Scaphoid Fracture ORIF: A Masterclass in Dorsal Approach Technique

Key Takeaway
Welcome to the OR, fellows. Today, we're tackling open reduction and internal fixation of a scaphoid fracture via the dorsal approach. This masterclass will cover meticulous anatomical considerations, exact patient positioning, step-by-step intraoperative execution from incision to screw insertion, critical pearls to avoid pitfalls, and comprehensive postoperative care. Precision is paramount for successful scaphoid healing and preventing long-term wrist dysfunction.
Comprehensive Introduction and Patho-Epidemiology
The scaphoid represents the critical biomechanical linchpin of the carpus, functioning as the primary mechanical tie-rod between the proximal and distal carpal rows. Fractures of the scaphoid are the most frequently encountered carpal fractures in orthopaedic traumatology, accounting for nearly 70% of all carpal bone injuries and a significant proportion of emergency department presentations for acute wrist trauma. Understanding the complex nuances of this injury is absolutely paramount for successful clinical outcomes, especially given the scaphoid's notorious propensity for delayed union, nonunion, and the subsequent, often devastating, progression to radiocarpal and midcarpal arthrosis.
Epidemiologically, these fractures predominantly afflict young, active individuals, with a peak incidence in males between the ages of 15 and 30 years. The mechanism of injury is almost universally a fall onto an outstretched hand (FOOSH), where the wrist is forced into extreme dorsiflexion, ulnar deviation, and intercarpal supination. As the wrist extends beyond 95 degrees, the scaphoid waist is forcefully impacted against the dorsal rim of the distal radius, creating a bending moment that ultimately results in failure of the volar cortex followed by tension failure of the dorsal cortex. While fractures most commonly occur at the scaphoid waist (approximately 70% to 80%), 10% to 20% involve the proximal pole, and the remainder affect the distal pole or tuberosity. In pediatric populations, distal pole avulsion fractures are more frequently observed due to the relative strength of the ligamentous attachments compared to the immature ossific nucleus.
The natural history of an untreated or inadequately managed scaphoid fracture is fraught with high morbidity. The overall risk of nonunion is estimated at 5% to 10% for all scaphoid fractures, but this risk escalates exponentially with nonoperative treatment of displaced waist fractures or any fracture involving the proximal pole. The scaphoid's complex three-dimensional anatomy, combined with its precarious, retrograde blood supply, makes both operative and nonoperative management technically demanding. If left unaddressed, scaphoid nonunions follow a predictable, degenerative cascade. The loss of the scaphoid's stabilizing strut effect allows the lunate to extend, driven by the intact triquetrum, leading to a dorsal intercalated segment instability (DISI) pattern.
This kinematic uncoupling predictably progresses to a condition termed SNAC (Scaphoid Nonunion Advanced Collapse) wrist. The SNAC progression occurs in distinct stages: initially manifesting as arthrosis at the radioscaphoid articulation (specifically the radial styloid and the distal scaphoid fragment), progressing to involve the entire scaphoscaphoid and scaphocapitate joints, and eventually resulting in global carpal collapse, proximal migration of the capitate, and end-stage pancarpal arthritis. Preventing this catastrophic functional decline is the primary imperative driving modern indications for early operative intervention.
Detailed Surgical Anatomy and Biomechanics
Mastery of scaphoid anatomy is the foundational prerequisite for executing a safe and effective dorsal open reduction and internal fixation (ORIF). The scaphoid is uniquely shaped, often likened to a "twisted peanut" or a boat (from the Greek skaphos), curving in both the sagittal and coronal planes. It is almost entirely intra-articular, with over 80% of its surface covered by hyaline cartilage. It articulates with five bones: the radius proximally, the lunate ulnarly, and the capitate, trapezium, and trapezoid distally. Because it lacks direct tendinous insertions, the scaphoid relies entirely on its complex ligamentous attachments for stability, including the radioscaphocapitate (RSC) ligament volarly and the dorsal intercarpal (DIC) and scapholunate interosseous (SLIL) ligaments dorsally.
The most critical anatomical consideration—and the primary driver of its high nonunion rate—is its tenuous vascular supply. The scaphoid is perfused predominantly by branches of the radial artery. The dorsal carpal branch of the radial artery provides the dominant blood supply, entering the scaphoid through a narrow non-articular ridge on its dorsal surface. Crucially, this dorsal supply accounts for 70% to 80% of the bone's vascularity and perfuses the entire proximal pole via a retrograde endosteal network. Because the intraosseous blood flow is directed from distal to proximal, any fracture at the waist or proximal pole inherently disrupts the blood supply to the proximal fragment, rendering it highly susceptible to avascular necrosis (AVN). A secondary volar branch, entering through the distal tubercle, supplies only the remaining 20% to 30% of the bone, primarily nourishing the distal pole.
Neurovascular Risks and Muscular Intervals
When executing the dorsal approach to the scaphoid, the surgeon must meticulously navigate specific neurovascular structures and muscular intervals to avoid iatrogenic morbidity. The superficial radial nerve (SRN) courses along the radial aspect of the wrist and forearm, transitioning from deep to the brachioradialis to a subcutaneous position approximately 5 to 8 cm proximal to the radial styloid. Its branches frequently cross the surgical field; therefore, blunt subcutaneous dissection and gentle retraction are mandatory to prevent painful neuromas or disabling sensory deficits. Similarly, while the dorsal sensory branch of the ulnar nerve (DSBUN) is typically ulnar to the primary operative field, variations exist, and general vigilance is required during wide exposures.
The muscular intervals define the surgical corridor. The dorsal approach utilizes the interval between the third and fourth extensor compartments. Lister's tubercle, a prominent bony landmark on the dorsal distal radius, serves as the critical guide. The extensor pollicis longus (EPL) tendon (third compartment) angles around Lister's tubercle. By incising the extensor retinaculum and transposing the EPL radially, the surgeon gains access to the interval between the extensor carpi radialis brevis and longus (ECRB/ECRL, second compartment) radially, and the extensor digitorum communis (EDC, fourth compartment) ulnarly. This interval provides direct, extensile access to the dorsal radiocarpal capsule and the underlying proximal pole and waist of the scaphoid.
Biomechanically, the scaphoid acts as a dynamic strut. During wrist radial deviation and flexion, the scaphoid palmar flexes to avoid impingement against the radial styloid. Conversely, during ulnar deviation and extension, the scaphoid extends. A fracture disrupts this synchronous motion. The distal fragment tends to flex (driven by the STT joint and volar ligaments), while the proximal fragment extends with the lunate (driven by the intact SLIL). This opposing force creates a "humpback" deformity, leading to a loss of carpal height and a biomechanically disadvantaged wrist that cannot tolerate physiologic loads, further emphasizing the need for anatomic reduction and rigid internal fixation.
Exhaustive Indications and Contraindications
The decision-making algorithm for scaphoid fractures has evolved significantly, shifting toward earlier operative intervention to mitigate the risks of nonunion and prolonged immobilization. The indications for surgical fixation are dictated by fracture location, degree of displacement, chronicity, and the functional demands of the patient. Operative management is absolutely indicated for any unstable or displaced scaphoid fracture.
Displacement is rigorously defined by specific radiographic criteria. Any step-off or gap greater than 1 millimeter on any radiographic view is considered displaced and warrants fixation. Furthermore, angular instability is a strict operative indication; this includes a radiolunate angle exceeding 15 degrees (indicating a DISI deformity), a scapholunate angle greater than 60 degrees, or an intrascaphoid angle greater than 35 degrees (indicative of a humpback deformity). Comminuted fractures, particularly those with volar cortical fragmentation, are inherently unstable and require surgical stabilization, often supplemented with bone grafting.
Fracture location is equally critical. Proximal pole fractures, even when entirely nondisplaced, possess an unacceptably high rate of nonunion (approaching 30-50% with cast immobilization) due to the retrograde vascularity discussed previously. Therefore, proximal pole fractures are considered an absolute indication for operative fixation, almost exclusively via a dorsal approach to allow for direct visualization and central screw placement. Additionally, in high-demand patients—such as elite athletes, military personnel, or manual laborers—early percutaneous or minimally invasive ORIF of nondisplaced waist fractures is increasingly recommended to expedite functional recovery, avoid the morbidity of prolonged casting, and ensure a higher rate of primary bone healing.
| Clinical Scenario | Operative Indications (ORIF) | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Displacement | >1 mm translation or gap | Advanced SNAC wrist (requires salvage) | Severe osteopenia/osteoporosis |
| Angulation | Radiolunate angle > 15°, Scapholunate > 60° | Active local or systemic infection | Poor patient compliance |
| Location | All proximal pole fractures | Medically unfit for anesthesia | Heavy tobacco use (relative) |
| Comminution | Volar or dorsal cortical comminution | Charcot arthropathy of the wrist | Nondisplaced distal pole avulsions |
| Patient Factors | High-demand athlete/laborer desiring early ROM | Asymptomatic established nonunion in elderly | Pediatric fractures (often heal non-op) |
Contraindications to scaphoid ORIF must be carefully respected to avoid catastrophic failures. The presence of advanced radiocarpal or midcarpal arthritis (SNAC stages II-III) is an absolute contraindication to isolated scaphoid fixation; these patients require salvage procedures such as proximal row carpectomy (PRC) or scaphoid excision with four-corner fusion. Active infection, whether local soft tissue or systemic, precludes the placement of internal hardware. Relative contraindications include severe osteopenia, which may compromise screw purchase, and heavy tobacco use, which significantly impairs microvascular perfusion and bone healing, though many surgeons will still operate while aggressively counseling on smoking cessation.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the absolute cornerstone of a successful scaphoid ORIF. The surgeon must construct a comprehensive three-dimensional mental model of the fracture morphology before making the incision. This begins with a rigorous radiographic evaluation. Standard posteroanterior (PA) and lateral views are insufficient. A dedicated scaphoid series is mandatory, including a PA view with the wrist in ulnar deviation (which extends the scaphoid to profile its true length), a semipronated oblique view (optimal for the waist and distal pole), and a semisupinated oblique view (optimal for the dorsal ridge).


While plain radiographs are the first line of diagnosis, advanced imaging is routinely required for surgical planning. High-resolution Computed Tomography (CT) scans, reformatted in the sagittal and coronal planes along the longitudinal axis of the scaphoid, provide exquisite detail regarding fracture comminution, humpback deformity, and the precise location of the proximal pole fragment. CT is invaluable for templating the trajectory and length of the headless compression screw. Magnetic Resonance Imaging (MRI) is utilized primarily for detecting radiographically occult fractures in the acute setting and for evaluating the vascular status of the proximal pole in delayed presentations or established nonunions. A lack of T1 signal intensity in the proximal fragment suggests avascular necrosis, which dictates the need for vascularized bone grafting in addition to rigid fixation.


Anesthesia, Positioning, and Equipment
The procedure may be performed under general anesthesia or regional anesthesia (e.g., supraclavicular or axillary brachial plexus block). Regional anesthesia is highly favored as it provides excellent intraoperative muscle relaxation and superior postoperative analgesia, minimizing the need for systemic opioids.
The patient is positioned supine on the operating table. The operative arm is abducted and placed on a radiolucent hand table. A well-padded upper arm tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying the small anatomical structures and assessing the vascularity of the bone ends. The fluoroscopy unit (C-arm) is brought in from the foot of the hand table, perpendicular to the long axis of the arm, allowing the surgeon to seamlessly transition between PA, lateral, and oblique views without moving the patient's arm excessively.
Preoperative templating involves measuring the anticipated screw length on the CT scan or calibrated radiographs. The goal is to select a headless compression screw that will reside entirely within the bone (subchondral to subchondral) while maximizing thread purchase in both the proximal and distal fragments. The surgeon must ensure that a full scaphoid specific tray, including various sizes of headless cannulated screws (typically 2.4mm to 3.0mm in diameter), K-wires (0.045 and 0.062 inch), and specialized reduction forceps, is immediately available.
Step-by-Step Surgical Approach and Fixation Technique
The dorsal approach is the gold standard for proximal pole fractures and is highly effective for waist fractures, particularly when a humpback deformity requires correction or when the proximal pole is too small to engage via a volar approach. The dorsal approach allows direct visualization of the proximal pole and facilitates screw placement down the central, biomechanical axis of the scaphoid.
Incision and Superficial Dissection
A longitudinal or slightly lazy-S incision, approximately 3 to 4 cm in length, is centered over Lister's tubercle on the dorsal aspect of the distal radius. The incision extends distally toward the base of the third metacarpal. Meticulous hemostasis is achieved using bipolar electrocautery. The subcutaneous tissues are spread longitudinally to identify and protect the terminal branches of the superficial radial nerve and the dorsal venous network.


The extensor retinaculum is identified, and the third extensor compartment is opened by incising the retinaculum sharply along the ulnar border of Lister's tubercle. The extensor pollicis longus (EPL) tendon is mobilized and retracted radially using a vessel loop. This exposes the floor of the third compartment and the interval between the second compartment (ECRB/ECRL) and the fourth compartment (EDC).


Capsulotomy and Joint Exposure
Deep dissection involves a ligament-sparing capsulotomy to expose the radiocarpal joint. A Berger dorsal capsulotomy is frequently employed. A longitudinal incision is made through the dorsal radiocarpal capsule, taking care to preserve the integrity of the dorsal intercarpal (DIC) and radiocarpal ligaments where possible. The capsule is elevated as full-thickness flaps radially and ulnarly, exposing the proximal pole of the scaphoid, the scapholunate interval, and the dorsal ridge of the scaphoid.


The fracture site is systematically identified. In acute fractures, hematoma is evacuated. In delayed unions or nonunions, fibrous tissue and necrotic bone are meticulously debrided back to bleeding, punctate cortical bone using a combination of sharp curettes and a high-speed burr. The scapholunate interosseous ligament must be inspected to ensure it has not been concurrently injured.
Fracture Reduction and Provisional Fixation
Anatomic reduction is the most critical step. The scaphoid must be restored to its native length and alignment, correcting any flexion (humpback) deformity. This is often achieved using 0.045-inch Kirschner wires (K-wires) inserted into the proximal and distal fragments to act as "joysticks." By manipulating these joysticks, the surgeon can extend the distal fragment and reduce it to the proximal pole.


Once reduced, the fracture is provisionally stabilized with a 0.045-inch K-wire driven from the proximal pole, across the fracture site, and into the distal pole. This provisional wire should be placed peripherally to avoid interfering with the central trajectory of the definitive guide wire. Fluoroscopy in multiple planes (PA, lateral, and scaphoid views) is utilized to confirm anatomic reduction and the correction of the intrascaphoid angle.

Guide Wire Placement and Screw Insertion
With the fracture anatomically reduced and provisionally pinned, the central guide wire for the cannulated screw system is introduced. The starting point for the dorsal approach is at the very apex of the proximal pole, adjacent to the scapholunate ligament insertion. The wrist is acutely flexed to allow the drill to clear the dorsal lip of the radius. The guide wire is driven down the central longitudinal axis of the scaphoid, aiming for the distal pole tubercle.


Fluoroscopy is essential here. The wire must be perfectly central in both the PA and lateral planes. A centrally placed screw provides superior biomechanical stiffness and requires less force to achieve compression compared to an eccentrically placed screw. Once the guide wire is confirmed to be in the subchondral bone of the distal pole, a depth gauge is used to measure the required screw length. The surgeon typically subtracts 2 to 4 millimeters from the measured length to ensure the screw is completely countersunk and does not penetrate the distal STT joint.
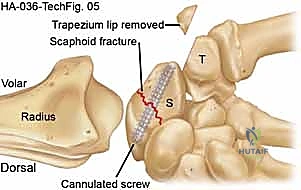
The near cortex is overdrilled, and the entire tract is drilled with the cannulated bit over the guide wire. A headless compression screw of the appropriate length is then advanced over the wire. As the trailing threads engage the proximal pole, compression across the fracture site is achieved. The screw must be buried beneath the articular cartilage of the proximal pole to prevent catastrophic damage to the scaphoid fossa of the radius.

Final fluoroscopic images are obtained through a full range of motion to confirm stable fixation, adequate compression, and the absolute absence of intra-articular hardware penetration. The surgical site is irrigated, the capsule is closed with absorbable suture, the EPL is left transposed radially, and the extensor retinaculum is repaired. The skin is closed in a standard fashion, and a sterile dressing and volar thumb spica splint are applied.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, scaphoid ORIF is associated with a distinct profile of potential complications. The surgeon must be prepared to identify and manage these adverse events promptly. The most dreaded complication remains nonunion, which, even with operative intervention, occurs in approximately 5% to 10% of cases, though this rate is higher for proximal pole fractures or those with delayed presentation.
Avascular necrosis (AVN) of the proximal pole is another profound complication, resulting from the disruption of the retrograde intraosseous blood supply. AVN can lead to fragmentation of the proximal pole, loss of fixation, and rapid joint destruction. Hardware complications are also notable; prominent screws that are not fully countersunk can act as an abrasive gouge against the radial articular surface, leading to rapid, iatrogenic radiocarpal arthritis. Conversely, screws that are too short may fail to provide adequate compression or pull out of the osteopenic proximal fragment.
| Complication | Estimated Incidence | Etiology / Risk Factors | Management / Salvage Strategy |
|---|---|---|---|
| Nonunion | 5% - 10% (Overall) | Proximal pole, AVN, inadequate fixation | Revision ORIF with vascularized bone graft (e.g., 1,2 ICSRA) |
| Avascular Necrosis | 15% - 30% (Prox. Pole) | Disruption of dorsal retrograde blood supply | Vascularized bone grafting; if fragmented, proximal row carpectomy |
| Hardware Prominence | 2% - 5% | Inaccurate measurement, failure to countersink | Immediate hardware removal/revision to prevent chondral damage |
| Infection (Superficial/Deep) | < 2% | Standard surgical risks, poor soft tissue envelope | Oral/IV antibiotics; I&D with hardware removal if deep/persistent |
| Wrist Stiffness | 10% - 20% | Prolonged immobilization, capsular scarring | Aggressive occupational therapy, dynamic splinting, late capsular release |
When primary fixation fails and progresses to a symptomatic nonunion or AVN with carpal collapse (SNAC wrist), salvage procedures are indicated. The choice of salvage depends on the stage of arthritis. For SNAC Stage I (arthritis limited to the radial styloid), a radial styloidectomy combined with scaphoid nonunion repair and bone grafting may suffice. For SNAC Stage II (involving the scaphocapitate joint) or Stage III (periscaphoid arthritis), motion-preserving salvage procedures such as a Proximal Row Carpectomy (PRC) or Scaphoid Excision with Four-Corner Fusion (lunate, capitate, hamate, triquetrum) are required. These procedures reliably relieve pain but permanently reduce wrist range of motion by approximately 40% to 50%.
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following scaphoid ORIF is a delicate balance between protecting the fragile osteosynthesis and preventing debilitating wrist stiffness. The protocol is heavily influenced by the security of the intraoperative fixation, the presence of comminution, and the patient's compliance.
Phase I: Immediate Post-Operative (Weeks 0-2)
Following surgery, the wrist is immobilized in a well-padded volar thumb spica splint. The primary goals during this phase are edema control, wound healing, and pain management. The patient is instructed to keep the extremity elevated above the level of the heart and to perform active range of motion exercises of the fingers, elbow, and shoulder to prevent generalized upper extremity stiffness. At
