Mastering Glenoid Labral Tears and SLAP Lesions: An Evidence-Based Surgical Guide
Key Takeaway
Glenoid labral tears, particularly Superior Labrum Anterior and Posterior (SLAP) lesions, present significant diagnostic and therapeutic challenges in sports medicine. This comprehensive guide details the biomechanical foundations, pathoaetiology, and evidence-based surgical management of labral pathology. Utilizing the Snyder classification, we explore arthroscopic techniques ranging from simple debridement to complex suture anchor repairs and biceps tenodesis, optimizing outcomes for overhead athletes and degenerative populations alike.
Introduction to Glenoid Labral Pathology
The glenoid labrum is a critical fibrocartilaginous structure that serves as the cornerstone of glenohumeral stability. Pathology of the labrum, particularly Superior Labrum Anterior and Posterior (SLAP) lesions, represents a complex intersection of acute trauma, chronic microtrauma, and degenerative changes. For the orthopedic surgeon, mastering the diagnosis and management of glenoid labral tears requires a profound understanding of shoulder biomechanics, precise arthroscopic skills, and nuanced clinical decision-making tailored to the patient's physiological age and functional demands.
Anatomy and Biomechanics of the Glenoid Labrum
The glenoid labrum consists predominantly of dense fibrocartilaginous tissues interspersed with elastic fibers, allowing for both structural rigidity and dynamic deformation.
Histological and Structural Composition
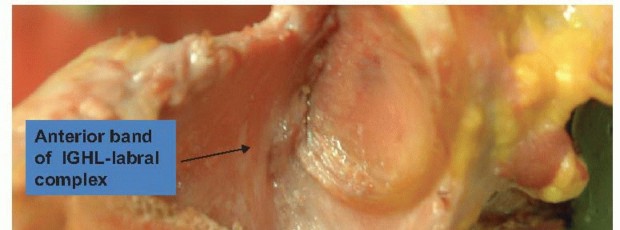
On its inner articular margin, the labrum is continuous with the hyaline cartilage of the glenoid fossa. On its outer peripheral margin, it blends seamlessly into the fibrous tissue of the joint capsule. The capsule and the glenohumeral ligaments—along with the long head of the biceps tendon (LHBT)—are intimately attached to and become an indistinguishable part of the glenoid labrum before inserting onto the bony glenoid.
Biomechanical Contributions to Stability
The labrum encircles the glenoid rim, functioning as a "chock-block" that significantly increases the depth and concavity of the glenoid fossa.
* Surface Area Augmentation: Landmark biomechanical studies by Saha demonstrated that the presence of the glenoid labrum increases the effective articular surface of the glenoid to 75% of the humeral head vertically and 57% horizontally.
* Contact Stress Distribution: Karzel et al., utilizing biomechanical testing of cadaveric shoulder specimens, proved that the labrum fundamentally alters the distribution of contact stresses across the joint when a compressive load is applied, particularly at 90 degrees of abduction.
* Concavity Compression: By deepening the socket, the labrum enhances the concavity compression effect, wherein the rotator cuff compresses the humeral head into the glenoid, resisting shear forces and preventing translation.
Clinical Pearl: The superior labrum and the biceps anchor function as a coupled biomechanical unit. Disruption of this complex not only causes localized pain but fundamentally alters glenohumeral kinematics, leading to microinstability and secondary rotator cuff overload.
Pathoaetiology and Mechanisms of Injury
The etiology of labral tears is multifactorial, encompassing acute traumatic events and repetitive microtraumatic forces. Compression, shear forces, and degenerative changes—exacerbated by decreased peripheral vascularity with advancing age—significantly increase the likelihood of labral failure.
Extrinsic Mechanisms
Extrinsic injuries are typically acute and secondary to sudden traction on the upper extremity. Classic examples include:
* Unexpectedly lifting a heavy object.
* Water skiing injuries (sudden traction on the tow rope).
* Falls onto an outstretched hand (FOOSH) resulting in superior compression and shear.
Intrinsic Mechanisms and the "Peel-Back" Phenomenon
Intrinsic injuries occur predominantly during the overhead throwing motion, which produces immense traction on the biceps anchor.
Burkhart and Morgan proposed the highly influential torsional peel-back mechanism. During the late cocking phase of throwing, the shoulder is placed in maximum abduction and external rotation. In this position, the vector of the biceps tendon shifts posteriorly, creating a torsional force that "peels back" the posterior superior labrum from the glenoid rim.
Topographical Classification of the Glenoid Labrum
To standardize communication and aid in localizing the exact site of labral injury, the glenoid labrum is divided into six distinct anatomical zones:
- Superior Labrum
- Anterior Labrum (above the midglenoid notch)
- Anterior Labrum (below the midglenoid notch)
- Inferior Labrum
- Posteroinferior Labrum
- Posterosuperior Labrum
The "Equator" Concept
A critical diagnostic heuristic involves the "equator" of the glenoid—an imaginary horizontal line drawn between the 3-o’clock and 9-o’clock positions.
* Above the Equator: Lesions located in the superior hemisphere are frequently associated with rotator cuff pathology or biceps tendon disease (e.g., SLAP lesions).
* Below the Equator: Lesions located in the inferior hemisphere—most commonly split, nondetached lesions anteriorly (Bankart) and posteriorly (Reverse Bankart)—are highly pathognomonic for overt shoulder instability.
Evolution of Surgical Management
Historically, the management of superior labral lesions relied heavily on arthroscopic debridement. Andrews and Carson initially described superior labral lesions in throwing athletes, reporting 88% good to excellent results with simple debridement in short-term follow-ups.
However, long-term outcome studies revealed a stark deterioration of these results over time. Altchek et al. conducted a pivotal study evaluating anterosuperior, anteroinferior, and posteroinferior labral debridement. They found that while 72% of patients experienced symptomatic relief during the first postoperative year, only 7% maintained significant relief at the 2-year follow-up mark. This high failure rate catalyzed the shift toward anatomical repair and the development of comprehensive classification systems.
The Snyder Classification of SLAP Lesions
Snyder revolutionized the understanding of superior labral pathology by coining the term SLAP (Superior Labrum Anterior to Posterior) lesions. He categorized them into four primary types, plus a complex variety, which dictate specific treatment algorithms.
Type I SLAP Lesion
- Pathology: Characterized by degenerative fraying of the superior labrum. Crucially, the peripheral labral attachment and the biceps tendon anchor remain solidly attached to the supraglenoid tubercle.
- Treatment: Simple arthroscopic debridement of the frayed edges to prevent mechanical catching. Repair is contraindicated as the anchor is stable.
Type II SLAP Lesion
- Pathology: The most common SLAP variant. Involves a pathological detachment of both the superior labrum and the biceps anchor from the superior glenoid rim. These lesions frequently progress posterior to the biceps anchor.
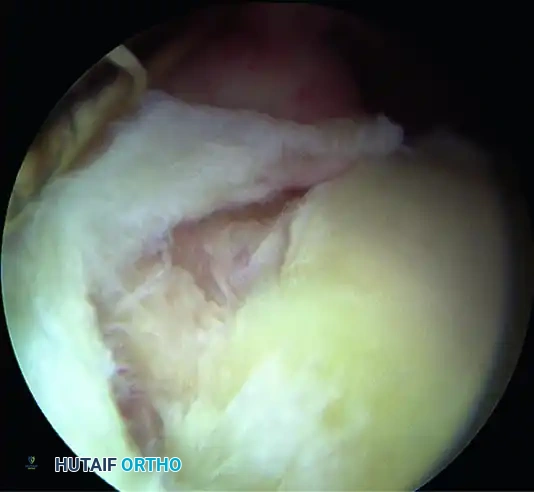
- Biomechanics & Diagnosis: Pagnani et al. demonstrated that Type II lesions cause a significant increase in anteroposterior and superoinferior glenohumeral translation in laboratory settings. Clinically, while they may not produce overt gross instability, they result in profound "microinstability" symptoms. The diagnosis is confirmed intraoperatively via the Peel-Back Test: The arm is removed from traction and placed in 90 degrees of abduction. As the shoulder is externally rotated to 90 degrees, the detached labrum is observed displacing medially over the scapular neck.
- Treatment Algorithm: Type II lesions must be addressed to prevent further destabilization.
- Patients < 35 Years Old: Arthroscopic repair using suture anchors and knot-tying (or knotless) techniques is the gold standard. Kim et al. reported 94% satisfactory results in this demographic.
- Patients > 50 Years Old: Older patients exhibit diminished healing potential, a higher risk of postoperative stiffness, and persistent pain following repair. In this demographic, biceps tenodesis (with or without labral debridement) yields vastly superior and more predictable clinical outcomes.
Type III SLAP Lesion
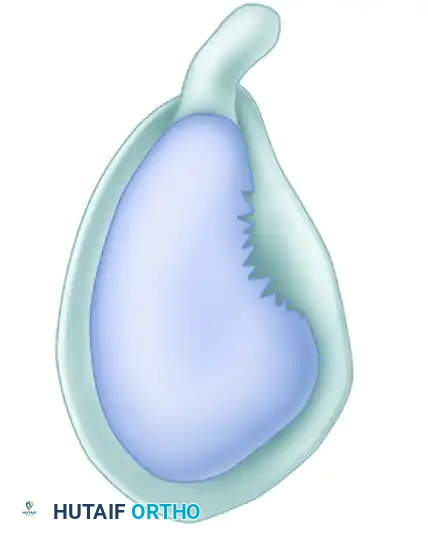
- Pathology: A vertical tear within the substance of the labrum that produces a displaced "bucket-handle" fragment. The biceps anchor and the peripheral labral attachment remain securely fixed to the bone.
- Treatment: The bucket-handle fragment acts as a mechanical irritant within the joint. Provided the biceps anchor is probed and confirmed to be absolutely stable, the treatment of choice is arthroscopic excision (resection) of the torn meniscoid fragment.
Type IV SLAP Lesion
- Pathology: A bucket-handle tear of the superior labrum that extends proximally into the substance of the long head of the biceps tendon. The biceps anchor itself is partially destabilized by the split.
- Treatment Algorithm: Management depends on the percentage of biceps tendon involvement and patient age.
- < 30% Tendon Involvement: The labral fragment and the involved portion of the tendon can be safely excised.
- ~ 33% Tendon Involvement (Young Patient): Snyder suggests primary suture repair of the torn biceps segment alongside labral repair.
- > 33% Tendon Involvement (Older Patient): Resection of the labral tear combined with a primary biceps tenodesis is highly recommended to eliminate the damaged tendon as a pain generator.
Complex SLAP Lesions
- Pathology: A combination of two or more of the standard SLAP categories (e.g., a Type II detachment combined with a Type III bucket-handle tear).
- Treatment: The surgical strategy is modular. The surgeon must repair the Type II detachment to restore the biceps anchor stability, followed by careful resection of the bucket-handle or frayed components.
Surgical Warning: Over-tensioning a SLAP repair, particularly posterior to the biceps anchor, can severely restrict external rotation. Always tie knots with the arm in neutral to slight external rotation to avoid capturing the capsule and inducing iatrogenic stiffness.
Operative Technique: Arthroscopic SLAP Repair
Patient Positioning and Anesthesia
Surgery is typically performed under general anesthesia supplemented with an interscalene regional block for postoperative pain control. The patient may be positioned in either the Beach Chair or Lateral Decubitus position.
* Lateral Decubitus provides excellent visualization of the superior and inferior labrum due to longitudinal and lateral traction.
* Beach Chair allows for an easier transition to open procedures (if necessary) and provides a more anatomical orientation of the shoulder girdle, which is preferred by many surgeons performing concomitant biceps tenodesis.
Portal Placement
- Standard Posterior Portal: Used for initial diagnostic arthroscopy.
- Anterosuperior Portal: Placed high in the rotator interval, just anterior to the biceps tendon. Used for viewing and instrumentation.
- Anteroinferior Portal: Placed just above the subscapularis tendon.
- Wilmington Portal (Optional but Recommended): Placed posterolaterally (1 cm anterior and 1 cm lateral to the posterolateral corner of the acromion). This portal provides the optimal trajectory for anchor placement in the posterosuperior glenoid (the most common site of Type II peel-back).
Step-by-Step Repair (Type II Lesion)
- Diagnostic Arthroscopy & Debridement: Probe the biceps anchor. Perform the dynamic peel-back test. Debride any Type I fraying using an arthroscopic shaver.
- Bed Preparation: Use an arthroscopic elevator or rasp to mobilize the detached labrum. The superior glenoid neck must be decorticated using a motorized burr or rasp down to bleeding cancellous bone to optimize the biological healing environment.
- Anchor Placement: Introduce a drill guide through the appropriate portal (often the Wilmington portal for posterior anchors). Drill and insert a bioabsorbable or all-suture anchor at the articular margin. Crucial: The anchor must be inserted at a 45-degree angle to the articular surface (the "deadman's angle") to maximize pull-out strength and prevent articular cartilage penetration.
- Suture Passage: Pass the sutures around the labrum using a suture shuttle device (e.g., crescent hook or penetrating grasper). Ensure a healthy bite of capsulolabral tissue is captured.
- Knot Tying: Tie the sutures using a sliding, locking knot followed by alternating half-hitches. Ensure the knot post is positioned on the capsular side, away from the articular surface, to prevent chondral abrasion. Knotless anchor constructs are increasingly popular to eliminate this risk entirely.
- Final Assessment: Probe the repair to confirm the restoration of the "chock-block" effect and the elimination of the peel-back sign.
Postoperative Rehabilitation Protocol
The success of a labral repair is heavily dependent on strict adherence to a phased rehabilitation protocol. The goal is to protect the healing fibrocartilage while preventing adhesive capsulitis.
Phase I: Maximum Protection (Weeks 0–4)
- Immobilization: The shoulder is immobilized in a sling.
- Range of Motion (ROM): Passive ROM only. Forward flexion is limited to 90 degrees. External rotation is limited to neutral (0 degrees) to protect the anterior/superior repair.
- Restrictions: Absolute avoidance of active biceps contraction (no active elbow flexion or supination) to prevent traction on the repaired anchor.
Phase II: Moderate Protection (Weeks 4–8)
- Sling: Discontinued at 4 weeks.
- ROM: Transition to Active-Assisted ROM (AAROM) and gradually to Active ROM (AROM). Gradual progression of external rotation.
- Strengthening: Begin submaximal isometric exercises for the rotator cuff and scapular stabilizers. Continue to avoid resisted biceps activity.
Phase III: Early Strengthening (Weeks 8–12)
- ROM: Achieve full, symmetric AROM by week 10.
- Strengthening: Initiate isotonic strengthening for the rotator cuff, deltoid, and periscapular musculature. Light, progressive biceps strengthening may commence at week 8-10.
Phase IV: Return to Sport (Months 3–6+)
- Advanced Strengthening: Plyometrics and kinetic chain integration.
- Throwing Athletes: Initiate an interval throwing program at 4 months, provided the patient has full, painless ROM and normal strength ratios. Full return to competitive overhead sports typically requires 6 to 9 months.
Conclusion
The management of glenoid labral tears demands a rigorous, evidence-based approach. While historical reliance on simple debridement proved inadequate for long-term relief, the advent of the Snyder classification and modern arthroscopic repair techniques has dramatically improved patient outcomes. By carefully selecting patients—reserving anatomical repair for younger, active individuals and utilizing biceps tenodesis for the older, degenerative population—orthopedic surgeons can reliably restore glenohumeral stability, alleviate pain, and return patients to their highest levels of function.
📚 Medical References
- glenoid labral tears in athletes, Arthroscopy 11:42, 1995.
- Treacy SH, Savoie FH III, Field LD: Arthroscopic treatment of multidirectional instability, J Shoulder Elbow Surg 8:345, 1999.
- Tytherleigh-Strong G, Hirahara A, Miniaci A: Rotator cuff disease, Curr Opin Rheumatol 13:135, 2001.
- Uhthoff HK, Lohr J, Sarker K: The pathogenesis of rotator cuff tears. Paper presented at the Third International Conference on Surgery of the Shoulder. Fukuora, Japan, 1986.
- Urbaniak JR, Hansen PE, Beissinger SF, et al: Correction of post-traumatic fl exion contracture of the elbow by anterior capsulotomy, J Bone Joint Surg 67A:1160, 1985.
- Vick CW, Bell SA: Rotator cuff tears: diagnosis with sonography, Am J Radiol 154:121, 1990.
- Visotsky JL, Basamania C, Seebauer L, et al:
You Might Also Like