Operative Management of Major Upper Extremity Tendon Ruptures: Biceps, Triceps, and Pectoralis Major
Key Takeaway
Surgical management of upper extremity tendon ruptures—including the distal biceps, triceps, and pectoralis major—requires meticulous anatomical knowledge and robust fixation strategies. This comprehensive guide details evidence-based operative techniques, from single-incision distal biceps repair to anatomic triceps footprint reconstruction and pectoralis major bone-trough fixation. Proper patient selection, precise surgical execution, and structured postoperative rehabilitation are paramount for restoring optimal biomechanics and functional strength in active patients.
INTRODUCTION TO UPPER EXTREMITY TENDON RUPTURES
The surgical management of major musculotendinous ruptures in the upper extremity—specifically the distal biceps, triceps, and pectoralis major—demands a profound understanding of regional anatomy, biomechanics, and modern fixation principles. These injuries predominantly affect active, high-demand populations, often resulting from sudden, eccentric loading. Failure to restore the anatomic footprint of these tendons can lead to significant deficits in strength, endurance, and overall upper extremity kinematics. This comprehensive academic guide delineates the evidence-based surgical techniques, intraoperative pearls, and postoperative rehabilitation protocols required to achieve optimal clinical outcomes.
SINGLE-INCISION TECHNIQUE FOR REPAIR OF THE DISTAL BICEPS TENDON
Rupture of the distal biceps tendon typically occurs in middle-aged males during an unexpected eccentric extension load applied to a flexed and supinated forearm. The biceps brachii is the primary supinator of the forearm and a secondary flexor of the elbow. Nonoperative management results in a 40% loss of supination strength and a 30% loss of flexion strength; therefore, anatomic surgical reattachment to the radial tuberosity is the gold standard for active patients.
Surgical Anatomy and Biomechanics
The distal biceps tendon inserts onto the ulnar aspect of the radial tuberosity. This eccentric insertion acts as a cam, maximizing the moment arm for supination. Anatomic repair must restore this ulnar footprint to optimize supination torque. The single-incision anterior approach utilizes the internervous plane between the brachioradialis (radial nerve) and the pronator teres (median nerve).
Surgical Warning: The lateral antebrachial cutaneous nerve (LABCN) and the superficial branch of the radial nerve (SBRN) are at high risk during the anterior approach. Meticulous superficial dissection and avoidance of aggressive lateral retraction are mandatory. Furthermore, the posterior interosseous nerve (PIN) wraps around the radial neck and is vulnerable if retractors are placed carelessly along the posterior cortex of the radius.
Patient Positioning and Preparation
- Place the patient in the supine position with the operative arm extended on a radiolucent hand table.
- Apply a non-sterile tourniquet high on the brachium.
- Administer regional anesthesia (supraclavicular or axillary block) combined with general anesthesia or deep sedation.
- Prep and drape the arm in a standard sterile fashion, ensuring full mobility of the elbow and forearm.
Step-by-Step Surgical Technique
- Incision and Superficial Dissection: Make a 3- to 4-cm anterior longitudinal incision starting at the elbow crease and extending distally over the proximal forearm, following the medial border of the brachioradialis (the classic Henry approach).
- Venous and Neural Protection: Carefully identify and mobilize the superficial antecubital veins; ligate them only if necessary to prevent postoperative hematoma. Identify, mobilize, and meticulously preserve the lateral antebrachial cutaneous nerve (LABCN), which typically courses just lateral to the biceps tendon in the subcutaneous tissue.
- Tendon Retrieval: Deepen the dissection through the deep fascia. The lacertus fibrosus (bicipital aponeurosis) is usually torn but should be divided if intact to facilitate exposure. Locate the proximally retracted torn biceps tendon. Grasp the tendon end, deliver it into the wound, and place it in a moist surgical sponge. Debride the degenerative distal stump and place a locking heavy nonabsorbable suture (e.g., #2 FiberWire or #5 Ethibond) using a Krackow or Bunnell technique.
- Vascular Ligation: To safely mobilize the brachioradialis laterally and expose the deep structures, identify the radial recurrent vessels (the "leash of Henry"). Ligate and divide these vessels to prevent catastrophic postoperative bleeding and to allow unimpeded access to the radial tuberosity.
- Tuberosity Preparation: Maximize supination of the forearm to bring the radial tuberosity anteriorly into the surgical field. Place deep blunt retractors (such as knee or Hohmann retractors) carefully around the radius. Do not place retractors blindly over the posterior radial neck to avoid PIN palsy. Débride the remnant of the tuberosity free of any remaining degenerative tendon. Elevate the periosteum over the bone and use a curette or motorized burr to decorticate the footprint down to a bleeding cancellous bed, enhancing biological healing.
- Tendon Fixation: Fix the prepared tendon to the radial tuberosity. Modern fixation constructs include cortical buttons, suture anchors, transosseous bone tunnels, or interference screws. Biomechanical studies demonstrate that a cortical button combined with an interference screw provides the highest ultimate load to failure and minimizes gap formation.
- Kinematic Verification: Once the tendon is securely approximated to the tuberosity, move the forearm through a full, unrestricted range of pronation and supination. Directly visualize the repair to ensure that the tendon tracks smoothly without impingement or excessive tension.
Postoperative Care and Rehabilitation
The elbow is immobilized in a posterior splint at 90 degrees of flexion and neutral rotation for 1 to 2 weeks to allow soft tissue rest and incision healing. At 2 weeks, sutures are removed, and the patient is transitioned to a hinged elbow brace locked with an extension block at 80 degrees.
Full passive flexion is permitted immediately, alongside passive pronation and supination to 90 degrees. At 6 weeks postoperatively, progressive extension in the brace is initiated at a rate of 20 degrees per week. Active flexion is permitted at 8 weeks, and progressive resistance strengthening begins at 12 weeks. Full, unrestricted functional use, including heavy lifting and sports, is typically allowed at 16 to 20 weeks.
SURGICAL MANAGEMENT OF TRICEPS TENDON RUPTURE
Pathoanatomy and Clinical Presentation
Rupture of the triceps tendon is a relatively uncommon injury, accounting for less than 1% of all upper extremity tendon ruptures. It typically occurs as an avulsion of the tendon—often accompanied by a small osseous fragment—from its insertion on the olecranon tip. The mechanism of injury is usually a deceleration force applied to an extending elbow or a direct blow to the posterior elbow.
Systemic risk factors play a significant role in triceps ruptures. There is a well-documented association with local corticosteroid injections for olecranon bursitis, chronic renal failure, hyperparathyroidism, and the systemic use of anabolic steroids in weightlifters.
Patients present with acute pain, swelling, and ecchymosis over the posterior aspect of the elbow. Physical examination reveals exquisite tenderness to palpation. A palpable defect or gap may be present just proximal to the olecranon.
Clinical Pearl: The modified Thompson test for the triceps (squeezing the muscle belly to elicit passive extension) can be utilized. While an inability to actively extend the elbow against gravity or resistance is the hallmark sign of a complete rupture, the presence of an intact lateral expansion or anconeus muscle may mask this deficit, allowing weak active extension.
Imaging and Indications for Surgery
Standard anteroposterior and lateral radiographs may reveal the "fleck sign"—a small avulsed fragment of the olecranon indicating the site of rupture. Sagittal Magnetic Resonance Imaging (MRI) is the modality of choice for determining the integrity of the triceps tendon and distinguishing between partial and complete tears.
- Partial ruptures appear as a small fluid-filled defect within the distal tendon, presenting as a hyperintense (bright) signal on T2-weighted images.
- Complete ruptures are characterized by a large, fluid-filled gap between the retracted distal end of the triceps tendon and the olecranon process.
Nonoperative treatment is strictly reserved for partial tears with intact active extension against gravity, or for elderly, low-demand patients with significant medical comorbidities. For the vast majority of complete ruptures, acute surgical repair is indicated to restore elbow extension power.
Surgical Technique: Olecranon Reattachment
- Positioning and Approach: The patient is positioned in the lateral decubitus position with the arm draped over a padded post, or in the prone position. A posterior midline longitudinal incision is made, curving slightly laterally around the tip of the olecranon to prevent painful scar formation directly over the bony prominence.
- Nerve Protection: The ulnar nerve must be identified and protected in the cubital tunnel, especially if medial dissection or drill holes are required.
- Footprint Preparation: The ruptured end of the triceps is mobilized and debrided. The olecranon footprint is decorticated with a burr to expose a bleeding cancellous bed.
- Transosseous Fixation: Most ruptures at the olecranon insertion are repaired using heavy, nonabsorbable sutures (No. 2 or No. 5 FiberWire/Orthocord). These are woven through the distal tendon using a locking Krackow technique. Converging transosseous drill holes are created in the olecranon. The sutures are passed through these holes and tied securely over the cortical bone bridge. A tension-relieving suture (No. 5 nonabsorbable) can be placed as a figure-of-eight to protect the primary repair during early mobilization.
- Suture Anchor and Footprint Repair: Suture anchors are increasingly utilized for their biomechanical strength and ease of use. Yeh et al. described an “anatomic triceps tendon footprint repair” utilizing a double-row suture bridge technique with anchors. This method compresses the tendon flat against the olecranon, restoring a wider area of tendon-to-bone contact and creating a watertight, biomechanically superior construct.
- V-Y Advancement for Myotendinous Ruptures: For rare ruptures occurring at the myotendinous junction, or for chronic retracted tears where primary approximation is impossible, a V-Y triceps tendon advancement technique is employed. In severe cases of retraction, an autologous plantaris tendon, hamstring tendon, or Achilles allograft is interwoven with the native tissue to bridge the defect.
Postoperative Care
Following triceps repair, the elbow is immobilized in a splint at 30 to 45 degrees of flexion for 2 to 3 weeks. Immobilizing in slight flexion prevents excessive tension on the repair while avoiding the stiffness associated with full extension. After 3 weeks, the patient is transitioned to a hinged brace, and progressive active flexion and passive extension are initiated. Active strengthening of the triceps is delayed until approximately 3 months postoperatively. Isometric exercises may be started earlier, contingent upon the surgeon's assessment of repair security and soft tissue healing.
OPERATIVE REPAIR OF THE PECTORALIS MAJOR MUSCLE
Mechanism of Injury and Patient Demographics
Rupture of the pectoralis major muscle is a high-energy injury most commonly caused by forced abduction, external rotation, and extension of the shoulder against maximal resistance. Once considered a rare clinical entity, the incidence of pectoralis major ruptures has surged over the past two decades. This increase is heavily correlated with the rise in high-intensity weightlifting, specifically the bench press. However, traumatic ruptures are also frequently reported in contact sports such as rugby, football, wrestling, hockey, and water skiing.
These injuries occur almost exclusively in muscular men between the ages of 20 and 40 years. The tendon typically fails at its insertion site on the proximal humerus, lateral to the bicipital groove.
Clinical Diagnosis and Imaging
Patients present with acute, tearing pain in the anterior shoulder, accompanied by an audible "pop." Extensive swelling and ecchymosis track down the medial brachium and lateral chest wall.
Pathognomonic Sign: A highly specific sign of a pectoralis major rupture—both in acute and chronic settings—is the loss or thinning of the anterior axillary fold on the affected side.
This muscular deformity is often accentuated when the patient is asked to press their hands together in front of their chest (contracted adduction). The defect is easily palpable when compared to the contralateral, uninjured side. Physical examination will reveal marked weakness in shoulder adduction and internal rotation. MRI and dynamic ultrasound are highly effective modalities for confirming the diagnosis, determining the exact location (tendinous avulsion vs. musculotendinous junction), and assessing the degree of retraction.
Surgical Indications and Timing
Direct surgical repair is strongly indicated for acute, traumatic ruptures in young, active adults, particularly athletes and manual laborers who require full muscle power. Surgery is also indicated for patients who object to the significant cosmetic deformity.
Delayed repair may be successful if the muscle ends have not significantly retracted and if the patient exhibits some remaining tendon function during resisted adduction and internal rotation testing. However, chronic retracted tears present a formidable surgical challenge and often require allograft reconstruction.
Surgical Technique: Bone Trough and Anchor Fixation
- Positioning: The patient is placed in the beach-chair position. The arm must be freely draped to allow full manipulation during the procedure.
- Approach: A standard deltopectoral incision is utilized. The cephalic vein is identified and typically retracted laterally with the deltoid muscle. The clavipectoral fascia is incised to expose the underlying pectoralis major.
- Tendon Mobilization: The ruptured tendon is identified, often retracted medially beneath the intact clavicular head. Heavy traction sutures are placed into the tendon stump, and blunt dissection is used to release adhesions and mobilize the muscle belly laterally.
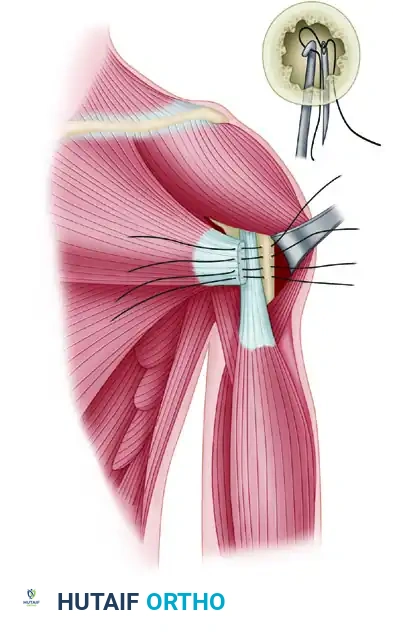
- Footprint Preparation: The anatomic insertion site on the humerus—located lateral to the long head of the biceps tendon—is identified. A high-speed burr is used to create a longitudinal bone trough at the footprint.
- Fixation: Repair is most robustly achieved by tying nonabsorbable sutures through transosseous drill holes or utilizing modern suture anchors.
Figure A: Sutures are passed through the prepared bone trough in the anatomic tendon footprint. Drill holes are created lateral to the trough to allow suture passage.
Heavy nonabsorbable sutures (e.g., #2 or #5) are woven through the mobilized pectoralis tendon using a locking mattress configuration. The free ends of the sutures are then passed into the bone trough and out through the lateral drill holes.
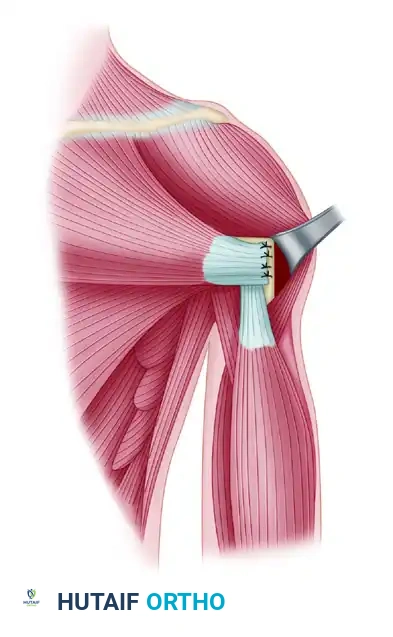
Figure B: Tying of the sutures over the lateral cortical bridge securely pulls the ruptured tendon deep into the bone trough, maximizing the surface area for biologic healing.
- Management of Chronic Ruptures: If circumferential mobilization of the tendon does not restore sufficient length to allow tension-free reattachment to the humerus, reconstruction is required. An allograft—typically an Achilles tendon with a bone block or a robust hamstring tendon—is interwoven into the native pectoralis muscle belly to provide the necessary length, allowing direct repair to the humeral footprint.
Postoperative Rehabilitation
Postoperative protocols must balance the protection of the repair with the prevention of adhesive capsulitis.
1. Phase I (0-6 weeks): The patient is placed in a shoulder immobilizer or sling. Pendulum exercises are initiated within the first or second week to maintain glenohumeral mobility. Passive forward elevation is gradually introduced, but external rotation and abduction are strictly limited to protect the repair.
2. Phase II (6-12 weeks): The sling is discontinued. Active-assisted and active range of motion exercises are progressed.
3. Phase III (3-4 months): Progressive resistance exercises are begun, focusing on gradual loading of the adductors and internal rotators.
4. Phase IV (4-6 months): Unrestricted activity, including heavy weightlifting and contact sports, is usually permitted once full, symmetric strength and range of motion are achieved. Careful evaluation of soft tissue healing is mandatory before clearing the patient for maximal eccentric loading.
📚 Medical References
- tendon rupture repair using Dall-Miles cable, Am J Knee Surg 14:17, 2001.
- Siwek CW, Rao JP: Ruptures of the extensor mechanism of the knee joint, J Bone Joint Surg 63A:932, 1981.
- Sollender JL, Rayan GM, Barden GA: Triceps tendon rupture in weight lifters, J Shoulder Elbow Surg 7:151, 1998.
- Soto-Hall R, Stroot JH: Treatment of ruptures of the long head of biceps brachii, Am J Orthop 2:192, 1960.
- Stannard JP, Bucknell AL: Rupture of the triceps tendon associated with steroid injections, Am J Sports Med 21:482, 1993.
- Stein SR, Luekens CA Jr: Closed treatment of Achilles tendon ruptures, Orthop Clin North Am 7:241, 1976.
- [Steindler A: Orthopedic operations, Springfi eld, Ill, 1940, Charles C Thomas.
Strauch RJ, Michelson H, Rosenwasser MP: Repair of rupture of the distal tendon of the biceps brachii: review of the literature and report of three cases treated with a single anterior incision and suture anchors, Am J Orthop 2:151, 1997.](https://pubmed.ncbi.nlm.nih.gov/?term=Steindler%20A%3A%20Orthopedic%20operations%2C%20Spring%EF%AC%81%20eld%2C%20Ill%2C%201940%2C%20Charles%20C%20Thomas.%0A%0AStrauch%20RJ%2C%20Michelson%20H%2C%20Rosenwasser%20MP%3A%20Repair%20of%20rupture%20of%20the%20distal%20tendon%20of%20the%20biceps%20brachii%3A%20review%20of%20the%20literature%20and%20report%20of%20three%20cases%20treated%20with%20a%20single%20anterior%20incision%20and%20suture%20anchors%2C%20Am%20J%20Orthop%202%3A151%2C%201997.)
- Symeonides PP: Isolated traumatic rupture of the adductor longus muscle of the thigh, Clin Orthop Relat Res 88:64, 1972.
- Takao M, Ochi M, Naito K, et al: Repair of neglected Achilles tendon rupture using gastrocnemius fascial fl aps, Arch Orthop Trauma Surg 123:471, 2003.
- Tang KL, Thermann H, Dai G, et al: Arthroscopically assisted percutaneous repair of fresh closed Achilles tendon rupture by Kessler’s suture, Am J Sports Med 35:589, 2007.
- Teuffer AP: Traumatic rupture of the Achilles tendon: reconstruction by transplant and graft using the lateral peroneus brevis, Orthop Clin North Am 5:89, 1974.
- Thompson TC: A test for rupture of the tendo Achillis, Acta Orthop Scand 32:461, 1962.
- Turco V, Spinella AJ:
You Might Also Like
