Full Question & Answer Text (for Search Engines)
Question 1:
Which of the following is not a typical characteristic of Scheuermannâ s kyphosis:
Options:
- Endplate irregularity
- Wedging of three vertebrae
- Narrowing of disk space
- Schmorlâ s nodes
- C urve apex at or above T8
Correct Answer: C urve apex at or above T8
Explanation:
Scheuermannâ s kyphosis may affect any region of the thoracic spine; it also may affect the thoracolumbar junction or the lumbar spine. Endplate irregularity, wedging of three vertebrae, narrowing of disk space, and Schmorls nodes are characteristic of Scheuermanns kyphosis.
Question 2:
A 17-year-old boy presents with thoracic kyphosis. He has minimal discomfort in his back. Radiographs show a 62° Scheuermanns kyphosis, with wedging of T8-T10. His Risser sign is 4, and his Tanner stage is 4. He states that he is not cosmetically aware of his kyphosis. Recommended treatment includes:
Options:
- A Milwaukee brace
- A Boston brace
- A posterior spine fusion
- An anterior and posterior spine fusion
- Observation
Correct Answer: Observation
Explanation:
This patient is too skeletally mature to benefit from bracing. Bracing is not likely to change the natural history of the curve at maturity. Surgery is indicated if a patient experiences pain or dissatisfaction with the appearance of the back. Otherwise, the natural history is benign and observation is indicated.
Question 3:
Adults with untreated Scheuermannâ s kyphosis do not differ from controls in terms of this parameter:
Options:
- Pulmonary function
- Severity of back pain
- Activity levels in job
- Location of greatest backache
- Presence of scoliosis
Correct Answer: Pulmonary function
Explanation:
Patients with Scheuermannâ s kyphosis have no decrease in pulmonary function compared to controls; however, they have increased severity of back pain, seek jobs with lower activity levels, and have more thoracic back pain and less trunk extension. They also have a 30% incidence of scoliosis of less than 35°.
Question 4:
Correction of Scheuermannâ s kyphosis from a posterior approach involves this mechanical principle:
Options:
- C ompression of the posterior column of the spine
- Distraction of the posterior column
- Transverse approximation
- Rod rotation
- Hemiepiphyseodesis
Correct Answer: C ompression of the posterior column of the spine
Explanation:
Compression of the posterior column is the principal method of correcting Scheuermannâ s kyphosis. Compresssion is usually achieved by resecting portions of the elongation.
Question 5:
A 13-year-old boy has a Scheuermanns kyphosis of 68°, apex at T8. His Risser sign is 1. His mother is concerned about his appearance and possible future progression. Recommended treatment includes:
Options:
- A Milwaukee brace
- Exercise
- A posterior spine fusion
- An anterior and posterior spine fusion
- Observation
Correct Answer: A Milwaukee brace
Explanation:
Brace treatment for Scheuermannâ s kyphosis is successful in decreasing the kyphosis, usually permanently, by 10° to 20° if worn properly. A patientâ s Risser sign must be below 3. Because this patient has a Risser sign of 1, bracing is appropriate treatment. The Milwaukee brace is the most effective type of brace for kyphosis. However, the Boston brace is also somewhat effective in treating patients with Scheuermannâ s kyphosis because it corrects the compensatory lordosis and stimulates active correction of the thoracic curve.
Question 6:
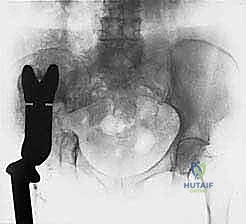
The mother of a 4-month-old boy brings him to a physician to be evaluated for a swollen leg (Slide). The most likely diagnosis is:
Options:
- Rickets
- Osteogenesis imperfecta (OI)
- Scurvy
- Nonaccidental injury
- C affeys disease
Correct Answer: Nonaccidental injury
Explanation:
This radiograph shows two fractures in different stages of healing. Note the old femur fracture at the top of the field. No evidence of decreased cortical thickness, diaphyseal thinning, or bowing suggests OI. The physis of the distal femur and proximal femur show no signs of rickets. The presence of fractures rather than periosteal reaction make C affeyâ s disease unlikely. The fractures in scurvy are more commonly located in the physis. The diagnosis of nonaccidental injury should be made only after performing a thorough patient history and physical.
Question 7:
Which of the following is not a contraindication to the repair of a spondylolytic defect:
Options:
- Age older than 35 years
- Slip greater than 25%
- Disk degeneration at the same level
- Bilateral pars defect
- Minimal symptoms
Correct Answer: Bilateral pars defect
Explanation:
Repair of a spondylolytic defect is usually a successful procedure for relieving symptoms. Repair is not indicated in patients older than 35 years of age. Repair should not be done if there is a significant slip over a grade 1 at most or if the patient has minimal, tolerable symptoms or has symptoms complicated by a degenerative disk at the same level.
Question 8:
A 14-year-old boy has grade 1 isthmic L5-S1 spondylolisthesis. He has no back pain and wants to play football. The patient should be advised to:
Options:
- Play football if his condition is treated by grafting and wiring
- Play football if he has a L5-S1 fusion
- Play football if he wears a lumbosacral orthosis during all games
- Not play football at all
- Play football as desired
Correct Answer: Play football if his condition is treated by grafting and wiring
Explanation:
Asymptomatic spondylolisthesis occurs in approximately 5% of the pediatric population. Slips of up to grade 1 develop in at least one third of patients with asymptomatic spondylolisthesis. Most patients with asymptomatic spondylolisthesis are minimally symptomatic or asymptomatic. The patient presented in this scenario may be allowed to play football as long as he understands that he may develop symptoms.
Question 9:
Most cases of L5 spondylolysis develop in patients by:
Options:
- Birth
- Age 3 years
- Age 6 years
- Age 9 years
- Age 12 years
Correct Answer: Age 6 years
Explanation:
A study was conducted to monitor the development of L5 spondylolysis in patients from birth to 6 years of age. The study showed that no cases of L5 spondylolysis were present at birth in any of the patients. The majority of the patients developed L5 spondylolysis by the time they had reached 6 years of age. A 45-year follow-up study showed that none of the 30 patients had more than a 40% slip and that only 1 patient required fusion.
Question 10:
Patients with high-grade spondylolisthesis develop a vertical position of the sacrum in response to which condition:
Options:
- Lumbar lordosis
- Tight hamstrings
- Olisthetic scoliosis
- Lumbar kyphosis
- Lumbosacral kyphosis
Correct Answer: Lumbar kyphosis
Explanation:
As spondylolisthesis progresses to a high grade, the fifth lumbar vertebra shifts forward into a kyphotic position termed a slip angle. The slip angle can reach a value of more than 30° and results in verticalization of a patients sacrum to decrease force on the involved vertebra.
Question 11:
Which of the following is not a feature of Klippel-Trénaunay-Weber syndrome:
Options:
- Varicose veins
- C utaneous nevus
- Increased length of the involved limb
- Increased width of the involved limb
- Seizure disorder
Correct Answer: Seizure disorder
Explanation:
Klippel-Trnaunay-Weber syndrome is a constellation of varicose veins, cutaneous nevus, and an increase in the length or width of the involved limb. Seizure disorder is a feature of von Hippel- Lindau disease.
Question 12:
Epiphyseal osteochondroma is also known as:
Options:
- Mafuccis syndrome
- Freibergs fracture
- Larsen-Johansson disease
- Trevors disease
- Iselins disease
Correct Answer: Trevors disease
Explanation:
Epiphyseal osteochondroma is also known as Trevorâ s disease. Epiphyseal osteochondroma is localized to a specific region of the body, unlike multiple osteochondroma, which affects the entire body. Epiphyseal osteochondroma and multiple osteochondroma are unrelated disorders.
Question 13:
All of the disorders listed below are examples of osteochondrosis except:
Options:
- Legg-Calv-Perthes disease
- Scheuermannâ s disease
- Osgood Schlatter disorder
- Gorhams disease
- Blount disease
Correct Answer: Gorhams disease
Explanation:
The term osteochondrosis refers to symptomatic disorders involving cartilage growth. Cartilage affected by osteochondrosis may be epiphyseal, physeal, or apophyseal. Gorhamâ s disease is not an example of osteochondrosis. Gorhams disease is a lymphatic disorder known as disappearing bone disease.
Question 14:
Which of the following symptoms is not characteristic of congenital constriction band syndrome:
Options:
- C ircular grooves in the limb
- C omplex complete syndactyly
- Terminal amputations
- C lubfoot
- Lymphedema
Correct Answer: C omplex complete syndactyly
Explanation:
Syndactyly in constriction band syndrome is a fenestrated syndactyly, is incomplete, and has slits between the digits proximally. Syndactyly in constriction band syndrome is also not complex because the bones are not fused.
Question 15:
Which of the following conditions requires an ultrasound of the abdomen:
Options:
- Russell-Silver syndrome
- C amurati-Engelmann disease
- Idiopathic hemihypertrophy
- Congenital constriction band syndrome
- Blue rubber bleb nevus syndrome
Correct Answer: Idiopathic hemihypertrophy
Explanation:
An ultrasound of the abdomen is indicated for patients with idiopathic hemihypertrophy to determine the development of Wilms tumor. Children with idiopathic hemihypertrophy have an increased incidence of Wilmsâ tumor. C hildren require periodic monitoring, and they should have an abdominal ultrasound 2 to 3 times per year until 8 years of age.
Question 16:
How often should patients with hemihypertrophy have an abdominal ultrasound:
Options:
- Once at 2 years old
- Yearly until 5 years old
- Two to three times per year until 8 years old
- Quarterly until 18 years old
- Yearly until 18 years old
Correct Answer: Two to three times per year until 8 years old
Explanation:
Patients with idiopathic hemihypertrophy require periodic monitoring to determine the risk of Wilms tumor. The best method to monitor patients with idiopathic hemihypertrophy is a renal ultrasound two to three times per year until the patient is 8 years of age.
Question 17:
Which of the following rays is most commonly used to treat patients with macrodactyly of the foot:
Options:
- First
- Second
- Third
- Fourth
- Fifth
Correct Answer: Second
Explanation:
The second ray is most commonly used to treat patients with macrodactyly of the foot. The third ray is the next most commonly used ray in treating patients with macrodactyly of the foot.
Question 18:
Macrodactyly of the foot commonly displays which of the following patterns of overgrowth:
Options:
- Greatest dorsally and distally
- Greatest plantarly and distally
- Greatest plantarly and proximally
- Greatest laterally and distally
- Greatest medially and proximally
Correct Answer: Greatest plantarly and distally
Explanation:
Macrodactyly displays overgrowth that is greatest plantarly and distally. Plantar overgrowth causes the sole to become convex plantarly and the toes to become dorsiflexed.
Question 19:
A 1-year-old patient presents with a pseudarthrosis of the left clavicle. Which of the following conditions is most likely to coexist with pseudarthrosis of the left clavicle:
Options:
- Neurofibromatosis
- Proteus syndrome
- Osteogenesis imperfecta
- Fibrous dysplasia
- Dextrocardia
Correct Answer: Neurofibromatosis
Explanation:
Almost all cases of congenital pseudarthrosis involve the right clavicle. C ases of congenital pseudarthrosis involving the left clavicle often coexist with dextrocardia. Patients with pseudarthrosis of the clavicle respond well to standard orthopedic treatment, unlike patients with congenital pseudarthrosis of the tibia.C orrect Answer: Dextrocardia
Question 20:
A 14-year-old girl presents with a swollen foot. She had sustained a contusion to the dorsum of her foot for 4 weeks. Her temperature is 99.2° F. Her foot is tender to touch. She is able to dorsiflex and plantarflex her toes. Radiographs are normal. The best treatment is:
Options:
- Physical therapy
- Ankle block
- Sciatic block
- Ankle joint aspiration
- Blood culture
Correct Answer: Physical therapy
Explanation:
This patient demonstrates signs of early reflex sympathetic dystrophy. She may later develop osteopenia, a positive bone scan, and contracture. Physical therapy is the best treatment for reflex sympathetic dystrophy in this case because it will increase the patients range of movement and her tolerance to touch. Multimodality therapy is also required to treat reflex sympathetic dystrophy. Analgesics may be appropriate treatment for the patient and can be supplemented by antidepressants, if needed. Repeated regional block treatment is recommended for patients with established cases of reflex sympathetic dystrophy.