Tibial Plateau Fractures: Comprehensive Evaluation and Surgical Management
Key Takeaway
The management of tibial plateau fractures requires a meticulous approach to restore articular congruity, axial alignment, and joint stability. Evaluation mandates advanced imaging, notably CT, to assess depression and comminution. Treatment ranges from nonoperative bracing for stable, minimally displaced patterns to complex internal or external fixation for bicondylar injuries. Surgical decision-making hinges on the degree of articular step-off, coronal plane instability, and the integrity of the surrounding soft-tissue envelope.
CLINICAL EVALUATION AND DIAGNOSTIC PROTOCOLS
The evaluation of a patient with a suspected tibial plateau fracture demands a systematic, highly disciplined approach. A thorough history must be obtained, focusing on the mechanism of injury—typically an axial load combined with varus or valgus stress—as well as the patient’s overall medical status, physiological age, and functional and economic demands. High-energy trauma (e.g., motor vehicle collisions, falls from height) often results in complex, bicondylar fracture patterns with severe soft tissue compromise, whereas low-energy mechanisms in osteoporotic bone frequently produce isolated lateral depression fractures.
A detailed physical examination is paramount. The surgeon must actively seek to detect concomitant ligamentous disruptions, neurovascular injuries, evolving compartment syndrome, and ipsilateral skeletal trauma.
Clinical Pearl: The soft tissue envelope dictates the timing and type of surgical intervention. Abrasions, fracture blisters, and severe contusions (Tscherne classification) must be meticulously documented. Surgical incisions through compromised soft tissue exponentially increase the risk of deep infection and wound dehiscence.
Neurovascular and Compartment Assessment
Vascular injuries, particularly to the popliteal artery, are highly associated with medial plateau (Schatzker IV) and bicondylar (Schatzker V and VI) fractures, as well as any fracture-dislocation variant. If clinical suspicion exists—indicated by diminished distal pulses, an Ankle-Brachial Index (ABI) less than 0.9, or asymmetric capillary refill—a CT angiogram or formal arteriogram must be obtained emergently. Patients with obvious vascular occlusion or transection require prompt transfer to the operating room for immediate vascular exploration, temporary skeletal stabilization (spanning external fixation), and revascularization.
Compartment syndrome is a devastating complication that can develop insidiously. The leg compartments must be palpated for tenseness, and pain out of proportion to the injury or pain with passive stretch of the toes should raise immediate alarm. If clinical suspicion exists, compartmental pressures must be measured using an accurate, objective method (e.g., Stryker needle). A differential pressure (ΔP) of less than 30 mm Hg between the diastolic blood pressure and the compartment pressure is an absolute indication for emergent four-compartment fasciotomy.
RADIOGRAPHIC AND ADVANCED IMAGING
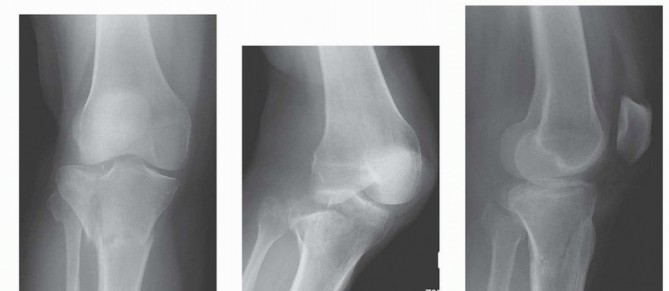
Standard radiographic evaluation includes anteroposterior (AP), lateral, and oblique views of the knee.
Surgical Warning: The upper tibial articular surface normally slopes posteriorly at an angle of 10 to 15 degrees. Therefore, a standard AP radiograph may obscure articular step-offs. An AP radiograph with the beam angled caudally 10 to 15 degrees (the "plateau view") is essential to provide a tangential view of the articular surface and accurately assess depression.
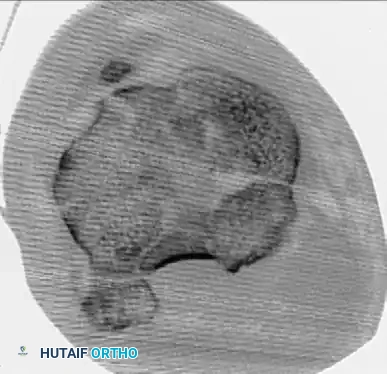
Computed Tomography (CT)
CT scanning with sagittal and coronal reconstructions is the gold standard for preoperative planning. Standard radiographs consistently underestimate the degree of articular depression and comminution. Assessment of the exact size, location, and depth of depressed articular fragments is often only possible with CT. It is common for the initial fracture classification based on plain films to be upgraded to a more complex type once the CT scan is reviewed, fundamentally altering the surgical approach and implant selection.
Magnetic Resonance Imaging (MRI)
The role of MRI in the acute evaluation of tibial plateau fractures is evolving. While not routinely indicated for fracture classification, MRI is unparalleled in identifying associated soft tissue injuries. Colletti, Greenberg, and Terk analyzed MRI findings in 29 tibial plateau fractures and reported a staggering incidence of concomitant injuries:
* Tibial collateral ligament injuries: 55%
* Lateral meniscal tears: 45%
* Anterior cruciate ligament (ACL) injuries: 41%
* Fibular collateral ligament injuries: 34%
* Posterior cruciate ligament (PCL) injuries: 28%
* Medial meniscal tears: 21%
Furthermore, Mustonen et al. demonstrated a 42% incidence of abnormal meniscal findings on MRI in plateau fractures, noting that 88% of patients with meniscal tears had unstable injury patterns.
PATHOANATOMY AND BIOMECHANICS
Regardless of the specific fracture pattern, intra-articular damage is almost universally more extensive than radiographs suggest. The bony attachments of one or both cruciate ligaments may be avulsed, lying as free osteochondral fragments within the joint space. Comminuted articular fragments are frequently rotated, lying at sharp angles to their normal anatomical plane, or even inverted.
The menisci are particularly vulnerable. The lateral meniscus is frequently torn at its periphery or detached, and a portion—or the entirety—of the meniscus may become incarcerated between the comminuted fracture fragments, blocking closed reduction.
The Role of the Fibula
Sarmiento et al. provided critical biomechanical insights into the behavior of these fractures under weight-bearing loads, noting that the integrity of the proximal fibula dictates the angular collapse of the tibia:
* Intact Fibula: Isolated lateral condyle fractures with an intact fibula resist further valgus collapse due to the lateral strut support. However, in bicondylar fractures with an intact fibula, the medial condyle tends to collapse, driving the knee into a varus deformity.
* Fractured Fibula: Lateral condyle fractures associated with a proximal fibula fracture lose their lateral support and have a high tendency to collapse into severe valgus.
TREATMENT PHILOSOPHY AND GOALS
The overarching goals in the treatment of proximal tibial articular fractures are:
1. Restoration of articular congruity.
2. Restoration of mechanical axial alignment.
3. Establishment of joint stability.
4. Return of functional, pain-free motion.
If operative intervention is selected, the internal or external fixation must be biomechanically stable enough to permit early range of motion (ROM). Prolonged postoperative immobilization inevitably leads to arthrofibrosis, resulting in a joint that is neither stable nor functional.
Indications for Operative vs. Nonoperative Management
Surgical treatment is definitively recommended for:
* Fractures associated with coronal or sagittal plane instability.
* Concomitant ligamentous injuries requiring repair/reconstruction.
* Significant articular displacement or depression.
* Open fractures.
* Fractures associated with compartment syndrome or vascular injury.
The exact degree of acceptable articular displacement remains highly controversial in orthopedic literature. Recommendations for surgical reduction vary from an articular step-off of >2 mm to >5 mm, or an axial alignment deviation of >5 degrees. Some authors have reported acceptable clinical outcomes with nonoperative treatment in stable fractures with up to 8 mm of depression. However, a universal consensus exists that depression or displacement exceeding 10 mm mandates surgical elevation and stabilization.
For stable fractures with less than 5 mm of depression, nonoperative treatment is appropriate. This consists of a few days of initial splinting to allow soft tissue swelling to subside, followed by early active ROM in a hinged knee brace and strictly delayed weight-bearing (typically 8 to 10 weeks).
Clinical Pearl: Long-term follow-up studies consistently demonstrate that post-traumatic osteoarthritis correlates more strongly with residual axial malalignment and joint instability than with the absolute millimeter measurement of initial articular depression. Therefore, the presence of varus or valgus instability of >10 degrees (tested with the knee flexed at 20 degrees to relax the posterior capsule) is an absolute indication for surgery, regardless of the radiographic step-off.
SURGICAL APPROACHES AND TECHNIQUES
Treatment modalities span a wide spectrum, including closed reduction and cast bracing, arthroscopically assisted percutaneous fixation, open reduction and internal fixation (ORIF) with plating, and external fixation (ring, wire, or monolateral). No single method is universally applicable; treatment must be highly individualized.
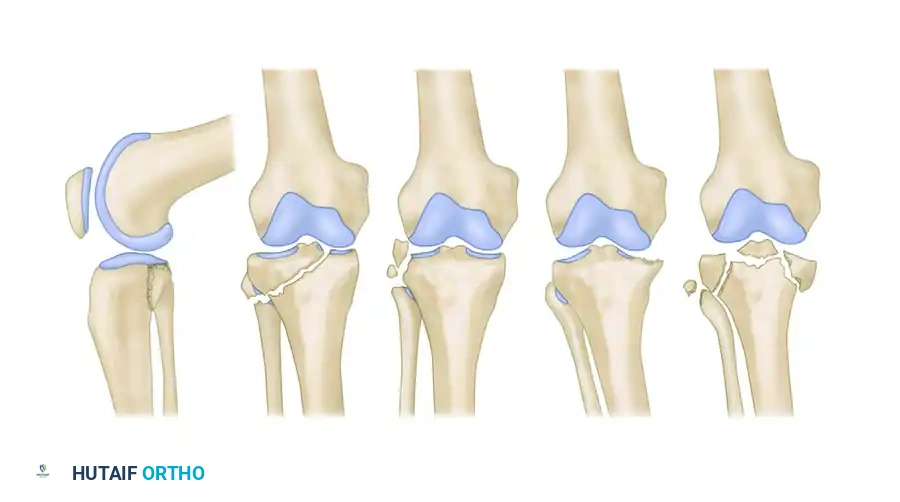
Arthroscopic and Percutaneous Techniques (Schatzker I-III)
Many lateral split fractures (Schatzker I) can be reduced percutaneously using large pointed reduction forceps under fluoroscopic guidance. Arthroscopic evaluation is highly recommended for operatively treated Schatzker I fractures to ensure the lateral meniscus is not incarcerated within the split. Once reduced, the fracture is stabilized with percutaneously placed large-fragment (6.5 mm or 7.3 mm) partially threaded cancellous screws.
For depressed articular segments (Schatzker II and III), ligamentotaxis alone is insufficient. These require elevation from below. A cortical window is created in the anterolateral tibial metaphysis. A bone tamp is advanced under fluoroscopic or arthroscopic visualization to carefully elevate the depressed subchondral bone. The resulting metaphyseal void must be filled with autograft, allograft, or a structural bone graft substitute to prevent subsidence.
Fixation is achieved using subchondral "rafting" screws. Biomechanical data by Patil et al. demonstrated that a raft of four 3.5-mm screws provides superior resistance to axial compression compared to two traditional 6.5-mm screws.


If the lateral condylar fracture is associated with a fibular head fracture or significant comminution, a lateral anatomically contoured buttress plate is required to prevent valgus collapse.
Open Reduction and Internal Fixation (ORIF)
Displaced fractures of the medial condyle (Schatzker IV) are high-energy, highly unstable injuries. They are best treated with open reduction and application of a medial buttress plate. Because the medial plateau bears approximately 60% of the knee's weight-bearing load, robust biomechanical support is mandatory.
For complex bicondylar fractures (Schatzker V and VI), traditional extensile exposures (e.g., Mercedes-Benz incisions or massive single midline incisions with extensive stripping) have historically resulted in catastrophic soft tissue complications, including flap necrosis and deep osteomyelitis.
Modern techniques emphasize minimally invasive plate osteosynthesis (MIPO) and dual plating through separate incisions. Mills and Nork demonstrated that dual plating can be safely achieved by utilizing an anterolateral incision combined with a posteromedial incision, leaving a wide, well-vascularized soft tissue bridge. Subperiosteal dissection is strictly limited to the fracture margins and the footprint of the plate. The use of small-fragment (3.5-mm) AO/ASIF T-plates has gained favor; their lower profile and increased malleability provide excellent buttressing of osteochondral fragments with significantly less soft tissue irritation than bulky 6.5-mm L-plates.
MANAGEMENT OF COMPLEX FRACTURES (SCHATZKER V & VI)
Severe tibial plateau fractures—characterized by bicondylar involvement, metaphyseal-diaphyseal dissociation, open wounds, or severe closed soft tissue crush injuries (Tscherne II/III)—present a formidable challenge.
Damage Control Orthopedics
In the presence of severe soft tissue compromise, immediate definitive internal fixation is contraindicated. Tscherne and Lobenhoffer established the protocol of temporarily spanning the knee with a joint-spanning external fixator. This maintains axial alignment and length via ligamentotaxis while allowing the soft tissue envelope to recover. Definitive internal fixation is delayed for 7 to 14 days until the "wrinkle sign" appears, indicating subsided edema.
Definitive External Fixation
When soft tissue conditions preclude internal fixation entirely, or in highly contaminated open fractures, definitive treatment with external fixation is indicated. Minimal soft tissue dissection is required, drastically reducing the risk of iatrogenic devascularization and deep infection.
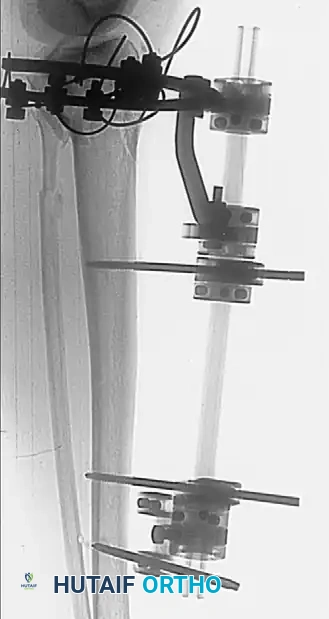
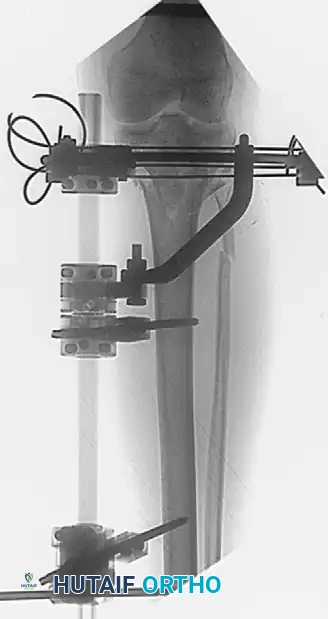

Ring and Wire Fixation (Ilizarov Method):
Clinical studies demonstrate that fine-wire circular fixators yield 87% to 88% good or excellent functional results in complex plateau fractures, with superficial pin tract infections occurring in only 6.5% to 12% of cases. A properly tensioned four-wire construct provides biomechanical stability comparable to dual plating.
In a series of 57 patients with Schatzker type VI fractures treated with Ilizarov fixation (38% of which were open fractures), acceptable reductions yielded an average knee ROM of 115 degrees.




Surgical Warning: Anatomical studies confirm that the knee joint capsule reflects distally up to 14 mm below the articular margin. To prevent the catastrophic complication of septic arthritis tracking from a superficial pin site, all wires and half-pins must be placed strictly extra-capsularly—at least 14 mm distal to the joint line.
Hybrid and Monolateral Fixation:
Monolateral half-pin external fixators or hybrid frames (combining a proximal tensioned wire ring with distal diaphyseal half-pins) offer alternative solutions. These frames are technically less demanding to apply than full Ilizarov frames and allow excellent access for wound care. Accessory percutaneous cancellous screws are frequently utilized in conjunction with the frame to compress and maintain the articular reduction, while the frame neutralizes bending and torsional forces across the metaphyseal-diaphyseal junction.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of tibial plateau fracture surgery relies heavily on postoperative rehabilitation.
* Immobilization: The knee is typically placed in a hinged knee brace.
* Motion: Continuous Passive Motion (CPM) or active-assisted ROM is initiated immediately postoperatively, provided the fixation is rigid. Early motion is critical for cartilage nutrition and preventing arthrofibrosis.
* Weight-Bearing: Patients are maintained on strict non-weight-bearing (NWB) or toe-touch weight-bearing (TTWB) status for 8 to 12 weeks, depending on the fracture pattern and radiographic evidence of callus formation. Premature weight-bearing is the leading cause of hardware failure and late articular subsidence.
Routine clinical and radiographic follow-up is required to monitor for loss of reduction, hardware complications, and the late development of post-traumatic osteoarthritis, which may eventually necessitate total knee arthroplasty (TKA) in severe cases.
You Might Also Like