Mastering Tibial Fractures: Complex Sequelae, Plateau Injuries, and Advanced Management Strategies
Key Takeaway
Tibial fractures frequently present with complex sequelae, including delayed union, compartment syndrome, and post-traumatic foot deformities. Successful management requires a thorough understanding of fracture biomechanics, soft tissue envelopes, and precise surgical interventions. This guide details evidence-based protocols for addressing tibial plateau fractures, checkrein deformities, intramedullary nail exchange, and external fixation techniques to optimize patient outcomes and restore lower extremity function.
INTRODUCTION TO TIBIAL FRACTURE COMPLICATIONS AND SEQUELAE
The management of tibial fractures extends far beyond the achievement of osseous union. Due to the tibia’s precarious subcutaneous anteromedial border, tenuous blood supply, and proximity to complex multi-articular muscle groups, fractures of the tibial shaft and plateau are fraught with potential complications. These range from acute neurovascular compromise and compartment syndrome to chronic, debilitating conditions such as delayed union, nonunion, and post-traumatic foot deformities.
For the practicing orthopedic surgeon, mastering the nuances of these complications is paramount. This comprehensive guide explores the pathoanatomy, biomechanics, and advanced surgical management of post-traumatic foot deformities, complex tibial plateau fractures, delayed unions, and the strategic use of adjuvant fibular fixation and external fixators.
DEFORMITIES OF THE FOOT AND TOES AFTER TIBIAL FRACTURE
Fractures of the tibial diaphysis, particularly those involving the distal third, can precipitate unique and functionally limiting deformities of the foot and toes. These deformities are often the result of soft tissue tethering, ischemic contracture, or unrecognized compartment syndrome rather than primary osseous malalignment.
The Checkrein Deformity
First described by McKeever, the checkrein deformity is a highly specific dynamic contracture of the great toe that occurs following fractures of the distal third of the tibia.
Pathoanatomy and Biomechanics
The deformity arises when the flexor hallucis longus (FHL) muscle or its tendon becomes densely adherent to the fracture callus or scar tissue at the distal tibial fracture site. This tethering creates a functional "bowstring" effect between the point of adherence and the tendon’s insertion at the base of the distal phalanx of the great toe.
Clinical Presentation
The hallmark of a checkrein deformity is its dynamic nature, which is directly linked to the position of the ankle joint:
* Ankle Dorsiflexion: The great toe is pulled into sharp, rigid plantarflexion. The pressure of the plantar surface of the great toe against the sole of the shoe during the terminal stance phase of gait produces a painful, intractable plantar keratosis (callus).
* Ankle Plantarflexion: The tension on the tethered FHL is relieved, allowing the interphalangeal (IP) joint of the great toe to extend completely.
Clinical Pearl: Always perform a dynamic assessment of toe extension with the ankle in varying degrees of dorsiflexion and plantarflexion in patients presenting with toe clawing post-tibial fracture. This differentiates a tethered FHL from a fixed structural contracture.
Surgical Management
If conservative measures (such as shoe modifications) fail and the fracture has fully united, surgical intervention is indicated.
1. Attempted Tenolysis: Initial attempts may be made to free the FHL muscle belly and tendon from the distal tibial callus. However, due to dense fibrosis, this is often technically demanding and carries a high risk of recurrence.
2. Tendon Lengthening: If proximal tenolysis is impossible or deemed high-risk, the definitive treatment is lengthening of the FHL tendon within the foot.
* Approach: A medial longitudinal incision is made along the midfoot.
* Technique: A Z-lengthening (Z-plasty) of the FHL tendon is performed posterior to the master knot of Henry. The tendon is lengthened sufficiently to allow full IP joint extension with the ankle in maximal dorsiflexion.
* Postoperative Protocol: The foot is immobilized in a short leg cast with the ankle in neutral and the great toe in extension for 4 to 6 weeks, followed by aggressive active range-of-motion (ROM) exercises.
Clawfoot and Cavus Deformities
Clawfoot or cavus deformities are severe, rigid structural abnormalities that can develop after tibial shaft fractures.
Pathophysiology
These deformities are almost exclusively the sequelae of unrecognized or late-diagnosed deep posterior compartment syndrome. Trauma, edema, and ischemia lead to myonecrosis and subsequent fibrous contracture of the deep posterior compartment musculature (tibialis posterior, flexor digitorum longus, and flexor hallucis longus).
Diagnostic Pitfalls
A critical diagnostic error is misinterpreting a cavovarus foot deformity as an inward malrotation (internal tibial torsion) of the healed tibial fracture.
* Differentiation: Assess the transmalleolar axis and the thigh-foot angle. In ischemic contracture, the tibial alignment may be anatomic, but the midfoot and hindfoot will demonstrate rigid varus and cavus driven by the contracted deep flexors.
Surgical Management
Management of established ischemic contracture is complex and often requires radical soft tissue releases, such as fractional lengthening of the deep flexors, plantar fascia release, and in severe cases, corrective midfoot or hindfoot osteotomies (e.g., triple arthrodesis) to restore a plantigrade, braceable foot.
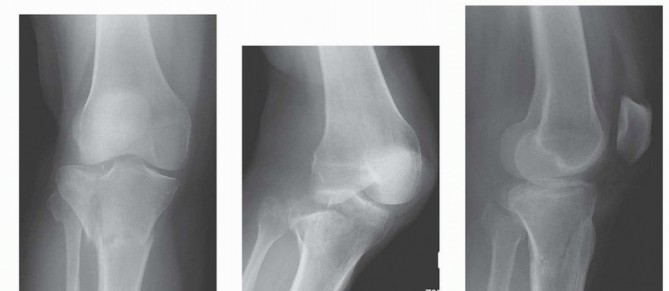
TIBIAL PLATEAU FRACTURES AND COMPLEX KNEE TRAUMA
Proximal tibial articular fractures represent a spectrum of injuries ranging from low-energy osteoporotic depressions to high-energy, limb-threatening fracture-dislocations. The management of these injuries requires a meticulous understanding of both the osseous architecture and the surrounding soft tissue envelope.
Mechanism of Injury and Energy Patterns
High-Energy Trauma
Fractures caused by motor vehicle collisions, pedestrian-bumper strikes, or falls from significant heights impart massive kinetic energy to the proximal tibia. These are frequently associated with:
* Severe soft tissue contusions and degloving (Morel-Lavallée lesions).
* Open wounds.
* Acute compartment syndrome.
* Popliteal artery and peroneal nerve injuries.
Low-Energy Trauma
Conversely, sports injuries or simple falls in elderly patients with osteopenia typically produce "pure" fracture patterns, such as local compression (depression) or split-compression fractures. Schulak and Gunn demonstrated that the frequency of specific fracture types and associated collateral ligament injuries correlates directly with the vector and magnitude of the applied force.
Classification and Soft Tissue Assessment
Tscherne and Lobenhoffer Classification
Tscherne and Lobenhoffer provided a critical distinction between "pure" plateau fracture patterns and fracture-dislocation patterns:
* Pure Plateau Fractures: Account for the majority of meniscal injuries (67%). The primary force is axial loading with varus/valgus stress.
* Fracture-Dislocation Patterns: Highly unstable injuries where the primary force involves translation or subluxation. These account for 96% of cruciate ligament injuries and 85% of medial collateral ligament (MCL) injuries. Peroneal nerve injury is twice as common in this group.
Surgical Warning: In minimally displaced, local compression, or split-compression fractures, the osseous injury may mask severe ligamentous instability. It is imperative to obtain stress radiographs or MRI of the knee to evaluate the cruciate and collateral ligaments once the fracture is provisionally stabilized.
Complex Knee Trauma
This term describes injuries with significant damage to two or more of the following:
1. The soft tissue envelope.
2. The ligamentous stabilizers.
3. The bony structures of the distal femur and proximal tibia.
In complex fractures involving both femoral and tibial articular surfaces, the incidence of vascular injury is 25%, and compartment syndrome is 25%. In the presence of severe soft tissue injury, these rates climb to 31% for vascular injury, 31% for compartment syndrome, and 23% for peroneal nerve injury.
The Schatzker Classification and Type VI Fractures
The Schatzker classification remains the gold standard for categorizing tibial plateau fractures. Schatzker Type VI is particularly challenging, defined by a transverse or oblique fracture through the metaphysis that dissociates the diaphysis from the articular metaphysis.
* Biomechanics: This pattern represents a complete loss of structural continuity between the knee joint and the tibial shaft, requiring robust dual-plate fixation or hybrid external fixation to restore the mechanical axis and prevent varus/valgus collapse.
MANAGEMENT OF DELAYED UNION IN TIBIAL FRACTURES
Delayed union and nonunion are formidable complications, particularly following high-energy open fractures or fractures with significant comminution. When a tibial fracture treated with an unreamed intramedullary nail fails to progress toward union by 4 to 6 months, strategic intervention is required.
Intramedullary Nail Exchange and Reaming
The gold standard for treating aseptic delayed union of a diaphyseal tibial fracture previously treated with an unreamed nail is nail exchange with sequential reaming.
Indications
* Delayed unions in fractures with small diameter (e.g., 8 mm) or loose implants.
* Axially unstable fractures.
* Perimetaphyseal fractures where the initial nail failed to provide adequate working length.
Biomechanical and Biological Rationale
Removing the small unreamed nail and sequentially reaming the medullary canal serves a dual purpose:
1. Biological Stimulation: Reaming generates autologous bone graft (reamings) that is deposited at the fracture site. It also incites a localized inflammatory response, increasing endosteal blood flow and stimulating osteogenesis.
2. Biomechanical Stability: Inserting a larger diameter nail increases the area moment of inertia, significantly enhancing the construct's resistance to bending and torsional forces.
Contraindications
Nail exchange is generally unsuccessful and potentially contraindicated in:
* Fractures with segmental bone loss exceeding one-third to one-half of the cortical circumference.
* Type IIIB open fractures with a history of deep infection, where reaming may precipitate a fulminant osteomyelitis.
Percutaneous Bone Grafting
For fractures with significant bone loss, or in cases of severe Type IIIB open fractures where reaming is contraindicated, percutaneous autologous bone grafting (typically harvested from the iliac crest or utilizing Reamer-Irrigator-Aspirator [RIA] systems) remains a time-tested, highly effective method to stimulate union.
Dynamization
Historically, dynamization—the removal of static interlocking screws from the longer segment of the nail—was widely used to allow axial impaction of the fracture site during weight-bearing.
* Prerequisite: The fibula must not have healed; an intact fibula will act as a strut, preventing tibial compression.
* Risks: Dynamization carries a significant risk of destabilization. Loss of reduction, leading to shortening or angular malalignment, has been reported in up to 16% of proximal and distal third tibial fractures following dynamization. It should be used judiciously and is generally reserved for axially stable, transverse midshaft fractures.
ADJUVANT FIXATION OF THE FIBULA
While routine internal fixation of the fibula is unnecessary in the majority of tibial shaft fractures, there are specific biomechanical scenarios where fibular stabilization is a critical adjuvant procedure.
Indications for Fibular Fixation
1. Distal Tibial Metaphyseal Fractures: In highly comminuted fractures of the distal tibia treated with intramedullary nailing, the lack of cortical contact can lead to valgus collapse. Plating the fibula restores the lateral column of the leg, acting as a lateral tension band and preventing valgus malalignment of the tibia.
2. Severe Soft Tissue Compromise: When severe soft tissue damage or gross contamination over the medial tibia precludes safe internal fixation of the tibia, stabilizing the fibula with a plate or a retrograde intramedullary nail (inserted through the lateral malleolus) can provide partial, indirect stability to the tibial fracture.
3. Syndesmotic Instability: Any fibular fracture associated with distal tibiofibular syndesmotic disruption requires anatomic reduction and fixation to restore the ankle mortise.
EXTERNAL FIXATION MANAGEMENT AND SOFT TISSUE PROTECTION
In the acute management of complex tibial fractures (such as Schatzker VI plateau fractures or severe open diaphyseal fractures), external fixation—either spanning damage-control frames or definitive circular/hybrid frames—is frequently employed.
Frame Modification and Skin Protection
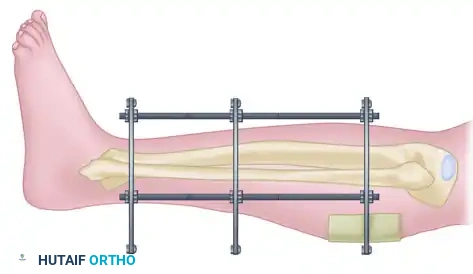
A critical aspect of external fixation management is the continuous assessment of the soft tissue envelope. Post-traumatic edema can cause the skin to swell significantly, leading to impingement against the rigid components of the external fixator frame.
Figure A: Impingement of the edematous skin on the rigid components of the external fixation frame, a precursor to pressure necrosis and pin tract infection.
If skin impingement occurs, the frame must be modified immediately to prevent pressure necrosis, which can rapidly progress to deep infection or expose underlying hardware/bone.
Modification Technique
If a smaller frame or ring needs to be disassembled or adjusted to accommodate swelling, cannulated wire fixation bolts from the original frame can be carefully taped or secured against the new frame construct. This modular modification can often be executed without loosening the tensioned transfixion wires or losing the osseous reduction.
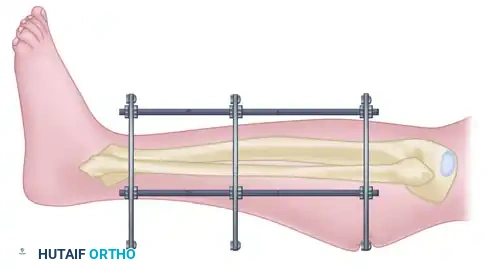
Figure B: The strategic use of thin cardboard or sterile padding interposed between the frame and the skin to distribute pressure and prevent focal pressure necrosis during acute edema phases.
Clinical Pearl: Always leave a minimum of two fingerbreadths (approx. 3-4 cm) of clearance between the skin and the external fixator rings or bars during initial application to accommodate anticipated postoperative swelling. If swelling exceeds this clearance, prompt frame adjustment and the use of sterile pressure-distributing barriers are mandatory.
CONCLUSION
The successful management of tibial fractures demands a comprehensive approach that anticipates and aggressively manages complications. Whether addressing the dynamic tethering of a checkrein deformity, navigating the complex soft-tissue and osseous disruption of a Schatzker VI plateau fracture, or executing a biologically sound nail exchange for a delayed union, the orthopedic surgeon must rely on strict evidence-based principles. By respecting the soft tissue envelope, understanding the biomechanics of fixation, and intervening decisively when complications arise, surgeons can optimize functional recovery and mitigate the long-term morbidity associated with these challenging injuries.
You Might Also Like