Diagnostic Approach to Median Nerve Schwannoma: A Detailed Orthopedic Case Study
Key Takeaway
Median nerve schwannoma diagnosis involves progressive pain, paresthesia, and a palpable forearm mass, often with a positive Tinel's sign. Clinical examination reveals neurological deficits. MRI is key, demonstrating a characteristic 'target sign' on T2-weighted images and avid, heterogeneous post-contrast enhancement, confirming the nerve's involvement and guiding further management.
Patient Presentation and History
A 48-year-old right-hand dominant male presented to the orthopedic oncology clinic with a chief complaint of progressive right forearm pain, paresthesia, and a palpable mass. The patient reported an insidious onset of symptoms approximately 10 months prior to presentation. Initially, the pain was intermittent, described as a deep ache localized to the volar aspect of the distal forearm, occasionally radiating into the thumb, index, and middle fingers. Over the past 4 months, the pain had become constant, exacerbated by repetitive wrist movements and direct pressure on the mass. He also reported a subjective increase in numbness and tingling in the median nerve distribution, accompanied by a perceived decrease in grip strength and difficulty with fine motor tasks, such as buttoning shirts.
His past medical history was significant for well-controlled essential hypertension, managed with an angiotensin-converting enzyme inhibitor, and mild osteoarthritis of the knees. There was no personal or family history of neurofibromatosis or other genetic syndromes predisposing to nerve sheath tumors. He denied any history of trauma to the affected limb, previous surgeries, or infections. He was a non-smoker and consumed alcohol socially. His occupational history involved prolonged desk work with extensive computer use, which he initially attributed his symptoms to, attempting self-management with ergonomic adjustments and over-the-counter non-steroidal anti-inflammatory drugs, none of which provided significant relief. The progressive nature of his neurological symptoms, despite conservative measures, prompted his referral to the orthopedic oncology service.
Epidemiological and Pathophysiological Context
Peripheral nerve sheath tumors represent a distinct subset of soft tissue neoplasms encountered in orthopedic oncology, with schwannomas being the most common benign peripheral nerve sheath tumor. Arising from the Schwann cells that form the myelin sheath of peripheral nerves, these tumors are typically slow-growing, encapsulated, and solitary. The presentation of this 48-year-old patient aligns with the peak incidence of sporadic schwannomas, which typically occur in the third to fifth decades of life. The absence of a family history or clinical stigmata of neurofibromatosis type 1 or type 2, or schwannomatosis, strongly suggests a sporadic etiology.
The insidious progression of symptoms over a 10-month period is characteristic of benign nerve sheath tumors. Due to their slow growth rate, the affected nerve can often accommodate the expanding mass through fascicular displacement and axonal stretching before ischemic or compressive neuropathy becomes clinically apparent. The transition from intermittent, activity-related deep aching to constant pain, coupled with progressive motor and sensory deficits, indicates critical compression of the functional fascicles within the epineurium, necessitating definitive diagnostic and therapeutic intervention.
Clinical Examination Findings
Inspection and Palpation Assessment
On inspection of the right upper extremity, there was a subtle, localized fusiform fullness visible on the volar aspect of the distal forearm, approximately 8 cm proximal to the wrist crease, slightly radial to the midline. No skin discoloration, erythema, atrophy, or trophic changes were noted. The overall alignment of the limb appeared normal.
Palpation revealed a firm, well-circumscribed, ovoid mass, approximately 3 x 2 cm in size, situated deep within the flexor compartment of the forearm. The mass was mobile in a transverse plane but restricted longitudinally, consistent with a nerve sheath tumor tethered to its nerve of origin. This specific mobility pattern is a hallmark clinical sign differentiating intraneural pathology from extraneural soft tissue masses. It was mildly tender to direct palpation. A strongly positive Tinel's sign was elicited directly over the mass, producing electric-shock-like sensations radiating distally into the thumb, index, and middle fingers. There was no warmth or crepitus. Proximal and distal palpation of the median nerve revealed no additional masses or areas of tenderness, reducing the clinical suspicion for multifocal disease.
Range of Motion and Motor Evaluation
Active and passive range of motion of the wrist, elbow, and shoulder were full and pain-free, although forceful resisted wrist flexion and forearm pronation marginally aggravated the deep forearm pain, likely due to dynamic compression of the mass by the contracting flexor digitorum superficialis and pronator teres muscle bellies. Grip strength was subjectively reduced on the right side (measured at 4/5 compared to 5/5 on the left via Jamar dynamometer), and pinch strength was also mildly impaired.
Manual muscle testing revealed mild weakness in muscles innervated by the median nerve distal to the lesion:
* Flexor pollicis longus: 4+/5
* Flexor digitorum profundus to index and middle fingers: 4+/5
* Abductor pollicis brevis: 4/5
* Opponens pollicis: 4/5
* All other motor groups in the right upper extremity were 5/5.
* Mild thenar atrophy was noted on the right compared to the left, indicating early chronic axonal loss and denervation of the intrinsic thenar musculature.
Neurological and Vascular Status
Diminished sensation to light touch and pinprick was observed in the palmar aspect of the thumb, index, middle fingers, and the radial half of the ring finger, as well as the distal palmar crease, consistent with median nerve involvement. Two-point discrimination was impaired at 7mm on the right index fingertip (normal <6mm) compared to 4mm on the left.
Biceps and triceps reflexes were 2+ bilaterally and symmetric. Brachioradialis reflexes were also normal. Vascular examination demonstrated palpable and bounding radial and ulnar pulses (2+ bilaterally) with a brisk capillary refill time of less than 2 seconds in all digits. Allen's test was negative, confirming a patent superficial palmar arch.
Imaging and Diagnostics
The diagnostic workup for a suspected peripheral nerve sheath tumor requires a multimodal approach to define the anatomical location, characterize the lesion, assess the degree of nerve involvement, and plan surgical intervention.
Plain Radiography
Initial orthogonal radiographs (anteroposterior and lateral views) of the right forearm and wrist were obtained. These demonstrated normal osseous architecture with no evidence of periosteal reaction, cortical erosion, or intrinsic bone lesions. A faint, non-calcified soft tissue shadow was visible in the volar distal forearm, corresponding to the palpable mass. The primary utility of plain radiography in this context is to rule out osseous pathology, calcified lesions such as myositis ossificans, or soft tissue chondromas.
High Resolution Ultrasound
High-resolution ultrasound was utilized as an immediate, dynamic adjunct in the clinic. Sonographic evaluation revealed a well-defined, hypoechoic, solid ovoid mass measuring 3.1 x 1.9 x 1.8 cm within the distal forearm. The mass was in direct continuity with the median nerve at its proximal and distal poles. Posterior acoustic enhancement was noted, a common feature in cellular tumors like schwannomas. Color Doppler interrogation demonstrated minimal internal vascularity. The dynamic evaluation confirmed the mass moved with the median nerve during passive wrist flexion and extension, solidifying the diagnosis of a peripheral nerve sheath tumor.

Magnetic Resonance Imaging Protocols
Magnetic Resonance Imaging with and without intravenous gadolinium contrast is the gold standard for evaluating peripheral nerve sheath tumors. The patient underwent a dedicated peripheral nerve MRI protocol of the right forearm.
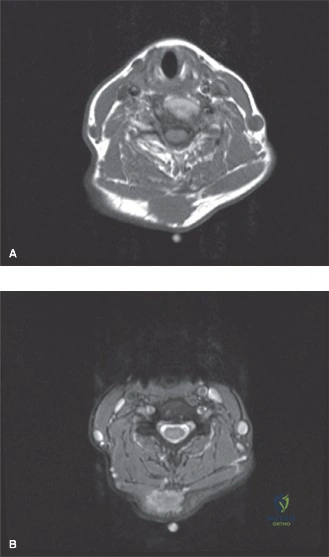
T1 Weighted Sequences: The mass demonstrated isointense signal relative to the adjacent skeletal muscle. The "split-fat sign" was distinctly visible at the proximal and distal poles of the tumor, representing a rim of normal perineural adipose tissue displaced by the slowly expanding intraneural mass.
T2 Weighted and STIR Sequences: On fluid-sensitive sequences, the mass exhibited a hyperintense signal. A classic "target sign" was observed, characterized by a hyperintense peripheral rim and a centrally hypointense core. This imaging phenomenon corresponds histologically to the peripheral hypocellular, myxoid Antoni B tissue and the central hypercellular Antoni A tissue. Furthermore, the "fascicular sign" was evident, displaying multiple small ring-like structures within the lesion, representing displaced but intact nerve fascicles splayed over the capsule of the tumor.
Post Contrast Sequences: Following gadolinium administration, the mass demonstrated avid, heterogeneous enhancement. The central portion (Antoni A areas) typically enhances more robustly than the peripheral myxoid regions.
Electrodiagnostic Studies
To quantify the degree of functional impairment and establish a baseline prior to surgical intervention, Electromyography and Nerve Conduction Studies were ordered.
Nerve Conduction Studies demonstrated prolonged distal motor latencies and decreased compound muscle action potential amplitudes in the right median nerve recording from the abductor pollicis brevis. Sensory nerve action potentials for the median nerve were also diminished in amplitude with prolonged peak latencies. Ulnar and radial nerve conduction parameters were within normal limits.
Electromyography revealed increased insertional activity, positive sharp waves, and fibrillation potentials in the abductor pollicis brevis and opponens pollicis, indicating active denervation. Motor unit action potentials showed reduced recruitment patterns. The flexor pollicis longus and flexor digitorum profundus demonstrated mild neurogenic changes. These findings confirmed a focal, severe median neuropathy localized to the distal forearm, correlating perfectly with the anatomical location of the mass.
Differential Diagnosis
The clinical and radiographic presentation of a soft tissue mass in the volar forearm with associated neurological symptoms necessitates a precise differential diagnosis. Distinguishing between various peripheral nerve sheath tumors and non-neurogenic soft tissue masses is critical for surgical planning.
| Pathology | Clinical Features | MRI Characteristics | Malignant Potential |
|---|---|---|---|
| Schwannoma | Eccentric to nerve, mobile transversely, positive Tinel's, slow growth. | Target sign, fascicular sign, split-fat sign. Isointense T1, hyperintense T2, avid enhancement. Encapsulated. | Extremely rare malignant transformation. |
| Neurofibroma | Central to nerve, fusiform swelling, often associated with NF1. | Target sign may be present. Inseparable from normal nerve fascicles. Central enhancement. Unencapsulated. | Low (sporadic) to moderate (plexiform in NF1). |
| Malignant Peripheral Nerve Sheath Tumor | Rapid growth, severe pain, progressive severe neurological deficit, history of prior radiation or NF1. | Large size (>5cm), ill-defined margins, perilesional edema, heterogeneous enhancement, necrosis, hemorrhage. | High. Aggressive sarcoma requiring wide margins. |
| Ganglion Cyst | Fluctuant mass, variable pain, transilluminates. May compress adjacent nerves (e.g., ulnar nerve in Guyon's canal). | Well-circumscribed, lobulated. Hypointense T1, markedly hyperintense T2. Rim enhancement only. | None. |
| Lipoma | Soft, doughy mass, painless unless compressing a nerve, slow growth. | Isointense to subcutaneous fat on all sequences. Suppresses on fat-sat sequences. No enhancement. | Extremely rare (atypical lipomatous tumor). |
Diagnostic Differentiation
Differentiating between a schwannoma and a neurofibroma is the most critical and challenging aspect of the preoperative evaluation. Schwannomas arise eccentrically from a single nerve fascicle and displace the remaining functional fascicles over their well-defined epineurial capsule. This anatomical arrangement allows for surgical enucleation with a high probability of preserving neurological function.
Conversely, neurofibromas are unencapsulated tumors that infiltrate the nerve, growing intrinsically between and within multiple fascicles. The fascicles are inextricably intertwined with the tumor matrix. Consequently, complete resection of a neurofibroma typically requires resection of the involved nerve segment, leading to inevitable neurological deficit, unless the tumor involves a purely sensory, non-critical branch. The eccentric nature of the mass on MRI, combined with the classic target and fascicular signs in a patient without neurofibromatosis, strongly favored the diagnosis of a schwannoma in this case.
Surgical Decision Making and Classification
Indications for Operative Intervention
The decision to proceed with surgical intervention was based on several compelling factors. Firstly, the patient was experiencing progressive, unrelenting pain that was refractory to conservative management and significantly impacting his quality of life and occupational function. Secondly, there was objective clinical and electrodiagnostic evidence of progressive motor and sensory deficits. Prolonged compression of the median nerve by the expanding tumor mass leads to localized ischemia, myelin degradation, and eventually Wallerian degeneration of the distal axons. If left untreated, the chronic denervation would result in irreversible muscle atrophy and permanent functional impairment of the hand.
Thirdly, while the clinical and radiographic features were highly suggestive of a benign schwannoma, definitive histopathological diagnosis is required to categorically rule out malignancy, although a core needle biopsy is generally contraindicated for suspected benign nerve sheath tumors due to the high risk of iatrogenic fascicular injury and induction of severe neuropathic pain.
Enneking Staging and Surgical Goals
According to the Enneking classification system for benign musculoskeletal tumors, this lesion was classified as a Stage 2 (active) benign tumor. It was symptomatic, slowly enlarging, and causing localized compression of surrounding structures, but remained contained within its anatomical compartment and capsular boundaries.
The primary surgical goal was complete marginal excision (enucleation) of the tumor while meticulously preserving the continuity and function of the uninvolved median nerve fascicles. Unlike sarcomas, which require wide or radical resection margins, benign schwannomas can be safely treated with marginal excision along their pseudocapsule. The risk of local recurrence following complete enucleation is exceptionally low, reported to be less than 5% in the orthopedic oncology literature.
Surgical Technique and Intervention
The patient was taken to the operating room and placed in the supine position with the right upper extremity extended on a radiolucent hand table. General anesthesia was induced, avoiding long-acting paralytic agents to facilitate intraoperative nerve monitoring. A non-sterile pneumatic tourniquet was placed proximally on the brachium. The limb was prepped and draped in standard sterile orthopedic fashion. Prophylactic intravenous antibiotics (Cefazolin 2g) were administered prior to inflation of the tourniquet to 250 mmHg.
Surgical Approach and Dissection
Surgical loupe magnification (3.5x) was utilized throughout the procedure. A longitudinal incision, approximately 6 cm in length, was planned over the volar aspect of the distal forearm, centered directly over the palpable mass and following the anatomical course of the median nerve. The incision was carefully designed to avoid crossing the wrist flexion creases perpendicularly.
The skin and subcutaneous tissues were sharply divided. Hemostasis of superficial veins was achieved with bipolar electrocautery to prevent thermal injury to underlying neural structures. The antebrachial fascia was identified and incised longitudinally. The flexor carpi radialis and palmaris longus tendons were identified and retracted radially and ulnarly, respectively, exposing the flexor digitorum superficialis muscle belly.
Nerve Identification and Epineurotomy
The median nerve was first identified in virgin, unaffected tissue both proximal and distal to the tumor mass. This is a critical oncologic and microsurgical principle to ensure safe dissection and anatomical orientation. Vessel loops were passed loosely around the normal nerve proximally and distally for gentle manipulation.
Dissection proceeded toward the mass. The median nerve was found to be significantly expanded by an eccentric, yellowish, encapsulated mass measuring approximately 3.5 x 2.0 cm. The normal nerve fascicles were observed to be splayed and stretched thinly over the volar and radial aspects of the tumor capsule.
Under operative microscope magnification, a longitudinal epineurotomy was performed in a relatively avascular zone, carefully choosing an area devoid of crossing functional fascicles. The epineurium was gently elevated and retracted using fine jeweler's forceps and micro-scissors.
Fascicular Dissection and Enucleation
Once the epineurium was opened, the true capsule of the schwannoma was visualized. Using microsurgical blunt dissection techniques, the attenuated, functional nerve fascicles were meticulously separated from the tumor capsule. The plane between the tumor capsule and the surrounding fascicles is typically well-defined in schwannomas.
The tumor was progressively mobilized. It was confirmed to arise from a single, small, distinct fascicle entering the proximal pole and exiting the distal pole of the mass. Intraoperative direct nerve stimulation was utilized. Stimulation of the splayed peripheral fascicles elicited robust motor responses in the thenar musculature and forearm flexors. Stimulation of the specific fascicle of origin entering the tumor yielded no distal motor response, confirming it was a non-functional or purely sensory fascicle that had been rendered non-conductive by the tumor burden.
With the functional fascicles safely retracted and protected, the fascicle of origin was sharply transected at the proximal and distal poles of the tumor using micro-scissors. The tumor was then successfully enucleated en bloc and passed off the sterile field for permanent histopathological analysis.
Hemostasis and Closure
The remaining median nerve bed was inspected. The splayed fascicles were observed to relax and partially re-approximate following the removal of the mass effect. No attempt was made to suture the epineurium closed, as this can lead to postoperative hematoma accumulation within the nerve sheath and subsequent compressive neuropathy.
The tourniquet was deflated, and meticulous hemostasis was achieved using bipolar electrocautery and warm saline irrigation. The surgical field was heavily irrigated. The antebrachial fascia was left open to prevent compartment syndrome or localized tension. The subcutaneous tissue was approximated with interrupted 3-0 absorbable sutures, and the skin was closed with a running 4-0 subcuticular absorbable suture. A sterile, non-adherent dressing was applied, followed by a well-padded volar resting splint maintaining the wrist in a neutral position.
Histopathological Confirmation
Subsequent histopathological examination of the specimen confirmed the diagnosis of a benign schwannoma. The macroscopic description noted a well-circumscribed, encapsulated, tan-yellow mass. Microscopic evaluation revealed a classic biphasic architectural pattern. The Antoni A areas were highly cellular, consisting of spindle-shaped Schwann cells with elongated nuclei arranged in interlacing fascicles. Palisading nuclei forming Verocay bodies were prominent. The Antoni B areas were hypocellular, featuring a loose, myxoid stroma with prominent, thick-walled hyalinized blood vessels. Immunohistochemical staining demonstrated strong, diffuse positivity for S-100 protein and SOX10, confirming the neural crest origin of the tumor cells. No significant cytologic atypia, necrosis, or elevated mitotic activity was observed, ruling out malignancy.
Post Operative Protocol and Rehabilitation
The postoperative management following median nerve schwannoma enucleation requires a balance between protecting the surgical site and preventing perineural adhesions.
Immediate Post Operative Phase (Weeks 0 to 2)
The patient was discharged on the day of surgery with adequate oral analgesia and strict instructions for elevation of the affected extremity to minimize edema. The volar resting splint was maintained for 10 to 14 days to immobilize the wrist and protect the surgical incision. The patient was encouraged to perform active range of motion exercises of the fingers, elbow, and shoulder immediately to prevent stiffness and promote venous return.
At the two-week postoperative visit, the splint and dressings were removed. The surgical incision demonstrated excellent primary healing with no signs of infection or dehiscence. The patient reported immediate, near-complete resolution of the deep, aching forearm pain that had characterized his preoperative state.
Intermediate Rehabilitation Phase (Weeks 2 to 6)
Following suture removal, the patient was referred to a specialized hand/occupational therapist. The primary goals during this phase were scar management, restoration of full wrist and forearm range of motion, and the initiation of median nerve gliding exercises.
Nerve gliding exercises are critical in the postoperative period to prevent the median nerve from adhering to the surrounding surgical scar tissue within the flexor compartment. These exercises promote longitudinal excursion of the nerve, maintaining its mobility and preventing traction neuropathies during terminal ranges of motion.
The patient experienced expected transient postoperative paresthesias and hypersensitivity in the median nerve distribution, a phenomenon common after significant intraneural manipulation. Sensory re-education techniques, including the use of various textures and vibration, were initiated by the occupational therapist to help the central nervous system process the altered sensory input and reduce allodynia.
Late Rehabilitation Phase (Weeks 6 and Beyond)
Progressive strengthening exercises for the grip, pinch, and forearm musculature were introduced at six weeks postoperatively. By the three-month follow-up, the patient demonstrated full, painless range of motion of the right wrist and forearm. Grip strength had improved to 5/5, equal to the contralateral side.
The preoperative thenar atrophy stabilized, and the patient reported a significant improvement in fine motor tasks and the ability to perform his occupational duties without restriction. Sensation in the median nerve distribution improved subjectively, although mild two-point discrimination deficits (5-6mm) persisted at the index fingertip, which is an expected sequela of chronic preoperative compression and the necessary sacrifice of the fascicle of origin.
Clinical Pearls and Pitfalls
The management of peripheral nerve sheath tumors requires a high index of suspicion, precise diagnostic imaging, and meticulous microsurgical technique. The following clinical pearls and pitfalls are essential for the orthopedic surgeon managing these complex cases.
- Diagnostic Delay: Do not dismiss progressive, radiating extremity pain as simple tendinopathy or repetitive strain injury, especially when accompanied by a palpable mass or neurological deficits. A low threshold for advanced imaging (MRI) is paramount to prevent chronic, irreversible nerve damage.
- The Value of the Split-Fat Sign: On MRI, the split-fat sign is highly indicative of an intraneural tumor. It helps differentiate a nerve sheath tumor from an extraneural mass that is simply compressing the nerve from the outside.
- Biopsy Contraindications: Avoid percutaneous core needle biopsy for suspected benign peripheral nerve sheath tumors. The risk of permanent iatrogenic nerve injury far outweighs the diagnostic benefit. Diagnosis should rely on clinical presentation, MRI characteristics, and intraoperative findings.
- Microsurgical Principles: Enucleation must be performed under loop magnification or an operating microscope. Use microsurgical instruments to minimize trauma to the delicate functional fascicles.
- Identification of Normal Anatomy: Always identify the nerve in normal, unscarred tissue proximal and distal to the tumor before dissecting the mass itself. This ensures orientation and protects the main nerve trunk.
- Epineurotomy Placement: Plan the longitudinal epineurotomy in an avascular zone that avoids crossing functional fascicles.
- Managing the Fascicle of Origin: Accept that the specific fascicle from which the schwannoma arises will almost always need to be sacrificed to achieve complete enucleation. Intraoperative stimulation should be used to confirm that this fascicle is non-functional or redundant, thereby minimizing postoperative deficits.
- Patient Counseling: Preoperative counseling is critical. Patients must be informed that while the goal is to improve pain and prevent further deterioration, transient postoperative worsening of paresthesias is common due to surgical manipulation. Complete recovery of chronic sensory or motor deficits present prior to surgery is not guaranteed.
Clinical & Radiographic Imaging
