Comprehensive Introduction and Patho-Epidemiology
The Burden of Achilles Tendon Ruptures
Achilles tendon ruptures represent a significant and evolving challenge in orthopedic surgery, demanding a rigorous understanding of both the pathology and the biomechanical requirements for successful restoration of function. Historically considered an injury of the "weekend warrior," the demographic profile of the Achilles tendon rupture has broadened significantly. We are increasingly observing this injury in both high-level, elite athletes and in an aging population attempting to maintain active lifestyles. The incidence has risen to approximately 18 to 32 per 100,000 person-years, a surge likely attributable to the growing participation in high-demand, intermittent-impact sports such as basketball, tennis, and soccer among middle-aged individuals.
The socioeconomic burden of this injury is substantial, often resulting in prolonged absences from work and athletic endeavors. A ruptured Achilles tendon fundamentally disrupts the posterior tension band of the lower extremity, severely compromising the plantarflexion power required for normal gait, running, and jumping. The decision-making process regarding management—whether operative or non-operative—remains a subject of intense academic debate. However, for the physiologically active patient seeking a reliable return to pre-injury activity levels with a minimized risk of re-rupture, operative intervention remains the gold standard.
Pathophysiology of Tendinosis and Failure
Understanding the pathophysiology of Achilles tendon rupture is crucial for both surgical planning and managing patient expectations. Acute ruptures rarely occur in a perfectly healthy tendon; rather, they are typically the catastrophic culmination of chronic, often asymptomatic, degenerative tendinopathy. Histological analysis of ruptured tendons consistently reveals profound mucoid degeneration, lipomatosis, and disruption of the normal parallel collagen fibril architecture. This degenerative cascade compromises the tensile strength of the tendon, making it highly susceptible to failure under sudden, eccentric loading conditions.
Several intrinsic and extrinsic risk factors accelerate this degenerative process. Systemic conditions such as poorly controlled diabetes mellitus, inflammatory arthropathies, and chronic renal failure impair tissue homeostasis and microvascular perfusion. Iatrogenic factors, most notably the administration of systemic or locally injected corticosteroids, drastically reduce collagen synthesis and weaken the tendon structure. Furthermore, the use of fluoroquinolone antibiotics has been definitively linked to an increased risk of Achilles tendinopathy and rupture, likely due to direct toxicity to tenocytes and the upregulation of matrix metalloproteinases.
When the tendon ultimately fails, the rupture typically occurs in a highly specific anatomical region: the hypovascular zone, located approximately 2 to 6 centimeters proximal to the calcaneal insertion. The mechanism of injury usually involves a sudden, forceful eccentric contraction of the triceps surae—such as rapidly pushing off the weight-bearing foot while the knee is extending, or an unexpected, violent dorsiflexion of the ankle. The resulting gap formation and retraction of the tendon ends present a complex surgical challenge that requires meticulous technique to restore the anatomic length-tension relationship.
Detailed Surgical Anatomy and Biomechanics
Musculotendinous Architecture of the Triceps Surae
Before we even consider making an incision, a thorough, three-dimensional understanding of the regional anatomy is non-negotiable. The Achilles tendon is the strongest and thickest tendon in the human body, serving as the confluent structure formed by the "triceps surae" – the medial and lateral heads of the gastrocnemius, and the deeper soleus muscle. The gastrocnemius originates from the medial and lateral femoral condyles, making it a two-joint muscle that is highly active during dynamic, explosive movements. Its aponeurotic contribution tends to be more superficial and forms the lateral aspect of the Achilles tendon as it courses distally.

Lying deep to the gastrocnemius is the soleus muscle, which originates from the posterior aspect of the tibia and fibula. Because it does not cross the knee joint, the soleus is primarily a postural muscle, composed predominantly of slow-twitch Type I muscle fibers. Its tendinous contribution is typically more medial and deeper within the Achilles tendon. As these distinct muscle components converge and descend toward the heel, the Achilles tendon undergoes a characteristic 90-degree internal rotation. Consequently, the fibers originating from the soleus end up inserting medially, while the gastrocnemius fibers insert laterally on the calcaneus.

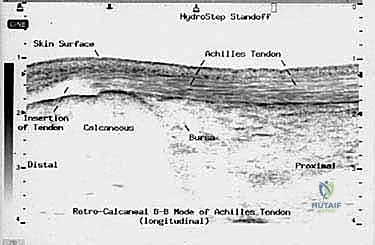
The Achilles tendon ultimately inserts into the middle third of the flat, posterior calcaneal tuberosity. This broad, robust insertion provides an exceptional lever arm for its primary biomechanical function: powerful plantarflexion of the ankle joint. The retrocalcaneal bursa lies interposed between the anterior aspect of the distal tendon and the superior calcaneal tuberosity, reducing friction during ankle motion. Understanding this rotational anatomy is critical during surgical repair, as it aids the surgeon in correctly orienting and apposing the ruptured tendon fascicles to restore normal biomechanical tracking.
Vascularity, The Paratenon, and the Hypovascular Zone
The vascular supply to the Achilles tendon is a critical determinant of both its susceptibility to injury and its capacity for postoperative healing. Unlike tendons enclosed within a true synovial sheath, the Achilles tendon is enveloped by a paratenon—a highly vascularized, single-layered adventitial structure composed of loose connective tissue. The paratenon is crucial for two primary reasons: it facilitates frictionless tendon gliding against surrounding fascial structures, and it serves as the primary conduit for the extrinsic blood supply to the tendon via a rich capillary network.
Critically, the middle section of the tendon, approximately 2 to 6 cm proximal to its calcaneal insertion, is universally recognized as a hypovascular zone. Injection studies have demonstrated a relative paucity of intrinsic blood vessels in this region compared to the highly vascularized musculotendinous junction proximally and the osseous insertion distally. This watershed area relies heavily on diffusion from the surrounding paratenon. Consequently, this zone is the most prone to degenerative pathology and acute rupture.
During surgical intervention, the preservation of the paratenon is of paramount importance. Indiscriminate dissection, particularly wide stripping of the paratenon or excessive exploration anterior to the tendon, can devascularize the tendon ends, leading to delayed healing, wound breakdown, or catastrophic re-rupture. The surgical approach must respect this delicate vascular envelope, utilizing precise incisions and atraumatic tissue handling to maintain the biological potential of the repair site.
Neurovascular Topography and Iatrogenic Risks
Navigating the posterior ankle requires a heightened awareness of the regional neurovascular topography to prevent debilitating iatrogenic injuries. The primary neural structure at risk during an Achilles tendon repair is the sural nerve. This sensory nerve provides cutaneous innervation to the lateral aspect of the hindfoot and midfoot. It typically courses distally down the posterior calf, crossing the lateral border of the Achilles tendon from medial to lateral at a mean distance of 9.8 cm proximal to the calcaneal insertion.
As the sural nerve continues distally, it lies a mean of 18.8 mm lateral to the lateral border of the tendon. However, its anatomical position is highly variable. Studies have shown that the nerve can cross the tendon much further distally, placing it directly in the surgical field during lateral or even midline approaches. An iatrogenic injury to the sural nerve—whether through direct transection, aggressive retraction, or entrapment within a suture—results in painful neuromas and annoying numbness along the lateral foot, which can severely impact patient satisfaction despite a structurally sound tendon repair.
Accompanying the sural nerve is the lesser saphenous vein, a superficial venous structure that also typically courses lateral to the paratenon. This vein must be carefully identified and protected during the initial subcutaneous dissection. Inadvertent laceration of the lesser saphenous vein can lead to troublesome intraoperative bleeding, obscuring the surgical field, and increases the risk of postoperative hematoma formation, which in turn elevates the risk of deep infection and wound dehiscence.
Biomechanical Considerations in Tendon Repair
The ultimate goal of operative intervention is to create a biomechanically robust construct that can withstand the early forces of rehabilitation while facilitating biological healing. The Achilles tendon is subjected to immense loads during normal daily activities, experiencing forces up to 3-4 times body weight during walking and up to 10-12 times body weight during running and jumping. Therefore, the chosen suture technique must provide exceptional tensile strength and resistance to gap formation.
Gap formation at the repair site is the enemy of successful tendon healing. Even a few millimeters of elongation can lead to a healed tendon that is functionally lengthened, resulting in a permanent loss of plantarflexion power and a noticeable limp. The ideal repair technique must securely grasp the longitudinal collagen fibers of the tendon, preventing suture pull-through under cyclic loading.
This is where advanced suturing configurations, such as the "Gift Box" modification of the Krackow technique, become essential. By utilizing locking loops that firmly engage the tendon fascicles and routing the suture strands to create a compressive, box-like construct, we maximize the load-to-failure strength. Furthermore, burying the knots away from the immediate rupture site minimizes local tissue ischemia and reduces the bulk of the repair, allowing for a smoother closure of the overlying paratenon and skin.
Exhaustive Indications and Contraindications
Criteria for Surgical Intervention
The decision to proceed with operative repair of an acute Achilles tendon rupture is individualized, weighing the patient's functional demands against their surgical risk profile. The primary indication for open surgical repair is an acute, complete rupture in a young, healthy, and physically active patient who desires a return to high-impact sports or demanding physical labor. In this demographic, operative management has historically demonstrated a lower rate of re-rupture compared to non-operative casting, alongside a more reliable restoration of baseline plantarflexion strength and endurance.
Surgical intervention is also strongly indicated in cases of delayed presentation or chronic ruptures (typically defined as presenting more than 4-6 weeks post-injury). In these scenarios, the proximal tendon stump has often retracted significantly, and the gap has filled with non-functional scar tissue. Non-operative management is virtually guaranteed to fail in chronic cases, as the tendon ends cannot be apposed through plantarflexion alone. These complex cases frequently require open debridement and often necessitate augmentation with V-Y fascial advancements, local tendon transfers (such as the Flexor Hallucis Longus), or allograft reconstruction.
Furthermore, patients who present with a re-rupture following a previous non-operative or operative treatment course are generally considered candidates for formal open repair and augmentation. The tissue quality in a re-rupture is inherently poor, requiring a highly stable mechanical construct and enhanced biological support to achieve successful union.
Absolute and Relative Contraindications
While operative repair offers distinct functional advantages for the appropriate candidate, it is not without significant risks. The posterior ankle has relatively poor soft tissue coverage, making wound complications a devastating potential outcome. Therefore, absolute contraindications to surgery include active local or systemic infection, severe peripheral arterial disease compromising distal perfusion, and an inability or unwillingness of the patient to comply with the strict postoperative rehabilitation protocol.
Relative contraindications require careful preoperative optimization and a frank discussion with the patient regarding the elevated risk profile. Elderly, sedentary individuals with low functional demands are often better served with functional rehabilitation in a controlled ankle motion (CAM) boot, as the risks of surgery may outweigh the marginal functional benefits. Patients with long-standing, poorly controlled diabetes mellitus are at a profoundly increased risk for deep wound infections and delayed healing.
Active tobacco use is a major relative contraindication. Nicotine causes potent microvascular vasoconstriction, severely impairing blood flow to the already hypovascular healing zone and the delicate overlying skin flaps. I strongly advise smoking cessation for at least 4-6 weeks perioperatively. Chronic systemic corticosteroid use also significantly impairs collagen synthesis and wound healing, necessitating a highly cautious approach to surgical intervention.
| Factor | Operative Management | Non-Operative Management |
|---|---|---|
| Ideal Patient Profile | Young, athletic, high functional demands, delayed presentation (>4 weeks). | Elderly, sedentary, severe medical comorbidities, immediate presentation (<48 hours). |
| Re-Rupture Rate | Historically lower (1.5% - 3.5%). | Historically higher, but modern functional rehab protocols show comparable rates (3% - 5%). |
| Plantarflexion Strength | Reliable restoration of peak torque and endurance. | Higher risk of slight elongation and subtle strength deficits. |
| Complication Profile | Wound infection, nerve injury, scar adhesions. | DVT, pressure ulcers from casting, functional lengthening. |
| Return to Sport | Generally faster and more predictable for high-impact activities. | May be prolonged; potential limitations in explosive power. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging Modalities
Proper planning is the cornerstone of any successful surgical intervention. For an Achilles repair, this involves a thorough review of imaging and careful consideration of patient-specific factors. While the diagnosis of an acute Achilles rupture is primarily clinical—relying on a palpable gap, a positive Thompson test, and loss of resting ankle equinus—imaging plays a crucial role in surgical planning.
Plain radiographs (AP, Lateral, and Mortise views of the ankle) are obtained routinely. While they do not visualize the tendon directly, they are essential to rule out concomitant fractures of the ankle or tarsals, particularly a bony avulsion of the calcaneal tuberosity. On the lateral view, we specifically look for disruption of the normal triangular fat pad anterior to the Achilles tendon, known as Kager's triangle. This is an indirect sign of Achilles pathology, often obliterated by edema or hematoma in a rupture. We also assess for any calcific changes within the tendon itself, which could indicate chronic, end-stage tendinopathy.
Ultrasonography is a rapid, cost-effective, and dynamic imaging tool. While operator-dependent, it allows us to visualize the tendon structure in real-time. We can accurately measure the gap between the ruptured ends with the ankle in neutral and in plantarflexion, assessing whether the ends can be apposed non-operatively. It also helps evaluate the degree of tendinosis in the remaining tendon stumps.

Magnetic Resonance Imaging (MRI) remains the gold standard for evaluating complex or delayed Achilles tendon pathology. MRI offers superior sensitivity and specificity, providing invaluable information regarding the exact level of the rupture (midportion, musculotendinous junction, or insertional). It meticulously details the degree of tendon degeneration, the exact size of the tendon gap, and identifies any associated injuries such as partial tears, severe tendinosis, or surrounding soft tissue pathology. This information dictates whether a primary repair is feasible or if augmentation will be required.

Patient Optimization and Counseling
Based on the clinical examination and MRI findings, we engage in comprehensive patient counseling. If severe tendon degeneration or a massive gap is identified, we discuss the implications with the patient. They must understand that a larger incision may be necessary, and that augmentation with a local tendon transfer (such as the FHL or plantaris) or an allograft might be required intraoperatively. Managing patient expectations regarding the length of recovery, the rigorous nature of the rehabilitation, and the potential need for more complex, time-consuming procedures is vital for postoperative satisfaction.
We carefully screen for patients who may be better candidates for nonoperative management due to increased surgical risks. We optimize modifiable risk factors where possible. Diabetic patients must demonstrate tight glycemic control (HbA1c < 7.5%) prior to elective intervention. Smokers are provided with cessation resources and warned of the catastrophic risks of flap necrosis.
Precision Patient Positioning and Operating Room Setup
Patient positioning is crucial for optimal exposure, surgeon ergonomics, and the prevention of iatrogenic injury during a prolonged case. The patient is placed in the prone position after the induction of general anesthesia or a regional neuraxial block. This provides excellent, unobstructed access to the posterior aspect of the lower leg and ankle.
We utilize a Wilson frame or chest rolls to maintain proper spinal alignment and facilitate respiratory excursion. A commercially available foam headrest is mandatory to protect the patient's face, eyes, and airway, ensuring the cervical spine remains in a neutral position. Meticulous padding of all pressure points—especially the forehead, malar eminences, breasts, iliac crests, genitals, and knees—is essential to prevent devastating peripheral nerve palsies or ischemic skin breakdown.
A pneumatic thigh tourniquet is applied to the proximal thigh of the operative leg. This provides a bloodless field, which is critical for identifying delicate structures like the sural nerve and ensuring precise suture placement within the tendon fascicles.
Surgical Warning: A leg/calf tourniquet is absolutely contraindicated for Achilles tendon repair. It tethers the gastrocnemius-soleus complex, making it impossible to pull the proximal tendon stump distally, thereby preventing adequate intraoperative tendon apposition and accurate tensioning.
I strongly prefer to prepare and drape both lower extremities. This allows for continuous intraoperative comparison of the ankle resting position (the resting equinus angle). By comparing the injured side to the draped, uninjured contralateral leg, we can accurately restore the resting tendon length. This subtle comparison is a critical guide to avoid over-tensioning (which restricts dorsiflexion) or under-tensioning (which causes permanent weakness) of the repair.

Step-by-Step Surgical Approach and Fixation Technique
Incision Strategy and Paratenon Preservation
With the tourniquet inflated and the time-out complete, we commence the procedure. I favor a longitudinal incision placed approximately 1 to 2 centimeters medial to the medial border of the palpable Achilles tendon.
Rationale: This posteromedial approach offers excellent exposure to the ruptured tendon ends and provides immediate access to the plantaris tendon if augmentation is required. Most importantly, it keeps our dissection far away from the sural nerve, which courses laterally.
Surgical Warning: A direct posterior midline incision is strongly discouraged. It places the surgical scar directly over the posterior shoe counter, leading to chronic irritation and pain due to high-tension shear forces. A purely posterolateral incision places the sural nerve at an unacceptably high risk of transection.

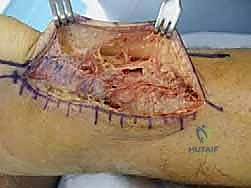
Using a #15 blade, the skin incision is made. We then proceed with meticulous, sharp dissection using Metzenbaum scissors to mobilize the thick skin and subcutaneous fat as a single, full-thickness flap laterally.
Critical Step: It is imperative to take great care to preserve the underlying paratenon. We must avoid wide, superficial undermining of the skin edges, as this destroys the subdermal plexus and drastically increases the risk of marginal skin necrosis and wound dehiscence.

Once the paratenon is clearly exposed and the skin flaps are gently retracted, we make a precise, midline longitudinal incision directly through the paratenon.
Rationale: Making the paratenon incision in the midline, offset from the medial skin incision, creates a stepped closure. This prevents the skin from tethering directly to the repaired tendon postoperatively, facilitating better tendon excursion. It also allows for a robust, watertight repair of the paratenon at the conclusion of the case.
Debridement and Preparation of Tendon Ends
Through the incised paratenon, the ruptured tendon ends and the intervening hematoma are exposed. The hematoma is thoroughly evacuated and irrigated. We then assess the quality of the tendon ends. The ruptured stumps typically exhibit a "mop-end" appearance, characterized by frayed, disorganized, and degenerated collagen fibers.

Using a scalpel or sharp scissors, we meticulously debride the devitalized, frayed tissue back to healthy, parallel-oriented collagen bundles. This step is a delicate balance: we must resect enough tissue to ensure we are suturing into structurally sound tendon, but we must avoid excessive resection that would create an unbridgeable gap.
Surgical Warning: Limit deep dissection at the anterior tendon-paratenon plane. Excessive dissection anterior to the tendon destroys the delicate mesotenon blood vessels, compromising the intrinsic vascularity of the repair site.

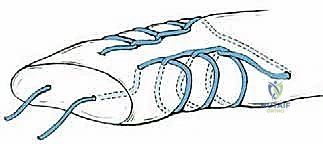
The Gift Box Technique Masterclass
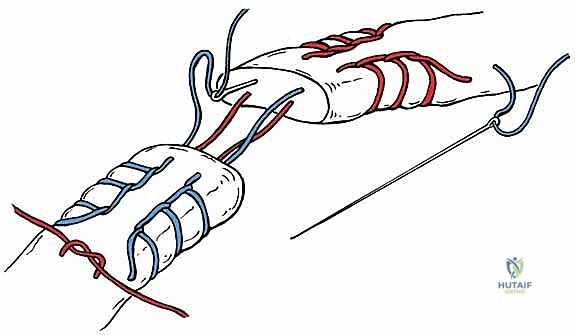
We now proceed with the core fixation using the "Gift Box" technique, a highly advanced modification of the traditional Krackow suture. This technique is designed to maximize grip on the longitudinal tendon fibers, resist gap formation under cyclic loading, and bury the bulky knots away from the healing interface. We utilize a heavy, non-absorbable, braided polyblend suture (e.g., #2 or #5 FiberWire or Orthocord) on a large taper needle.
- Proximal Stump Preparation: We begin on the proximal tendon stump. Starting approximately 3-4 cm proximal to the rupture site on the medial aspect, we pass the needle transversely through the tendon. We then execute 3 to 4 locking Krackow loops, advancing distally along the medial border toward the rupture site.
- Crossing the Rupture: Once the medial locking loops reach the debrided edge of the proximal stump, the suture is passed across the rupture gap and enters the distal tendon stump on its medial side.
- Distal Stump Preparation: We then execute 3 to 4 locking Krackow loops moving distally along the medial border of the distal stump. At the most distal point (near the calcaneal insertion), the needle is passed transversely across the tendon to the lateral side.
- Completing the Box: We now work proximally, placing 3 to 4 locking Krackow loops along the lateral border of the distal stump. The suture is then passed back across the rupture gap, entering the lateral side of the proximal stump. Finally, 3 to 4 locking loops are placed moving proximally along the lateral border of the proximal stump, finishing directly across from our initial starting point.
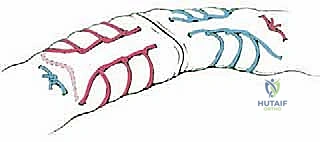
This continuous loop creates a biomechanical "box" that captures both tendon stumps. The two free ends of the suture now exit the proximal tendon at the same transverse level, far away from the rupture site.
Tensioning, Paratenon Closure, and Wound Management
With the core sutures placed, we must accurately tension the repair. The assistant plantarflexes the ankle to appose the tendon ends. We draw the two free ends of our heavy suture tight, eliminating all slack from the locking loops.
We then look at the draped contralateral leg to assess the resting equinus angle. The operative ankle is positioned to perfectly match this resting tension. While holding this precise position, the core suture is tied securely. Because the knot is tied proximally, it is buried deep within the healthy muscle-tendon junction, preventing a bulky prominence under the skin incision.


