Orthopedic Surgery Board Review 2026 | High-Yield MCQs - Set 10

Key Takeaway
We review everything you need to understand about Orthopedic Surgery Board Review 2026 | High-Yield MCQs - Set 10. New High-Yield Orthopedic Board Review MCQs (Set 10). 100 fresh randomized questions with timers, scoring, and explanations.
Orthopedic Surgery Board Review 2026 | High-Yield MCQs - Set 10
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
In the nonsurgical management of posterior tibial tendon dysfunction with flexible deformity, a common strategy is to prescribe an ankle-foot orthosis or a University of California Biomechanics Laboratory (UCBL) orthosis with medial posting. A high patient satisfaction rating and favorable outcome with this nonsurgical management is most likely in which of the following situations?
Explanation
Question 2
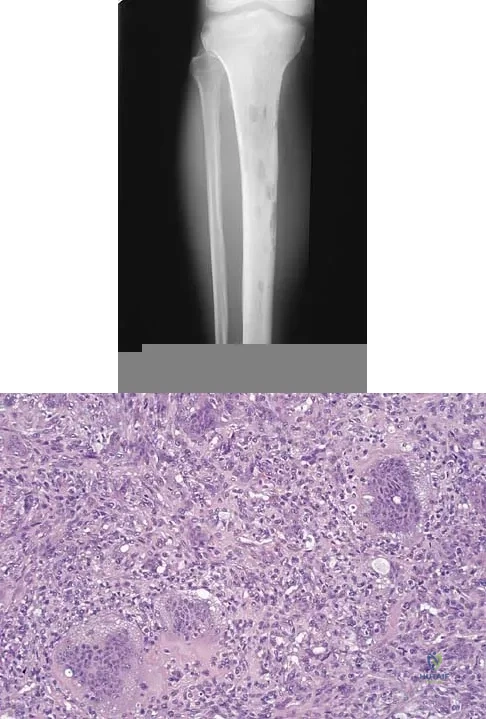
A 34-year-old woman reports constant midlateral arm pain after sustaining minimal trauma to the shoulder. Radiographs and a biopsy specimen are shown in Figures 29a and 29b. What is the most likely diagnosis?
Explanation
Question 3
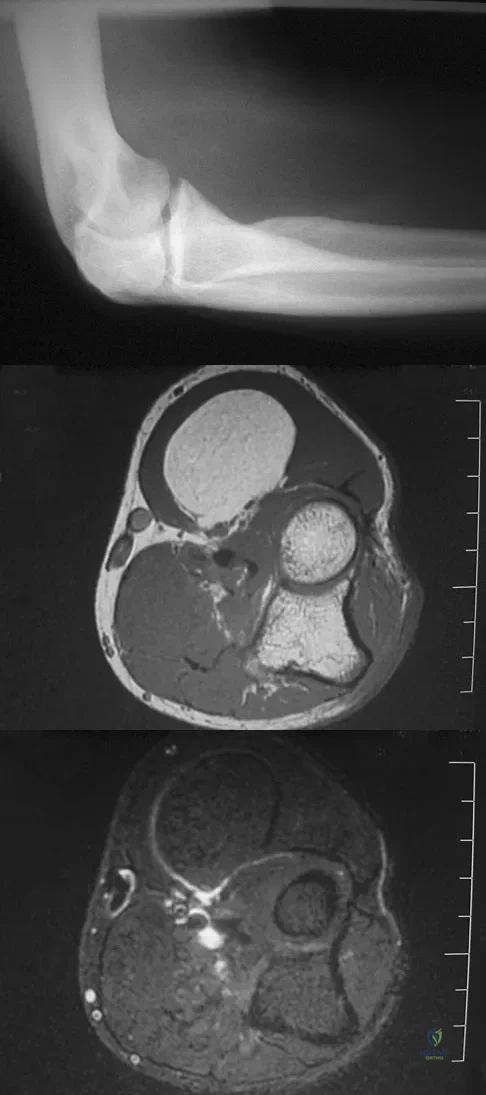
A 33-year-old man reports an enlarging painful soft-tissue mass in his right forearm. A radiograph and MRI scans are shown in Figures 45a through 45c. Treatment should consist of
Explanation
Question 4
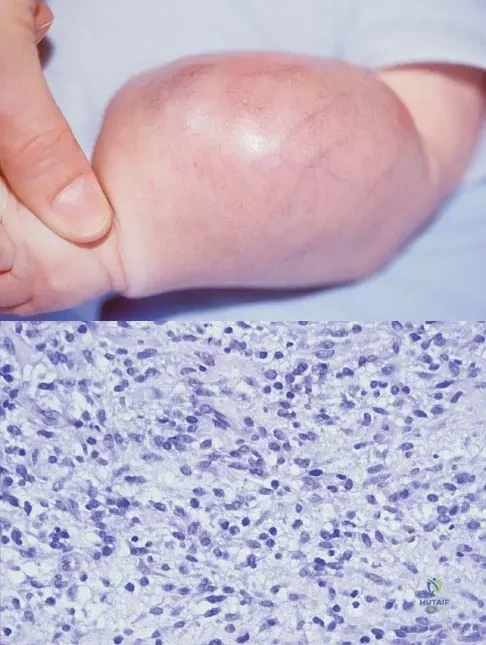
An infant is born with a mass that involves both the volar and dorsal compartments of the left arm. A clinical photograph and biopsy specimen are shown in Figures 41a and 41b. What is the best initial course of action?
Explanation
Question 5
The wear resistance of ultra-high molecular weight polyethylene can be improved by exposing the polymer to high-energy radiation (eg, gamma or electron beam), followed by a thermal treatment. What is one detrimental side effect of this process?
Explanation
Question 6
A 3-year-old boy with severe cerebral palsy is unable to sit independently and does not crawl. Examination reveals a 40-degree hip flexion contracture by the Thomas test and 25 degrees of passive abduction. A radiograph of the pelvis shows subluxation of both hips, with a migration index of 30%. Management should consist of
Explanation
Question 7
A metal-on-metal bearing used for total hip arthroplasty shows which of the following properties?

Explanation
Question 8
A 38-year-old man sustains a complete avulsion with retraction of the ischial attachment of the hamstring muscles in a fall while water skiing. He indicates that he is an aggressive athlete who participates regularly in multiple running and cutting-type sports, and he strongly desires to continue his athletic competition. Management should consist of
Explanation
Question 9
To preserve blood supply to the fractured bone seen in Figures 12a and 12b, care should be taken when exposing which of the following areas?

Explanation
Question 10
A 29-year-old woman was injured in a high-speed motor vehicle accident 3 hours ago. Radiographs are shown in Figures 7a through 7e. Her right foot injury is open and contaminated. Her associated injuries include a closed head injury and a ruptured spleen requiring resection. She has had 6 units of packed red blood cells and the trauma surgeon has turned her care over to you. Her current base deficit is 10 and her urinary output has averaged 0.4 mL/kg for the last 2 hours. What is the best treatment at this time?

Explanation
Question 11
A 26-year-old woman is seen in the emergency department with an intra-articular distal tibia fracture and a fibular fracture (pilon). The patient, her husband, and three small children have recently immigrated to the United States from Mexico. The husband and wife have both been in a migrant labor camp but have no immediate relatives in the States. What factor is most important when considering her recommended care and treatment?

Explanation
Question 12
Figure 12 shows a lateral radiograph of the elbow. What is the most likely diagnosis?

Explanation
Question 13
Soft-tissue sarcomas most commonly metastasize to the

Explanation
Question 14
The best patient-related outcomes, following the surgical treatment of cauda equina syndrome secondary to a large L5-S1 disk herniation, are most closely related to which of the following?
Explanation
Question 15
Which of the following infectious organisms may be associated with underlying malignancy?
Explanation
Question 16
Figure 22 shows the radiograph of a 7-year-old boy who underwent retrograde elastic nailing of a femoral shaft fracture. What is the most common problem following this procedure?

Explanation
Question 17
A 35-year-old man is brought to the emergency department following a motorcycle accident. He is breathing spontaneously and has a systolic blood pressure of 80 mm Hg, a pulse rate of 120/min, and a temperature of 98.6 degrees F (37 degrees C). Examination suggests an unstable pelvic fracture; AP radiographs confirm an open book injury with vertical displacement on the left side. Ultrasound evaluation of the abdomen is negative. Despite administration of 4 L of normal saline solution, he still has a systolic pressure of 90 mm Hg and a pulse rate of 110. Urine output has been about 20 mL since arrival 35 minutes ago. What is the next best course of action?
Explanation
Question 18
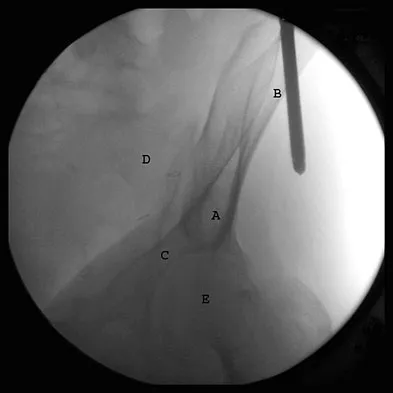
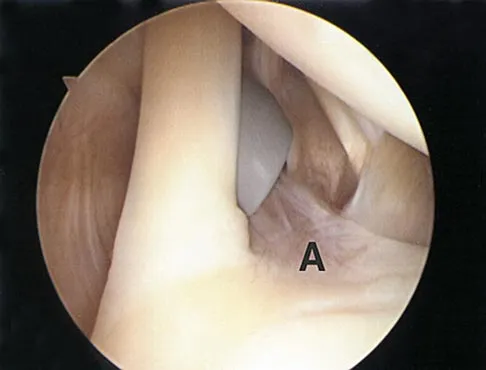
The correct starting point for an external fixation half pin placed into the anterior inferior iliac spine (AIIS) is labeled by what letter in Figure 3?
Explanation
Question 19
Figure 1 shows the radiograph of an 18-year-old patient who has severe knee pain. Treatment consisting of osteotomy should be perfomed

Explanation
Question 20
Figure 16 shows the radiograph of a 56-year-old man who has neck pain after a rollover accident on his lawnmower. The injury appears to be isolated, and he is neurologically intact. Management of the fracture should consist of

Explanation
Question 21
Use of prophylactic knee bracing in contact sports participants results in which of the following?

Explanation
Question 22
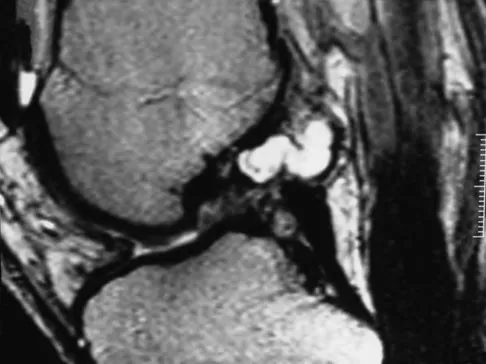
A 35-year-old woman who is a recreational runner reports posterior knee pain and tightness in the knee with flexion during running. She denies any history of trauma. Examination reveals normal patellar glide and tilt and no patellar apprehension. Range of motion is 5 degrees to 120 degrees, and quadriceps function and knee ligamentous examination are normal. Radiographs are normal. An MRI scan is shown in Figure 18. What is the most likely diagnosis?
Explanation
Question 23
A 39-year-old competitive cyclist sustains an injury to her left hip in a fall. Gadolinium arthrography, with an accompanying MRI scan, is shown in Figure 31. A cleft, or defect, identified by the arrow, indicates a detachment of the

Explanation
Question 24
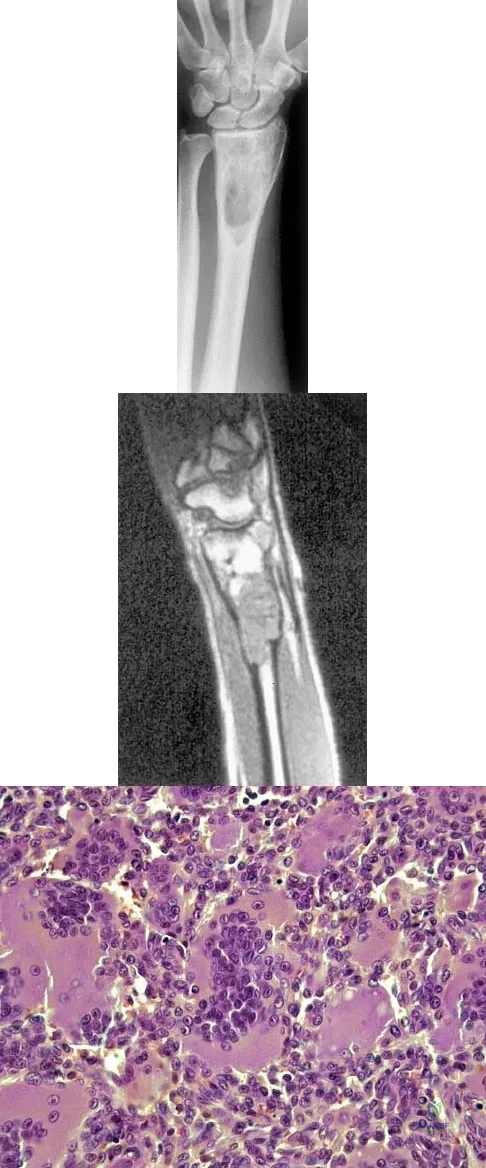
Figures 27a through 27c show the AP radiograph, MRI scan, and biopsy specimen of an otherwise healthy man who has a painful wrist. Serum chemistry studies are normal. What is the most likely diagnosis?
Explanation
Question 25
A 17-year-old high school long distance runner is seeking advice before running a marathon for the first time. What advice should be given regarding his fluid, carbohydrate, and electrolyte intake around the time of the race?
Explanation
Question 26
Which of the following is most commonly associated with an open clavicular fracture?

Explanation
Question 27
A 14-year-old girl with polyarticular juvenile rheumatoid arthritis (JRA) has severe neck pain and reports the onset of urinary incontinence. A lateral radiograph and lateral tomogram of the cervical spine are shown in Figures 15a and 15b. An MRI scan of the upper cervical spine is shown in Figure 15c. Management should consist of

Explanation
Question 28
An 8-year-old boy sustains injuries to his head, abdomen, and left lower extremity after being struck by a truck. In the emergency department, his mental status deteriorates and he is intubated after assessment reveals a Glasgow Coma Scale score of 3; the score subsequently improves to 10. A CT scan reveals a right parietal intracranial hemorrhage, and an abdominal ultrasound reveals free fluid. Prior to an emergency laparotomy, the swollen left thigh is evaluated. Radiographs reveal a transverse fracture of the mid-diaphysis. Management of the fracture should consist of
Explanation
Question 29
A 66-year-old man has a high-grade angiosarcoma of the right tibia. A radiograph is shown in Figure 43. Treatment should consist of

Explanation
Question 30
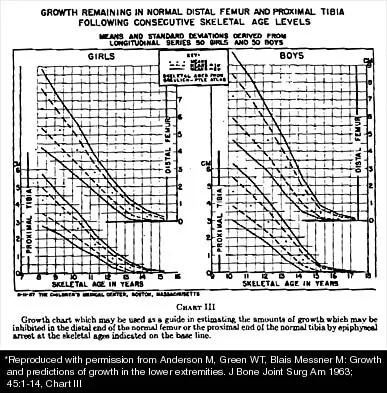
A 10-year-old girl with a monoarticular pattern of juvenile rheumatoid arthritis (JRA) has had a 3-cm limb-length discrepancy since age 8 years when inflammation in the right knee came under good medical control. Because her right leg is longer, the patient states that she would like her legs to be close to equal in length in the future. A growth-remaining chart is shown in Figure 14. Management should consist of
Explanation
Question 31
A 19-year-old wrestler has numbness along the radial aspect of the forearm after undergoing an open Bankart repair through an anterior deltopectoral approach. Motor weakness would be expected along with what other finding?

Explanation
Question 32
Which of the following orthotic features best reduces pain in patients with hallux rigidus?
Explanation
Question 33
Which of the following changes to heart rate, blood pressure, and bulbocavernosus reflex are typical of spinal shock?
Explanation
Question 34
What is the most important factor in determining recovery after surgical repair of a complete laceration of a nerve at the wrist?
Explanation
Question 35
What percent of patients initially diagnosed with classic, high-grade osteosarcoma of the extremity have visible evidence of pulmonary metastasis on CT of the chest?
Explanation
Question 36
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of

Explanation
Question 37
Which of following side effects is most commonly seen in a pediatric patient undergoing ketamine anesthesia?

Explanation
Question 38
The major benefit of irrigation with a castile soap solution over irrigation with bacitracin solution for the treatment of the open fracture shown in Figure 42 can be seen in which of the following outcomes?

Explanation
Question 39
A 45-year-old man undergoes an open reduction and internal fixation of a displaced proximal third humeral shaft fracture via an anterolateral approach. Postoperatively, he is unable to extend his wrist or fingers, though he had full function preoperatively. Which of the following is the most appropriate initial management for this neurological deficit?
Explanation
Question 40
A 65-year-old man presents with progressive hand clumsiness, difficulty buttoning his shirt, and a wide-based gait. Physical examination demonstrates a positive Hoffmann sign bilaterally and sustained ankle clonus. An MRI of the cervical spine confirms severe central canal stenosis from C3-C6. He undergoes a posterior cervical laminectomy and instrumented fusion. On postoperative day 2, he develops isolated, severe weakness in bilateral shoulder abduction and elbow flexion (0/5 strength), with normal hand grip and lower extremity function. Sensation is intact. What is the most likely etiology of this complication?
Explanation
Question 41
A 28-year-old man sustains a closed midshaft tibia fracture and is treated with reamed intramedullary nailing. Which of the following biological processes best characterizes the primary mode of bone healing expected in this scenario?
Explanation
Question 42
A 24-year-old male presents with persistent wrist pain 6 months after a fall onto an outstretched hand. Initial radiographs at an outside clinic were interpreted as normal. Current imaging reveals a scaphoid proximal pole fracture nonunion with sclerosis of the proximal fragment, indicating avascular necrosis (AVN). There is no evidence of carpal collapse or radiocarpal arthritis. What is the most appropriate surgical intervention?
Explanation
Question 43
A 14-year-old obese male presents with an acute exacerbation of chronic left knee pain and a severe limp. Examination reveals obligate external rotation of the hip during passive flexion. He is completely unable to bear weight on the left leg. Radiographs confirm a severe, acute-on-chronic slipped capital femoral epiphysis (SCFE). Which of the following is the most serious and highly prevalent complication specifically associated with this patient's inability to bear weight?
Explanation
Question 44
A 55-year-old woman with a 15-year history of poorly controlled type 2 diabetes mellitus presents with a swollen, warm, and erythematous right foot. She denies any specific trauma. She has no fevers or chills, and laboratory markers for infection (WBC, CRP, ESR) are within normal limits. Radiographs demonstrate fragmentation of the tarsometatarsal joints, joint subluxation, and soft tissue swelling. What is the gold standard initial management for this condition?
Explanation
Question 45
During a total hip arthroplasty, the surgeon elects to use a highly cross-linked polyethylene (HXLPE) liner. Compared to conventional ultra-high-molecular-weight polyethylene (UHMWPE), the primary trade-off of the highly cross-linked polyethylene manufacturing process is a decrease in which of the following mechanical properties?
Explanation
Question 46
A 19-year-old male presents with persistent knee pain. Radiographs demonstrate a large, ill-defined, mixed lytic and sclerotic lesion in the distal femoral metaphysis with a 'sunburst' periosteal reaction. Biopsy confirms high-grade, conventional intramedullary osteosarcoma. He undergoes neoadjuvant chemotherapy followed by wide surgical resection. Pathologic examination of the resected specimen reveals 95% tumor necrosis. What is the primary clinical significance of this pathologic finding?
Explanation
Question 47
A 35-year-old woman with advanced rheumatoid arthritis presents with progressive neck pain and occipital headaches. Lateral flexion-extension radiographs of the cervical spine demonstrate 9 mm of anterior atlantoaxial subluxation (AAS). The posterior atlantodental interval (PADI) measures 12 mm. Physical examination reveals diffuse hyperreflexia and a positive Babinski sign. What is the most appropriate definitive management?
Explanation
Question 48
A 22-year-old collegiate football player sustains a complete rupture of the anterior cruciate ligament (ACL) and opts for reconstruction using a bone-patellar tendon-bone (BTB) autograft. When comparing this specific graft choice to a quadrupled hamstring autograft, which of the following is the most commonly reported donor-site complication?
Explanation
Question 49
A 12-year-old boy with obesity presents with left hip pain and an obligatory external rotation during hip flexion. He is diagnosed with a slipped capital femoral epiphysis (SCFE). Which of the following is the strongest indication for prophylactic pinning of the asymptomatic contralateral hip?
Explanation
Question 50
A 65-year-old woman undergoes open reduction and internal fixation of a distal radius fracture with a volar locking plate. Six months postoperatively, she suddenly loses the ability to actively flex her thumb interphalangeal joint. Which of the following is the most likely cause of this complication?
Explanation
Question 51
A 55-year-old man undergoes total hip arthroplasty using a highly cross-linked polyethylene (HXLPE) liner and a cobalt-chromium femoral head. Ten years later, he is asymptomatic, and radiographs show no evidence of osteolysis. Compared to conventional ultra-high molecular weight polyethylene (UHMWPE), what is the primary mechanism by which HXLPE reduces the incidence of osteolysis?
Explanation
Question 52
A 10-year-old boy (Tanner stage I) sustains an anterior cruciate ligament (ACL) tear. His parents opt for surgical reconstruction due to recurrent instability. To minimize the risk of physeal arrest and subsequent growth disturbance, which of the following techniques is most appropriate?
Explanation
Question 53
A 45-year-old woman presents with neck pain radiating down her right arm. Physical examination reveals weakness in wrist extension, a diminished brachioradialis reflex, and numbness over the dorsal aspect of the thumb and index finger. Which cervical nerve root is most likely compressed?
Explanation
Question 54
A 16-year-old boy is diagnosed with high-grade conventional osteosarcoma of the distal femur without pulmonary metastases. He receives neoadjuvant chemotherapy, undergoes wide local excision, and the tumor necrosis rate in the resected specimen is found to be 95%. Which of the following represents the most significant prognostic factor for long-term survival in this patient?
Explanation
Question 55
A 22-year-old man falls on an outstretched hand and presents with anatomic snuffbox tenderness. Radiographs show a displaced fracture of the proximal pole of the scaphoid. He is informed that he is at high risk for avascular necrosis (AVN) and nonunion. This risk is primarily due to the scaphoid's blood supply, which predominantly enters the bone at which location?
Explanation
Question 56
A 42-year-old recreational athlete sustains an acute Achilles tendon rupture while playing tennis. He opts for functional rehabilitation utilizing an early weight-bearing protocol in a functional orthosis. Compared to surgical repair, which of the following is true regarding this nonoperative treatment strategy?
Explanation
Question 57
A transverse midshaft femur fracture is treated with a rigid locked intramedullary nail, resulting in a small gap with very low interfragmentary strain (< 2%). According to Perren's strain theory, what type of tissue will predominantly form in the fracture gap during the healing process?
Explanation
Question 58
A 28-year-old motorcyclist is brought to the trauma bay after a high-speed collision. Radiographs demonstrate widening of the pubic symphysis of 3.5 cm and widening of the anterior sacroiliac joints bilaterally. The posterior sacroiliac ligaments appear intact on CT scan. According to the Young-Burgess classification, which of the following is the most likely associated systemic injury or complication?
Explanation
Question 59
A 68-year-old man who underwent a total hip arthroplasty 5 years ago with a cobalt-chromium head and highly cross-linked polyethylene liner on a titanium stem presents with insidious onset of groin pain. Inflammatory markers are within normal limits. Aspiration yields fluid with 500 WBCs/uL (mostly mononuclear), but serum metal ions show isolated elevated cobalt levels. What is the most likely source of the cobalt?
Explanation
Question 60
A 25-year-old man sustains a displaced, Pauwels type III femoral neck fracture after a high-energy motor vehicle collision. Which of the following fixation constructs offers the highest biomechanical stability against shear forces for this specific fracture pattern?
Explanation
Question 61
A 32-year-old manual laborer presents with progressive dorsal wrist pain and decreased grip strength. Radiographs show sclerosis and fragmentation of the lunate, with negative ulnar variance. The carpal height ratio is maintained. Which of the following is the most appropriate surgical treatment?
Explanation
Question 62
A 72-year-old man undergoes a wide L4-L5 decompressive laminectomy for spinal stenosis. Intraoperatively, a dural tear is encountered and primarily repaired with 4-0 nonabsorbable suture. Postoperatively, the patient develops a positional headache, and clear fluid is noted draining from the wound. Neurologic exam is normal. What is the most appropriate initial step in management?
Explanation
Question 63
A 13-year-old boy with a BMI of 32 presents with 3 weeks of left knee pain and an antalgic gait. He is able to bear weight on the affected limb. Radiographs demonstrate a mild left slipped capital femoral epiphysis (SCFE). Which of the following accurately describes the anatomic displacement that occurs in SCFE?
Explanation
Question 64
A 42-year-old man sustains an acute Achilles tendon rupture while playing basketball. He elects for nonoperative management utilizing a functional rehabilitation protocol. Compared to traditional surgical repair, current evidence suggests nonoperative functional rehabilitation is associated with:
Explanation
Question 65
A 19-year-old female collegiate soccer player is undergoing an anterior cruciate ligament (ACL) reconstruction. The surgeon discusses the use of a bone-patellar tendon-bone (BTB) autograft versus a hamstring autograft. When comparing these two graft choices, the BTB autograft is generally associated with a higher incidence of:
Explanation
Question 66
A 35-year-old man undergoes open reduction and internal fixation of a diaphyseal radius fracture with a compression plate and lag screw. During the healing process of a fracture treated with this type of absolute stability, which mechanism of bone healing predominates?
Explanation
Question 67
A 14-year-old boy presents with progressive distal thigh pain. Radiographs reveal a destructive, mixed lytic and sclerotic lesion in the distal femoral metaphysis with a 'sunburst' periosteal reaction. A core needle biopsy confirms a high-grade intramedullary osteosarcoma. Which of the following genetic alterations is most strongly associated with the pathogenesis of this tumor?
Explanation
Question 68
A 70-year-old woman undergoes a reverse total shoulder arthroplasty (rTSA) for massive rotator cuff tear arthropathy. The Grammont reverse design fundamentally alters the biomechanics of the glenohumeral joint to restore active forward elevation. Which of the following best describes the biomechanical change induced by the rTSA?
Explanation
Question 69
Ceramic-on-ceramic (CoC) bearing surfaces in total hip arthroplasty are known for excellent wear characteristics. Which of the following is the most commonly cited cause of squeaking in a CoC THA?
Explanation
Question 70
A 28-year-old male sustains a high-energy motor vehicle collision resulting in a Hawkins type III fracture of the talar neck. Which of the following accurately describes the fracture pattern and the associated risk of avascular necrosis (AVN)?
Explanation
Question 71
A 13-year-old obese male presents with 3 weeks of left knee pain and a limp. Examination reveals obligate external rotation of the left hip with passive flexion. Radiographs confirm a mild stable slipped capital femoral epiphysis (SCFE). Which of the following is the most appropriate definitive management?
Explanation
Question 72
A 65-year-old man presents with progressive clumsiness in his hands, difficulty buttoning his shirts, and a broad-based gait. Physical examination reveals a positive Hoffmann sign bilaterally and hyperreflexia in the lower extremities. MRI of the cervical spine shows severe stenosis at C4-C5 and C5-C6 with T2 signal change in the spinal cord. What is the most appropriate management?
Explanation
Question 73
During an anterior cruciate ligament (ACL) reconstruction, positioning the femoral tunnel too anteriorly (shallow) will result in which of the following graft behaviors during knee range of motion?
Explanation
Question 74
Following a zone II flexor tendon repair of the index finger, a patient is placed in an early active mobilization protocol. Which of the following is the primary physiological advantage of early active motion compared to prolonged immobilization?
Explanation
Question 75
Which of the following cytokines is most responsible for the differentiation of macrophages into osteoclasts during bone remodeling and fracture healing?
Explanation
Question 76
A 55-year-old patient with long-standing poorly controlled diabetes presents with a swollen, erythematous, and warm left foot. Radiographs reveal fragmentation and periarticular debris at the tarsometatarsal joints. Which of the following is the most appropriate initial management for this acute condition?
Explanation
Question 77
A 16-year-old male presents with persistent distal thigh pain. Imaging reveals a destructive, bone-forming lesion in the distal femoral metaphysis with a 'sunburst' periosteal reaction. Biopsy confirms a high-grade intramedullary osteosarcoma. What is the standard sequence of treatment for this patient?
Explanation
Question 78
A 68-year-old woman is evaluated for a stiff and painful total knee arthroplasty (TKA) 2 years postoperatively. Her range of motion is 10 to 80 degrees. Radiographs show a well-fixed TKA, but the joint line is elevated, and the patella appears significantly inferior to the joint line. Which of the following intraoperative technical errors is the most likely cause of this presentation?
Explanation
Question 79
A 35-year-old male is brought to the emergency department after a high-speed motor vehicle collision. He has an anteroposterior compression type III (APC-III) pelvic ring injury. A pelvic binder is appropriately placed. Despite the administration of 2 units of packed red blood cells, he remains hemodynamically unstable. A Focused Assessment with Sonography for Trauma (FAST) scan is negative. What is the most appropriate next step in management?
Explanation
Question 80
A 65-year-old man presents with progressive clumsiness in his hands, frequent dropping of objects, and a wide-based, unsteady gait. Suspecting cervical spondylotic myelopathy, you perform a thorough neurologic examination. Which of the following physical examination findings is considered the most specific for this condition?
Explanation
Question 81
A 60-year-old female presents with progressive groin pain 7 years after undergoing an uncomplicated primary total hip arthroplasty. Her implants consist of a large-diameter cobalt-chromium head on a titanium stem with a highly cross-linked polyethylene liner. Radiographs show well-fixed components with no osteolysis. Laboratory analysis reveals significantly elevated serum cobalt levels with normal serum chromium levels. What is the most likely source of the elevated metal ions?
Explanation
Question 82
A 22-year-old soccer player sustains a twisting injury to his knee. Radiographs demonstrate a small, elliptical cortical avulsion fracture of the anterolateral proximal tibia. Biomechanical studies indicate that the primary anatomical structure avulsed in this injury pattern functions to resist which of the following knee motions?
Explanation
Question 83
A 50-year-old male presents with chronic wrist pain and stiffness. Radiographs demonstrate advanced Scapholunate Advanced Collapse (SLAC) with arthritis at the radioscaphoid and capitolunate joints. Which of the following articulations is classically spared from degenerative changes in this condition?
Explanation
Question 84
A 13-year-old obese boy is brought to the clinic due to left groin pain and an absolute inability to bear weight on the left leg, even with the assistance of crutches, for the past 2 days following a minor fall. Pelvic radiographs confirm a severe slipped capital femoral epiphysis (SCFE). According to the Loder classification, this patient is at the highest risk for developing which of the following complications?
Explanation
Question 85
A 15-year-old boy is diagnosed with a conventional high-grade intramedullary osteosarcoma of the distal femur. He undergoes a standardized protocol of neoadjuvant chemotherapy followed by wide surgical resection. Which of the following factors determined from the surgical specimen is the most important prognostic indicator for long-term survival?
Explanation
Question 86
A 32-year-old man sustains a closed comminuted tibial shaft fracture. Two hours later, he complains of severe leg pain refractory to intravenous opioids. His blood pressure is 110/70 mmHg (Mean Arterial Pressure = 83 mmHg). Intracompartmental pressure monitoring is performed using a side-port needle. A measured compartment pressure of at least what value would result in a Delta P strictly indicating the need for an emergent four-compartment fasciotomy?
Explanation
Question 87
Recombinant human bone morphogenetic protein-2 (rhBMP-2) is utilized in various spine and trauma applications to promote osteoinduction and bone healing. What is the primary intracellular signaling pathway directly activated upon BMP-2 binding to its cell surface receptor?
Explanation
Question 88
A 42-year-old recreational athlete sustains an acute mid-substance Achilles tendon rupture. After an extensive discussion regarding treatment options, the patient elects for functional rehabilitation (nonoperative management with early weight-bearing in an orthosis) over surgical repair. Based on recent Level I evidence and meta-analyses, how does the expected clinical outcome of this approach compare to open surgical repair?
Explanation
Question 89
A 65-year-old man presents with persistent right groin pain 5 years after undergoing a primary metal-on-polyethylene total hip arthroplasty. Aspiration of the hip yields clear fluid with a negative Gram stain and negative cultures. Laboratory workup reveals substantially elevated serum cobalt levels with normal chromium levels. Which of the following is the most likely source of the metal ions?
Explanation
Question 90
A 42-year-old patient sustains a high-energy bicondylar tibial plateau fracture. Computed tomography reveals a large, vertically oriented, displaced posteromedial shear fragment. The surgical plan includes anti-glide buttress plating of this specific fragment. Which surgical interval provides the most direct and appropriate access?
Explanation
Question 91
A 12-year-old boy presents with right hip pain and an obligatory external rotation with hip flexion. Radiographs confirm a stable slipped capital femoral epiphysis (SCFE) on the right. In which of the following clinical scenarios is prophylactic in situ pinning of the asymptomatic, contralateral (left) hip most strongly indicated?
Explanation
Question 92
When evaluating graft choices for anterior cruciate ligament (ACL) reconstruction, understanding their native biomechanical properties is critical. Compared to the intact native ACL (ultimate tensile load ~2160 N), which of the following graft options has the highest ultimate tensile load at the time of implantation?
Explanation
Question 93
A 68-year-old man with cervical spondylotic myelopathy presents with worsening hand clumsiness, a positive Hoffman reflex, and gait instability. Preoperative magnetic resonance imaging (MRI) of the cervical spine is obtained. Which of the following MRI findings correlates most strongly with irreversible spinal cord damage and a poor prognosis for neurologic recovery after surgical decompression?
Explanation
Question 94
During a flexor tendon repair in Zone II of the index finger, a surgeon must manage the flexor tendon sheath carefully. To maintain the mechanical advantage of the flexor tendons and prevent clinically significant bowstringing, which two pulleys must be optimally preserved or reconstructed?
Explanation
Question 95
A 55-year-old patient with poorly controlled type 2 diabetes and peripheral neuropathy presents with a warm, swollen, and erythematous right foot. Radiographs demonstrate periarticular bony fragmentation, debris, and midfoot subluxation. According to the Eichenholtz classification of Charcot arthropathy, which stage does this represent?
Explanation
Question 96
A 16-year-old male recently completed neoadjuvant chemotherapy for an osteosarcoma of the distal femur and subsequently undergoes wide local excision. Pathologic analysis of the resected specimen is performed. Which of the following factors is the most important independent prognostic indicator for overall survival in this patient?
Explanation
Question 97
A 30-year-old patient undergoes an antegrade reamed intramedullary nailing of a diaphyseal femur fracture utilizing dynamic locking holes. This mechanical construct permits controlled axial micromotion. This relative stability primarily promotes fracture healing through which of the following biological processes?
Explanation
Question 98
A 28-year-old woman is brought to the trauma bay following a high-speed motor vehicle collision. Pelvic radiographs demonstrate a symphysis pubis diastasis of 3.5 cm and widening of the anterior sacroiliac joints bilaterally. The posterior sacroiliac complex appears intact, and there is no vertical displacement of the hemipelvis. According to the Young-Burgess classification system, this injury pattern is best categorized as:
Explanation
Question 99
A 62-year-old man presents with progressive right groin pain and a palpable anterior thigh mass 7 years after undergoing a primary total hip arthroplasty. His implants include a highly cross-linked polyethylene liner, a titanium alloy femoral stem, and a cobalt-chromium femoral head. Serum cobalt levels are 8.5 ppb and chromium is 1.2 ppb. Aspiration of the hip yields synovial fluid with 1,200 WBC/µL and 60% polymorphonuclear leukocytes. Cultures are negative at 7 days. Metal artifact reduction sequence (MARS) MRI demonstrates a large, thick-walled solid and cystic mass compressing the femoral vein. During revision surgery, severe mechanically assisted crevice corrosion (MACC) is noted at the modular head-neck junction. The femoral stem is found to be solidly fixed with no evidence of loosening. Which of the following is the most appropriate definitive management of the femoral side?
Explanation
Question 100
A 28-year-old man is brought to the trauma center after a high-speed motorcycle collision. Radiographs reveal an isolated, highly displaced, vertically oriented basicervical femoral neck fracture (Pauwels type III). Open reduction and internal fixation is planned. Which of the following fixation constructs is most biomechanically appropriate to resist the predominant deforming forces in this specific fracture pattern?
Explanation
None
