Patient Presentation and History
A 78-year-old male presented to the emergency department following a mechanical fall at home. He reported immediate, severe left hip pain and an inability to bear weight. The patient was ambulating independently prior to the fall, with a full activities of daily living capacity and no significant gait aids. He lives alone in a single-story residence, which highlights a high baseline level of functional independence and physiological reserve, a critical factor when determining the appropriate surgical intervention for proximal femoral fractures.
His medical history is notable for hypertension, well-controlled on a single anti-hypertensive agent, and hyperlipidemia, managed with statin therapy. He also has mild osteoarthritis of the contralateral knee, managed conservatively. There is no history of previous hip pathology, inflammatory arthropathy, or significant systemic comorbidities. His current medications include Amlodipine 5mg daily and Atorvastatin 20mg daily. He has no known allergies. His social history reveals he is a non-smoker with occasional alcohol use. Mentally, he is astute and fully oriented, scoring a 0 on the Clinical Frailty Scale, placing him in the "Very Fit" to "Well" category for his chronological age.
The mechanism of injury involved tripping over a rug and falling directly onto his left hip. There was no preceding prodromal pain or weakness. A comprehensive review of systems was otherwise unremarkable, with no signs of systemic illness or prodromal symptoms suggesting a pathological fracture or a transient ischemic attack as a precipitating factor for the fall. The absence of prodromal thigh or groin pain significantly lowers the clinical suspicion for an atypical femoral fracture or an impending pathological lesion secondary to metastatic disease.
Understanding the patient's preoperative functional status is paramount. The physiological age of this patient appears significantly lower than his chronological age. In the context of geriatric trauma, assessing the patient's baseline mobility, cognitive status, and independent living situation is just as critical as evaluating the fracture pattern itself. These factors directly dictate the survivorship of the implant, the rehabilitation potential, and the ultimate surgical decision between internal fixation, hemiarthroplasty, and total hip arthroplasty.
Clinical Examination Findings
Upon initial assessment in the trauma bay, the patient was alert, oriented, and in significant distress secondary to pain. The primary survey was intact, with airway, breathing, and circulation stabilized.
Inspection and Palpation
Inspection of the left lower extremity revealed a classic deformity associated with displaced intracapsular proximal femur fractures. The limb was shortened by approximately 2 cm and held in fixed external rotation. This characteristic deformity is driven by the unopposed pull of the iliopsoas muscle on the lesser trochanter, which externally rotates and flexes the distal fragment, combined with the proximal migration of the femur due to the spasm of the gluteal musculature and the hamstrings following the loss of the skeletal fulcrum at the femoral neck. There was no obvious ecchymosis, degloving injury, or open wound, ruling out an open fracture or a Morel-Lavallée lesion.
Palpation elicited diffuse tenderness over the left greater trochanter and the anterior groin. Axial loading of the femur and gentle internal or external rotation maneuvers of the hip were excruciatingly painful, confirming the clinical suspicion of a complete, unstable osseous disruption.
Range of Motion and Neurovascular Assessment
Range of motion was grossly restricted and painful in all planes, with particular resistance to internal rotation and abduction. Attempts at passive motion were met with severe guarding.
A meticulous neurological assessment was performed to rule out concurrent neurapraxia or pre-existing neuropathies.
* Motor function: The patient was unable to voluntarily move the left hip due to pain. However, distal motor function was intact (5/5), including knee extension (femoral nerve), ankle dorsiflexion (deep peroneal nerve), plantarflexion (tibial nerve), and great toe extension (L5 root).
* Sensory function: Light touch and pinprick sensation were intact across the L2-S1 dermatomes.
* Reflexes: Patellar and Achilles reflexes were symmetrically 2+ bilaterally.
The vascular assessment demonstrated strong, bilaterally symmetric peripheral pulses (femoral, popliteal, dorsalis pedis, posterior tibial). Capillary refill time was less than 2 seconds in all toes, and there were no signs of acute limb ischemia. Systemic examination revealed regular heart sounds without murmurs and clear lung fields, essential for clearing the patient for imminent surgical intervention.
Imaging and Diagnostics
Initial Radiographic Evaluation
Standard antero-posterior and cross-table lateral radiographs of the pelvis and left hip were obtained immediately following the primary clinical assessment.

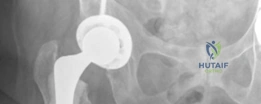
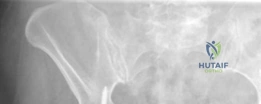
The initial AP pelvis radiograph clearly demonstrated a displaced left femoral neck fracture. The fracture line was entirely intracapsular. The femoral head was superiorly and posteriorly displaced relative to the femoral neck, with evidence of approximately 1.5 cm of shortening. The bone quality appeared reasonable for the patient's age, with a preserved Singh index and cortical thickness in the diaphyseal region, though some osteopenia was evident in the proximal trabecular patterns. No signs of pre-existing significant hip osteoarthritis (such as joint space narrowing, subchondral sclerosis, or osteophytosis) in the ipsilateral joint were noted. The contralateral hip appeared unremarkable.
Further radiographic views confirmed the complete displacement and the lack of cortical contact between the proximal and distal fragments. The fracture was classified as a Garden Type IV, indicating complete displacement with a loss of trabecular alignment between the femoral head and the acetabulum, where the head has rotated independently of the neck. Furthermore, it was classified as a Pauwels Type III, meaning the fracture line angle was greater than 70 degrees from the horizontal. This vertical fracture orientation indicates extremely high shear forces across the fracture site, portending a very poor prognosis for osteosynthesis and a high risk of nonunion or fixation failure if internal fixation were to be attempted.

Preoperative Templating and Advanced Imaging Considerations
In cases of displaced femoral neck fractures in the elderly, advanced imaging such as CT or MRI is rarely indicated unless the fracture is occult on plain radiographs or if there is a high suspicion of a pathological lesion requiring further characterization of bone stock or tumor margins. In this instance, plain radiographs were sufficient for diagnosis and surgical planning.

Preoperative digital templating is a mandatory step in the surgical workflow for arthroplasty. Templating was performed on the AP pelvis radiograph, utilizing the contralateral, uninjured hip as a reference for restoring the center of rotation, femoral offset, and leg length. The templating process involves:
1. Determining the Center of Rotation: Identifying the true acetabular floor and the teardrop to position the acetabular component.
2. Sizing the Acetabular Cup: Selecting a cup size that achieves peripheral rim fit while preserving subchondral bone.
3. Restoring Femoral Offset: Measuring the distance from the center of rotation to the anatomic axis of the femur to ensure the abductor musculature is appropriately tensioned postoperatively.
4. Correcting Leg Length Discrepancy: Utilizing the inter-teardrop line and the lesser trochanters to template the appropriate neck cut level and stem size.

Given the patient's age and the presence of proximal femoral osteopenia (Dorr Type B/C bone morphology), templating was directed toward a hybrid total hip arthroplasty construct. This involves an uncemented, press-fit acetabular component and a cemented femoral stem. The templating confirmed that a standard offset cemented stem would adequately restore the patient's native biomechanics.
Differential Diagnosis
When evaluating a patient with an acute, painful, shortened, and externally rotated lower extremity following trauma, the differential diagnosis must encompass various proximal femoral and pelvic pathologies. Accurate differentiation is critical, as the surgical management and implant selection vary drastically depending on the exact anatomical location and nature of the fracture.
| Condition | Clinical Presentation | Radiographic Hallmarks | Surgical Management Implications |
|---|---|---|---|
| Displaced Intracapsular Femoral Neck Fracture | Severe groin pain, shortened and externally rotated limb. High risk of AVN. | Fracture line proximal to the intertrochanteric line. Disruption of Shenton's line. | Arthroplasty (Hemi or THA) preferred in the elderly due to high nonunion/AVN rates. ORIF reserved for young patients. |
| Extracapsular Intertrochanteric Fracture | Severe pain, significant ecchymosis often present. Limb markedly shortened and externally rotated. | Fracture line extends between the greater and lesser trochanters. Extracapsular. | Osteosynthesis is the gold standard (Cephalomedullary nail or Sliding Hip Screw). Arthroplasty is rarely indicated. |
| Subtrochanteric Femur Fracture | Thigh pain, inability to bear weight. Deformity driven by proximal fragment flexion/abduction. | Fracture line located within 5 cm distal to the lesser trochanter. | Intramedullary nailing (long cephalomedullary nail) is the standard of care. High mechanical failure risk with plates. |
| Pathological Proximal Femur Fracture | Prodromal pain prior to the fall. History of malignancy. Disproportionate pain. | Lytic or blastic lesions. Cortical thinning. "Moth-eaten" appearance. | Requires oncologic workup. Often requires longer stemmed arthroplasty, cemented fixation, or prophylactic stabilization of the entire femur. |
| Occult Femoral Neck Fracture | Groin pain with weight-bearing. Minimal to no gross deformity. Normal initial X-rays. | Normal plain films. MRI reveals bone marrow edema and a distinct fracture line. | In situ fixation with cannulated screws to prevent displacement, regardless of age. |
In this clinical scenario, the radiographic evidence definitively confirmed a displaced intracapsular femoral neck fracture, ruling out extracapsular variants and pathological etiologies based on the absence of lytic lesions and the classic traumatic mechanism.
Surgical Decision Making and Classification
The management of femoral neck fractures is dictated by patient age, functional demand, cognitive status, and the anatomic characteristics of the fracture. The two primary classification systems utilized are the Garden classification and the Pauwels classification.
Classification Analysis
The Garden classification assesses the degree of displacement on the AP radiograph:
* Type I: Incomplete or valgus impacted.
* Type II: Complete fracture, non-displaced.
* Type III: Complete fracture, partially displaced (trabecular lines of the femoral head do not align with the acetabulum).
* Type IV: Complete fracture, fully displaced (femoral head rotates back to a neutral position within the acetabulum, completely disconnected from the neck).
This patient presented with a Garden IV fracture. The blood supply to the femoral head, primarily derived from the medial femoral circumflex artery via the retinacular vessels, is almost certainly disrupted in Garden III and IV fractures. This high probability of vascular compromise leads to unacceptable rates of avascular necrosis (AVN) and nonunion if internal fixation is attempted in the elderly population.
The Pauwels classification evaluates the angle of the fracture line relative to the horizontal plane:
* Type I: < 30 degrees (compressive forces dominate).
* Type II: 30-50 degrees.
* Type III: > 50 degrees (shear forces dominate).
This patient's Pauwels III fracture pattern (>70 degrees) further contraindicates internal fixation. High shear forces lead to varus collapse and implant cutout, even in younger patients with excellent bone stock. Therefore, joint replacement is the definitive treatment pathway.
Arthroplasty Selection Total Hip vs Hemiarthroplasty
Once arthroplasty is chosen, the surgeon must decide between a hemiarthroplasty and a total hip arthroplasty (THA).
Hemiarthroplasty is generally reserved for patients with lower functional demands, significant cognitive impairment, or a limited life expectancy. It carries a lower risk of dislocation and requires less surgical time. However, it is associated with long-term complications such as acetabular wear, groin pain, and inferior functional outcomes in active patients.
Total Hip Arthroplasty is the gold standard for active, independent, lucid elderly patients with displaced femoral neck fractures. Large-scale randomized controlled trials, such as the HEALTH trial, have demonstrated that THA provides superior functional outcomes, less residual pain, and lower rates of revision surgery compared to hemiarthroplasty in this specific demographic. Given this patient's independent living status, lack of cognitive impairment, and active lifestyle, THA was the clear choice.
The Rationale for a Hybrid Construct
The term "Hybrid Primary Hip Arthroplasty" refers to the use of an uncemented (press-fit) acetabular component combined with a cemented femoral stem.
- Uncemented Acetabular Component: In the absence of severe acetabular osteoporosis or prior radiation, uncemented cups provide excellent long-term biologic fixation. They allow for the use of highly cross-linked polyethylene liners and larger femoral heads, which optimize the head-to-neck ratio and maximize the jump distance, thereby reducing the risk of postoperative dislocation.
- Cemented Femoral Stem: The use of cemented femoral stems in the elderly trauma population is strongly supported by contemporary orthopedic literature. The WHiTE 3 trial and various national joint registry data have conclusively shown that uncemented stems in elderly patients with Dorr B or C bone (osteopenic/osteoporotic) carry a significantly higher risk of intraoperative and early postoperative periprosthetic femoral fractures. Cemented stems provide immediate, rigid fixation, bypassing the need for biologic ingrowth, and distribute stress more evenly across the weakened proximal femur.
Therefore, a hybrid construct offers the optimal balance: minimizing the risk of periprosthetic femoral fracture while maximizing the longevity and stability of the acetabular reconstruction.

Surgical Technique and Intervention
The patient was medically optimized and cleared for surgery within 24 hours of admission, adhering to the standard of care for geriatric hip fractures to minimize mortality and morbidity associated with prolonged recumbency.
Patient Positioning and Anesthesia
The patient was brought to the operating theater and administered spinal anesthesia. Regional anesthesia is often preferred in this demographic to reduce postoperative delirium, minimize blood loss, and avoid the hemodynamic fluctuations associated with general anesthesia.
The patient was positioned in the lateral decubitus position on the operating table. Rigid pelvic fixation was achieved using a peg board system, ensuring the pelvis was perfectly orthogonal to the floor. This positioning is critical; any unrecognized pelvic tilt or roll can lead to malpositioning of the acetabular component, resulting in a high risk of impingement and dislocation. All bony prominences were meticulously padded.
Surgical Approach and Exposure
A standard posterior approach to the hip (Moore/Southern approach) was utilized. This approach offers excellent visualization of both the acetabulum and the proximal femur and is highly versatile for trauma arthroplasty.
An incision was made centered over the greater trochanter, extending proximally and posteriorly in line with the fibers of the gluteus maximus, and distally along the femoral shaft. The fascia lata was incised, and the gluteus maximus was split bluntly in line with its fibers. A Charnley retractor was placed to maintain exposure.
The short external rotators (piriformis, superior gemellus, obturator internus, inferior gemellus) and the quadratus femoris were identified. The sciatic nerve was palpated and protected throughout the procedure. A robust, full-thickness tenotomy of the short external rotators and the posterior capsule was performed, tagging the tissue with heavy non-absorbable sutures for later repair. This enhanced capsular repair is vital for restoring posterior soft-tissue tension and preventing dislocation.

The hip was dislocated with gentle internal rotation. The femoral head, which was completely detached from the neck due to the Garden IV fracture, was extracted using a corkscrew. The femoral head was measured to confirm the templated size and then sent to pathology. The femoral neck was resected at the templated level using an oscillating saw, referencing the distance from the lesser trochanter.
Acetabular Preparation and Component Implantation
Exposure of the acetabulum was achieved by placing a superior pin in the ilium, an anterior retractor over the anterior wall, and an inferior retractor clearing the transverse acetabular ligament. The labrum and any obstructing osteophytes were excised to fully visualize the true acetabular floor and the teardrop.
Sequential reaming of the acetabulum was performed, starting with a small reamer and increasing in 1mm increments. Reaming was directed medially to the true floor, then expanded peripherally to achieve a bleeding subchondral bone bed. The goal is to achieve a hemispherical construct that allows for a 1-2mm press-fit of the uncemented cup.
Once the appropriate size was reached, a highly porous, titanium-coated hemispherical cup was impacted into place. The target orientation was 40-45 degrees of inclination and 15-20 degrees of anteversion. Excellent primary stability was achieved via the equatorial press-fit. Two cancellous screws were placed in the postero-superior quadrant (the safe zone) to augment initial fixation. A highly cross-linked polyethylene liner was then impacted into the shell.
Femoral Preparation and Cementing Technique
Attention was then turned to the femur. The proximal femur was elevated and externally rotated. The femoral canal was entered using a box osteotome, taking care to lateralize the entry point into the greater trochanter to avoid varus malpositioning of the stem.
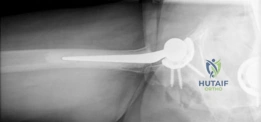
The canal was sequentially broached using a collarless, polished, double-tapered stem system. In a cemented technique, the broach size determines the size of the cement mantle, not the press-fit of the stem. A line-to-line broaching technique was used to allow for a uniform 2mm cement mantle.
Modern, third-generation cementing techniques are mandatory to ensure long-term survivorship and minimize the risk of Bone Cement Implantation Syndrome (BCIS). The steps performed included:
1. Canal Preparation: The intramedullary canal was aggressively brushed to remove loose cancellous bone and marrow fat.
2. Pulsatile Lavage: High-pressure pulsatile lavage was used to thoroughly irrigate the canal, removing debris and exposing the cancellous bone interstices for optimal cement interdigitation.
3. Drying and Packing: The canal was dried using a sponge soaked in dilute epinephrine to minimize bleeding, followed by packing with dry laparotomy sponges.
4. Cement Restrictor: A distal intramedullary cement restrictor (plug) was sized and inserted 1-2 cm distal to the planned tip of the stem. This prevents distal migration of the cement and allows for effective pressurization.
5. Cement Mixing and Delivery: Polymethyl methacrylate (PMMA) bone cement was mixed under vacuum to reduce porosity and increase fatigue strength. Once the cement reached the doughy phase, it was injected into the canal in a retrograde fashion using a cement gun, starting from the restrictor and withdrawing the nozzle as the canal filled.
6. Pressurization: A proximal seal was applied, and the cement was pressurized to force it into the cancellous bone micro-architecture.
7. Stem Insertion: The polished, double-tapered stem was inserted in the correct version (approximately 10-15 degrees of anteversion) and held rigidly until the cement fully polymerized.

Trialing and Biomechanical Optimization
Prior to cementing the final stem, trial reductions were performed using the broach and trial heads. The goals of trialing are to assess stability, restore leg length, and optimize soft tissue tension (offset).
- Shuck Test: Traction is applied to the leg. Less than 2-3mm of distraction indicates adequate soft tissue tension.
- Impingement Testing: The hip is taken through a full range of motion. Flexion to 90 degrees with internal rotation assesses for anterior impingement and posterior instability. Extension with external rotation assesses for posterior impingement and anterior instability.
- Leg Length Assessment: The relationship of the knees and heels was checked, and the distance from the greater trochanter to the center of the head was compared to the preoperative template.
Following final stem cementation, the definitive femoral head (typically a 32mm or 36mm ceramic or cobalt-chrome head, depending on the cup size) was impacted onto the trunnion. The hip was reduced, and final stability checks were performed.
Closure and Soft Tissue Reconstruction
Thorough irrigation was performed to remove any third-body wear particles or residual cement debris. The posterior capsule and the short external rotators were meticulously repaired through transosseous drill holes in the greater trochanter. This
Clinical & Radiographic Imaging