Management of Massive Contracted Rotator Cuff and Subscapularis Tears
Key Takeaway
Massive contracted rotator cuff tears present a formidable challenge in orthopedic surgery, often requiring advanced mobilization techniques such as the arthroscopic interval slide. This comprehensive guide details the step-by-step surgical execution of capsular releases, margin convergence, and subscapularis tendon repair. By mastering these advanced arthroscopic techniques, surgeons can restore biomechanical function, address concurrent biceps pathology, and achieve stable, tension-free repairs in complex, retracted cuff lesions.
INTRODUCTION TO MASSIVE CONTRACTED ROTATOR CUFF TEARS
The management of massive, contracted rotator cuff tears represents one of the most technically demanding challenges in modern orthopedic sports medicine and shoulder surgery. By definition, a massive rotator cuff tear involves either a tear diameter exceeding 5 centimeters or the complete detachment of two or more rotator cuff tendons. Chronicity in these lesions inevitably leads to tendon retraction, severe capsular contracture, and secondary changes within the muscle belly, including atrophy and fatty infiltration (Goutallier changes).
When a tear becomes massive and contracted, the biomechanical force couples of the glenohumeral joint—both in the coronal and transverse planes—are profoundly disrupted. The supraspinatus and infraspinatus fail to effectively depress the humeral head, leading to superior migration, subacromial impingement, and eventual cuff tear arthropathy if left untreated. Achieving a tension-free repair is the paramount goal of surgical intervention; however, direct tendon-to-bone repair is frequently impossible without advanced mobilization techniques.
The arthroscopic interval slide technique, pioneered and popularized by Tauro et al., is an indispensable surgical strategy designed to release capsular and ligamentous contractures, thereby restoring tendon excursion and facilitating a biomechanically sound, tension-free repair.
PREOPERATIVE EVALUATION AND IMAGING
A meticulous preoperative evaluation is critical for surgical planning. Patients typically present with profound weakness in elevation and external rotation, often accompanied by debilitating night pain.
Clinical Assessment
Physical examination must assess the functional status of the remaining rotator cuff. The "horn blower's sign" and "drop sign" indicate severe infraspinatus and teres minor dysfunction. Pseudoparalysis—defined as the inability to actively elevate the arm beyond 90 degrees in the presence of free passive range of motion—must be carefully evaluated, as its reversibility post-repair depends heavily on the integrity of the force couples and the degree of fatty infiltration.
Radiographic and MRI Evaluation
Standard radiographs (true anteroposterior, scapular Y, and axillary lateral views) are essential to evaluate the acromiohumeral interval (AHI). An AHI of less than 7 mm is highly suggestive of a massive tear, while an AHI of less than 5 mm often indicates irreversible changes and potential early cuff tear arthropathy.
Magnetic Resonance Imaging (MRI) without or with intra-articular contrast (MR arthrogram) is the gold standard for evaluating tendon retraction (Patte classification) and muscle quality (Goutallier classification). Advanced fatty infiltration (Goutallier Stage 3 or 4) in the supraspinatus and infraspinatus is generally considered a poor prognostic indicator for structural healing, often steering the surgeon toward alternative procedures such as superior capsular reconstruction (SCR) or reverse total shoulder arthroplasty (RTSA) in older patients.
ARTHROSCOPIC MOBILIZATION: THE INTERVAL SLIDE TECHNIQUE
When a crescent-shaped tear fails to reduce to the anatomic footprint on the greater tuberosity, or when a longitudinal U-shaped tear cannot be approximated side-to-side without excessive tension, advanced mobilization is required. The arthroscopic interval slide is a highly effective soft tissue release that adapts the principles of open capsular release to an all-arthroscopic environment.
CLINICAL PEARL:
The primary impediment to lateral excursion of a chronically retracted supraspinatus tendon is the contracted coracohumeral ligament (CHL) and the thickened superior capsule. Releasing these structures is the cornerstone of the interval slide technique.
Surgical Setup and Diagnostic Arthroscopy
- Positioning: The patient may be positioned in either the beach chair or lateral decubitus position, depending on surgeon preference. The lateral decubitus position often provides superior visualization of the subacromial space and facilitates traction, while the beach chair position allows for easier conversion to an open procedure or arthroplasty if deemed necessary.
- Diagnostic Arthroscopy: A routine diagnostic arthroscopy is performed via a standard posterior viewing portal. The glenohumeral joint is systematically inspected to assess the size, shape, and chronicity of the tear, as well as the status of the articular cartilage, labrum, and long head of the biceps tendon.
- Mobility Assessment: An atraumatic grasper is inserted through an anterior or lateral portal. The surgeon must assess the mobility of the rotator cuff from the articular side. Traction is applied to the supraspinatus and infraspinatus tendons to determine their excursion toward the greater tuberosity.
Step-by-Step Surgical Technique (Tauro et al.)
1. Superior Capsular Release
If the supraspinatus tendon exhibits poor mobility during the initial articular assessment, a superior capsular release is the first step.
* Instrumentation: An arthroscopic elevator, a blunt trocar, or a radiofrequency (RF) electrosurgical cutting device is inserted through the lateral subacromial portal.
* Execution: The release is accomplished by meticulously cutting through the capsule between the undersurface of the rotator cuff tendon and the superior glenoid rim.
* Trajectory: The release extends from the rotator interval anteriorly to the base of the scapular spine posteriorly.
SURGICAL WARNING:
When performing the posterior aspect of the superior capsular release, the surgeon must remain acutely aware of the suprascapular nerve. The nerve passes through the suprascapular notch and winds around the spinoglenoid notch. Dissection should remain strictly lateral to the glenoid rim and avoid aggressive medial penetration into the muscle belly to prevent devastating iatrogenic denervation.
2. The Arthroscopic Interval Slide
If the superior capsular release is insufficient to achieve a tension-free reduction, the surgeon proceeds to the formal interval slide.
* Viewing and Portal Setup: The arthroscope is maintained in the posterior intra-articular portal. A narrow basket punch or arthroscopic scissors are inserted into the lateral subacromial portal, passing directly through the tear in the cuff and into the joint space.
* Anterior Release: The surgeon divides the interval between the anterior border of the supraspinatus and the superior capsule (the rotator interval) from lateral to medial. This critical step releases the supraspinatus tendon from the severely contracted coracohumeral ligament on the bursal side.
* Biceps Tendon Considerations:
* Intact Biceps: If the long head of the biceps tendon is intact and is to be preserved, the release must be made just caudad (inferior/posterior) to the tendon to avoid iatrogenic injury to the biceps or its stabilizing pulley system.
* Absent/Tenotomized Biceps: If the biceps is absent, previously ruptured, or planned for tenodesis/tenotomy, the release can be started more aggressively at the anterosuperior pole of the glenoid.
* Tactile Feedback: The adequacy of the release can often be judged by the character of the tissue being cut. The contracted CHL feels thick and fibrotic; once divided, a sudden "give" is often palpable, and the supraspinatus will immediately demonstrate improved lateral excursion.
3. Percutaneous Traction
To facilitate the release and maintain tension on the contracted tissues, establishing a small percutaneous portal just adjacent to the lateral subacromial portal is highly recommended. An atraumatic grasper is introduced through this accessory portal to pull the tendon laterally. This constant lateral traction places the contracted interval tissues under tension, making them easier to identify and safely divide with the basket punch or RF wand.
Cuff Repair and Margin Convergence
Once adequate mobilization is achieved, the focus shifts to structural repair.
* Footprint Preparation: The greater tuberosity footprint is decorticated to a bleeding cancellous bone bed using an arthroscopic burr or shaver, optimizing the biological environment for tendon-to-bone healing.
* Margin Convergence: For large U-shaped or L-shaped tears, side-to-side repair (margin convergence) is performed before anchoring the tendon to the bone. Margin convergence fundamentally alters the biomechanics of the tear by reducing the strain at the margin of the tear and converting a massive U-shaped defect into a smaller crescent-shaped tear. Heavy non-absorbable sutures are passed side-to-side using a suture shuttle or penetrating device.
* Tuberosity Fixation: Following margin convergence, the newly created free edge of the rotator cuff is repaired down to the prepared tuberosity. Depending on the remaining tendon length and tissue quality, this can be achieved using a single-row, double-row, or transosseous-equivalent (suture bridge) construct utilizing modern suture anchors.
SUBSCAPULARIS TENDON TEARS
While massive posterosuperior tears dominate the literature, the subscapularis tendon—the largest and most powerful of the rotator cuff muscles—plays an equally critical role in glenohumeral kinematics. Subscapularis tears are frequently underdiagnosed and are often associated with eccentric overload of the cuff, massive anterior trauma, or chronic coracoid impingement.
Pathomechanics and Coracoid Impingement
Coracoid impingement syndrome is a recognized etiology for degenerative subscapularis tearing. It occurs when the coracohumeral distance (the space between the tip of the coracoid process and the lesser tuberosity) is congenitally narrowed or secondarily reduced due to posterior capsular contracture. Chronic friction leads to fraying, partial tearing, and eventual complete rupture of the subscapularis tendon, often beginning at its superior insertion.
Clinical Evaluation of the Subscapularis
Accurate clinical diagnosis relies on specific provocative tests designed to isolate the subscapularis muscle:
1. The Lift-Off Test (Gerber's Test): The patient places the dorsum of their hand against their mid-lumbar spine and attempts to lift the hand away from the back against the examiner's resistance. Inability to do so indicates a lower/inferior subscapularis tear. This test requires full internal rotation, which may be limited in patients with massive tears.
2. The Napoleon Test (Belly-Press Test): Ideal for patients who lack the internal rotation required for the lift-off test. The patient presses the palm of their hand against their abdomen. A positive Napoleon test occurs when the patient can only maintain pressure on the abdomen by flexing the wrist to 90 degrees and allowing the elbow to drop posteriorly, indicating profound subscapularis weakness.
3. The Bear-Hug Test: The patient places the palm of the affected arm on the opposite shoulder, with the elbow elevated. The examiner attempts to pull the hand away from the shoulder. Weakness compared to the contralateral side is highly sensitive for upper subscapularis lesions.
Imaging and Biceps Tendon Pathology
MRI is paramount for evaluating subscapularis lesions. Axial and sagittal oblique sequences are scrutinized to assess the integrity of the tendon footprint on the lesser tuberosity and the degree of muscle atrophy.
Crucially, the subscapularis tendon is intimately associated with the long head of the biceps tendon (LHBT). The superior fibers of the subscapularis form the medial wall of the bicipital groove and contribute to the biceps pulley system (along with the CHL and supraspinatus).
PITFALL:
A tear of the superior subscapularis almost universally compromises the biceps pulley. Failure to address biceps instability during a subscapularis repair will lead to persistent anterior shoulder pain, recurrent subluxation, and potential failure of the subscapularis repair due to the "sawing" effect of the unstable biceps tendon.
Management of the Long Head of the Biceps
When a subscapularis tear is identified alongside biceps tendon instability (medial subluxation or dislocation into the joint), the biceps must be addressed surgically:
* Biceps Tenotomy: In older, lower-demand patients, or those with massive, irreparable cuff tears, a simple arthroscopic release (tenotomy) of the biceps tendon at its superior labral origin provides excellent pain relief with minimal surgical morbidity. Patients must be counseled regarding the potential for a cosmetic "Popeye" deformity and mild cramping pain in the biceps muscle belly.
* Biceps Tenodesis: In younger, more active patients, laborers, or those who wish to preserve normal biceps contour and supination strength, a biceps tenodesis is indicated. This can be performed arthroscopically (suprapectoral) or via a mini-open approach (subpectoral), securing the tendon in the bicipital groove or lower humeral shaft using interference screws or suture anchors.
Subscapularis Repair Technique
Arthroscopic repair of the subscapularis requires specialized portal placement, typically utilizing an anterolateral viewing portal and accessory anterior working portals.
1. Preparation: The lesser tuberosity is debrided to a bleeding bone bed. The coracoid process is evaluated; if the coracohumeral distance is less than 6 mm, a coracoplasty (resection of the posterolateral tip of the coracoid) is performed to decompress the subscapularis.
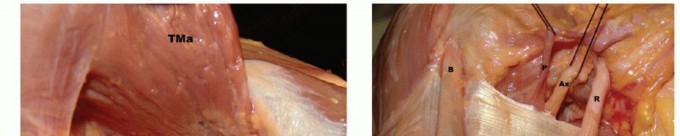
2. Mobilization: The subscapularis is mobilized by releasing adhesions between the tendon and the base of the coracoid, taking care to avoid the axillary and musculocutaneous nerves located medially. The "comma sign" (the avulsed superior glenohumeral ligament/CHL complex) is a vital landmark for identifying the retracted superolateral corner of the subscapularis.
3. Fixation: Suture anchors are placed in the lesser tuberosity. Sutures are passed through the tendon using penetrating instruments, and the tendon is securely tied down to its anatomic footprint.
POSTOPERATIVE REHABILITATION
Rehabilitation following the repair of massive contracted rotator cuff tears and subscapularis tears must be highly individualized, balancing the need for tissue protection with the prevention of postoperative stiffness.
- Phase I (0-6 Weeks): Strict immobilization in an abduction sling (for posterosuperior tears) or neutral rotation sling (for subscapularis tears). Passive range of motion (PROM) is initiated cautiously. For subscapularis repairs, external rotation is strictly limited to neutral or 30 degrees to protect the repair.
- Phase II (6-12 Weeks): Transition to active-assisted range of motion (AAROM) and eventually active range of motion (AROM). The sling is discontinued. Scapular stabilization exercises are emphasized.
- Phase III (12-24 Weeks): Gradual introduction of progressive resistance exercises. Strengthening begins with isometric exercises and advances to isotonic bands and light weights.
- Phase IV (6 Months+): Return to advanced functional activities and heavy lifting. Maximum medical improvement may not be reached until 12 to 18 months postoperatively.
CONCLUSION
The surgical management of massive contracted rotator cuff tears demands a profound understanding of glenohumeral biomechanics, advanced arthroscopic skills, and meticulous preoperative planning. The arthroscopic interval slide technique remains a cornerstone for mobilizing chronically retracted tissues, allowing for tension-free margin convergence and anatomic footprint restoration. Concurrently, the vigilant assessment and repair of associated subscapularis tears and biceps pathology are essential for restoring the transverse force couple and achieving optimal, pain-free functional outcomes in this challenging patient population.
📚 Medical References
- massive rotator cuff tears: the evolution of a concept, Orthop Clin North Am 28:125, 1997.
- Burkhart SS, Athanasiou KA, Writh MA: Margin convergence: a method of reducing strain in massive rotator cuff tears, Arthroscopy 12:335, 1996.
- Burkhart SS, Nottage WM, Ogilvie-Harris DJ, et al: Partial repair of irreparable rotator cuff tears, Arthroscopy 10:363, 1994.
- Burns WC, Whipple TL: Anatomic relationships in the
You Might Also Like