Comprehensive Introduction and Patho-Epidemiology
Fractures of the proximal and middle phalanges represent a profound clinical challenge, standing among the most frequently encountered skeletal injuries within the realm of orthopedic hand trauma. Epidemiological studies indicate that phalangeal fractures account for approximately 10% to 20% of all fractures presenting to emergency departments, with a peak incidence in the active, working-age population. While a substantial proportion of these fractures can be managed non-operatively with precise closed reduction and protective splinting, a significant and complex subset demands meticulous surgical intervention. The etiology of these injuries is diverse, ranging from low-energy direct blows on the dorsum of the digits to high-energy crush injuries, industrial accidents, and complex torsional forces sustained during athletic endeavors.
The mechanism of injury directly dictates the resulting fracture pattern, which in turn governs the surgical strategy. A direct perpendicular blow typically yields a transverse or comminuted fracture pattern, whereas an axial load combined with a twisting force frequently results in oblique or spiral configurations. Intra-articular fractures at the metacarpophalangeal (MCP) or proximal interphalangeal (PIP) joints are predominantly driven by sheer forces or axial impaction. Recognizing the specific patho-epidemiology is the first critical step for the orthopedic surgeon, as it provides invaluable insight into the degree of underlying soft tissue trauma, periosteal stripping, and the potential for neurovascular compromise.
The primary, unyielding goal of operative management is to achieve a stable, anatomic reduction that permits immediate or early active mobilization of the affected digit. The hand is a notoriously unforgiving anatomic region; it is a densely packed, highly specialized organ where tendons, ligaments, and neurovascular structures glide in intimate proximity to the osseous framework. Prolonged immobilization of the phalanges inevitably leads to a cascade of deleterious effects, including dense tendon adhesions, severe joint contractures, capsular fibrosis, and profound functional impairment that can permanently disable the patient. The margin for error is virtually nonexistent; even a few degrees of rotational malalignment can cause the fingers to scissor and overlap during grip, severely diminishing hand function.
Therefore, the modern orthopedic hand surgeon must possess an encyclopedic understanding of phalangeal biomechanics, intricate surgical anatomy, and advanced internal fixation techniques. The evolution of osteosynthesis in the hand has transitioned from historical reliance on prolonged casting to the sophisticated application of minifragment screws, low-profile titanium plates, and precise intramedullary devices. Optimizing patient outcomes requires not only technical mastery in the operating theater but also a comprehensive, phased approach to preoperative planning, soft tissue management, and rigorous postoperative rehabilitation.
Detailed Surgical Anatomy and Biomechanics
Understanding the complex deforming forces acting upon the phalanges is the absolute foundation for both successful closed reduction and stable surgical fixation. The proximal phalanx is uniquely vulnerable to displacement because it lacks direct tendinous insertions along its diaphysis. Instead, it functions as an intercalated bone segment, suspended precariously between the powerful and intricate intrinsic and extrinsic muscle systems of the hand. This lack of direct muscular attachment means that once the structural integrity of the bony cylinder is breached, the fragment positions are entirely dictated by the pull of the surrounding tendons and ligaments.
When a transverse or short oblique fracture occurs in the proximal phalanx, the predictable and classic displacement pattern is volar apex angulation. This pathognomonic deformity occurs due to a relentless biomechanical tug-of-war between two distinct muscular forces. Proximally, the interosseous muscles, which insert onto the base of the proximal phalanx and the extensor hood, exert a powerful flexion force on the proximal fracture fragment. Distally, the central slip of the extensor mechanism, which traverses the dorsum of the proximal phalanx to insert on the dorsal base of the middle phalanx, exerts an unyielding extension force on the distal fragment.
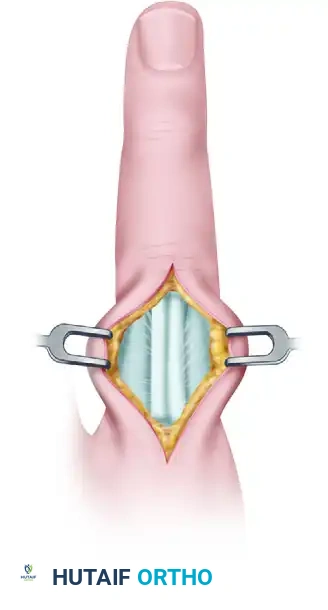
FIGURE 67-43: Biomechanical representation of deforming forces. Full flexion of the metacarpophalangeal (MCP) joint is required to relax these deforming intrinsic forces and maintain reduction.
This combination of proximal flexion and distal extension results in the characteristic volar angulation. If left uncorrected, the digit may assume a rigid "claw" position, drastically altering the resting tension of the flexor and extensor tendons. To neutralize these deforming forces during closed reduction or provisional surgical pinning, the metacarpophalangeal (MCP) joint must be placed in 70 to 90 degrees of flexion. This "intrinsic plus" position maximizes the tension on the collateral ligaments, preventing their contracture, while simultaneously relaxing the interossei and lumbricals, thereby facilitating the anatomic alignment of the fracture fragments.
In the middle phalanx, the biomechanical forces and resulting deformities are slightly more complex and are entirely dependent on the fracture's anatomic location relative to the insertion of the flexor digitorum superficialis (FDS). The FDS tendon bifurcates and inserts along the volar-lateral margins of the proximal half of the middle phalanx. If a fracture occurs proximal to the FDS insertion, the distal fragment is pulled into flexion by the FDS, while the proximal fragment is extended by the central slip, resulting in dorsal apex angulation. Conversely, if the fracture occurs distal to the FDS insertion, the proximal fragment is flexed by the FDS, and the distal fragment is extended by the terminal extensor tendon, resulting in volar apex angulation. Mastery of these dynamic forces is essential for executing a logical and mechanically sound surgical reduction.
Exhaustive Indications and Contraindications
While undisplaced, impacted, or inherently stable fractures of the phalanges are highly amenable to conservative care via functional splinting or buddy taping, surgical stabilization is strictly indicated under a specific set of clinical parameters. The decision to operate must be carefully weighed against the risks of surgical trauma, particularly the iatrogenic creation of scar tissue that can tether the delicate gliding mechanisms of the extensor and flexor apparatus. However, failure to operate on an unstable fracture will predictably lead to malunion, stiffness, and loss of hand function.
Absolute and Relative Indications
Surgical intervention is absolutely mandated in the presence of open fractures, which require meticulous surgical debridement, copious irrigation, and rigid skeletal stabilization to prevent deep space infection, osteomyelitis, and to promote optimal soft tissue healing. Multiple digit fractures within the same hand also represent a strong indication for surgery; fixing these fractures restores the structural skeletal cascade of the hand, allowing the uninjured joints to mobilize early and preventing global hand stiffness. Intra-articular fractures, particularly those involving more than 25% of the articular surface of the MCP or PIP joints, or those with a step-off greater than 1 mm, require open reduction and internal fixation (ORIF) to restore joint congruity and mitigate the rapid onset of post-traumatic osteoarthritis.
Rotational malalignment is an absolute indication for surgical correction, regardless of the radiographic appearance of the fracture on standard AP and lateral views. The hand tolerates angular deformity poorly, but it tolerates rotational deformity not at all. Even a minor rotational error of 5 degrees at the proximal phalanx can lead to 1.5 centimeters of digital overlap at the level of the fingertips during composite fist flexion, a condition known as "scissoring." Unstable fracture patterns, such as long spiral fractures, short oblique fractures, or highly comminuted diaphyseal fractures that demonstrate a propensity to lose reduction in a well-molded cast or splint, also necessitate surgical fixation to maintain length, alignment, and rotation.
Contraindications to Surgical Fixation
Despite the broad indications for operative management, several strict contraindications exist that the orthopedic surgeon must respect. Severe, life-threatening polytrauma takes absolute precedence; hand fractures must be temporarily splinted until the patient is hemodynamically stable and cleared for elective or semi-elective peripheral surgery. Active, untreated local infections (e.g., severe cellulitis, purulent flexor tenosynovitis unrelated to the fracture) are absolute contraindications to the placement of internal hardware, as this will inevitably lead to hardware seeding and chronic osteomyelitis.
Relative contraindications include severe pre-existing osteoarthritis of the adjacent joints, where the functional gain of perfect anatomic reduction may be negligible compared to the surgical risk. Additionally, patients with profound medical comorbidities that preclude safe anesthesia, or those with severe cognitive impairments or psychiatric conditions that guarantee non-compliance with the rigorous postoperative rehabilitation protocols, are generally poor candidates for complex internal fixation. In such scenarios, the surgeon may opt for closed reduction and percutaneous pinning (CRPP) under local anesthesia or accept a functional malunion rather than risk catastrophic surgical failure.
| Clinical Parameter | Indications for Surgical Fixation | Contraindications to Surgical Fixation |
|---|---|---|
| Fracture Pattern | Open, Intra-articular (>25%), Unstable, Spiral/Oblique | Undisplaced, Stable transverse, Impacted |
| Deformity | Rotational malalignment (scissoring), Volar/Dorsal apex angulation failing closed reduction | Acceptable angular deformity in a low-demand patient |
| Patient Factors | Multiple digit trauma, Polytrauma requiring hand use for transfers | Medically unfit, Severe non-compliance, Active local soft-tissue infection |
| Soft Tissue | Associated tendon/nerve lacerations requiring simultaneous repair | Crushed, non-viable soft tissue envelope precluding hardware coverage |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the hallmark of successful phalangeal fracture surgery. The foundation of this planning rests upon acquiring high-quality, orthogonal radiographic imaging. A standard hand series (Posteroanterior, Oblique, and Lateral) is often insufficient for isolated phalangeal injuries due to the superimposition of adjacent digits on the lateral view. Therefore, a "true lateral" radiograph of the specific injured digit must be obtained. This requires the radiology technician to isolate the affected finger, extending it while flexing the remaining digits out of the radiographic beam.
For complex intra-articular fractures, particularly those involving the condyles of the proximal or middle phalanx, or complex pilon-type fractures of the PIP joint base, a dedicated fine-cut Computed Tomography (CT) scan is invaluable. CT imaging with 3D reconstructions allows the surgeon to precisely map the fracture lines, quantify the degree of articular comminution, and identify the size and location of specific osteochondral fragments. This three-dimensional understanding dictates the choice of surgical approach and the specific hardware required, whether it be 1.0 mm minifragment screws, a low-profile condylar plate, or dynamic external fixation.
Preoperative templating, while often overlooked in hand surgery compared to large joint arthroplasty, is highly recommended. Using digital templating software or physical overlays, the surgeon should measure the medullary canal diameter and the length of the intact bone segments. This ensures that the appropriate inventory of minifragment sets (typically 1.3 mm, 1.5 mm, and 2.0 mm systems) and Kirschner wires (0.028, 0.035, and 0.045 inches) are available in the operating room. Furthermore, planning the exact trajectory of lag screws on the preoperative images prevents intraoperative trial and error, which can rapidly deplete the limited bone stock of the phalanges.
Patient positioning and operating room setup must be optimized for efficiency and ergonomic comfort. The patient is typically positioned supine with the operative arm extended on a radiolucent hand table. A pneumatic upper arm tourniquet is applied over generous padding to provide a bloodless surgical field, which is critical for identifying delicate digital nerves and vessels. The fluoroscopy unit (C-arm) should be positioned opposite the surgeon, entering perpendicular to the hand table, allowing for seamless live imaging without disrupting the sterile field. The surgeon must ensure that all specialized hand instruments, including fine dental picks, reduction forceps with point-to-point tips, and low-speed power drills, are readily available before the incision is made.
Step-by-Step Surgical Approach and Fixation Technique
The execution of phalangeal osteosynthesis requires a delicate balance between achieving rigid mechanical stability and preserving the vital soft tissue gliding layers. The choice of surgical approach is dictated by the fracture geometry, the planned fixation construct, and the absolute necessity to minimize iatrogenic trauma to the extensor apparatus and digital neurovascular bundles.
Surgical Approaches to the Phalanges
The Dorsolateral (Mid-axial) Approach is frequently utilized for diaphyseal fractures of the proximal and middle phalanges. The incision is placed longitudinally along the mid-axial line, which connects the apices of the flexion creases, remaining dorsal to the volar neurovascular bundle. The transverse retinacular ligaments are carefully incised, allowing the entire extensor mechanism to be elevated and retracted dorsally. This approach provides excellent, unhindered exposure of the lateral aspect of the phalanx, making it the premier choice for the application of lateral neutralization or compression plates, as well as the placement of interfragmentary lag screws.
The Direct Dorsal Approach is often required for complex proximal phalangeal fractures, particularly those with intra-articular extension into the MCP or PIP joints. However, a straight longitudinal incision over the dorsum of the digit must be strictly avoided; such incisions predictably lead to severe, bowstringing scar contractures that physically block finger flexion. Instead, the incision should extend from the MCP joint to the PIP joint in a gentle, sweeping "S" or zigzag curve. Once full-thickness skin flaps are elevated, the extensor mechanism is exposed. Depending on the fracture location, the surgeon may perform a longitudinal tendon-splitting approach (splitting the central slip precisely in the midline) or a tendon-sparing Chamay approach, which involves elevating the lateral bands and retracting them laterally to expose the dorsal diaphysis and metaphysis.
Technique 1: Minifragment Screw Fixation for Intra-articular Fractures
Displaced intra-articular fractures of the proximal phalanx base are challenging injuries that severely compromise the congruity and kinematics of the MCP joint. Rigid internal fixation using minifragment lag screws (typically 1.0 mm to 1.5 mm in diameter) is the gold standard for achieving anatomic articular reduction and allowing immediate postoperative mobilization.
Case Example: Three-Part Displaced Intra-articular Fracture
Preoperative Evaluation:
The following radiographs demonstrate a complex, high-energy three-part displaced intra-articular fracture of the proximal phalanx in a 27-year-old male laborer. The articular surface is significantly disrupted, with a profound step-off that necessitates precise open reduction.

FIGURE 67-41 A: Preoperative anteroposterior radiograph demonstrating the intra-articular split.

FIGURE 67-41 B: Preoperative oblique radiograph highlighting the displacement and articular step-off.
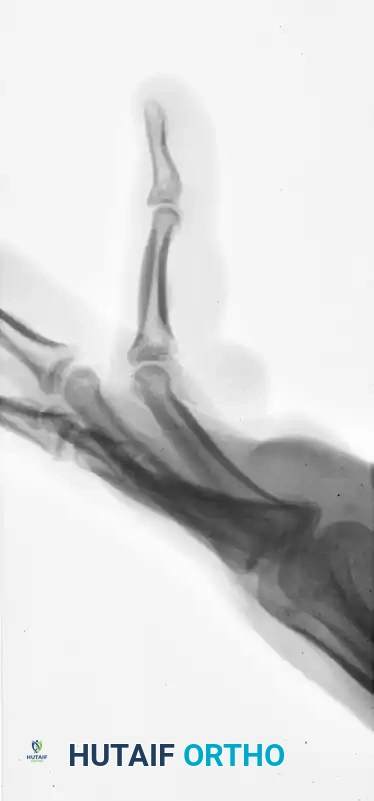
FIGURE 67-41 C: Preoperative lateral radiograph showing the volar subluxation tendency.
Surgical Execution:
1. Exposure: A dorsal S-shaped incision is utilized over the MCP joint. The sagittal bands are incised, and the extensor tendon is retracted to expose the dorsal capsule. The joint capsule is opened horizontally to directly visualize the articular surface and the fracture hematoma is evacuated.
2. Reduction: The articular fragments are meticulously manipulated into anatomic alignment using fine dental picks and a Freer elevator. The reduction is provisionally stabilized using 0.028-inch Kirschner wires driven parallel to the joint surface.
3. Fixation: Minifragment lag screws are sequentially placed to compress the articular fragments. The glide hole is drilled in the near cortex, followed by the thread hole in the far cortex. It is imperative that the screws are directed exactly perpendicular to the fracture plane to achieve maximum interfragmentary compression without inducing shear forces.
Pitfall: The collateral ligaments of the MCP joint are dynamic structures that glide over the base of the proximal phalanx during the arc of flexion and extension. If screw heads are left proud or prominent, they will mechanically impinge on these ligaments, leading to severe, intractable postoperative stiffness, pain, and eventual hardware failure.
Postoperative Result:
The screw heads must be meticulously countersunk into the cortical bone, or headless compression screws must be carefully selected to ensure an ultra-low profile. The following radiographs demonstrate the successful anatomic reduction and rigid fixation achieved in this case.

FIGURE 67-41 D: Postoperative AP radiograph showing anatomic restoration of the joint line.

FIGURE 67-41 E: Postoperative oblique radiograph confirming flush seating of the minifragment screws.

FIGURE 67-41 F: Postoperative lateral radiograph demonstrating restoration of the sagittal alignment. Note that the small screw heads do not interfere with collateral ligament function.
Technique 2: Pratt’s Technique for Phalangeal Shaft Fractures
While many transverse or short oblique diaphyseal fractures can be successfully managed with closed reduction and percutaneous pinning (CRPP), certain phalangeal shaft fractures require open reduction due to irreducible soft tissue interposition (often the periosteum or lateral bands) or severe comminution that precludes closed alignment. In these difficult instances, Pratt’s technique offers a highly reliable method for intramedullary stabilization using Kirschner wires augmented by monofilament wire loops.
Step-by-Step Execution of Pratt's Technique:
-
Incision and Exposure: A dorsal S-shaped approach is utilized. The skin and subcutaneous tissues are carefully dissected to expose the dorsal extensor mechanism. Hemostasis is achieved using bipolar electrocautery to avoid thermal injury to the delicate tendons.
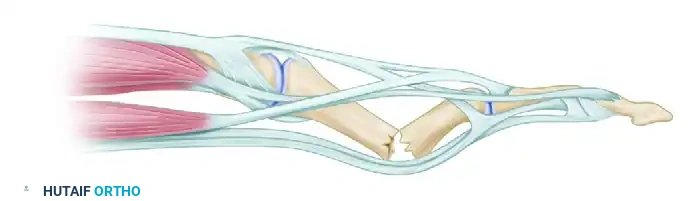
FIGURE 67-44 A: Initial dorsal exposure of the extensor mechanism over the fractured phalanx. -
Tendon Incision: The extensor mechanism is longitudinally incised precisely in the midline to expose the underlying fracture site. This split must be sharply defined. Extreme care must be taken to avoid stripping the delicate periosteum away from the fracture fragments, as this periosteal sleeve carries the critical blood supply necessary for fracture union.
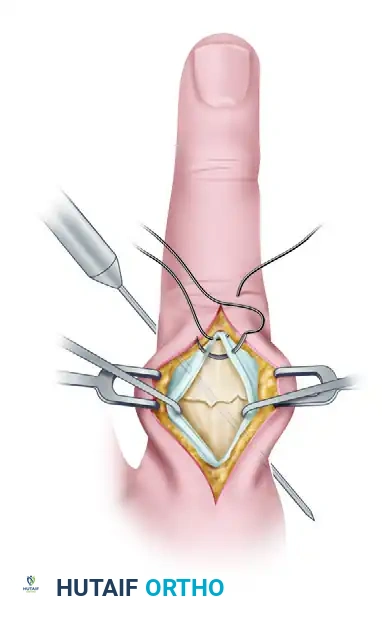
FIGURE 67-44 B: The extensor mechanism is incised, revealing the displaced phalangeal shaft fracture. -
Intramedullary Drilling and Pinning: The fracture is cleared of hematoma and anatomically reduced using point-to-point clamps. A Kirschner wire (typically 0.035 or 0.045 inch) is introduced into the medullary canal. Depending on the specific fracture pattern, crossed K-wires or a single stout intramedullary wire may be utilized. The wire is driven using a low-speed power drill to ensure precise placement, preventing the spinning wire from wrapping up soft tissue or displacing the meticulously reduced fracture fragments.

FIGURE 67-44 C: A Kirschner wire is drilled across the fracture site to provide longitudinal and rotational stability. -
Closure and Supplemental Fixation: Once absolute skeletal stability is achieved and confirmed via fluoroscopy, the extensor mechanism must be meticulously repaired. A fine monofilament wire or a strong, non-absorbable synthetic suture (e.g., 4-0 Prolene) is used to close the extensor split in a figure-of-eight or continuous locking fashion. This soft tissue repair must be incredibly robust, as it must withstand the tensile forces generated during early active motion rehabilitation protocols.
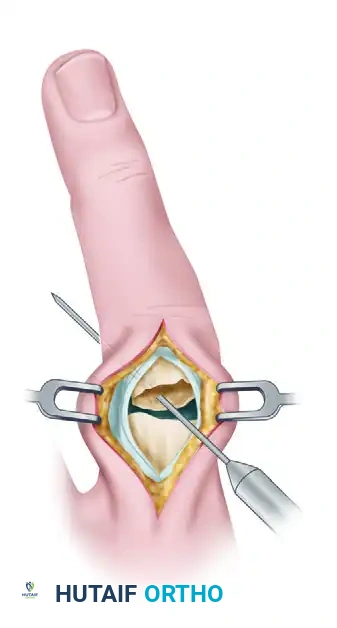
FIGURE 67-44 D: Final closure of the extensor mechanism over the stabilized fracture using monofilament wire.
Adjunctive Principles: Metacarpal Shaft Fixation
The sophisticated biomechanical principles and fixation strategies applied to phalangeal fractures are frequently extrapolated to metacarpal shaft fractures. When dealing with long oblique or spiral fractures of the metacarpals, interfragmentary lag screw fixation is highly effective, adhering to the principle that the length of the fracture line must be at least twice the diameter of the bone to accommodate two or more lag screws safely. However, the metacarpals are subjected to massive sagittal bending moments during power grip and lifting activities.
To counteract these substantial bending forces, supplemental fixation is often required to protect the lag screws from catastrophic failure. The following case illustrates the advanced use of lag screws augmented by cerclage wiring in a 75-year-old woman presenting with severe, shortened middle and ring metacarpal shaft fractures.
Preoperative Imaging:

FIGURE 67-42 A: Preoperative AP radiograph showing shortened and oblique middle and ring metacarpal fractures.

FIGURE 67-42 B: Preoperative oblique radiograph demonstrating the fracture geometry, which is highly suitable for interfragmentary fixation.
Postoperative Imaging:
Through a dorsal longitudinal approach between the metacarpals, the fractures were reduced anatomically, restoring length and rotation. Multiple 1.5 mm lag screws were placed to provide rigid interfragmentary compression. To neutralize the significant sagittal bending moment—particularly in the ring metacarpal, which has greater mobility at its carpometacarpal joint—a supplemental 24-gauge stainless steel cerclage wire was circumferentially applied.

FIGURE 67-42 C: Postoperative AP radiograph showing anatomic reduction and rigid fixation.

FIGURE 67-42 D: Postoperative oblique radiograph. Note that the sagittal bending moment of the ring metacarpal shaft fracture was successfully offset by the supplemental 24-gauge cerclage wire fixation.
Complications, Incidence Rates, and Salvage Management
Despite flawless surgical execution, the operative management of phalangeal fractures is fraught with potential complications. The hand is an unforgiving environment where the margin between a triumphant functional recovery and a devastatingly stiff digit is measured in millimeters of tendon glide. The surgeon must be acutely aware of these complications, actively working to prevent them during the primary surgery, and prepared to execute complex salvage procedures when they arise.
Stiffness is, without question, the most ubiquitous complication following phalangeal fracture fixation, occurring to some degree in up to 30-40% of operatively managed cases. This stiffness is primarily driven by dense tendon adhesions, where the extensor or flexor tendons become scarred to the underlying periosteum or the implanted hardware. Furthermore, capsular contracture of the PIP and MCP joints can occur rapidly if the digit is immobilized in a non-functional position for even a short duration. Prevention is the ultimate cure; achieving rigid fixation that permits immediate active motion is paramount.
Malunion and nonunion are less common but mechanically devastating. Rotational malunion, as previously discussed, leads to digital scissoring and a weakened grip. Angular malunion alters the biomechanical axis of the flexor tendons, leading to a loss of mechanical advantage. Nonunion is relatively rare in the well-vascularized phalanges (occurring in less than 2% of cases) but can be precipitated by excessive periosteal stripping, thermal necrosis from aggressive drilling, or inadequate mechanical stabilization. Infection is a catastrophic complication, particularly when hardware is present, demanding immediate surgical debridement, hardware removal if stability is compromised, and culture-directed intravenous antibiotic therapy.
When complications become established, salvage management requires advanced reconstructive techniques. Tenolysis (the surgical release of tendon adhesions) is a highly specialized procedure that should strictly be delayed until at least 6 months post-injury. This waiting period allows the fracture to fully consolidate and the inflammatory scar tissue to mature and soften. Performing a tenolysis prematurely risks refracturing the bone or triggering a massive, renewed inflammatory response that worsens
