Adult Reconstructive Of The Hip And Review | Dr Hutaif - ...
14 Apr 2026
59 min read
112 Views
Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Adult Reconstructive Of The Hip And Review | ...
00:00
Start Quiz
Question 1High Yield
What is the single most important nutritional factor affecting athletic performance?
Explanation
Maintenance of adequate hydration is the single most important factor affecting athletic performance. While carbohydrate loading may be beneficial for some endurance athletes, the consumption of carbohydrates during exercise does not appear to be beneficial for athletes engaged in events that last less than 1 hour. In general, athletes consuming a balanced diet do not need electrolyte supplementation.
REFERENCES: Maughan RJ, Noakes TD: Fluid replacement and exercise stress: A brief review of studies on fluid replacement and some guidelines for the athlete. Sports Med 1991;12:16-31.
Barr SI, Costill DL, Fink WJ: Fluid replacement during prolonged exercise: Effects of water, saline, or no fluid. Med Sci Sports Exerc 1991;23:811-817.
REFERENCES: Maughan RJ, Noakes TD: Fluid replacement and exercise stress: A brief review of studies on fluid replacement and some guidelines for the athlete. Sports Med 1991;12:16-31.
Barr SI, Costill DL, Fink WJ: Fluid replacement during prolonged exercise: Effects of water, saline, or no fluid. Med Sci Sports Exerc 1991;23:811-817.
Question 2High Yield
Figure 80a
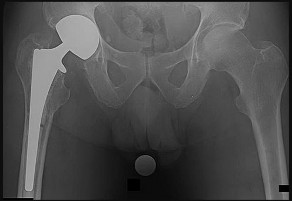
Explanation
- Loose cemented stem_
Question 3High Yield
During the course of a revision total knee arthroplasty via a medial parapatellar exposure, the surgeon does a complete intra-articular release and synovectomy but exposure is still inadequate. A quadriceps snip is performed and, at the end of the procedure, the knee is stable throughout a range of motion and the postoperative radiographs show acceptable alignment of the components. The patient’s postoperative physical therapy regimen should include which of the following?


Explanation
**DISCUSSION** : A quadriceps snip is performed by extending a medial parapatellar approach superiorly and laterally across the quadriceps tendon. It is then repaired primarily at the end of the procedure. The primary advantage of this technique over other surgical maneuvers that improve exposure at the time of revision total knee arthroplasty is that the postoperative regimen for physical therapy does not need to be altered.
**
**DISCUSSION** : A quadriceps snip is performed by extending a medial parapatellar approach superiorly and laterally across the quadriceps tendon. It is then repaired primarily at the end of the procedure. The primary advantage of this technique over other surgical maneuvers that improve exposure at the time of revision total knee arthroplasty is that the postoperative regimen for physical therapy does not need to be altered.
**
Scientific References
- : Younger AS, Duncan CP, Masri BA: Surgical exposures in revision total knee arthroplasty. J Am Acad Orthop Surg 1998;6:55-64.
Della Valle CJ, Berger RA, Rosenberg AG: Surgical exposures in revision total knee arthroplasty. Clin Orthop Relat Res 2006;446:59-68.
Barrack RL, Smith P, Munn B, et al: The Ranawat Award. Comparison of surgical approaches in total knee
arthroplasty. Clin Orthop Relat Res 1998;356:16-21.
Question 2
A healthy 72-year-old woman is seen 14 days after cemented total knee arthroplasty. She reports increasing pain and swelling for the last 4 days accompanied by 4 days of wound drainage. Examination reveals that she is afebrile, and has erythema and moderate serosanguinous drainage from the wound. The knee is moderately swollen. Aspiration of the knee reveals no organisms on Gram stain. Culture results are expected back in 48 hours. Optimal management should consist of
1. ### initiation of a first-generation cephalosporin while awaiting culture results.
2. ### initiation of broad-spectrum antibiotics while awaiting culture results.
3. ### ultrasound to evaluate for fluid collection around the knee.
4. ### surgical debridement of the knee before culture results are available.
5. ### inpatient observation and no antibiotics until culture results are available.
PREFERRED RESPONSE: 4**
**DISCUSSION** : Increased pain, swelling, erythema, and drainage 2 weeks removed from the primary arthroplasty are all signs of a probable infection. Erythrocyte sedimentation rate and C-reactive protein may not be helpful as they are elevated postoperatively even in the absence of infection. Even in the absence of infection, persistent wound drainage is an indication for surgical debridement to prevent subsequent infection. When a postoperative infection is easily recognized by clinical examination, there is no need to wait for a positive culture before proceeding with debridement.
REFERENCES: Weiss AP, Krackow KA: Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty 1993;8:285-289.
Jaberi FM, Parvizi J, Haytmanek CT, et al: Procrastination of wound drainage and malnutrition affect the outcome of joint arthroplasty. Clin Orthop Relat Res 2008;466:1368-1371.
Insall JN, Windsor RE, Scott, WN: Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 959-964.
Figure 3a Figure 3b
Question 4High Yield
A 40-year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years
ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. What is the most appropriate management of this condition?
ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. What is the most appropriate management of this condition?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross- sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 5High Yield
The structure at highest risk for injury in total hip arthroplasty (THA) is the:
Explanation
The external iliaCartery and vein are immobile and lie close to the pelvis, and thus are at high risk for injury in THA. The external iliaCvein lies within 7 mm of the anterior column of the pelvis at the anterior inferior iliaCspine and within 4 mm at the acetabula dome. The external iliaCartery is at less risk due to its thicker intima and increased distance from the bone. The external iliaCartery lies within 10 mm of the bone at the anterior inferior iliaCspine and within 7 mm at the acetabular dome. The common femoral artery lies anterior and medial to the hip capsule. Only the iliopsoas lies between the vessel and capsule at this point. The femoral vein lies medial to the artery and is not likely to be injured. The obturator vessels are also at risk, lying fixed within 1 mm of the bony surface at the quadrilateral surface, with their only protection being the interposition of the obturator internus muscle
Question 6High Yield
Figures 27a and 27b are the radiographs of a 2-month-old with a swollen ankle and abdominal bruising.
Explanation
- Plain radiographs
Question 7High Yield
Figure 1 is the CT scan of a 12-month-old boy who has a neck injury from a motor vehicle accident. He is neurologically intact without any other injuries. Following successful closed reduction of the fracture, what is the best next step in management?

Explanation
■
The patient has sustained a displaced odontoid fracture through the dentocentral synchondrosis. Reduction of the fracture can usually be achieved by extending the neck under fluoroscopic control. An irreducible fracture may be successfully reduced by transoral digital manipulation. After closed reduction, immobilization in a Minerva cast, halo cast, or halo vest are good options.
A cervical collar will not adequately immobilize the upper cervical spine to maintain reduction of an unstable odontoid fracture. Anterior odontoid fixation or posterior C1-C2 instrumented arthrodesis should be reserved for irreducible fractures or a rare pediatric odontoid fracture nonunion.
The patient has sustained a displaced odontoid fracture through the dentocentral synchondrosis. Reduction of the fracture can usually be achieved by extending the neck under fluoroscopic control. An irreducible fracture may be successfully reduced by transoral digital manipulation. After closed reduction, immobilization in a Minerva cast, halo cast, or halo vest are good options.
A cervical collar will not adequately immobilize the upper cervical spine to maintain reduction of an unstable odontoid fracture. Anterior odontoid fixation or posterior C1-C2 instrumented arthrodesis should be reserved for irreducible fractures or a rare pediatric odontoid fracture nonunion.
Question 8High Yield
Which of the following is the seating arrangement recommended for a 5-year-old in a family automobile:
Explanation
C hildren ages 4 to 8 (40 lbs to 60 lbs) are at risk for airbag injuries and should not be in the front seat. In addition, they require booster seats to allow proper fitting of the shoulder harness on the upper torso. Rear-facing seats are only appropriate for infants. C hildren should not be in the front seat until after age 12 and over 100 lbs.
Question 9High Yield
**CLINICAL SITUATION**
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
How is syndesmotic reduction best assessed intra-operatively?
---
Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight.
How is syndesmotic reduction best assessed intra-operatively?
---

Explanation
The radiographs reveal a trimalleolar ankle fracture dislocation with an associated distal tibiofibular syndesmotic disruption. Medial and lateral malleolar stabilization are consistently agreed upon. The decision to stabilize the posterior
malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
9. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
10. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
11. Maximizes the surface area for ankle joint loading
12. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
malleolus is more controversial. Posterior malleolar stabilization accomplishes the following:
9. Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
10. Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
11. Maximizes the surface area for ankle joint loading
12. Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
Question 10High Yield
Figure 1 is the sagittal MR image of a 56-year-old woman who has a 3-year history of severe back pain. Her pain is worse with flexion at the lumbosacral junction and is relieved with extension. She denies any pain in her lower extremities and has no symptoms of neurogenic claudication. Which mediators play roles in the pathogenesis of this condition?

Explanation
■
The patient has degenerative disk disease with diskogenic back pain. Several studies in both humans and animals have implicated TNF-α, IL-1, and MMP in extracellular matrix degeneration and disk degradation. TGF-β, BMP-2, latent membrane protein 1, and growth and development factor-5 are all postulated to play anabolic roles in the intervertebral disk. Biglycan is a small leucine-rich proteoglycan that regulates extracellular matrix assembly within the disk. Noggin and gremlin are biochemical factors not involved in disk degradation.
The patient has degenerative disk disease with diskogenic back pain. Several studies in both humans and animals have implicated TNF-α, IL-1, and MMP in extracellular matrix degeneration and disk degradation. TGF-β, BMP-2, latent membrane protein 1, and growth and development factor-5 are all postulated to play anabolic roles in the intervertebral disk. Biglycan is a small leucine-rich proteoglycan that regulates extracellular matrix assembly within the disk. Noggin and gremlin are biochemical factors not involved in disk degradation.
Question 11High Yield
ORTHO MCQS RECON019
**Adult Reconstructive Surgery of the Hip and Knee Scored and**
**Recorded Self-Assessment Examination 2019**
**Question 1**
What factor is associated with a higher risk of dislocation after total hip arthroplasty?
**Adult Reconstructive Surgery of the Hip and Knee Scored and**
**Recorded Self-Assessment Examination 2019**
**Question 1**
What factor is associated with a higher risk of dislocation after total hip arthroplasty?






Explanation
**
DISCUSSION:**
Dislocation after total hip arthroplasty is a multifactorial problem. Numerous risk factors may act independently or cumulatively to increase the risk of this complication. Previous hip surgery of any kind is associated with a twofold increased risk for dislocation. Other risk factors include female gender, impaired mental status, inflammatory arthritis, and older age. Numerous studies have shown a lower dislocation rate with a direct lateral approach, although surgical techniques such as capsular repair have significantly lowered the incidence of dislocation after using the posterior approach. Metal-on-metal bearings have been associated with other complications such as adverse tissue reactions but are often used with larger-diameter bearings, which pose a lower risk of dislocation.
**Question 2**
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which
test(s) best correlate with a prognosis if this patient is having a reaction to metal debris?
A. Erythrocyte sedimentation rate, C-reactive protein, and white blood cell count
B. Serum cobalt and chromium ion levels
C. MRI with metal artifact reduction sequence (MARS) D. CT of pelvis
**CORRECT ANSWER: C DISCUSSION:**
Painful MOM THA and taper corrosion can cause substantial damage to a patient's hip if left untreated. In this case, the workup for a painful MOM THA starts the same as a workup for a painful metal-on- polyethylene bearing couple. Infection must be ruled out in every case with a set of inflammatory markers. If these markers are remotely elevated, this is an indication for joint aspiration. In patients with metal debris, the pathology report often indicates too many cells to count or cellular debris. Metal ion levels do not seem to correlate with prognosis. There are well-functioning patients with high ion levels and poor- functioning patients with low ion levels. Advanced imaging with MARS MRI to evaluate for peritrochanteric fluid collection, a soft-tissue mass, or synovial/capsular hypertrophy will reveal signs of a metal reaction that indicate the need for a revision discussion. A CT scan can show more advanced bony destruction as an indicator of poor prognosis. These films can be used to determine the need for a structural graft or augments for reconstruction of bone loss attributable to metal debris.
**Question 3**
**Figures** **below** **demonstrate** **the** **radiographs** **obtained** **from** **a** **35-year-old** **woman** **with** **end-stage**
**debilitating** **osteoarthritis** **of** **the** **right** **hip.** **She** **is** **contemplating** **total** **hip** **arthroplasty** **(THA).** **She** **has** **a history** **of** **right** **hip** **dysplasia** **and** **underwent** **hip** **osteotomy** **as** **an** **adolescent.** **Over** **the** **years,** **nonsurgical treatment,** **including** **weight** **loss,** **activity** **modifications,** **and** **intra-articular** **injections,** **has** **failed.** **Her infection** **work-up** **reveals** **laboratory** **findings** **within** **defined** **limits.** **A** **further** **work-up** **reveals** **elevations in** **serum** **cobalt** **and** **chromium** **levels** **and** **fluid** **collections** **surrounding** **the** **hip** **on** **MRI** **with** **MARS. Revision** **THA** **is** **recommended.** **The** **most** **common** **complication** **following** **revision** **of** **a** **failed** **metal-on- metal** **hip** **arthroplasty** **is**
**A.** **infection. B.** **instability. C.** **loosening.**
D. periprosthetic fracture.
**CORRECT ANSWER: B DISCUSSION:**
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on- metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child- bearing age. The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cellcounts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
**Question 4**
Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with a
2-month history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?
A. Pain during sitting; flexion abduction and external rotation of the hip
B. Groin pain; pain with internal rotation and adduction while supine with the hip and knee flexed 90°
C. Clicking; abductor lurch
D. Buttock pain; pain with hip extension, adduction, and external rotation while prone
**CORRECT ANSWER: B DISCUSSION:**
MRI reveals an anterior labral tear, and the radiograph shows minimal arthritis with possible dysplasia. The most common location of pain in patients with a labral tear is the groin, and the most common physical finding is a positive impingement test result. Pain during sitting, clicking, and buttock pain are frequently described by patients with a labral tear, but these symptoms are less common than groin pain. A positive posterior impingement test finding is more common in patients with a posterior labral tear. Although age over 40 years and a body mass index higher than 30 can adversely affect clinical outcomes after joint preservation procedures such as PAO, hip arthroscopy, and femoral acetabular impingement surgery, the presence of hip arthritis on presurgical radiographs is the most commonly mentioned cause of failed hip joint preservation surgery. Tönnis grade is a radiographic measure of hip arthritis. A higher Outerbridge score is associated with more frequent poor outcomes after hip arthroscopy; however, the Outerbridge cartilage score is determined by direct visualization at the time of surgery. The Outerbridge score cannot be determined presurgically.
**Question 5**
**Figures** **1** **and** **2** **demonstrate** **the** **radiographs** **obtained** **from** **a** **35-year-old** **woman** **with** **end-stage**
**debilitating** **osteoarthritis** **of** **the** **right** **hip.** **She** **is** **contemplating** **total** **hip** **arthroplasty** **(THA).** **She** **has** **a history** **of** **right** **hip** **dysplasia** **and** **underwent** **hip** **osteotomy** **as** **an** **adolescent.** **Over** **the** **years,** **nonsurgical treatment,** **including** **weight** **loss,** **activity** **modifications,** **and** **intra-articular** **injections,** **has** **failed.** **Her infection** **work-up** **reveals** **laboratory** **findings** **within** **defined** **limits.The** **patient** **undergoes** **successful primary** **THA** **with** **a** **metal-on-metal** **bearing.** **At** **1-year** **follow-up,** **she** **reports** **no** **pain** **and** **is** **highly satisfied** **with** **the** **procedure.** **However,** **3** **years** **after** **the** **index** **procedure,** **she** **reports** **atraumatic** **right** **hip pain** **that** **worsens** **with** **activities.** **Radiographs** **reveal** **the** **implants** **in** **good** **position** **with** **no** **sign** **of loosening** **or** **lysis.** **An** **initial** **laboratory** **evaluation** **reveals** **a** **normal** **sedimentation** **rate** **and** **C-reactive protein** **(CRP)** **level.** **The** **most** **appropriate** **next** **diagnostic** **step** **is**
**A.** **MRI** **with** **metal** **artifact** **reduction** **sequence** **(MARS)** **only. B.** **serum** **cobalt** **only.**
**C.** **serum** **cobalt** **and** **chromium** **levels.**
D. serum cobalt and chromium levels and MRI with MARS.
**CORRECT ANSWER: D**
**DISCUSSION:**
THA has proven to be durable and reliable for pain relief and improvement of function in patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A
metal-on-metal articulation is associated with excellent wear rates in vitro. Because it offers a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions—including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis after the possible transfer of metal ions across the placental barrier—make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.The work-up of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including the erythrocyte sedimentation rate, C-reactive protein (CRP) level, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging, including MRI with MARS, should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following a revision of failed metal-on-metal hip replacements.
**Question 6**
**A** **59-year-old** **woman** **with** **a** **history** **of** **osteoporosis** **is** **involved** **in** **a** **high-speed** **motor** **vehicle** **accident,**
**resulting** **in** **left** **hip** **pain** **and** **deformity.** **The** **initial** **radiograph** **from** **the** **trauma** **bay** **is** **shown** **in** **Figure** **1/. Postreduction** **CT** **is** **shown** **in** **Figures** **2** **through** **4.** **What** **is** **the** **most** **appropriate** **definitive** **surgical treatment?**
**A.** **Open** **reduction** **and** **internal** **fixation** **(ORIF)** **of** **the** **acetabular** **fracture** **with** **concomitant** **acute total** **hip** **arthroplasty**
**B.** **ORIF** **of** **the** **acetabular** **fracture** **and** **ORIF** **of** **the** **femoral** **head** **fracture** **fragments**
**C.** **ORIF** **of** **the** **acetabular** **fracture** **and** **hemiarthroplasty**
D. Skeletal traction with delayed total hip arthroplasty after the acetabular fracture has healed
**CORRECT ANSWER: A**
**DISCUSSION:**
The radiograph shows a posterior wall acetabular fracture-dislocation. Post reduction CT indicates a large comminuted posterior wall fracture with marginal impaction of the articular surface. A comminuted femoral head fracture also is seen extending to the superior weight-bearing surface. Given the marginal
impaction of the acetabulum and the considerable comminution of the femoral head (which is likely unreconstructible), this injury would have a high risk of causing posttraumatic arthritis if treated with ORIF of the fractures alone. Considering this fact and the patient’s age, ORIF of the posterior wall and acute total hip arthroplasty would likely have the best functional result and the lowest risk of reoperation. Hemiarthroplasty is inappropriate for this injury considering the acetabular fracture. Skeletal traction currently plays a limited role in the definitive treatment of acetabular fractures.
**Question 7**
**Figures** **below** **show** **the** **radiographs,** **MRI,** **and** **MR** **arthrogram** **obtained** **from** **a** **25-year-old** **collegiate**
**soccer** **player** **who** **has** **new-onset** **left** **groin** **pain.** **He** **played** **competitive** **soccer** **from** **a** **young** **age** **and** **has competed** **or** **practiced** **5** **to** **6** **times** **per** **week** **since** **the** **age** **of** **10.** **He** **denies** **any** **specific** **hip** **injury** **that necessitated** **treatment,** **but** **his** **trainer** **contends** **that** **he** **had** **a** **groin** **pull.** **He** **reports** **groin** **pain** **with** **passive flexion** **and** **internal** **rotation** **of** **the** **left** **hip,** **and** **his** **hip** **has** **less** **internal** **rotation** **than** **his** **asymptomatic right** **hip.** **He** **is** **otherwise** **healthy.** **What** **is** **the** **primary** **cause** **of** **a** **cam** **deformity?**
A. **A** **genetic** **problem**
B. **Repetitive** **activities** **involving** **an** **open** **proximal** **femoral** **physis**
C. **Early** **closure** **of** **the** **proximal** **femoral** **physis**
D. Hip dysplasia
**CORRECT ANSWER: B DISCUSSION:**
Multiple studies have confirmed that cam or pincer anatomy is commonly present in asymptomatic hips. According to a large systematic review, cam deformities are present in approximately one-third of asymptomatic hips in young adults, and the proportion is higher than 50% in the subgroup of athletes. Ganz and associates proposed that femoral acetabular impingement is the root cause of osteoarthritis in most nontraumatic, nondysplastic hips, and functional improvement with surgical correction of the deformity has been demonstrated. Despite the link between cam deformity and hip osteoarthritis, a corresponding link between the correction of the deformity and prevention of osteoarthritis has never been proven. The results of cam deformity correction, typically including repair of the degenerative labral tear, are much poorer when substantial joint space loss is present. A typical joint space cutoff of 2 mm or less is used to recommend against hip preservation surgery.
**Question 8**
**Figures**
Adult Reconstructive Surgery of the Hip and Knee Scored and
Recorded Self-Assessment Examination 2019
DISCUSSION:**
Dislocation after total hip arthroplasty is a multifactorial problem. Numerous risk factors may act independently or cumulatively to increase the risk of this complication. Previous hip surgery of any kind is associated with a twofold increased risk for dislocation. Other risk factors include female gender, impaired mental status, inflammatory arthritis, and older age. Numerous studies have shown a lower dislocation rate with a direct lateral approach, although surgical techniques such as capsular repair have significantly lowered the incidence of dislocation after using the posterior approach. Metal-on-metal bearings have been associated with other complications such as adverse tissue reactions but are often used with larger-diameter bearings, which pose a lower risk of dislocation.
**Question 2**
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which
test(s) best correlate with a prognosis if this patient is having a reaction to metal debris?
A. Erythrocyte sedimentation rate, C-reactive protein, and white blood cell count
B. Serum cobalt and chromium ion levels
C. MRI with metal artifact reduction sequence (MARS) D. CT of pelvis
**CORRECT ANSWER: C DISCUSSION:**
Painful MOM THA and taper corrosion can cause substantial damage to a patient's hip if left untreated. In this case, the workup for a painful MOM THA starts the same as a workup for a painful metal-on- polyethylene bearing couple. Infection must be ruled out in every case with a set of inflammatory markers. If these markers are remotely elevated, this is an indication for joint aspiration. In patients with metal debris, the pathology report often indicates too many cells to count or cellular debris. Metal ion levels do not seem to correlate with prognosis. There are well-functioning patients with high ion levels and poor- functioning patients with low ion levels. Advanced imaging with MARS MRI to evaluate for peritrochanteric fluid collection, a soft-tissue mass, or synovial/capsular hypertrophy will reveal signs of a metal reaction that indicate the need for a revision discussion. A CT scan can show more advanced bony destruction as an indicator of poor prognosis. These films can be used to determine the need for a structural graft or augments for reconstruction of bone loss attributable to metal debris.
**Question 3**
**Figures** **below** **demonstrate** **the** **radiographs** **obtained** **from** **a** **35-year-old** **woman** **with** **end-stage**
**debilitating** **osteoarthritis** **of** **the** **right** **hip.** **She** **is** **contemplating** **total** **hip** **arthroplasty** **(THA).** **She** **has** **a history** **of** **right** **hip** **dysplasia** **and** **underwent** **hip** **osteotomy** **as** **an** **adolescent.** **Over** **the** **years,** **nonsurgical treatment,** **including** **weight** **loss,** **activity** **modifications,** **and** **intra-articular** **injections,** **has** **failed.** **Her infection** **work-up** **reveals** **laboratory** **findings** **within** **defined** **limits.** **A** **further** **work-up** **reveals** **elevations in** **serum** **cobalt** **and** **chromium** **levels** **and** **fluid** **collections** **surrounding** **the** **hip** **on** **MRI** **with** **MARS. Revision** **THA** **is** **recommended.** **The** **most** **common** **complication** **following** **revision** **of** **a** **failed** **metal-on- metal** **hip** **arthroplasty** **is**
**A.** **infection. B.** **instability. C.** **loosening.**
D. periprosthetic fracture.
**CORRECT ANSWER: B DISCUSSION:**
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on- metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child- bearing age. The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cellcounts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
**Question 4**
Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with a
2-month history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?
A. Pain during sitting; flexion abduction and external rotation of the hip
B. Groin pain; pain with internal rotation and adduction while supine with the hip and knee flexed 90°
C. Clicking; abductor lurch
D. Buttock pain; pain with hip extension, adduction, and external rotation while prone
**CORRECT ANSWER: B DISCUSSION:**
MRI reveals an anterior labral tear, and the radiograph shows minimal arthritis with possible dysplasia. The most common location of pain in patients with a labral tear is the groin, and the most common physical finding is a positive impingement test result. Pain during sitting, clicking, and buttock pain are frequently described by patients with a labral tear, but these symptoms are less common than groin pain. A positive posterior impingement test finding is more common in patients with a posterior labral tear. Although age over 40 years and a body mass index higher than 30 can adversely affect clinical outcomes after joint preservation procedures such as PAO, hip arthroscopy, and femoral acetabular impingement surgery, the presence of hip arthritis on presurgical radiographs is the most commonly mentioned cause of failed hip joint preservation surgery. Tönnis grade is a radiographic measure of hip arthritis. A higher Outerbridge score is associated with more frequent poor outcomes after hip arthroscopy; however, the Outerbridge cartilage score is determined by direct visualization at the time of surgery. The Outerbridge score cannot be determined presurgically.
**Question 5**
**Figures** **1** **and** **2** **demonstrate** **the** **radiographs** **obtained** **from** **a** **35-year-old** **woman** **with** **end-stage**
**debilitating** **osteoarthritis** **of** **the** **right** **hip.** **She** **is** **contemplating** **total** **hip** **arthroplasty** **(THA).** **She** **has** **a history** **of** **right** **hip** **dysplasia** **and** **underwent** **hip** **osteotomy** **as** **an** **adolescent.** **Over** **the** **years,** **nonsurgical treatment,** **including** **weight** **loss,** **activity** **modifications,** **and** **intra-articular** **injections,** **has** **failed.** **Her infection** **work-up** **reveals** **laboratory** **findings** **within** **defined** **limits.The** **patient** **undergoes** **successful primary** **THA** **with** **a** **metal-on-metal** **bearing.** **At** **1-year** **follow-up,** **she** **reports** **no** **pain** **and** **is** **highly satisfied** **with** **the** **procedure.** **However,** **3** **years** **after** **the** **index** **procedure,** **she** **reports** **atraumatic** **right** **hip pain** **that** **worsens** **with** **activities.** **Radiographs** **reveal** **the** **implants** **in** **good** **position** **with** **no** **sign** **of loosening** **or** **lysis.** **An** **initial** **laboratory** **evaluation** **reveals** **a** **normal** **sedimentation** **rate** **and** **C-reactive protein** **(CRP)** **level.** **The** **most** **appropriate** **next** **diagnostic** **step** **is**
**A.** **MRI** **with** **metal** **artifact** **reduction** **sequence** **(MARS)** **only. B.** **serum** **cobalt** **only.**
**C.** **serum** **cobalt** **and** **chromium** **levels.**
D. serum cobalt and chromium levels and MRI with MARS.
**CORRECT ANSWER: D**
**DISCUSSION:**
THA has proven to be durable and reliable for pain relief and improvement of function in patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A
metal-on-metal articulation is associated with excellent wear rates in vitro. Because it offers a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions—including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis after the possible transfer of metal ions across the placental barrier—make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.The work-up of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including the erythrocyte sedimentation rate, C-reactive protein (CRP) level, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging, including MRI with MARS, should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following a revision of failed metal-on-metal hip replacements.
**Question 6**
**A** **59-year-old** **woman** **with** **a** **history** **of** **osteoporosis** **is** **involved** **in** **a** **high-speed** **motor** **vehicle** **accident,**
**resulting** **in** **left** **hip** **pain** **and** **deformity.** **The** **initial** **radiograph** **from** **the** **trauma** **bay** **is** **shown** **in** **Figure** **1/. Postreduction** **CT** **is** **shown** **in** **Figures** **2** **through** **4.** **What** **is** **the** **most** **appropriate** **definitive** **surgical treatment?**
**A.** **Open** **reduction** **and** **internal** **fixation** **(ORIF)** **of** **the** **acetabular** **fracture** **with** **concomitant** **acute total** **hip** **arthroplasty**
**B.** **ORIF** **of** **the** **acetabular** **fracture** **and** **ORIF** **of** **the** **femoral** **head** **fracture** **fragments**
**C.** **ORIF** **of** **the** **acetabular** **fracture** **and** **hemiarthroplasty**
D. Skeletal traction with delayed total hip arthroplasty after the acetabular fracture has healed
**CORRECT ANSWER: A**
**DISCUSSION:**
The radiograph shows a posterior wall acetabular fracture-dislocation. Post reduction CT indicates a large comminuted posterior wall fracture with marginal impaction of the articular surface. A comminuted femoral head fracture also is seen extending to the superior weight-bearing surface. Given the marginal
impaction of the acetabulum and the considerable comminution of the femoral head (which is likely unreconstructible), this injury would have a high risk of causing posttraumatic arthritis if treated with ORIF of the fractures alone. Considering this fact and the patient’s age, ORIF of the posterior wall and acute total hip arthroplasty would likely have the best functional result and the lowest risk of reoperation. Hemiarthroplasty is inappropriate for this injury considering the acetabular fracture. Skeletal traction currently plays a limited role in the definitive treatment of acetabular fractures.
**Question 7**
**Figures** **below** **show** **the** **radiographs,** **MRI,** **and** **MR** **arthrogram** **obtained** **from** **a** **25-year-old** **collegiate**
**soccer** **player** **who** **has** **new-onset** **left** **groin** **pain.** **He** **played** **competitive** **soccer** **from** **a** **young** **age** **and** **has competed** **or** **practiced** **5** **to** **6** **times** **per** **week** **since** **the** **age** **of** **10.** **He** **denies** **any** **specific** **hip** **injury** **that necessitated** **treatment,** **but** **his** **trainer** **contends** **that** **he** **had** **a** **groin** **pull.** **He** **reports** **groin** **pain** **with** **passive flexion** **and** **internal** **rotation** **of** **the** **left** **hip,** **and** **his** **hip** **has** **less** **internal** **rotation** **than** **his** **asymptomatic right** **hip.** **He** **is** **otherwise** **healthy.** **What** **is** **the** **primary** **cause** **of** **a** **cam** **deformity?**
A. **A** **genetic** **problem**
B. **Repetitive** **activities** **involving** **an** **open** **proximal** **femoral** **physis**
C. **Early** **closure** **of** **the** **proximal** **femoral** **physis**
D. Hip dysplasia
**CORRECT ANSWER: B DISCUSSION:**
Multiple studies have confirmed that cam or pincer anatomy is commonly present in asymptomatic hips. According to a large systematic review, cam deformities are present in approximately one-third of asymptomatic hips in young adults, and the proportion is higher than 50% in the subgroup of athletes. Ganz and associates proposed that femoral acetabular impingement is the root cause of osteoarthritis in most nontraumatic, nondysplastic hips, and functional improvement with surgical correction of the deformity has been demonstrated. Despite the link between cam deformity and hip osteoarthritis, a corresponding link between the correction of the deformity and prevention of osteoarthritis has never been proven. The results of cam deformity correction, typically including repair of the degenerative labral tear, are much poorer when substantial joint space loss is present. A typical joint space cutoff of 2 mm or less is used to recommend against hip preservation surgery.
**Question 8**
**Figures**
Adult Reconstructive Surgery of the Hip and Knee Scored and
Recorded Self-Assessment Examination 2019
Question 12High Yield
A 17-year-old high school football player sustains a traumatic anterior shoulder dislocation, resulting in a small bony Bankart lesion and small Hill-Sachs lesion. The patient undergoes an arthroscopic Bankart repair with incorporation of the bone fragment and returns to play football the following year. He has a recurrent dislocation at football practice but decides to finish the football season before considering additional treatment. He sustains nine additional dislocations, with the last dislocation occurring while sleeping.What diagnostic test is most appropriate when planning revision surgery?
Explanation
DISCUSSION
A failed bony Bankart repair with multiple dislocations can further erode the anteroinferior glenoid, changing the sagittal morphology of the glenoid into an “inverted pear.” Quantitative bone loss is best evaluated by CT scan with 3-D reconstructions and subtraction of the humeral head. MRI and ultrasonography can assist in evaluating soft-tissue injury, but they are not as helpful in determining bone loss compared with a CT scan. An arthrogram alone is not sufficient to evaluate bone loss. Bone loss >30% necessitates glenoid augmentation with either a Latarjet procedure or iliac crest bone grafting. A revision arthroscopic or open Bankart repair with capsular shift or remplissage do not address bone loss. The Latarjet procedure can effectively restore stability with glenoid bone loss and after failed stabilizing procedures. Patients with pain before surgery are
more likely to have pain after surgery. Age and activity level are lesser influences on satisfaction.
DISCUSSION
A failed bony Bankart repair with multiple dislocations can further erode the anteroinferior glenoid, changing the sagittal morphology of the glenoid into an “inverted pear.” Quantitative bone loss is best evaluated by CT scan with 3-D reconstructions and subtraction of the humeral head. MRI and ultrasonography can assist in evaluating soft-tissue injury, but they are not as helpful in determining bone loss compared with a CT scan. An arthrogram alone is not sufficient to evaluate bone loss. Bone loss >30% necessitates glenoid augmentation with either a Latarjet procedure or iliac crest bone grafting. A revision arthroscopic or open Bankart repair with capsular shift or remplissage do not address bone loss. The Latarjet procedure can effectively restore stability with glenoid bone loss and after failed stabilizing procedures. Patients with pain before surgery are
more likely to have pain after surgery. Age and activity level are lesser influences on satisfaction.
Question 13High Yield
1236) Which of the following structures is at risk during proximal dissection of a single lateral perifibular approach for compartment syndrome of the leg?
Explanation
The perifibular approach is carried out through a straight lateral incision beginning just posterior and parallel to the fibula from the fibular head to the tip of the lateral malleolus. At the proximal end of the incision, the common peroneal nerve must be identified and protected. Elevation of the soleus off the posterior fibula ensures proper deep compartment release. The anterior edge of the incision is then retracted to expose the anterior and lateral compartments, and at this point, care must be taken to avoid the superficial
peroneal nerve as it exits the fascia of the lateral compartment and runs anteriorly in the distal third of the leg.
The referenced article by Whitesides is a review of compartment syndrome pathology, diagnosis, and treatment.
peroneal nerve as it exits the fascia of the lateral compartment and runs anteriorly in the distal third of the leg.
The referenced article by Whitesides is a review of compartment syndrome pathology, diagnosis, and treatment.
Question 14High Yield
A 37-year-old woman has had intermittent paresthesias and numbness in the plantar foot for the past 6 months. She reports that the symptoms are worse with activity, and the paresthesias are beginning to awaken her at night. MRI scans are shown in Figures 6a and 6b. What is the most likely diagnosis?
Explanation
The symptoms are consistent with tarsal tunnel syndrome. Ganglion cysts are a well-known cause of tarsal tunnel syndrome. The MRI scans show a high intensity, well-circumscribed mass in the tarsal tunnel that is consistent with a fluid-filled cyst. Patients usually respond well to excision of the ganglion and resolution of the tarsal tunnel symptoms. The surrounding fat is a different signal intensity on the MRI scans, which rules out a lipoma. Synovial cell sarcoma has a heterogeneous appearance on an MRI scan. Metastatic tumors are most commonly found in the osseous structures of the foot, not the soft tissues.
REFERENCES: Rozbruch SR, Chang V, Bohne WH, et al: Ganglion cysts of the lower extremity: An analysis of 54 cases and review of the literature. Orthopedics 1998;21:141-148.
Llauger J, Palmer J, Monill JM, et al: MR imaging of benign soft-tissue masses of the foot and ankle. Radiographics 1998;18:1481-1498.
Takakura Y, Kitada C, Sugimoto K, et al: Tarsal tunnel syndrome: Causes and results of operative treatment. J Bone Joint Surg Br 1991;73:125-128.
REFERENCES: Rozbruch SR, Chang V, Bohne WH, et al: Ganglion cysts of the lower extremity: An analysis of 54 cases and review of the literature. Orthopedics 1998;21:141-148.
Llauger J, Palmer J, Monill JM, et al: MR imaging of benign soft-tissue masses of the foot and ankle. Radiographics 1998;18:1481-1498.
Takakura Y, Kitada C, Sugimoto K, et al: Tarsal tunnel syndrome: Causes and results of operative treatment. J Bone Joint Surg Br 1991;73:125-128.
Question 15High Yield
A 36-year-old softball player sustains a shoulder dislocation making a diving catch. The shoulder is successfully reduced in the emergency department. A postreduction MRI is shown in Figure 35. What anatomic lesion is a result of the dislocation?
Explanation
DISCUSSION: The MRI scan reveals a HAGL lesion. It more commonly affects older patients and is associated with more violent trauma.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 53-54.
Bokor DJ, Conboy VB, Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the
glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br 1999;81:93-96. Question 36
An 18-year-old woman injures her left knee playing soccer. At the time of anterior cruciate ligament (ACL) reconstruction, she was noted to have an irreparable posterior horn medial meniscus tear. Partial meniscectomy will have what primary effect?
1. #### Increase medial compartment peak loads
2. #### Increase medial compartment contact area
3. #### Decrease in situ forces in the ACL graft
4. #### Decrease anterior tibial translation
5. #### Increase posterior tibial translation PREFERRED RESPONSE: 1
DISCUSSION: The medial meniscus distributes force through the medial compartment. Peak loads in the affected compartment are increased by partial and complete meniscectomy. The posterior horn of the medial meniscus is also an important secondary restraint to anterior tibial translation in the ACL-deficient knee. In situ forces in the reconstructed ACL are increased with loss of the posterior horn of the medial meniscus.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 199-201.
Greis PE, Bardana DD, Holmstrom MC, et al: Meniscal injury: I. Basic science and evaluation. J Am Acad Orthop Surg 2002; 10:168-176.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 53-54.
Bokor DJ, Conboy VB, Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the
glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br 1999;81:93-96. Question 36
An 18-year-old woman injures her left knee playing soccer. At the time of anterior cruciate ligament (ACL) reconstruction, she was noted to have an irreparable posterior horn medial meniscus tear. Partial meniscectomy will have what primary effect?
1. #### Increase medial compartment peak loads
2. #### Increase medial compartment contact area
3. #### Decrease in situ forces in the ACL graft
4. #### Decrease anterior tibial translation
5. #### Increase posterior tibial translation PREFERRED RESPONSE: 1
DISCUSSION: The medial meniscus distributes force through the medial compartment. Peak loads in the affected compartment are increased by partial and complete meniscectomy. The posterior horn of the medial meniscus is also an important secondary restraint to anterior tibial translation in the ACL-deficient knee. In situ forces in the reconstructed ACL are increased with loss of the posterior horn of the medial meniscus.
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 199-201.
Greis PE, Bardana DD, Holmstrom MC, et al: Meniscal injury: I. Basic science and evaluation. J Am Acad Orthop Surg 2002; 10:168-176.
Question 16High Yield
When comparing surgical and nonsurgical extremities in patients who underwent anterior cruciate ligament (ACL) reconstruction using patellar tendon or hamstrings autografts, isokinetic strength measurements obtained 6 months after the surgery would most
likely reveal **
likely reveal **
Explanation
Follow-up examination at 6 months revealed no statistically significant differences in quadricep or hamstring strength when comparing surgical versus nonsurgical extremities isokinetically. Therefore, the selection of autogenous hamstring or patellar tendon for ACL reconstruction should not be based solely on the assumption of the graft tissue source altering the recovery of quadricep and/or hamstring strength.
REFERENCES: Carter TR, Edinger S: Isokinetic evaluation of anterior cruciate ligament reconstruction: Hamstring versus patellar tendon. Arthroscopy 1999;15:169-172
Howell SM, Taylor MA: Brace-free rehabilitation, with early return to activity, for knees reconstructed with a double-looped semitendinosus and gracilis graft. J Bone Joint Surg Am 1996;78:814-825.
Shelbourne KD, Nitz P: Accelerated rehabilitation after anterior cruciate ligament reconstruction. Am J Sports Med 1990;18:292-299.
REFERENCES: Carter TR, Edinger S: Isokinetic evaluation of anterior cruciate ligament reconstruction: Hamstring versus patellar tendon. Arthroscopy 1999;15:169-172
Howell SM, Taylor MA: Brace-free rehabilitation, with early return to activity, for knees reconstructed with a double-looped semitendinosus and gracilis graft. J Bone Joint Surg Am 1996;78:814-825.
Shelbourne KD, Nitz P: Accelerated rehabilitation after anterior cruciate ligament reconstruction. Am J Sports Med 1990;18:292-299.
Question 17High Yield
Examination of a 10-year-old girl with a hypoplastic breast and atrophic pectoralis major may also reveal which of the following findings?
Explanation
Poland’s syndrome has four main features: 1) short digits as the result of absence or shortening of the middle phalanx; 2) syndactyly of the short digits usually consisting of a simple, complete type; 3) hypoplasia of the hand and forearm; and 4) absence of the sternocostal head of the pectoralis major on the same side.
REFERENCES: Wilson MR, Louis DS, Stevenson TR: Poland’s syndrome: Variable expression and associated anomalies. J Hand Surg 1988;13:880-882.
Poland A: Deficiency of the pectoralis muscle. Guys Hosp Rep 1841;6:191.
REFERENCES: Wilson MR, Louis DS, Stevenson TR: Poland’s syndrome: Variable expression and associated anomalies. J Hand Surg 1988;13:880-882.
Poland A: Deficiency of the pectoralis muscle. Guys Hosp Rep 1841;6:191.
Question 18High Yield
A 5-year-old boy had a 1-week history of left hip pain and a limp that resolved 5 weeks prior to his office visit. Examination demonstrates a pain-free and symmetric range of motion. A radiograph is seen in Figure 42. What is the next step in management?
Explanation
DISCUSSION: Whereas bilateral Perthes of the hips occurs in 11% of cases, in patients with symmetric changes/stages, other diagnoses must be considered such as Meyers dysplasia. Multiple epiphyseal dysplasia is most _A_ r _L_ e _-_ a _M_ d _a_ il _d_ y _en_ d _a_ ia _C_ g _o_ n _p_ o _y_ sed by evaluation of other radiographs, in particular of the knee and, if confirmatory, of the
**2010 Pediatric Orthopaedic Examination Answer Book • 37**
spine to assess for spondyloepiphyseal dysplasia.
REFERENCES: Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 806-810.
Hesse B, Kohler G: Does it always have to be Perthes’ disease? What is epiphyseal dysplasia? Clin Orthop Relat
Res 2003;414:219-227.
**2010 Pediatric Orthopaedic Examination Answer Book • 37**
spine to assess for spondyloepiphyseal dysplasia.
REFERENCES: Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 806-810.
Hesse B, Kohler G: Does it always have to be Perthes’ disease? What is epiphyseal dysplasia? Clin Orthop Relat
Res 2003;414:219-227.
Question 19High Yield
_AL-Madena Copy_
A 220-lb high school basketball player injured his knee while landing after a rebound. Figure 61 shows a lateral view of the knee. This fracture is associated with which of the following complications?
A 220-lb high school basketball player injured his knee while landing after a rebound. Figure 61 shows a lateral view of the knee. This fracture is associated with which of the following complications?
Explanation
There is a high incidence of compartment syndrome seen in type III tibial tubercle fractures. Fasciotomy should be considered at the time of initial repair. Type III tibial tubercle fractures extending through the joint are often associated with meniscal injuries, which must be repaired. Delayed complications included recurvatum and refracture. Its association with Osgood-Schlatter’s disease has not been proven. This is a fracture that occurs in later adolescence, so significant limb-length discrepencies are unusual after this fracture.
REFERENCES: Ogden JA, Tross RB, Murphy MJ: Fracture of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
Sponseller PE, Beaty JH: Fractures and dislocations about the knee, in Rockwood CA, Wilkins KE,
Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott Raven, 1996, pp 1273-1281.
REFERENCES: Ogden JA, Tross RB, Murphy MJ: Fracture of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
Sponseller PE, Beaty JH: Fractures and dislocations about the knee, in Rockwood CA, Wilkins KE,
Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott Raven, 1996, pp 1273-1281.
Question 20High Yield
Slide 1 Slide 2 Slide 3
A patient with diabetes and severe peripheral neuropathy has been treated for a C harcot ankle deformity for 9 months (Slide 1, Slide 2, and Slide 3). An ankle foot orthosis has been used for 4 months. No skin breakdown occurred in the brace. Swelling is present but has decreased over the past month. Ankle range of motion is limited, and crepitus is present upon examination of the ankle. Which surgical procedure is most consistent with the future treatment of this patient:
A patient with diabetes and severe peripheral neuropathy has been treated for a C harcot ankle deformity for 9 months (Slide 1, Slide 2, and Slide 3). An ankle foot orthosis has been used for 4 months. No skin breakdown occurred in the brace. Swelling is present but has decreased over the past month. Ankle range of motion is limited, and crepitus is present upon examination of the ankle. Which surgical procedure is most consistent with the future treatment of this patient:
Explanation
The indication for surgery is intractable deformity, which is refractory to all forms of bracing. By refractory, one implies that skin breakdown or imminent infection is present. If surgery were performed, then it would consist of a tibiotalocalcaneal arthrodesis. There are no indications for this surgery in this patient. Once the neuropathic process has reached a stable point, a deformity is not likely to progress.
Question 21High Yield
An 8-year-old girl with a history of Down syndrome is being evaluated to participate in gym activities. She is otherwise doing well and has appropriate motor developmental milestones. Her neurological exam is normal and cervical spine AP, lateral, flexion and extension radiographs reveal an atlanto-dens interval (ADI) of 7 mm, and normal occipitoatlantal mobility. What is the most appropriate recommendation?
Explanation
■
Down syndrome, with an incidence of 1 in 660 live births, remains the most common human malformation pattern. Individuals with Down syndrome have an increased incidence of congenital heart disease, ophthalmologic disorders, gastrointestinal disorders, thyroid disease, and leukemia.
Musculoskeletal problems commonly occur in Down syndrome and include patellofemoral and hip instability, bunions, severe flatfoot, and instability of cervical spine, which could result in cord compromise and neurological impairment or death.
Increased ADI in the Down syndrome population has not been directly correlated with a concomitant increase in neurologic compromise. The radiographs of the cervical spine in the Down syndrome population must be evaluated by standards specific to that population, and not by traditional standards derived from the radiographs of the cervical spine in the general population. Radiographic evaluation of the cervical spine in the young athlete with Down syndrome is only one component of the preparticipation screening and must be correlated with a pertinent history of physical activity and a detailed physical exam.
When a Down patient presents with an ADI >10 mm and evidence of spinal cord compression, there is little disagreement about the need for surgical intervention. When the ADI is between 4.5 mm and 10 mm in a patient with no decrease in physical activities and no abnormal neurological finding, this may represent hypermobility rather than instability in the Down syndrome population. With an ADI between 4.5 mm and 10 mm, athletes with Down syndrome may participate in most activities but have been advised to avoid high-risk sports such as diving and football.
Down syndrome, with an incidence of 1 in 660 live births, remains the most common human malformation pattern. Individuals with Down syndrome have an increased incidence of congenital heart disease, ophthalmologic disorders, gastrointestinal disorders, thyroid disease, and leukemia.
Musculoskeletal problems commonly occur in Down syndrome and include patellofemoral and hip instability, bunions, severe flatfoot, and instability of cervical spine, which could result in cord compromise and neurological impairment or death.
Increased ADI in the Down syndrome population has not been directly correlated with a concomitant increase in neurologic compromise. The radiographs of the cervical spine in the Down syndrome population must be evaluated by standards specific to that population, and not by traditional standards derived from the radiographs of the cervical spine in the general population. Radiographic evaluation of the cervical spine in the young athlete with Down syndrome is only one component of the preparticipation screening and must be correlated with a pertinent history of physical activity and a detailed physical exam.
When a Down patient presents with an ADI >10 mm and evidence of spinal cord compression, there is little disagreement about the need for surgical intervention. When the ADI is between 4.5 mm and 10 mm in a patient with no decrease in physical activities and no abnormal neurological finding, this may represent hypermobility rather than instability in the Down syndrome population. With an ADI between 4.5 mm and 10 mm, athletes with Down syndrome may participate in most activities but have been advised to avoid high-risk sports such as diving and football.
Question 22High Yield
A 25-year-old professional baseball pitcher reports a 4-month history of gradually increasing medial elbow pain that occurs during the late cocking and acceleration phases of throwing. The pain occasionally refers distally along the ulnar aspect of the forearm. He denies any weakness; however, he notes occasional paresthesias. A nerve conduction velocity study demonstrates increased latency across the cubital tunnel. Management consisting of 6 weeks of rest and rehabilitation fails to provide relief as the symptoms returned when he resumed throwing. What is the best course of action?
Explanation
In the thrower’s elbow, ulnar neuritis is felt to result from both chronic compression and traction on the nerve that occurs during the throwing motion. Occasionally, subluxation of the nerve also can lead to symptoms. If nonsurgical management fails to provide relief, transposition of the nerve to an anterior subcutaneous location is the surgical procedure of choice. The nerve is held in its new position by one or two fascial slings created from the fascia of the common flexor origin.
REFERENCES: Schickendantz MS: Diagnosis and treatment of elbow disorders in the overhead athlete. Hand Clin 2002;18:65-75.
Eaton RG, Crowe JF, Parkes JC III: Anterior transposition of the ulnar nerve using a non-compressing fasciodermal sling. J Bone Joint Surg Am 1980;62:820-825.
REFERENCES: Schickendantz MS: Diagnosis and treatment of elbow disorders in the overhead athlete. Hand Clin 2002;18:65-75.
Eaton RG, Crowe JF, Parkes JC III: Anterior transposition of the ulnar nerve using a non-compressing fasciodermal sling. J Bone Joint Surg Am 1980;62:820-825.
Question 23High Yield
The greatest amount of step-off that is well-tolerated in a Bennettâs fracture is:
Explanation
Studies by Livesley, Kjaer-Petersen, and others have shown that patients with fractures with more than a 1-mm step-off after reduction were more likely to develop arthritis at the thumb carpometacarpal joint. Although some studies have not shown functional outcome correlating with the presence of arthritis, Oosterbos and De Boer found that all their patients with fair and poor overall results had nonanatomic reductions. Although a cadaveric study by C ullen has shown that a 2-mm step-off may be acceptable, this contrasts with the clinical evidence currently available.
Question 24High Yield
..What is the most appropriate treatment if instability is present at the time of evaluation?

Explanation
- Soft-tissue interposition arthroplasty PREFERRED RESPONSE: 1- TEA
Question 25High Yield
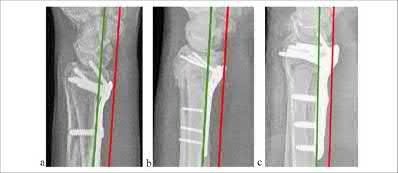
A 57-year-old woman underwent open reduction internal fixation from a volar approach for a displaced distal radius fracture. Immediate
post-operative radiographs are seen in Figure A. The patient recovered well initially but presents after 6 months with grip weakness. What complication is most likely to occur in this patient?
post-operative radiographs are seen in Figure A. The patient recovered well initially but presents after 6 months with grip weakness. What complication is most likely to occur in this patient?

Explanation
A complication of very distal or prominent volar distal radius plate placement as seen in Figure A is rupture of the flexor pollicis longus (FPL) tendon. This would cause an inability to flex the thumb interphalangeal (IP) joint.
Flexor and extensor pollicis longus ruptures are known complications of distal radius fracture fixation. Volar plate placement distal to the watershed line, or prominence at the volar lip, can result in tendinopathy and eventual rupture of the FPL. With proper plate placement but screws protruding through the dorsal cortex, the extensor tendons are at risk, particularly extensor pollicis longus (EPL). Nonoperative treatment of distal radius fractures is also associated with EPL rupture.
Soong et al. compared flexor tendon ruptures between patients treated with 2 different volar distal radius plate designs. Most notably, they create and use a volar prominence grading system and demonstrate more tendon ruptures with 1 plate design that was more often found to be prominent and distal, suggesting position to contribute to tendon rupture.
Kitay et al. performed a case-control study assessing distal radius volar plate position in patients who did or did not develop flexor tendon ruptures. They found a significant association, reporting that plate position 3.0mm distal to the volar rim or prominence 2.0mm volar to the critical line (Soong grading system) each had an 88% sensitivity for flexor tendon rupture.
Figure A is a lateral radiograph of a distal radius fracture treated with a volar locking plate with distal prominence.
Illustration A shows the Soong classification of distal radius volar plate prominence, displaying the volar critical line as a line parallel to the volar radius shaft drawn tangentially from the most volar part of the distal volar rim (red line). Grade 0 is plate below this line, Grade 1 is plate crossing this line but proximal to volar rim, Grade 2 is plate crossing this line and distal to volar rim.
Incorrect Answers:
Answer 1: This would be rupture of extensor indices or central slip of index finger.
Answer 2: This would be rupture of flexor digitorum superficalis (FDS) to index finger.
Answer 3: This would be rupture of extensor pollicus longus (EPL). Answer 5: This would be rupture of either abductor pollicis brevis (APB) or longus (APL).
Rupture of FPL is more common with distal volar plate placement than the above tendons.
Flexor and extensor pollicis longus ruptures are known complications of distal radius fracture fixation. Volar plate placement distal to the watershed line, or prominence at the volar lip, can result in tendinopathy and eventual rupture of the FPL. With proper plate placement but screws protruding through the dorsal cortex, the extensor tendons are at risk, particularly extensor pollicis longus (EPL). Nonoperative treatment of distal radius fractures is also associated with EPL rupture.
Soong et al. compared flexor tendon ruptures between patients treated with 2 different volar distal radius plate designs. Most notably, they create and use a volar prominence grading system and demonstrate more tendon ruptures with 1 plate design that was more often found to be prominent and distal, suggesting position to contribute to tendon rupture.
Kitay et al. performed a case-control study assessing distal radius volar plate position in patients who did or did not develop flexor tendon ruptures. They found a significant association, reporting that plate position 3.0mm distal to the volar rim or prominence 2.0mm volar to the critical line (Soong grading system) each had an 88% sensitivity for flexor tendon rupture.
Figure A is a lateral radiograph of a distal radius fracture treated with a volar locking plate with distal prominence.
Illustration A shows the Soong classification of distal radius volar plate prominence, displaying the volar critical line as a line parallel to the volar radius shaft drawn tangentially from the most volar part of the distal volar rim (red line). Grade 0 is plate below this line, Grade 1 is plate crossing this line but proximal to volar rim, Grade 2 is plate crossing this line and distal to volar rim.
Incorrect Answers:
Answer 1: This would be rupture of extensor indices or central slip of index finger.
Answer 2: This would be rupture of flexor digitorum superficalis (FDS) to index finger.
Answer 3: This would be rupture of extensor pollicus longus (EPL). Answer 5: This would be rupture of either abductor pollicis brevis (APB) or longus (APL).
Rupture of FPL is more common with distal volar plate placement than the above tendons.
Question 26High Yield
Figure 20 shows the radiograph of a 21-year-old college basketball player who jammed his left index finger on the rim. He reports pain and tenderness over the dorsum of the distal interphalangeal (DIP) joint. Examination reveals that he is unable to actively extend the DIP joint; however, the skin is intact. Management should consist of
Explanation
Mallet fingers without DIP joint subluxation can be treated with extension splinting. Surgical fixation may be necessary in bony mallet injuries when the joint is subluxated. Size of the bony fragment, while often correlating with stability, is not always an indication for fixation. Buddy taping allows motion; therefore, the fragment will not heal in the appropriate position. Intermittent splinting with range-of-motion exercises also will not allow the fragment to heal in the appropriate position.
REFERENCES: Crawford GP: The molded polyethylene splint for mallet finger deformities.
J Hand Surg Am 1984;9:231-237.
Wehbe MA, Schneider LH: Mallet fractures. J Bone Joint Surg Am 1984;66:658-669.
REFERENCES: Crawford GP: The molded polyethylene splint for mallet finger deformities.
J Hand Surg Am 1984;9:231-237.
Wehbe MA, Schneider LH: Mallet fractures. J Bone Joint Surg Am 1984;66:658-669.
Question 27High Yield
A 70-year-old woman has a preoperative anterior interscalene block prior to undergoing a total shoulder arthroplasty. After seating her in the beach chair position, she becomes acutely hypotensive. What is the most likely cause for the hypotension?
Explanation
The beach chair position may cause sudden hypotension and bradycardia as a result of the Bezold-Jarisch reflex. This reflex occurs when venous pooling and increased sympathetic tone induce a low-volume, hypercontractile ventricle, resulting in activation of the parasympathetic nervous system and sympathetic withdrawal. The reported incidence of this phenomenon associated with the sitting position is between 13% to 24%. Left untreated, the result may be cardiac arrest. Pneumothorax or central nervous system toxicity after interscalene block is rare and has an incidence of less than 0.2%. Laryngeal nerve block associated with interscalene nerve block can occur but usually results in hoarseness secondary to ipsilateral vocal cord palsy.
REFERENCES: Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14:546-556.
Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
REFERENCES: Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14:546-556.
Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
Question 28High Yield
A complication associated with using the Morrey approach (triceps reflecting) to implant a semiconstrained total elbow arthroplasty is
Explanation
Numerous approaches can be used to implant a total elbow arthroplasty. The Morrey approach identifies, transposes, and protects the ulnar nerve, and then subperiosteally reflects the triceps off the ulna. The sleeve of tissue is very thin distally, and the triceps need to be meticulously repaired at the time of closure. Implant dislocation and malposition are less likely with an extensile approach, and dislocation is unlikely with a semiconstrained implant. The development of heterotopic ossification is unrelated to the surgical approach used for elbow arthroplasty.
Question 29High Yield
Which of the following phenotypes occurs in patients with achondroplasia:
Explanation
The phenotype of achondroplasia includes: Varus knee deformity
Spinal stenosis
Atlantoaxial instability
The other responses:
Neurofibromatosis: C afé au lait spots, pseudoarthrosis of tibia and scoliosis C harcot-Marie-Tooth disease: C avovarus feet, areflexia, and distal motor wasting Duchenne muscular dystrophy: Proximal muscle weakness and calf hypertrophy Marfanâs syndrome: Dolichostenomelia and scoliosis
C orrect Answer: Knee varus and spinal stenosis
Spinal stenosis
Atlantoaxial instability
The other responses:
Neurofibromatosis: C afé au lait spots, pseudoarthrosis of tibia and scoliosis C harcot-Marie-Tooth disease: C avovarus feet, areflexia, and distal motor wasting Duchenne muscular dystrophy: Proximal muscle weakness and calf hypertrophy Marfanâs syndrome: Dolichostenomelia and scoliosis
C orrect Answer: Knee varus and spinal stenosis
Question 30High Yield
Orthopedic MCQS online Shoulder and Elbow 017
SHOULDER AND ELBOW SELF-
SCORED SELF-ASSESSMENT EXAMINATION
_AAOS 2017_
CLINICAL SITUATION FOR QUESTIONS 1 THROUGH 4
A 55-year-old man falls on his outstretched arm and sustains the injury shown in the 3-dimensional CT scans in Figures 1a and 1b.
Which ligamentous structure attaches to the fracture fragment?
SHOULDER AND ELBOW SELF-
SCORED SELF-ASSESSMENT EXAMINATION
_AAOS 2017_
CLINICAL SITUATION FOR QUESTIONS 1 THROUGH 4
A 55-year-old man falls on his outstretched arm and sustains the injury shown in the 3-dimensional CT scans in Figures 1a and 1b.
Which ligamentous structure attaches to the fracture fragment?









Explanation
Varus posteromedial rotatory instability is a complex injury pattern that starts with varus stress resulting in a fracture of the anteromedial coronoid. The anterior MCL attaches to the sublime tubercle, which is part of the anteromedial coronoid facet. The posterior MCL attaches to the posterior medial aspect of the ulna. The radial collateral and lateral ulnar collateral attach to the ulna at the crista supinatoris. The bony landmark is the sublime tubercle; as noted above, the crista supinatoris is lateral on the ulna. The radial notch is also lateral and is the articulation between the proximal ulna and proximal radius. The anteromedial coronoid facet is part of the coronoid, which extends more lateral and anterior than the anteromedial facet. The anteromedial facet represents the critical weight-bearing portion of the ulnohumeral joint. Damage to this structure causes posteromedial subluxation that often results in severe progressive arthritis. The coronoid is the larger structure of which the anteromedial coronoid facet is a portion. The posteromedial coronoid facet does not appear to be critical in weight bearing. The radial notch is not associated with increased stress with weight bearing. The treatment of displaced fractures of this structure is open reduction and internal fixation utilizing buttress plating. Closed treatment is acceptable only for nondisplaced fractures with appropriate radiographic follow-up. Suture fixation is not advocated because of inadequate strength.
RECOMMENDED READINGS
1. Pollock JW, Brownhill J, Ferreira L, McDonald CP, Johnson J, King G. The effect of anteromedial facet fractures of the coronoid and lateral collateral ligament injury on elbow stability and kinematics. J Bone Joint Surg Am. 2009 Jun;91(6):1448-58. doi: 10.2106/JBJS.H.00222.
2. Sanchez-Sotelo J, O'Driscoll SW, Morrey BF. Anteromedial fracture of the coronoid process of the ulna. J Shoulder Elbow Surg. 2006 Sep-Oct;15(5):e5-8. Epub 2006 Jul 26. Erratum in: J Shoulder Elbow Surg. 2007 Jan-Feb;16(1):127. PubMed PMID: 16979044.
RECOMMENDED READINGS
1. Pollock JW, Brownhill J, Ferreira L, McDonald CP, Johnson J, King G. The effect of anteromedial facet fractures of the coronoid and lateral collateral ligament injury on elbow stability and kinematics. J Bone Joint Surg Am. 2009 Jun;91(6):1448-58. doi: 10.2106/JBJS.H.00222.
2. Sanchez-Sotelo J, O'Driscoll SW, Morrey BF. Anteromedial fracture of the coronoid process of the ulna. J Shoulder Elbow Surg. 2006 Sep-Oct;15(5):e5-8. Epub 2006 Jul 26. Erratum in: J Shoulder Elbow Surg. 2007 Jan-Feb;16(1):127. PubMed PMID: 16979044.
Question 31High Yield
A 30-year-old woman sustains a transverse amputation of the distal phalanx of the index finger, leaving exposed bone. What is the most appropriate management of the soft-tissue defect?
Explanation
V-Y advancement flaps are ideal for fingertip amputations that are transverse or dorsal oblique in nature. Healing by secondary intention is contraindicated with exposed bone. Shortening of exposed bone to allow primary skin closure is a possible alternative, as long as significant shortening of the index finger is avoided. A Moberg flap is useful only for distal amputations of the thumb. The first dorsal metacarpal artery-island pedicled flap uses tissue from the dorsum of the proximal index finger, and is typically used to resurface defects of
the thumb.
REFERENCES: Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Atasoy E, Ioakimidis E, Kasdan ML, et al: Reconstruction of the amputated fingertip with a triangular volar flap: A new surgical procedure. J Bone Joint Surg Am 1970;52:921-926.
the thumb.
REFERENCES: Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Atasoy E, Ioakimidis E, Kasdan ML, et al: Reconstruction of the amputated fingertip with a triangular volar flap: A new surgical procedure. J Bone Joint Surg Am 1970;52:921-926.
Question 32High Yield
A right-handed 44-year-old construction worker reports pain and limited range of motion in his right elbow that has limited his ability to work for the past year. Examination reveals range of motion from 60 to 90 degrees, and he has pain at the extremes of flexion and extension. Pronation and supination are minimally restricted. Anti-inflammatory drugs have failed to provide relief. A radiograph is shown in Figure 8. Management should now consist of
Explanation
The radiograph reveals primary osteoarthritis of the elbow; therefore, ulnohumeral arthroplasty is the preferred procedure. Patients with severely limited preoperative elbow extension of more than 60 degrees and flexion of less than 100 degrees are at risk for ulnar nerve dysfunction postoperatively and should undergo a concomitant ulnar nerve decompression. Nonsurgical methods are unlikely to improve his chronic condition. Elbow arthroplasty is contraindicated for patients in this age group and with this diagnosis.
REFERENCES: Antuna SA, Morrey BF, Adams RA, et al: Ulnohumeral arthroplasty for primary degenerative arthritis of the elbow: Long-term outcome and complications. J Bone Joint Surg Am 2002;84:2168-2173.
Phillips NJ, Ali A, Stanley D: Treatment of primary degenerative arthritis of the elbow by ulnohumeral arthroplasty: A long-term follow-up. J Bone Joint Surg Br 2003;85:347-350.
REFERENCES: Antuna SA, Morrey BF, Adams RA, et al: Ulnohumeral arthroplasty for primary degenerative arthritis of the elbow: Long-term outcome and complications. J Bone Joint Surg Am 2002;84:2168-2173.
Phillips NJ, Ali A, Stanley D: Treatment of primary degenerative arthritis of the elbow by ulnohumeral arthroplasty: A long-term follow-up. J Bone Joint Surg Br 2003;85:347-350.
Question 33High Yield
Surgical repair of the injury shown in the MRI scans in Figures 1 through 4 through a single-incision approach has a higher incidence of
33
33
Explanation
The MRI scans show a distal biceps tendon avulsion with significant retraction. When addressing these injuries, a single-incision approach has been associated with an increased risk of lateral antebrachial cutaneous nerve injury. A two-incision approach has been associated with an increased risk of heterotopic ossification, second surgeries and posterior interosseous nerve injury.
34
34
Question 34High Yield
Figure 1
The radiograph of a 22-year-old woman with ankle pain and instability is presented. She has noted this problem for 10 years, and it appears to be worsening. The opposite ankle is not symptomatic. She has not had any previous treatment for foot or ankle problems. The cause of this ankle deformity is most likely to be associated with which of the following conditions:
The radiograph of a 22-year-old woman with ankle pain and instability is presented. She has noted this problem for 10 years, and it appears to be worsening. The opposite ankle is not symptomatic. She has not had any previous treatment for foot or ankle problems. The cause of this ankle deformity is most likely to be associated with which of the following conditions:
Explanation
This patient has a ball and socket ankle, which results from limited motion of the hindfoot during early childhood, either from extensive tarsal coalition, premature hindfoot arthrodesis, or trauma. The condition most commonly associated with a ball and socket ankle is a form of hemimelia of the fibula with lateral ray deficiencies and associated tarsal coalition of which the latter is usually extensive.
Question 35High Yield
1232) A 34-year-old male presents with elbow pain after sustaining a ground level fall 2 weeks ago. An injury radiograph is shown in Figure
A. Which of the following provocative maneuvers will most likely be positive?
A. Which of the following provocative maneuvers will most likely be positive?



Explanation
Figure A demonstrates a fracture of the anteromedial coronoid. Patients with this injury pattern will have feelings of instability with the gravity-assisted varus stress test.
Varus posteromedial rotatory instability (VPMRI) of the elbow is caused by a varus and posteromedial rotation force, resulting in rupture of the lateral collateral ligament (LCL) from its humeral origin. The medial coronoid process is subsequently forced against the medial trochlea, which results in fracture of the anteromedial portion. The most sensitive test is the gravity-assisted varus stress test. The arm is abducted to 90° and the patient is asked to flex and extend the elbow. The test is positive for pain, grinding, or instability during range of motion, as the ulnohumeral joint is closed medially by the lack of the buttress from the anteromedial coronoid. Treatment involves surgically addressing the anteromedial facet of the coronoid and repairing the LCL.
Steinmann performed a review of coronoid process fractures. He reports that with an anteromedial coronoid fracture, the anteroposterior (AP) radiograph of the elbow will demonstrate progressive narrowing of the joint space from lateral to medial. They conclude that an important determinant of stability is the involvement of the sublime tubercle (insertion point of the MCL). When the sublime tubercle is involved, medial elbow instability is likely.
Doornberg et al. performed a retrospective review of coronoid fracture patterns. They found that large fractures of the coronoid were involved with anterior and posterior olecranon fracture/dislocations, small transverse fractures were involved with terrible triad injuries, and anteromedial facet fractures were associated with VPMRI.
Doornberg et al. performed a retrospective review of patients with fracture of the anteromedial facet of the coronoid. They report that if the fracture is not specifically treated, patients ultimately developed arthrosis. They report that the coronoid fracture may be secured with a plate, screw, or sutures. They conclude that secure fixation of the coronoid usually restores good elbow function.
Figure A is an AP radiograph of the elbow demonstrating a fracture of the anteromedial facet of the coronoid. Illustration A is a fluoroscopic stress view demonstrating ulnohumeral instability due to an associated LCL injury.
Illustration B is an AP radiograph demonstrating plate and screw fixation of the coronoid and suture anchor repair of the LCL.
Incorrect Answers:
Answer 1: The lateral pivot shift test is performed with the patient supine with the affected arm overhead. The forearm is supinated and valgus stress is applied while flexing the elbow. Subluxation constitutes a positive finding and is seen in valgus posterolateral rotatory instability of the elbow.
Answer 2: The milking maneuver is performed by creating valgus stress by pulling the patient's thumb with the forearm supinated and elbow flexed to 90°. Subluxation constitutes a positive finding and is seen in valgus posterolateral rotatory instability of the elbow.
Answer 3: The chair rise test is performed by asking the patient to push off from a seated position in a chair. Subluxation when transitioning to elbow extension constitutes a positive finding and is seen in valgus posterolateral rotatory instability of the elbow.
Answer 4: The posterior drawer test is performed with the patient in a seated position with the elbow flexed to 90°. The clinician stabilizes the humerus and gives a superior and inferior force to the forearm. Subluxation constitutes a
positive finding and is seen in valgus posterolateral rotatory instability of the elbow.
Varus posteromedial rotatory instability (VPMRI) of the elbow is caused by a varus and posteromedial rotation force, resulting in rupture of the lateral collateral ligament (LCL) from its humeral origin. The medial coronoid process is subsequently forced against the medial trochlea, which results in fracture of the anteromedial portion. The most sensitive test is the gravity-assisted varus stress test. The arm is abducted to 90° and the patient is asked to flex and extend the elbow. The test is positive for pain, grinding, or instability during range of motion, as the ulnohumeral joint is closed medially by the lack of the buttress from the anteromedial coronoid. Treatment involves surgically addressing the anteromedial facet of the coronoid and repairing the LCL.
Steinmann performed a review of coronoid process fractures. He reports that with an anteromedial coronoid fracture, the anteroposterior (AP) radiograph of the elbow will demonstrate progressive narrowing of the joint space from lateral to medial. They conclude that an important determinant of stability is the involvement of the sublime tubercle (insertion point of the MCL). When the sublime tubercle is involved, medial elbow instability is likely.
Doornberg et al. performed a retrospective review of coronoid fracture patterns. They found that large fractures of the coronoid were involved with anterior and posterior olecranon fracture/dislocations, small transverse fractures were involved with terrible triad injuries, and anteromedial facet fractures were associated with VPMRI.
Doornberg et al. performed a retrospective review of patients with fracture of the anteromedial facet of the coronoid. They report that if the fracture is not specifically treated, patients ultimately developed arthrosis. They report that the coronoid fracture may be secured with a plate, screw, or sutures. They conclude that secure fixation of the coronoid usually restores good elbow function.
Figure A is an AP radiograph of the elbow demonstrating a fracture of the anteromedial facet of the coronoid. Illustration A is a fluoroscopic stress view demonstrating ulnohumeral instability due to an associated LCL injury.
Illustration B is an AP radiograph demonstrating plate and screw fixation of the coronoid and suture anchor repair of the LCL.
Incorrect Answers:
Answer 1: The lateral pivot shift test is performed with the patient supine with the affected arm overhead. The forearm is supinated and valgus stress is applied while flexing the elbow. Subluxation constitutes a positive finding and is seen in valgus posterolateral rotatory instability of the elbow.
Answer 2: The milking maneuver is performed by creating valgus stress by pulling the patient's thumb with the forearm supinated and elbow flexed to 90°. Subluxation constitutes a positive finding and is seen in valgus posterolateral rotatory instability of the elbow.
Answer 3: The chair rise test is performed by asking the patient to push off from a seated position in a chair. Subluxation when transitioning to elbow extension constitutes a positive finding and is seen in valgus posterolateral rotatory instability of the elbow.
Answer 4: The posterior drawer test is performed with the patient in a seated position with the elbow flexed to 90°. The clinician stabilizes the humerus and gives a superior and inferior force to the forearm. Subluxation constitutes a
positive finding and is seen in valgus posterolateral rotatory instability of the elbow.
Question 36High Yield
The peroneus brevis is the primary antagonist to which of the following structures?
Explanation
The primary function of the peroneus brevis is eversion of the foot, thus acting as the primary antagonist of the posterior tibialis, which inverts the foot, and secondarily plantar flexes the ankle.The anterior tibialis secondarily inverts the foot and only acts as a partial antagonist of the posterior tibialis. The peroneus longus plantar flexes the first ray.
Question 37High Yield
A patient with a history of rheumatoid arthritis reports a painful total hip arthroplasty 3 years after the index procedure. Radiographs reveal loosening of the femoral component. Preoperative blood work shows an erythrocyte sedimentation rate (ESR) of 38 mm/h (normal 0-29 mm/h) and a C-reactive protein (CRP) of 8.9 (0.2- 8.0). What is the most appropriate action at this time?

Explanation
DISCUSSION: The question centers on the appropriate work-up for a failed total hip arthroplasty prior to revision surgery. The preoperative ESR is elevated and the CRP is at the upper end of normal. If either the ESR or CRP is elevated, further investigations are required to exclude infection as a cause of loosening, particularly in a patient only 3 years after the index procedure. A technetium scan alone is nonspecific and will show increased uptake because of the loose femoral component. An intraoperative frozen section is a helpful confirmatory investigation, but whenever possible the diagnosis should be made preoperatively to allow for appropriate surgical planning. Recently, investigators have shown the value of FDG-PET scanning as a useful investigation for diagnosing infection; however, it is no more accurate than the combined use of an ESR and CRP, and does not allow for identification of an infecting organism. At this point, a hip aspiration for culture is the most appropriate investigation.
REFERENCES: Bauer TW, Parvizi J, Kobayashi N, et al: Diagnosis of periprosthetic infection. J Bone Joint Surg Am 2006;88:869-882.
Pill SG, Parvizi J, Tang PH, et al: Comparison of fiuorodeoxyglucose positron emission tomography and (111
)indium-white blood cell imaging in the diagnosis of periprosthetic infection of the hip. J Arthroplasty 2006;21:91-97.
Spangehl MJ, Masri BA, O’Connell JX, et al: Prospective analysis of preoperative and intraoperative investigations for the diagnosis of infection at the sites of two hundred and two revision total hip arthroplasties. J Bone Joint Surg Am 1999;81:672-683.
Figure 5a Figure 5b
REFERENCES: Bauer TW, Parvizi J, Kobayashi N, et al: Diagnosis of periprosthetic infection. J Bone Joint Surg Am 2006;88:869-882.
Pill SG, Parvizi J, Tang PH, et al: Comparison of fiuorodeoxyglucose positron emission tomography and (111
)indium-white blood cell imaging in the diagnosis of periprosthetic infection of the hip. J Arthroplasty 2006;21:91-97.
Spangehl MJ, Masri BA, O’Connell JX, et al: Prospective analysis of preoperative and intraoperative investigations for the diagnosis of infection at the sites of two hundred and two revision total hip arthroplasties. J Bone Joint Surg Am 1999;81:672-683.
Figure 5a Figure 5b
Question 38High Yield
Figures 95a and 95b
Explanation
- Chromosome 17 mutation
Question 39High Yield
Which 2 things generally need to be present for this injury to occur?
Explanation
- Tendinosis and a sudden eccentric contraction_
Question 40High Yield
In total knee arthroplasty, in vitro testing has shown that cross-linking can diminish the rate of
polyethylene wear by 30% to 80%. What other change in material properties is possible when polyethylene is highly cross-linked?
polyethylene wear by 30% to 80%. What other change in material properties is possible when polyethylene is highly cross-linked?
Explanation
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been shown to cause implant failure in the most recent clinical trials, but they remain the most important mechanical issues associated with current material processing methods.
Question 41High Yield
Figure 1 is the radiograph of a 73-year-old woman who had a right hip arthroplasty one year prior. Her BMI is 48. Postoperative radiographs at 6 weeks showed early stem subsidence of 4 mm compared with intraoperative radiographs. The current radiographic findings likely resulted from the
Explanation
24
The observed subsidence in the first 6 weeks indicates lack of initial stability and is likely related to undersizing of the implant at the time of surgery. High BMI has been associated with higher rates of loosening. Based on the other hip, it is unlikely there is mismatch between the metaphysis and diaphysis. The modular neck design has not been associated with higher rates of aseptic loosening.
The observed subsidence in the first 6 weeks indicates lack of initial stability and is likely related to undersizing of the implant at the time of surgery. High BMI has been associated with higher rates of loosening. Based on the other hip, it is unlikely there is mismatch between the metaphysis and diaphysis. The modular neck design has not been associated with higher rates of aseptic loosening.
Question 42High Yield
A 23-year-old collegiate gymnast sustains a rupture of his medial collateral ligament of the elbow when he falls off the parallel bars. On physical examination, he has instability to valgus stress and tenderness along the medial elbow. Radiographs show no fracture. Which component of the medial collateral ligament of the elbow is the dominant restraint to valgus stress?
Explanation
DISCUSSION:
The anterior bundle of the medial collateral ligament is the prime stabilizer against valgus stress. The posterior bundle, which originates on the medial epicondyle and inserts broadly along the medial edge of the trochlea from the sublime tubercle posteriorly, has stress only in elbow flexion. The transverse band, which originates on the posteromedial olecranon and inserts on the sublime tubercle, deepens the trochlea, but neither the band nor the posterior capsule provides significant restraint. The lateral collateral ligament, which originates from the lateral epicondyle and inserts on the crista supinatoris of the ulna, is the prime stabilizer of varus stress and posterolateral rotatory subluxation.
The anterior bundle of the medial collateral ligament is the prime stabilizer against valgus stress. The posterior bundle, which originates on the medial epicondyle and inserts broadly along the medial edge of the trochlea from the sublime tubercle posteriorly, has stress only in elbow flexion. The transverse band, which originates on the posteromedial olecranon and inserts on the sublime tubercle, deepens the trochlea, but neither the band nor the posterior capsule provides significant restraint. The lateral collateral ligament, which originates from the lateral epicondyle and inserts on the crista supinatoris of the ulna, is the prime stabilizer of varus stress and posterolateral rotatory subluxation.
Question 43High Yield
Figures 16a and 16b show the radiographs of a 2-year-old boy who has right arm swelling and pain. He also has multiple scalp lesions and chronic ear pain that has failed to respond to antibiotics. A biopsy specimen is shown in Figure 16c. Figure 16d shows an immunohistochemical stain with CD1a. What is the most likely diagnosis?


Explanation
No detailed explanation provided for this question.
Question 44High Yield
Figures 1 and 2 are the radiographs of an 18-year-old man who had surgery 6 months ago at an outside institution. He is being referred now because he has persistent pain. He is tender over the scaphoid at the snuffbox. What is the most appropriate next imaging step in his pain workup?
---
---
---
---


Explanation
Scaphoid nonunions are difficult to diagnose on plain radiographs, which offer poor reliability when attempting to determine if there is bridging trabeculae crossing the fractures site. CT scans are more useful for diagnosing scaphoid nonunion. When scanned using conventional axial cuts, the slices mayskip through the fracture nonunion site, thereby missing the defect, even with reformats. MR imaging is useful in diagnosing acute scaphoid fractures and has a high sensitivity and diagnostic value for excluding _scaphoid fractures as well. Contrast does not enhance the utility of MR imaging in fracture diagnosis._
Question 45High Yield
The four anatomic sites with highest risk of concomitant pediatric septic arthritis and osteomyelitis are
Explanation
■
The four high-risk sites for concomitant septic arthritis and osteomyelitis in children are the four intraarticular metaphyses: proximal humerus, proximal radius, proximal femur, and distal fibula. Knowledge of these specific anatomic sites can help with index of suspicion for both pathologies in the setting of acute infection. The key to recognizing these anatomic locations enables avoidance of isolated drainage of septic joints, while neglecting drainage of the causative osteomyelitis. Failing to drain the osteomyelitis has a higher likelihood of recurrent septic arthritis.
The four high-risk sites for concomitant septic arthritis and osteomyelitis in children are the four intraarticular metaphyses: proximal humerus, proximal radius, proximal femur, and distal fibula. Knowledge of these specific anatomic sites can help with index of suspicion for both pathologies in the setting of acute infection. The key to recognizing these anatomic locations enables avoidance of isolated drainage of septic joints, while neglecting drainage of the causative osteomyelitis. Failing to drain the osteomyelitis has a higher likelihood of recurrent septic arthritis.
Question 46High Yield
Figure 1
A 63-year-old woman who underwent attempted correction of a hallux valgus deformity 3 years previously presents to the office. She has pain in the hallux from dorsal abutment of the hallux on the shoe. There is no pain in the lesser toes or metatarsals. The recommended procedure to alleviate the irritation of the hallux is:
A 63-year-old woman who underwent attempted correction of a hallux valgus deformity 3 years previously presents to the office. She has pain in the hallux from dorsal abutment of the hallux on the shoe. There is no pain in the lesser toes or metatarsals. The recommended procedure to alleviate the irritation of the hallux is:
Explanation
This patient had previously undergone resection arthroplasty (Keller) for correction. A common complication of this procedure is a cock-up toe deformity due to insufficiency of the short flexors. This can be corrected with lengthening of the extensor hallucis. If the latter procedure fails, then an arthrodesis can be performed.
Question 47High Yield
Slide 1
A 42-year-old man with diabetes presents for treatment of a swollen foot (Slide). He does not recall the onset of swelling, and he states that his foot is not painful. On examination, the foot is hot to touch and swollen. Upon radiographic examination, no deformities are evident. Which of the following treatment options should be used next:
A 42-year-old man with diabetes presents for treatment of a swollen foot (Slide). He does not recall the onset of swelling, and he states that his foot is not painful. On examination, the foot is hot to touch and swollen. Upon radiographic examination, no deformities are evident. Which of the following treatment options should be used next:
Explanation
This patient presents with an acute neuroarthropathy. The acute painless swelling, associated with warmth and absence of radiographic findings, is typical of the acute phase of a C harcot process. A short leg cast or a boot to immobilize the foot is ideal, and no weight bearing should be permitted until the acute phase of this neuroarthropathy has subsided.
Question 48High Yield
An 11-year-old boy has right shoulder pain and has been unwilling to use the arm after throwing a baseball in a Little League game 3 weeks ago. Examination reveals upper arm and shoulder tenderness with swelling. A radiograph and MRI scan are shown in Figures 27a and 27b. Management should consist of
Explanation
The radiograph is consistent with a unicameral (simple) bone cyst. The MRI scan reveals that the cyst is juxtaposed to the physis and therefore can be classified as active (latent cysts are more than 1 cm away from the physis). Active cysts are treated with aspiration and steroid injection, although repeated injections may be necessary. Curettage and bone grafting results in more reliable healing but may lead to growth arrest in active cysts.
REFERENCES: Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 945-946.
Malawer MM: Tumors of the shoulder girdle: Techniques of resection and description of surgical classification. Orthop Clin North Am 1991;22:7-35.
REFERENCES: Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 945-946.
Malawer MM: Tumors of the shoulder girdle: Techniques of resection and description of surgical classification. Orthop Clin North Am 1991;22:7-35.
Question 49High Yield
A 35-year-old man has profound deltoid weakness after sustaining a traumatic anterior shoulder dislocation 6 weeks ago. Electromyographic (EMG) studies confirm an axillary nerve injury. Follow-up examination at 3 months reveals no recovery of function. What is the best course of action?
Explanation
Documenting the status of recovery at this time is appropriate; therefore, repeat EMG studies should be conducted to check for early signs of reinnervation. Timing of nerve exploration in this setting is debated, with authors suggesting exploration if there is no sign of recovery at 6 to 9 months.
REFERENCES: Perlmutter GS: Axillary nerve injury. Clin Orthop 1999;368:28-36.
Artico M, Salvati M, D’Andrea V, et al: Isolated lesions of the axillary nerves: Surgical treatment and outcome in twelve cases. Neurosurgery 1991;29:697-700.
Vissar CP, Coene LN, Brand R, et al: The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery: A prospective clinical and EMG study. J Bone Joint Surg Br 1999;81:679-685.
Pasila M, Jarma H, Kiviluoto O, et al: Early complications of primary shoulder dislocations. Acta Orthop Scand 1978;49:260-263.
REFERENCES: Perlmutter GS: Axillary nerve injury. Clin Orthop 1999;368:28-36.
Artico M, Salvati M, D’Andrea V, et al: Isolated lesions of the axillary nerves: Surgical treatment and outcome in twelve cases. Neurosurgery 1991;29:697-700.
Vissar CP, Coene LN, Brand R, et al: The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery: A prospective clinical and EMG study. J Bone Joint Surg Br 1999;81:679-685.
Pasila M, Jarma H, Kiviluoto O, et al: Early complications of primary shoulder dislocations. Acta Orthop Scand 1978;49:260-263.
Question 50High Yield
A 40-year-old male laborer with an acute left shoulder injury (Figures 94a and 94b).


Explanation
- Open reduction and internal fixation (ORIF)_
You Might Also Like



Medically Verified Content by
Prof. Dr. Mohammed Hutaif
Consultant Orthopedic & Spine Surgeon