This finding is highly pathognomonic for an injury to which structure, and what associated major ligamentous tear is likely present?
Explanation
Question 74
During a medial patellofemoral ligament (MPFL) reconstruction for recurrent patellar instability, the surgeon uses fluoroscopy to identify the femoral attachment point (Schöttle's point). This radiographic landmark is located:
Explanation
Question 75
A surgeon is performing a PCL reconstruction and chooses an open tibial inlay technique over a transtibial tunnel technique. The primary biomechanical advantage of the tibial inlay technique is:
Explanation
Question 76
A 35-year-old runner presents with a palpable, firm mass on the lateral joint line of the knee. The mass fluctuates in size and is tender to palpation. MRI confirms a lateral parameniscal cyst. The most appropriate definitive surgical management involves:
Explanation
Question 77
A 4-strand hamstring autograft used in anterior cruciate ligament (ACL) reconstruction has which of the following biomechanical characteristics compared to the native ACL?
Explanation
Question 78
A 24-year-old football player sustains a direct blow to the anteromedial aspect of his knee. Examination shows a positive dial test with 15 degrees of increased external rotation at 30 degrees of knee flexion, but symmetric external rotation compared to the contralateral knee at 90 degrees. Which structure is most likely injured?
Explanation
Question 79
A 55-year-old woman presents with acute medial knee pain after a deep squat. MRI reveals a medial meniscal extrusion of 4 mm and a hyperintense signal separating the posterior horn from its tibial attachment. What is the most appropriate management for an active patient with no significant osteoarthritis?
Explanation
Question 80
A 28-year-old skier sustains an isolated grade III medial collateral ligament (MCL) tear. MRI demonstrates an avulsion of the MCL from its distal tibial attachment with the torn end retracted superficial to the pes anserinus. What is the most appropriate treatment?
Explanation
Question 81
Six months following an uncomplicated bone-patellar tendon-bone ACL reconstruction, a patient complains of a painful "clunk" and an inability to achieve terminal knee extension. MRI shows a nodular mass anterior to the ACL graft. What surgical error is the most common cause of this complication?
Explanation
Question 82
A 32-year-old male presents with a grossly deformed knee after a motorcycle crash. Following closed reduction of an anterior knee dislocation, his pedal pulses are palpable and symmetric. His Ankle-Brachial Index (ABI) is calculated as 0.85. What is the most appropriate next step in management?

Explanation
Question 83
A 9-year-old boy (Tanner stage I) with widely open physes sustains a mid-substance ACL tear. His parents wish to proceed with surgical management due to recurrent instability episodes. Which surgical technique is most appropriate?
Explanation
Question 84
During an ACL reconstruction, a systematic arthroscopic evaluation is performed. Viewing from the anterolateral portal through the intercondylar notch reveals a tear at the meniscocapsular junction of the posterior horn of the medial meniscus. What is this specific lesion called?
Explanation
Question 85
To address residual anterolateral rotatory instability during an ACL reconstruction, an anterolateral ligament (ALL) reconstruction is planned. Which of the following describes the correct anatomic origin and insertion of the ALL?

Explanation
Question 86
A 21-year-old athlete complains of the knee "giving way" 1 year after an ACL reconstruction, despite having no new trauma. On physical exam, the Lachman test is negative, but the pivot-shift test is markedly positive. Radiographs reveal the femoral tunnel is positioned at the 12 o'clock position in the coronal plane. What is the primary cause of this clinical presentation?
Explanation
Question 87
When comparing the tibial inlay technique to the transtibial tunnel technique for posterior cruciate ligament (PCL) reconstruction, the tibial inlay technique specifically avoids which of the following biomechanical issues?
Explanation
Question 88
A 24-year-old athlete reports persistent loss of terminal knee extension 6 months following an anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. Radiographs demonstrate that the tibial tunnel is positioned anterior to the Blumensaat line with the knee in full extension. What is the most likely cause of his restricted motion?
Explanation
Question 89
A 48-year-old woman experiences a sudden "pop" in the posterior aspect of her knee while squatting. MRI reveals a posterior medial meniscal root tear with 4 mm of meniscal extrusion. Which of the following best describes the biomechanical consequence of this injury if left untreated?
Explanation
Question 90
A 26-year-old soccer player sustains a twisting injury to his knee. On examination, the dial test reveals 15 degrees of increased external rotation of the tibia at 30 degrees of knee flexion compared to the contralateral side. At 90 degrees of flexion, the side-to-side difference in external rotation is less than 5 degrees. Which of the following injuries is most likely present?
Explanation
Question 91
A 31-year-old male is brought to the emergency department after sustaining a traumatic knee dislocation during a rugby match. The knee was reduced on the field. On examination, the foot is warm, but the dorsalis pedis and posterior tibial pulses are palpable but asymmetric compared to the uninjured limb. The ankle-brachial index (ABI) is 0.85. What is the most appropriate next step in management?
Explanation
None
