Advanced Management of Cuff Tear Arthropathy and Adhesive Capsulitis
Key Takeaway
Cuff tear arthropathy represents the end-stage manifestation of massive, irreparable rotator cuff tears, characterized by superior humeral head migration and glenohumeral arthritis. This comprehensive guide details the biomechanical collapse inherent to this condition and outlines evidence-based surgical interventions, including reverse total shoulder arthroplasty. Additionally, it explores the diagnostic criteria, triphasic clinical progression, and targeted management strategies for primary adhesive capsulitis, providing orthopedic surgeons with essential clinical protocols.
CUFF TEAR ARTHROPATHY
End-stage rotator cuff disease leads to a complex and debilitating entity known as cuff tear arthropathy (CTA). Originally described by Charles Neer, CTA is characterized by the triad of a massive, irreparable rotator cuff tear, superior migration of the humeral head, and progressive glenohumeral osteoarthritis.
Pathomechanics and Biomechanical Collapse
The glenohumeral joint relies on a delicate balance of force couples for stability and function. In the coronal plane, the inferiorly directed vector of the supraspinatus and the remaining rotator cuff muscles counterbalances the superiorly directed shear force of the deltoid. Due to a massive rotator cuff tear, the normal humeral head depression provided by the supraspinatus is lost.
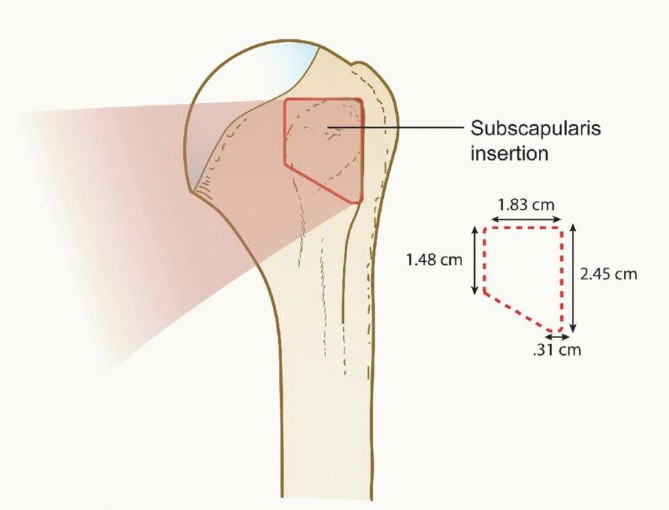
As the disease progresses, the unopposed pull of the deltoid drives the humeral head superiorly. This superior migration results in articulation between the humeral head and the coracoacromial (CA) arch. Over time, this abnormal articulation leads to "acetabularization" of the acromion and "femoralization" of the humeral head. The loss of the transverse force couple (subscapularis anteriorly and infraspinatus/teres minor posteriorly) further destabilizes the joint, leading to anterosuperior escape of the humeral head, severe functional deficit, and pseudoparalysis (an inability to actively elevate the arm beyond 90 degrees despite intact axillary nerve function).
Clinical Pearl: The integrity of the coracoacromial arch is paramount in patients with massive rotator cuff tears. An ill-advised acromioplasty or release of the CA ligament in a patient with a massive tear removes the secondary restraint to superior migration, rapidly accelerating the progression to severe cuff tear arthropathy and anterosuperior escape.
Radiographic Evaluation: The Hamada Classification
The progression of CTA is classically staged using the Hamada classification, based on weight-bearing anteroposterior (AP) radiographs:
* Grade 1: Massive rotator cuff tear with an acromiohumeral interval (AHI) > 6 mm.
* Grade 2: AHI ≤ 5 mm (superior migration).
* Grade 3: Acetabularization of the acromion (concave deformity of the acromial undersurface).
* Grade 4: Glenohumeral joint space narrowing (osteoarthritis).
* Grade 5: Humeral head collapse (osteonecrosis secondary to CTA).
Surgical Management Strategies
Operative treatment of cuff tear arthropathy generally involves arthroplasty in various forms. Because of the aforementioned shear forces that can lead to eccentric glenoid wear and catastrophic "rocking horse" loosening of a standard glenoid component, irreparable rotator cuff tears are an absolute contraindication to conventional anatomic total shoulder arthroplasty.
CTA Hemiarthroplasty
Humeral head replacement (hemiarthroplasty) with maintenance of the coracoacromial arch has been used extensively in the past and remains a durable solution for specific low-demand patients. Newer prosthetic designs feature an extended articular surface with a lateral extension over the greater tuberosity. This design improves articulation with the acromion and avoids impingement from the greater tuberosity during abduction. While hemiarthroplasty provides reliable pain relief, improvements in active forward elevation and functional kinematics are often unpredictable.
Reverse Total Shoulder Arthroplasty (rTSA)
The reverse total shoulder arthroplasty is the modern gold standard treatment for patients with irreparable rotator cuffs and/or rotator cuff arthropathy. It is particularly beneficial for patients with anterosuperior escape or subluxation of the humeral head and clinical pseudoparalysis.
The rTSA relies on the biomechanical principles pioneered by Paul Grammont. The glenoid is resurfaced with a baseplate (metaglene) and a convex sphere (glenosphere), while the humeral head is replaced with a concave bearing surface to form a semi-constrained articulation. This design achieves two critical biomechanical alterations:
1. Medialization of the Center of Rotation: Decreases the torque on the glenoid component and recruits more deltoid muscle fibers for elevation.
2. Distalization of the Humerus: Tensions the deltoid, increasing its resting length and optimizing its moment arm.
In this manner, a stable fulcrum is reestablished at the ball-socket interface, and the deltoid is empowered to drive forward elevation independently of the deficient rotator cuff.
Surgical Approach and Closure (Anterosuperior Approach)
While the deltopectoral approach is standard for most shoulder arthroplasties, the anterosuperior (Mackenzie) approach is occasionally utilized for CTA hemiarthroplasty or specific rTSA techniques, particularly when addressing superior pathology. This approach requires splitting the anterior deltoid and detaching a portion of its origin from the anterior acromion.
Surgical Warning: If an anterosuperior approach is utilized, meticulous repair of the deltoid origin is the most critical step of the procedure. Postoperative deltoid dehiscence in the setting of a reverse shoulder arthroplasty is a catastrophic, often irreparable complication.
Closure Protocol:
* Irrigate the joint copiously to remove all bone debris and cement fragments.
* Reattach the deltoid and the coracoacromial ligaments securely to the acromion. This must be performed using transosseous drill holes through the anterior acromion.
* Pass nonabsorbable No. 2 sutures (e.g., FiberWire or Ethibond) through the transosseous tunnels and incorporate the full thickness of the deltoid fascia and the CA ligament.
* Tie the sutures securely, ensuring a watertight, robust repair of the deltoid origin against the bleeding bone of the acromion.
* Close the subcutaneous tissue and skin incision in the usual manner.
Postoperative Care and Rehabilitation
The postoperative protocol following arthroplasty for CTA must balance the need for early motion with the protection of soft tissue repairs (especially the subscapularis in a deltopectoral approach or the anterior deltoid in an anterosuperior approach).
- Immobilization and Pain Control: The upper extremity of the patient is supported in a commercially available shoulder sling immobilizer. A single-shot or 3-day continuous interscalene nerve block can be placed preoperatively for optimal pain control, and a cold therapy device can be used as desired to minimize edema and narcotic consumption.
- Phase I (0-4 Weeks): The initial objective is to obtain and maintain the maximal range of passive glenohumeral flexion and rotation while the deltoid muscle heals to the acromion (if detached) or the subscapularis heals to the lesser tuberosity. Active motion is strictly prohibited.
- Phase II (4-8 Weeks): When the initial glenohumeral motion has been obtained and soft tissue healing is secure, active-assisted range of motion (AAROM) is initiated.
- Phase III (8+ Weeks): Strengthening of the deltoid (especially the anterior portion), the remaining intact muscles of the rotator cuff, and the scapular stabilizers becomes the focus of therapy.
- Return to Activity: Return to full, unrestricted activity usually requires 4 to 6 months. Patients are counseled to avoid heavy lifting (>15 lbs) indefinitely to prolong the survivorship of the rTSA construct.
ADHESIVE CAPSULITIS (FROZEN SHOULDER)
While cuff tear arthropathy represents a structural collapse of the shoulder, adhesive capsulitis (commonly referred to as frozen shoulder) is a profound inflammatory and fibrotic condition of the glenohumeral joint capsule. The pathophysiology and treatment are fundamentally different from CTA. These conditions perhaps should be considered more of an arthrofibrosis, characterized by fibroblastic proliferation and multicytokine-mediated capsular contracture.
Diagnostic Criteria and Clinical Presentation
There are no universally accepted, rigid criteria for the diagnosis of frozen shoulder; however, the clinical pattern is highly characteristic. The hallmark of adhesive capsulitis is a severe, global loss of both active and passive range of motion.
We have noted that internal rotation frequently is lost initially, followed by a progressive loss of flexion and external rotation. Most often, our patients present with a specific clinical triad:
1. They can internally rotate only to the sacrum.
2. They have a 50% or greater loss of external rotation (especially with the arm at the side, indicating contracture of the coracohumeral ligament and rotator interval).
3. They have less than 90 degrees of active and passive abduction.
We include these patients in the diagnosis of frozen shoulder, but we have no formal inclusion criteria beyond this classic restrictive pattern.
Imaging and Diagnostic Modalities
Diagnostic tests in patients with a frozen shoulder are utilized primarily to rule out other pathologies (such as osteoarthritis, avascular necrosis, or locked posterior dislocations).
- Radiographs: Plain film radiographs usually are normal, except in patients with underlying medical disorders such as diabetes mellitus or thyroid disease, which may show incidental osteopenia from disuse.
- Bone Scans: Technetium-99m bone scans have been reported to be positive in some patients, demonstrating increased periarticular uptake. A positive bone scan has been shown to have a positive predictive value for successful treatment with intra-articular steroid injections.
- Magnetic Resonance Imaging (MRI): MRI has shown an increased blood flow to the synovium and thickening of the coracohumeral ligament (CHL) and joint capsule in the axillary recess. However, its primary value is in evaluating the other structures in the shoulder to eliminate other pathological conditions, such as occult rotator cuff tears.
- Arthrography: Arthrograms characteristically show a drastically reduced joint volume with irregular, contracted margins. A normal shoulder accepts 15 to 20 mL of fluid. A volume of less than 10 mL and a lack of filling of the axillary fold currently are accepted arthrographic findings indicative of a frozen shoulder. Clinical improvement has been reported after arthrography because of the brisement (rupture) of adhesions from forcefully injecting fluid into the joint (hydrodilatation).
The Triphasic Clinical Course of Primary Frozen Shoulder
The clinical course of primary (idiopathic) frozen shoulder is classically described as consisting of three distinct, overlapping phases. Secondary frozen shoulders (e.g., post-traumatic, post-surgical) may not exhibit all three phases and may not follow the exact chronology. Although treatment for the two entities often is similar, the underlying cause for the secondary frozen shoulder should be identified and treated as well.
Phase I — Pain (The "Freezing" Phase)
Patients usually have a gradual onset of diffuse shoulder pain, which is progressive over weeks to months. The pain usually is worse at night and is exacerbated by lying on the affected side. Inflammatory cytokines (such as TGF-beta and TNF-alpha) drive intense synovitis. As the patient uses the arm less due to pain, early capsular contracture leading to stiffness ensues.
Phase II — Stiffness (The "Frozen" Phase)
Patients seek pain relief by restricting movement. This heralds the beginning of the stiffness phase, which usually lasts 4 to 12 months. The synovitis begins to burn out, replaced by dense fibroplasia and collagen deposition. Patients describe profound difficulty with activities of daily living; men have trouble getting to their wallets in their back pockets, and women have trouble with fastening brassieres. As stiffness progresses, a dull ache is present nearly all the time (especially at night), and this often is accompanied by sharp, sudden pain during range of motion at or near the new, restricted end points of motion.
Phase III — Thawing
This phase lasts for weeks or months, and as motion gradually increases, pain diminishes. Without treatment (other than benign neglect), motion return is gradual in most but may never objectively return to normal. Long-term follow-up studies indicate that up to 40% of patients have some persistent, measurable loss of motion. However, most patients subjectively feel near normal, perhaps as a result of compensation or adjustment in ways of performing activities of daily living.
Treatment Algorithms
Traditionally, frozen shoulder has been considered a self-limiting condition, lasting 12 to 18 months without long-term sequelae. However, because approximately 10% of patients have long-term, severe functional deficits, and the duration of disability is unacceptable to many, active intervention is frequently warranted.
Non-Operative Management
- Physical Therapy: Gentle, sustained stretching is the cornerstone of treatment. Aggressive, painful stretching during Phase I is contraindicated as it exacerbates synovitis.
- Corticosteroid Injections: Intra-articular glenohumeral injections provide rapid, albeit sometimes temporary, relief of pain and inflammation, particularly when administered during Phase I.
- Hydrodilatation: As noted, forceful injection of saline and local anesthetic can rupture capsular adhesions, providing immediate improvements in volume and motion.
Operative Management
When non-operative modalities fail after 3 to 6 months of compliant therapy, surgical intervention is considered.
* Manipulation Under Anesthesia (MUA): A controlled, short-lever-arm manipulation is performed to rupture the inferior capsule.
* Arthroscopic Capsular Release: For refractory cases, or in diabetic patients who historically respond poorly to MUA alone, a 360-degree arthroscopic capsular release is the gold standard. This involves electrothermal ablation of the rotator interval, release of the coracohumeral ligament, and sequential release of the anterior, inferior, and posterior capsule, ensuring precise restoration of kinematics without the risk of iatrogenic fracture associated with aggressive MUA.
📚 Medical References
- cuff tear arthropathy, J Shoulder Elbow Surg 9:169, 2000.
- Total Shoulder Arthroplasty Arroyo JS: Surgical technique and results. In Crosby LA, ed: Total shoulder arthroplasty, Rosemont Ill, 2000, American Academy of Orthopaedic Surgeons. Barrett WP, Thornhill TS, Thomas WH, et al: Nonconstrained total shoulder arthroplasty in patients with polyarticular rheumatoid arthritis, J Arthroplasty 4:91, 1989.
- Baumgarten KM, Lashgari CJ, Yamaguchi K: Glenoid resurfacing in shoulder arthroplasty: indications and contraindications, Instr Course Lect 53:3, 2004.
- Bell RH, Noble JS: The management of signifi cant glenoid defi ciency in total shoulder arthroplasty, J Shoulder Elbow Surg 9:248, 2000.
- Boardman ND III, Cofi eld RH, Bengtson KA, et al: Rehabilitation after total shoulder arthroplasty, J Arthroplasty 16:483, 2001.
- Boileau P, Avidor C, Krishnan SG, et al: Cemented polyethylene versus uncemented metal-backed glenoid components in total shoulder arthroplasty: a prospective, double-blind, randomized study, J Shoulder Elbow Surg 11:351, 2002.
- Brems JJ: Rehabilitation following total shoulder arthroplasty, Clin Orthop Relat Res 307:70, 1994.
- Brenner BC, Ferlic DC, Clayton ML, et al: Survivorship of unconstrained total shoulder arthroplasty, J Bone Joint Surg 71A:1289, 1989.
- Brown DD, Friedman RJ: Postoperative rehabilitation following total shoulder arthroplasty, Orthop Clin North Am 29:535, 1998.
- Burroughs PL, Gearen PF, Petty WR, et al: Shoulder arthroplasty in the young patient, J Arthroplasty 18:792, 2003.
- Cameron B, Galatz L, Williams GR Jr: Factors affecting the outcome of total shoulder arthroplasty, Am J Orthop 30:613, 2001.
- Cofi eld RH: Total shoulder arthroplasty with the Neer prosthesis, J Bone Joint Surg 66A:899, 1984.
- Cofi eld RH: Uncemented total shoulder arthroplasty, Clin Orthop Relat Res 307:86, 1994.
- Cofi eld RH: Total shoulder replacement: managing bone defi ciencies. In Craig EV, ed: Master techniques in orthopaedic surgery: the shoulder, Philadelphia, 1995, Lippincott. Collins D, Tencer A, Sidles J, Matsen F: Edge displacement and deformation of glenoid components in response to eccentric loading. The effect of preparation of the glenoid bone, J Bone Joint Surg 74A:501, 1992.
- Craig EV: Total shoulder replacement. In Chapman M, ed:
You Might Also Like