Digital & Thumb Joint Arthrodesis: An Intraoperative Masterclass

Key Takeaway
Join us in the OR for a masterclass on hand joint arthrodesis. We'll meticulously cover indications, comprehensive anatomy, precise preoperative planning, and detailed step-by-step intraoperative execution for DIP, PIP, and MCP fusions. Learn critical techniques, fixation options, and how to navigate potential pitfalls, ensuring optimal outcomes and stability for your patients.
Introduction: The Art of Small Joint Arthrodesis in the Hand
Alright, fellows, welcome to the operating theater. Today, we're delving into the nuanced world of small joint arthrodesis in the hand – a fundamental procedure that, when executed with precision, offers profound pain relief and stability for our patients. This isn't just about fusing bones; it's about restoring function, improving quality of life, and making a critical decision to eliminate motion for the greater good of the digit.
Indications for Arthrodesis
The need for arthrodesis in the hand arises from a spectrum of challenging conditions. Fundamentally, we consider this procedure when a joint is irrevocably damaged, unstable, or painful, and motion preservation is either impossible, undesirable, or detrimental to overall hand function.
Let's break down the primary indications:
- Arthritis: This is, by far, the most common culprit.
- Osteoarthritis (OA): Primarily affects the distal interphalangeal (DIP) joints, but can also involve the proximal interphalangeal (PIP) and metacarpophalangeal (MCP) joints, particularly in the index and middle fingers. Patients often present with painful, swollen joints, osteophytes, mucous cysts, Heberden nodes at the DIPs, and angular deformities.
- Inflammatory Arthritis: Conditions like rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), psoriatic arthritis, and scleroderma.
- In RA, persistent synovitis leads to cartilage loss and attenuation of supporting structures (collateral ligaments, extensor tendons), causing deformities like ulnar drift at the MCPs, or boutonnière deformities at the PIPs due to central slip attenuation.
- SLE primarily affects supporting structures, resulting in joint subluxation or dislocation despite relatively normal cartilage, making joint salvage attempts difficult.
- Psoriatic arthritis can lead to remarkable bone loss, often presenting as "pencil-in-cup" deformities or the severe bone resorption characteristic of arthritis mutilans. Arthrodesis is often the most reliable method to halt this destructive process.
- Scleroderma typically causes PIP flexion and MCP extension contractures, often compounded by impaired digital vascularity leading to dorsal PIP ulcers and central slip attenuation.
- Crystalline Arthropathy: Gout, for example, can present as indolent gouty tophi over the DIP joint or as an acutely painful, swollen, tender joint. Untreated, it progresses to a resorptive arthritis.
- Infection: Septic arthritis can rapidly destroy a joint. A "fight bite" directly inoculates the MCP joint, demanding aggressive management. Contiguous spread from adjacent infections (e.g., felon) or wounds can also destroy joints. Hematogenous spread is rare in the hand.
- Unreconstructable Soft Tissue Problems: Severe periarticular soft tissue injuries can lead to profound joint stiffness even if the articular cartilage is initially spared. Conditions like central slip disruptions can confound reconstruction efforts, making arthrodesis a more predictable solution.
- Certain Neurologic Conditions: Nerve injuries can create profound muscle imbalances in the hand. Arthrodesis can simplify complex reconstructions, stabilizing a joint to improve overall functional grasp or pinch.
- Posttraumatic Arthritis: Intra-articular fractures and fracture-dislocations, especially if they result in residual joint incongruity, frequently lead to posttraumatic arthritis. The PIP joint, in particular, has a low tolerance for injury.
Arthrodesis Versus Arthroplasty: A Critical Decision
This is often the first major decision point, and it's one we make in conjunction with the patient, carefully weighing the trade-offs. The fundamental difference: arthrodesis eliminates motion for stability and pain relief, while arthroplasty aims to preserve some motion.
- DIP Joint: For the DIP joint, arthrodesis is a highly reliable procedure. The functional impairment from losing DIP joint motion is minimal, often imperceptible to the patient. Stability and pain relief are the paramount goals here.
- PIP Joint: This is where the decision becomes more complex. We must weigh the benefits of stability and pain relief against the functional impact of losing PIP joint motion.
- Index Finger: PIP joint stability is absolutely critical for precision pinch. Therefore, for isolated, unreconstructable PIP problems, the index finger typically gets an arthrodesis.
- Small Finger: Conversely, mobility in the small finger PIP joint is crucial for a strong power grip. Thus, the small finger often receives an arthroplasty.
- Middle and Ring Fingers: For these digits, the choice is more nuanced; the middle finger may get an arthrodesis or arthroplasty, and the ring finger often gets an arthroplasty.
- Exceptions: Always remember, fellows, that associated unsalvageable tendon problems or significant soft tissue coverage issues may push us towards arthrodesis even in digits where arthroplasty might otherwise be considered.
- Adjacent Joints in Inflammatory Arthritis: In patients with rheumatoid arthritis, particularly with both MCP and PIP involvement, there's a temptation to perform arthroplasties on all affected joints. However, so-called "double-row arthroplasties" tend to compromise the results at both levels. In these complex scenarios, the strategic goal is often to prioritize stability at the PIP joint (arthrodesis) and motion at the MCP joint (arthroplasty) to optimize overall hand function.
- Thumb MCP Joint: Arthrodesis of the thumb MCP joint is a remarkably reliable procedure for managing arthritis and unreconstructable ligament problems. It is, in fact, a far superior procedure to arthroplasty for the thumb MCP. A classic indication is a chronic radial collateral ligament tear with static volarulnar subluxation. However, before committing to a thumb MCP fusion, it is absolutely critical to ensure adequate motion and function of the adjacent joints – specifically, the interphalangeal (IP) and carpometacarpal (CMC) joints. If these joints are stiff, fusing the MCP will severely cripple the thumb.
- Digital MCP Joints (Digits 2-5): Arthrodesis of the digital MCP joints is not commonly performed, as motion here is quite important for grasp. Indications are reserved for very specific, challenging cases:
- Multiply failed arthroplasty.
- Inadequate bone stock for arthroplasty.
- Unrelenting infection.
- Refractory instability, particularly of the index MCP joint.
- An unreconstructable extensor mechanism.
Ultimately, remember that candidates for arthrodesis must fully understand that all motion in the affected joint will be permanently eliminated. The principal, non-negotiable goals are pain relief and enhanced stability.
Comprehensive Surgical Anatomy of the Hand Joints
Before we make any incision, a thorough understanding of the intricate anatomy of the hand joints is paramount. This knowledge guides our dissection, protects vital structures, and informs our fusion strategy.
Distal Interphalangeal (DIP) Joint Anatomy
Let's begin distally. The DIP joints are classic hinge joints, primarily allowing flexion and extension.
- Bony Architecture: The condylar head of the middle phalanx is biconvex, while the reciprocal base of the distal phalanx is biconcave with a central ridge. This configuration inherently limits lateral translation and rotation.
- Volar Plate: This strong fibrocartilaginous structure extends from the neck of the middle phalanx to the volar base of the distal phalanx, acting as a critical checkrein against hyperextension.
- Collateral Ligaments:
- True Collateral Ligaments: These originate from the condylar head of the middle phalanx and insert onto the volar-lateral aspects of the distal phalanx. They are effectively isometric throughout the range of motion, providing primary stability.
- Accessory Collateral Ligaments: These extend from the condylar head to the volar plate, resisting lateral translation when the joint is extended.
- Extensor Mechanism: Dorsally, the extensor tendon crosses the DIP joint as the terminal tendon, inserting slightly distal to the dorsal base of the distal phalanx.
- Clinical Pearl: Be acutely aware that the germinal matrix of the nailbed is remarkably close to this terminal tendon insertion, averaging only 1.3 mm distal. Any aggressive dorsal dissection or drilling can easily damage the nail matrix, leading to permanent nail deformity.
- Flexor Mechanism: Volarly, the flexor digitorum profundus (FDP) tendon inserts broadly onto the volar aspect of the distal phalanx, extending from the base to the midshaft. This powerful tendon provides the primary flexion force for the DIP joint.
- Neurovascular Structures: The digital nerves and arteries run along the lateral aspects of the digit, volar to the collateral ligaments. While less vulnerable in a direct dorsal approach, careful lateral retraction is essential to avoid injury, especially during bone preparation or K-wire insertion.
Proximal Interphalangeal (PIP) Joint Anatomy
Moving proximally, the PIP joints are also highly constrained hinge joints, structurally quite similar to the DIPs but with greater functional demands.
- Bony Architecture: Like the DIPs, the condylar head of the proximal phalanx is biconvex, articulating with the biconcave base of the middle phalanx, again featuring a central ridge.
- Volar Plate: Similar to the DIP, the PIP volar plate prevents hyperextension, extending from the neck of the proximal phalanx to the volar base of the middle phalanx.
- Collateral Ligaments:
- True Collateral Ligaments: Originating from the condylar head of the proximal phalanx, inserting onto the volar-lateral aspects of the middle phalanx. Isometric.
- Accessory Collateral Ligaments: Extending from the condylar head to the volar plate, resisting lateral translation in extension.
- Extensor Mechanism: Over the PIP joint, the extensor apparatus is more complex, splitting into three distinct components:
- Central Slip: Formed by contributions from the extensor tendon, interosseous tendons, and lumbricals, it inserts onto the dorsal base of the middle phalanx. This is the primary extensor of the PIP joint.
- Lateral Bands: These travel past the PIP joint along the lateral margins of the middle phalanx, eventually combining distally to form the terminal tendon for DIP extension.
- Flexor Mechanism: The flexor digitorum superficialis (FDS) tendon splits to insert on the volar-lateral margins of the proximal shaft of the middle phalanx, providing primary PIP flexion. Deep to the FDS, the FDP tendon continues distally to the DIP joint.
- Neurovascular Structures: Again, the digital nerves and arteries run along the lateral aspects, volar to the collateral ligaments. They are particularly vulnerable during lateral dissection or if K-wires are placed too far laterally or volarly.
Metacarpophalangeal (MCP) Joint Anatomy (Digits 2-5)
The MCP joints are distinct from the interphalangeal joints; they are multiaxial, permitting motion in multiple planes – flexion/extension, abduction/adduction, and some rotation.
- Bony Architecture: The metacarpal head has a complex, convex, pear-shaped configuration, being wider volarly than dorsally. The radius of curvature increases progressively from dorsal to volar. The reciprocal base of the proximal phalanx is biconcave.
- Collateral Ligaments:
- Metacarpal Attachment: Crucially, the metacarpal attachment of the true collateral ligaments is dorsal to the axis of rotation.
- Phalangeal and Volar Plate Attachments: Similar to the interphalangeal joints.
- Functional Consequence: Due to the metacarpal head shape and ligament attachments, the MCP joints are typically more lax in extension and become tight in flexion. This is vital for understanding functional positioning.
- Volar Plate: A robust structure preventing hyperextension, extending from the neck of the metacarpal to the volar base of the proximal phalanx.
- Extensor Mechanism: In the other digits (2-5), there is no direct extensor tendon attachment to the proximal phalanx. MCP joint extension occurs through a "sling effect" of the sagittal hood fibers lifting the proximal phalanx via the pull of the extensor digitorum communis tendon.
- Flexor Mechanism: MCP joint flexion is produced by a combination of direct intrinsic tendon attachments to the volar-lateral phalangeal base and indirect actions of the intrinsics on the more distal transverse fibers of the extensor hood.
- Neurovascular Structures: The common digital nerves and vessels branch into proper digital nerves and vessels just proximal to the MCP joint. They run along the lateral aspects of the metacarpal neck and proximal phalanx, making them susceptible to injury during capsular dissection, particularly on the radial side of the index finger and ulnar side of the small finger.
Thumb Metacarpophalangeal (MCP) Joint and Interphalangeal (IP) Joint Anatomy
The thumb's joints, while similar in principle, have unique features crucial for its specialized function.
- Thumb MCP Joint:
- Bony Architecture: Significant variability exists in the shape of the thumb metacarpal head; some are more square than round, potentially limiting lateral translation and MCP flexion.
- Extensor Mechanism: The extensor pollicis brevis (EPB) tendon inserts onto the dorsal base of the proximal phalanx. The size of the EPB tendon is variable. For some patients, the extensor pollicis longus (EPL) tendon assumes the major role in MCP joint extension.
- Collateral Ligaments & Volar Plate: Similar to the digital MCPs in structure and function.
- Neurovascular Structures: Proper digital nerves and vessels run laterally, volar to the collateral ligaments. The radial digital nerve to the thumb is particularly vulnerable dorsoradially.
- Thumb IP Joint:
- Structurally, it functions as a hinge joint, very similar to the digital DIP and PIP joints.
- Extensor Mechanism: The EPL tendon crosses the IP joint dorsally, inserting onto the dorsal base of the distal phalanx.
- Flexor Mechanism: The flexor pollicis longus (FPL) tendon inserts onto the volar aspect of the distal phalanx.
- Neurovascular Structures: Proper digital nerves and vessels run along the lateral aspects.
Neurovascular Considerations
A constant awareness of the neurovascular bundles is critical across all these joints. The proper digital nerves and arteries run along the lateral aspects of each digit, volar to the collateral ligaments. Dissection must be meticulous, staying dorsal and central when possible, and employing careful, blunt dissection laterally. Always consider the potential for nerve irritation or injury during hardware placement, especially K-wires, which can directly impinge on these structures if misplaced.
Patient Assessment and Preoperative Planning
Fellows, the success of any surgical procedure begins long before the first incision. It starts with a comprehensive understanding of the patient, their condition, and meticulous preoperative planning.
Patient History and Physical Examination
- Chief Complaint: Pain is the most common complaint prompting consideration for arthrodesis. It's crucial to ensure the location of the pain correlates precisely with the joint in question.
- Functional Impact: Clearly define the functional limitations imposed by the problem. How does it affect their daily activities, occupation, and avocational pursuits? Document handedness.
- History of Present Illness:
- For single joint involvement, always seek a history of trauma.
- For acute, painful swelling, consider penetrating injury, gout, or recent infection.
- For chronic conditions, inquire about the progression of symptoms and previous treatments.
- Past Medical History: Specifically inquire about inflammatory conditions (rheumatoid arthritis, SLE, psoriatic arthritis, scleroderma), crystalline arthropathies, and any history of infection. For rheumatoid patients, discuss their current medication regimen with their rheumatologist.
- Physical Examination: This must be thorough and systematic.
- Inspection: Observe the appearance of the joints and overlying skin. Look for Heberden nodes (DIP OA), mucous cysts (DIP OA), onycholysis or eczema (psoriatic arthritis), and deformities like swan-neck (DIP flexion deformity with secondary PIP hyperextension) or boutonnière (PIP central slip attenuation). Note any erythema, swelling, or skin changes.
- Palpation: Localize tenderness to the affected joint. Assess for warmth or effusions.
- Range of Motion (ROM): Measure active and passive ROM for the affected joint and, critically, all adjacent joints. Discrepancies between active and passive motion may indicate associated tendon problems.
- Stability: Perform stress examination to demonstrate collateral ligament incompetence, especially at the MCP joints.
- Neurovascular Status: Assess sensibility (two-point discrimination) and capillary refill.
- Grip and Pinch Strength: Quantify these to establish a baseline and assess functional impact.
- Adjacent Joint Status: This is paramount. For example, in a rheumatoid patient with both MCP and PIP involvement, the status of both joints dictates the overall surgical strategy. For the thumb MCP, ensure adequate motion at the IP and CMC joints.
Diagnostic Imaging and Laboratory Studies
- Plain Radiographs: These are the cornerstone. Obtain posteroanterior (PA), lateral, and oblique views of the affected digit. These are usually sufficient for diagnosis.
- Look for joint space narrowing, osteophytes, subchondral cysts, erosions, and subluxation.
- In psoriatic arthritis, look for "pencil-in-cup" deformities or severe bone resorption (arthritis mutilans).
- Assess bone stock, quality, and size, which are crucial for determining the optimal fixation type.
- Laboratory Studies:
- Inflammatory Arthritis: If suspected, order a collagen vascular screen: rheumatoid factor (RF), antinuclear antibody (ANA), complete blood count (CBC) with differential, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP).
- Crystalline Arthropathy: A uric acid level may be drawn in cases of suspected gout.
- Infection: While blood tests are generally not helpful for acute finger infections, a CBC with differential and inflammatory markers (ESR, CRP) can support the diagnosis of septic arthritis.
- Advanced Imaging (Rarely Needed): MRI or ultrasound may rarely be ordered to evaluate specific tendon pathology if stiffness is associated with a suspected tendon abnormality.
Nonoperative Management Strategies
Before considering surgery, we always explore and optimize nonoperative management.
- Oral Medications: For OA and posttraumatic arthritis, oral anti-inflammatory agents (NSAIDs) can reduce pain and stiffness. For rheumatoid patients, modifications in their medication regimen, supervised by a rheumatologist, are essential. Glucosamine and chondroitin sulfate appear to be of limited value for hand arthritis.
- Splints:
- Resting Splints: Simple padded aluminum splints for DIP and PIP joints, or hand-based thermoplast splints for the thumb MCP joint, can reduce pain and inflammation by immobilizing the joint.
- Corrective Splints: Dynamic or static progressive splints (e.g., safety pin static progressive or LMB dynamic splint) are generally not tolerated when the joint is inflamed.
- Buddy Taping: May be appropriate for some MCP joint problems to provide support.
- Corticosteroid Injections: Intra-articular corticosteroid injections can provide temporary relief of pain and synovitis.
- Technique: Use a 27-gauge needle and inject 0.5 mL of Celestone Soluspan mixed with 0.5 mL of 1% Xylocaine.
- Approach: A dorsal approach is generally preferred.
- Consideration: Be aware that the joint capacity is quite small, and the joint may be difficult to access.
Preoperative Surgical Planning
Once the decision for arthrodesis is made, meticulous planning is key.
Patient Positioning and OR Setup
- Patient Position: The patient is typically supine on the operating table.
- Arm Positioning: The affected arm is placed on a radiolucent hand table, ensuring full access for the surgeon and unobstructed fluoroscopy. A pneumatic tourniquet is applied to the upper arm.
- Anesthesia: Regional block (e.g., axillary block) combined with sedation, or general anesthesia, is preferred.
- Sterile Prep and Drape: The entire hand and forearm are prepped and draped in a sterile fashion, allowing for full range of motion of the digits during positioning.
Fluoroscopy and Imaging Setup
- C-arm: A C-arm fluoroscopy unit is essential. It should be positioned to allow for immediate, unobstructed anteroposterior (AP) and lateral views of the affected joint without repositioning the hand.
- Image Intensifier: Ensure the image intensifier is draped sterilely.
- Pre-op Check: Before incision, confirm that clear, undistorted AP and lateral views can be obtained of the target joint, and critically, that the desired fusion angle can be accurately assessed.
Choosing the Optimal Fusion Angle
This is a critical decision, fellows, a compromise between appearance and function. The ideal posture should replicate the normal digital cascade. We need to achieve a position that allows functional pinch and grasp without creating an unsightly or obstructive deformity.
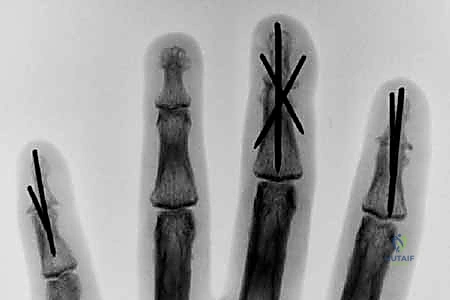
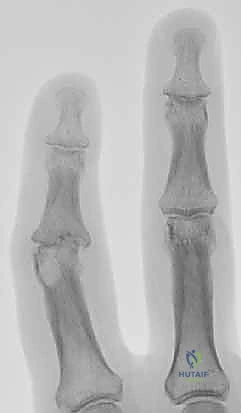
- DIP Joints and Thumb Interphalangeal Joint: These joints should generally be fused in 0 to 10 degrees of flexion. This allows for optimal tip-to-tip pinch and avoids impingement during grasp.
Figure 1: Recommended positions for digital joint fusion.
* PIP Joint:
* Some authors recommend a uniform 40-degree flexion position for all digits.
* Others recommend a cascade: 40 degrees for the index finger, progressing ulnarward in 5-degree increments to 55 degrees in the small finger.
* Clinical Pearl: Many surgeons prefer a slightly more extended position for the index PIP (e.g., 30-35 degrees) to optimize tip-to-tip pinch, which is crucial for this digit.
* Digital MCP Joints (Digits 2-5): The recommended fusion angle is a cascade from 25 degrees of flexion in the index digit, progressing ulnarward in 5-degree increments to 40 degrees in the small finger.
* Thumb MCP Joint: The recommended fusion angle is 10 to 15 degrees of flexion. This provides stability for pinch and power grip without hindering the crucial IP and CMC motion.
Selecting the Fixation Method
The choice of surgical technique depends on several factors: the specific joint, implant availability and cost, adequacy of bone stock, and surgeon comfort and experience. The ultimate goal is always to achieve a solid fusion in a timely manner. Bone preparation is essential, regardless of fixation.
- Kirschner Wire (K-wire) Fixation:
- Advantages: Simplicity of technique, ready availability, low-cost implants. Historically, fusion rates up to 99% have been reported.
- Disadvantages: Less rigid fixation, often requiring additional external immobilization (splint/cast) which can lead to stiffness in surrounding joints. Higher risk of infection (superficial pin site, deep wound, osteomyelitis). Potential for pin migration. Minimal compression across the fusion site, which is biomechanically less favorable.
- Interosseous Wiring:
- Advantages: Biomechanically stronger than K-wire fixation, especially useful for PIP and thumb IP fusion. Readily available, low-cost implants.
- Disadvantages: Requires a larger amount of soft tissue stripping for appropriate placement of drill holes, increasing the risk of soft tissue and tendon scarring. Has been associated with a higher rate of nonunion, up to 9%.
- Tension Band Fixation: This is a biomechanically superior method, often considered the gold standard for small joint arthrodesis.
- Mechanism: It combines parallel Kirschner wires for rotational control with interosseous wiring for compression. The genius of this
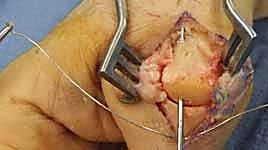
Additional Intraoperative Imaging & Surgical Steps






































REFERENCES
-
For the thumb MCP joint treated with tension band fixation, a protective custom-molded thermoplast hand-based MCP splint is used for about 6 weeks. Early IP joint motion is encouraged.
-
Allende B, Engelem JC. Tension-band arthrodesis in the finger joints. J Hand Surg Am 1980;5A:269–271.
-
Ayres JR, Goldstrohm GL, Miller GJ, et al. Proximal interphalangeal joint arthrodesis with the Herbert Screw. J Hand Surg Am 1988;13A: 600–603.
-
Brutus JP, Palmer AK, Mosher JF, et al. Use of a headless compressive screw for distal interphalangeal joint arthrodesis in digits: clinical outcome and review of complications. J Hand Surg Am 2006; 31A:85–89.
-
Buchler U, Aiken MA. Arthrodesis of the proximal interphalangeal joint by solid bone grafting and plate fixation in extensive injuries to the dorsal aspect of the finger. J Hand Surg Am 1988;13A:589–594.
-
Burton R, Margles SW, Lunseth PA. Small joint arthrodesis in the hand. J Hand Surg Am 1986;11A:678–682.
-
Carroll RE, Dick HM. Arthrodesis of the wrist for rheumatoid arthritis. J Bone Joint Surg Am 1971;53A:1365–1369.
-
Carroll RE, Hill NA. Small joint arthrodesis in hand reconstruction. J Bone Joint Surg Am 1969;51A:1219–1221.
-
Ijsselstein CB, van Egmond DB, Hovius SE, et al. Results of smalljoint arthrodesis: comparison of Kirschner wire fixation with tension band wire technique. J Hand Surg Am 1992;17A:952–956.
-
Kovach JC, Werner FW, Palmer AK, et al. Biomechanical analysis of internal fixation techniques for proximal interphalangeal joint arthrodesis. J Hand Surg Am 1986;11A:562–566.
-
Leibovic SJ, Strickland JW. Arthrodesis of the proximal interphalangeal joint of the finger: comparison of the use of the Herbert screw with other fixation methods. J Hand Surg Am 1994;19A: 181–188.
-
Lister G. Intraosseous wiring of the digital skeleton. J Hand Surg Am 1978;3A:427.
-
McGlynn J, Smith RA, Boqumill GP. Arthrodesis of small joint of the hand: a rapid and effective technique. J Hand Surg Am 1988;13A: 595–599.
-
In general, arthrodesis of the other MCP joints must be protected with a handor forearm-based splint, regardless of the type of fixation. Significant flexion and lateral stresses must be neutralized while simultaneously allowing for PIP and DIP motion. It may be necessary to splint the PIP joint in extension part-time to prevent an extensor lag from developing.
OUTCOMES
- Multiple studies have evaluated the biomechanical advantages of one type of surgical technique versus another in order to establish the most rigid type of fixation that will allow a rapid and complete arthrodesis.
-
A comparison between the failure load of a Herbert screw and the failure load of a tension band construct showed no significant difference between the two 2 ; the authors concluded that these two methods of fixation have similar biomechanical strength.
-
A comparison of multiple fixation techniques showed that arthrodesis by screw fixation had a better fusion rate than Kirschner wires, tension band construct, and plate fixation. 10
-
A comparison of tension band constructs versus Kirschner wire fixation for PIP joint arthrodesis concluded that tension bands provide more rigid fixation. 9
-
Moberg E. Arthrodesis of finger joints. Surg Clin North Am 1960;40: 465–470.
-
Shin A, Amadio P. Stiff finger joints. In: Green’s Operative Hand Surgery. Philadelphia: Elsevier, 2006:417–457.
-
Stern PJ, Fulton DB. Distal interphalangeal joint arthrodesis: an analysis of complications. J Hand Surg Am 1992;17A: 1139–1145.
-
Stern PJ, Gates NT, Jones TB. Tension band arthrodesis of small joints in the hand. J Hand Surg Am 1993;18A:194–197.
-
Tubiana R. Arthrodesis of the fingers. In: Tubiana R, ed. The Hand, vol
-
Philadelphia: WB Saunders, 1985.
-
Vanik RK, Weber RC, Matloub HS, et al. The comparative strengths of internal fixation techniques. J Hand Surg Am 1984;9A:216–221.
-
Wright CS, McMurtry RY. AO arthrodesis in the hand. J Hand Surg Am 1983;8A:932–935.
-
Wyrsch B, Dawson J Aufranc S, et al. Distal interphalangeal joint arthrodesis comparing tension-band wire and Herbert screw: a biomechanical and dimensional analysis. J Hand Surg 1996;21A:438–443.
You Might Also Like

