Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater, colleagues. Today, we confront the nuanced and often unforgiving realm of extra-articular phalangeal fractures. While these injuries might initially appear straightforward on a standard radiograph, they demand meticulous attention to detail, profound spatial awareness, and a masterful understanding of hand biomechanics to ensure optimal functional recovery. Our primary objective as hand and upper extremity surgeons is not merely the restoration of bony architecture, but the preservation of the intricate, dynamic glide of the surrounding tendinous structures. This chapter serves as an intraoperative masterclass in precision, patience, and the delicate preservation of the digital extensor and flexor mechanisms.
Phalangeal fractures are among the most common skeletal injuries encountered in orthopedic trauma, accounting for a significant proportion of all hand fractures. The epidemiology of these injuries spans all age groups and demographics, frequently resulting from occupational hazards, athletic participation, and accidental crush injuries. Despite their high incidence, the economic and functional impact of a poorly managed phalangeal fracture is immense. A stiff, malrotated, or painful digit can severely compromise a patient's livelihood, independence, and overall quality of life. Therefore, we must approach every phalangeal fracture with the same rigor and respect as we would a complex intra-articular periarticular fracture of a major weight-bearing joint.
The fundamental philosophy guiding our treatment algorithm—whether we opt for conservative splinting or complex internal fixation—is the absolute necessity of early, controlled motion. The extensor mechanism glides directly over the dorsal cortex of the phalanges, separated by only a microscopic layer of periosteum and peritenon. Fractures, and the subsequent cascade of hematoma formation, edema, and fibroblastic proliferation, can severely tether this vital extensor apparatus. Early motion is the primary weapon in our arsenal against peritendinous adhesions. Consequently, our surgical constructs must be biomechanically robust enough to withstand the forces of early active rehabilitation without compromising the biological envelope.
Throughout this masterclass, we will dissect the why behind our surgical decision-making. We will explore the biomechanical rationale for specific fixation techniques, the anatomical pitfalls that lead to iatrogenic complications, and the salvage strategies required when primary interventions fail. By mastering the principles outlined in this chapter, you will be equipped to navigate the complexities of extra-articular phalangeal fractures, transforming potentially debilitating injuries into successful, functional outcomes for your patients.


Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches the skin, a profound, three-dimensional understanding of digital anatomy is mandatory. The phalanges are not merely isolated tubular bones; they are the central scaffolding of a highly complex, interconnected kinetic chain. Each phalanx possesses unique morphological characteristics—from the concave volar surface that accommodates the flexor tendons to the specialized condylar geometry that dictates the arc of motion. Navigating this landscape requires an intimate knowledge of the surrounding soft tissue envelope, which dictates both fracture displacement patterns and our surgical approaches.
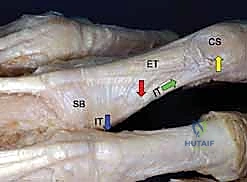
The Delicate Extensor Mechanism Overlay
The extensor mechanism is arguably the most unforgiving structure encountered in phalangeal trauma surgery. Unlike the robust flexor tendons enclosed within their synovial sheaths, the extensor apparatus is a broad, thin, and highly complex aponeurotic expansion. The Extensor Digitorum Communis (EDC) tendon travels centrally over the metacarpophalangeal (MCP) joint, stabilized by the sagittal bands, before receiving crucial contributions from the intrinsic muscles (lumbricals and interossei).


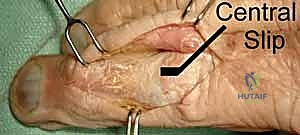
As we move distally over the proximal phalanx, the extensor mechanism divides. The central slip inserts into the dorsal base of the middle phalanx—a critical insertion that must be meticulously preserved or repaired during dorsal surgical approaches. The lateral bands, formed by the confluence of the intrinsic tendons and the lateral slips of the EDC, diverge around the proximal interphalangeal (PIP) joint. They are maintained in their dorsal position by the triangular ligament. Distally, these lateral bands converge to form the terminal tendon, which inserts onto the dorsal base of the distal phalanx.

Any surgical approach to the dorsal phalanx risks violating this intricate web. Dorsal implants, even those marketed as "low-profile," can lead to profound extensor imbalance. A plate placed on the dorsal aspect of the proximal phalanx effectively shortens and tightens the central slip, leading to an insidious loss of PIP joint flexion. Furthermore, hardware placed beneath the triangular ligament and terminal tendon over the middle phalanx risks severe tendon abrasion, rupture, and functional tethering. This anatomical reality heavily influences our preference for lateral plate placement or intramedullary fixation whenever biomechanically feasible.
Flexor Tendons and Intrinsic Muscle Dynamics
On the volar aspect, the digital flexor system presents its own set of challenges. The Flexor Digitorum Superficialis (FDS) bifurcates at the level of the proximal phalanx (Camper's chiasm) to insert onto the volar base and shafts of the middle phalanx. The Flexor Digitorum Profundus (FDP) travels through this bifurcation to insert onto the volar base of the distal phalanx. These tendons are housed within a complex fibro-osseous tunnel composed of annular and cruciate pulleys, which prevent bowstringing and ensure mechanical efficiency.
The intrinsic muscles—the lumbricals and interossei—play a dual role. They are primary flexors of the MCP joints and extensors of the PIP and distal interphalangeal (DIP) joints. Their insertion onto the base of the proximal phalanx and integration into the extensor hood make them primary deforming forces in proximal phalanx fractures. Understanding the vector forces exerted by these flexor and intrinsic tendons is paramount for achieving and maintaining closed reductions, as well as for designing biomechanically sound internal fixation constructs.

Neurovascular Bundles and Soft Tissue Envelope
The digital neurovascular bundles are the lifelines of the finger, coursing along the volar-lateral aspects of the phalanges. They consist of the proper digital nerves and arteries, accompanied by venae comitantes. These structures are exceptionally vulnerable during lateral surgical approaches, percutaneous pin placement, and even during aggressive closed reduction maneuvers.
Meticulous, blunt dissection and the use of specialized retractors are mandatory to protect these structures. Retraction should always be gentle and dynamic to prevent traction neuropraxia or vascular intimal injury. Furthermore, the soft tissue envelope of the digit is notoriously thin and unforgiving. Excessive periosteal stripping during open reduction not only devitalizes the fracture fragments, leading to delayed union or nonunion, but also creates a dense bed of scar tissue that will inevitably tether the overlying tendons. The modern orthopedic surgeon must prioritize biological fixation principles, utilizing minimally invasive techniques and tissue-sparing approaches whenever the fracture pattern allows.

Pathogenesis and Fracture Deformity Patterns
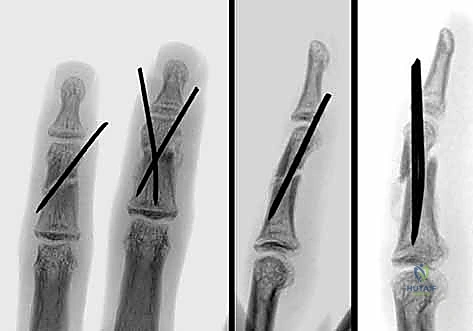
The specific fracture pattern observed on initial radiographs is a direct historical record of the biomechanical forces applied to the digit at the exact moment of failure. By reverse-engineering these forces, we can better understand the inherent instability of the fracture and anticipate the deforming muscle forces we must overcome during reduction and fixation.
Torsional, Angular, and Direct Trauma Mechanics
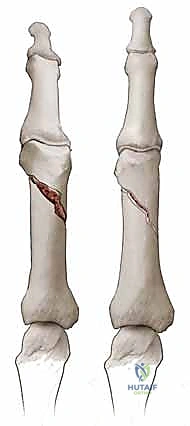
Torsional forces, often occurring when a digit is caught in a rotating machine or twisted during a fall, typically result in long spiral fractures. These fractures are inherently unstable, prone to both shortening and, critically, rotational malalignment. Angular and three-point bending forces, such as a direct blow to the side of the finger, generally produce transverse or short oblique fractures. The stability of these fractures depends heavily on the integrity of the periosteal hinge and the degree of initial displacement.
Direct crush trauma, frequently seen with hammer blows or heavy machinery accidents, results in highly comminuted fracture patterns. These are particularly common in the distal phalanx, where the bone is crushed between the traumatizing object and the underlying rigid surface. These injuries are almost universally associated with severe soft tissue compromise, including nail bed lacerations, subungual hematomas, and tuft amputations, necessitating a comprehensive approach that addresses both the skeletal and soft tissue envelopes simultaneously.

The Tendon Tug-of-War in Proximal and Middle Phalanges
Understanding the predictable deformity patterns driven by tendinous attachments is the cornerstone of successful reduction. Proximal phalanx fractures classically present with an apex volar angulation. This is not a random occurrence; it is the result of a fierce tendinous tug-of-war. The intrinsic muscles (interossei and lumbricals), inserting onto the base of the proximal phalanx, exert a strong flexing force on the proximal fragment. Simultaneously, the central slip of the extensor mechanism exerts an extending force on the distal fragment. This combined biomechanical vector forces the fracture apex volarly.
Middle phalanx fractures present a slightly more variable, yet predictable, deformity pattern dependent on the fracture line's relationship to the FDS insertion. If the fracture occurs proximal to the FDS insertion, the distal fragment is pulled into flexion by the FDS, while the proximal fragment is extended by the central slip, resulting in an apex dorsal angulation. Conversely, if the fracture is distal to the FDS insertion, the proximal fragment is flexed by the FDS, and the distal fragment is extended by the terminal tendon, resulting in an apex volar angulation. Recognizing these patterns allows the surgeon to utilize the intact soft tissue hinges and apply specific counter-forces during closed reduction maneuvers.

Clinical Evaluation and Diagnostic Imaging
A rigorous, systematic clinical evaluation is the diagnostic blueprint that guides our entire treatment strategy. We must look beyond the obvious skeletal deformity and assess the entire functional unit of the hand. The history should elicit the exact mechanism, energy level, and chronicity of the injury, as well as the patient's occupational demands and compliance potential.
The Diagnostic Blueprint of Physical Examination
The physical examination begins with a critical observation of the resting digital cascade. In a normal, relaxed hand, the digits exhibit a progressive increase in flexion from the index to the small finger. A disruption in this cascade is a glaring red flag for an underlying structural injury, be it a fracture, tendon rupture, or joint dislocation.
Palpation must be precise, localizing maximal point tenderness to differentiate between collateral ligament sprains, volar plate injuries, and true osseous fractures. However, the most critical aspect of the physical exam is the assessment of rotational deformity. Rotational malalignment is the most unforgiving complication in phalangeal fracture management; even a few degrees of rotation can cause the injured digit to cross over or "scissor" its neighbor during active flexion, severely impairing grip strength and hand function.
To accurately assess rotation, the patient must actively flex and extend the digits as a synchronized unit. During full flexion, the tips of all digits should point toward a single anatomical landmark: the distal pole of the scaphoid. If the injured digit deviates from this trajectory and scissors over an adjacent finger, rotational malrotation is present and must be corrected. If pain precludes active flexion, a digital anesthetic block should be administered. Alternatively, comparing the plane of the nail bed of the injured finger to those of the adjacent, uninjured digits provides a highly reliable, static indicator of rotational alignment.


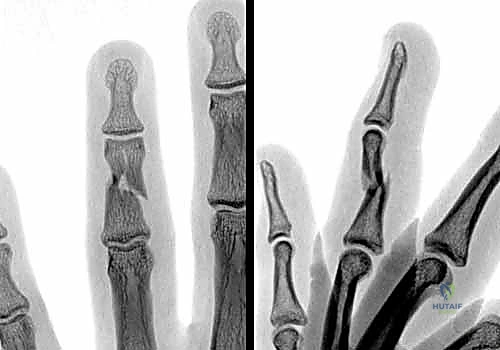
Advanced Radiographic Assessment and Fluoroscopy
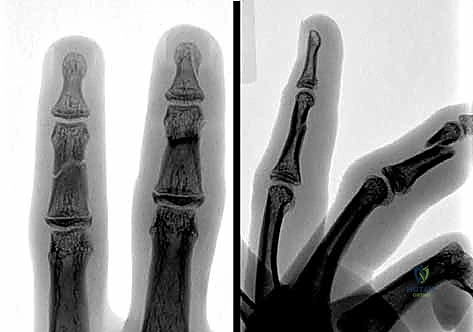
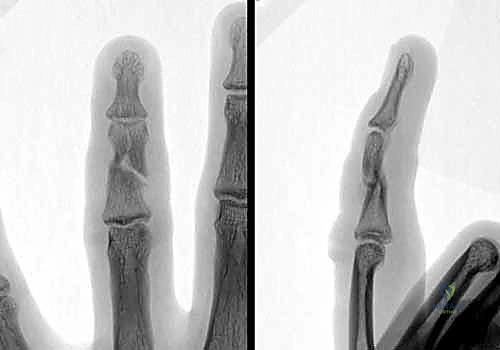
Standard, high-quality radiographs remain the gold standard for diagnosing extra-articular phalangeal fractures. A complete series must include true anterior-posterior (AP), true lateral, and oblique views of the specific digit involved. A common pitfall is relying on a lateral radiograph of the entire hand, which inevitably results in overlapping digital shadows that obscure critical fracture details.
The true lateral view is paramount for assessing apex angulation and subtle articular step-offs. A perfectly positioned true lateral radiograph of a phalanx should demonstrate concentric alignment of the condyles; a "double density" or mismatch of the condylar outlines suggests either a non-true lateral projection or, more concerningly, rotational malalignment of the fracture fragments.
Intraoperative fluoroscopy utilizing a mini C-arm is an indispensable tool. It allows for dynamic, real-time assessment of fracture stability throughout a full arc of motion. We routinely utilize fluoroscopy to stress the fracture under live imaging, determining whether a seemingly stable fracture displaces under physiological loads, thereby dictating the need for operative intervention. Advanced imaging modalities such as CT or MRI are rarely indicated for acute, isolated extra-articular phalangeal fractures, though CT can be invaluable for preoperative planning in complex, multi-fragmentary periarticular extensions or established nonunions.

Exhaustive Indications and Contraindications
The decision to transition from conservative management to operative intervention is nuanced, requiring a careful balancing of fracture stability, soft tissue integrity, and patient-specific factors. The overarching goal is to achieve a reduction stable enough to permit early active motion. If this cannot be achieved and maintained with a splint, surgery is indicated.
| Category | Operative Indications | Non-Operative Indications | Absolute/Relative Contraindications to Surgery |
|---|---|---|---|
| Fracture Displacement | Any rotational malalignment (Zero tolerance). Angulation > 10-15° in proximal phalanx. Angulation > 20° in middle phalanx. Shortening > 2mm. |
Nondisplaced or minimally displaced fractures. Stable impacted fractures. Angulation within acceptable parameters without rotational deformity. |
Absolute: Active, profound local skin infection (cellulitis/abscess) over the surgical site. Relative: Severe, untreatable medical comorbidities precluding anesthesia. |
| Fracture Pattern | Unstable patterns: Long spiral, short oblique, multi-fragmentary comminution. Multiple digital fractures (to allow early mobilization of the hand as a unit). |
Transverse fractures that are stable after closed reduction. Tuft fractures of the distal phalanx (unless associated with severe nail bed laceration requiring repair). |
Relative: Extreme osteopenia where hardware purchase is impossible (consider CRPP over ORIF). |
| Soft Tissue / Associated Injuries | Open fractures requiring irrigation and debridement. Fractures associated with tendon ruptures or neurovascular compromise requiring repair. "Seymour" fractures (open physeal fractures of distal phalanx). |
Closed injuries with a robust, intact soft tissue envelope capable of tolerating cast/splint pressure. | Relative: Severe crush injuries with compromised vascularity where extensive surgical dissection might precipitate digital necrosis. |
| Patient Factors | Polytrauma patients requiring immediate hand use. Non-compliant patients unable to manage complex splinting protocols. |
Patients who are highly compliant with splinting and close follow-up. Low-demand patients where minor deformity does not impair function. |
Relative: Patients unable or unwilling to participate in rigorous post-operative rehabilitation (stiffness is guaranteed). |
Determining Operative Versus Nonoperative Management
The parameters for acceptable non-operative reduction are strict. We generally accept no rotational deformity, less than 2 millimeters of shortening, and less than 10 to 15 degrees of apex volar angulation in the proximal phalanx. Angulation beyond these limits alters the biomechanical advantage of the extrinsic flexors and extensors, leading to a pseudo-claw deformity and a significant loss of grip strength.
When evaluating a fracture for non-operative management, the "tenodesis test" under fluoroscopy is highly informative. If the fracture remains stable and aligned while the wrist is passively flexed and extended (utilizing the natural tenodesis effect to load the digital tendons), it may be amenable to buddy taping and a protective orthosis. However, if the fracture gaps or angulates under this physiological load, it is inherently unstable and warrants surgical fixation to prevent delayed displacement and subsequent malunion.

Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the hallmark of a master surgeon. For phalangeal fractures, this begins with a detailed analysis of the radiographs to determine the fracture morphology, the size of the fragments, and the optimal trajectory for internal fixation. Templating, even mentally or using digital software, helps in selecting the appropriate implant size—whether it be 1.2mm or 1.5mm screws, or specific low-profile mini-fragment plates.
Equipment Selection and Operating Room Setup
The operating room must be configured to optimize workflow and visualization. The patient is positioned supine with the operative extremity extended on a radiolucent hand table. A mini C-arm is brought in from the head or the foot of the table, depending on the surgeon's preference, ensuring it can freely arc over the hand without compromising the sterile field.
Anesthesia selection is a critical preoperative decision. While general anesthesia or regional brachial plexus blocks are standard, the Wide Awake Local Anesthesia No Tourniquet (WALANT) technique has revolutionized hand trauma surgery. Utilizing a mixture of lidocaine and epinephrine provides excellent hemostasis and profound local anesthesia, allowing the surgeon to assess active digital motion, tendon gliding, and fracture stability intraoperatively before closing the skin. This real-time functional feedback is invaluable for preventing extensor lag and confirming the elimination of rotational malalignment.
If a pneumatic tourniquet is utilized, it should be placed on the upper arm and inflated to 250 mmHg after exsanguination with an Esmarch bandage. However, tourniquet time must be strictly monitored to prevent ischemic injury to the delicate intrinsic musculature. A comprehensive hand tray equipped with dental picks, fine Freer elevators, reduction forceps with point-to-point clamps, and a high-speed burr must be readily available.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution must be precise, respecting the delicate soft tissue envelope while achieving absolute biomechanical stability. The choice of fixation—ranging from percutaneous K-wires to rigid plate osteosynthesis—is dictated by the fracture pattern, the degree of comminution, and the surgeon's experience.
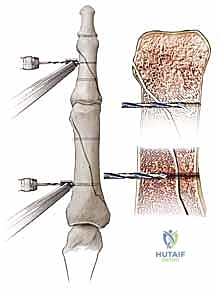
Closed Reduction and Percutaneous Pinning (CRPP)
For extra-articular fractures that are unstable but reducible closed (e.g., transverse or short oblique fractures), CRPP remains a highly effective, biologically friendly option. The goal is to achieve reduction using longitudinal traction and specific counter-pressure to correct apex angulation.
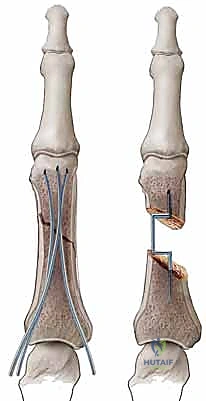
Once reduced, fixation is typically achieved using 0.035-inch or 0.045-inch Kirschner wires. Techniques vary based on the fracture location. For proximal phalanx fractures, crossed K-wires can be introduced percutaneously from the condyles, aiming proximally. Care must be taken to avoid tethering the lateral bands. Alternatively, intramedullary K-wires (the "bouquet" technique) can be introduced antegrade through the metacarpal head or retrograde through the condyles. This technique provides excellent bending stability while minimizing soft tissue tethering, though it offers less rotational control than crossed pins. Pins are typically left protruding through the skin, bent, and capped for easy removal in the clinic at 3 to 4 weeks.

Open Reduction and Internal Fixation (ORIF) Strategies
When closed reduction is impossible due to soft tissue interposition, or when the fracture pattern demands absolute rigid fixation (e.g., long spiral fractures requiring lag screws), ORIF is indicated.
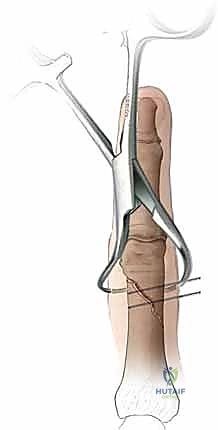
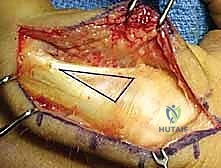
The Surgical Approach: The approach must be carefully selected. A dorsal longitudinal incision is common, but the extensor mechanism must be managed meticulously. We advocate for a tendon-sparing approach whenever possible, splitting the EDC longitudinally or elevating the lateral bands carefully without detaching the central slip. Mid-axial approaches (lateral incisions along the glabrous line) provide excellent access to the phalangeal shaft while completely avoiding the dorsal extensor apparatus, making it our preferred approach for lateral plating.
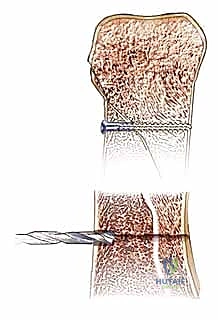
Lag Screw Fixation: For long spiral or oblique fractures where the fracture line is at least twice the diameter of the bone, multiple lag screws provide superior biomechanical stability. The technique requires precise execution: drilling a glide hole in the near cortex, a thread hole in the far cortex, countersinking the near cortex to prevent stress risers and hardware prominence, and meticulous measurement before screw insertion. We typically utilize 1.2mm or 1.5mm cortical screws. The screws must be placed perpendicular to the fracture plane to achieve maximal interfragmentary compression without inducing shear forces.
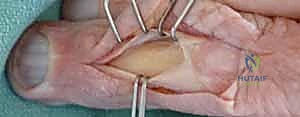

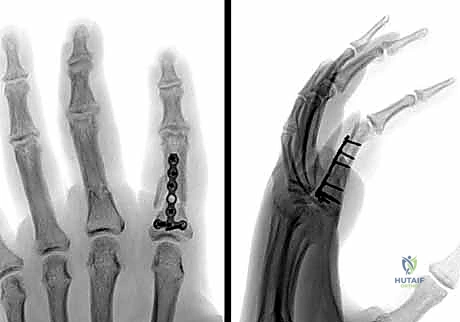
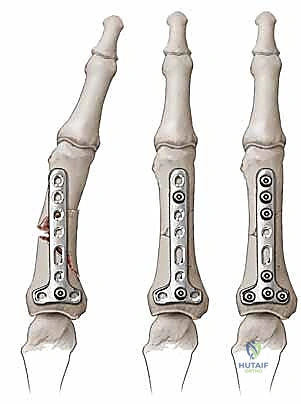
Plate Osteosynthesis: When comminution is present or the fracture pattern is not amenable to lag screws alone, plate fixation is necessary. We strongly reiterate the Surgical Warning regarding dorsal plates: they are notorious for causing extensor tendon adhesions and loss of PIP flexion. Therefore, we highly prefer lateral placement of low-profile mini-fragment plates (1.3mm or 1.5mm systems) along the mid-axial line. The plate should be contoured perfectly to the bone to avoid secondary displacement during screw tightening. At least two, and preferably three, bicortical screws should be placed on each side of the fracture.

Intramedullary Fixation Techniques
In recent years, the use of intramedullary headless compression screws has gained significant traction for transverse and short oblique extra-articular phalangeal fractures. This technique offers the ultimate biological advantage: rigid internal fixation with zero periosteal stripping and no prominent hardware to tether the extensor mechanism.
The technique involves a mini-open or percutaneous approach to the articular surface (usually the MCP joint for proximal phalanges or the PIP joint for middle phalanges). A guide wire is passed centrally down the intramedullary canal across the reduced fracture. A cannulated drill is used, followed by the insertion of a headless compression screw. The screw must be countersunk below the articular cartilage to prevent joint damage. This construct provides excellent bending and rotational stability, allowing for immediate, aggressive active motion protocols.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications in phalangeal fracture management are common and can be devastating to hand function. Anticipating these pitfalls and knowing how to manage them is what separates a competent surgeon from a master.
| Complication | Estimated Incidence | Etiology / Risk Factors | Prevention and Salvage Management |
|---|---|---|---|
| Joint Stiffness / Tendon Adhesions | 20% - 50% (Most Common) | Prolonged immobilization (>3 weeks), extensive surgical dissection, dorsal plate placement, severe initial trauma. | Prevention: Rigid fixation allowing immediate active motion, tissue- |
Clinical & Radiographic Imaging Archive